 Chen-Yu Han†
Chen-Yu Han† Wei-Wei Xu
Wei-Wei Xu Min Zhang
Min Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Endocrinol., 06 December 2023
Sec. Clinical Diabetes
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1267503
This article is part of the Research TopicThe Underlying Mechanisms and Novel Approaches for Diabetes and its Related ComplicationsView all 36 articles
Objective: This prospective study aimed to evaluate the effect of beinaglutide combined with metformin versus aspart 30 with metformin on metabolic profiles and antidrug antibodies (ADAs) in patients with type 2 diabetes (T2D).
Methods: A total of 134 eligible participants were randomly assigned to the test group and the control group. Patients in the test group were treated with beinaglutide and metformin, whereas patients in the control group were randomly treated with aspart 30 and metformin, with a follow-up period of 6 months. The metabolic profiles and ADAs over 6 months were evaluated.
Results: After 6 months, 101 (75.37%) patients completed the study. Compared with the control group, the beinaglutide group had significant reductions in 2-h postprandial blood glucose (2hBG) and low blood glucose index (LBGI). Glycated hemoglobin (HbA1c) decreased in both groups relative to baseline. In the test group, one had treatment-emergent beinaglutide ADAs. Significant reductions in triglycerides (TG), non-fasting TG, weight, waist circumference (WC), and body mass index (BMI) were observed. The values of insulin sensitivity index (HOMA-IR) were decreased to a statistically higher degree with beinaglutide treatment.
Conclusion: Beinaglutide reduces metabolic dysfunction, LBGI, and weight in patients of T2D with a low risk of ADAs. Beinaglutide may offer the potential for a disease-modifying intervention in cardiovascular disease (CVD).
Clinical trial registration: www.chictr.org.cn, identifier ChiCTR2200061003.
Type 2 diabetes (T2D) epidemic is a major health concern, and obesity is contributing to the increase in T2D prevalence (1). T2D is currently considered a systemic disease in which there is dysfunction in multiple organs and tissues (2). Disturbed glucose levels due to obesity-related insulin resistance or release of inflammatory factors cause endothelial and smooth muscle cell dysfunction (3). Thus, microvascular and macrovascular complications are common complications of T2D and the latter remains the most common cause of death (4). People with diabetes have a 1.6 to 2.6 times increased risk of cardiovascular disease (CVD) compared with non-diabetics (5). Obesity and dyslipidemia are important contributors to the increased risk of CVD. Recently, triglyceride (TG) levels have become a predictor and therapeutic target for reducing CVD (6). In clinical practice, serum TG values are usually measured after an 8–12-h fast to avoid the effects of diet. However, most people are not fasting except for a few hours in the early morning. Therefore, fasting serum TG levels may not reflect average daily serum TG levels, which may have a greater impact on atherosclerosis (7). Therefore, the non-fasting period reflects the true atherosclerotic load better than the fasting period (8).
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are a new emerging drug class in treatment of T2D that act on several targets including the pancreatic β-cell, liver, kidney, brain, and CV system (9). In general, GLP-1 RAs reduce body weight, lower blood pressure, and positively affect the lipid profile (10). Other pleiotropic effects could involve protection against CVD since GLP-1 receptors have been found in the heart and endothelium (11). Different homologies to human GLP-1 (7–36) among GLP-1 RAs may result in various actions, efficacy, and tolerability of these medications in the administration (12). Beinaglutide is one of the GLP-1 RAs that have 100% homology to human GLP-1 approved in China for the treatment of patients with T2D (13). Previous studies have shown that patients with T2D who were treated with beinaglutide for 3 months have a mean reduction in body weight of 10.05 kg and improved glycemic control (14). Currently, there is still limited evidence for the incidence of antidrug antibodies (ADAs) and the effect on non-fasting TG levels of beinaglutide. The aim of this study was to evaluate the effect of beinaglutide combined with metformin versus aspart 30 with metformin on metabolic profiles including glucose and lipid profile and ADAs of beinaglutide in patients with T2D.
A prospective randomized controlled study was conducted from 14/02/2020 to 26/08.2022 in Qingpu Hospital Affiliated to Fudan University. Ethical approval was obtained by the Ethical Committee of Qingpu Hospital Affiliated to Fudan University (ID number: IEC-C-007-A08-V.03), and all participants provided a written informed consent. The study was also registered on www.chictr.org.cn (ID number ChiCTR2200061003).
