 Mingming Xu1†
Mingming Xu1† Hang Zhou
Hang Zhou Ruihao Zhang
Ruihao Zhang Yang Pan
Yang Pan Xiaoqiang Liu
Xiaoqiang Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 06 December 2023
Sec. Obesity
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1301284
Background: The risk of visceral obesity on erectile function has recently attracted much attention. The visceral adiposity index (VAI) is a brief and reliable indicator of visceral obesity measurement. Nevertheless, the association between VAI and erectile dysfunction (ED) is not completely clarified.
Methods: Data from NHANES 2001–2004 were enrolled in this study. Erectile function was assessed by a database-self-administered questionnaire. VAI was calculated with body mass index (BMI), waist circumference (WC), triglyceride (TG), and high-density lipoprotein (HDL) cholesterol. The weighted logistic regression model was performed to evaluate the association between VAI and ED.
Results: Ultimately, 3380 participants were enrolled in the study, including 900 with ED and 2480 without ED. Compared to participants without ED, those with ED generally had higher levels of VAI (1.76 vs. 1.53). The weighted logistic regression analyses demonstrated increased odds of developing ED in participants within the 4th quartile (Q4) of VAI compared to the 1st quartile (Q1) of VAI (OR = 2.023; 95% CI, 1.534–2.669; P < 0.001). Similar results were still obtained after adjusting for the relevant covariates (OR = 1.404; 95% CI, 1.008–1.954; P = 0.044). In subgroup analyses grouped by smoking status, higher VAI was associated with increased odds of developing ED only in the current smoking group (OR = 1.092; 95% CI, 1.021–1.167; P = 0.010).
Conclusion: This study indicated that higher VAI is independently related to ED risk and that early intervention is necessary to reduce the progression of ED with high VAI levels.
Erectile dysfunction (ED) is the inability to attain and sustain an erection that is sufficiently satisfactory (1, 2). It is an extremely prevalent male disease that usually affects males over the age of 40 (1). It is estimated that about 322 million males will suffer from it by 2025 (3). The mechanism of ED is complex, involving the psychological, neurological, hormonal, and vascular systems. Endothelial dysfunction and sex hormone abnormalities are two of the most prominent aspects (4, 5). Old age, inadequate physical activity, abnormal lipid profiles, and obesity are strongly related to ED (6, 7). Some studies have shown that patients with ED normally have a higher waist circumference (WC) (8). ED is not only a sexual dysfunction but also has a potential association with cardiovascular disease. A large amount of evidence supports the view that ED may be an early predictor of cardiovascular disease (9).
The visceral adiposity index (VAI) has gained significant popularity as a precise and widely used index for assessing the distribution and function of visceral fat in contemporary times (10). It stands out as an innovative index, as it combines both physical measurements and metabolic markers. The determination of VAI necessitates the integration of body mass index (BMI), waist circumference (WC), triglyceride (TG), and high-density lipoprotein (HDL) cholesterol by means of a mathematical equation (11). Amato et al. demonstrated that an increase in VAI was tightly tied to cardiometabolism. Furthermore, a large cohort study from Beijing, China, suggested that VAI was an independent risk factor for diabetic nephropathy in the Chinese population (12). In addition, a considerable body of research has shown that higher VAI is positively associated with female sexual dysfunction (13, 14).
Several previous studies have analyzed the association between VAI and ED (15, 16). The findings showed that the mean VAI of the ED group was greater than that of the non-ED group. However, the number of participants in these studies was extremely small. Therefore, this study was further analyzed with data from a large sample of the National Health and Nutrition Examination Survey (NHANES). And hopefully, more reliable evidence between VAI and ED will be available.
The National Health and Nutrition Examination Survey (NHANES) is a multifaceted study undertaken by the U.S. government to comprehensively assess the health and nutritional status of the population (17). The wealth of data obtained through NHANES serves as a crucial resource for researchers and healthcare professionals, empowering them to make well-informed decisions pertaining to public health and nutrition. Because the NHANES database is publicly accessible, no additional ethics are needed. NHANES data from 2001–2004 were used in this study because only these two survey cycles contained the information from the ED questionnaire. Participants with missing information on ED, VAI, and related covariates were removed from this study, and the detailed process was described in the flowchart (Figure 1).
