
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol., 26 February 2024
Sec. Reproduction
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1226858
This article is part of the Research TopicMale Fertility: Lessons Learnt from the SARS-CoV-2 PandemicView all 6 articles
 Meshari A. Alzahrani1*†Khalid O. Alkhani2Abdullah M. Alassaf2Jehad I. Alorainy2Saleh Binsaleh3Raed Almannie3
Meshari A. Alzahrani1*†Khalid O. Alkhani2Abdullah M. Alassaf2Jehad I. Alorainy2Saleh Binsaleh3Raed Almannie3This extensive comprehensive review explores the impact of the Coronavirus disease 2019 (COVID-19) pandemic on men’s sexual and reproductive health. We conducted a literature review focusing on the possible pathophysiology by which severe acute respiratory syndrome corona virus 2 (SARS-CoV-2) affects men’s sexual and reproductive systems. We reviewed most of the studies that reported the impact of SARS-CoV-2 infection on the Testicular, Epididymal, Prostatic, and Penile tissue. Also, we focused on evaluating the SARS-CoV-2 infection on semen parameters and male reproductive hormones. Finally, we reviewed the COVID-19 vaccine’s effect on male reproductive and sexual health. Findings revealed the adverse consequences of SARS-CoV-2 at cellular and organ levels on the male genital tract. However, the reported data are still controversial. The initial data regarding COVID-19 vaccination was promising promoted safety for men’s reproductive and sexual health. We conclude this paper by offering recommendations to address these adverse consequences and potentially improve sexual and reproductive health among men in the post-COVID-19 pandemic era.
Coronavirus disease 2019 (COVID-19), first detected in China in December 2019, has since spread globally, with 132 million reported cases and 3 million deaths as of April 2021. (1, 2). The first publications from China and Italy reported higher fatality rates in men than in women due to the pandemic (3). New data reported in November 2021 continue to show that men have a more significant share of hospitalizations (55%), Intensive Care Unit (ICU) admissions (63%), and deaths (57%) (4).
SARS-CoV-2 infects cells through its spike protein binding to angiotensin-converting enzyme 2 (ACE2), with host transmembrane protease serine 2 (TMPRSS2) playing a crucial role in activating and cleaving the S protein as the virus binds to ACE2 (5). ACE2 is expressed in many organs and tissues. Studies have found that ACE2 and TMPRSS2 are expressed abundantly in testis somatic cells, spermatogonia, and peritubular myoid cells (6). Thus, a high level of susceptibility to SARS-CoV-2 for the testis has been established. However, there is controversy surrounding this conclusion. According to other studies ACE2 does not co-express with TMPRSS2 in testicular cells, supporting the notion that testicular cells are not highly susceptible to viral infection (7–9). SARS-CoV-2 entry and priming can be affected by testosterone and are linked to a weaker immune response, higher infection rates, and thromboembolic predisposition in male hosts (10). Compared with female subjects, Males appear to have a slower clearance rate of SARS-CoV-2, possibly as a result of higher ACE2 levels in the testis (11).
These findings have the potential to be very important for male sexual health; indeed, based on this preliminary evidence, there is quite enough evidence to hypothesize that the consequences of COVID-19 can extend to sexual and reproductive health. A retrospective study involving 1099 cases showed that the percentage of male COVID-19 patients was nearly 60%, and around 55% of them were reproductive-aged (15-49 years old). Therefore, concern was raised about whether SARS-CoV-2 may affect the male reproductive system (12, 13).
In this review, we aim to summarize the latest scientific updates on the effects of the novel coronavirus on several aspects of male reproductive health and fertility and to discuss the theories explaining the pathophysiology of these effects.
The pathological effects of SARS-CoV-2 infection on testicular tissue have been studied through molecular tests on deceased COVID-19 patients. The most common are Reverse transcription polymerase chain reaction (RT-PCR), Immunohistochemistry (IHC), and Transmission electron microscopy (TEM). Bian et al. (14) reported during the earlier stages of the pandemic that in deceased patients, SARS-CoV-2 was detected through RT-PCR. Since that study, conflicting evidence on the presence of SARS-CoV-2 in testicular histology has been published. Despite another study also confirming positive SARS-CoV-2 RT-PCR in the testis, three more recent studies reported a negative test in either all or the majority of their subjects (15–18). Masterson et al. (18) hypothesize that their adverse finding conflicted with previous studies due to the method of harvesting testicular tissue. At the same time, they used an open fashion in contrast to previous studies, which used a percutaneous biopsy which may raise concerns for potential contamination. Bian et al. (14) also reported positive IHC staining. However, IHC in the context of SARS-CoV-2 positive participants remains ambiguous. This is because there is no positive control for IHC staining, studies that reported positive findings have not shown a significant correlation within positive SARS-CoV-2 RT-PCR participants, and the molecules targeted in IHC staining have not been consistent throughout all the previous studies (15–18). Despite these higher levels of ACE2, IHC staining has been correlated with worse clinical outcomes regarding testis injury severity (19).
Similarly, reported data on the histopathological effect of SARS-CoV-2 on the testis have been conflicting. While these differences could be secondary to different methodologies in conducting the biopsies and reporting them, other theories should be considered. Bian et al. (14) initially said various degrees of injury to the testis and reduced spermatogenesis. Shortly after that study, another publication reported negative histopathological findings, which the authors attributed to the duration after the infection of which they obtained the biopsy. They hypothesize that the injury to the testis might have occurred at the earlier stage of the disease and have resolved later (15). Other studies with a shorter duration between the onset of symptoms and biopsy showed varying degrees of injury, including interstitial edema, vascular changes, and germ cell loss (16, 17). Finally, Masterson et al. (18) found no injury to testicular tissue in postmortem biopsies of deceased patients following SARS-CoV-2 infection. Their study was the first to conduct the biopsy using an open fashion, contrary to a percutaneous biopsy performed by a previous study. The authors hypothesize that positive findings reported previously could be secondary to contamination during a percutaneous biopsy. Summary for reported studies about impact of SARS-CoV-2 infection on testicular function at (Table 1).
