 Xiaosong Li
Xiaosong Li Wei Ding
Wei Ding Hong Zhang
Hong Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol. , 04 December 2023
Sec. Cancer Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1256209
Objectives: This network meta-analysis assesses the outcomes of seven endoscopic approaches, offering valuable insights for researchers and practitioners in choosing the best method for thyroid cancer patients.
Methods: A systematic literature search was conducted in the PubMed, Embase and Web of Science databases up to March 2023. The analysis included seven endoscopic approaches, with a focus on their respective outcomes through network meta-analysis.
Results: This meta-analysis included 44 studies involving 8,672 patients. The axillo-bilateral breast approach (ABBA) and unilateral axillo-breast approach (UABA) showed advantages in terms of reduced operative time compared to other approaches (MD = 19.66 minutes, 95% CI = -31.66 to 70.98; MD = 30.32 minutes, 95% CI = -1.45 to 62.09, respectively). The UABA and anterior chest approach (ACA) exhibited superiority in controlling intraoperative bleeding (MD = -3.37 mL, 95% CI = -22.58 to 15.85; MD = -13.77 mL, 95% CI = -28.85 1.31, respectively). UABA and ACA also showed advantages in reducing hospital stays (MD = -0.39 days, 95% CI = -1.48 to 0.71; MD = -0.26 days, 95% CI = -1.33 to 0.81, respectively). The transoral approach (OA) yielded results comparable to those of conventional open thyroidectomy (COT) and outperformed other endoscopic surgeries with regards to lymph node retrieval and metastatic lymph node assessment. For the stimulated serum thyroglobulin (TG) levels, no significant difference was observed between bilateral axillo-breast approach (BABA) and OA compared to COT. However, chest-breast approach (CBA) showed significantly lower levels than COT (MD=-0.40 ng/ml, 95% CI =-0.72 to -0.09). Patients in the gasless unilateral transaxillary approach (GUA) group experienced a significant improvement in cosmetic satisfaction (MD=-2.08, 95% CI =-3.35 to -0.82). Importantly, no significant difference was observed in the incidence of surgical complications between endoscopic thyroidectomy and COT.
Conclusion: Endoscopic thyroid surgery is a safe and effective choice for thyroid cancer patients. Different approaches have their advantages, allowing personalized selection based on the patient’s needs. ABBA and UABA have shorter operative times, while UABA and ACA excel at controlling bleeding and shortening hospital stays. OA shows promise for lymph node assessment. These findings contribute to the growing evidence supporting endoscopic methods, expanding treatment options for thyroid cancer patients.
Thyroid cancer, the most common endocrine-related cancer, has been increasing rapidly in recent years and is particularly prevalent in young women (1). Conventional open thyroidectomy (COT) is the standard surgical treatment for thyroid cancer; however, the conspicuous scarring and the associated emotional burden pose significant challenges, especially for young female patients. Endoscopic thyroidectomies were first performed in 1997 (2). This minimally invasive surgery not only provides better cosmetic results, but also contribute to reduces surgical complications. The introduction of endoscopic thyroidectomy has attracted the interest of a wide range of surgeons. Over the past 20 years, lumpectomies have developed rapidly. The most common surgical approaches are the gasless unilateral transaxillary approach (GUA), bilateral axillo-breast approach (BABA), axillo-bilateral breast approach (ABBA), unilateral axillo-breast approach (UABA), chest-breast approach (CBA), anterior chest approach (ACA) and transoral approach (OA).
It is important to acknowledge that endoscopic surgeries are not uniformly “minimally invasive” and do not universally reduce invasiveness. While they offer advantages in terms of cosmesis and surgical complication reduction, these advantages may not be consistently realized in every case. Endoscopic surgeries, while typically associated with reduced scarring and fewer complications, can, in certain circumstances, present unique challenges. For example, the use of unconventional entry sites can increase the risk of injury to critical nerves, such as brachial plexus injury with the axillary approach (3), or central nerve palsy with the transoral approach can lead to central nerve palsy (4). In light of these nuances and the potential variability in outcomes, a comprehensive evaluation of the efficacy and safety of endoscopic thyroid surgery is imperative. Previous meta-analyses have often compared different surgical approaches solely with COT, leaving critical gaps in our understanding. To address these limitations and provide a more nuanced assessment, we employ network meta-analysis (NMA). This approach integrates a wealth of clinical experiences, allowing us to offer a more balanced perspective on the advantages and disadvantages of endoscopic thyroid surgery across various surgical techniques. Network meta-analysis can showcase direct and indirect comparison results (5). Through NMA, we aim to gain a more comprehensive understanding of when and how endoscopic procedures can truly be minimally invasive and when they might not offer significant advantages over conventional approaches.
In summary, this network meta-analysis seeks to provide a comprehensive evaluation of endoscopic thyroid surgery, considering the variable nature of “minimally invasive” outcomes. By doing so, we aim to offer a more detailed perspective on the true merits and limitations of endoscopic surgery in the treatment of thyroid cancer.
Our systematic review was designed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PROSPERO) guidelines (6) and registered with PROSPERO (CRD42023430413). Ethical approval or registration was not required as this study involved an analysis of existing published data.
The PubMed, Embase and Web of Science Core Collection (WoSCC) were searched up to March 28, 2023. The following keywords and comprehensive combinations thereof were included: (“endoscopic” OR “endoscopic surgery” OR “endoscopic-surgery”) AND (“thyroid cancer” OR “thyroid carcinoma”) AND (“thyroidectomy” OR “ thyroid surgery”).
The inclusion criteria were as follows: (1) Original English articles; (2) studies comparing endoscopic surgery with COT or different endoscopic surgical approaches; (3) studies reporting indicators such as surgical results or complications; and (4) studies in which the patients were diagnosed with thyroid cancer. The exclusion criteria were as follows: (1) letters, reviews, meeting abstracts, case reports, and editorials; (2) studies without control groups; and (3) studies that did not report original data.
Two researchers independently extracted the data. We documented study characteristics (the first author, publication year, surgery approach, country, study design, number of patients, age, extent of surgery and follow-up); surgical outcomes [operative time, intraoperative bleeding volume, hospital days, volume of drainage, duration of drainage, retrieved LNs, metastatic LNs, stimulated serum thyroglobulin (TG) levels and TG levels after postoperative radioactive iodine (RAI)], and surgical complications (transient hypocalcemia, permanent hypocalcemia, transient vocal cord palsy, permanent vocal cord palsy, transient hypoparathyroidism, permanent hypoparathyroidism, postoperative bleeding, chyle leakage, hematoma, seroma, recurrence and infection).
Two researchers independently evaluated the quality of the articles using the Newcastle-Ottawa Scale (NOS), and disagreements were settled through joint discussion. An article with an NOS score ≥ 6 was considered a high-quality study (7); the NOS scores of the articles we included were all > 6.
Data analysis was conducted using Stata14.1 software (Stata Corporation, College Station, TX, USA). Continuous variables (operative time, intraoperative bleeding volume, hospital days, volume of drainage, duration of drainage, retrieved LNs, metastatic LNs, stimulated TG levels, and TG levels after postoperative RAI) were recorded as mean differences (MD) with 95% confidence intervals (CI). Odds risks (OR) with 95% CI were calculated for dichotomous variables (transient hypocalcemia, permanent hypocalcemia, transient vocal cord palsy, permanent vocal cord palsy, transient hypoparathyroidism, permanent hypoparathyroidism, postoperative bleeding, chyle leakage, hematoma, seroma, recurrence, and infection). The consistency of the network was verified using local and global inconsistency tests. We used the node-splitting method to detect local inconsistencies between direct and indirect evaluations; If P< 0.05, local inconsistency was considered to exist. The surfaces under the cumulative ranking (SUCRA) curves and mean ranks were used to rank the eight surgical methods. The higher the SUCRA value, the higher the efficiency. We assessed potential publication bias by “comparison-adjusted” funnel plots.
