
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Endocrinol. , 04 October 2023
Sec. Obesity
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1222101
 Chloé Rauzier1,2Dominic J. Chartrand1,3Natalie Alméras1,3
Chloé Rauzier1,2Dominic J. Chartrand1,3Natalie Alméras1,3 Isabelle Lemieux1Eric Larose1,4
Isabelle Lemieux1Eric Larose1,4 Patrick Mathieu1,5Philippe Pibarot1,4
Patrick Mathieu1,5Philippe Pibarot1,4 Benoît Lamarche6,7
Benoît Lamarche6,7 Caroline Rhéaume1,8,9
Caroline Rhéaume1,8,9 Paul Poirier1,2Jean-Pierre Després1,3,9*
Paul Poirier1,2Jean-Pierre Després1,3,9* Frédéric Picard1,2*
Frédéric Picard1,2*Lay summary: Obesity is frequently accompanied by a fatty liver. However, some individuals with high abdominal fat levels nevertheless have low levels of liver fat. Reasons for such discordant phenotypes are unclear. In this paper, we report that among asymptomatic individuals with high levels of visceral fat, low concentrations of IGFBP-2 in the circulation were associated with significantly higher hepatic fat content compared to those with high IGFBP-2 levels. We conclude that quantification of plasma IGFBP-2 concentrations may be useful to identify the early risk for liver fat accumulation in apparently healthy individuals without cardiovascular symptoms.
Aim/hypothesis: Although excess visceral adiposity (VAT) is generally associated with increased liver fat (LF), recent evidence has revealed heterogeneity in LF content among adults with visceral obesity, potentially contributing to specific differences in cardiometabolic outcomes. Reasons for such discordant VAT-LF phenotypes are largely unknown. The present study aimed at assessing whether circulating levels of insulin growth-factor binding protein-2 (IGFBP-2) could be a useful biomarker in the identification of heterogenous and discordant VAT-LF phenotypes.
Methods: A sample of 308 middle-aged Caucasian apparently healthy men and women without cardiovascular symptoms were studied for the present cross-sectional analyses. Fasting plasma glucose and lipid levels were assessed and an oral glucose tolerance test was performed. Hepatic fat fraction (HFF) was measured using magnetic resonance spectroscopy whereas VAT was assessed by magnetic resonance imaging. Plasma IGFBP-2 levels were quantified by ELISA. Participants were then classified on the basis of median VAT (81 mL) and IGFBP-2 levels (233 ng/mL).
Results: Individuals with high levels of VAT were characterized by higher waist circumference, lower insulin sensitivity, as well as by higher plasma triglyceride and lower HDL-cholesterol levels. Plasma IGFBP-2 levels were inversely correlated with HFF (r = -0.39, p < 0.0001). Among men and women with high levels of VAT, those with low levels of IGFBP-2 had significantly higher HFF (7.5 ± 0.7%), compared to participants with high IGFBP-2 concentrations (3.2 ± 0.5%, p < 0.0001).
Conclusion: In the presence of excess VAT, high IGFBP-2 concentrations are associated with low levels of LF. Although additional studies will be necessary to establish causality and further clarify the clinical implications of these observations, these findings are concordant with a novel function of IGFBP-2 in modulating susceptibility to non-alcoholic fatty liver disease (NAFLD) in the presence of visceral obesity.
Chronic positive energy balance results in excess body fat accumulation, not only in adipose tissue, but also in non-adipose tissue-containing organs, such as the liver. In particular, deposition of lipids in the abdominal region, whether as visceral adipose tissue (VAT) and/or liver fat (LF), has been established as an important factor in the development of cardiometabolic diseases (1). Non-alcoholic fatty liver disease (NAFLD) is diagnosed when hepatic fat fraction (HFF) is higher than 5% (2). Although LF typically develops proportionally as a consequence of dysfunctional subcutaneous adipose tissue also leading to VAT accumulation (3), recent data from large cardiometabolic imaging cohorts have revealed the existence of discordant VAT-LF phenotypes, with individuals having high levels of LF without the presence of excess VAT, or vice versa (4). These discordant phenotypes have also been shown to be associated with different clinical outcomes, with high VAT being mainly linked with cardiovascular disease events independently of LF levels, whereas a high LF content was found to be predictive of an increased risk of type 2 diabetes (T2D) independently of VAT (4). Reasons for such discordant VAT-LF phenotypes are largely unknown.