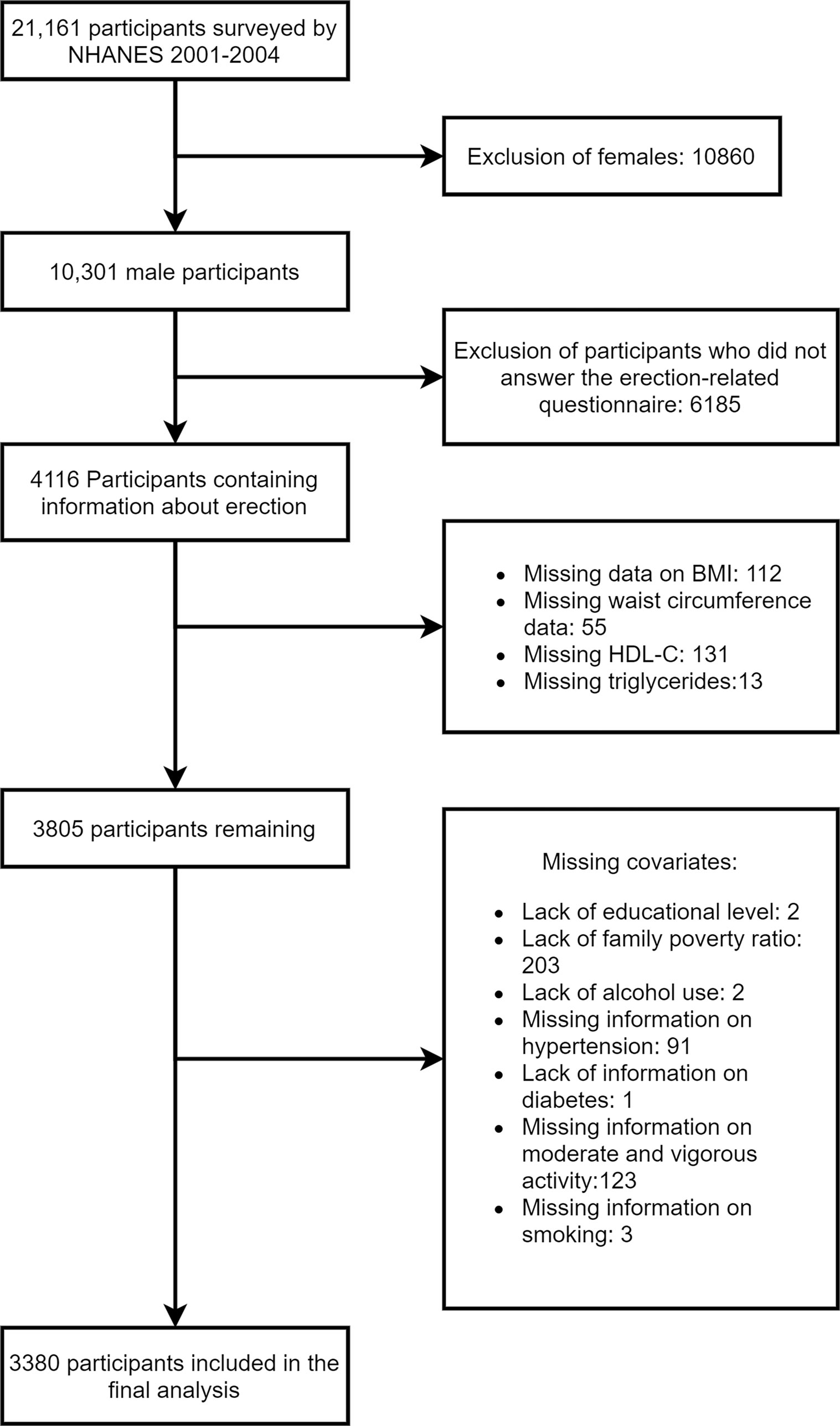
Figure 1 Research flow chart for the present study.
