 Juan R. Ulloque-Badaracco1
Juan R. Ulloque-Badaracco1 Enrique A. Hernandez-Bustamante2,3Esteban A. Alarcon-Braga1
Enrique A. Hernandez-Bustamante2,3Esteban A. Alarcon-Braga1 Ali Al-kassab-Córdova4
Ali Al-kassab-Córdova4 Juan C. Cabrera-Guzmán1
Juan C. Cabrera-Guzmán1 Percy Herrera-Añazco5,6
Percy Herrera-Añazco5,6 Vicente A. Benites-Zapata7*
Vicente A. Benites-Zapata7*- 1Facultad De Ciencias De La Salud, Universidad Peruana De Ciencias Aplicadas, Lima, Peru
- 2Sociedad Científica De Estudiantes De Medicina De La Universidad Nacional De Trujillo, Trujillo, Peru
- 3Grupo Peruano De Investigación Epidemiológica, Unidad Para La Generación y Síntesis De Evidencias En Salud, Universidad San Ignacio De Loyola, Lima, Peru
- 4Centro de Excelencia en Investigaciones Económicas y Sociales en Salud, Universidad San Ignacio de Loyola, Lima, Peru
- 5Universidad Privada Del Norte, Trujillo, Peru
- 6Red Peruana De Salud Colectiva, Lima, Peru
- 7Unidad De Investigación Para La Generación y Síntesis De Evidencias En Salud, Vicerrectorado De Investigación, Universidad San Ignacio De Loyola, Lima, Peru
Background & aims: Metabolic syndrome (MetS) is associated with life-threatening conditions. Several studies have reported an association of vitamin B12, folic acid, or homocysteine (Hcy) levels with MetS. This systematic review and meta-analysis assessed the association of vitamin B12, folic acid, and Hcy levels with MetS.
Methods: PubMed, Scopus, Embase, Ovid/Medline, and Web of Science were searched up to February 13, 2023. Cross-sectional, case-control, or cohort studies were included. A random-effects model was performed using the DerSimonian and Laird method to estimate the between-study variance. Effect measures were expressed as odds ratios (OR) with their corresponding 95% confidence intervals (95% CI). Between-study heterogeneity was evaluated using Cochran’s Q test and the I2 statistic.
Results: Sixty-six articles (n = 87,988 patients) were included. Higher vitamin B12 levels were inversely associated with MetS (OR = 0.87; 95% CI: 0.81–0.93; p < 0.01; I2 = 90%). Higher Hcy levels were associated with MetS (OR = 1.19; 95% CI: 1.14–1.24; p < 0.01; I2 = 90%). Folate levels were not associated with MetS (OR = 0.83; 95% CI: 0.66–1.03; p = 0.09; I2 = 90%).
Conclusion: Higher vitamin B12 levels were inversely associated with MetS, whereas higher Hcy levels were associated with MetS. Studies assessing the pathways underlying this association are required.
1 Introduction
Metabolic syndrome (MetS) refers to a cluster of interrelated, and often coexisting, disorders such as hyperglycemia, dyslipidemia, hypertension, and abdominal obesity, each of which are independently associated with the risk of developing cardiovascular disease, diabetes, stroke, and increased all-cause mortality (1–5). The incidence of MetS is proportional to the incidence of obesity and type 2 diabetes mellitus; however, the prevalence estimates vary according to the criteria used for the definition of MetS (6). Despite this, studies have shown an increase in its prevalence in recent years. For example, the prevalence of MetS increased from 28.23%–37.09% between 1999 and 2018 in the United States (7), and from 40.2% to 56.31% between 2006 and 2018 in Mexico (8).
