 Weixiang He
Weixiang He Ting Ding
Ting Ding Zhiping Niu
Zhiping Niu Chunlin Hao1
Chunlin Hao1 Weijun Qin
Weijun Qin- 1Department of Urology, Xijing Hospital, The Fourth Military Medical University, Xi’an, China
- 2Department of Clinical Laboratory Medicine, Xijing Hospital, The Fourth Military Medical University, Xi’an, China
- 3Department of Environmental Health, School of Public Health, Fudan University, Shanghai, China
Context: Surgical treatment is important for male lower urinary tract symptom (LUTS) management, but there are few reviews of the risks of reoperation.
Objective: To systematically evaluate the current evidence regarding the reoperation rates of surgical treatment for LUTS in accordance with current recommendations and guidelines.
Evidence acquisition: Eligible studies published up to July 2023, were searched for in the PubMed® (National Library of Medicine, Bethesda, MD, USA), Embase® (Elsevier, Amsterdam, the Netherlands), and Web of Science™ (Clarivate™, Philadelphia, PA, USA) databases. STATA® (StataCorp LP, College Station, TX, USA) software was used to conduct the meta-analysis. Random-effects models were used to calculate the pooled incidences (PIs) of reoperation and the 95% confidence intervals (CIs).
Evidence synthesis: A total of 119 studies with 130,106 patients were included. The reoperation rate of transurethral resection of the prostate (TURP) at 1, 2, 3, and 5 years was 4.0%, 5.0%, 6.0%, and 7.7%, respectively. The reoperation rate of plasma kinetic loop resection of the prostate (PKRP) at 1, 2, 3, and 5 years was 3.5%, 3.6%, 5.7%, and 6.6%, respectively. The reoperation rate of holmium laser enucleation of the prostate (HoLEP) at 1, 2, 3, and 5 years was 2.4%, 3.3%, 5.4%, and 6.6%, respectively. The reoperation rate of photoselective vaporization of the prostate (PVP) at 1, 2, 3, and 5 years was 3.3%, 4.1%, 6.7%, and 7.1%, respectively. The reoperation rate of surgery with AquaBeam® at 1, 2, 3, and 5 years was 2.6%, 3.1%, 3.0%, and 4.1%, respectively. The reoperation rate of prostatic artery embolization (PAE) at 1, 2, 3, and 5 years was 12.2%, 20.0%, 26.4%, and 23.8%, respectively. The reoperation rate of transurethral microwave thermotherapy (TUMT) at 1, 2, 3, and 5 years was 9.9%, 19.9%, 23.3%, and 31.2%, respectively. The reoperation rate of transurethral incision of the prostate (TUIP) at 5 years was 13.4%. The reoperation rate of open prostatectomy (OP) at 1 and 5 years was 1.3% and 4.4%, respectively. The reoperation rate of thulium laser enucleation of the prostate (ThuLEP) at 1, 2, and 5 years was 3.7%, 7.7%, and 8.4%, respectively.
Conclusion: Our results summarized the reoperation rates of 10 surgical procedures over follow-up durations of 1, 2, 3, and 5 years, which could provide reference for urologists and LUTS patients.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO, identifier CRD42023445780.
Introduction
Lower urinary tract symptoms (LUTSs) related to benign prostatic hyperplasia (BPH) are very common in older men and seriously affect their quality of life (1). Although α1-adrenoceptor antagonists and 5α-reductase inhibitors are first-line drugs with good efficacy, many adverse events such as dizziness, asthenia, postural hypotension, and low libido may occur as a result of treatment with them (1). In addition, there are some patients who have poor drug responsiveness or for whom these drugs are eventually unable to delay disease progress. Therefore, many patients ultimately require surgical intervention (1). According to the current guidelines, indications of the need for surgery include renal insufficiency, refractory urinary retention, recurrent urinary tract infections (UTIs) or gross hematuria, bladder stones, or the patient being refractory to or unwilling to use other therapies (2, 3). Transurethral resection of prostate (TURP) has long been considered the “gold standard” for the surgical management of LUTSs/BPH (4). In recent decades, many new technologies and procedures have been widely used and recommended by clinical guidelines, such as plasma kinetic resection of prostate (PKRP), holmium laser enucleation of the prostate (HoLEP), and photoselective vaporization of the prostate (PVP) (2, 3). Based on the current guidelines, the most suitable type of surgery for a patient depends on their prostate volume (PV), physical condition, and economic situation, and can also even be dependent on the preference of the surgeon and the machines owned by the hospital (2, 3).
Since the physical characteristics of the surgical technique and the anatomy of the prostate vary across patients, some may suffer bladder neck contracture (BNC), urethral stricture, or other complex complications postoperatively, and these may need surgical retreatment (1). In addition, some surgical procedures do not provide patients with satisfactory relief from their symptoms, or do not prevent the reappearance of bladder outlet obstruction over time after surgery, which may also require surgical retreatment. Moreover, some recommended surgical procedures are still under investigation such as surgery with AquaBeam® and prostatic artery embolization (PAE), of which the efficacy, safety, and tolerability still need to be confirmed (3). When selecting an appropriate surgical approach, knowledge of the reoperation rates could be used to predict the cost and management of disease in the years following the operation.
In the past, many studies have reported on the reoperation rate after various kinds of surgery. For patients who had undergone TURP, an Austrian nationwide study reported that the retreatment rate at the 1-year follow-up was 3.7%, and that this increased by approximately 1%–2% with each subsequent year (5, 6). A recent study reported that the rate of secondary surgery for TURP, transurethral incision of prostate (TUIP), and PVP at the 5-year follow-up was 10.3%, 13.6%, and 11.6%, respectively (7). Other procedures such as PAE and transurethral microwave thermotherapy (TUMT) were reported to have a higher risk of retreatment (8, 9). Recently, a systematic review also summarized the pharmacologic and surgical retreatment rates after newer office-based treatments, including water vapor thermal therapy (WVTT), prostatic urethral lift (PUL), and that using a temporarily implanted nitinol device (iTIND) (10). However, there is still a limited number of reviews on the reoperation rate of common surgeries recommended by the guidelines. We therefore conducted an updated systematic review and meta-analysis to summarize the reoperation rates of common surgical treatment for LUTSs/BPH. This review could be important to both BPH/LUTS patients and urologists when they are selecting an appropriate surgical procedure.
Methods
Literature search
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (11). The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (registration number CRD42023445780).
Studies were searched for in the PubMed® (National Library of Medicine, Bethesda, MD, USA), Embase® (Elsevier, Amsterdam, the Netherlands), and Web of Science™ (Clarivate™, Philadelphia, PA, USA) databases up to July 2023. The primary outcomes were the rates of surgical retreatment during follow-up. The search strategy is provided in the Supplementary Files. The initial screening, which included reading the title and abstract, was performed by the two authors independently (WXH and TD). Subsequently, the full text of potentially relevant studies was acquired for further confirmation and the data extraction process. Any conflicts that arose between the two authors during article selection and data extraction were resolved through discussion with an arbitrator (ZPN).
Inclusion and exclusion criteria
Articles that met the following criteria were included: (1) those that reported on the surgical retreatment rate of BPH/LUTS patients who had undergone operations in hospitals during the follow-up period; (2) those that were focused only on procedures recommended in the recent guidelines of the Association of University Administrators (AUA) and the European Association of Urology (EAU), including TURP, PKRP, TUIP, open prostatectomy (OP), thulium:yttrium aluminum garnet laser (Tm : YAG), enucleation of the prostate (ThuLEP), HoLEP, PVP, surgery with AquaBeam, PAE, and TUMT; (3) those that reported on a randomized controlled trial (RCT), non-randomized prospective study, or retrospective study; (4) those that were original peer-reviewed human participant research studies; (5) those that were published in English; and (6) those with a follow-up duration of 1, 2, 3, or 5 years. Studies such as reviews, editorials, commentaries, meeting abstracts of unpublished studies, and case reports were excluded. For duplicate publications, the higher-quality study, or the study that had been most recently published was selected.
Data extraction
Data were extracted from eligible studies by the two authors independently (WXH and TD). The extracted data included the first author’s surname, publication year, country of research, study design, patient information, follow-up time, and rates of surgical retreatment. The patient information collected included the patient’s number, age, prostate volume (PV), International Prostate Symptom Score (IPSS), postvoid residual volume (PVR), and maximum urinary flow rate (Qmax). It should be noted that surgical retreatment included both the management of the prostatic obstruction and of postoperative complications such as bladder neck contracture or urethral stricture. For some studies, we calculated the rate for further investigation if authors reported only the number of retreatment patients.
Quality assessment
The risk of bias (RoB) and quality of each eligible study were assessed by two authors independently (WXH and TD). For RCTs, the RoB was assessed, summarized, and then visualized using the Cochrane Collaboration RoB tool embedded in the RevMan (The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen, Denmark) software (version 5.4). For single-arm studies, the RoB was assessed in accordance with the EAU guidelines for systematic reviews (12).
Data synthesis
For each surgical type, the baseline characteristics of patients were summarized and then pooled using Microsoft Excel® (Microsoft Corporation, Redmond, WA, USA) software (2016). In addition, the pooled incidences (PIs) and corresponding 95% confidence intervals (CIs) of the surgical retreatment rates were evaluated and stratified by the surgical type and follow-up duration (i.e., 1 year, 2 years, 3 years, and 5 years) using STATA (version 17.0; StataCorp LP, College Station, TX, USA). A random-effects model was used to estimate the pooled incidences.
Results
Study selection and characteristics
The study selection process is presented in the PRISMA flow chart shown in Figure 1. A total of 119 studies met our inclusion criteria. The baseline characteristics of the included studies are presented in Table 1. A total of 130,106 patients were included, of whom 100,295 had undergone TURP, 1,530 had undergone PKRP, 90 had undergone TUIP, 4,621 had undergone OP, 3,956 had undergone HoLEP, 1,584 had undergone ThuLEP, 14,058 had undergone PVP, 217 had undergone surgery with AquaBeam, 1,796 had undergone PAE, and 1,959 had undergone TUMT procedures. Forty-two studies were RCTs, 29 were non-randomized prospective studies, and 48 were retrospective single-arm case series. Forty-nine studies were conducted in Europe, 34 were conducted in Asia, 22 studies were conducted in North America, six studies were conducted in Africa, and two studies were conducted in Oceania. In addition, another six multi-institutional studies were conducted in Europe and North America.