VAI was the main exposure factor in this study. It was calculated by combining waist circumference, BMI, triglycerides, and HDL. For males, the formula for its calculation was as follows: (WC/(39.68+(1.88×BMI))) × (TG/1.03) × (1.31/HDL).
In NHANES data, EDs were typically ascertained through a self-report format. Specifically, it was assessed via questions in a questionnaire: How would you describe your ability to get and keep an erection adequate for satisfactory intercourse? Participants who answered “sometimes able” or “never able” were usually considered to be ED.
To further assess the association between VAI and ED, this study adjusted for nine relevant covariates: age, diabetes, hypertension, smoking, moderate physical activity, vigorous physical activity, alcohol use, education level, and family poverty ratio. Hypertension was operationally defined as meeting one of the following criteria: systolic blood pressure equal to or exceeding 140 mmHg, diastolic blood pressure equal to or exceeding 90 mmHg, or a self-reported diagnosis of hypertension by medical personnel. Diabetes was assessed based on a questionnaire. In the past 30 days, having done any vigorous activity for at least 10 minutes was defined as vigorous activity. similarly seen in moderate activity. Alcohol use was defined as the consumption of a minimum of 12 alcoholic beverages within a one-year period.
Continuous variables were commonly expressed as the mean (standard deviation, SD) or median (interquartile range, IQR). Categorical variables were then expressed in terms of numbers (percentage). The t-test, Mann-Whitney U test, and chi-square test were performed to compare the analysis between the different groups. In the context of statistical analysis, a p-value that is lower than 0.05 is deemed to possess significant statistical relevance. To further analyze the association between VAI and ED, univariate and multivariate logistic regression models were constructed in this study. Finally, all analyses in this study were based on SPSS 26 and Stata 15 software.
In the final analysis, a total of 3380 participants were included, with comprehensive details of all individuals provided in Table 1. Notably, the group with ED exhibited a significantly higher age compared to the group without ED (68.00 vs. 42.00). Moreover, a relatively elevated proportion of participants within the ED group displayed comorbidities such as hypertension, diabetes, and physical inactivity when compared to their counterparts without ED (Table 1). Furthermore, the ED group demonstrated a higher VAI compared to the non-ED group (1.76 vs. 1.53) (Table 1).
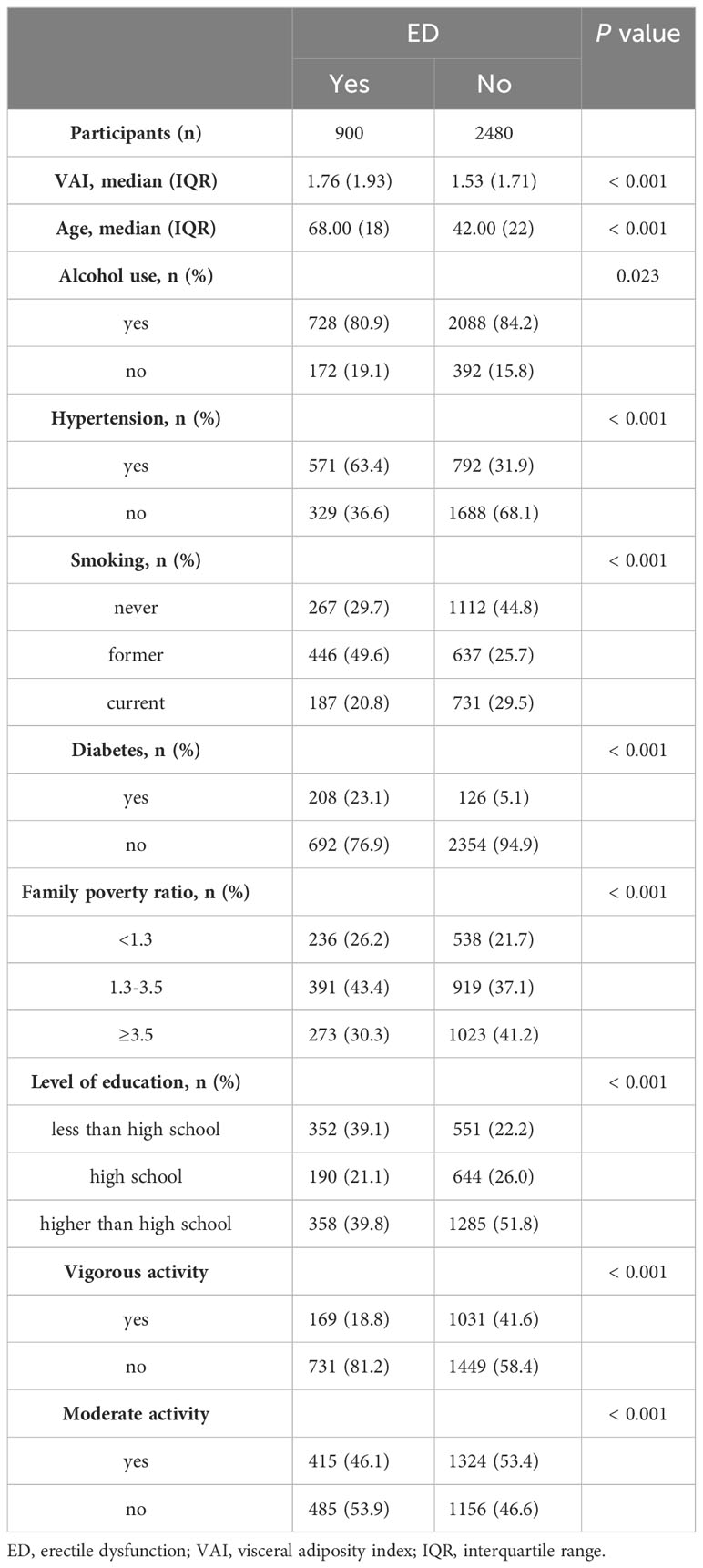
Table 1 Demographic features of the participants in this study.
In univariate analysis, the present study observed increased odds of developing ED in participants within the 4th quartile (Q4) of VAI compared to the 1st quartile (Q1) of VAI (OR = 2.023; 95% CI, 1.534–2.669; P < 0.001). Even after adjusting for pertinent covariates, the observed findings persisted, and all of them demonstrated statistically significant associations (OR = 1.404; 95% CI, 1.008–1.954; P = 0.044) (Table 2).
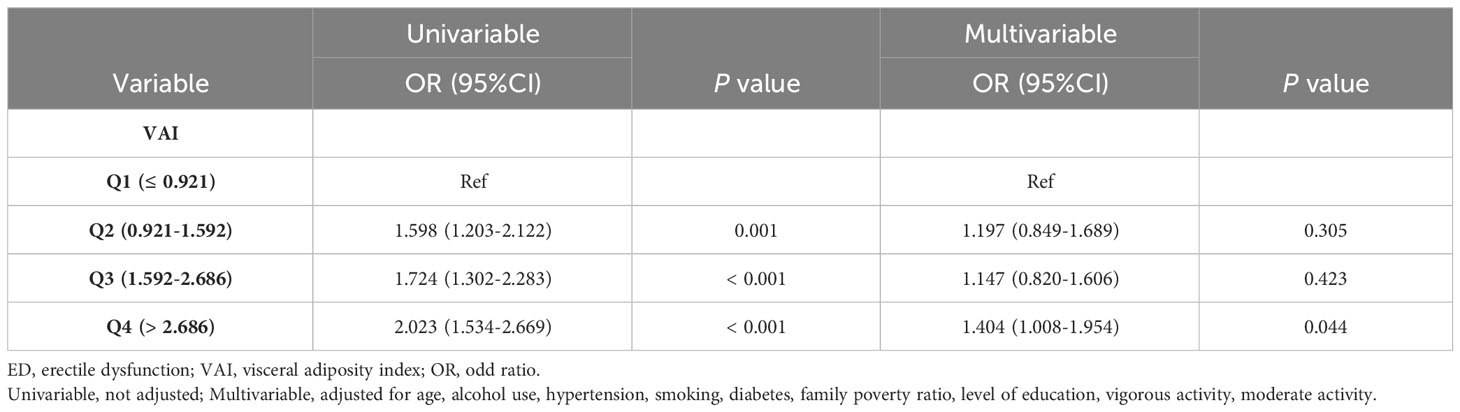
Table 2 Association between VAI and ED.
