
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 13 September 2023
Sec. Bone Research
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1252966
 Marine Forien1*
Marine Forien1* Romain Coralli1Constance Verdonk2Sébastien Ottaviani1Esther Ebstein1Lucie Demaria1Elisabeth Palazzo1Richard Dorent2Philippe Dieudé1
Romain Coralli1Constance Verdonk2Sébastien Ottaviani1Esther Ebstein1Lucie Demaria1Elisabeth Palazzo1Richard Dorent2Philippe Dieudé1Introduction: Significant bone loss occurs after heart transplantation, predominantly in the first year, with increased risk of incident fractures. The goal of this study was to evaluate the prevalence of fragility fractures in a population of heart transplantation patients and to identify the independent risk factors for fractures.
Methods: This was a prospective monocentric study that included patients with heart transplantation occurring < 10 years who were undergoing heart transplantation monitoring. All patients underwent bone mineral density evaluation by dual-energy X-ray absorptiometry and radiographies to establish the presence of vertebral fractures.
Results: We included 79 patients (61 men); the mean age was 56.8 ± 10.8 years. The mean time between transplantation and inclusion was 32.3 ± 35.0 months. Incident fractures were diagnosed in 21 (27%) patients after heart transplantation. Vertebral fractures were the most frequent (30 vertebral fractures for 15 patients). Osteoporosis was confirmed in 22 (28%) patients. Mean bone mineral density at the femoral neck and total hip was lower with than without fracture (femoral neck: 0.777 ± 0.125 vs 0.892 ± 0.174 g/cm2, p<0.01; total hip: 0.892 ± 0.165 vs 0.748 ± 0.07 g/cm2, p<0.001), with a significant result on multivariate analysis. The mean time from transplantation to the first fracture was 8.0 ± 7.6 months.
Discussion: Our study confirmed a high vertebral fracture risk in heart transplant patients, especially during the first year after transplantation.
Heart transplantation is an established therapy for end-stage heart failure, and the number of transplantations has increased during the past decades (1). Medical advances have improved the survival of these patients, but new challenges arise, such as osteoporosis and increased risk of fragility fractures.
Bone disease causes morbidity and mortality pre- and post-heart transplantation. The prevalence of osteoporosis at the time of heart transplantation ranges from 7% to 23% (2–4), with significant bone loss after transplantation (3–5). The significant bone loss after heart transplantation is predominant in the first year, with a prevalence ranging from 3% to 10% at the spine and 6% to 11% at the femoral neck (3–5) and 20% increased risk of fracture in the first year (3, 6).
Several factors could be linked to osteoporosis in patients with heart transplantation: prolonged immobilization, impaired renal function, lack of exposure to sunlight (vitamin D deficiency), the etiology of the heart disease (excessive alcohol consumption), cardiac insufficiency-related treatments, and immunosuppressive drugs, notably glucocorticoids. However, the prevalence of fragility fractures in patients with heart transplantation and the independent risk factors associated with incident fractures remain unclear (6–8).
Mortality is increased after a fragility fracture. A large study showed increased mortality risk for 5 to 10 years after a low trauma fracture. The age-adjusted standardized mortality during the first 5 years after fracture was estimated at 2.5 to 3.5 for hip fractures and 1.7 to 2.3 for vertebral fractures (9). To our knowledge, no study has evaluated mortality after fracture in heart transplant patients, but the results in a general population suggest a similar result in this specific population. Consequently, improving risk stratification for incident fractures could be of great value in that therapeutic intervention could help reduce the decline of bone loss (10, 11).
Therefore, the goal of this study was to evaluate the prevalence of incident fragility fractures after heart transplantation and identify independent risk factors.
This was a cross-sectional monocentric study that included patients with heart transplantation < 10 years previous who were undergoing heart transplantation monitoring from January 2017 to December 2019. Exclusion criteria were age < 18 years, multiorgan transplantation and dialysis. All patients were evaluated by a senior rheumatologist. The following data were systematically collected: 1) demographic characteristics including sex, age, smoking status, excessive alcohol consumption (>20 g/day for women and >30 g/day for men), and diabetes; 2) the etiology of heart disease and treatment received after the transplant; 3) previous history of fractures and previous treatments for osteoporosis (calcium, vitamin D and osteoporotic therapies). Dietary calcium intake was evaluated with a specific questionnaire (12).