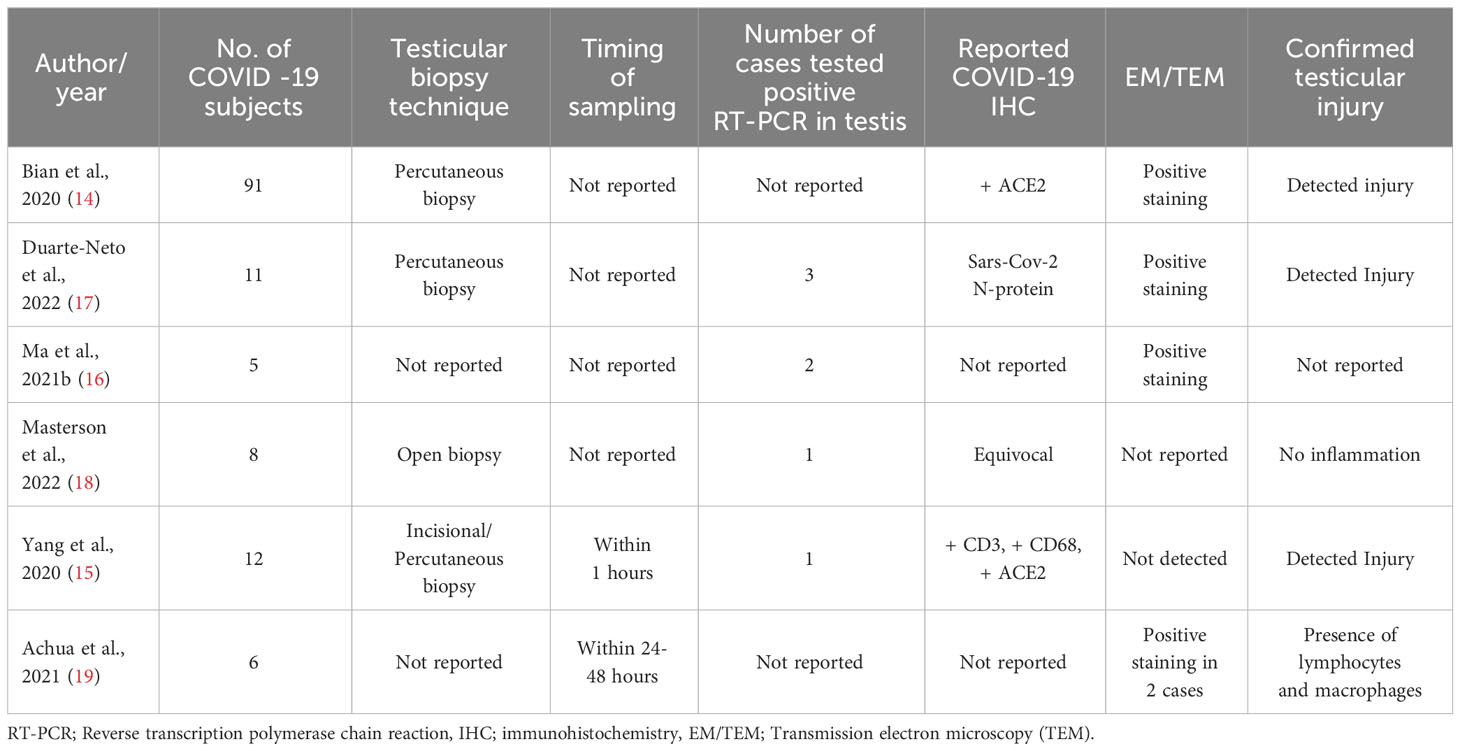
Table 1 Testicular histological features of patient diagnosed with COVID-19.
The limited expression of ACE2 in the epididymis has been reported (20). However, highly expressed receptors such as Neuropilin 1 (NRP1) and Cluster of Differentiation 147 (CD147) in the epididymis has been reported (21). Evidence suggest that the expression of the mentioned receptors play a significant role in the entry of SARS CoV 2 to host cells (22, 23). In addition, SARS-CoV-2’s spike protein can bind to epididymal sperm (24). Analysis of the epididymis in deceased COVID-19 patients found many immature spermatocytes and sperm accumulated in the cauda (25). Orchiepididymitis was diagnosed in a pediatric patient with COVID-19 who presented with testis swelling and epididymal inflammation with reactive hydrocele (26). Similarly, La Marca et al. (27) reported COVID-19-induced epididymitis symptoms, such as slight swelling and vascularization accentuation in the epididymis. COVID-19-induced epididymitis presents as a reactional hydrocele with nonuniform echo or microcyst dissemination, resulting in caput augmentation (>1.2 cm) and scrotum incrassation (28).
Prostatic fluid, also known as expressed prostatic secretion (EPS), is a vital component of semen secreted by the prostate gland, and it accounts for around 33% of the volume of ejaculation. Since ACE2 and TMPRSS2 are highly expressed in the epithelium of the human prostate, it is plausible to assume that SARS-CoV-2 could impact the prostate (29). The Androgen Receptor (AR) is vital in managing cellular activities associated with prostate function and physiology. Prostate cancer is directly connected to imbalances in androgen and AR signaling (30). Moreover, new studies suggest that ACE2 could be controlled by AR signaling (31, 32). Behavioral factors like smoking and obesity, as well as comorbidities such as diabetes, hypertension, and alcoholism, are known to affect COVID-19 severity as well as the progression and outcomes of prostate cancer (33–37). The most prominent shared risk factor for prostate cancer and COVID-19 complications and mortality is age, with men over 50 being at higher risk for prostate cancer and more prone to severe outcomes from COVID-19 (38–41). Several studies have demonstrated that androgens can influence the range of immune responses by modifying the behavior of particular immune subsets responsible for removing viruses (42, 43). Studies involving 84 subjects found no evidence of SARS-CoV-2 RNA in the EPS (44, 45).
Over the past few decades, a good amount of evidence supports erectile function as an excellent indicator of systemic health in general and vascular health in particular (46), effects of COVID-19 on the cardiovascular system (i.e., acute cardiac injury, myocarditis) as well growing evidence in the role of endothelial cell dysfunction during COVID-19 infection most importantly, the endothelium expresses the ACE2 led many have hypothesized there may be an increased risk of Erectile dysfunction (ED) following COVID-19 (47).
Three studies have assessed the association between COVID-19 and ED on a population level. Compared men with prior COVID-19 infection to men without documented COVID-19 infection. They all reported that newly diagnosed erectile dysfunction is higher in men with prior COVID-19 compared to age-matched control (47–49).
The pathophysiology behind this association between COVID-19 and ED has been described by a pilot study examined the histopathological features of two cases developing severe erectile dysfunction post-COVID-19 infection which revealed decreased expression of endothelial netric oxide synthase (eNOS), which is consistent with endothelial dysfunction (2). Moreover, this study reported positive spiked Coronavirus-like viral particles in the peri-vascular erectile tissue observed via TEM and Viral RNA was detected in the tissue samples using PCR (2).