In recent years, several studies have investigated the factors affecting MetS, such as physical activity and genetic profile (9, 10). Likewise, the role of some dietary elements in the risk of MetS has also been studied. Some studies have found a lower risk of MetS in patients with a higher intake of fiber, magnesium, selenium, or calcium (11–13). Vitamins have also been suggested to play a role in the risk of MetS. Some studies have found that altered levels of vitamin C, vitamin D, and carotenoids are associated with MetS or some of its components (14–17). Likewise, the association between low levels of folate, vitamin B6, and vitamin B12 or increased homocysteine (Hcy) with the risk of MetS was also suggested because their alterations may also trigger various changes involved in its pathogenesis (18). These three elements are interrelated. Folate is an essential nutrient involved in many crucial functions in the body, and its deficiency is related to an increase in serum Hcy levels. Likewise, vitamin B12 is a cofactor in the synthesis of Hcy from methionine; therefore, deficiency of vitamin B12 can lead to hyperhomocysteinemia (19).
Although not always simultaneously, levels of vitamin B12, folate, and Hcy have been shown to be associated with the risk of stroke, thyroid disease, kidney disease, cardiovascular mortality, and general mortality (20–23). Moreover, there is evidence to suggest that modifying the levels of these macromolecules may prevent some of these outcomes (19). Therefore, evidence of the association between the levels of vitamin B12, folate, and Hcy with MetS would open the possibility of exploring the use of these nutrients as a preventive therapy for MetS or its consequences (24, 25).
Although several primary studies have found an association between levels of vitamin B12, folate, or Hcy and MetS, their results have been inconsistent. To the best of our knowledge, the available evidence has not been systematically reported. Therefore, the objective of this research was to perform a systematic literature review and meta-analysis to synthesize the available evidence of the association between the levels of vitamin B12, folic acid, or Hcy and MetS.
2 Methods
2.1 Registration and reporting
This study was conducted in line with the methods recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for reporting the results (26), taking into account the AMSTAR 2 domains (27). A short version of the protocol of this systematic review has been submitted to the International Prospective Register of Systematic Reviews (PROSPERO) [CRD42023402162].
2.2 Search Strategy and databases
The search strategy was aligned with the Peer Review of Electronic Search Strategies (PRESS) Checklist (28). It was based on using MeSH, Emtree, and free terms. Subsequently, the search formula was adapted for all databases with no restrictions for date or language. The systematic search was simultaneously run from inception through February 13, 2023, in the following databases: PubMed, Scopus, Embase, Ovid/Medline, and Web of Science. The complete search strategy is presented as Supplementary Material (Table S1).
2.3 Study eligibility criteria and data extraction
Cross-sectional, case-control, or cohort studies assessing the associations between vitamin B12, folate, or Hcy and MetS were included. Narrative reviews, scoping reviews, systematic reviews, and conference abstracts were excluded. Four authors independently performed all phases of the study-selection process. All retrieved references were exported from databases to Rayyan© (29). After eliminating duplicate records, four researchers (J.R.U-B, E.A.H-B, E.A.A-B, and J.C.C-G) independently screened the titles and abstracts of each article. After identifying the potential eligible references, the same researchers independently assessed the full-text version of each article. Discrepancies were resolved by consensus. The data extraction was independently performed by this authors using a standardized data extraction sheet built in Google Sheets©. Thereafter, the following information was extracted: first author, publication date, study location, sample size, age, sex, MetS proportion, MetS diagnostic criteria, folate levels (ng/mL), vitamin B12 levels (pg/mL), Hcy levels (µmol/L), and assay methods. The outcome was the association between these markers and MetS.
2.4 Risk of bias and publication bias
The quality assessment was independently conducted by two authors (J.R.U-B and A.A-C) using the Newcastle-Ottawa Scale (NOS) for cohort and case-control studies (30), and an adaptation of the NOS for cross-sectional studies (NOS-CS). A score ≥7 stars was considered indicative of a low risk of bias, whereas a score <7 stars was considered indicative of a high risk of bias. Publication bias was assessed using funnel plots, the Begg test, and the trim-and-fill method (31, 32).