BMD was measured by dual-energy X-ray absorptiometry (Hologic Inc., Waltham, MA) at the lumbar spine (second to fourth vertebrae and vertebral fractures were excluded for BMD evaluation) and the upper part of the left femur (total femur and femoral neck). The results were given as BMD (g/cm2) and T-scores (standard deviation). Sex-specific T-scores were based on female and male reference curves. The device was controlled by measuring a spine phantom at least three times per week throughout the study. All examinations were performed according to the manufacturer’s recommendations. Osteoporosis was defined for patients ≥50 and <50 years as a T-score ≤-2.5 SD and Z-score ≤-2 SD at the lumbar spine (L1-L4), femoral neck or total femur. Osteopenia was defined for patients ≥50 and <50 years old as a T-score ≤-1 SD and Z-score ≤-1 SD at the lumbar spine (L1-L4), femoral neck or total femur (13).
Data on previous fractures (location, date) were collected. All patients underwent radiography with anteroposterior and lateral views of the dorsal and lumbar spine to establish the presence of vertebral fractures. Vertebral fracture diagnosis was confirmed in the presence of a reduction > 20% of the height of the vertebra (14). An experienced rheumatologist analyzed the radiographs.
At inclusion, all patients were assessed for calcium, phosphorus, creatinine, parathyroid hormone, 25 hydroxy-vitamin D, ß C-terminal propeptides of type I procollagen (ßCTX), osteocalcin (N-Mid osteocalcin) and bone-specific alkaline phosphatase levels (B-ALP). Serum for biochemical analysis was obtained in the morning under fasting conditions in the same laboratory. Serum calcium (normally 2.20-2.55 mmol/l), phosphorus (normally 0.81-1.5 mmol/l) and creatinine (normally <84 μmol/l) were measured by standard automated techniques (Cobas Pro, Roche). Intact parathormone 1-84 (normally 15-65 ng/l) was measured by electrochemiluminescence immunoassay (Cobas Pro, Roche), 25 hydroxy-vitamin D (normally 75-200 nmol/l), ßCTX (normally <0.635 μg/l), osteocalcin (normally 10.4-45.6 μg/l) and B-ALP (normally 4.7-27.0 μg/l) were measured by immunoassay (IDS-iSYS). Vitamin D deficiency was defined as serum level of 25 hydroxy-vitamin D < 50 nmol/l, insufficiency 50 to 75 nmol/l (15).
The Institutional Review Board (No. 12-011) of Paris North Hospitals approved this study. Written informed consent was obtained from all participants in agreement with French bioethics laws.
All data are expressed as mean ± SD and were compared by Mann Whitney test. Categorical data are described with number (%; percentages were calculated excluding missing data) and were compared by chi-square test or Fisher exact test, as appropriate. Univariate analysis (p<0.15) was performed to select potential explanatory variables that were then tested in the multivariable model (stepwise method). Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated. P < 0.05 was considered statistically significant.
From January 2017 to December 2019, 161 patients who underwent heart transplantation were screened for inclusion; 15 were excluded (age < 18 years, n=1; multiorgan transplantation, n=1; dialysis, n=13), 39 patients died and 28 were lost to follow-up (Figure 1). The baseline characteristics of the 79 patients are summarized in Table 1. Briefly, 61 were male (77.2%), the mean age was 54.1 ± 10.8 years, the mean body mass index (BMI) was 27.2 ± 4.99 kg/m², 49 (62%) were ever-smokers and 7 (8.9%) were current smokers. Twelve (15.2%) had excessive alcohol consumption and 29 (37%) had diabetes mellitus. Among 18 women, 15 had been menopausal for 5.3 years. The heart disease leading to transplantation was dilated cardiomyopathy for 34 (43%) patients, ischemic for 31 (39.2%), valvular cardiopathy for 6 (7.6%) and idiopathic or other cardiopathies for 8 (10.1%). The mean time from heart transplantation to inclusion was 32.3 ± 35.0 months. All patients except 2 received corticosteroids, with a mean dose of 10 ± 4.21 mg per day of prednisone. All patients received vitamin D supplementation. A total of 59 (75%) patients received ciclosporin, 67 (86%) mycophenolate mofetil, 14 (18%) tacrolimus and 24 (31%) everlimus. Two patients received osteoporotic treatment: alendronate, n=1, and zoledronic acid, n=1.