Sample size was determined based on glycated hemoglobin (HbA1c), a key variable from previous studies (15). Considering a = 0.05 and statistical efficacy 1 − b = 0.8, the sample size was calculated as 47 cases in each group. Of 490 prescreened T2D patients, 449 met the eligibility criteria. Taking into account the 30% dropout rate, a total of 134 participants (67 per group) were included in the study. All participants diagnosed with T2D according to World Health Organization (WHO) 1999 criteria (16) underwent monotherapy with metformin but with poor metabolic control (7%≤ HbA1c ≤10%). Inclusion criteria included the following: subjects willing and able to comply with the requirements of the trial program and agree to sign the informed consent form; subjects aged 18–65 on the date of signing the informed consent form (including the threshold); at least 8 weeks of stable treatment with metformin alone (daily dose ≥1,000 mg) prior to screening; body mass index (BMI) of 22.0–40.0 kg/m2 (both extremes) at screening and change in body weight (difference between maximum and minimum body weight in 3 months) of not more than 5 kg in the 3 months prior to screening. The following were the exclusion criteria: treated with GLP-1RAs previously; acute complications of diabetes such as diabetic ketoacidosis (DKA) or hyperosmotic hyperglycemia syndrome (HHS) that occurred in the past 6 months; glucocorticoid treatment (oral or intravenous) that lasted for more than 7 days within 6 months; have a history of idiopathic pancreatitis, chronic pancreatitis, or gastrointestinal diseases; moderate to severe renal insufficiency or end-stage renal disease; there were significant cardiovascular and cerebrovascular events within 3 months; pregnant and lactating women.
Participants who met the inclusion criteria were randomly divided into two groups at a 1:1 ratio. Patients in the test group (n = 67) were randomly treated with beinaglutide and metformin, whereas patients in the control group (n = 67) were randomly treated with aspart 30 and metformin, with a follow-up period of 6 months. The recommended dosage of beinaglutide is 0.1mg three times daily (tid) by subcutaneous injection in the upper arm, thigh, or abdomen. The dosage may be increased to 0.2 mg tid if the glycemic response is inadequate (17). The dosage of aspart 30 is determined by the endocrinologist according to the patient’s blood glucose (BG).
The primary objective of this study was to demonstrate the superiority of beinaglutide versus aspart 30 in reducing blood glucose and the low blood glucose index (LBGI) levels after 6 months. At the same time, the incidence of ADAs was used to assess the safety of beinaglutide. The secondary efficacy endpoints were lipid profile, especially non-fasting TG levels. Other endpoints were weight, waist circumference (WC), BMI, subcutaneous fat, and insulin sensitivity index (HOMA-IR).
All participants were required to undergo anthropometric and laboratory examinations at baseline and after the intervention. Height (in centimeters) was measured using a wall-mounted height-measuring device, barefoot. Weight was measured with light clothing and no shoes, and the same electronic scale is used before and after the intervention. The previous calibration error may be ±100 g. BMI is calculated in kg/m2. WC is measured while standing, with the tape measure placed above the umbilical cord, against the skin.
Venous blood was drawn at 5:30 am after fasting for 12 h. Blood samples were sent to the laboratory within an hour. The serum levels of fasting blood glucose (FBG), total cholesterol (TC), TG, low density lipoprotein (LDL) cholesterol, and high density lipoprotein cholesterol (HDL) were measured using the standard enzymatic procedure (Hitachi LABOSPECT 008 AS, Japan).
Non-fasting TG was taken 120 min after eating 100 g of standard carbohydrate provided by China Foods Limited (Beijing, China) (18). Blood was used with K2EDTA anticoagulant for HbA1c and determined by high-performance liquid chromatography (HPLC) (Tosoh HLC-723G11, Japan).
The commercial Roche test on the Cobas 8000/801 automatic analyzer (Roche Diagnostics, Mannheim, Germany) was used to measure fasting insulin (FI) by electrochemiluminescence (ECL). HOMA-IR was calculated by the formula HOMA-IR = FBG (mmol/L) × FI (mIU/L)/22.5 (19).
LBGI was used to evaluate the frequency and degree of hypoglycemia based on the mathematical processing of BG measurements. The specific calculation methods were as follows:
1) The BG value was transformed:
Xi is the converted BG; G is the measured BG.
2) The risk value for BG was calculated according to Xi:
N is the total number of blood glucose measurements; rl is the risk of hypoglycemia (Xi<0) (20).
ADAs of beinaglutide were measured by the electrochemiluminescence method, which is based on beinaglutide labeled with biotin and metal ruthenium, using the classic bridging principle to detect ADAs against beinaglutide in human serum. The ruthenium in the complex “biotin-labeled beinaglutide–ADAs–ruthenium-labeled beinaglutide” excites a light signal value at 620 nm and is captured by an MSD (Meso Scale Discovery) instrument. The captured signal intensity is proportional to the titer of ADAs.
Baseline and post-intervention data were summarized as mean and standard deviation (SD) for normal variables, median and quartile ranges for abnormal variables, and number and percentage for categorical variables. Baseline and 6-month follow-up characteristics of each group were compared using an independent two-sample t test or chi-square test. Paired t test was used to compare the differences before and after the same intervention. The missing values were interpolated with the mean. Double-tailed P value<0.05 was considered statistically significant. SPSS Statistics 25 (IBM) software was used for statistical analysis.