A total of 44 articles, involving a total of 8672 patients, were included in the NMA (Figure 1). Of these, 38 were retrospective studies and six were prospective studies. Details of the articles’ characteristics are listed in Table 1. Fifteen studies compared CBA with COT, five compared BABA with COT, eight compared OA with COT, two compared OA with CBA, nine compared GUA with COT, two compared ACA with COT, and two compared UABA with COT or CBA.
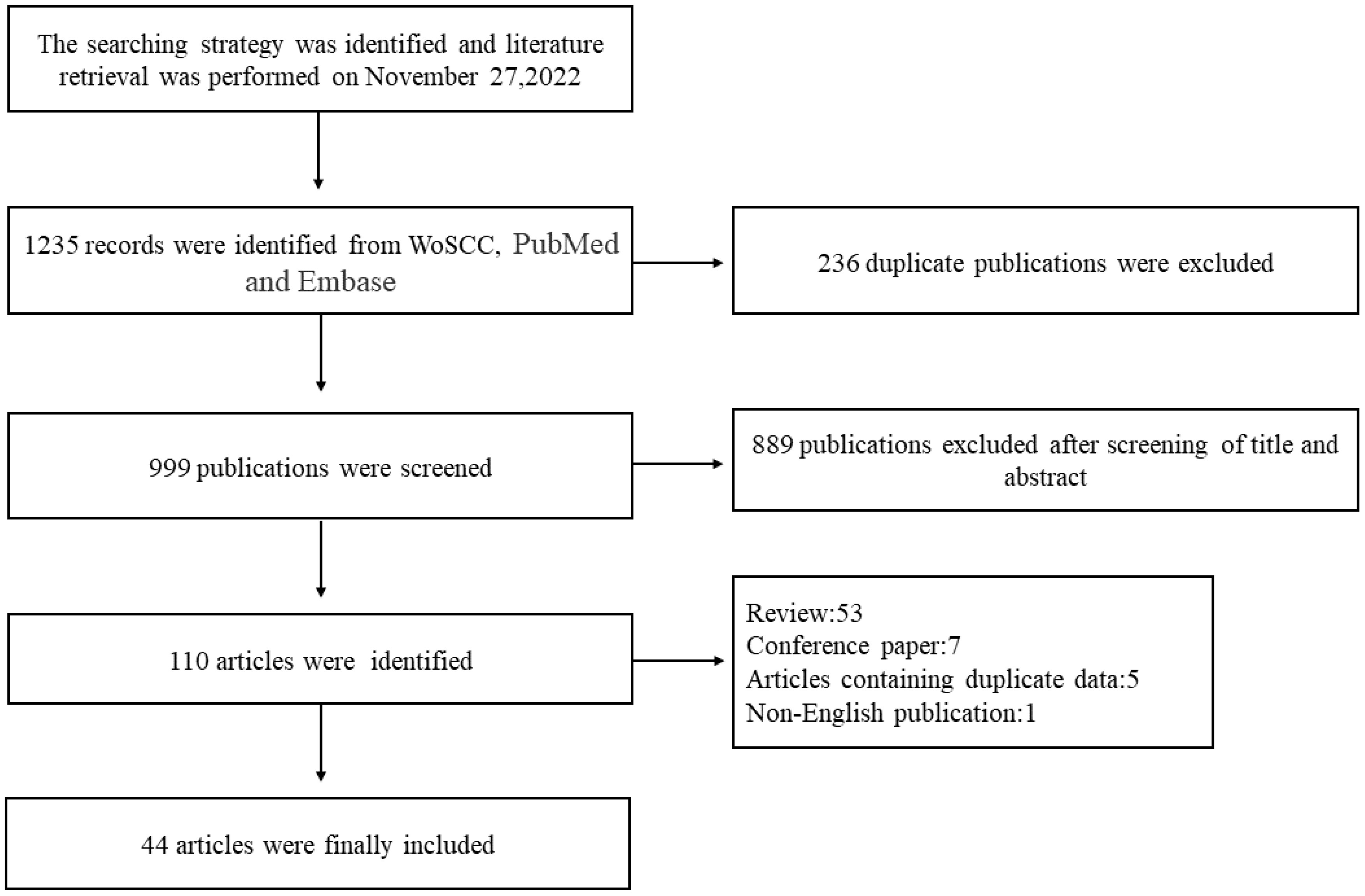
Figure 1 Flowchart of article screening. WoSCC, Web of Science Core Collection.
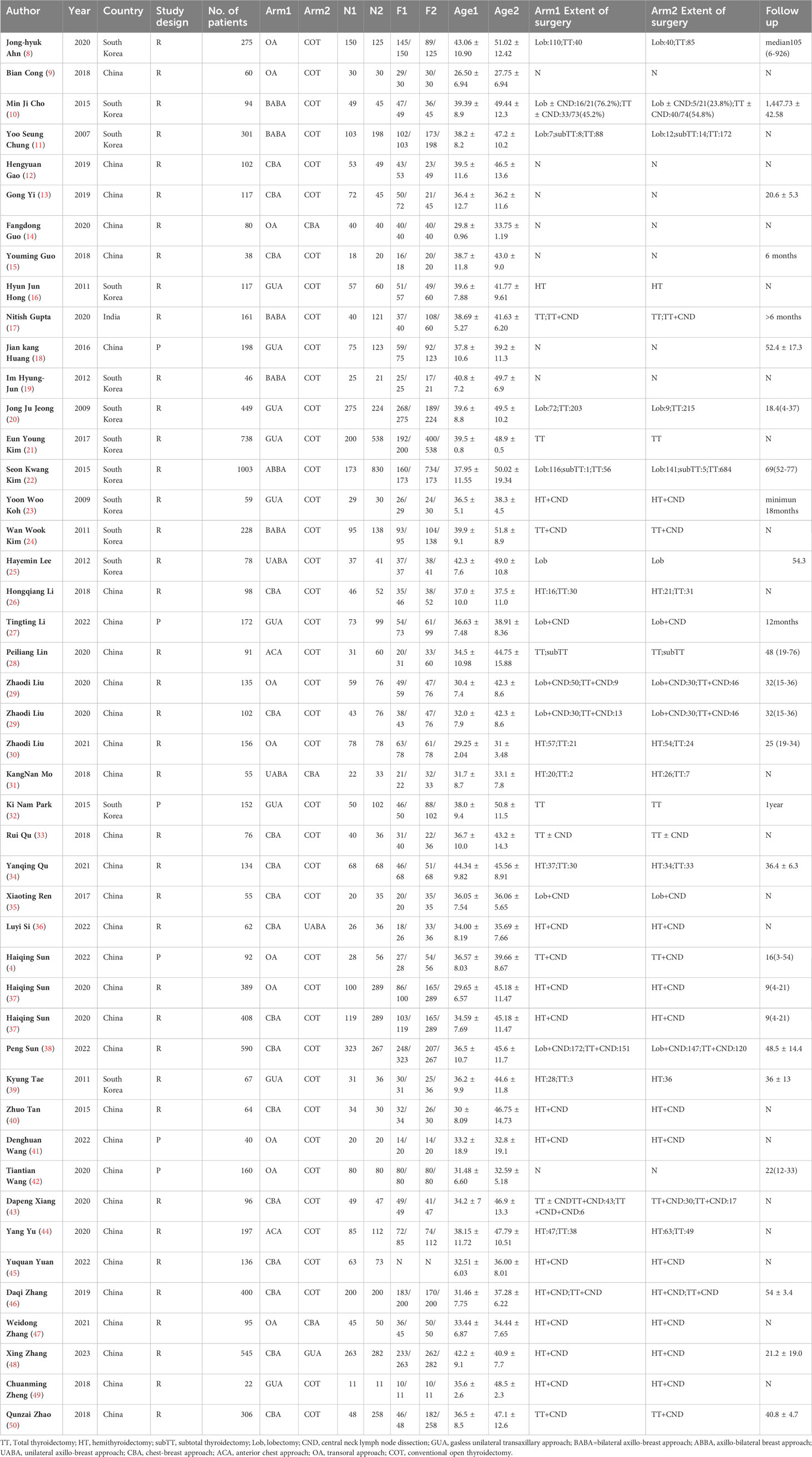
Table 1 Characteristics of meta-analysis included studies.