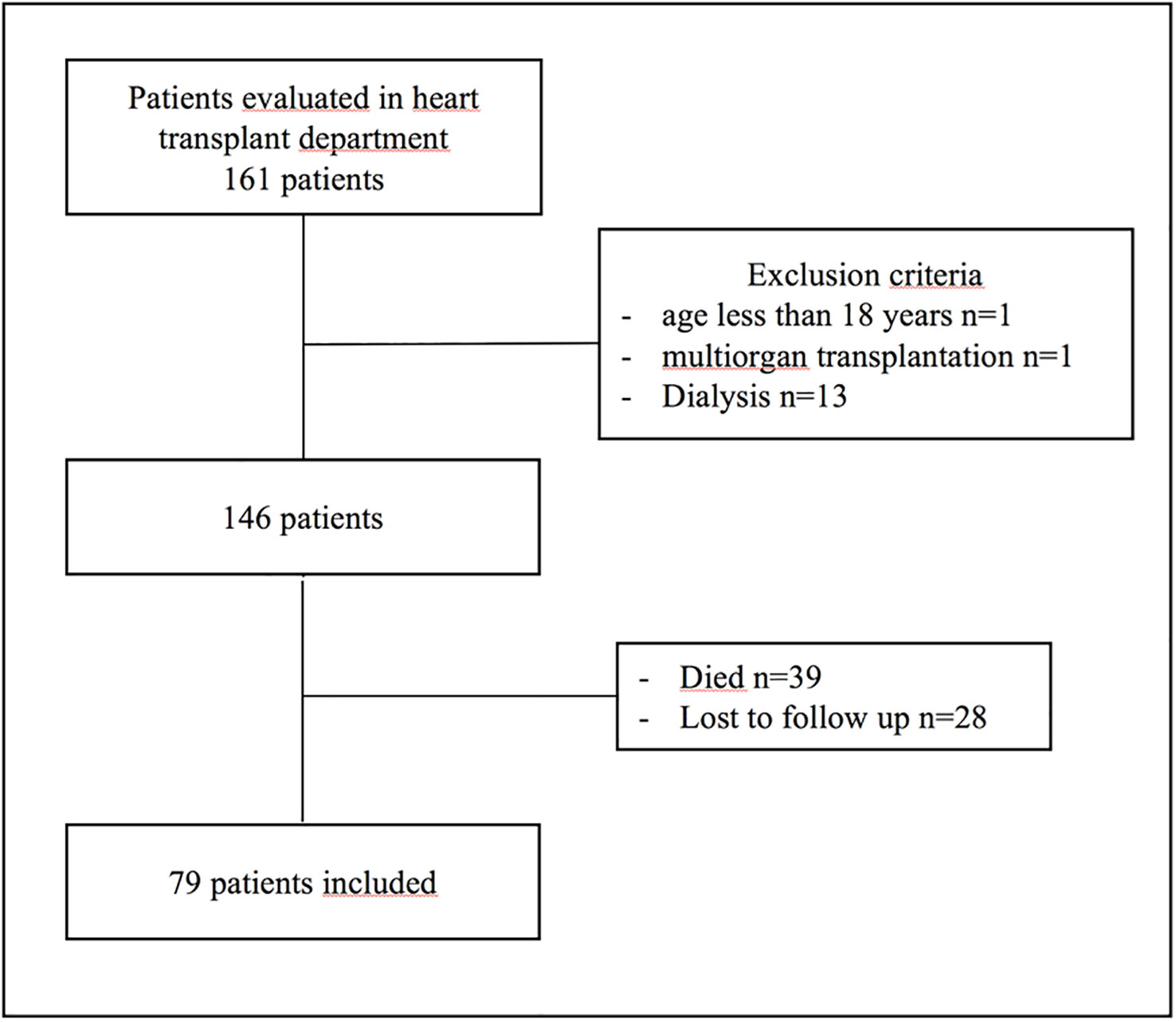
Figure 1 Flowchart of patients in the study.

Table 1 Main characteristics of the overall study population and patients with and without fracture after heart transplantation.
Osteopenia and osteoporosis were diagnosed in 38 (48%) and 22 (28%) patients, respectively. Diabetes mellitus was less prevalent in patients with than without osteoporosis: 4 (18%) versus 24 (44%), p=0.036 (Table 2). Pre-transplant osteoporotic fractures were noted for 2 patients (2 femoral neck fractures). At the time of the visit, 21 (27%) patients had fractures diagnosed after transplantation. Vertebral fractures were the most frequent (15, 71.4%). In total, 15 patients had 30 vertebral fractures (11 thoracic and 19 lumbar vertebral) (Figure 2). For 7 patients, vertebral fractures were unknown and were diagnosed on systematic X-rays. The other sites of fractures were femoral neck (n=2), pelvic (n=1), humeral (n=1), fibula (n=1), ad clavicular (n=1). Mean ages of patients with and without fracture after transplantation were 57.6±9.84 and 52.9±10.9 years, respectively (p=0.04). Estimated glomerular filtration rate (eGFR) was lower with than without fracture (44.8 ± 14.8 vs 53.3 ± 18.6, p=0.011), but osteoporosis was more frequent (9 [43%] vs 13 [22%], p=0.073) (Table 3). The prevalence of osteopenia did not significantly differ between the 2 groups. Mean BMD at the femoral neck and total hip was lower with than without fracture (femoral neck: 0.777 ± 0.125 vs 0.892 ± 0.174 g/cm², p<0.01; total hip: 0.892 ± 0.165 vs 0.748 ± 0.07 g/cm², p<0.001). The mean femoral neck and total hip T-scores were lower in patients with than without fractures: -1.79 ± 0.987 vs -0.955 ± 1.33 SD (p=0.01) and -2.07 ± 0.556 vs -0.976 ± 1.26 SD (p<0.001), but the difference was not significant for spine BMD. We performed a logistic regression analysis including age at transplantation eGFR and confirmed lower femoral neck BMD and total hip BMD for patients with fracture (OR 0.939 [95% CI 0.891–0.980], p<0.01, and OR 0.924 [95% CI 0.873–0.967], p<0.01, respectively). Age at transplantation and eGFR were not associated with fractures on multivariate analysis. The mean time from transplantation to the first fracture was 8.0 ± 7.6 months. Only two patients with fracture were < 50 years old at the time of transplantation (39 and 44 years) and 9 (43%) had a T-score <-2.5 SD at at least one site.