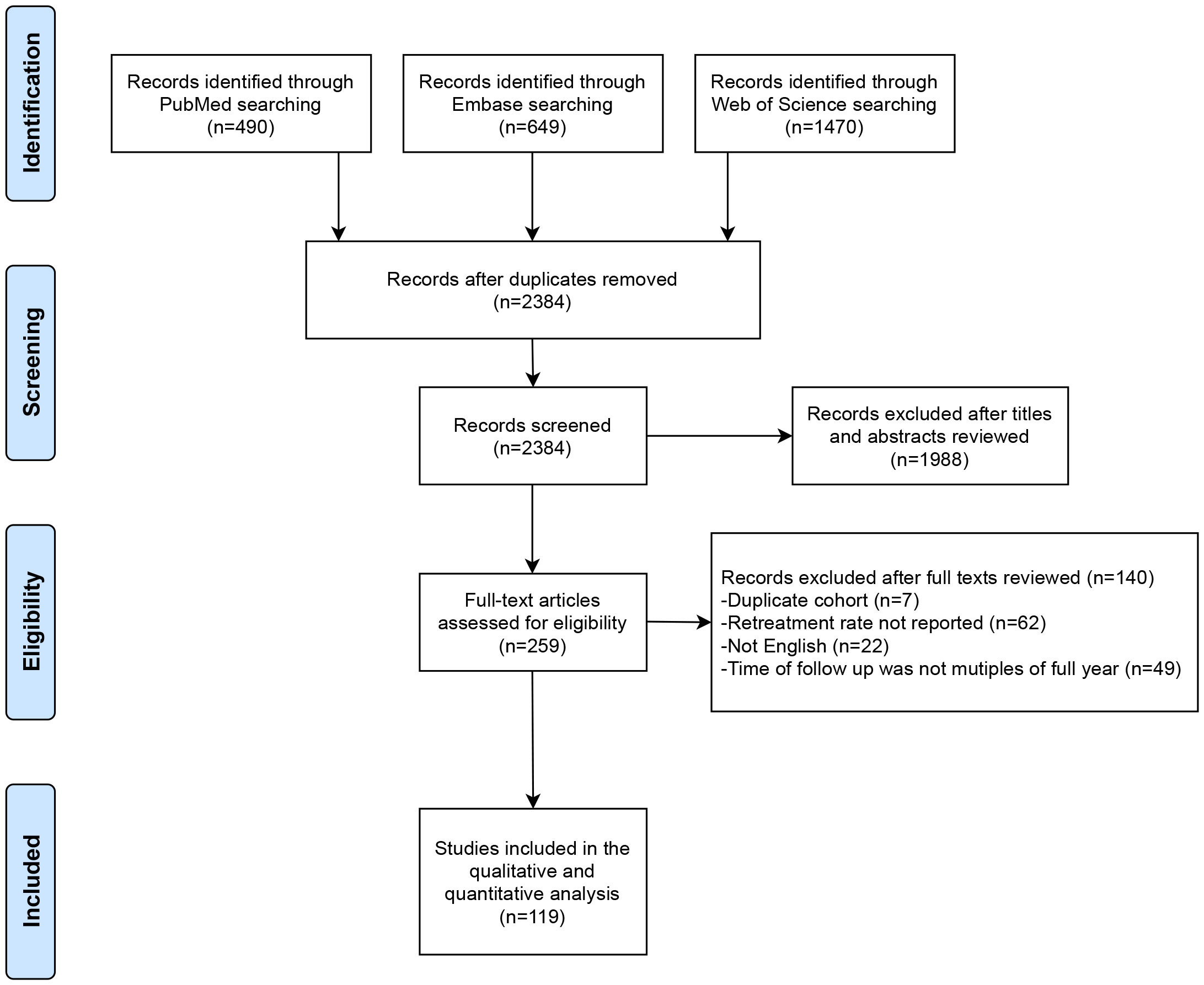
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.

Table 1 Study characteristics.
Risk of bias
The quality and RoB assessments are summarized in the Supplementary Files. For the 42 RCT studies, the RoBs of the 32 studies were considered unclear, whereas 47 of the 77 single-arm studies were assessed as having a high RoB.
Baseline patient characteristics
As shown in Table 2, the preoperative characteristics of the patients were summarized and pooled in accordance with the type of procedure. It appeared that the PV, IPSS, and PVR values of patients who had undergone TUIP, OP, or TUMT were different from those of other groups. For patients who had undergone TURP, the average age was 70 years, the average PV was 55 cm3, the average IPSS was 22, the average PVR was 184 mL, and the average Qmax was 8 mL per s. For patients who had undergone PKRP, the average age was 69 years, the average PV was 67 cm3, the average IPSS was 21, the average PVR was 112 mL, and the average Qmax was 7 mL per s. For patients who had undergone TUIP, the average age was 71 years, the average PV was 26 cm3, the average IPSS was 16, the average PVR was 139 mL, and the average Qmax was 9 mL per s. For patients who had undergone OP, the average age was 71 years, the average PV was 106 cm3, the average IPSS was 24, the average PVR was 147 mL, and the average Qmax was 6 mL per s. For patients who had undergone HoLEP, the average age was 70 years, the average PV was 79 cm3, the average IPSS was 21, the average PVR was 186 mL, and the average Qmax was 8 mL per s. For patients who had undergone ThuLEP, the average age was 70 years, the average PV was 65 cm3, the average IPSS was 24, the average PVR was 138 mL, and the average Qmax was 7 mL per s. For patients who had undergone PVP, the average age was 72 years, the average PV was 63 cm3, the average IPSS was 22, the average PVR was 166 mL, and the average Qmax was 8 mL per s. For patients who had undergone surgery with AquaBeam, the average age was 67 years, the average PV was 79 cm3, the average IPSS was 23, the average PVR was 117 mL, and the average Qmax was 7 mL per s. For patients who had undergone PAE, the average age was 66 years, the average PV was 86 cm3, the average IPSS was 22, the average PVR was 124 mL, and the average Qmax was 10 mL per s. For patients who had undergone TUMT, the average age was 67 years, the average PV was 48 cm3, the average IPSS was 21, the average PVR was 76 mL, and the average Qmax was 9 mL per s.
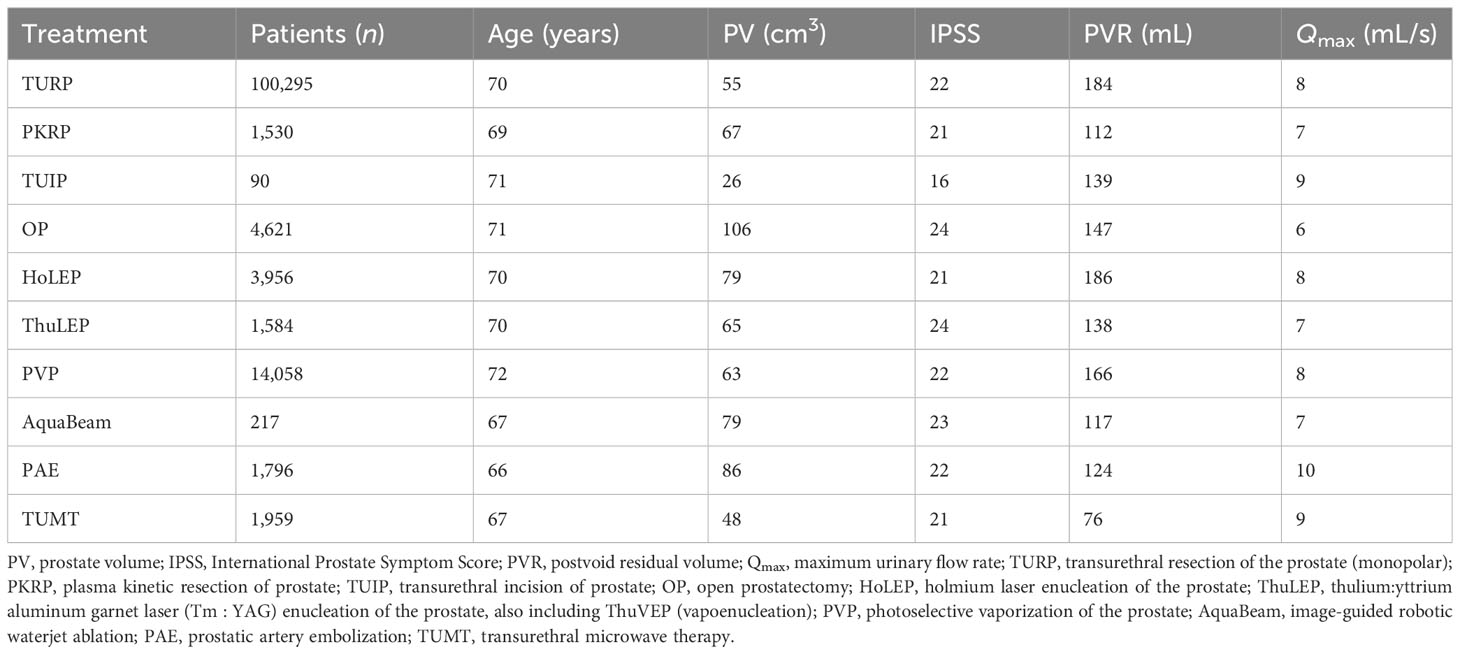
Table 2 Pooled estimates for baseline confounders.
Surgical retreatments after different procedures
In Table 3, the surgical retreatment rates of various procedures in different follow-up years are shown. Most of the evidence was derived from studies on TURP, PKRP HoLEP, and PVP, as there were fewer studies on TUIP, OP, ThuLEP, AquaBeam, PAE, and TUMT. For almost every procedure, the risk of surgical retreatment increased over time.