Operative time was reported in 41 studies. A total of 8301 patients and eight surgical methods were included. The network relationships for different surgical modalities are shown in Figure 2A. The global inconsistency test was not significant (p= 0.7353), and a comparison of the estimated operative time of different surgical methods using NMA is shown in the Table 2. There was no significant difference (p>0.05) in operative time between the direct and indirect evaluations of the node-splitting models of local consistency. The shortest operative times were for the COT (95.6%), ABBA (71.5%), and UABA (61.4%), according to the SUCRA score.
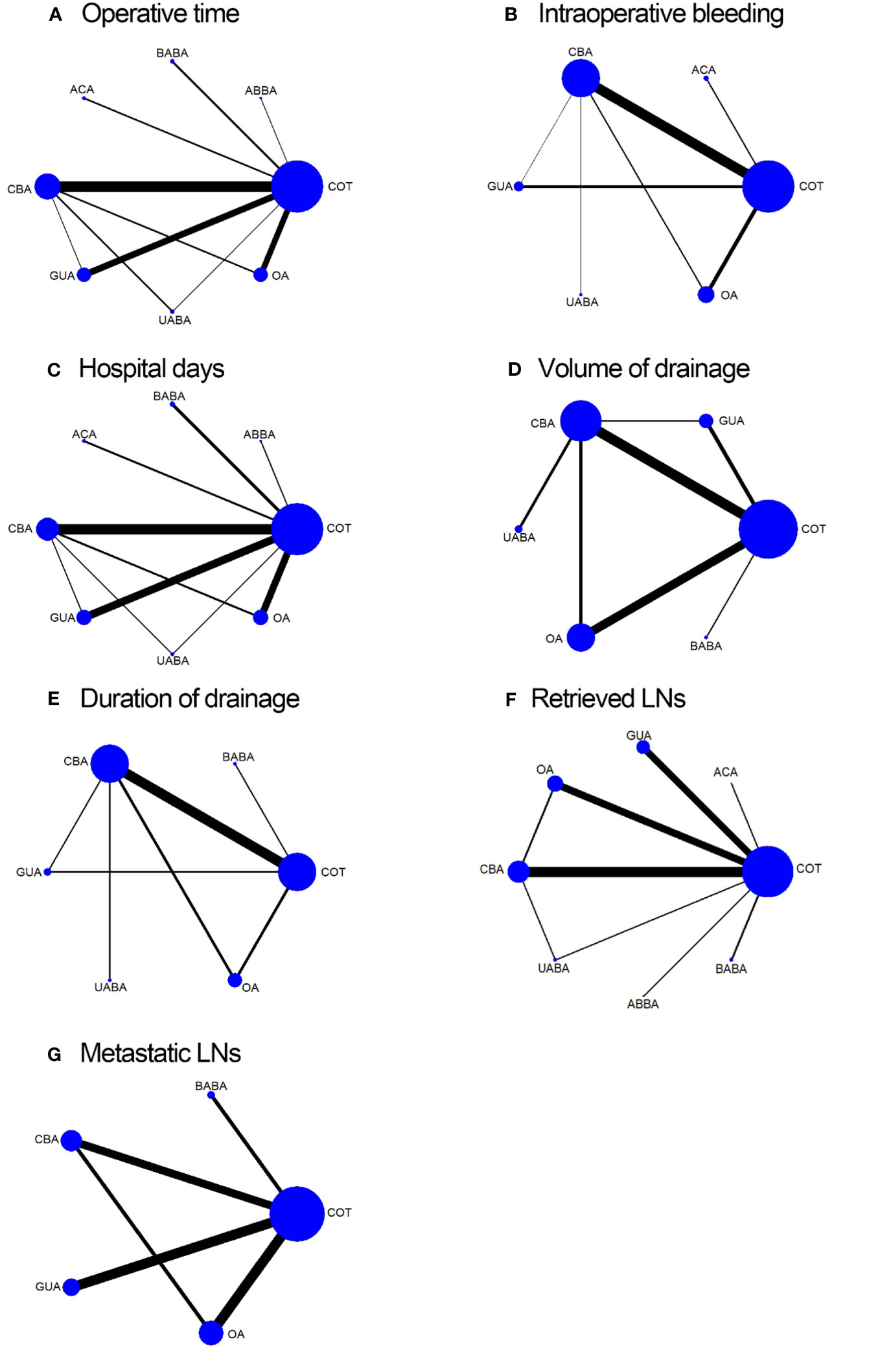
Figure 2 Network map of eligible comparisons for operative time (A); intraoperative bleeding volume (B); hospital days (C); volume of drainage (D); duration of drainage (E); retrieved LNs (F); metastatic LNs (G).
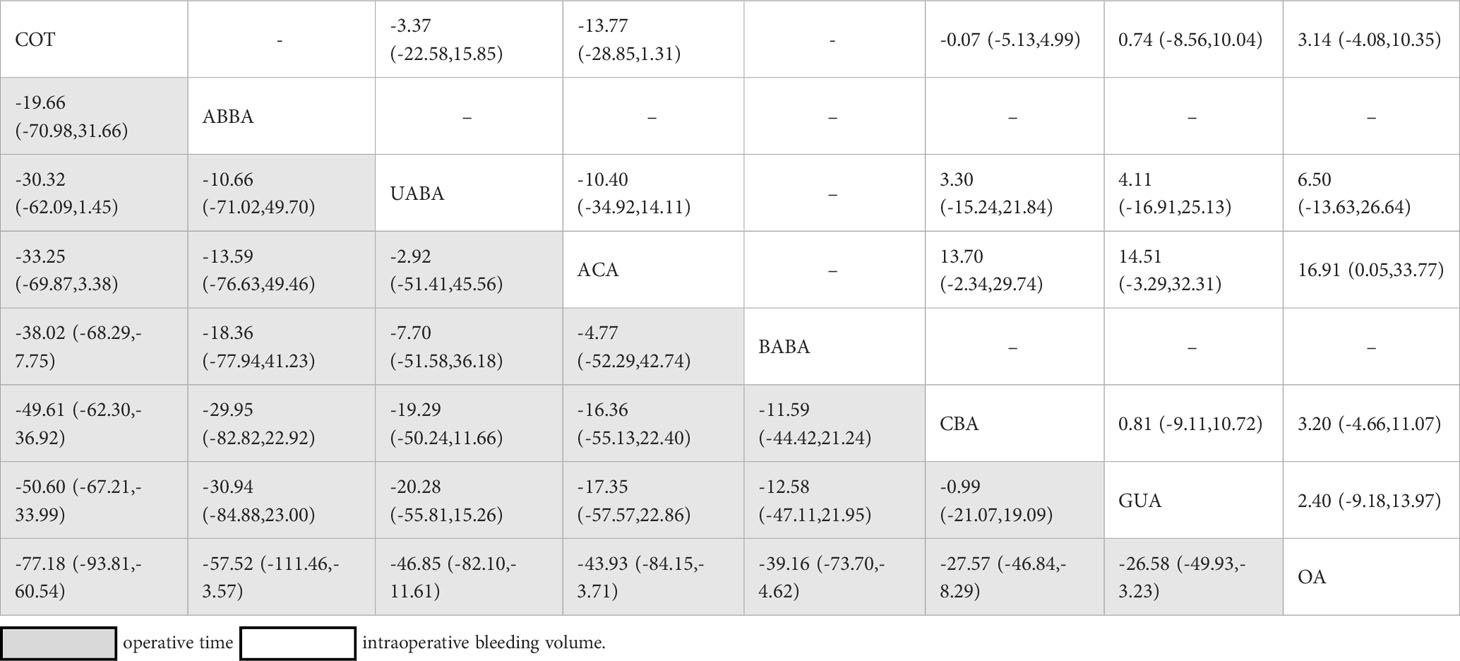
Table 2 Network estimates of surgery comparisons for operative time and intraoperative bleeding volume.