In subgroup analyses grouped by smoking status, higher VAI was associated with increased odds of developing ED only in the current smoking group (Table 3). In addition, grouping by family poverty ratio, we found that VAI was associated with ED and was statistically significant in the group with a family poverty ratio greater than or equal to 3.5 (Table 3).

Table 3 Subgroup analysis.
Visceral obesity represents a form of central obesity that is more hazardous. A large body of evidence suggests that visceral obesity increases the risk of cardiovascular disease to some extent. Some studies have shown that visceral obesity predisposes to venous thrombosis (18). In addition, a study from Turkey showed that visceral obesity is strongly associated with poor semen parameters (19). Visceral fat area (VFA) and VAI are key indicators for assessing visceral obesity (20). However, VFA is more complex and costly to measure, making VAI a better choice. VAI is widely used as a reliable indicator of visceral obesity to explore the relationship between disease risk. However, the association between VAI and ED remains to be investigated.
This study analyzed the relationship between VAI and ED in the US population on the basis of data from NHANES. For the current analysis, we observed that VAI was higher in the ED group than in the non-ED group. The current findings align with the outcomes of prior research investigations (15). In addition, the regression results showed that higher VAI was associated with increased odds of having ED, and similar findings remained after fully adjusting for covariates. These results indicate that VAI is probably an independent risk factor for ED.
However, the underlying mechanisms of VAI and ED remained to be investigated, but several explanations might exist. VAI is a reliable indicator of visceral fat accumulation and functional metabolic dysfunction. Visceral obesity has been shown to lead to endothelial dysfunction. And a randomized controlled trial in the United States demonstrated that increased visceral fat can lead to endothelial dysfunction even in a healthy young population of normal weight (21). Weight loss would improve the situation to a greater extent. In addition, animal experiments have confirmed that bariatric surgery improves endothelial function by attenuating IFNγ-mediated inflammation in visceral fat (22). In parallel to the effects on endothelial function, obesity typically provokes a decrease in testosterone levels, which may be associated with hypothalamic-pituitary-testicular (HPT) axis suppression and insulin resistance (23). Furthermore, Sebo et al. found a significant increase in adiposity in denuded mice, and when supplemented with testosterone, the increase in visceral fat was inhibited and fat distribution was regulated (24). Caretta et al. (25) found a strong negative correlation between VAI and TT levels and that high VAI was strongly associated with hypogonadism in men with type 2 diabetes. At the same time, dyslipidemia may cause damage to peripheral nerves, of which diabetic peripheral neuropathy is a classic example (26). Not only can dyslipidemia lead to nerve damage, but it can also contribute to ED by damaging smooth muscle cells (27).
Although a previous cross-sectional study initially confirmed that high VAI was independently associated with ED, that study had a particularly small sample size and did not adjust for major confounders, such as diabetes or physical activity (16). Hence, a larger sample of data is required for further analysis. And the present study precisely fills in the shortcomings of the previous study.