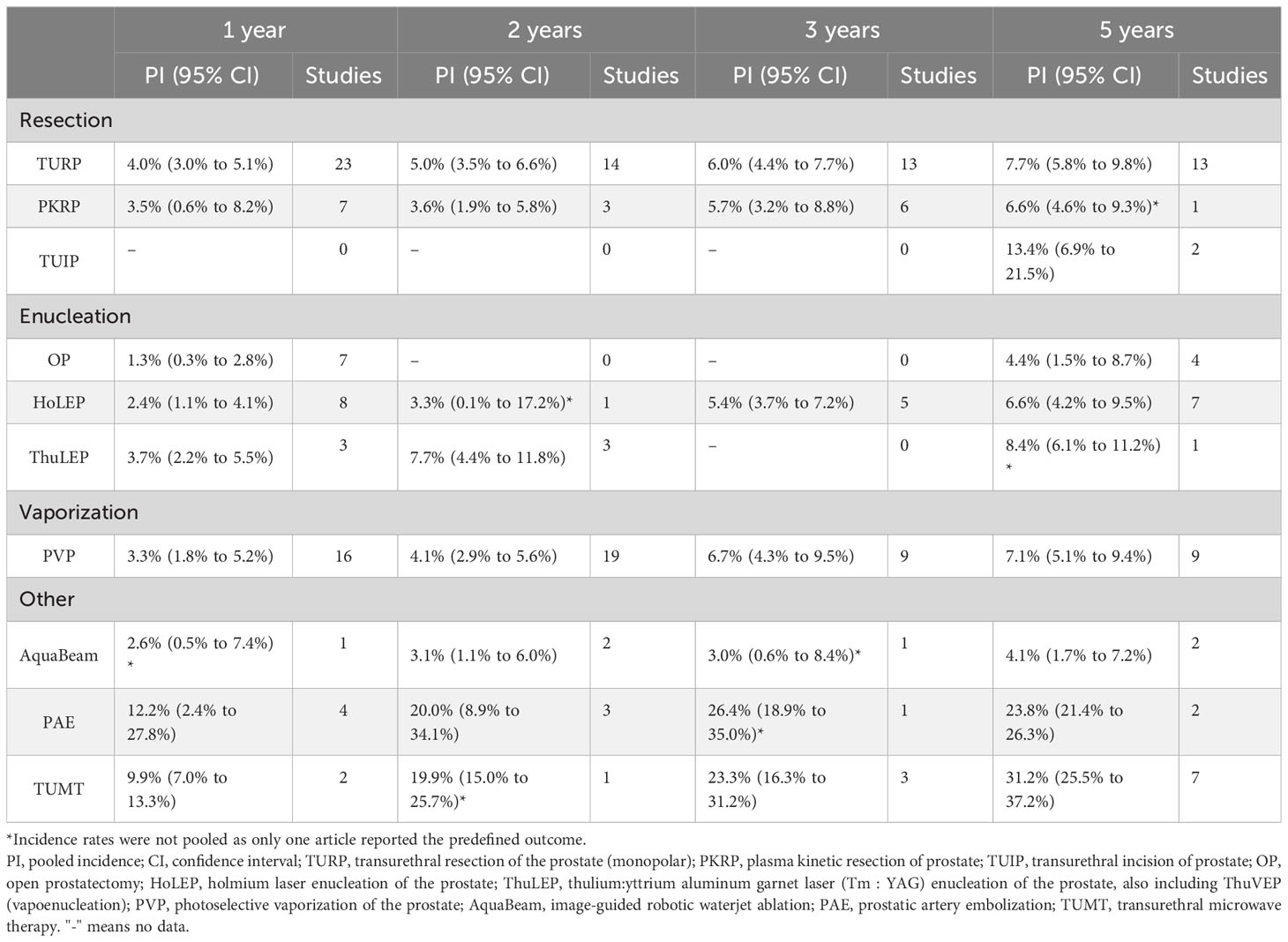
Table 3 Surgical retreatment after different operation procedures.
At 1 year, the pooled incidence of surgical retreatment was 4.0% (95% CI 3.0% to 5.1%) for the TURP cohort, 3.5% (95% CI 0.6% to 8.2%) for the PKRP cohort, 1.3% (95% CI 0.3% to 2.8%) for the OP cohort, 2.4% (95% CI 1.1% to 4.1%) for the HoLEP cohort, 3.7% (95% CI 2.2% to 5.5%) for the ThuLEP cohort, 3.3% (95% CI 1.8% to 5.2%) for the PVP cohort, 2.6% (95% CI 0.5% to 7.4%) for the AquaBeam cohort, 12.2% (95% CI 2.4% to 27.8%) for the PAE cohort, and 9.9% (95% CI 7.0% to 13.3%) for the TUMT cohort.
At 2 years, the pooled incidence of surgical retreatment was 5.0% (95% CI 3.5% to 6.6%) for the TURP cohort, 3.6% (95% CI 1.9% to 5.8%) for the PKRP cohort, 3.3% (95% CI 0.1% to 17.2%) for the HoLEP cohort, 7.7% (95% CI 4.4% to 11.8%) for the ThuLEP cohort, 4.1% (95% CI 2.9% to 5.6%) for the PVP cohort, 3.1% (95% CI 1.1% to 6.0%) for the AquaBeam cohort, 20.0% (95% CI 8.9% to 34.1%) for the PAE cohort, and 19.9% (95% CI 15.0% to 25.7%) for the TUMT cohort.
At 3 years, the pooled incidence of surgical retreatment was 6.0% (95% CI 4.4% to 7.7%) for the TURP cohort, 5.7% (95% CI 3.2% to 8.8%) for the PKRP cohort, 5.4% (95% CI 3.7% to 7.2%) for the HoLEP cohort, 6.7% (95% CI 4.3% to 9.5%) for the PVP cohort, 3.0% (95% CI 0.6% to 8.4%) for the AquaBeam cohort, 26.4% (95% CI 18.9% to 35.0%) for the PAE cohort, and 23.3% (95% CI 16.3% to 31.2%) for the TUMT cohort.
At 5 years, the pooled incidence of surgical retreatment was 7.7% (95% CI 5.8% to 9.8%) for the TURP cohort, 6.6% (95% CI 4.6% to 9.3%) for the PKRP cohort, 13.4% (95% CI 6.9% to 21.5%) for the TUIP cohort, 4.4% (95% CI 1.5% to 8.7%) for the OP cohort, 6.6% (95% CI 4.2% to 9.5%) for the HoLEP cohort, 8.4% (95% CI 6.1% to 11.2%) for the ThuLEP cohort, 7.1% (95% CI 5.1% to 9.4%) for the PVP cohort, 4.1% (95% CI 1.7% to 7.2%) for the AquaBeam cohort, 23.8% (95% CI 21.4% to 26.3%) for the PAE cohort, and 31.2% (95% CI 25.5% to 37.2%) for the TUMT cohort.
Discussion
This systematic review comprehensively summarized the reoperation rates after surgeries for male LUTS management. We found that the retreatment rates increased over time and differed among procedures. Our results can be used to counsel both the urologists and patients regarding the different therapeutic strategies.
As the gold standard of surgical treatment for BPH/LUTSs, it was reported after a nationwide analysis of 20,671 patients that the surgical retreatment rate of TURP was 3.7% for 1 year and 9.5% for 5 years (5), which was similar to our current result. As the most widely investigated alternative to TURP and PKRP (bipolar TURP) was found to have a comparable efficacy in regard to the long-term follow-up, but was safer during the perioperative period (3). Numerous studies have reported that PKRP exhibited similar rates of surgical retreatment as TURP (3), which was consistent with our results.
Moreover, TUIP was recommended for patients with a PV of < 30 mL and those without a middle lobe (2, 3). A meta-analysis of six trials published 13 years ago showed that reoperation was more common after TUIP (18.4%) than it was after TURP (7.2%) (128). The follow-up periods of the six trials included above were different, which may introduce some bias; however, our updated review showed a similar result in that the reoperation rate of TUIP was 13.4% in 5 years, which was higher among these surgical procedures. The higher risk of surgical retreatment associated with TUIP may be due to its method, which involves only incising the bladder outlet without removing prostatic tissue. However, TUIP has been underutilized in the urological community over the years, the reasons for this include concerns related to the limitations of PV as an indicator of the need for surgery and also its long-term efficacy (129). In contrast to TUIP, during OP, the whole prostate is removed, which is recommended for patients with a PV of > 80 mL (2, 3). A nationwide analysis reported that the surgical retreatment rate of OP was 3.0% for 1 year and 6.0% for 5 years (130), which was similar to our result. Although its long-term reoperation rate seems lower than those of the other procedures, OP showed poorer perioperative safety than the other transurethral approaches, and was associated with higher rates of blood transfusions and even death (131, 132). Therefore, OP was less popular than the other minimally invasive surgeries. However, in recent years, prostatectomy with laparoscopy or robot-assisted surgery showed better safety and were also recommended by guidelines (2).
As an alternative to open enucleation, some studies reported that HoLEP has a lower risk of reoperation than TURP or PKRP (59, 133, 134), whereas another reported that there was no difference (135, 136). Indeed, our results suggest that the reoperation rates for HoLEP are similar to (and possibly slightly lower than) those for TURP or PKRP. Enucleation using another laser, ThuLEP has a rate of reoperation that is similar to (and possibly slightly higher than) that of HoLEP, which may be due to them being similar procedures. A recent interesting study from Italy reported that an improved ThuLEP technique successfully preserved the ejaculation function in most patients (137), which suggested its potential in decreasing the reoperation rates.