Table 1 shows the baseline demographic characteristics of the study population. There were no significant differences in clinical and biochemical indexes among all groups. Of the 490 prescreened patients, 134 agreed to participate in the study. Of the 134 participants with T2D starting on treatment, 101 patients completed the study (Figure 1).
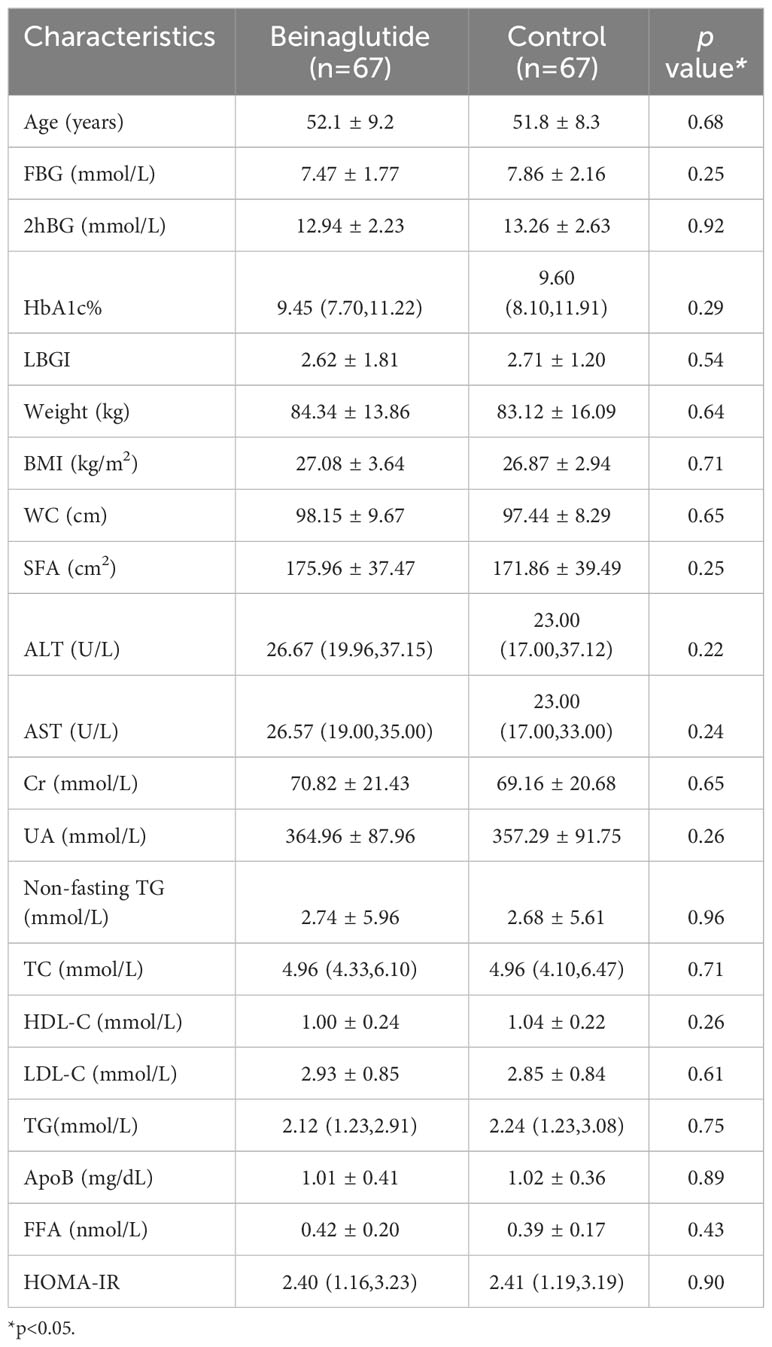
Table 1 Patients’ characteristics on baseline.

Figure 1 Study design and flowchart.
Compared with the control group, the beinaglutide group had significant reductions in 2hBG (p< 0.01) and LBGI (p = 0.02) (Table 2). HbA1c decreased in both groups relative to baseline (p< 0.01) (Table 2). There was no significant difference in HbA1c levels between groups (p = 0.86). In the beinaglutide group, one had treatment-emergent beinaglutide ADAs, exhibiting low titers. For the lipid profile, beinaglutide significantly reduced FTG and non-fasting triglyceride (TG) levels after 6 months of supplementation (p<0.01) (Table 2). At the same time, significant reductions in weight, WC, hip, and BMI were observed (p<0.05) (Table 2). The values of HOMA-IR were decreased to a statistically higher degree with beinaglutide treatment (p<0.01) (Table 2).