A total of 10 observational studies that have been reviewed investigated the impact of SARS-CoV-2 infection and semen parameters (semen volume, sperm concentration, total sperm counts, percentages of total motile and progressively motile spermatozoa, percentage of normal morphology) in semen specimens collected from men who were acutely infected or those who were recovering/recovered from SARS-CoV-2 (1, 13, 45, 50–56), 9 of them reported a significant decline in one or more of the semen parameters in semen specimens of men with active or recent SARS-CoV2 infection in comparison to healthy controls or concerning WHO guidelines (57). However, the results of these studies were inconsistent regarding which semen parameter is affected, as two studies revealed a global decline in all semen parameters (50, 52), while the rest reported the change in only a few specific semen parameters that have been analyzed, Summary reported studies about the impact of COVID-19 on semen parameters are summarized in Table 2.

Table 2 COVID-19 effect on Semen parameters.
Guo et al. (55) revealed that all semen parameters were within normal reference range according to WHO guidelines; what distinguishes this study from the others that have been reviewed is the median interval from confirmation of SARS-CoV2 infection to providing semen samples from study subjects was only 32 days, and 52% of the subjects were still tested positive by pharyngeal swabs. This conflict between the studies suggests that SARS-CoV-2 infection is unlikely to cause semen quality to decline at the onset but rather be delayed with indirect pathophysiology. They considered the duration of human spermatogenesis, which is 78 days (55, 59).
Several theories have been put forward to explain the Impact of SARS-CoV-2 infection on semen quality; one of them is direct invasion and damage of the testicular tissue by the virus since It is known that a broad range of virus families, including human immunodeficiency virus (HIV), mumps virus, influenza, Zika virus, etc., may attack testes and affect male reproductive function (59).
Preliminary studies on SARS-CoV-2 infection had indicated the possibility of SARS-CoV-2 outreach to male gonads, suggesting the role of ACE2 as the cellular receptor for SARS-CoV-2 may be the mechanism for access to the male reproductive organs where ACE2 is predominantly (51). Therefore, theoretically regarded as a vulnerable target to SARS-CoV-2. 8 studies reported the absence of SARS-CoV-2 in all semen specimens collected from men who were acutely infected or those who were recovering/recovered from SARS-CoV-2; these reports suggest that the testis might be not a target organ for SARS-CoV-2 (13, 45, 50, 51, 54, 55, 60, 61). Contrary to these reports, two studies demonstrated SARS-Cov-2 positivity in semen samples. In contrast, one study conducted in China revealed that SARS-CoV-2 was detectable in 6 out of 38 (15.8%) semen specimens collected from male COVID-19 patients, including the patients recovered from the infection (2 out of 23, 8.7%) (58). However, this study did not describe the semen collection or analysis in detail, nor was there evidence of SARS-CoV-2 in the urine of these patients, so the possibility of viral contamination from non-semen sources could not be excluded completely; the other study conducted in Italy reported detection of one positive SARS-CoV-2 genome in semen sample after 21 days after the second negative swab (53). Li et al. (51) suggests that detecting SARS-CoV-2 in the seminal fluid is not necessarily considered an absolute determinant of the impact of SARS-CoV-2 on male fertility and semen quality. And there are multiple other probable indirect mechanisms where SARS-CoV-2 infection could affect semen quality apart from a natural condition. Carlsen et al. (62) investigated the effect of febrile illness on semen parameters during the different phases of spermatogenesis; the study found that sperm concentration, morphology, and motility were significantly affected by fever occurring during the period of meiosis and the postmitotic period (spermiogenesis), but not by fever occurring during mitotic proliferation or after completion of spermiogenesis. An effect on sperm morphology and motility can only be seen when fever occurs during spermiogenesis, where the spermatids undergo morphological changes to sperm and acquire motility. However, the study couldn’t attribute the difference due to fever or the underlying cause of febrile illness (62).
Li et al. (51) investigated levels of proinflammatory cytokines and chemokines in semen samples in recovering COVID-19 men, the study shows increased seminal levels of IL-6, TNF- a, and MCP-1 compared to control males were observed. Although the absence of RNA virus detection was demonstrated by the studies discussed earlier including the aforementioned study. Altered seminal immune markers signifying immune impairment by COVID-19 illness Li et al. (51). This suggests that impaired semen quality among COVID-19 patients could be a result of the immune response in the testis and epididymis in COVID-19 patients.
In addition to these theories, several articles have been attributed the change in semen parameters to hormonal changes (low testosterone levels) (53, 54). The impact of SARS-CoV-2 on axis male reproductive hormonal function will be discussed below in further details.
Testosterone (T) and Follicle-stimulating hormone (FSH) serum levels were lower in infected males and serum Luteinizing Hormone (LH) levels were considerably higher. Also, a significant elevation in serum prolactin (PRL) levels was noted (63). It is important to point out that PRL can be influenced by many factors. Higher PRL levels may suppress the pituitary gland resulting in decreased gonadotropin levels (64). In a follow-up study of men recovering from COVID-19 over seven months, it was found that almost 90% of patients had increased total testosterone (tT) levels after recovery compared to baseline levels. However, further decreased tT levels were observed in 10% of the patients, suggesting persistent hypogonadism. Additionally, 55% of men had tT concentrations suggestive of hypogonadism, especially when comorbid conditions are present (65). Also, Apaydin et al. found that hypogonadism persisted in 48.2% of men with lower T concentrations over a six-month follow-up post-recovery (66). Even after 12 months of recovery, almost 30% of men still had serum T levels consistent with biochemical hypogonadism. Of clinical relevance, the lower the serum T at admission, the poorer the outcomes and the lower the probability of achieving a state of eugonadal, even after a long period of follow-up (67). Summary reported studies about the impact of COVID-19 on male reproductive hormones are summarized in Table 3.