For vaporization, PVP has been used in clinical settings for many years and there are many related studies that have shown it has a similar efficacy to TURP (2, 3). A previous meta-analysis published by Zhou and colleagues reported that the reoperation rate after PVP was higher than that after TURP (138). However, there were only three related trials included in Zhou’s study, and the follow-up durations of these trials were different (138). Our current summarized results, which included 53 trials, reported that the reoperation rates are similar between PVP and TURP. The difference between the results of these two meta-analyses may be due to the number of articles included.
AquaBeam has come under investigation in recent years and two related trails, WATER and WATER II, reported the reoperation rate associated with it (50, 117, 118). However, there are few studies on this technique and a lack of long-term follow-up data. Although the rate of surgical retreatment appeared to be better than other procedures in our current review, whether or not AquaBeam could be an alternative to traditional procedures still needs a lot of studies and long-term follow-up to be carried out. Previous studies indicate that PAE, another surgical procedure that remains under investigation, has a higher risk of surgical retreatment than that shown in our results (9). Due to the variability of blood supply to the human prostate, non-target embolization may occur, and secondary surgical retreatment is required (139). In addition, it takes time for the prostate to shrink after vessel embolization, and PV will also stop decreasing and begin to increase after a period of time (140). Therefore, both complications and insufficient treatment response may result in a higher risk of reoperation. Overall, the efficacy and reliability of PAE remain undetermined, and further investigations and improvements are still needed. TUMT, one of the earliest technologies used for the treatment of BPH/LUTSs, has been used and studied less in recent years, due to its higher risk of retreatment and the emergence of newer, minimally invasive technologies (2, 8). Our current results confirmed that it has a higher rate of surgical retreatment. In fact, TUMT was not recommended by the latest version of the EAU guidelines, whereas the AUA guidelines still suggest that this is a reasonable approach. However, considering its higher reoperation rate and the newer, minimally invasive technologies, TUMT will likely be displaced within the next several years (2, 141).
There are some limitations or shortcomings in our current analysis and review which must be acknowledged. First, RoB was in some of the studies included through assessment. Second, our review focused only on the reoperation rates at follow-up periods of 1, 2, 3, and 5 years. However, the follow-up duration was different among studies; examples of follow-up periods were 6 months, 4 years, long term (> 5 years), and some did not last for a ‘regular’ (i.e., a multiple of a year, half a year, or 1 year) length of time. Therefore, our results are limited by the lack of data obtained during these follow-up durations. Third, 10 surgical procedures were included in our current review, of which the indication that recommended by guidelines are different. The baseline characteristics and therapeutic outcomes of patients may also have varied. Meanwhile, the great difference between data retrieved across techniques may also have led to bias. Fourth, the risk of misestimating the reoperation rate must be noted since patients lost to follow-up are common in studies. Finally, the reoperation rates of other surgical approaches excluded in our review while recommended by guidelines were also obtained during the literature search. However, as their surgical methods were outdated, less commonly used, or they were associated with a smaller number of studies, we excluded them from our current review.
In future, studies of higher quality and longer follow-up durations should be included. With the development of surgical approaches and techniques, the reoperation rate data should also be updated every few years. Meanwhile, the reoperation rate should be further refined based on its cause, and studies exploring the reason for reoperation are needed. In addition to the reoperation rate, the cost of surgical management across procedures varies, and sometimes there are even huge differences, which also affects what procedures are available for patients to choose from (142, 143). For example, a recent study reported that robotic-assisted simple prostatectomy (RASP) showed comparable efficacy and safety with a shorter hospitalization than laparoscopic simple prostatectomy (LSP) (144). However, considering the cost and unavailability of robot-assisted surgery, LSP is also a better alternative (144). Therefore, studies that evaluate the cost-effectiveness of these surgical approaches are also needed. Overall, these further investigations may lead to a reduction in the reoperation rate or prevent some common reoperation cases, which may give more information for clinical practitioners, better improve patient quality of life, and reduce medical expenses for patients.
Conclusions
Our results summarized the reoperation rates of 10 surgical procedures over follow-up durations of 1, 2, 3, and 5 years. There was a great difference in the reoperation rate among these procedures. The OP, AquaBeam, PKRP, and HoLEP procedures exhibited a lower reoperation rate, whereas the PAE and TUMT procedures exhibited a higher rate. These data could provide reference for urologists and BPH/LUTS patients.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
WH: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Writing – review and editing. TD: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Writing – review and editing. ZN: Software, Writing – review and editing. CH: Validation, Writing – review and editing. CL: Validation, Writing – review and editing. ZX: Data curation, Writing – review and editing. YJ: Data curation, Writing – review and editing. WQ: Funding acquisition, Supervision, Writing – review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by grants from the National Natural Science Foundation of China (No. 81772734).
Acknowledgments
The authors acknowledge all the participants and administrators of this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1287212/full#supplementary-material
References
1. Claus G, Roehrborn DWS. Benign prostatic hyperplasia: etiology, pathophysiology, epidemiology and natural history. TWELFTH ed. Alan W, Partin RRD, Kavoussi LR, Peters CA, editors. Elsevier: Campbell-Walsh-Wein Urology (2021).
2. Lerner LB, McVary KT, Barry MJ, Bixler BR, Dahm P, Das AK, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA GUIDELINE PART II-surgical evaluation and treatment. J Urol (2021) 206(4):818–26. doi: 10.1097/JU.0000000000002184
3. Cornu MG JN, Hashim H, Herrmann TRW, Malde S, Netsch C, Rieken M, et al. EAU guidelines on non-neurogenic male lower urinary tract symptoms (LUTS), incl. Benign prostatic obstruction (BPO). EAU Guidelines (2023).
4. Rassweiler J, Teber D, Kuntz R, Hofmann R. Complications of transurethral resection of the prostate (TURP) - Incidence, management, and prevention. Eur Urol (2006) 50(5):969–79. doi: 10.1016/j.eururo.2005.12.042
5. Madersbacher S, Lackner J, Brossner C, Rohlich M, Stancik I, Willinger M, et al. Reoperation, myocardial infarction and mortality after transurethral and open prostatectomy: A nation-wide, long-term analysis of 23,123 cases. Eur Urol (2005) 47(4):499–504. doi: 10.1016/j.eururo.2004.12.010
6. Eredics K, Wachabauer D, Röthlin F, Madersbacher S, Schauer I. Reoperation rates and mortality after transurethral and open prostatectomy in a long-term nationwide analysis: have we improved over a decade? Urology (2018) 118:152–7. doi: 10.1016/j.urology.2018.04.032
7. Jain A, Nassour AJ, Khannani H, Wines MP, Chalasani V, Katelaris P, et al. Australian surgical revision rate for benign prostatic obstruction. BJU Int (2023) 131 Suppl 4:43–7. doi: 10.1111/bju.16031
8. Franco JV, Jung JH, Imamura M, Borofsky M, Omar MI, Liquitay CME, et al. Minimally invasive treatments for benign prostatic hyperplasia: a Cochrane network meta-analysis. Bju Int (2022) 130(2):142–56. doi: 10.1111/bju.15653
9. Jung JH, McCutcheon KA, Borofsky M, Young S, Golzarian J, Kim MH, et al. Prostatic arterial embolization for the treatment of lower urinary tract symptoms in men with benign prostatic hyperplasia. Cochrane Database Syst Rev (2022) 3). doi: 10.1002/14651858.CD012867.pub2
10. Baboudjian M, Cornu JN, Gondran-Tellier B, Fourmarier M, Robert G, Peyronnet B, et al. Pharmacologic and surgical retreatment after office-based treatments for benign prostatic hyperplasia: A systematic review. Eur Urol Focus (2023). doi: 10.1016/j.euf.2023.03.004
11. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj (2021) 372:n71. doi: 10.1136/bmj.n71
12. Knoll T, Omar MI, Maclennan S, Hernández V, Canfield S, Yuan Y, et al. Key steps in conducting systematic reviews for underpinning clinical practice guidelines: methodology of the european association of urology. Eur Urol (2018) 73(2):290–300. doi: 10.1136/bmj.n71
13. Stephenson WP, Chute CG, Guess HA, Schwartz S, Lieber M. Incidence and outcome of surgery for benign prostatic hyperplasia among residents of rochester, minnesota - 1980-87 - a population-based study. Urology (1991) 38(1):32–42. doi: 10.1136/bmj.n71
14. Sidney S, Quesenberry CP, Sadler MC, Cattolica EV, Lydick EG, Guess HA. Reoperation and mortality after surgical-treatment of benign prostatic hypertrophy in a large prepaid medical-care program. Med Care (1992) 30(2):117–25. doi: 10.1136/bmj.n71
15. Matani Y, Mottrie AM, Stockle M, Voges GE, Fichtner J, Hohenfellner R. Transurethral prostatectomy: A long-term follow-up study of 166 patients over 80 years of age. Eur Urol (1996) 30(4):414–7. doi: 10.1159/000474208