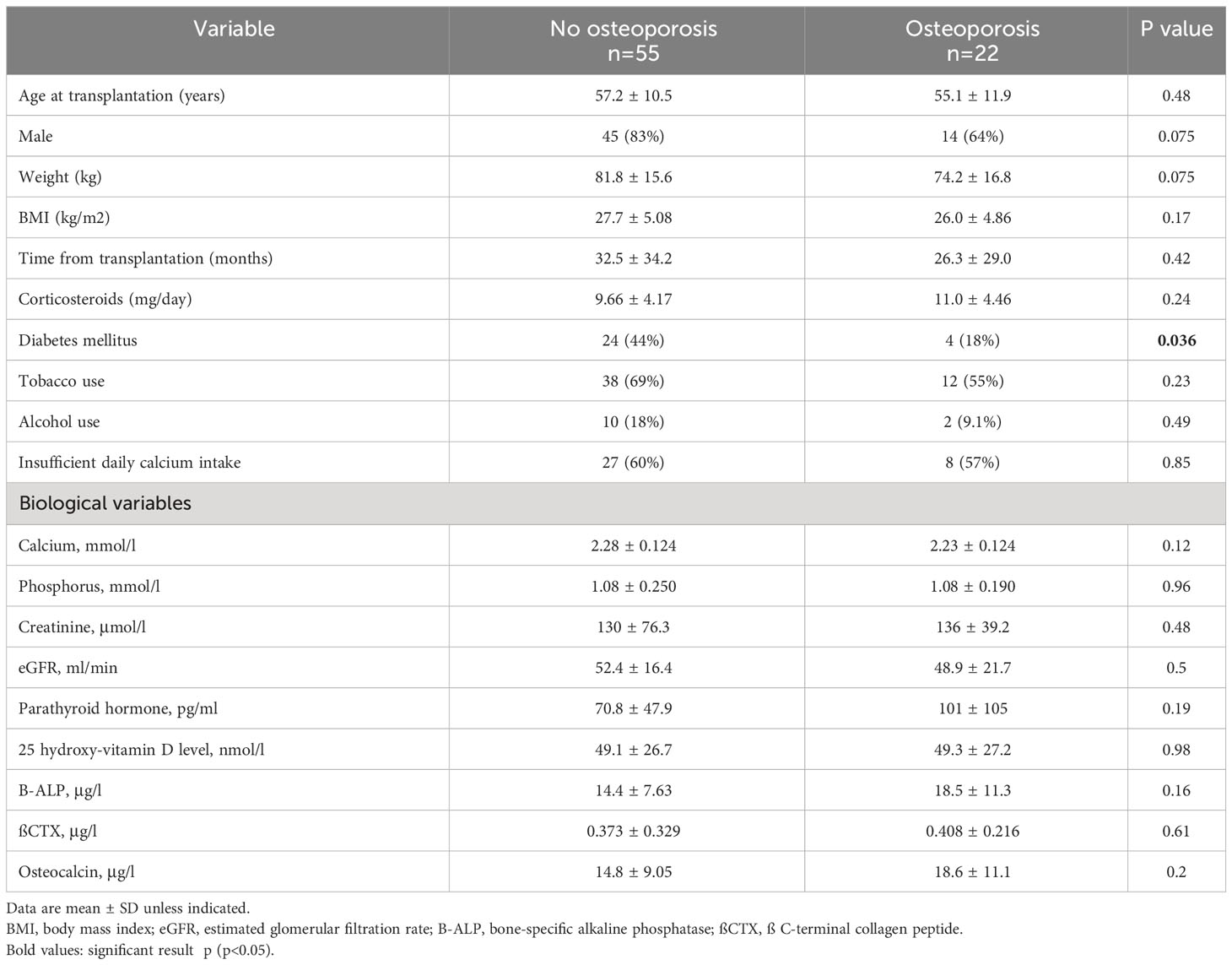
Table 2 Main characteristics of patients with and without osteoporosos after heart transplantation.