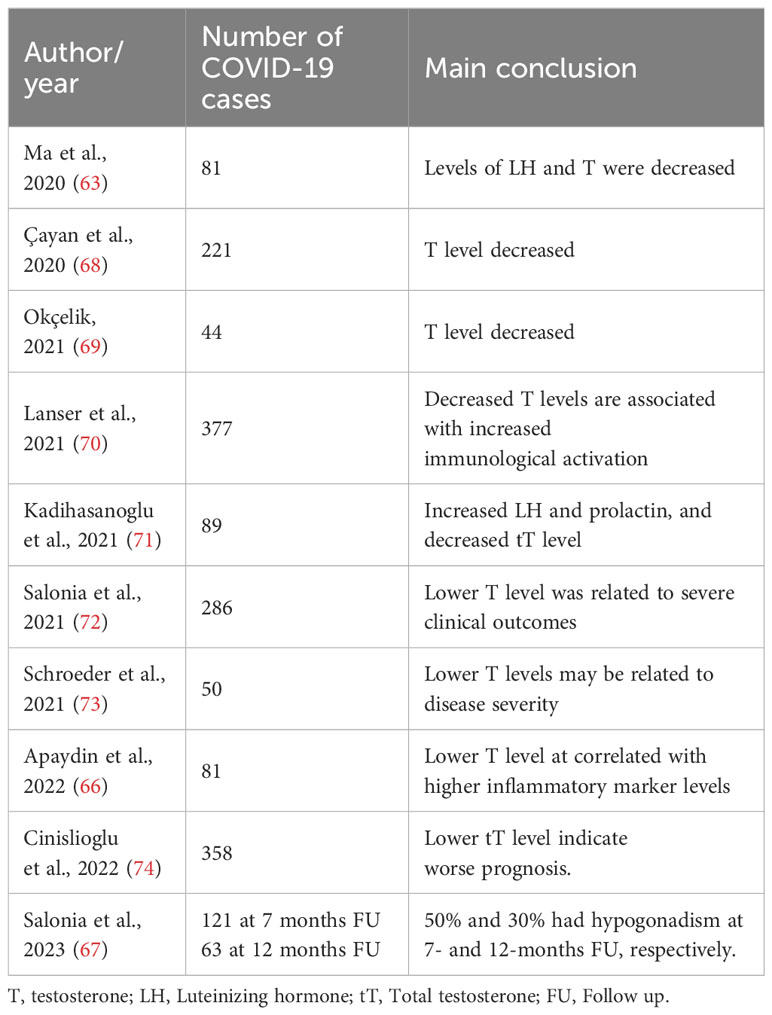
Table 3 COVID-19 effect on male reproductive hormones.
Furthermore, autopsy analysis from the testicular tissue of patients with COVID-19 found that Leydig cells were significantly reduced in the testicular interstitium, which suggests that SARS-CoV-2 may have caused ultrastructural damage to the cells. ACE2 was diffusely expressed in Sertoli cells and strongly expressed in Leydig cells, as revealed by immunostaining (15).
While there has been evidence of the effect of SARS-CoV-2 on sperm parameters, studying the impact of the COVID-19 vaccine is of equal importance, if not more. Not only assuring the vaccine’s safety but also addressing the fears of the general population and increasing acceptance of the vaccine. Several prospective cohort studies have assessed the effect of the SARS-CoV-2 vaccine on semen parameters and found evidence for changes in semen parameters (75, 76). However, one cohort study found that there has been an increase in sperm concentration (77), and another case report found that patients with ankylosing spondylitis who were vaccinated had improved morphology compared to those who were unvaccinated (78). Another study that tested the effect of both the mRNA vaccine and the viral vector vaccine showed no impact on sperm quality (79). Similar results were replicated by multiple studies (79–85). Summary of the reported studies about the impact of COVID-19 vaccine on semen parameters are summarized in Table 4.
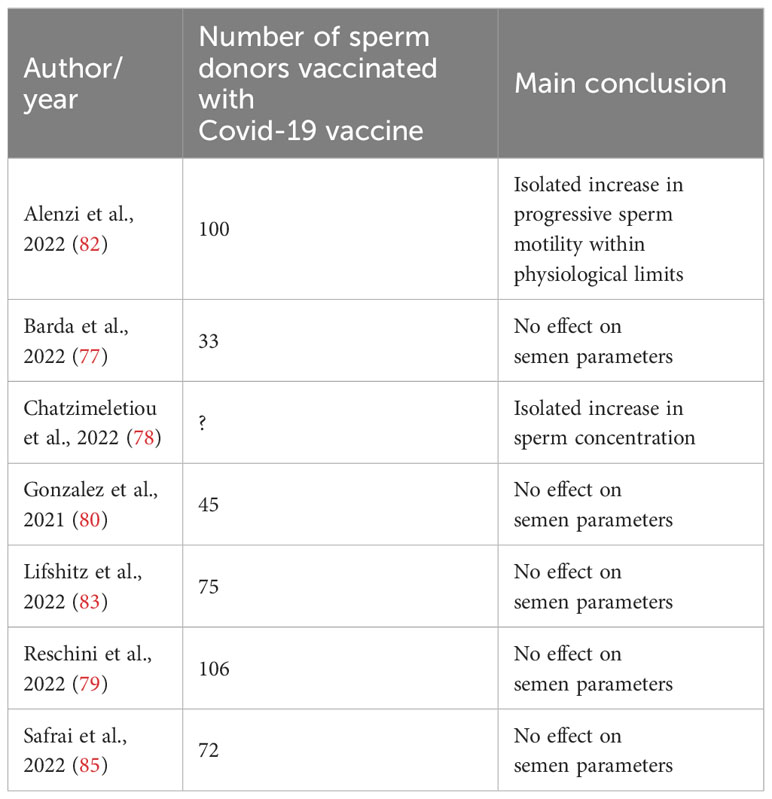
Table 4 Effects of COVID-19 vaccine on semen parameters.
Since a meta-analysis was published that showed no significant effect of the mRNA vaccine on semen parameters (86). And following that, a more considerable multinational analysis found no association between BNT162b2 and mRNA-1273 and sub-fertility in men (87).
Other factors studied in correlation to the COVID-19 vaccine include male reproductive hormones. A study conducted by Adamyan et al. found no effect of the SARS-CoV-2 vaccine on the level of testosterone, FSH, LH, or Estradiol hormones (88). Another study showed that the mRNA vaccine showed no association with the risk of developing orchitis or epididymitis, as reported for the SARS-CoV-2 infection (89). Furthermore, when the rate of orchitis and epididymitis was compared between vaccinated and non-vaccinated participants, the rate was significantly lower in vaccinated participants after only a single dose (90). Several systematic reviews and other reviews conclude to find no significant negative effect of the SARS-CoV-2 vaccine on male reproductive health (88, 91). As for Sexual Health, in a large study that isolated all reported urological symptoms from a sample of 15,785 participants, no symptoms related to Erectile function, ejaculatory function, or sexual function were reported (92). Furthermore, a prospective questionnaire-based study concluded that the COVID-19 vaccine did not affect male sexual function (93).
This review is not without limitations. The study concentrated on papers published within a defined time frame and in specific databases, which may have eliminated relevant articles. Nonetheless, the review provided valuable updated insights into the impact of the COVID-19 pandemic on men’s sexual and reproductive health.
COVID-19 and its control measures appear to disproportionately impact men’s and women’s sexual and reproductive outcomes. As a result of the COVID-19 pandemic response, the availability of sexual and reproductive services, as well as access to family planning and contraception, has significantly decreased. Men infected with COVID-19 have more severe illness and a greater fatality rate than women. Understanding why males are more prone than women to suffer serious diseases can aid in developing effective therapies, public health policies, and focused tactics such as early detection and intensive testing in subgroups.