Twenty-five studies, involving a total of 4440 patients and six surgical methods, reported intraoperative bleeding volume. The network relationships between the different surgical methods are shown in Figure 2B. The global inconsistency test was not significant (p=0.6823), and the comparison of the NMA estimation of intraoperative bleeding volume between the different surgical methods is shown in Table 2. There was no significant difference (p>0.05) between the direct and indirect evaluations of the node-splitting models of local consistency for intraoperative bleeding volume. The surgical methods with the least amount of intraoperative bleeding were ACA (92.4%), UABA (57.1%), and COT (45.5%) according to the SUCRA score.
Hospital days were reported in 34 studies, involving a total of 7682 patients and a comparison of eight surgical methods. The network relationships between the different surgical methods are shown in Figure 2C. The global inconsistency test was not significant (p=0.6894), and the comparison of hospital days estimated by the NMA for the different surgical methods is shown in Table S1(Supplementary). No significant difference (p>0.05) was observed between the direct and indirect evaluations of the node-splitting models of local consistency for hospital days. The surgical procedures with the shortest hospital days were UABA (72.8%), ACA (66%), and COT (52.5%), according to the SUCRA score.
Twenty studies, involving a total of 3281 patients and the comparison of six surgical methods, recorded the volume of drainage. The network relationships between the different surgical methods are shown in Figure 2D. The global inconsistency test was not significant (p=0.2120). A comparison of the NMA estimation for different surgical methods is shown in Table S2 (Supplementary). There was no significant difference (p>0.05) between the direct and indirect evaluations of the node-splitting models of local consistency for volume of drainage. The surgical methods with the lowest volume of drainage were COT (92.1%), UABA (65.7%), and BABA (61.1%), according to the SUCRA score. Fourteen studies, involving a total of 2238 patients and the comparison of six surgical methods, recorded the duration of drainage. The network relationships between the different surgical methods are shown in Figure 2E. The global inconsistency test was not significant (p=0.8308). A comparison of the duration of drainage estimated by NMA for different surgical methods is shown in Table S3. There was no significant difference (p>0.05) between the direct and indirect evaluations of the node-splitting models of local consistency for duration of drainage. The shortest surgical procedures for the duration of drainage were COT (76.9%), UABA (68.2%), and OA (50.2%), according to the SUCRA score.
The number of retrieved LNs was reported in 33 studies, involving a total of 6569 patients and eight surgical methods. The network relationship between the number of retrieved LNs and the different surgical methods is shown in Figure 2F. The global inconsistency test was not significant (p=0.2835), and a comparison of the number of lymph node recoveries estimated by the NMA for different surgical methods is shown in Table S4(Supplementary). There was no significant difference (p>0.05) between the direct and indirect evaluations of the node-splitting models of local consistency for the number of retrieved LNs. The surgical methods with the highest number of retrieved LNs were ACA (81.4%), COT (72.7%), and OA (71.6%) according to the SUCRA grade. Seventeen studies discussed the number of metastatic LNs, involving a total of 3453 patients and comparing five surgical methods. The network relationship between the number of metastatic LNs and different surgical methods is shown in Figure 2G. The global inconsistency test was not significant (p=0.3129), and a comparison of the number of metastatic LNs estimated by NMA for different surgical methods is shown in Table S5 (Supplementary). There was no significant difference (p>0.05) between the direct and indirect evaluations of the node-splitting models of local consistency for the number of metastatic LNs. The surgical methods with the highest number of metastatic LNs were OA (63.3%), BABA (61.4%), and COT (54.9%), according to the SUCRA grade.
In our meta-analysis, we found that stimulated TG levels were not significantly different between BABA (MD=0.04 ng/ml,[-0.41,0.49], p =0.86), OA (MD=-0.46 ng/ml,[-1.39,0.48],p =0.34), and COT groups. However, it was significantly lower in the CBA group (MD=-0.40 ng/ml,[-0.72,-0.09];p =0.01) than in the COT group (Figure S1 in Supplementary). There was no significant difference in TG levels after RAI treatment between the CBA (MD=-0.13[-0.31,0.06],p =0.18)and COT groups (Figure S2 in Supplementary).
Five studies reported postoperative pain using the visual analog scale (VAS); detailed information is shown in the Figure S3 (Supplementary). Our meta-analysis showed that CBA was not significantly lower than COT in terms of postoperative pain (MD=-0.66[-1.39,0.07], p =0.08).
There have been reports of postoperative cosmetic satisfaction with the common measurement method, detailed information was shown in Figure S4 (Supplementary). Our meta-analysis showed that GUA was significantly better than COT in terms of cosmetic satisfaction (MD=-2.08[-3.35,-0.82], p =0.001).
We compared the incidence of bleeding, transient or permanent hypoparathyroidism, transient or permanent vocal cord palsy, transient or permanent hypocalcemia, chyle leak, infection, seroma, hematoma, and recurrence between the endoscopic and COT groups. Our results suggested no significant difference in the incidence of surgical complications between the two groups (Table 3).