Insulin like-growth factor binding protein-2 (IGFBP-2) is a pleiotropic circulating factor involved in the modulation of energy metabolism (5). In mice and humans, low plasma levels of IGFBP-2 are associated with higher body weight, adiposity, insulin resistance, and the development of NAFLD (6–8). In this context, we tested the links between plasma IGFBP-2 and LF content associated with variation in VAT in a sample of asymptomatic adult volunteers who were involved in a cardiometabolic imaging study.
The present study reports additional IGFBP-2 data quantified in a previously described cohort of 312 individuals, including details about recruitment of participants and approval by the local institutional review board (#20769) (9). Informed written consent was obtained from all participants prior to their inclusion in the study. Samples were taken and deposited in a biobank for future analyses. The biobank is administered by a management framework. The present specific study has received ethics approval from the local institutional review board (#21433).
Briefly, men and women between 35 and 66 years old were enrolled from the Québec metropolitan area for voluntary participation in the visceral obesity/ectopic fat and non-invasive markers of atherosclerosis: a cardiometabolic-cardiovascular imaging study (CMCV imaging study). Data used in the present analyses are the baseline characteristics of study participants. Data for plasma IGFBP-2 levels were missing for 4 individuals, resulting in a cohort of 308 men and women.
Inclusion criteria for baseline measurements were body mass index (BMI) < 40 kg/m2 and being nonsmoker for at least 12 months before enrollment. Participants presenting symptoms or being treated for cardiovascular disease (including cerebrovascular disease), dyslipidemia, hypertension, and diabetes were excluded. Were also excluded participants undergoing hormonal or corticosteroid therapy, presenting a cancer not in remission or with a contraindication for magnetic resonance imaging (MRI), were on any medication in the past 3 months, as well as women who were in postmenopause for less than 12 months before enrollment.
Weight and waist circumference were measured as described (10). Body composition was quantified by dual-energy X-ray absorptiometry on a Lunar Prodigy system (GE Healthcare, Madison, WI, USA) whereas levels of abdominal subcutaneous adipose tissue (SAT) and VAT were assessed by MRI as previously described (9). HFF was evaluated using magnetic resonance spectroscopy (MRS) by breath-hold single‐shot stimulated echo acquisition mode (STEAM) sequence exactly as described (9). Blood samples were collected from the antecubital vein after a 12-h overnight fast. Circulating triglyceride (TG), total cholesterol, HDL and LDL cholesterol levels were quantified as described (9). Oral glucose tolerance tests (OGTT) were performed in overnight-fasted individuals by ingestion of a 300 ml solution containing 75 g of glucose (9). Plasma glucose and insulin levels were quantified throughout the test, allowing calculation of the total area under their excursion curve (AUC) by the trapezoid method. The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as glucose x insulin/22.5. Plasma IGFBP-2 levels were quantified by ELISA (Alpco kit #22-BP2HU-E01, Salem, NH, USA) according to the manufacturer’s instructions. The detection limit was 0.2 ng/mL. The inter- and intra-assay coefficient of variability was < 10%.
To determine the variation in LF content related to both VAT and IGFBP-2, participants were classified according to their respective medians (above or below) in VAT (81.2 mL) and IGFBP-2 levels (233.4 ng/mL). Differences between these groups were assessed by two-way ANOVA with Bonferroni’s post-hoc test when appropriate. A mediation model was performed with SAS v9.4 (SAS Institute Inc., Cary, NC) to assess potential causal relationships between variations in HFF and the link between IGFBP-2 and VAT. Differences between groups were considered statistically different when p < 0.05. Data analyses were performed using GraphPad Prism v8.1.