Our review attempted to synthesize the published literature about the impact of the COVID-19 pandemic on sexual and reproductive health among men. To date, many studies reported controversial data specifically related to the COVID-19 pathophysiology on men’s sexual and reproductive experiences during the pandemic, which warrants further clinical investigation.
MA, RM, and SB participated in the design of this study. MA and RM conducted the literature search. MA, RM, and SB retrieved and selected the articles. MAA and KA conducted the data extraction. MA, KA, AA, and JA wrote the manuscript draft. MA supervised the study. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors would like to thank the Deanship of Scientific Research at Majmaah University for supporting this work under project number (R-2024-921).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Falahieh FM, Zarabadipour M, Mirani M, Abdiyan M, DInparvar M, Alizadeh H, et al. Effects of moderate COVID-19 infection on semen oxidative status and parameters 14 and 120 days after diagnosis. Reprod Fertil Dev (2021) 33:683–90. doi: 10.1071/RD21153
2. Kresch E, Achua J, Saltzman R, Khodamoradi K, Arora H, Ibrahim E, et al. COVID-19 endothelial dysfunction can cause erectile dysfunction: histopathological, immunohistochemical, and ultrastructural study of the human penis. World J Mens Health (2021) 39. doi: 10.5534/WJMH.210055
3. Rozenberg S, Vandromme J, Charlotte M. Are we equal in adversity? Does Covid-19 affect women and men differently? Maturitas (2020) 138:62–8. doi: 10.1016/J.MATURITAS.2020.05.009
4. THE COVID-19 SEX-DISAGGREGATED DATA TRACKER NOVEMBER UPDATE. (2021). Available at: https://globalhealth5050.org/wp-content/uploads/November-2021-data-tracker-update.pdf (Accessed May 6, 2023).
5. Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-coV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell (2020) 181:271–280.e8. doi: 10.1016/J.CELL.2020.02.052
6. Qi J, Zhou Y, Hua J, Zhang L, Bian J, Liu B, et al. The scRNA-seq expression profiling of the receptor ACE2 and the cellular protease TMPRSS2 reveals human organs susceptible to SARS-coV-2 infection. Int J Environ Res Public Health (2021) 18:1–17. doi: 10.3390/IJERPH18010284
7. Baughn LB, Sharma N, Elhaik E, Sekulic A, Bryce AH, Fonseca R. Targeting TMPRSS2 in SARS-coV-2 infection. Mayo Clin Proc (2020) 95:1989–99. doi: 10.1016/J.MAYOCP.2020.06.018
8. Pan F, Xiao X, Guo J, Song Y, Li H, Patel DP, et al. No evidence of severe acute respiratory syndrome-coronavirus 2 in semen of males recovering from coronavirus disease 2019. Fertil Steril (2020) 113:1135–9. doi: 10.1016/J.FERTNSTERT.2020.04.024
9. Borges E, Setti AS, Iaconelli A, de Braga DPAF. Current status of the COVID-19 and male reproduction: A review of the literature. Andrology (2021) 9:1066–75. doi: 10.1111/ANDR.13037
10. Pivonello R, Auriemma RS, Pivonello C, Isidori AM, Corona G, Colao A, et al. Sex disparities in COVID-19 severity and outcome: are men weaker or women stronger? Neuroendocrinology (2021) 111:1066–85. doi: 10.1159/000513346
11. Shastri A, Wheat J, Agrawal S, Chaterjee N, Pradhan K, Goldfinger M, et al. Delayed clearance of SARS-CoV2 in male compared to female patients: High ACE2 expression in testes suggests possible existence of gender-specific viral reservoirs. medRxiv (2020), 2020.04.16.20060566. doi: 10.1101/2020.04.16.20060566
12. Eastin C, Eastin T. Clinical characteristics of coronavirus disease 2019 in China. J Emerg Med (2020) 58:711–2. doi: 10.1016/j.jemermed.2020.04.004
13. Ma L, Xie W, Li D, Shi L, Ye G, Mao Y, et al. Evaluation of sex-related hormones and semen characteristics in reproductive-aged male COVID-19 patients. J Med Virol (2021) 93:456–62. doi: 10.1002/JMV.26259
14. Bian XW, Yao XH, Ping YF, Yu S, Shi Y, Luo T, et al. Autopsy of COVID-19 patients in China. Natl Sci Rev (2020) 7:1414–8. doi: 10.1093/NSR/NWAA123
15. Yang M, Chen S, Huang B, Zhong JM, Su H, Chen YJ, et al. Pathological findings in the testes of COVID-19 patients: clinical implications. Eur Urol Focus (2020) 6:1124–9. doi: 10.1016/J.EUF.2020.05.009
16. Ma X, Guan C, Chen R, Wang Y, Feng S, Wang R, et al. Pathological and molecular examinations of postmortem testis biopsies reveal SARS-CoV-2 infection in the testis and spermatogenesis damage in COVID-19 patients. Cell Mol Immunol (2021) 18:487–9. doi: 10.1038/S41423-020-00604-5
17. Duarte-Neto AN, Teixeira TA, Caldini EG, Kanamura CT, Gomes-Gouvêa MS, dos Santos ABG, et al. Testicular pathology in fatal COVID-19: A descriptive autopsy study. Andrology (2022) 10:13–23. doi: 10.1111/ANDR.13073
18. Masterson JM, Bui C, Hasan W, Zhang Y, Huynh C, Jawanda H, et al. Case series - COVID-19 is unlikely to affect male fertility: Results of histopathological and reverse transcriptase polymerase chain reaction analysis. Can Urol Assoc J (2022) 16. doi: 10.5489/CUAJ.7850
19. Achua JK, Chu KY, Ibrahim E, Khodamoradi K, Delma KS, Iakymenko OA, et al. Histopathology and ultrastructural findings of fatal COVID-19 infections on testis. World J Mens Health (2021) 39:65–74. doi: 10.5534/WJMH.200170
20. Hikmet F, Méar L, Edvinsson Å, Micke P, Uhlén M, Lindskog C. The protein expression profile of ACE2 in human tissues. Mol Syst Biol (2020) 16. doi: 10.15252/MSB.20209610