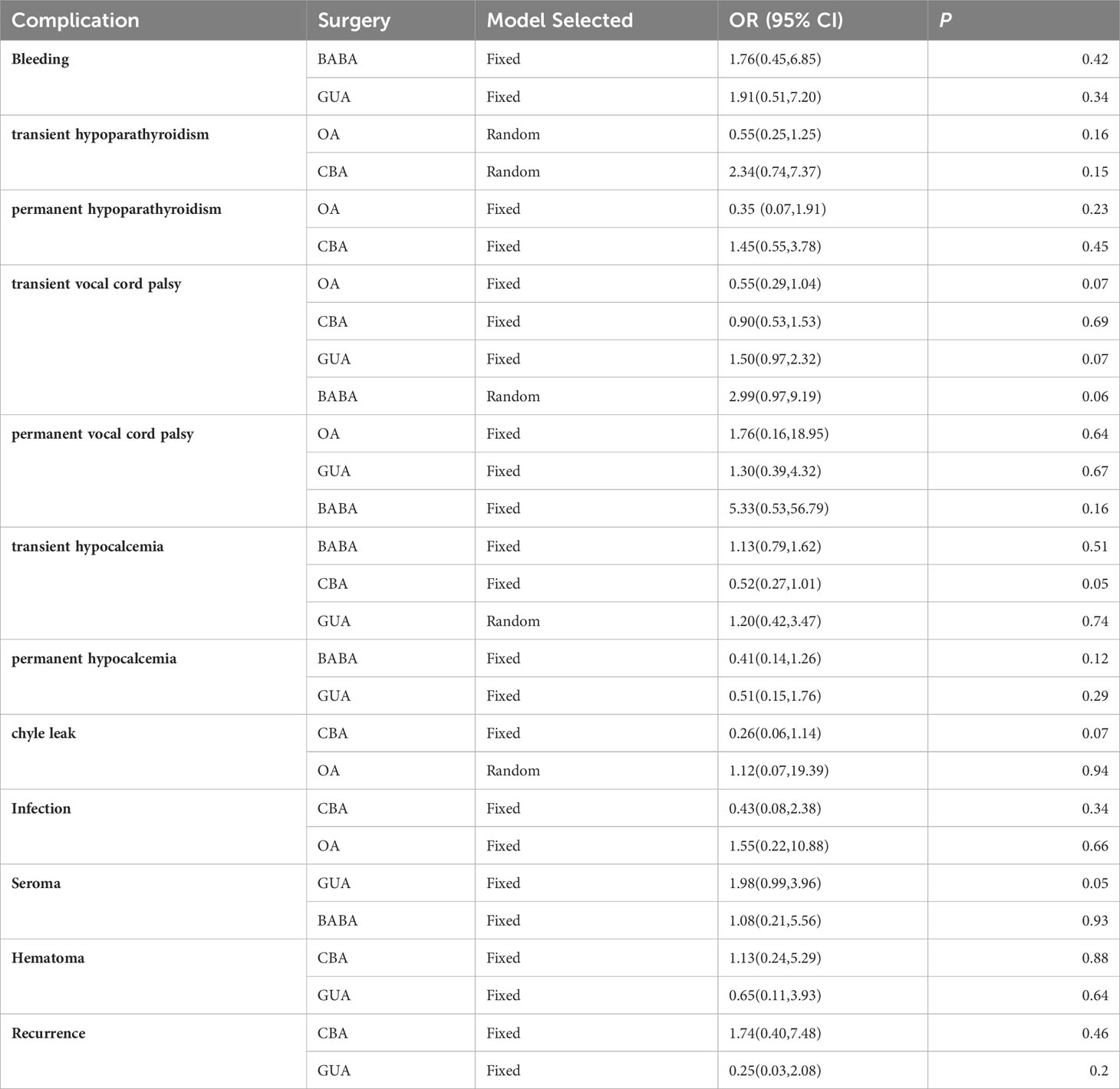
Table 3 Comparison of endoscopic thyroidectomy and COT for surgical complications.
Our NMA ranked various surgical methods for operative time, intraoperative bleeding volume, hospital days, volume of drainage, duration of drainage, retrieved LNs and metastatic LNs (Figure 3).
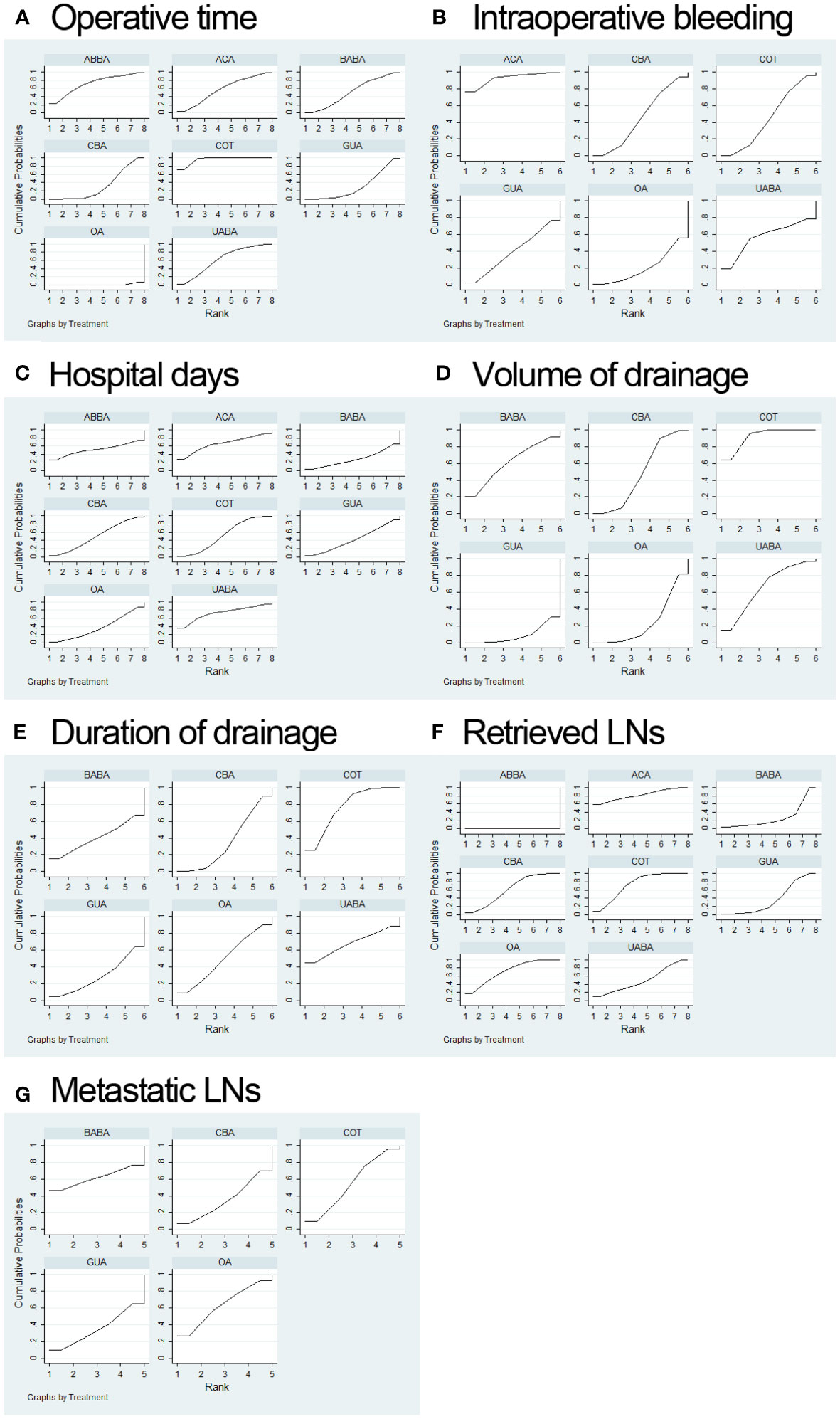
Figure 3 Surgery ranking curves for operative time (A); intraoperative bleeding volume (B); hospital days (C); volume of drainage (D); duration of drainage (E); retrieved LNs (F); metastatic LNs (G).
The comparison-adjusted funnel plots of this meta-analysis clearly showed that the included studies were symmetrical, indicating a relatively low publication bias in terms of operative time, intraoperative bleeding volume, hospital days, volume of drainage, duration of drainage, retrieved LNs, metastatic LNs. Detailed information is provided in the Figure S5 (Supplementary).
This meta-analysis found that endoscopic surgery not only has a lower incidence of complications than COT but may even be superior to COT in terms of operative bleeding volume, hospital days, and retrieved LNs. Previous meta-analyses have explored the efficacy of endoscopic thyroidectomy for thyroid neoplasms, but only compared different endoscopic surgeries or conventional surgeries (51, 52). Our study adopted an NMA approach to comprehensively and meticulously discuss the advantages of seven surgical approaches. Among the various surgical approaches, ABBA stands out for its notably shorter operative time and proximity to COT. ACA excels in effectively controlling intraoperative bleeding. UABA demonstrates superior outcomes in terms of hospital stay and drainage, while OA prove to be more conducive to straightforward lymph node acquisition. The patients included in the study were all patients with thyroid cancer, and studies only focused on different endoscopic surgeries, which greatly reduced research heterogeneity and made our results more reliable.