Specifically, this study has the following strengths. Firstly, our study was based on the data in NHANES, which has the advantage of a large sample size. Moreover, we adjusted for relevant covariates and performed subgroup analysis, which made the results of this study more robust. However, this study still had a few limitations. First, the determination of ED in this study was based on self-report, which was also a limitation of this database. Second, although we adjusted for covariates to the extent possible, there may be factors that were not controlled for.
In conclusion, this study indicated that higher VAI is independently related to ED risk and that early intervention is necessary to reduce the progression of ED with high VAI levels.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by NCHS Research Ethics Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MX: Conceptualization, Methodology, Writing – original draft. HZ: Data curation, Methodology, Writing – review & editing. ZR: Methodology, Writing – review & editing. YP: Investigation, Methodology, Writing – review & editing. XL: Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The research was financially supported by the National Natural Science Funds of China (82171594).
Thanks to the NHANES database and those who participated in the survey for their selflessness.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Najari BB, Kashanian JA. Erectile dysfunction. JAMA (2016) 316:1838. doi: 10.1001/jama.2016.12284
2. Shamloul R, Ghanem H. Erectile dysfunction. Lancet (2013) 381:153–65. doi: 10.1016/S0140-6736(12)60520-0
3. Ayta IA, McKinlay JB, Krane RJ. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int (1999) 84:50–6. doi: 10.1046/j.1464-410x.1999.00142.x
4. Bhasin S, Enzlin P, Coviello A, Basson R. Sexual dysfunction in men and women with endocrine disorders. Lancet (2007) 369:597–611. doi: 10.1016/S0140-6736(07)60280-3
5. Mitidieri E, Cirino G, d'Emmanuele di Villa Bianca R, Sorrentino R. Pharmacology and perspectives in erectile dysfunction in man. Pharmacol Ther (2020) 208:107493. doi: 10.1016/j.pharmthera.2020.107493
6. McMahon CG. Current diagnosis and management of erectile dysfunction. Med J Aust (2019) 210:469–76. doi: 10.5694/mja2.50167
7. Romano L, Pellegrino R, Sciorio C, Barone B, Gravina AG, Santonastaso A, et al. Erectile and sexual dysfunction in male and female patients with celiac disease: A cross-sectional observational study. Andrology (2022) 10:910–8. doi: 10.1111/andr.13186
8. Pizzol D, Smith L, Fontana L, Caruso MG, Bertoldo A, Demurtas J, et al. Associations between body mass index, waist circumference and erectile dysfunction: a systematic review and META-analysis. Rev Endocr Metab Disord (2020) 21:657–66. doi: 10.1007/s11154-020-09541-0
9. Terentes-Printzios D, Ioakeimidis N, Rokkas K, Vlachopoulos C. Interactions between erectile dysfunction, cardiovascular disease and cardiovascular drugs. Nat Rev Cardiol (2022) 19:59–74. doi: 10.1038/s41569-021-00593-6
10. He S, Yang J, Li X, Gu H, Su Q, Qin L. Visceral adiposity index is associated with lung function impairment: a population-based study. Respir Res (2021) 22:2. doi: 10.1186/s12931-020-01599-3
11. Amato MC, Giordano C, Galia M, Criscimanna A, Vitabile S, Midiri M, et al. Visceral Adiposity Index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care (2010) 33:920–2. doi: 10.2337/dc09-1825
12. Wu Z, Yu S, Kang X, Liu Y, Xu Z, Li Z, et al. Association of visceral adiposity index with incident nephropathy and retinopathy: a cohort study in the diabetic population. Cardiovasc Diabetol (2022) 21:32. doi: 10.1186/s12933-022-01464-1