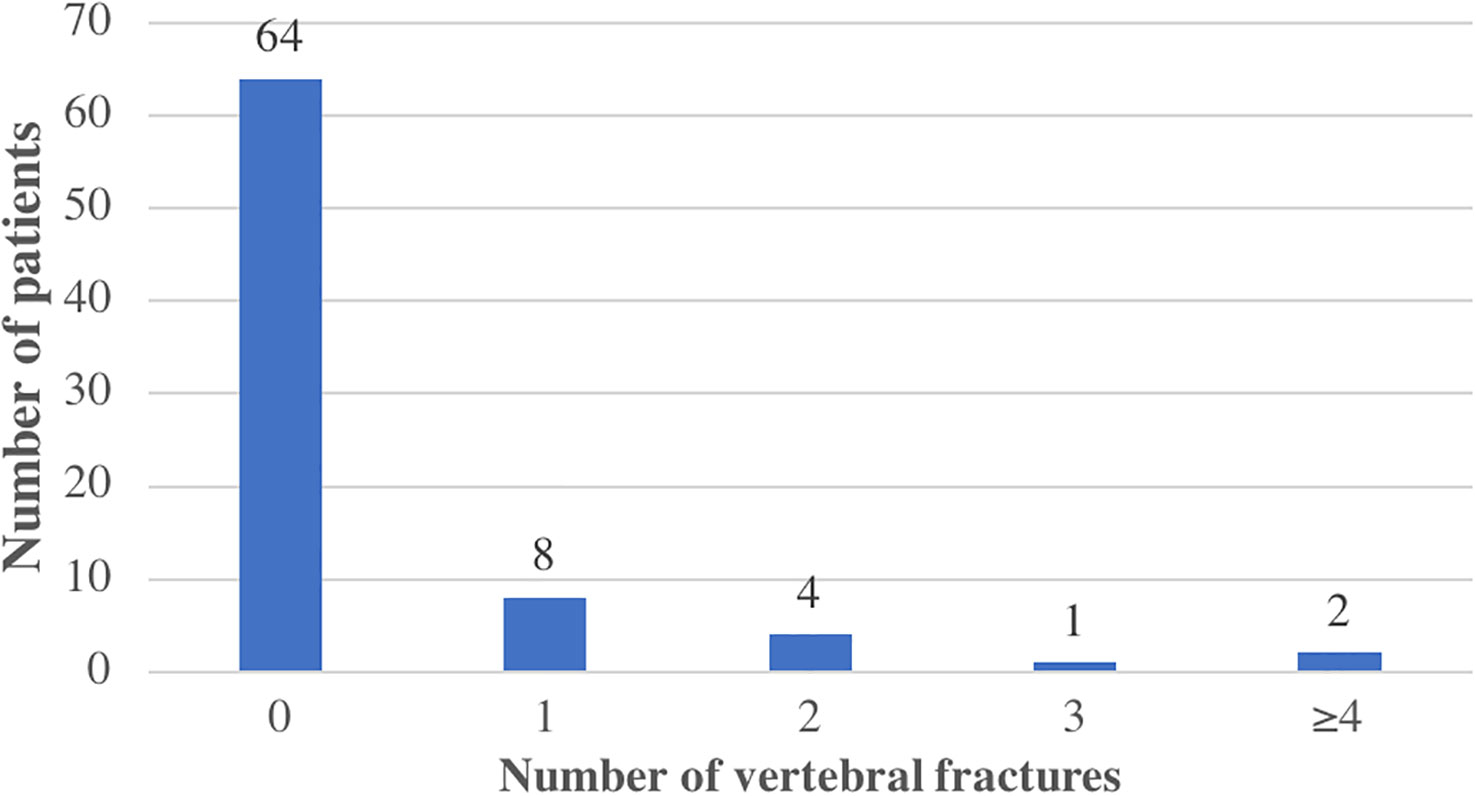
Figure 2 Vertebral fractures in the study population.