COT required the least operative time, which is consistent with previous research results (15, 16, 22). This may be because of the need for additional surgical channels and workspaces for endoscopic surgery. For endoscopic surgery, the ABBA and UABA require shorter operative times. It needs to be emphasized that OA serves as the “shortest surgical pathway” for endoscopic surgery, but the results show that it has the longest operative time. The main reason for this phenomenon may be: 1) To improve safety and feasibility, OA usually involves three oral vestibular incisions (53), and during the surgical process, the three trocars often encounter unavoidable collisions in the limited workspace, subsequently increasing the difficulty of the surgery; 2) OA is a top-down operation. Owing to the presence of the thyroid cartilage, treatment of the superior thyroid requires more time than other methods. Many of the operation time data included in this study did not specify whether it was a total thyroidectomy or lobectomy, and roughly categorizing them into the same category would, to some extent, have affected our conclusion. ACA and UABA show obvious advantages in terms of intraoperative bleeding volume and hospital stay, while OA and GUA often have poor control of intraoperative bleeding volume due to the need for more extensive free platysma muscle to create surgical space. In the transaxillary approach, the UABA is relatively better than the GUA in bleeding control; however, because it does not require CO2 insufflation, it avoids the occurrence of mediastinal emphysema, subcutaneous emphysema, and other related gas complications.
Thyroid cancer has a high rate of central lymph node metastasis (54), which is associated with high patient mortality (55). This study reveals that ACA outperforms COT in terms of retrieving LNs; however, it’s important to note that the limited inclusion of only two articles involving ACA may introduce potential bias into the interpretation of this result. OA exhibits superior results in the retrieval of both total LNs and metastatic LNs compared to other endoscopic procedures. This can be attributed to the fact that, from top to bottom, the field of view in OA can seamlessly encompass the central region, thereby circumventing sternum and clavicle limitations, which uniquely facilitates the removal of central LNs.
TG is an important indicator for the postoperative follow-up of thyroid cancer, and lower stimulated TG levels are considered to be associated with total thyroidectomy and low recurrence rate (56). We found no difference between the endoscopic surgery and COT groups for TG, with CBA being significantly lower than COT. Regarding postoperative pain, CBA was not significantly better than COT. The reasons for this may be as follows: (1) fewer articles were included and (2) inconsistent measurement time points after surgery. We found that many studies used different methods to measure postoperative pain, which made it difficult to merge the results of the studies. However, this meta-analysis included studies that used VAS scores. It is well known that endoscopic thyroid surgery avoids scarring on the neck, and our results fully demonstrate this advantage. However, we also encountered a difficulty, there is no common scoring criterion for objective evaluation, and it is necessary for us to find a more objective standard in future research. The incidence of postoperative complications was not lower in the endoscopic surgery group than that in the COT group. Each surgical approach has its own drawbacks; for example, OA is prone to incision infection (8), CBA causes subcutaneous effusion (57), and GUA causes brachial plexus nerve injury (58).
Our NMA had some limitations. First, most of the included articles were retrospective studies, and further large-scale randomized controlled trials are needed. Second, the articles we included were all from Asia, which may limit the generalisability of our results. Third, the scope of surgery included in the article was not specified, and there was a certain degree of heterogeneity.
Based on comprehensive NMA, endoscopic thyroidectomy is safe and feasible. Endoscopic surgical approaches have unique advantages. ABBA and UABA are the closest to COT in terms of operative time and are superior to other endoscopic surgeries. The UABA and ACA are superior to other surgical approaches in controlling intraoperative bleeding and hospital stay. UABA and BABA showed significant advantages in terms of postoperative drainage volume. The OA is more adept at retrieving lymph nodes. Endoscopic thyroidectomy did not increase the incidence of postoperative complications. However, it is clear that careful selection and consideration of the surgical approach are essential. In light of these findings, it is apparent that prospective, randomized studies are needed to validate and further refine the findings of our NMA, providing a more robust foundation for surgeons to make informed decisions when selecting appropriate endoscopic surgical approaches.
XL: Data curation, Writing – original draft. HZ: Writing – review & editing. WD: Data curation, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1256209/full#supplementary-material
1. Kitahara CM, Sosa JA. The changing incidence of thyroid cancer. Nat Rev Endocrinol (2016) 12(11):646–53. doi: 10.1038/nrendo.2016.110
2. Huscher CSG, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endoscopy-Ultrasound Interventional Techniques (1997) 11(8):877–7. doi: 10.1007/s004649900476
3. Kudpaje A, Subash A, Subramaniam N, Palme CE, Rao USV, Arakeri G. Remote access thyroid surgery: A review of literature. Indian J Surg Oncol (2022) 13(1):191–8. doi: 10.1007/s13193-021-01364-y
4. Sun HQ, Wang XJ, Zheng GB, Wu GC, Zeng QD, Zheng HT. Comparison between transoral endoscopic thyroidectomy vestibular approach (TOETVA) and conventional open thyroidectomy for patients undergoing total thyroidectomy and central neck dissection: A propensity score-matching analysis. Front Oncol (2022) 12. doi: 10.3389/fonc.2022.856021
5. Rouse B, Chaimani A, Li TJ. Network meta-analysis: an introduction for clinicians. Internal Emergency Med (2017) 12(1):103–11. doi: 10.1007/s11739-016-1583-7
6. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Internal Med (2015) 162(11):777–84. doi: 10.7326/M14-2385
7. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol (2010) 25(9):603–5. doi: 10.1007/s10654-010-9491-z
8. Ahn JH, Yi JW. Transoral endoscopic thyroidectomy for thyroid carcinoma: outcomes and surgical completeness in 150 single-surgeon cases. Surg Endoscopy Other Interventional Techniques (2020) 34(2):861–7. doi: 10.1007/s00464-019-06841-8
9. Bian C, Liu H, Yao XY, Wu SP, Wu Y, Liu C, et al. Complete endoscopic radical resection of thyroid cancer via an oral vestibule approach. Oncol Lett (2018) 16(5):5599–606. doi: 10.3892/ol.2018.9369
10. Cho MJ, Park KS, Cho MJ, Yoo YB, Yang JH. A comparative analysis of endoscopic thyroidectomy versus conventional thyroidectomy in clinically lymph node negative thyroid cancer. Ann Surg Treat Res (2015) 88(2):69–76. doi: 10.4174/astr.2015.88.2.69