21. Wang Y, Wang Y, Luo W, Huang L, Xiao J, Li F, et al. A comprehensive investigation of the mRNA and protein level of ACE2, the putative receptor of SARS-CoV-2, in human tissues and blood cells. Int J Med Sci (2020) 17:1522–31. doi: 10.7150/IJMS.46695
22. Cantuti-Castelvetri L, Ojha R, Pedro LD, Djannatian M, Franz J, Kuivanen S, et al. Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science (2020) 370. doi: 10.1126/SCIENCE.ABD2985
23. Fenizia C, Galbiati S, Vanetti C, Vago R, Clerici M, Tacchetti C, et al. SARS-coV-2 entry: at the crossroads of CD147 and ACE2. Cells (2021) 10. doi: 10.3390/CELLS10061434
24. Yao XH, Luo T, Shi Y, He ZC, Tang R, Zhang PP, et al. A cohort autopsy study defines COVID-19 systemic pathogenesis. Cell Res (2021) 31:836–46. doi: 10.1038/S41422-021-00523-8
25. Flaifel A, Guzzetta M, Occidental M, Najari BB, Melamed J, Thomas KM, et al. Testicular changes associated with severe acute respiratory syndrome coronavirus 2 (SARS-coV-2). Arch Pathol Lab Med (2021) 145:8–9. doi: 10.5858/ARPA.2020-0487-LE
26. Gagliardi L, Bertacca C, Centenari C, Merusi I, Parolo E, Ragazzo V, et al. Orchiepididymitis in a boy with COVID-19. Pediatr Infect Dis J (2020) 39:E200–2. doi: 10.1097/INF.0000000000002769
27. La Marca A, Busani S, Donno V, Guaraldi G, Ligabue G, Girardis M. Testicular pain as an unusual presentation of COVID-19: a brief review of SARS-CoV-2 and the testis. Reprod BioMed Online (2020) 41:903–6. doi: 10.1016/J.RBMO.2020.07.017
28. Carneiro F, Teixeira TA, Bernardes FS, Pereira MS, Milani G, Duarte-Neto AN, et al. Radiological patterns of incidental epididymitis in mild-to-moderate COVID-19 patients revealed by color Doppler ultrasound. Andrologia (2021) 53. doi: 10.1111/AND.13973
29. Chen YW, Lee MS, Lucht A, Chou FP, Huang W, Havighurst TC, et al. TMPRSS2, a serine protease expressed in the prostate on the apical surface of luminal epithelial cells and released into semen in prostasomes, is misregulated in prostate cancer cells. Am J Pathol (2010) 176:2986–96. doi: 10.2353/AJPATH.2010.090665
30. Toivanen R, Shen MM. Prostate organogenesis: tissue induction, hormonal regulation and cell type specification. Development (2017) 144:1382–98. doi: 10.1242/DEV.148270
31. Lucas JM, True L, Hawley S, Matsumura M, Morrissey C, Vessella R, et al. The androgen-regulated type II serine protease TMPRSS2 is differentially expressed and mislocalized in prostate adenocarcinoma. J Pathol (2008) 215:118–25. doi: 10.1002/PATH.2330
32. Wambier CG, Goren A, Vaño-Galván S, Ramos PM, Ossimetha A, Nau G, et al. Androgen sensitivity gateway to COVID-19 disease severity. Drug Dev Res (2020) 81:771–6. doi: 10.1002/DDR.21688
33. Huncharek M, Sue Haddock K, Reid R, Kupelnick B. Smoking as a risk factor for prostate cancer: a meta-analysis of 24 prospective cohort studies. Am J Public Health (2010) 100:693–701. doi: 10.2105/AJPH.2008.150508
34. Lee J, Giovannucci E, Jeon JY. Diabetes and mortality in patients with prostate cancer: a meta-analysis. Springerplus (2016) 5. doi: 10.1186/S40064-016-3233-Y
35. Liang Z, Xie B, Li J, Wang X, Wang S, Meng S, et al. Hypertension and risk of prostate cancer: a systematic review and meta-analysis. Sci Rep (2016) 6. doi: 10.1038/SREP31358
36. Navin S, Ioffe V. The association between hypertension and prostate cancer. Rev Urol (2017) 19:113–8. doi: 10.3909/RIU0758
37. Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med (2020) 8:e21. doi: 10.1016/S2213-2600(20)30116-8
38. Banerjee A, Pasea L, Harris S, Gonzalez-Izquierdo A, Torralbo A, Shallcross L, et al. Estimating excess 1-year mortality associated with the COVID-19 pandemic according to underlying conditions and age: a population-based cohort study. Lancet (2020) 395:1715–25. doi: 10.1016/S0140-6736(20)30854-0
39. Di Stadio A, Ricci G, Greco A, De Vincentiis M, Ralli M. Mortality rate and gender differences in COVID-19 patients dying in Italy: A comparison with other countries. Eur Rev Med Pharmacol Sci (2020) 24:4066–7. doi: 10.26355/EURREV_202004_20980
40. Liu W, Tao ZW, Wang L, Yuan ML, Liu K, Zhou L, et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin Med J (Engl) (2020) 133:1032–8. doi: 10.1097/CM9.0000000000000775
41. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
42. Cutolo M, Sulli A, Capellino S, Villaggio B, Montagna P, Seriolo B, et al. Sex hormones influence on the immune system: basic and clinical aspects in autoimmunity. Lupus (2004) 13:635–8. doi: 10.1191/0961203304LU1094OA
43. Bupp MRG, Jorgensen TN. Androgen-induced immunosuppression. Front Immunol (2018) 9:794. doi: 10.3389/FIMMU.2018.00794
44. Zhang S, Wang X, Zhang H, Xu A, Fei G, Jiang X, et al. The absence of coronavirus in expressed prostatic secretion in COVID-19 patients in Wuhan city. Reprod Toxicol (2020) 96:90–4. doi: 10.1016/J.REPROTOX.2020.06.006
45. Ruan Y, Hu B, Liu Z, Liu K, Jiang H, Li H, et al. No detection of SARS-CoV-2 from urine, expressed prostatic secretions, and semen in 74 recovered COVID-19 male patients: A perspective and urogenital evaluation. Andrology (2021) 9:99–106. doi: 10.1111/ANDR.12939
46. Sansone A, Mollaioli D, Ciocca G, Limoncin E, Colonnello E, Vena W, et al. Addressing male sexual and reproductive health in the wake of COVID-19 outbreak. J Endocrinol Invest (2021) 44:223–31. doi: 10.1007/S40618-020-01350-1