16. Jahnson S, Dalén M, Gustavsson G, Pedersen J. Transurethral incision versus resection of the prostate for small to medium benign prostatic hyperplasia. Br J Urol (1998) 81(2):276–81. doi: 10.1046/j.1464-410x.1998.00535.x
17. Carter A, Sells H, Speakman M, Ewings P, MacDonagh R, O’Boyle P. A prospective randomized controlled trial of hybrid laser treatment or transurethral resection of the prostate, with a 1-year follow-up. BJU Int (1999) 83(3):254–9. doi: 10.1046/j.1464-410x.1999.00936.x
18. Hammadeh MY, Madaan S, Singh M, Philp T. A 3-year follow-up of a prospective randomized trial comparing transurethral electrovaporization of the prostate with standard transurethral prostatectomy. BJU Int (2000) 86(6):648–51. doi: 10.1046/j.1464-410x.2000.00879.x
19. Schatzl G, Madersbacher S, Djavan B, Lang T, Marberger M. Two-year results of transurethral resection of the prostate versus four ‘less invasive’ treatment options. Eur Urol (2000) 37(6):695–700. doi: 10.1159/000020220
20. Keoghane SR, Lawrence KC, Gray AM, Doll HA, Hancock AM, Turner K, et al. A double-blind randomized controlled trial and economic evaluation of transurethral resection vs contact laser vaporization for benign prostatic enlargement: a 3-year follow-up. Bju Int (2000) 85(1):74–8. doi: 10.1046/j.1464-410x.2000.00407.x
21. Floratos DL, Kiemeney LA, Rossi C, Kortmann BB, Debruyne FM, de la Rosette JJ. Long-term followup of randomized transurethral microwave thermotherapy versus transurethral prostatic resection study. J Urol (2001) 165(5):1533–8. doi: 10.1016/S0022-5347(05)66343-4
22. Tuhkanen K, Heino A, Ala-Opas M. Two-year follow-up results of a prospective randomized trial comparing hybrid laser prostatectomy with TURP in the treatment of big benign prostates. Scand J Urol Nephrol (2001) 35(3):200–4. doi: 10.1080/003655901750291962
23. Helke C, Manseck A, Hakenberg OW, Wirth MP. Is transurethral vaporesection of the prostate better than standard transurethral resection? Eur Urol (2001) 39(5):551–7. doi: 10.1159/000052502
24. Hammadeh MY, Madaan S, Hines J, Philp T. 5-year outcome of a prospective randomized trial to compare transurethral electrovaporization of the prostate and standard transurethral resection. Urology (2003) 61(6):1166–71. doi: 10.1016/S0090-4295(03)00109-2
25. van Melick HHE, van Venrooij G, Boon TA. Long-term follow-up after transurethral resection of the prostate, contact laser prostatectomy, and electrovaporization. Urology (2003) 62(6):1029–34. doi: 10.1016/S0090-4295(03)00769-6
26. Tan AHH, Gilling PJ, Kennett KM, Frampton C, Westenberg AM, Fraundorfer MR. A randomized trial comparing holmium laser enucleation of the prostate with transurethral resection of the prostate for the treatment of bladder outlet obstruction secondary to benign prostatic hyperplasia in large glands (40 to 200 grams). J Urol (2003) 170(4):1270–4. doi: 10.1097/01.ju.0000086948.55973.00
27. Hill B, Belville W, Bruskewitz R, Issa M, Perez-Marrero R, Roehrborn C, et al. Transurethral needle ablation versus transurethral resection of the prostate for the treatment of symptomatic benign prostatic hyperplasia: 5-year results of a prospective, randomized, multicenter clinical trial. J Urol (2004) 171(6):2336–40. doi: 10.1097/01.ju.0000127761.87421.a0
28. Liu CK, Lee WK, Ko MC, Chiang HS, Wan KS. Transurethral electrovapor resection versus standard transurethral resection treatment for a large prostate: A 2-year follow-up study conducted in Taiwan. Urol. Internationalis (2006) 76(2):144–9. doi: 10.1159/000090878
29. Wilson LC, Gilling PJ, Williams A, Kennett KM, Frampton CM, Westenberg AM, et al. A randomised trial comparing holmium laser enucleation versus transurethral resection in the treatment of prostates larger than 40 grams: Results at 2 years. Eur Urol (2006) 50(3):569–73. doi: 10.1016/j.eururo.2006.04.002
30. Ahyai SA, Lehrich K, Kuntz RM. Holmium laser enucleation versus transurethral resection of the prostate: 3-year follow-up results of a Randomized clinical trial. Eur Urol (2007) 52(5):1456–64. doi: 10.1016/j.eururo.2007.04.053
31. Tasci AI, Tugcu V, Sahin S, Zorluoglu F. Photoselective vaporization of the prostate versus transurethral resection of the prostate for the large prostate: A prospective nonrandomized bicenter trial with 2-year follow-up. J Endourol (2008) 22(2):347–53. doi: 10.1089/end.2007.0137
32. Zhao ZG, Zeng GH, Zhong W, Mai ZL, Zeng SH, Tao XT. A prospective, randomised trial comparing plasmakinetic enucleation to standard transurethral resection of the prostate for symptomatic benign prostatic hyperplasia: three-year follow-up results. Eur Urol (2010) 58(5):752–8. doi: 10.1016/j.eururo.2010.08.026
33. Ou RB, You M, Tang P, Chen H, Deng XR, Xie KJ. A randomized trial of transvesical prostatectomy versus transurethral resection of the prostate for prostate greater than 80 mL. Urology (2010) 76(4):958–61. doi: 10.1016/j.urology.2010.01.079
34. Muslumanoglu AY, Yuruk E, Binbay M, Akman T. Transurethral resection of prostate with plasmakinetic energy: 100 months results of a prospective randomized trial. Bju Int (2012) 110(4):546–9. doi: 10.1111/j.1464-410X.2011.10770.x
35. Xue B, Zang Y, Zhang Y, Yang D, Gao J, Sun C, et al. GreenLight HPS 120-W laser vaporization versus transurethral resection of the prostate for treatment of benign prostatic hyperplasia: a prospective randomized trial. J Xray Sci Technol (2013) 21(1):125–32. doi: 10.3233/XST-130359
36. Cui D, Sun F, Zhuo J, Sun X, Han B, Zhao F, et al. A randomized trial comparing thulium laser resection to standard transurethral resection of the prostate for symptomatic benign prostatic hyperplasia: four-year follow-up results. World J Urol (2014) 32(3):683–9. doi: 10.1007/s00345-013-1103-6
37. Mamoulakis C, Schulze M, Skolarikos A, Alivizatos G, Scarpa RM, Rassweiler JJ, et al. Midterm results from an international multicentre randomised controlled trial comparing bipolar with monopolar transurethral resection of the prostate. Eur Urol (2013) 63(4):667–76. doi: 10.1016/j.eururo.2012.10.003
38. Stucki P, Marini L, Mattei A, Xafis K, Boldini M, Danuser H. Bipolar versus monopolar transurethral resection of the prostate: A prospective randomized trial focusing on bleeding complications. J Urol (2015) 193(4):1371–5. doi: 10.1016/j.juro.2014.08.137
39. Bachmann A, Tubaro A, Barber N, d’Ancona F, Muir G, Witzsch U, et al. 180-W XPS greenLight laser vaporisation versus transurethral resection of the prostate for the treatment of benign prostatic obstruction: 6-month safety and efficacy results of a European multicentre randomised trial-the GOLIATH study. Eur Urol (2014) 65(5):931–42. doi: 10.1016/j.eururo.2013.10.040
40. Guo S, Müller G, Lehmann K, Talimi S, Bonkat G, Püschel H, et al. The 80-W KTP GreenLight laser vaporization of the prostate versus transurethral resection of the prostate (TURP): adjusted analysis of 5-year results of a prospective non-randomized bi-center study. Lasers Med Sci (2015) 30(3):1147–51. doi: 10.1007/s10103-015-1721-x
41. Thomas JA, Tubaro A, Barber N, d’Ancona F, Muir G, Witzsch U, et al. A multicenter randomized noninferiority trial comparing greenLight-XPS laser vaporization of the prostate and transurethral resection of the prostate for the treatment of benign prostatic obstruction: two-yr outcomes of the GOLIATH study. Eur Urol (2016) 69(1):94–102. doi: 10.1016/j.eururo.2015.07.054
42. Al-Rawashdah SF, Pastore AL, Al Salhi Y, Fuschi A, Petrozza V, Maurizi A, et al. Prospective randomized study comparing monopolar with bipolar transurethral resection of prostate in benign prostatic obstruction: 36-month outcomes. World J Urol (2017) 35(10):1595–601. doi: 10.1007/s00345-017-2023-7
43. Mordasini L, Di Bona C, Klein J, Mattei A, Wirth GJ, Iselin CE. 80-W greenLight laser vaporization versus transurethral resection of the prostate for treatment of benign prostatic obstruction: 5-year outcomes of a single-center prospective randomized trial. Urology (2018) 116:144–9. doi: 10.1016/j.urology.2018.01.037
44. Ray AF, Powell J, Speakman MJ, Longford NT, DasGupta R, Bryant T, et al. Efficacy and safety of prostate artery embolization for benign prostatic hyperplasia: an observational study and propensity-matched comparison with transurethral resection of the prostate (the UK-ROPE study). Bju Int (2018) 122(2):270–82. doi: 10.1111/bju.14249
45. Prudhomme T, Marquette T, Pere M, Patard PM, Michiels C, Sallusto F, et al. Benign prostatic hyperplasia endoscopic surgical procedures in kidney transplant recipients: a comparison between HoLEP, GreenLight photoselective vaporization of the prostate and TURP. J endourology/Endourological Soc (2019) 34(2):184–91. doi: 10.1089/end.2019.0430
46. Sagen E, Nelzén O, Peeker R. Transurethral resection of the prostate: fate of the non-responders. Scand J Urol (2020) 54(5):443–8. doi: 10.1080/21681805.2020.1812712
47. Stoddard MD, Zheng XY, Mao JL, Te A, Sedrakyan A, Chughtai B. Safety and efficacy of outpatient surgical procedures for the treatment of benign prostatic enlargement in New York state and California (2005-2016). J Urol (2021) 205(3):848–54. doi: 10.1097/JU.0000000000001401
48. Abt D, Muellhaupt G, Hechelhammer L, Markart S, Gusewell S, Schmid HP, et al. Prostatic artery embolisation versus transurethral resection of the prostate for benign prostatic hyperplasia: 2-yr outcomes of a randomised, open-label, single-centre trial. Eur Urol (2021) 80(1):34–42. doi: 10.1016/j.eururo.2021.02.008
49. Ofoha CG, Raphael JE, Dakum NK, Shu’aibu SI, Akhaine J, Yaki IM. Surgical management of benign prostate hyperplasia in Nigeria: open prostatectomy versus transurethral resection of the prostate. Pan. Afr Med J (2021) 39:165. doi: 10.11604/pamj.2021.39.165.24767
50. Gilling PJ, Barber N, Bidair M, Anderson P, Sutton M, Aho T, et al. Five-year outcomes for Aquablation therapy compared to TURP: results from a double-blind, randomized trial in men with LUTS due to BPH. Can J Urol (2022) 29(1):10960–8.