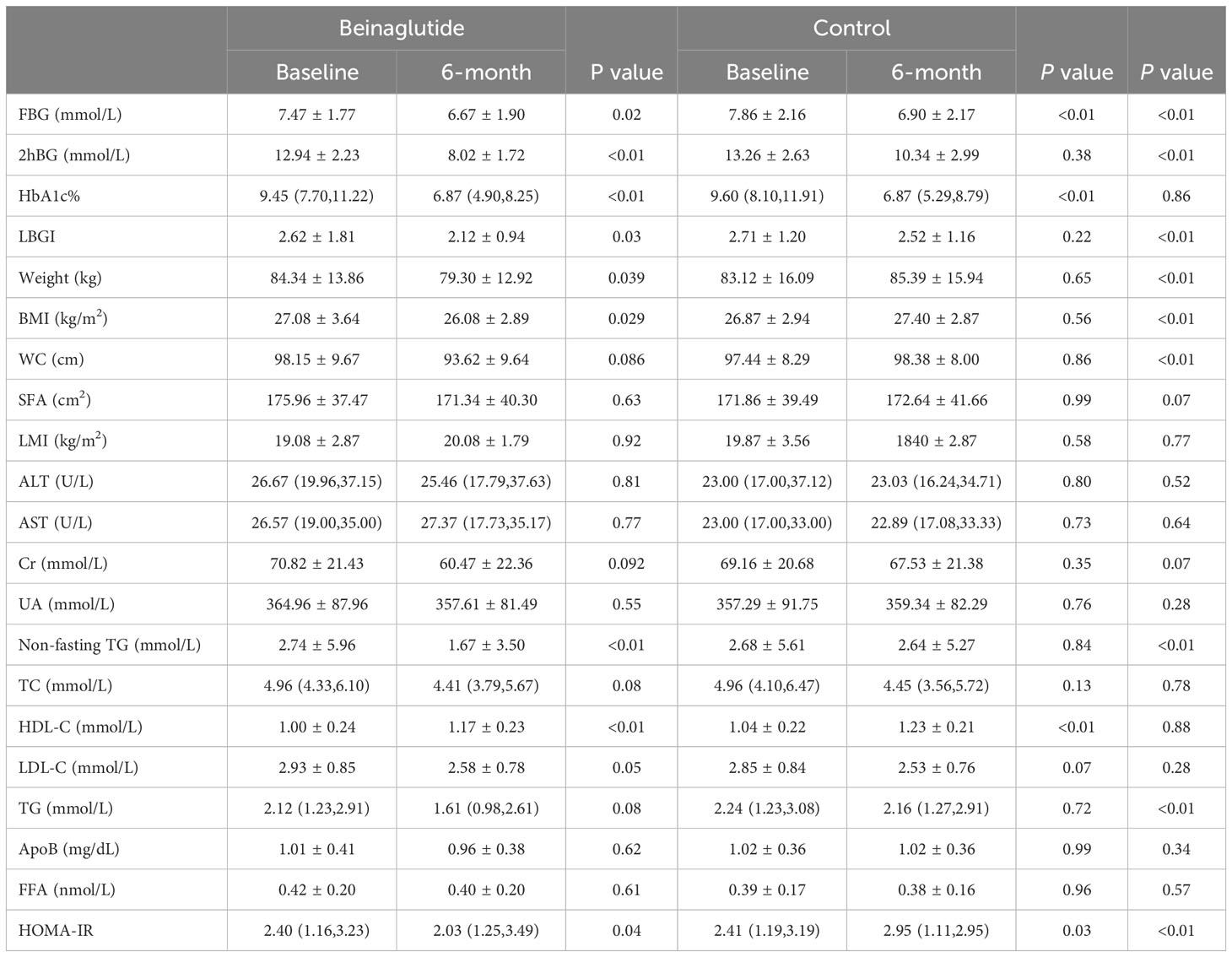
Table 2 Comparison of the differences between groups.
This study aimed to evaluate the efficacy and safety of beinaglutide in treatment of T2D. After 6 months, HbA1c decreased in both groups relative to baseline and the beinaglutide group had significant reductions in 2hBG compared with the control group. The LBGI of the test group was significantly lower than that of the control group, and no patient experienced hypoglycemia in the test group, suggesting that beinaglutide offered a treatment option that improved glycemic control with a low risk of hypoglycemia. Similar results were obtained in the study by Gao, Lijun et al. (13). Beinaglutide is a short-acting recombinant human GLP-1 (21). GLP-1, as a type of incretins, secreted from L cells in the distal ileum and colon within minutes of oral glucose load (22). Islet B cells contain GLP-1 receptors that, when activated by GLP-1, enhance insulin secretion. Incretins are responsible for around 50% to 70% of total insulin release (23). This clarifies why, around 50 years ago, it was observed that oral glucose intake leads to higher insulin release compared with an equal amount of intravenous glucose (23).