Mean age of participants was 50.5 ± 8.6 years with a mean BMI of 26.0 ± 3.8 kg/m2. To test the hypothesis that IGFBP-2 could be related to discordant VAT/LF phenotypes, the study sample was classified on the basis of median VAT volume (81.2 mL) and median circulating IGFBP-2 levels (233.4 ng/mL). Individuals with high VAT were characterized by higher waist circumference and levels of insulin resistance as well as by higher triglyceride and lower HDL-cholesterol levels (Table 1). Individuals with high IGFBP-2 had lower BMI, more favorable indices of plasma glucose-insulin homeostasis, lower TG and higher HDL-cholesterol levels (Table 1).
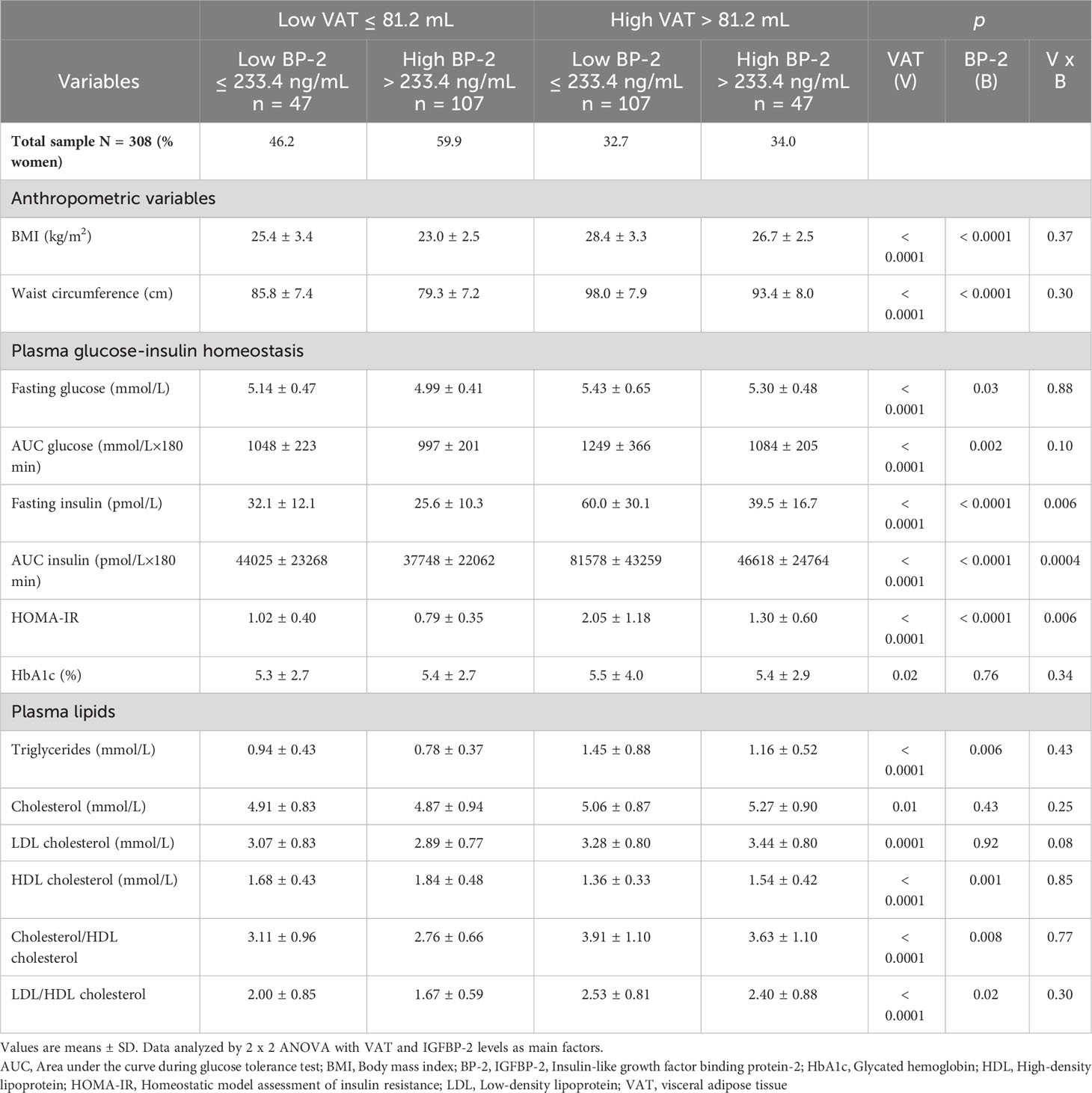
Table 1 Anthropometric, biochemical and cardiometabolic characteristics of a sample of 308 adult participants classified on the basis of their median visceral adiposity (VAT) and median fasting plasma IGFBP-2 concentrations.