47. Hebert KJ, Matta R, Horns JJ, Paudel N, Das R, McCormick BJ, et al. Prior COVID-19 infection associated with increased risk of newly diagnosed erectile dysfunction. Int J Impot Res (2023). doi: 10.1038/S41443-023-00687-4
48. Chu KY, Nackeeran S, Horodyski L, Masterson TA, Ramasamy R. COVID-19 infection is associated with new onset erectile dysfunction: insights from a national registry. Sex Med (2022) 10. doi: 10.1016/J.ESXM.2021.100478
49. Katz J, Yue S, Xue W, Gao H. Increased odds ratio for erectile dysfunction in COVID-19 patients. J Endocrinol Invest (2022) 45:859–64. doi: 10.1007/S40618-021-01717-Y
50. Holtmann N, Edimiris P, Andree M, Doehmen C, Baston-Buest D, Adams O, et al. Assessment of SARS-CoV-2 in human semen-a cohort study. Fertil Steril (2020) 114:233–8. doi: 10.1016/J.FERTNSTERT.2020.05.028
51. Li H, Xiao X, Zhang J, Zafar MI, Wu C, Long Y, et al. Impaired spermatogenesis in COVID-19 patients. EClinicalMedicine (2020) 28. doi: 10.1016/J.ECLINM.2020.100604
52. Erbay G, Sanli A, Turel H, Yavuz U, Erdogan A, Karabakan M, et al. Short-term effects of COVID-19 on semen parameters: A multicenter study of 69 cases. Andrology (2021) 9:1060–5. doi: 10.1111/ANDR.13019
53. Gacci M, Coppi M, Baldi E, Sebastianelli A, Zaccaro C, Morselli S, et al. Semen impairment and occurrence of SARS-CoV-2 virus in semen after recovery from COVID-19. Hum Reprod (2021) 36:1520–9. doi: 10.1093/HUMREP/DEAB026
54. Temiz MZ, Dincer MM, Hacibey I, Yazar RO, Celik C, Kucuk SH, et al. Investigation of SARS-CoV-2 in semen samples and the effects of COVID-19 on male sexual health by using semen analysis and serum male hormone profile: A cross-sectional, pilot study. Andrologia (2021) 53. doi: 10.1111/AND.13912
55. Guo L, Zhao S, Li W, Wang Y, Li L, Jiang S, et al. Absence of SARS-CoV-2 in semen of a COVID-19 patient cohort. Andrology (2021) 9:42–7. doi: 10.1111/ANDR.12848
56. Guo TH, Sang MY, Bai S, Ma H, Wan YY, Jiang XH, et al. Semen parameters in men recovered from COVID-19. Asian J Androl (2021) 23:479–83. doi: 10.4103/AJA.AJA_31_21
57. Boitrelle F, Shah R, Saleh R, Henkel R, Kandil H, Chung E, et al. The sixth edition of the WHO manual for human semen analysis: A critical review and SWOT analysis. Life (2021) 11. doi: 10.3390/LIFE11121368
58. Li D, Jin M, Bao P, Zhao W, Zhang S. Clinical characteristics and results of semen tests among men with coronavirus disease 2019. JAMA Netw Open (2020) 3:e208292. doi: 10.1001/JAMANETWORKOPEN.2020.8292
59. Griswold MD. Spermatogenesis: the commitment to meiosis. Physiol Rev (2016) 96:1–17. doi: 10.1152/PHYSREV.00013.2015
60. Pavone C, Giammanco GM, Baiamonte D, Pinelli M, Bonura C, Montalbano M, et al. Italian males recovering from mild COVID-19 show no evidence of SARS-CoV-2 in semen despite prolonged nasopharyngeal swab positivity. Int J Impot Res (2020) 32:560–2. doi: 10.1038/S41443-020-00344-0
61. Song C, Wang Y, Li W, Hu B, Chen G, Xia P, et al. Absence of 2019 novel coronavirus in semen and testes of COVID-19 patients†. Biol Reprod (2020) 103:4–6. doi: 10.1093/BIOLRE/IOAA050
62. Carlsen E, Andersson AM, Petersen JH, Skakkebæk NE. History of febrile illness and variation in semen quality. Hum Reprod (2003) 18:2089–92. doi: 10.1093/HUMREP/DEG412
63. Ma L, Xie W, Li D, Shi L, Mao Y, Xiong Y, et al. Effect of SARS-CoV-2 infection upon male gonadal function: A single center-based study. medRxiv (2020), 2020.03.21.20037267. doi: 10.1101/2020.03.21.20037267
64. Brown RSE, Khant Aung Z, Phillipps HR, Barad Z, Lein HJ, Boehm U, et al. Acute suppression of LH secretion by prolactin in female mice is mediated by kisspeptin neurons in the arcuate nucleus. Endocrinology (2019) 160:1323–32. doi: 10.1210/EN.2019-00038
65. Salonia A, Pontillo M, Capogrosso P, Gregori S, Carenzi C, Ferrara AM, et al. Testosterone in males with COVID-19: A 7-month cohort study. Andrology (2022) 10:34–41. doi: 10.1111/ANDR.13097
66. Apaydin T, Sahin B, Dashdamirova S, Dincer Yazan C, Elbasan O, Ilgin C, et al. The association of free testosterone levels with coronavirus disease 2019. Andrology (2022) 10:1038–46. doi: 10.1111/ANDR.13152
67. Salonia A, Pontillo M, Capogrosso P, Pozzi E, Ferrara AM, Cotelessa A, et al. Testosterone in males with COVID-19: a 12-month cohort study. Andrology (2023) 11:17–23. doi: 10.1111/ANDR.13322
68. Çayan S, Uğuz M, Saylam B, Akbay E. Effect of serum total testosterone and its relationship with other laboratory parameters on the prognosis of coronavirus disease 2019 (COVID-19) in SARS-CoV-2 infected male patients: a cohort study. Aging Male (2020) 23:1493–503. doi: 10.1080/13685538.2020.1807930
69. Okçelik S. COVID-19 pneumonia causes lower testosterone levels. Andrologia (2021) 53. doi: 10.1111/AND.13909
70. Lanser L, Burkert FR, Thommes L, Egger A, Hoermann G, Kaser S, et al. Testosterone deficiency is a risk factor for severe COVID-19. Front Endocrinol (Lausanne) (2021) 12:694083. doi: 10.3389/FENDO.2021.694083
71. Kadihasanoglu M, Aktas S, Yardimci E, Aral H, Kadioglu A. SARS-coV-2 pneumonia affects male reproductive hormone levels: A prospective, cohort study. J Sex Med (2021) 18:256–64. doi: 10.1016/J.JSXM.2020.11.007
72. Salonia A, Pontillo M, Capogrosso P, Gregori S, Tassara M, Boeri L, et al. Severely low testosterone in males with COVID-19: A case-control study. Andrology (2021) 9:1043–52. doi: 10.1111/ANDR.12993