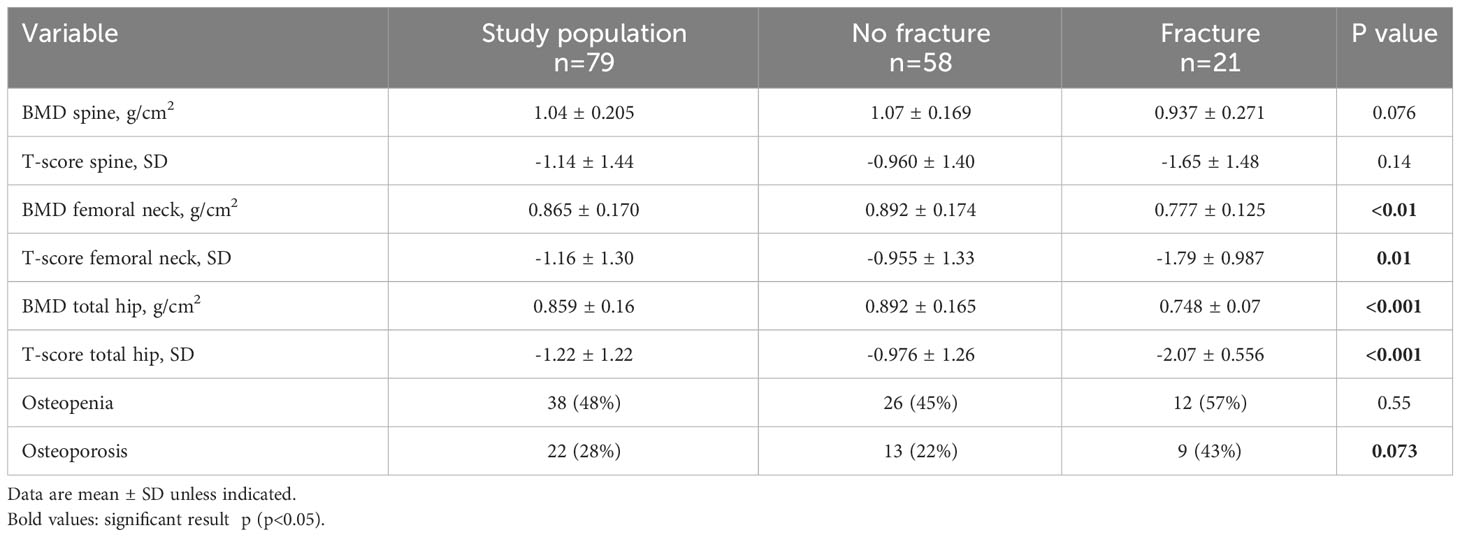
Table 3 Bone mineral density (BMD), T-score and prevalence of osteoporosis and osteopenia in the overall study population and in patients with and without fraction after heart transplantation.
Biochemical variables are described in Table 1. At the time of the visit, 58 (77%) patients had vitamin D deficiency and 44% (n=34) had increased level of parathyroid hormone. Patients with and without fracture and with and without osteoporosis did not differ in 25 hydroxy-vitamin D level, percentage of vitamin D deficiency, or secondary hyperparathyroidism (p>0.05). Bone turnover was assessed with ßCTX, osteocalcin and B-ALP levels. Bone turnover did not differ between patients with and without fracture or those with and without osteoporosis. Only 9.7% of patients had an increased ßCTX level.
All patients received 2 or 3 immunosuppressant therapies. Overall, 90% (n=71) received calcineurin inhibitors and 86% (n=77) mycophenolate mofetil. Patients with and without fracture and with and without osteoporosis did not differ in immunosuppressant therapies. Dietary daily calcium intake was lower than recommended levels in 58% (n=35) of patients, with no difference between groups (with and without fracture or with and without osteoporosis).
After global bone fragility evaluation, calcium and/or vitamin D therapy was initiated in 58 (73.4%) patients. Specific osteoporosis treatment was started for 56 (70.9%): zoledronic acid (n=42), denosumab (n=8), alendronate (n=4), and teriparatide (n=2).
In this study, the prevalence of fractures was 27% in patients with heart transplantation since 2.6 years. We found a significant association between fractures and femoral neck and total hip BMD.
The prevalence of fractures in this work is similar to that observed in other studies. Leidig-Bruckner et al. found 21% of 105 patients with at least one vertebral fracture in the first year after heart transplantation and 27% at 2 years after (6). Another study reported 40% of fractures in 180 patients with heart transplantation less than 10 years’ previous (8). In our population, the mean time from transplantation to the first fracture was 8 months; this result confirmed a high risk during the first year after the transplantation. Previous studies showed a decrease in BMD during the first year post-transplantation (3–6). This observation could be explained by a high dose of corticosteroids to avoid acute graft rejection. Glucocorticoids reduce bone formation (16), induce apoptosis of osteoblasts and osteocytes (17), increase bone resorption and reduce intestinal calcium absorption (18). We did not find an association between prednisone dose and risk of fractures probably because of lack of data of cumulative corticosteroids dose. In our study, only 28% of patients were osteoporotic, and for patients with fracture, 43% had a T-score <-2.5 SD at at least one site. We found no association between spine BMD and risk of fracture, even though vertebral fractures were the most frequent in our population. BMD is an important factor for evaluating the risk of fracture but is insufficient to identify all patients at risk. Osteocyte apoptosis decreases bone quality, which results in early increased risk of fracture even before BMD decreases. The indirect effects of glucocorticoids could also be involved in the risk of fracture: reduced muscle mass leading to increased risk of falls (19).