51. Loloi J, Wang S, Labagnara K, Plummer M, Douglass L, Watts K, et al. Predictors of reoperation after transurethral resection of the prostate in a diverse, urban academic centre. J Clin Urol (2022). doi: 10.1177/20514158221132102
52. Yang BB, Shen BX, Liu WZ, Cheng Y, Shao YP, Qian JH. Medium-term clinical efficacy and complications of plasmakinetic enucleation of the prostate versus transurethral resection of the prostate for benign prostatic hyperplasia. Urology (2022) 164:204–10. doi: 10.1016/j.urology.2022.01.013
53. Yang CY, Chen GM, Wu YX, Zhang WJ, Wang J, Chen PP, et al. Clinical efficacy and complications of transurethral resection of the prostate versus plasmakinetic enucleation of the prostate. Eur J Med Res (2023) 28(1):83. doi: 10.1186/s40001-023-00989-9
54. Raizenne BL, Zheng X, Oumedjbeur K, Mao J, Zorn KC, Elterman D, et al. Prostatic artery embolization compared to transurethral resection of the prostate and prostatic urethral lift: a real-world population-based study. World J Urol (2023) 41(1):179–88. doi: 10.1007/s00345-022-04218-6
55. Hu YY, Dong XC, Wang GC, Huang JH, Liu M, Peng B. Five-year follow-up study of transurethral plasmakinetic resection of the prostate for benign prostatic hyperplasia. J Endourol (2016) 30(1):97–101. doi: 10.1089/end.2015.0506
56. Cheng X, Qin CY, Xu P, Li YJ, Peng M, Wu SQ, et al. Comparison of bipolar plasmakinetic resection of prostate versus photoselective vaporization of prostate by a three year retrospective observational study. Sci Rep (2021) 11(1):10142. doi: 10.1038/s41598-021-89623-4
57. Zhu GB, Xie CY, Wang XH, Tang XQ. Bipolar plasmakinetic transurethral resection of prostate in 132 consecutive patients with large gland: three-year follow-up results. Urology (2012) 79(2):397–402. doi: 10.1016/j.urology.2011.08.052
58. Li K, Wang DJ, Hu C, Mao YH, Li MY, Jie ST, et al. A Novel Modification of Transurethral Enucleation and Resection of the Prostate in Patients With Prostate Glands Larger than 80 mL: Surgical Procedures and Clinical Outcomes. Urology (2018) 113:153–9. doi: 10.1016/j.urology.2017.11.036
59. Elshal AM, Soltan M, El-Tabey NA, Laymon M, Nabeeh A. Randomised trial of bipolar resection vs holmium laser enucleation vs Greenlight laser vapo-enucleation of the prostate for treatment of large benign prostate obstruction: 3-years outcomes. Bju Int (2020) 126(6):731–8. doi: 10.1111/bju.15161
60. Wei Y, Xu N, Chen SH, Li XD, Zheng QS, Lin YZ, et al. Bipolar transurethral enucleation and resection of the prostate versus bipolar resection of the prostate for prostates larger than 60gr: A retrospective study at a single academic tertiary care center. Int Braz J Urol (2016) 42(4):747–56. doi: 10.1590/S1677-5538.IBJU.2015.0225
61. Peng M, Yi L, Wang YH. Photoselective vaporization of the prostate vs plasmakinetic resection of the prostate: A randomized prospective trial with 12-month follow-up in Mainland China. Urology (2016) 87:161–5. doi: 10.1016/j.urology.2014.08.038
62. Yip SK, Chan NH, Chiu P, Lee KW, Ng CF. A randomized controlled trial comparing the efficacy of hybrid bipolar transurethral vaporization and resection of the prostate with bipolar transurethral resection of the prostate. J Endourol (2011) 25(12):1889–94. doi: 10.1089/end.2011.0269
63. Elshal AM, Elkoushy MA, Elmansy HM, Sampalis J, Elhilali MM. Holmium : YAG transurethral incision versus laser photoselective vaporization for benign prostatic hyperplasia in a small prostate. J Urol (2014) 191(1):148–54. doi: 10.1016/j.juro.2013.06.113
64. Kuntz RM, Lehrich K, Ahyai SA. Holmium laser enucleation of the prostate versus open prostatectomy for prostates greater than 100 grams: 5-year follow-up results of a randomised clinical trial. Eur Urol (2008) 53(1):160–8. doi: 10.1016/j.eururo.2007.08.036
65. Sofimajidpour H, Khoshyar A, Zareie B, Sofimajidpour H, Rasouli MA. Comparison of the effectiveness and safety of transvesical open prostatectomy versus transurethral resection of the prostate in patients with benign prostatic hyperplasia with a prostate weight of 65-40 gram. Urol J (2020) 18(3):289–94. doi: 10.22037/uj.v16i7.6342
66. Varkarakis I, Kyriakakis Z, Delis A, Protogerou V, Deliveliotis C. Long-term results of open transvesical prostatectomy from a contemporary series of patients. Urology (2004) 64(2):306–10. doi: 10.1016/j.urology.2004.03.033
67. Shah HN, Etafy MH, Katz JE, Garcia Lopez EA, Shah RH. A randomized controlled trial comparing high and medium power settings for holmium laser enucleation of prostate. World J Urol (2021) 39(8):3005–11. doi: 10.1007/s00345-020-03535-y
68. Gilling PJ, Aho TF, Frampton CM, King CJ, Fraundorfer MR. Holmium laser enucleation of the prostate: Results at 6 years. Eur Urol (2008) 53(4):744–9. doi: 10.1016/j.eururo.2007.04.052
69. Whiting D, Penev B, Guest K, Cynk M. Holmium laser enucleation of the prostate: A single-centre case series of 1000 patients. J Clin Urol (2022) 15(5):370–5. doi: 10.1177/20514158211033741
70. Elshal AM, Elmansy HM, Elhilali MM. Feasibility of holmium laser enucleation of the prostate (HoLEP) for recurrent/residual benign prostatic hyperplasia (BPH). Bju Int (2012) 110(11C):E845–E50. doi: 10.1111/j.1464-410X.2012.11290.x
71. Droghetti M, Porreca A, Bianchi L, Piazza P, Giampaoli M, Casablanca C, et al. Long-term outcomes of Holmium laser enucleation of prostate and predictive model for symptom recurrence. Prostate (2022) 82(2):203–9. doi: 10.1002/pros.24259
72. Enikeev D, Taratkin M, Morozov A, Singla N, Gabdulina S, Tarasov A, et al. Long-term outcomes of holmium laser enucleation of the prostate: A 5-year single-center experience. J Endourol (2020) 34(10):1055–63. doi: 10.1089/end.2020.0347
73. Bhandarkar A, Patel D. Comparison of holmium laser enucleation of the prostate with bipolar plasmakinetic enucleation of the prostate: A randomized, prospective controlled trial at midterm follow-up. J Endourol (2022) 36(12):1567–74. doi: 10.1089/end.2022.0449
74. Vavassori I, Valenti S, Naspro R, Vismara A, Dell’Acqua V, Manzetti A, et al. Three-year outcome following holmium laser enucleation of the prostate combined with mechanical morcellation in 330 consecutive patients. Eur Urol (2008) 53(3):599–606. doi: 10.1016/j.eururo.2007.10.059
75. Tan AHH, Gilling PJ, Kennett KM, Fletcher H, Fraundorfer MR. Long-term results of high-power holmium laser vaporization (ablation) of the prostate. Bju Int (2003) 92(7):707–9. doi: 10.1046/j.1464-410x.2003.04474.x
76. Bae J, Choo M, Park JH, Oh JK, Paick JS, Oh SJ. Holmium laser enucleation of prostate for benign prostatic hyperplasia: seoul national university hospital experience. Int Neurourol J (2011) 15(1):29–34. doi: 10.5213/inj.2011.15.1.29
77. Aho TF, Gilling PJ, Kennett KM, Westenberg AM, Fraundorfer MR, Frampton CM. Holmium laser bladder neck incision versus holmium enucleation of the prostate as outpatient procedures for prostates less than 40 grams: A randomized trial. J Urol (2005) 174(1):210–4. doi: 10.1097/01.ju.0000161610.68204.ee
78. Neill MG, Gilling PJ, Kennett KM, Frampton CM, Westenberg AM, Fraundorfer MR, et al. Randomized trial comparing holmium laser enucleation of prostate with plasmakinetic enucleation of prostate for treatment of benign prostatic hyperplasia. Urology (2006) 68(5):1020–4. doi: 10.1016/j.urology.2006.06.021
79. Castellani D, Di Rosa M, Gasparri L, Pucci M, Dellabella M. Thulium laser vapoenucleation of the prostate (ThuVEP) in men at high cardiovascular risk and on antithrombotic therapy: A single-center experience. J Clin Med (2020) 9(4):917. doi: 10.3390/jcm9040917
80. Gross AJ, Orywal AK, Becker B, Netsch C. Five-year outcomes of thulium vapoenucleation of the prostate for symptomatic benign prostatic obstruction. World J Urol (2017) 35(10):1585–93. doi: 10.1007/s00345-017-2034-4
81. Tao W, Xue B, Sun C, Yang D, Zhang Y, Shan Y. Comparison of vaporization using 120-W GreenLight laser versus 2-micrometer continuous laser for treating benign prostatic hyperplasia: A 24-month follow-up study of a single center. J Xray Sci Technol (2019) 27(4):755–64. doi: 10.3233/XST-190507