11. Chung YS, Choe JH, Kang KH, Kim SW, Chung KW, Park KS, et al. Endoscopic thyroidectomy for thyroid Malignancies: Comparison with conventional open thyroidectomy. World J Surg (2007) 31(12):2302–8. doi: 10.1007/s00268-007-9117-0
12. Gao HY, Chen C, Liu XJ, Xu N, Wang YY, Qu R, et al. The transareola endoscopic approach yields adequate oncological dissection as open approach in the treatment of papillary thyroid carcinoma. Surg Laparoscopy Endoscopy Percutaneous Techniques (2019) 29(6):489–92. doi: 10.1097/SLE.0000000000000729
13. Gong Y, Zuo ZK, Liu Z, Ye F, Huang JS. Clinical experience and efficacy of endoscopic surgery for papillary thyroid microcarcinoma through total areola approach. Zhong nan da xue xue bao. Yi xue ban = J Cent South University. Med Sci (2019) 44(9):1009–15. doi: 10.11817/j.issn.1672-7347.2019.190430
14. Guo FD, Wang WR, Zhu XY, Xiang C, Wang P, Wang Y. Comparative study between endoscopic thyroid surgery via the oral vestibular approach and the areola approach. J Laparoendoscopic Advanced Surg Techniques (2020) 30(2):170–4. doi: 10.1089/lap.2019.0562
15. Guo YM, Qu R, Huo JL, Wang CC, Hu XC, Chen C, et al. Technique for endoscopic thyroidectomy with selective lateral neck dissection via a chest-breast approach. Surg Endoscopy Other Interventional Techniques (2019) 33(4):1334–41. doi: 10.1007/s00464-018-06608-7
16. Hong HJ, Kim WS, Koh YW, Lee SY, Shin YS, Koo YC, et al. Endoscopic Thyroidectomy via an Axillo-Breast Approach without Gas Insufflation for Benign Thyroid Nodules and Micropapillary Carcinomas: Preliminary Results. Yonsei Med J (2011) 52(4):643–54. doi: 10.3349/ymj.2011.52.4.643
17. Gupta N, Chand G, Mishra A, Sabaretnam M, Agarwal G, Agarwal A, et al. A comparative study of clinicopathological profile and surgical outcomes of endoscopic (Bilateral axillo-breast approach) versus conventional total thyroidectomy for thyroid tumors. Indian J Surg (2021) 83(1):194–200. doi: 10.1007/s12262-020-02267-y
18. Huang JK, Ma L, Song WH, Lu BY, Huang YB, Dong HM, et al. Quality of life and cosmetic result of single-port access endoscopic thyroidectomy via axillary approach in patients with papillary thyroid carcinoma. Oncotargets Ther (2016) 9:4053–9. doi: 10.2147/OTT.S99980
19. Im HJ, Koo DH, Paeng JC, Lee KE, Chung YS, Lim I, et al. Evaluation of surgical completeness in endoscopic thyroidectomy compared with open thyroidectomy with regard to remnant ablation. Clin Nucl Med (2012) 37(2):148–51. doi: 10.1097/RLU.0b013e3182335fdc
20. Jeong JJ, Kang SW, Yun JS, Sung TY, Lee SC, Lee YS, et al. Comparative study of endoscopic thyroidectomy versus conventional open thyroidectomy in papillary thyroid microcarcinoma (PTMC) patients. J Surg Oncol (2009) 100(6):477–80. doi: 10.1002/jso.21367
21. Kim EY, Lee KH, Park YL, Park CH, Lee CR, Jeong JJ, et al. Single-incision, gasless, endoscopic trans-axillary total thyroidectomy: A feasible and oncologic safe surgery in patients with papillary thyroid carcinoma. J Laparoendoscopic Advanced Surg Techniques (2017) 27(11):1158–64. doi: 10.1089/lap.2016.0669
22. Kim SK, Kang SY, Youn HJ, Jung SH. Comparison of conventional thyroidectomy and endoscopic thyroidectomy via axillo-bilateral breast approach in papillary thyroid carcinoma patients. Surg Endoscopy Other Interventional Techniques (2016) 30(8):3419–25. doi: 10.1007/s00464-015-4624-9
23. Koh YW, Park JH, Kim JW, Lee SW, Choi EC. Endoscopic hemithyroidectomy with prophylactic ipsilateral central neck dissection via an unilateral axillo-breast approach without gas insufflation for unilateral micropapillary thyroid carcinoma: preliminary report. Surg Endoscopy Other Interventional Techniques (2010) 24(1):188–97. doi: 10.1007/s00464-009-0646-5
24. Kim WW, Kim JS, Hur SM, Kim SH, Lee SK, Choi JH, et al. Is robotic surgery superior to endoscopic and open surgeries in thyroid cancer? World J Surg (2011) 35(4):779–84. doi: 10.1007/s00268-011-0960-7
25. Lee H, Lee J, Sung KY. Comparative study comparing endoscopic thyroidectomy using the axillary approach and open thyroidectomy for papillary thyroid microcarcinoma. World J Surg Oncol (2012) 10:269. doi: 10.1186/1477-7819-10-269
26. Li HQ, Yin DT, Ma RS, Wang YF, Liu Z, Chang QG, et al. Therapeutic evaluation of endoscopic and open thyroidectomy for papillary thyroid microcarcinoma. J Xi'an Jiaotong Univ (Medical Sciences) (2018) 39(1):5–8. doi: 10.7652/jdyxb201801002
27. Li TT, Zhang ZC, Chen WS, Yu ST, Sun BH, Deng XQ, et al. Comparison of quality of life and cosmetic result between open and transaxillary endoscopic thyroid lobectomy for papillary thyroid microcarcinoma survivors: A single-center prospective cohort study. Cancer Med (2022) 11(22):4146–56. doi: 10.1002/cam4.4766
28. Lin PL, Liang FY, Cai Q, Han P, Chen RH, Xiao ZW, et al. Comparative study of gasless endoscopic selective lateral neck dissection via the anterior chest approach versus conventional open surgery for papillary thyroid carcinoma. Surg Endoscopy Other Interventional Techniques (2021) 35(2):693–701. doi: 10.1007/s00464-020-07434-6
29. Liu ZD, Li YJ, Yu X, Xiang C, Wang P, Wang Y. A comparative study on the efficacy of transoral vestibular approach, via bilateral areola approach endoscopic and open thyroidectomy on stage T1b papillary thyroid carcinoma. Zhonghua er bi yan hou tou jing wai ke za zhi = Chin J otorhinolaryngology Head Neck Surg (2020) 55(10):905–12. doi: 10.3760/cma.j.cn115330-20200520-00430
30. Liu ZD, Li YJ, Wang Y, Xiang C, Yu X, Zhang ML, et al. Comparison of the transoral endoscopic thyroidectomy vestibular approach and open thyroidectomy: A propensity score-matched analysis of surgical outcomes and safety in the treatment of papillary thyroid carcinoma. Surgery (2021) 170(6):1680–6. doi: 10.1016/j.surg.2021.06.032
31. Mo KN, Zhao M, Wang KJ, Gu JL, Tan Z. Comparison of endoscopic thyroidectomy via a modified axillo-breast approach with the conventional breast approach for treatment of unilateral papillary thyroid microcarcinoma. Medicine (2018) 97(45):e13030. doi: 10.1097/MD.0000000000013030
32. Park KN, Jung CH, Mok JO, Kwak JJ, Lee SW. Prospective comparative study of endoscopic via unilateral axillobreast approach versus open conventional total thyroidectomy in patients with papillary thyroid carcinoma. Surg Endoscopy Other Interventional Techniques (2016) 30(9):3797–801. doi: 10.1007/s00464-015-4676-x
33. Qu R, Li JY, Yang JG, Sun P, Gong J, Wang CC. Treatment of differentiated thyroid cancer: can endoscopic thyroidectomy via a chest-breast approach achieve similar therapeutic effects as open surgery? Surg Endoscopy Other Interventional Techniques (2018) 32(12):4749–56. doi: 10.1007/s00464-018-6221-1
34. Qu YQ, Han YB, Wang WJ, Zhang XJ, Ma GH. Clinical analysis of total endoscopic thyroidectomy via breast areola approach in early differentiated thyroid cancer. J B.U.ON. (2021) 26(3):1022–7.
35. Ren XT, Dai ZZ, Sha HC, Wu JY, Hong XM, Xiu ZL. Comparative study of endoscopic thyroidectomy via a breast approach versus conventional open thyroidectomy in papillary thyroid microcarcinoma patients. Biomed Research-India (2017) 28(12):5315–20.