Beinaglutide is a recombinant human GLP-1 analog with an identical amino acid sequence to native human GLP-1 (24). Zhang et al. postulated that beinaglutide may facilitate its beneficial effects by stimulating GLP-1R-dependent 3′5′-cyclic adenosine monophosphate (cAMP) generation in HEK 293 cells (12). This in turn augments insulin secretion in mice in response to glucose. Furthermore, beinaglutide has a half-life of approximately 5 min (25), akin to the half-life of endogenous GLP-1, which ranges from approximately 1.5 to 5 min. Consequently, compared with other long-acting GLP-1 receptor agonists, beinaglutide has a shorter onset time, rapidly reduces blood glucose levels, and more effectively controls postprandial blood glucose. At the 6-month follow-up in this study, the beinaglutide group showed a significant improvement in their 2hBG levels when compared with the control group. Additionally, the level of HbA1c decreased significantly from the initial value, and this reduction was as effective as that achieved with aspart 30. However, beinaglutide carries a reduced hypoglycemia risk. At the 6-month follow-up, the beinaglutide group exhibited significantly lower LBGI levels compared with the control group, which can be attributed to beinaglutide’s glucose-dependent hypoglycemic mechanism (26). In this study, antidrug antibodies to beinaglutide, a compound exhibiting 100% homology with human endogenous GLP-1 and minimal immunogenicity, were detected for the first time. Out of the 49 patients in the beinaglutide group, one patient generated ADAs during the 6 months of treatment. The patient with treatment-emergent beinaglutide ADAs showed a significant increase in FBG and HbA1c compared with baseline at the 6-month follow-up, and no weight loss was observed (Figure 2), indirectly confirming the production of ADAs. This patient was not observed to have a progressive increase in titers in 6 months. In summary, beinaglutide exhibits low hypoglycemia risk, minimal immunogenicity, and strong safety while effectively lowering blood glucose levels.
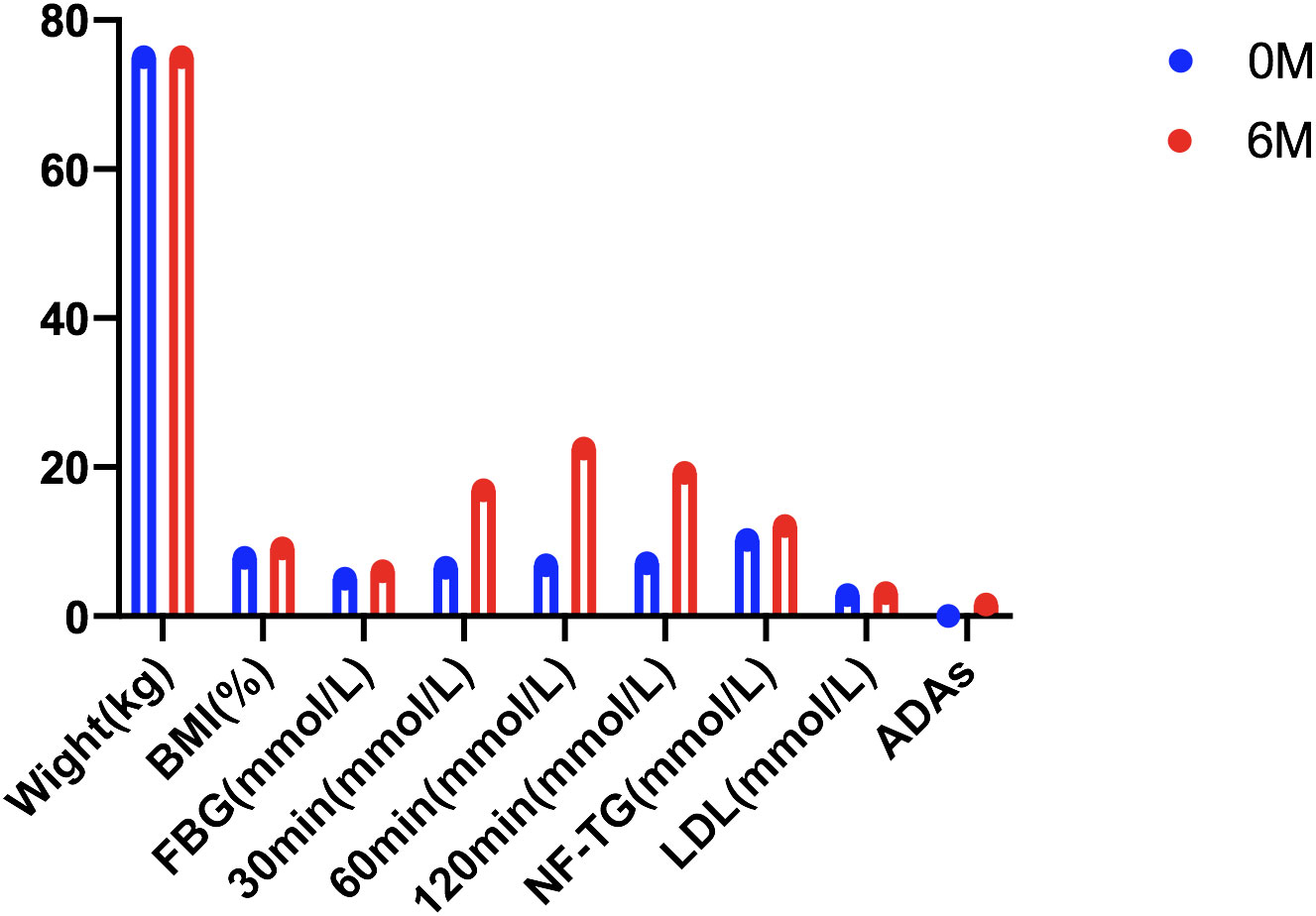
Figure 2 Clinical indicators of the patient with treatment-emergent beinaglutide ADAs.