Plasma IGFBP-2 concentrations were inversely correlated with HFF (r = -0.39, p < 0.0001). Participants with low levels of VAT had an average HFF of 3.3 ± 0.5% and 1.7 ± 0.1% when IGFBP-2 levels were low or high, respectively (Figure 1). Strikingly, individuals with high VAT levels but low IGFBP-2 levels had a significantly higher HFF (7.5 ± 0.7%) compared to those with high IGFBP-2 concentrations (3.2 ± 0.5%, p < 0.0001, Figure 1). This statistically significant interaction between VAT and IGFBP-2 as main factors for HFF (p = 0.0246) was also observed for variables linked to insulin sensitivity (fasting insulin, AUC insulin, HOMA-IR) but not with waist circumference nor with plasma lipids (Table 1). Mediation analyzes revealed that the variation in HFF could be explained by up to 42.8% through the relationship between IGFBP-2 and VAT.
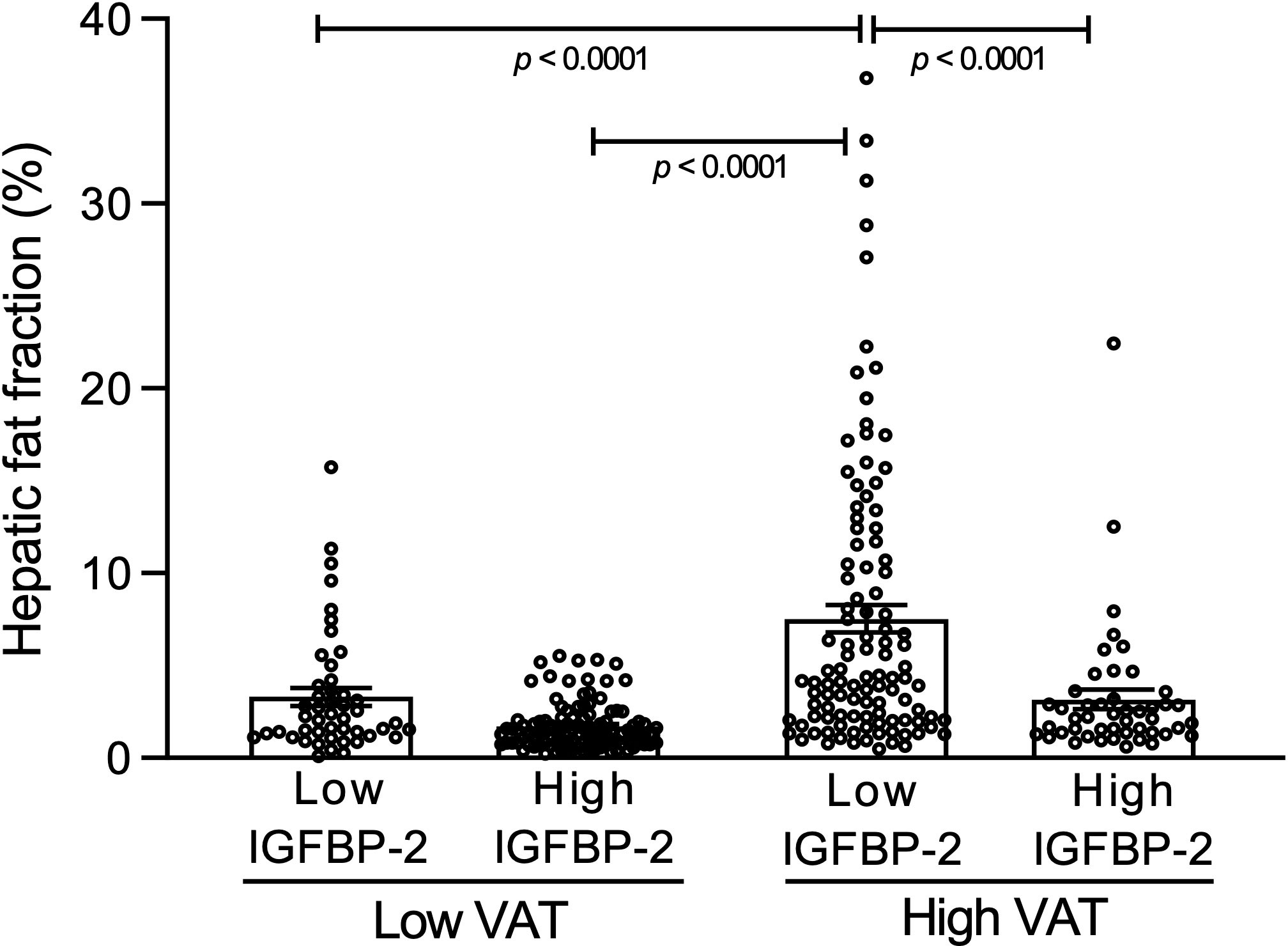
Figure 1 Hepatic fat fraction in a sample of 308 adult participants classified on the basis of their median visceral adipose tissue (VAT) (81.2 mL) and median fasting plasma IGFBP-2 concentrations (233.4 ng/mL). Each point represents one individual. Bars represent means ± SEM. p values were analyzed by post-hoc Bonferonni test performed after detecting a significant interaction (p=0.0246) upon 2 x 2 ANOVA with VAT (p<0.0001) and IGFBP-2 levels (p<0.0001) as main factors for hepatic fat fraction.
Results of this study show that in the presence of high levels of VAT, low circulating levels of IGFBP-2 are associated with the highest levels of LF. This novel finding is highly relevant because to the best of our knowledge no metabolic biomarker has yet been shown to convincingly discriminate levels of LF in the presence of visceral obesity (4). For instance, despite the fact that presence of excess VAT is associated with NAFLD at the population level, the two conditions are not always closely associated, resulting in different risks for various clinical outcomes (4). Although many studies have shown associations between IGFBP-2 and NAFLD in obesity (7, 11, 12), the present observations suggest that low plasma IGFBP-2 levels can indicate a higher risk for the development of NAFLD in asymptomatic, apparently healthy individuals with higher VAT. Moreover, in this subgroup, HFF levels were over the 5% threshold considered to indicate early NAFLD (2). In addition, in our study sample, median IGFBP-2 levels (233 ng/mL) were highly similar to the concentration of 220 ng/mL suggested as a cut-off value linked with the NCEP ATP III clinical criteria for the diagnosis of metabolic syndrome (13). However, additional studies conducted in larger and independent cohorts will be required to further validate these findings including thoroughly explore potential sexual dimorphism since it affects both IGFBP-2 and NAFLD (14, 15).