2.5 Data synthesis
The statistical analysis was performed using STATA 17.0© (Stata Corporation, College Station, TX, USA) and Review Manager v.5.4 (The Cochrane Collaboration, Copenhagen, Denmark). A random-effects model was performed using the DerSimonian and Laird method to estimate the between-study variance. Effect measures were only expressed as odds ratios (OR) with their corresponding 95% confidence intervals (95% CI). Thus, any other measure of effect was transformed into OR. Medians and their interquartile ranges were transformed into means and their corresponding standard deviations using Hozo’s method (33). Chinn’s method was used to transform standard mean differences to their corresponding natural logarithm of the OR (lnOR) and its standard error (34). Between-study heterogeneity was evaluated using Cochran’s Q test and the I2 statistic. High heterogeneity was defined as I2 ≥ 60% and a p-value < 0.05 in Cochran’s Q test. To identify sources of heterogeneity, subgroup analyses were performed disaggregated by continents, MetS diagnostic criteria, assay method, and sex. In addition, a sensitivity analysis using only studies with a low risk of bias was performed.
3 Results
3.1 Study selection
The systematic literature search yielded 2,852 records, of which 1,597 were eliminated due to duplication. After screening out articles by abstract-title and full-texts based on the inclusion criteria, 66 articles were identified as eligible for this systematic review and meta-analysis (18, 35–97). A schematic illustration of the literature search and selection is shown in Figure 1.
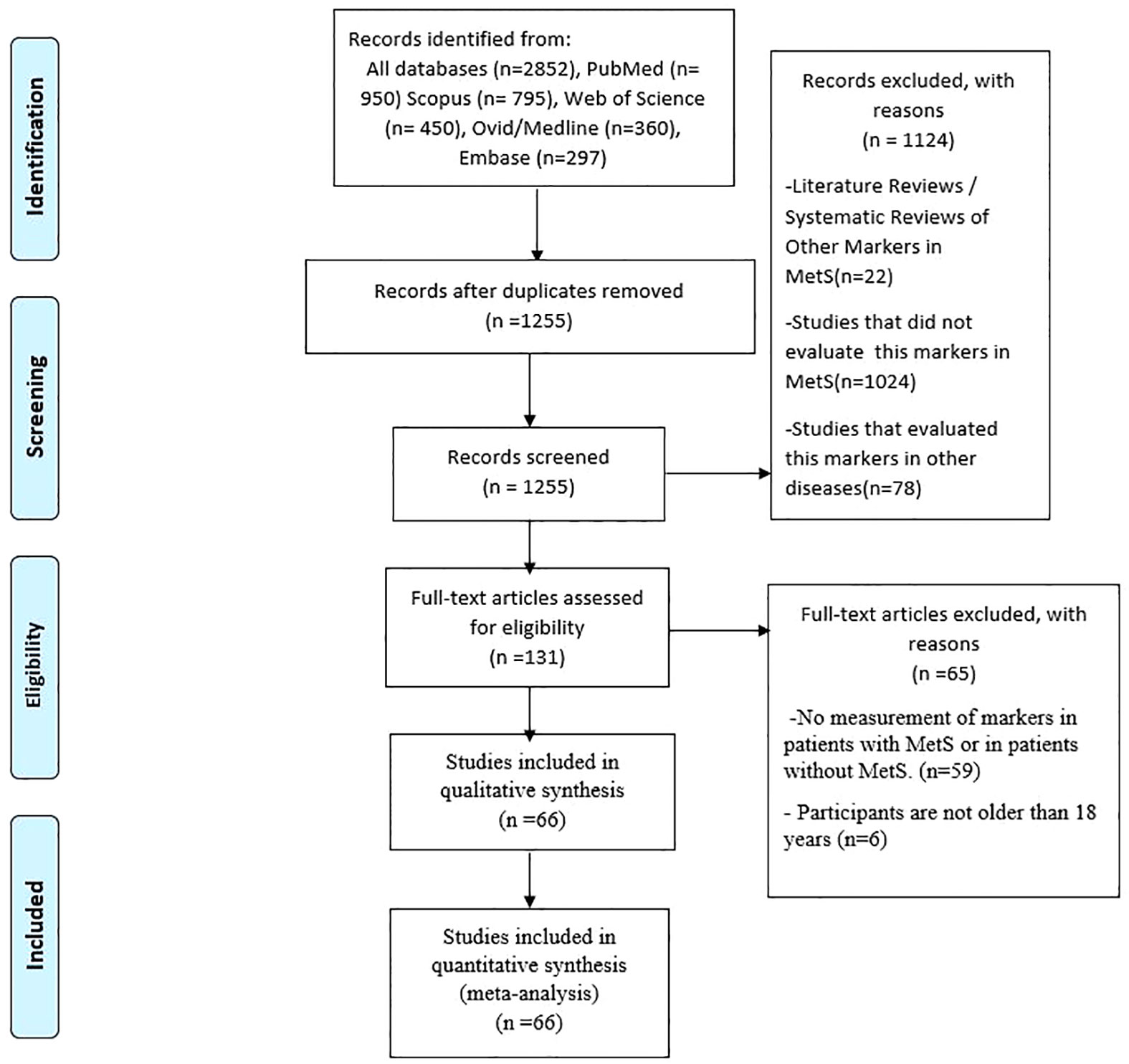
Figure 1 PRISMA Flow Diagram.