73. Schroeder M, Schaumburg B, Mueller Z, Parplys A, Jarczak D, Roedl K, et al. High estradiol and low testosterone levels are associated with critical illness in male but not in female COVID-19 patients: a retrospective cohort study. Emerg Microbes Infect (2021) 10:1807–18. doi: 10.1080/22221751.2021.1969869
74. Cinislioglu AE, Cinislioglu N, Demirdogen SO, Sam E, Akkas F, Altay MS, et al. The relationship of serum testosterone levels with the clinical course and prognosis of COVID-19 disease in male patients: A prospective study. Andrology (2022) 10:24–33. doi: 10.1111/ANDR.13081
75. Olana S, Mazzilli R, Salerno G, Zamponi V, Tarsitano MG, Simmaco M, et al. 4BNT162b2 mRNA COVID-19 vaccine and semen: What do we know? Andrology (2022) 10:1023–9. doi: 10.1111/ANDR.13199
76. Zhu H, Wang X, Zhang F, Zhu Y, Du MR, Tao ZW, et al. Evaluation of inactivated COVID-19 vaccine on semen parameters in reproductive-age males: a retrospective cohort study. Asian J Androl (2022) 24:441–4. doi: 10.4103/AJA202225
77. Barda S, Laskov I, Grisaru D, Lehavi O, Kleiman S, Wenkert A, et al. The impact of COVID-19 vaccine on sperm quality. Int J Gynaecol Obstet (2022) 158:116–20. doi: 10.1002/IJGO.14135
78. Chatzimeletiou K, Fleva A, Sioga A, Georgiou I, Nikolopoulos TT, Markopoulou M, et al. Effects of different drug therapies and COVID-19 mRNA vaccination on semen quality in a man with ankylosing spondylitis: A case report. Med (Kaunas) (2022) 58. doi: 10.3390/MEDICINA58020173
79. Reschini M, Pagliardini L, Boeri L, Piazzini F, Bandini V, Fornelli G, et al. COVID-19 vaccination does not affect reproductive health parameters in men. Front Public Health (2022) 10:839967. doi: 10.3389/FPUBH.2022.839967
80. Gonzalez DC, Nassau DE, Khodamoradi K, Ibrahim E, Blachman-Braun R, Ory J, et al. Sperm parameters before and after COVID-19 mRNA vaccination. JAMA (2021) 326:273–4. doi: 10.1001/JAMA.2021.9976
81. Gonzalez D, Nassau DE, Khodamoradi K, Ibrahim E, Blachman-Braun R, Dubin JM, et al. EFFECT OF COVID-19 mRNA VACCINES ON SPERM QUALITY. Fertil Steril (2021) 116:e297. doi: 10.1016/J.FERTNSTERT.2021.07.799
82. Alenzi MJ, Ikpi EE, Alshlash AS, Alkhaldi SM, Aljazi ZN, Alrawili M, et al. Do the Covid-19 vaccines affect the reproductive parameters of men?-A Northern Saudi experience. Niger J Clin Pract (2022) 25:1812–5. doi: 10.4103/NJCP.NJCP_188_22
83. Lifshitz D, Haas J, Lebovitz O, Raviv G, Orvieto R, Aizer A. Does mRNA SARS-CoV-2 vaccine detrimentally affect male fertility, as reflected by semen analysis? Reprod BioMed Online (2022) 44:145–9. doi: 10.1016/J.RBMO.2021.09.021
84. Omolaoye TS, Velilla PA, López JSM, du Plessis SS, Cardona Maya WD. SARS-coV-2 vaccine effects on semen parameters: A systematic review and meta-analysis. Arch Esp Urol (2022) 75:831–43. doi: 10.56434/J.ARCH.ESP.UROL.20227510.121
85. Safrai M, Herzberg S, Imbar T, Reubinoff B, Dior U, Ben-Meir A. The BNT162b2 mRNA Covid-19 vaccine does not impair sperm parameters. Reprod BioMed Online (2022) 44:685–8. doi: 10.1016/J.RBMO.2022.01.008
86. Corona G, Vena W, Pizzocaro A, Pallotti F, Paoli D, Rastrelli G, et al. Andrological effects of SARS-Cov-2 infection: a systematic review and meta-analysis. J Endocrinol Invest (2022) 45:2207–19. doi: 10.1007/S40618-022-01801-X
87. Dai P, Qiao F, Chen Y, Chan DYL, Yim HCH, Fok KL, et al. SARS-CoV-2 and male infertility: from short- to long-term impacts. J Endocrinol Invest (2023). doi: 10.1007/S40618-023-02055-X
88. Adamyan L, Elagin V, Vechorko V, Stepanian A, Dashko A, Doroshenko D, et al. A review of recent studies on the effects of SARS-coV-2 infection and SARS-coV-2 vaccines on male reproductive health. Med Sci Monit (2022) 28. doi: 10.12659/MSM.935879
89. Carto C, Nackeeran S, Ramasamy R. COVID-19 vaccination is associated with a decreased risk of orchitis and/or epididymitis in men. Andrologia (2022) 54. doi: 10.1111/AND.14281
91. Pourmasumi S, Nazari A, Ahmadi Z, Kouni SN, de Gregorio C, Koniari I, et al. The effect of long COVID-19 infection and vaccination on male fertility; A narrative review. Vaccines (Basel) (2022) 10. doi: 10.3390/VACCINES10121982
92. Zhao H, Souders C, Carmel M, Anger JT. Low rates of urologic side effects following coronavirus disease vaccination: an analysis of the food and drug administration vaccine adverse event reporting system. Urology (2021) 153:11–3. doi: 10.1016/J.UROLOGY.2021.04.002
Keywords: men, COVID-19, SAR-CoV-2, sexual health, reproductive health, pathophysiology
Citation: Alzahrani MA, Alkhani KO, Alassaf AM, Alorainy JI, Binsaleh S and Almannie R (2024) Updates in the pathophysiology of COVID-19 infection in male reproductive and sexual health: a literature review. Front. Endocrinol. 14:1226858. doi: 10.3389/fendo.2023.1226858
Received: 23 May 2023; Accepted: 26 December 2023;
Published: 26 February 2024.
Edited by:
Eva Tvrda, Slovak University of Agriculture, SlovakiaReviewed by:
Pavla Postlerova, Institute of Biotechnology (ASCR), CzechiaCopyright © 2024 Alzahrani, Alkhani, Alassaf, Alorainy, Binsaleh and Almannie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meshari A. Alzahrani, ma.alzahrani@mu.edu.sa
†ORCID: Meshari A. Alzahrani, orcid.org/0000-0002-8504-7486
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.