13. Asci R, Bolat MS, Dündar C, Özdemir AZ, Atmaca A. Impact of a high visceral adiposity index on female sexual dysfunction in sexually active women? Results cross-sectional study. Int J Clin Pract (2021) 75:e14611. doi: 10.1111/ijcp.14611
14. Sahin Y, Karacan T, Hacibey I, Aybek OY, Ozer Z, Cil G, et al. High visceral adiposity index is associated with female orgasmic disorder in premenopausal women: a cross-sectional study. J Obstet Gynaecol (2022) 42:2121–6. doi: 10.1080/01443615.2022.2033185
15. Dursun M, Besiroglu H, Cakir SS, Otunctemur A, Ozbek E. Increased visceral adiposity index associated with sexual dysfunction in men. Aging Male (2018) 21:187–92. doi: 10.1080/13685538.2017.1406468
16. Bolat MS, Kocamanoglu F, Ozbek ML, Buyukalpelli R, Asci R. Can high visceral adiposity index be a risk factor for sexual dysfunction in sexually active men? J Sex Med (2020) 17:1926–33. doi: 10.1016/j.jsxm.2020.06.014
17. Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES dietary data: focus on collection, release, analytical considerations, and uses to inform public policy. Adv Nutr (2016) 7:121–34. doi: 10.3945/an.115.009258
18. Morange PE, Alessi MC. Thrombosis in central obesity and metabolic syndrome: mechanisms and epidemiology. Thromb Haemost (2013) 110:669–80. doi: 10.1160/TH13-01-0075
19. Turan E, Öztekin Ü. Relationship between visceral adiposity index and male infertility. Andrologia (2020) 52:e13548. doi: 10.1111/and.13548
20. Xu Z, Liu Y, Yan C, Yang R, Xu L, Guo Z, et al. Measurement of visceral fat and abdominal obesity by single-frequency bioelectrical impedance and CT: a cross-sectional study. BMJ Open (2021) 11:e048221. doi: 10.1136/bmjopen-2020-048221
21. Romero-Corral A, Sert-Kuniyoshi FH, Sierra-Johnson J, Orban M, Gami A, Davison D, et al. Modest visceral fat gain causes endothelial dysfunction in healthy humans. J Am Coll Cardiol (2010) 56:662–6. doi: 10.1016/j.jacc.2010.03.063
22. Zhang H, Wang Y, Zhang J, Potter BJ, Sowers JR, Zhang C. Bariatric surgery reduces visceral adipose inflammation and improves endothelial function in type 2 diabetic mice. Arterioscler Thromb Vasc Biol (2011) 31:2063–9. doi: 10.1161/ATVBAHA.111.225870
23. Fui MN, Dupuis P, Grossmann M. Lowered testosterone in male obesity: mechanisms, morbidity and management. Asian J Androl (2014) 16:223–31. doi: 10.4103/1008-682X.122365
24. Sebo ZL, Rodeheffer MS. Testosterone metabolites differentially regulate obesogenesis and fat distribution. Mol Metab (2021) 44:101141. doi: 10.1016/j.molmet.2020.101141
25. Caretta N, Facondo P, Mereu S, Delbarba A, Crepaldi MC, Vedovato M, et al. Cardiometabolic indices predict hypogonadism in male patients with type 2 diabetes. J Endocrinol Invest (2023) 46:599–608. doi: 10.1007/s40618-022-01941-0
26. Iqbal Z, Bashir B, Ferdousi M, Kalteniece A, Alam U, Malik RA, et al. Lipids and peripheral neuropathy. Curr Opin Lipidol (2021) 32:249–57. doi: 10.1097/MOL.0000000000000770
Keywords: erectile dysfunction, visceral adiposity index, NHANES, cross-sectional study, male
Citation: Xu M, Zhou H, Zhang R, Pan Y and Liu X (2023) Correlation between visceral adiposity index and erectile dysfunction in American adult males: a cross-sectional study based on NHANES. Front. Endocrinol. 14:1301284. doi: 10.3389/fendo.2023.1301284
Received: 28 September 2023; Accepted: 23 November 2023;
Published: 06 December 2023.
Edited by:
Takayoshi Ubuka, International Cancer Laboratory Co., Ltd., JapanReviewed by:
Achille Aveta, University of Naples Federico II, ItalyCopyright © 2023 Xu, Zhou, Zhang, Pan and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoqiang Liu, eGlhb3FpYW5nbGl1MUAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.