Our results also show robust statistical interactions between IGFBP-2 levels and VAT for indices of plasma glucose-insulin homeostasis, but not for lipid metabolism nor for waist circumference. It is interesting to note that a high LF content was recently shown to be more strongly associated with T2D than VAT (4), and that low IGFBP-2 was recently reported as one of the strongest biomarkers for T2D independently of age and sex (16). Given the established links between insulin resistance and the development of NAFLD (3), it is possible that IGFBP-2 contributes indirectly to a low LF phenotype by enhancing insulin sensitivity despite the presence of visceral obesity. This possibility is hinted by the 57.2% of variation in HFF that remain unexplained by VAT itself. Additional clinical studies using multivariate designs and direct experiments in models with modified IGFBP-2 expression will be needed to test this hypothesis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité d’éthique de l’IUCPQ. The patients/participants provided their written informed consent to participate in this study.
EL, PM, PPi, BL, CRh, PPo, NA, J-PD, FP conceived and designed research project. CRa performed IGFBP-2 quantification. CRa, IL, and DJC analyzed data. CRa, NA, IL, J-PD, and FP interpreted the experimental results. CRa prepared the tables and figures. CRa and FP drafted manuscript. CRa, DJC, IL, NA, J-PD, and FP edited and revised the manuscript. All approved final version of the manuscript.
The CMCV study was supported by the Canadian Institutes of Health Research (CIHR) (MOP-114820) and is a component of a research program supported by a Foundation Scheme Grant (FDN – 167278) from the Canadian Institutes of Health Research awarded to J-PD. This work was supported by operating grants to FP from the CIHR. (PJT-148550) as well as from the IUCPQ Foundation. J-PD is the Scientific Director of the International Chair on Cardiometabolic Risk based at Université Laval. DJC is a recipient of the Frederick Banting & Charles Best Canada Graduate Scholarships-Doctoral Award from the CIHR and of a doctoral training award from the Fonds de recherche du Québec-Santé (FRQS). EL is a Senior Clinical Research Scholar supported by the FRQS and holds the Chair of Research and Innovation in Cardiovascular Imaging at Université Laval. PM holds the FRQS Chair on the Pathobiology of Calcific Aortic Valve Disease. PPi holds the Canada Research Chair in Valvular Heart Disease.
We are very thankful to those dedicated participants whose involvement made this study possible as well as to the research staff for their invaluable help in data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ross R, Neeland IJ, Yamashita S, Shai I, Seidell J, Magni P, et al. Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat Rev Endocrinol (2020) 16(3):177–89. doi: 10.1038/s41574-019-0310-7
2. Friedman SL, Neuschwander-Tetri BA, Rinella M, Sanyal AJ. Mechanisms of NAFLD development and therapeutic strategies. Nat Med (2018) 24(7):908–22. doi: 10.1038/s41591-018-0104-9
3. Mundi MS, Velapati S, Patel J, Kellogg TA, Abu Dayyeh BK, Hurt RT. Evolution of NAFLD and its management. Nutr Clin Pract (2020) 35(1):72–84. doi: 10.1002/ncp.10449
4. Tejani S, McCoy C, Ayers CR, Powell-Wiley TM, Després J-P, Linge J, et al. Cardiometabolic health outcomes associated with discordant visceral and liver fat phenotypes: insights from the dallas heart study and UK biobank. Mayo Clin Proc (2022) 97(2):225–37. doi: 10.1016/j.mayocp.2021.08.021
5. Haywood NJ, Slater TA, Matthews CJ, Wheatcroft SB. The insulin like growth factor and binding protein family: Novel therapeutic targets in obesity & diabetes. Mol Metab (2019) 19:86–96. doi: 10.1016/j.molmet.2018.10.008
6. Chen X, Tang Y, Chen S, Ling W, Wang Q. IGFBP-2 as a biomarker in NAFLD improves hepatic steatosis: an integrated bioinformatics and experimental study. Endocr Connect (2021) 10(10):1315–25. doi: 10.1530/EC-21-0353
7. Yang J, Zhou W, Wu Y, Xu L, Wang Y, Xu Z, et al. Circulating IGFBP-2 levels are inversely associated with the incidence of nonalcoholic fatty liver disease: A cohort study. J Int Med Res (2020) 48(8):300060520935219. doi: 10.1177/0300060520935219
8. Kammel A, Saussenthaler S, Jahnert M, Jonas M, Stirm M, Hoeflich M, et al. Early hypermethylation of hepatic Igfbp2 results in its reduced expression preceding fatty liver in mice. Hum Mol Genet (2016) 25(12):2588–99. doi: 10.1093/hmg/ddw121
9. Chartrand DJ, Larose E, Poirier P, Mathieu P, Alméras N, Pibarot P, et al. Visceral adiposity and liver fat as mediators of the association between cardiorespiratory fitness and plasma glucose-insulin homeostasis. Am J Physiol Endocrinol Metab (2020) 319(3):E548–56. doi: 10.1152/ajpendo.00251.2020
10. Gordon CC, Chumlea WC, Roche AF. Stature, recumbent length, and weight. In: Lohman TG, Roche AF, Martorell R, editors. Anthropometric Standardization Reference Manual. Champaign (IL, USA: Human Kinetics Books (1988). p. 3–8.