Postprandial elevated lipid levels are a significant aspect of dyslipidemia in patients with T2DM and are linked to atherosclerosis (5). Animal experiments have shown that beinaglutide can counteract weight gain from a high-fat diet, promote fat storage in adipose tissue, and improve the lipid profile associated with obesity (24). This study examined the effect of beinaglutide on non-fasting TG in T2D subjects for the first time, with a prominent decrease after use. In the fasting state, only hepatogenic lipoproteins are present in plasma, whereas in the non-fasting state, enterogenic lipoproteins coexist with hepatogenic lipoproteins in plasma (27). The development of atherosclerosis begins with damage to the endothelium of the artery, after which lipoproteins enter the intima (28). The monocytes are then activated and transformed into foam cells in the lining of the artery; then, the foam cells collect cholesterol and triglycerides from the blood (29). The exact mechanism through which GLP-1 and GLP-1 RAs influence postprandial lipid and lipoprotein metabolism is not fully elucidated at this time. However, it is commonly associated with enhanced clearance of intestinal lipoproteins. Beinaglutide, a recombinant human GLP-1, notably slows down the emptying of the stomach (30), a trait shared to some extent by the GLP-1 RAs used in clinical practice. This delayed gastric emptying results in a postponement of the passage of high-fat foods into the small intestine. GLP-1 suppresses gastric lipase secretion and intestinal movement (31). The findings of this study suggest that beinaglutide is effective in reducing body weight, alleviating insulin resistance, and improving insulin sensitivity. Insulin is a strong stimulator of lipoprotein lipase, speeding up the removal of triglyceride-rich particles after meals (32). In conclusion, it is plausible to suggest that various mechanisms, including those mentioned, could contribute to the impact of beinaglutide and other GLP-1 RAs on postprandial lipid metabolism. This study demonstrated that beinaglutide can influence postprandial TG in an “anti-atherogenic” fashion in patients with T2D, which related to atherosclerosis and CVD outcomes (5).
Our study had some limitations. Firstly, it was a randomized but not a placebo controlled trial. Secondly, it is a non-multicenter, non-double-blind study with a short follow-up time. Thirdly, only the ADAs of beinaglutide in the test group were tested, and the number of subjects was relatively small. All of this might have significantly affected the quality of the data.
Our study has indicated that beinaglutide improved glycemic control with a low risk of hypoglycemia and low titers of beinaglutide ADAs. In addition, beinaglutide reduced non-fasting TG, slowing atherogenesis and the progression of CVD via direct and indirect mechanisms, which may be a benefit beyond its pleiotropic effects.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethical Committee of Qingpu Branch of Zhongshan Hospital Affiliated to Fudan University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
C-YH: Conceptualization, Writing – review & editing, Investigation, Writing – original draft. J-PL: Writing – review & editing, Data curation, Methodology. X-MY: Writing – review & editing, Validation. H-YJ: Writing – review & editing, Formal analysis. W-WX: Writing – review & editing, Resources. PW: Resources, Writing – review & editing. MZ: Writing – review & editing, Conceptualization.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The work was supported by Shanghai Municipal Commission of Science and Technology (No. 17DZ1910605 and No. 15411970200), Shanghai Municipal Health Commission (No. 201540140 and No. 20204Y0060), Shanghai Qingpu District Science and Technology Commission (No. QKY2021-03), and Shanghai Qingpu District Health Commission (No. QWJ2022-01 and W2019-41).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer PY declared a shared affiliation with the authors to the handling editor at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ADAs, anti-drug antibodies; T2D, type 2 diabetes; 2hBG, 2h-postprandial blood glucose; LBGI, low blood glucose index; HbA1c, glycated hemoglobin; TG, triglycerides; WC, waist circumference; BMI, body mass index; CVD, cardiovascular disease; GLP-1RAs, glucagon like peptide-1 receptor agonists; WHO, World Health Organization; DKA, ketoacidosis; HHS, hyperosmotic hyperglycemia syndrome; Tid, three times daily; BG, blood glucose; HOMA-IR, insulin sensitivity index; FBG, fasting blood glucose; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; FI, fasting insulin.