We confirmed vitamin D deficiency in 57% of our patients, and 44% had secondary hyperparathyroidism. The vitamin D deficiency in heart transplant patients could be explained by heart disease, lack of exposure to sunlight and hepatic dysfunction. In candidates for heart transplantation, 17% had 25 hydroxy-vitamin D level < 9 ng/ml, with a significant association with bone turnover markers (20). The implication of vitamin D in bone metabolism and the high prevalence of severe deficiency in this population confirm that all transplantation patients and candidates should receive adequate supplementation. The objective is to maintain 25 hydroxy-vitamin D level > 75 nmol/l (30 ng/ml) (21).
We did not find a significant association between immunosuppressive therapies and fracture or osteoporotic state. The role of calcineurin inhibitors is controversial, with opposite results on bone turnover in rats treated with calcineurin inhibitors (22, 23). Carbonare et al. showed an association between femoral-neck T-score and daily cyclosporine dosage and suggested the protective effect of calcineurin inhibitors. In our work, the daily dosage of calcineurin inhibitors is unknown, and 90% of patients received calcineurin inhibitors, which could explain the lack of a significant difference (8).
Vertebral fractures are the most frequent localization of fractures in heart transplant patients. In our study, 15 patients had vertebral fractures, and for half of them the fractures were unknown and diagnosed on systematic radiography. This result remains that vertebral fracture could be asymptomatic. The International Society of Heart and Lung Transplantation proposed spine radiography for all adult heart transplant candidates (21). In case of acute dorsal or lumbar pain even without trauma in heart transplant patients or candidates, spine radiography (or CT if necessary) must be performed.
Our study has some limitations: the study was monocentric with a relative small number of patients. BMD was not assessed before heart transplantation, so the longitudinal evaluation of BMD after transplantation could not be evaluated. Data on cumulative glucocorticoids or calcineurin inhibitors use were not available. Nevertheless, the strength of our study was the systematic evaluation of BMD and radiography for all patients in a real-life study.
In summary, our study confirmed high vertebral fracture risk in heart transplant patients, especially during the first year after transplantation. The prevalence of vitamin D insufficiency and deficiency was high in this population. This study confirmed that more attention to bone fragility is necessary to reduce the fracture risk.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by The Institutional Review Board (No. 12-011) of Paris North Hospitals. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
The authors confirm contribution to the paper as follows: study conception and design: MF, PhD. Data collection: MF, RC, CV, SO, EE, LD, EP, RD. Analysis and interpretation of results: MF, CV, RD, PhD. Draft manuscript preparation: MF, PhD. All authors contributed to the article and approved the submitted version.
We thank Laura Smales (BioMedEditing) for copyediting.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lund LH, Edwards LB, Dipchand AI, Goldfarb S, Kucheryavaya AY, Levvey BJ, et al. The registry of the international society for heart and lung transplantation: thirty-third adult heart transplantation report-2016; focus theme: primary diagnostic indications for transplant. J Heart Lung Transplant (2016) 35:1158–69. doi: 10.1016/j.healun.2016.08.017
2. Dolgos S, Hartmann A, Isaksen GA, Simonsen S, Bjortuft O, Boberg KM, et al. Osteoporosis is a prevalent finding in patients with solid organ failure awaiting transplantation - a population based study. Clin Transplant (2010) 24:E145–52. doi: 10.1111/j.1399-0012.2010.01231.x
3. Shane E, Rivas M, McMahon DJ, Staron RB, Silverberg SJ, Seibel MJ, et al. Bone loss and turnover after cardiac transplantation. J Clin Endocrinol Metab (1997) 82:1497–506. doi: 10.1210/jc.82.5.1497
4. Wang TK, O'Sullivan S, Gamble GD, Ruygrok PN. Bone density in heart or lung transplant recipients–a longitudinal study. Transplant Proc (2013) 45:2357–65. doi: 10.1016/j.transproceed.2012.09.117