82. Tao W, Sun CY, Xue BX, Yang DR, Wang MC, Cai CJ, et al. The efficacy and safety of 2-mu m continuous laser in the treatment of high-risk patients with benign prostatic hyperplasia. Lasers Med Sci (2017) 32(2):351–6. doi: 10.1007/s10103-016-2122-5
83. Becker B, Buttice S, Magno C, Gross AJ, Netsch C. Thulium vaporesection of the prostate and thulium vapoenucleation of the prostate: A retrospective bicentric matched-paired comparison with 24-month follow-up. Urol Int (2018) 100(1):105–11. doi: 10.1159/000484444
84. Bach T, Netsch C, Pohlmann L, Herrmann TRW, Gross AJ. Thulium : YAG vapoenucleation in large volume prostates. J Urol (2011) 186(6):2323–7. doi: 10.1016/j.juro.2011.07.073
85. Netsch C, Bach T, Pohlmann L, Herrmann T, Gross AJ. Comparison of 120-200 W 2 mu m Thulium: Yttrium-Aluminum-Garnet Vapoenucleation of the Prostate. J Endourol (2012) 26(3):224–9. doi: 10.1089/end.2011.0173
86. Park J, Cho SY, Cho MC, Jeong H, Son H. 5-year long-term efficacy of 120-W GreenLight photoselective vaporization of the prostate for benign prostate hyperplasia. PloS One (2017) 12(9):e0184442. doi: 10.1371/journal.pone.0184442
87. Law KW, Tholomier C, Nguyen DD, Sadri I, Couture F, Zakaria AS, et al. Global Greenlight Group: largest international Greenlight experience for benign prostatic hyperplasia to assess efficacy and safety. World J Urol (2021) 39(12):4389–95. doi: 10.1007/s00345-021-03688-4
88. Yamada Y, Furusawa J, Sugimura Y, Kuromatsu I. Photoselective vaporization of the prostate: long-term outcomes and safety during 10 years of follow-up. J Endourol (2016) 30(12):1306–11. doi: 10.1089/end.2016.0522
89. Hai MA. Photoselective vaporization of prostate: five-year outcomes of entire clinic patient population. Urology (2009) 73(4):807–10. doi: 10.1016/j.urology.2008.08.502
90. Malde S, Rajagopalan A, Patel N, Simoes A, Choi W, Shrotri N. Potassium-titanyl-phosphate laser photoselective vaporization for benign prostatic hyperplasia: 5-year follow-up from a district general hospital. J Endourol (2012) 26(7):878–83. doi: 10.1089/end.2011.0370
91. Ajib K, Mansour M, Zanaty M, Alnazari M, Hueber PA, Meskawi M, et al. Photoselective vaporization of the prostate with the 180-W XPS-Greenlight laser: Five-year experience of safety, efficiency, and functional outcomes. Cuaj-Canadian. Urol Assoc J (2018) 12(7):E318–E24. doi: 10.1016/j.juro.2018.02.2019
92. Kim KS, Choi JB, Bae WJ, Kim SJ, Cho HJ, Hong SH, et al. Risk factors for reoperation after photoselective vaporization of the prostate using a 120 W greenLight high performance system laser for the treatment of benign prostatic hyperplasia. Photomed Laser Surgery (2016) 34(3):102–7. doi: 10.1089/pho.2015.4050
93. Te AE, Malloy TR, Stein BS, Ulchaker JC, Nseyo UO, Hais MA. Impact of prostate-specific antigen level and prostate volume as predictors of efficacy in photoselective vaporization prostatectomy: analysis and results of an ongoing prospective multicentre study at 3 years. Bju Int (2006) 97(6):1229–33. doi: 10.1111/j.1464-410X.2006.06197.x
94. Tasci AI, Ilbey YO, Luleci H, Cicekler O, Sahin S, Cevik C, et al. 120-W greenLight laser photoselective vaporization of prostate for benign prostatic hyperplasia: midterm outcomes. Urology (2011) 78(1):134–40. doi: 10.1016/j.urology.2010.12.085
95. Meskawi M, Hueber PA, Valdivieso R, Bruyere F, Misrai V, Fournier G, et al. Multicenter international experience of 532 nm-laser photo-vaporization with Greenlight XPS in men with large prostates (prostate volume > 100 cc). World J Urol (2017) 35(10):1603–9. doi: 10.1007/s00345-017-2007-7
96. Malek RS, Kuntzman RS, Barrett DM. High power potassium-titanyl-phosphate laser vaporization prostatectomy. J Urol (2000) 163(6):1730–3. doi: 10.1016/S0022-5347(05)67530-1
97. Hueber PA, Bienz MN, Valdivieso R, Lavigueur-Blouin H, Misrai V, Rutman M, et al. Photoselective vaporization of the prostate for benign prostatic hyperplasia using the 180 watt system: multicenter study of the impact of prostate size on safety and outcomes. J Urol (2015) 194(2):462–9. doi: 10.1016/j.juro.2015.03.113
98. Tao W, Xue BX, Zang YC, Sun CY, Yang DR, Zhang YY, et al. The application of 120-W high-performance system GreenLight laser vaporization of the prostate in high-risk patients. Lasers Med Sci (2013) 28(4):1151–7. doi: 10.1007/s10103-012-1212-2
99. Chung DE, Wysock JS, Lee RK, Melamed SR, Kaplan SA, Te AE. Outcomes and complications after 532 nm laser prostatectomy in anticoagulated patients with benign prostatic hyperplasia. J Urol (2011) 186(3):977–81. doi: 10.1016/j.juro.2011.04.068
100. Stone BV, Chughtai B, Forde JC, Tam AW, Lewicki P, Te AE. Safety and efficacy of greenLight XPS laser vapoenucleation in prostates measuring over 150mL. J Endourol (2016) 30(8):906–12. doi: 10.1089/end.2016.0288
101. Liu XL, Yuan F, Xue BX. GreenLight XPS 180-W laser vaporization of prostate in high-risk elderly patients: A single-center experience. Photobiomodulation Photomed Laser Surgery (2020) 38(6):380–4. doi: 10.1089/photob.2019.4735
102. Campobasso C, Marchioni M, Greco F, De Nunzio C, Destefanis P, Ricciardulli S, et al. No matter for prostate sizes: Multicentric Italian Green Light photoselective vaporization study. Eur Urol. Supplements (2019) 18(9):e3168. doi: 10.1016/S1569-9056(19)33500-6
103. Chen CH, Lin SE, Chiang PH. Outcome of GreenLight HPS laser therapy in surgically high-risk patients. Lasers Med Sci (2013) 28(5):1297–303. doi: 10.1007/s10103-012-1234-9
104. Valdivieso R, Meyer CP, Hueber PA, Meskawi M, Alenizi AM, Azizi M, et al. Assessment of energy density usage during 180W lithium triborate laser photoselective vaporization of the prostate for benign prostatic hyperplasia. Is there an optimum amount of kilo-Joules per gram of prostate? Bju Int (2016) 118(4):633–40. doi: 10.1111/bju.13479
105. Kim HS, Cho MC, Ku JH, Kim SW, Paick JS. The efficacy and safety of photoselective vaporization of the prostate with a potassium-titanyl-phosphate laser for symptomatic benign prostatic hyperplasia according to prostate size: 2-year surgical outcomes. Korean J Urol (2010) 51(5):330–6. doi: 10.4111/kju.2010.51.5.330
106. Ruszat R, Wyler S, Seifert HH, Reich O, Forster T, Sulser T, et al. Photoselective vaporization of the prostate: Subgroup analysis of men with refractory urinary retention. Eur Urol (2006) 50(5):1040–9. doi: 10.1016/j.eururo.2006.01.019
107. Ghobrial FK, Shoma A, Elshal AM, Laymon M, El-Tabey N, Nabeeh A, et al. A randomized trial comparing bipolar transurethral vaporization of the prostate with GreenLight laser (xps-180watt) photoselective vaporization of the prostate for treatment of small to moderate benign prostatic obstruction: outcomes after 2 years. Bju Int (2020) 125(1):144–52. doi: 10.1111/bju.14926
108. Huet R, Peyronnet B, Khene ZE, Freton L, Verhoest G, Manunta A, et al. Prospective assessment of the sexual function after greenlight endoscopic enucleation and greenlight 180W XPS photoselective vaporization of the prostate. Urology (2019) 131:184–9. doi: 10.1016/j.urology.2019.06.020
109. Liu ZC, Chen ZP, Yan DS, Jiang T, Fu J, Zheng J, et al. Photoselective sharp enucleation of the prostate with a front-firing 532-nm laser versus photoselective vaporization of the prostate in the treatment of benign prostatic hyperplasia: a randomised controlled trial with 1-year followup results. BMC Urol (2022) 22(1):173. doi: 10.1186/s12894-022-01129-x
110. Mosli HA, Abdel-Meguid TA, Abdulwahhab MH, Al-Sayyad A, Farsi HM, Tayib A. Photoselective vaporization of the prostate using GreenLight 120-W lithium triborate laser to treat symptomatic benign prostatic hyperplasia: A single-centre prospective study. Cuaj-Canadian. Urol Assoc J (2013) 7(3-4):E193–E6. doi: 10.1186/s12894-022-01129-x
111. Seki N, Nomura H, Yamaguchi A, Naito S. Effects of photoselective vaporization of the prostate on urodynamics in patients with benign prostatic hyperplasia. J Urol (2008) 180(3):1024–8. doi: 10.1186/s12894-022-01129-x
112. Hueber PA, Ben-Zvi T, Liberman D, Bhojani N, Gautam G, Deklaj T, et al. Mid term outcomes of initial 250 case experience with GreenLight 120W-HPS photoselective vaporization prostatectomy for benign prostatic hyperplasia: comparison of prostate volumes < 60 cc, 60 cc-100 cc and > 100 cc. Can J Urol (2012) 19(5):6450–8.