1. Chavda VP, Ajabiya J, Teli D, Bojarska J, Apostolopoulos V. Tirzepatide, a new era of dual-targeted treatment for diabetes and obesity: A mini-review. Molecules (Basel Switzerland) (2022) 27(13):4315. doi: 10.3390/molecules27134315
2. Liu L, Zhang J, Cheng Y, Zhu M, Xiao Z, Ruan G, et al. Gut microbiota: A new target for T2DM prevention and treatment. Front Endocrinol (2022) 13:958218. doi: 10.3389/fendo.2022.958218
3. Caussy C, Aubin A, Loomba R. The relationship between type 2 diabetes, NAFLD, and cardiovascular risk. Curr Diabetes Rep (2021) 21(5):15. doi: 10.1007/s11892-021-01383-7
4. Hariharan R, Odjidja EN, Scott D, Shivappa N, Hébert JR, Hodge A, et al. The dietary inflammatory index, obesity, type 2 diabetes, and cardiovascular risk factors and diseases. Obes Rev (2022) 23(1):e13349. doi: 10.1111/obr.13349
5. Novodvorský P, Haluzík M. The effect of GLP-1 receptor agonists on postprandial lipaemia. Curr Atheroscl Rep (2022) 24(1):13–21. doi: 10.1007/s11883-022-00982-3
6. Kajikawa M, Maruhashi T, Kishimoto S, Matsui S, Hashimoto H, Takaeko Y, et al. Target of triglycerides as residual risk for cardiovascular events in patients with coronary artery disease- Post Hoc analysis of the FMD-J study A. Circ journal: Off J Japanese Circ Soc (2019) 83(5):1064–71. doi: 10.1253/circj.CJ-18-1082
7. Miura Y, Suzuki Y, Kanamaru H, Shiba M, Yasuda R, Toma N, et al. Higher non-fasting serum triglyceride preceding the carotid stenosis progression. Neurologia medico-chirurgica (2021) 61(7):422–32. doi: 10.2176/nmc.oa.2020-0430
8. Miura Y, Kanamaru H, Yasuda R, Toma N, Suzuki H. Nonfasting triglyceride as an independent predictor of carotid restenosis after carotid endarterectomy or carotid artery stenting. World Neurosurg (2021) 156:e415–25. doi: 10.1016/j.wneu.2021.09.091
9. Bendotti G, Montefusco L, Lunati ME, Usuelli V, Pastore I, Lazzaroni E, et al. The anti-inflammatory and immunological properties of GLP-1 Receptor Agonists. Pharmacol Res (2022) 182:106320. doi: 10.1016/j.phrs.2022.106320
10. Scheen AJ. Dual GIP/GLP-1 receptor agonists: New advances for treating type-2 diabetes. Annales d’endocrinologie (2023) 84(2):316–21. doi: 10.1016/j.ando.2022.12.423
11. Marx N, Husain M, Lehrke M, Verma S, Sattar N. GLP-1 receptor agonists for the reduction of atherosclerotic cardiovascular risk in patients with type 2 diabetes. Circulation (2022) 146(24):1882–94. doi: 10.1161/CIRCULATIONAHA.122.059595
12. Zhang F, Chen Z, Wu D, Tian L, Chen Q, Ye Y, et al. Recombinant human GLP-1 beinaglutide regulates lipid metabolism of adipose tissues in diet-induced obese mice. iScience (2021) 24(12):103382. doi: 10.1016/j.isci.2021.103382
13. Wen Q, Fang S, Liang Y, Tian Y, Chen Y, Yuan J, et al. Short-term effect of beinaglutide combined with metformin versus metformin alone on weight loss and metabolic profiles in obese patients with polycystic ovary syndrome: a pilot randomized trial. Front Endocrinol (2023) 14:1156521. doi: 10.3389/fendo.2023.1156521
14. Gao L, Huang H, Zhang L, Zhang N, Fu Y, Zhu D, et al. Comparison of beinaglutide versus metformin for weight loss in overweight and obese non-diabetic patients. Exp Clin Endocrinol Diabetes (2022) 130(6):358–67. doi: 10.1055/a-1608-0345
15. Deng X, Zhang C, Wang P, Wei W, Shi X, Wang P, et al. Cardiovascular benefits of Empagliflozin are associated with gut microbiota and plasma metabolites in type 2 diabetes. J Clin Endocrinol Metab (2022) 107(7):1888–96. doi: 10.1210/clinem/dgac210
16. Jiang C, Yang R, Kuang M, Yu M, Zhong M, Zou Y. Triglyceride glucose-body mass index in identifying high-risk groups of pre-diabetes. Lipids Health Dis (2021) 20(1):161. doi: 10.1186/s12944-021-01594-7