5. Lofdahl E, Soderlund C, Radegran G. Bone mineral density and osteoporosis in heart transplanted patients: A single-center retrospective study at Skane University Hospital in Lund 1988-2016. Clin Transplant (2019) 33:e13477. doi: 10.1111/ctr.13477
6. Leidig-Bruckner G, Hosch S, Dodidou P, Ritschel D, Conradt C, Klose C, et al. Frequency and predictors of osteoporotic fractures after cardiac or liver transplantation: a follow-up study. Lancet (2001) 357:342–7. doi: 10.1016/S0140-6736(00)03641-2
7. Caffarelli C, Tomai Pitinca MD, Alessandri M, Cameli P, Bargagli E, Bennett D, et al. Timing of osteoporotic vertebral fractures in lung and heart transplantation: A longitudinal study. J Clin Med (2020) 9:9. doi: 10.3390/jcm9092941
8. Dalle Carbonare L, Zanatta M, Braga V, Sella S, Vilei MT, Feltrin G, et al. Densitometric threshold and vertebral fractures in heart transplant patients. Transplantation (2011) 92:106–11. doi: 10.1097/TP.0b013e31821cdeef
9. Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA (2009) 301:513–21. doi: 10.1001/jama.2009.50
10. Gilfraguas L, Guadalix S, Martinez G, Jodar E, Vara J, Gomez-Sanchez MA, et al. Bone loss after heart transplant: effect of alendronate, etidronate, calcitonin, and calcium plus vitamin D3. Prog Transplant (2012) 22:237–43. doi: 10.7182/pit2012969
11. Zhao X, Hu D, Qin J, Mohanan R, Chen L. Effect of bisphosphonates in preventing femoral periprosthetic bone resorption after primary cementless total hip arthroplasty: a meta-analysis. J Orthop Surg Res (2015) 10:65. doi: 10.1186/s13018-015-0206-8
12. Fardellone P, Sebert JL, Bouraya M, Bonidan O, Leclercq G, Doutrellot C, et al. [Evaluation of the calcium content of diet by frequential self-questionnaire]. Rev Rhum Mal Osteoartic (1991) 58:99–103.
13. Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group Osteoporos Int (1994) 4:368–81. doi: 10.1007/BF01622200
14. Genant HK, Jergas M, Palermo L, Nevitt M, Valentin RS, Black D, et al. Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis The Study of Osteoporotic Fractures Research Group. J Bone Miner Res (1996) 11:984–96. doi: 10.1002/jbmr.5650110716
15. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab (2011) 96:1911–30. doi: 10.1210/jc.2011-0385
16. Frenkel B, White W, Tuckermann J. Glucocorticoid-induced osteoporosis. Adv Exp Med Biol (2015) 872:179–215. doi: 10.1007/978-1-4939-2895-8_8
17. O'Brien CA, Jia D, Plotkin LI, Bellido T, Powers CC, Stewart SA, et al. Glucocorticoids act directly on osteoblasts and osteocytes to induce their apoptosis and reduce bone formation and strength. Endocrinology (2004) 145:1835–41. doi: 10.1210/en.2003-0990
18. Kim HJ, Zhao H, Kitaura H, Bhattacharyya S, Brewer JA, Muglia LJ, et al. Glucocorticoids suppress bone formation via the osteoclast. J Clin Invest (2006) 116:2152–60. doi: 10.1172/JCI28084
19. Buckley L, Humphrey MB. Glucocorticoid-induced osteoporosis. N Engl J Med (2018) 379:2547–56. doi: 10.1056/NEJMcp1800214
20. Shane E, Mancini D, Aaronson K, Silverberg SJ, Seibel MJ, Addesso V, et al. Bone mass, vitamin D deficiency, and hyperparathyroidism in congestive heart failure. Am J Med (1997) 103:197–207. doi: 10.1016/S0002-9343(97)00142-3
21. Costanzo MR, Dipchand A, Starling R, Anderson A, Chan M, Desai S, et al. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J Heart Lung Transplant (2010) 29:914–56. doi: 10.1016/j.healun.2010.05.034
22. Kanda J, Izumo N, Furukawa M, Shimakura T, Yamamoto N, Hee ET, et al. Effects of the calcineurin inhibitors cyclosporine and tacrolimus on bone metabolism in rats. BioMed Res (2018) 39:131–9. doi: 10.2220/biomedres.39.131
Keywords: heart transplant, bone mineral density, fractures, osteoporosis, vertebral fracture (VF)
Citation: Forien M, Coralli R, Verdonk C, Ottaviani S, Ebstein E, Demaria L, Palazzo E, Dorent R and Dieudé P (2023) Osteoporosis and risk of fracture in heart transplant patients. Front. Endocrinol. 14:1252966. doi: 10.3389/fendo.2023.1252966
Received: 04 July 2023; Accepted: 18 August 2023;
Published: 13 September 2023.
Edited by:
Giacomina Brunetti, University of Bari Aldo Moro, ItalyReviewed by:
Jan Josef Stepan, Charles University, CzechiaCopyright © 2023 Forien, Coralli, Verdonk, Ottaviani, Ebstein, Demaria, Palazzo, Dorent and Dieudé. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marine Forien, bWFyaW5lLmZvcmllbkBhcGhwLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.