36. Si LY, Mei HJ, Wang QH, Wang FR, Sha SN, He ZX, et al. Surgical outcomes of different approaches to dissection of lymph nodes posterior to right recurrent laryngeal nerve: a retrospective comparative cohort study of endoscopic thyroidectomy via the areolar approach and via the axillo-breast approach. Gland Surg (2022) 11(12):1936–45. doi: 10.21037/gs-22-661
37. Sun HQ, Zheng HT, Wang XJ, Zeng QD, Wang P, Wang Y. Comparison of transoral endoscopic thyroidectomy vestibular approach, total endoscopic thyroidectomy via areola approach, and conventional open thyroidectomy: a retrospective analysis of safety, trauma, and feasibility of central neck dissection in the treatment of papillary thyroid carcinoma. Surg Endoscopy Other Interventional Techniques (2020) 34(1):268–74. doi: 10.1007/s00464-019-06762-6
38. Sun P, Zhan JL, Chong TH, Li JY, Wang CC. Endoscopic central lymph node dissection of thyroid cancer via chest-breast approach: results, indications, and strategies. Surg Endoscopy Other Interventional Techniques (2022) 36(6):4239–47. doi: 10.1007/s00464-021-08758-7
39. Tae K, Ji YB, Cho SH, Kim KR, Kim DW, Kim DS. Initial experience with a gasless unilateral axillo-breast or axillary approach endoscopic thyroidectomy for papillary thyroid microcarcinoma: comparison with conventional open thyroidectomy. Surg Laparoscopy Endoscopy Percutaneous Techniques (2011) 21(3):162–9. doi: 10.1097/SLE.0b013e318218d1a4
40. Tan Z, Gu JL, Han QB, Wang WD, Wang KJ, Ge MH, et al. Comparison of conventional open thyroidectomy and endoscopic thyroidectomy via breast approach for papillary thyroid carcinoma. Int J Endocrinol (2015) 2015:239610. doi: 10.1155/2015/239610
41. Wang D, Zhang R, Feng E, Yuan X, Wu X, Yang J. Effectiveness of transoral endoscopic thyroid surgery for lymph node dissection in the central region of thyroid cancer. Lin chuang er bi yan hou tou jing wai ke za zhi = J Clin otorhinolaryngology head Neck Surg (2022) 36(7):540–544;558. doi: 10.13201/j.issn.2096-7993.2022.07.012
42. Wang TT, Wu YP, Xie QP, Yan HC, Zhou XM, Yu X, et al. Safety of central compartment neck dissection for transoral endoscopic thyroid surgery in papillary thyroid carcinoma. Japanese J Clin Oncol (2020) 50(4):387–91. doi: 10.1093/jjco/hyz195
43. Xiang DP, Xie LQ, Li ZY, Wang P, Ye M, Zhu MZ. Endoscopic thyroidectomy along with bilateral central neck dissection (ETBC) increases the risk of transient hypoparathyroidism for patients with thyroid carcinoma. Endocrine (2016) 53(3):747–53. doi: 10.1007/s12020-016-0884-y
44. Yang Y, Sun DL, Yang JS, Chen J, Duan YF. Endoscopic thyroidectomy in anterior chest approach versus open thyroidectomy for patients with papillary thyroid carcinomas, a retrospective study. J Laparoendoscopic Advanced Surg Techniques (2020) 30(5):488–94. doi: 10.1089/lap.2019.0694
45. Yuan YQ, Sun CY, Yin TJ, Shao C, Pan B, Lu DW, et al. Comparison of endoscopic thyroidectomy by complete areola approach and conventional open surgery in the treatment of differentiated thyroid carcinoma: A retrospective study and meta-analysis. Front Surg (2022) 9. doi: 10.3389/fsurg.2022.1000011
46. Zhang DQ, Wang T, Dionigi G, Zhang J, Xue GF, Sun H. Central lymph node dissection by endoscopic bilateral areola versus open thyroidectomy. Surg Laparoscopy Endoscopy Percutaneous Techniques (2019) 29(1):E1–6. doi: 10.1097/SLE.0000000000000579
47. Zhang WD, Dai L, Wang YC, Xie YY, Guo JY, Li JJ, et al. Transoral endoscopic thyroidectomy vestibular approach versus endoscopic thyroidectomy via areola approach for patients with unilateral papillary thyroid carcinoma: A retrospective study. Surg Laparoscopy Endoscopy Percutaneous Techniques (2021) 31(5):550–3. doi: 10.1097/SLE.0000000000000932
48. Zhang X, Hu XJ, Hua KJ. Endoscopic hemithyroidectomy plus prophylactic central neck dissection via breast approach versus gasless transaxillary approach in treating low-risk papillary thyroid cancer: a retrospective series. Updates Surg (2023) 75(3):707–15. doi: 10.1007/s13304-023-01486-8
49. Zhang WD, Dai L, Wang YC, Xie YY, Guo JY, Li JJ, et al. Preliminary evaluation of effect of endoscopic thyroidectomy using the gasless unilateral axillary approach. Chin J Clin Oncol (2018) 45(1):27–32. doi: 10.3969/j.issn.1000-8179.2018.01.801
50. Zhao QZ, Wang Y, Wang P. A comparative study of endoscopic and traditional open surgery in the treatment of papillary thyroid carcinoma. Zhonghua wai ke za zhi [Chinese J surgery] (2018) 56(2):135–8. doi: 10.3760/cma.j.issn.0529-5815.2018.02.011
51. Jiang WJ, Yan PJ, Zhao CL, Si MB, Tian W, Zhang YJ, et al. Comparison of total endoscopic thyroidectomy with conventional open thyroidectomy for treatment of papillary thyroid cancer: a systematic review and meta-analysis. Surg Endoscopy Other Interventional Techniques (2020) 34(5):1891–903. doi: 10.1007/s00464-019-07283-y
52. Zheng GB, Xu JJ, Wu GC, Ma C, Sun HQ, Ge MH, et al. Transoral versus gasless transaxillary endoscopic thyroidectomy: a comparative study. Updates Surg (2022) 74(1):295–302. doi: 10.1007/s13304-021-01062-y
53. Fu YL, Wu MW, Fu JB, Lin SQ, Song ZF, Chen JY, et al. TransOral endoscopic thyroidectomy via submental and vestibular approach: A preliminary report. Front Surg (2020) 7. doi: 10.3389/fsurg.2020.591522
54. Mehanna H, Al-Maqbili T, Carter B, Martin E, Campain N, Watkinson J, et al. Differences in the recurrence and mortality outcomes rates of incidental and nonincidental papillary thyroid microcarcinoma: A systematic review and meta-analysis of 21 329 person-years of follow-up. J Clin Endocrinol Metab (2014) 99(8):2834–43. doi: 10.1210/jc.2013-2118
55. Lundgren CI, Hall P, Dickman PW, Zedenius J. Clinically significant prognostic factors for differentiated thyroid carcinoma - A population-based, nested case-control study. Cancer (2006) 106(3):524–31. doi: 10.1002/cncr.21653
56. Lin YS, Li TJ, Liang J, Li XY, Qiu LH, Wang SS, et al. Predictive value of preablation stimulated thyroglobulin and thyroglobulin/thyroid-stimulating hormone ratio in differentiated thyroid cancer. Clin Nucl Med (2011) 36(12):1102–5. doi: 10.1097/RLU.0b013e3182291c65
57. Qu YQ, Han YB, Wang WJ, Zhang XJ, Ma GH. Clinical analysis of total endoscopic thyroidectomy via breast areola approach in early differentiated thyroid cancer. J Buon (2021) 26(3):1022–7.
Keywords: network meta-analysis, endoscopic thyroidectomy, conventional open thyroidectomy, thyroid cancer, surgical approaches
Citation: Li X, Ding W and Zhang H (2023) Surgical outcomes of endoscopic thyroidectomy approaches for thyroid cancer: a systematic review and network meta-analysis. Front. Endocrinol. 14:1256209. doi: 10.3389/fendo.2023.1256209
Received: 10 July 2023; Accepted: 01 November 2023;
Published: 04 December 2023.
Edited by:
Takahisa Hiramitsu, Japanese Red Cross Nagoya Daini Hospital, JapanReviewed by:
Mehmet Haciyanli, Izmir Katip Celebi University, TürkiyeCopyright © 2023 Li, Ding and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Zhang, emhhbmdoOTlAamx1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.