17. Wang G, Wu P, Qiu Y, Dong X, Wang Y, Chi Y, et al. Effect of beinaglutide treatment on weight loss in Chinese patients with type 2 diabetes mellitus and overweight/obesity. Arch Endocrinol Metab (2021) 65(4):421–7. doi: 10.20945/2359-3997000000388
18. Tada H, Nomura A, Yoshimura K, Itoh H, Komuro I, Yamagishi M, et al. Fasting and non-fasting triglycerides and risk of cardiovascular events in diabetic patients under statin therapy. Circ J (2020) 84(3):509–15. doi: 10.1253/circj.CJ-19-0981
19. Tahapary DL, Pratisthita LB, Fitri NA, Marcella C, Wafa S, Kurniawan F, et al. Challenges in the diagnosis of insulin resistance: Focusing on the role of HOMA-IR and Tryglyceride/glucose index. Diabetes Metab syndrome (2022) 16(8):102581. doi: 10.1016/j.dsx.2022.102581
20. Kovatchev B, Meng Z, Cali AMG, Perfetti R, Breton MD. Low blood glucose index and hypoglycaemia risk: insulin glargine 300 U/mL versus insulin glargine 100 U/mL in type 2 diabetes. Diabetes Ther (2020) 11(6):1293–302. doi: 10.1007/s13300-020-00808-y
21. Zhang YL, Zhou C, Li XF, Yang MN, Tao L, Zheng XY, et al. Beinaglutide showed significant weight-loss benefit and effective glycaemic control for the treatment of type 2 diabetes in a real-world setting: a 3-month, multicentre, observational, retrospective, open-label study. Obes Sci Pract (2019) 5:366–75. doi: 10.1002/osp4.342
22. Müller TD, Finan B, Bloom SR, D’Alessio D, Drucker DJ, Flatt PR, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab (2019) 30:72–130. doi: 10.1016/j.molmet.2019.09.010
23. Shaefer CF Jr, Kushner P, Aguilar R. User’s guide to mechanism of action and clinical use of GLP-1 receptor agonists. Postgraduate Med (2015) 127(8):818–26. doi: 10.1080/00325481.2015.1090295
24. Fang X, Du Z, Duan C, Zhan S, Wang T, Zhu M, et al. Beinaglutide shows significantly beneficial effects in diabetes/obesity-induced nonalcoholic steatohepatitis in ob/ob mouse model. Life Sci (2021) 270:118966. doi: 10.1016/j.lfs.2020.118966
25. Ding B, Hu Y, Yuan L, Yan RN, Ma JH. Effectiveness of beinaglutide in a patient with late dumping syndrome after gastrectomy: A case report. Medicine (2021) 100(21):e26086. doi: 10.1097/MD.0000000000026086
26. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab (2018) 27(4):740–56. doi: 10.1016/j.cmet.2018.03.001
27. Langsted A, Nordestgaard BG. Nonfasting versus fasting lipid profile for cardiovascular risk prediction. Pathology (2019) 51(2):131–41. doi: 10.1016/j.pathol.2018.09.062
28. Libby P. The changing landscape of atherosclerosis. Nature (2021) 592(7855):524–33. doi: 10.1038/s41586-021-03392-8
29. Fan J, Watanabe T. Atherosclerosis: known and unknown. Pathol Int (2022) 72(3):151–60. doi: 10.1111/pin.13202
30. Maselli DB, Camilleri M. Effects of GLP-1 and its analogs on gastric physiology in diabetes mellitus and obesity. Adv Exp Med Biol (2021) 1307:171–92. doi: 10.1007/5584_2020_496
31. Gribble FM, Reimann F. Metabolic Messengers: glucagon-like peptide 1. Nat Metab (2021) 3(2):142–8. doi: 10.1038/s42255-020-00327-x
Keywords: type 2 diabetes, beinaglutide, anti-drug antibodies, non-fasting triglyceride, cardiovascular disease
Citation: Han C-Y, Lu J-P, Ye X-M, Jin H-Y, Xu W-W, Wang P and Zhang M (2023) Effect of beinaglutide combined with metformin versus aspart 30 with metformin on metabolic profiles and antidrug antibodies in patients with type 2 diabetes: a randomized clinical trial. Front. Endocrinol. 14:1267503. doi: 10.3389/fendo.2023.1267503
Received: 26 July 2023; Accepted: 17 November 2023;
Published: 06 December 2023.
Edited by:
Qi Pan, Peking University, ChinaReviewed by:
Peng Yu, Fudan University, ChinaCopyright © 2023 Han, Lu, Ye, Jin, Xu, Wang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Zhang, MTgxMTYwMTYxODdAMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.