113. Tao W, Sun CY, Yang DR, Zang YC, Zhu J, Zhang YY, et al. Application of 180W XPS GreenLight laser vaporization of the prostate for treatment of benign prostatic hyperplasia. J X-Ray Sci Technol (2019) 27(6):1121–9. doi: 10.1186/s12894-022-01129-x
114. Tugcu V, Tasci AI, Sahin S, Ordekci Y, Karakas OF, Zorluoglu F. Outcomes of 80 WKTP laser vaporization of the large prostate. Urol Internationalis (2007) 79(4):316–20. doi: 10.1159/000109716
115. Pfitzenmaier J, Gilfrich C, Pritsch M, Herrmann D, Buse S, Haferkamp A, et al. Vaporization of prostates of > or =80 mL using a potassium-titanyl-phosphate laser: midterm-results and comparison with prostates of <80 mL. BJU Int (2008) 102(3):322–7. doi: 10.1111/j.1464-410X.2008.07563.x
116. Abolazm AE, El-Hefnawy AS, Laymon M, Shehab-El-Din AB, Elshal AM. Ejaculatory Hood Sparing versus Standard Laser Photoselective Vaporization of the Prostate: Sexual and Urodynamic Assessment through a Double Blinded, Randomized Trial. J Urol (2020) 203(4):792–801. doi: 10.1097/JU.0000000000000685
117. Bhojani N, Bidair M, Kramolowsky E, Desai M, Doumanian L, Zorn KC, et al. Aquablation therapy in large prostates (80-150 mL) for lower urinary tract symptoms due to benign prostatic hyperplasia: final WATER II 5-year clinical trial results. J Urol (2023) 210(1):143–53. doi: 10.1186/s12894-022-01129-x
118. Zorn KC, Bidair M, Trainer A, Arther A, Kramolowsky E, Desai M, et al. Aquablation therapy in large prostates (80-150 cc) for lower urinary tract symptoms due to benign prostatic hyperplasia: WATER II 3-year trial results. BJUI Compass (2022) 3(2):130–8. doi: 10.1186/s12894-022-01129-x
119. Bilhim T, Costa NV, Torres D, Pinheiro LC, Spaepen E. Long-term outcome of prostatic artery embolization for patients with benign prostatic hyperplasia: single-centre retrospective study in 1072 patients over a 10-year period. Cardiovasc Intervent Radiol (2022) 45(9):1324–36. doi: 10.1186/s12894-022-01129-x
120. Xu ZW, Zhou CG, Tian W, Shi HB, Liu S. Long-term efficacy and recurrence prediction of prostatic artery embolization for lower urinary tract symptoms secondary to benign prostatic hyperplasia. Cardiovasc Interventional Radiol (2022) 45(12):1801–9. doi: 10.1186/s12894-022-01129-x
121. Gravas S, Laguna P, Kiemeney L, de la Rosette J. Durability of 30-minute high-energy transurethral microwave therapy for treatment of benign prostatic hyperplasia: A study of 213 patients with and without urinary retention. Urology (2007) 69(5):854–8. doi: 10.1016/j.urology.2007.01.070
122. Francisca EA, Keijzers GB, d’Ancona FC, Debruyne FM, de la Rosette JJ. Lower-energy thermotherapy in the treatment of benign prostatic hyperplasia: long-term follow-up results of a multicenter international study. World J Urol (1999) 17(5):279–84. doi: 10.1007/s003450050146
123. Raizenne BL, Zheng X, Mao J, Zorn KC, Cho A, Elterman D, et al. Real-world data comparing minimally invasive surgeries for benign prostatic hyperplasia. World J Urol (2022) 40(5):1185–93. doi: 10.1007/s00345-021-03926-9
124. Lau KO, Li MK, Foo KT. Long-term follow-up of transurethral microwave thermotherapy. Urology (1998) 52(5):829–33. doi: 10.1016/S0090-4295(98)00285-4
125. Ohigashi T, Nakamura K, Nakashima J, Baba S, Murai M. Long-term results of three different minimally invasive therapies for lower urinary tract symptoms due to benign prostatic hyperplasia: Comparison at a single institute. Int J Urol (2007) 14(4):326–30. doi: 10.1111/j.1442-2042.2007.01692.x
126. Keijzers GB, Francisca EA, D’Ancona FC, Kiemeney LA, Debruyne FM, de la Rosette JJ. Long-term results of lower energy transurethral microwave thermotherapy. J Urol (1998) 159(6):1966–72; discussion 72-3. doi: 10.1016/S0022-5347(01)63211-7
127. Tsai YS, Lin JS, Tong YC, Tzai TS, Yang WH, Chang CC, et al. Transurethral microwave thermotherapy for symptomatic benign prostatic hyperplasia: long-term durability with Prostcare. Eur Urol (2001) 39(6):688–92; discussion 93-4. doi: 10.1159/000052528
128. Lourenco T, Shaw M, Fraser C, MacLennan G, N’Dow J, Pickard R. The clinical effectiveness of transurethral incision of the prostate: a systematic review of randomised controlled trials. World J Urol (2010) 28(1):23–32. doi: 10.1007/s00345-009-0496-8
129. Hueber PA, Zorn KC. Let’s not forget about TUIP: A highly underutilized, minimally-invasive and durable technique for men with <30 g prostates. Can Urol Assoc J (2015) 9(7-8):255–6. doi: 10.5489/cuaj.3239
130. Agarwal A, Eryuzlu LN, Cartwright R, Thorlund K, Tammela TL, Guyatt GH, et al. What is the most bothersome lower urinary tract symptom? Individual- and population-level perspectives for both men and women. Eur Urol (2014) 65(6):1211–7. doi: 10.1016/j.eururo.2014.01.019
131. Li M, Qiu J, Hou Q, Wang D, Huang W, Hu C, et al. Endoscopic enucleation versus open prostatectomy for treating large benign prostatic hyperplasia: a meta-analysis of randomized controlled trials. PloS One (2015) 10(3):e0121265. doi: 10.1371/journal.pone.0121265
132. Lin YC, Wu X, Xu AB, Ren R, Zhou XQ, Wen Y, et al. Transurethral enucleation of the prostate versus transvesical open prostatectomy for large benign prostatic hyperplasia: a systematic review and meta-analysis of randomized controlled trials. World J Urol (2016) 34(9):1207–19. doi: 10.1007/s00345-015-1735-9
133. Zhang Y, Yuan P, Ma D, Gao X, Wei C, Liu Z, et al. Efficacy and safety of enucleation vs. resection of prostate for treatment of benign prostatic hyperplasia: a meta-analysis of randomized controlled trials. Prostate. Cancer Prostatic Dis (2019) 22(4):493–508. doi: 10.1016/S0022-5347(01)63211-7
134. Tan A, Liao C, Mo Z, Cao Y. Meta-analysis of holmium laser enucleation versus transurethral resection of the prostate for symptomatic prostatic obstruction. Br J Surgery (2007) 94(10):1201–8. doi: 10.1002/bjs.5916
135. Qian XQ, Liu HL, Xu D, Xu L, Huang F, He W, et al. Functional outcomes and complications following B-TURP versus HoLEP for the treatment of benign prostatic hyperplasia: a review of the literature and Meta-analysis. Aging Male (2017) 20(3):184–91. doi: 10.1080/13685538.2017.1295436
136. Huang KC, Chow YC, Chen M, Chiu AW. Combination of thulium laser incision and bipolar resection offers higher resection velocity than bipolar resection alone in large prostates. Urol J (2019) 16(4):397–402. doi: 10.22037/uj.v0i0.4363
137. Trama F, Lauro GD, Illiano E, Iacono F, Romis L, Mordente S, et al. Ejaculation sparing thulium laser enucleation of the prostate: an observational prospective study. J Clin Med (2022) 11(21):6365. doi: 10.3390/jcm11216365
138. Zhou Y, Xue B, Mohammad NA, Chen D, Sun X, Yang J, et al. Greenlight high-performance system (HPS) 120-W laser vaporization versus transurethral resection of the prostate for the treatment of benign prostatic hyperplasia: a meta-analysis of the published results of randomized controlled trials. Lasers Med Sci (2016) 31(3):485–95. doi: 10.1007/s10103-016-1895-x
139. Moreira AM, de Assis AM, Carnevale FC, Antunes AA, Srougi M, Cerri GG. A review of adverse events related to prostatic artery embolization for treatment of bladder outlet obstruction due to BPH. Cardiovasc Intervent Radiol (2017) 40(10):1490–500. doi: 10.1007/s00270-017-1765-3
140. Pisco J, Campos Pinheiro L, Bilhim T, Duarte M, Rio Tinto H, Fernandes L, et al. Prostatic arterial embolization for benign prostatic hyperplasia: short- and intermediate-term results. Radiology (2013) 266(2):668–77. doi: 10.1148/radiol.12111601
141. Nishiya M, Miller GJ, Lookner DH, Crawford ED. Prostate-specific antigen density in patients with histologically proven prostate carcinoma. Cancer (1994) 74(11):3002–9. doi: 10.1002/1097-0142(19941201)74:11<3002::AID-CNCR2820741118>3.0.CO;2-G
142. Chughtai B, Rojanasarot S, Neeser K, Gultyaev D, Fu S, Bhattacharyya SK, et al. A comprehensive analysis of clinical, quality of life, and cost-effectiveness outcomes of key treatment options for benign prostatic hyperplasia. PloS One (2022) 17(4):e0266824. doi: 10.1371/journal.pone.0266824
143. DeWitt-Foy ME, Gill BC, Ulchaker JC. Cost comparison of benign prostatic hyperplasia treatment options. Curr Urol Rep (2019) 20(8):45. doi: 10.1007/s11934-019-0907-3
Keywords: benign prostate hyperplasia, lower urinary tract symptoms, surgery, retreatment, reoperation
Citation: He W, Ding T, Niu Z, Hao C, Li C, Xu Z, Jing Y and Qin W (2023) Reoperation after surgical treatment for benign prostatic hyperplasia: a systematic review. Front. Endocrinol. 14:1287212. doi: 10.3389/fendo.2023.1287212
Received: 01 September 2023; Accepted: 03 October 2023;
Published: 09 November 2023.
Edited by:
Kenju Shimomura, Fukushima Medical University, JapanReviewed by:
Jens Djurhuus, Aarhus University, DenmarkBiagio Barone, Azienda Ospedaliera di Caserta, Italy
Copyright © 2023 He, Ding, Niu, Hao, Li, Xu, Jing and Qin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weijun Qin, cWlud2pAZm1tdS5lZHUuY24=
†These authors have contributed equally to this work