11. Ahrens M, Ammerpohl O, von Schonfels W, Kolarova J, Bens S, Itzel T, et al. DNA methylation analysis in nonalcoholic fatty liver disease suggests distinct disease-specific and remodeling signatures after bariatric surgery. Cell Metab (2013) 18(2):296–302. doi: 10.1016/j.cmet.2013.07.004
12. Fahlbusch P, Knebel B, Hörbelt T, Barbosa DM, Nikolic A, Jacob S, et al. Physiological disturbance in fatty liver energy metabolism converges on IGFBP2 abundance and regulation in mice and men. Int J Mol Sci (2020) 21(11):4144. doi: 10.3390/ijms21114144
13. Carter S, Li Z, Lemieux I, Alméras N, Tremblay A, Bergeron J, et al. Circulating IGFBP-2 levels are incrementally linked to correlates of the metabolic syndrome and independently associated with VLDL triglycerides. Atherosclerosis (2014) 237(2):645–51. doi: 10.1016/j.atherosclerosis.2014.09.022
14. Al-Daghri NM, Manousopoulou A, Alokail MS, Yakout S, Alenad A, Garay-Baquero DJ, et al. Sex-specific correlation of IGFBP-2 and IGFBP-3 with vitamin D status in adults with obesity: a cross-sectional serum proteomics study. Nutr Diabetes (2018) 8(1):54. doi: 10.1038/s41387-018-0063-8
15. Lonardo A, Suzuki A. Sexual dimorphism of NAFLD in adults. Focus on clinical aspects and implications for practice and translational research. J Clin Med (2020) 9(5):1278. doi: 10.3390/jcm9051278
Keywords: humans, insulin-like growth factor binding protein-2, visceral adiposity, liver fat, ectopic lipid deposition
Citation: Rauzier C, Chartrand DJ, Alméras N, Lemieux I, Larose E, Mathieu P, Pibarot P, Lamarche B, Rhéaume C, Poirier P, Després J-P and Picard F (2023) Plasma IGFBP-2 levels reveal heterogeneity in hepatic fat content in adults with excess visceral adiposity. Front. Endocrinol. 14:1222101. doi: 10.3389/fendo.2023.1222101
Received: 13 May 2023; Accepted: 05 September 2023;
Published: 04 October 2023.
Edited by:
Ahmad Al-Mrabeh, University of Edinburgh, United KingdomReviewed by:
Ram Prakash Narayanan, University of Liverpool, United KingdomCopyright © 2023 Rauzier, Chartrand, Alméras, Lemieux, Larose, Mathieu, Pibarot, Lamarche, Rhéaume, Poirier, Després and Picard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frédéric Picard, RnJlZGVyaWMuUGljYXJkQGNyaXVjcHEudWxhdmFsLmNh; Jean-Pierre Després, amVhbi1waWVycmUuZGVzcHJlcy5jaXVzc3NjbkBzc3NzLmdvdXYucWMuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.