3.2 Study characteristics
A total of 66 articles were included, including 9 cohort studies, 48 cross-sectional studies, and 13 case-controls. As four articles (41, 51, 60, 68) had analyzed the association in two different groups of participants each, a total of 70 records were included. The geographic distribution was as follows: China (11 articles), South Korea (9 articles), Turkey (7 articles), United States (6 articles), Italy (3 articles), Iran (3 articles), India (3 articles), Serbia (2 articles), Bangladesh (2 articles), France (2 articles), Saudi Arabia (2 articles), Spain (1 article), Ecuador (1 article), Netherlands (1 article), Canada (1 article), Taiwan (1 article), Australia (1 article), Romania (1 article), Trinidad & Tobago (1 article), Nigeria (1 article), Poland (1 article), Greece (1 article), South Africa (1 article), Slovenia (1 article), Cameroon (1 article), Peru (1 article), and multiple Mesoamerican countries (1 article). A total of 87,988 patients (42,279 male and 35,727 female) were evaluated. Six studies (n = 9,982) did not report the sex of the included participants. These characteristics are summarized in Supplementary Table S2.
The criteria for diagnosing MetS in the included studies were those recommended by the American Heart Association/National Heart Lung and Blood Institute (AHA/NHLBI) (98), Chinese Diabetes Society (CDS) (99), National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP III) (100), International Diabetes Federation (IDF) (101), and the World Health Organization (WHO 1999) (102). The definitions of MetS used for each criterion are presented in Supplementary Table S3.
The methods used to measure Hcy, vitamin B12, and folate levels were chemiluminescence immunoassay (CLIA), electrochemiluminescence immunoassay (ECLIA), enzyme-linked immunosorbent assay (ELISA), fluorescence polarization immunoassay (FPI), high-performance liquid chromatography (HPLC), nephelometry immunoassay, radioimmunoassay, homogeneous enzyme immunoassay, and competitive displacement assay.
After the risk of bias assessment using the NOS, a total of 63 studies were classified as low risk of bias, and 7 studies as high risk of bias (Supplementary Table S4).
3.3 Association between vitamin B12 levels and MetS
This association was evaluated in 22 studies involving a total of 15,115 participants. Higher vitamin B12 levels were inversely associated with MetS (OR = 0.87; 95% CI: 0.81–0.93; p < 0.01; I2 = 90%) (Figure 2). Subgroup analyses were performed according to continents (Supplementary Figure S1), sex (Supplementary Figure S2), assay method (Supplementary Figure S3), and MetS diagnostic criteria (Supplementary Figure S4). Studies conducted in Asian countries (OR = 0.37; 95% CI: 0.22–0.64; p < 0.01; I2 = 95%), those using ECLIA to measure B12 levels (OR = 0.15; 95% CI: 0.02–0.85; p < 0.01; I2 = 97%), and those using the AHA/NHLBI criteria for MetS diagnosis (OR = 0.25; 95% CI: 0.09–0.72; p < 0.01; I2 = 96%) showed a consistent association with no decrease in heterogeneity. In the sensitivity analysis (Supplementary Figure S5), after eliminating studies at high risk of bias, the association persisted (OR = 0.62; 95% CI: 0.48–0.79; p < 0.01) and heterogeneity was high (I2 = 92%).
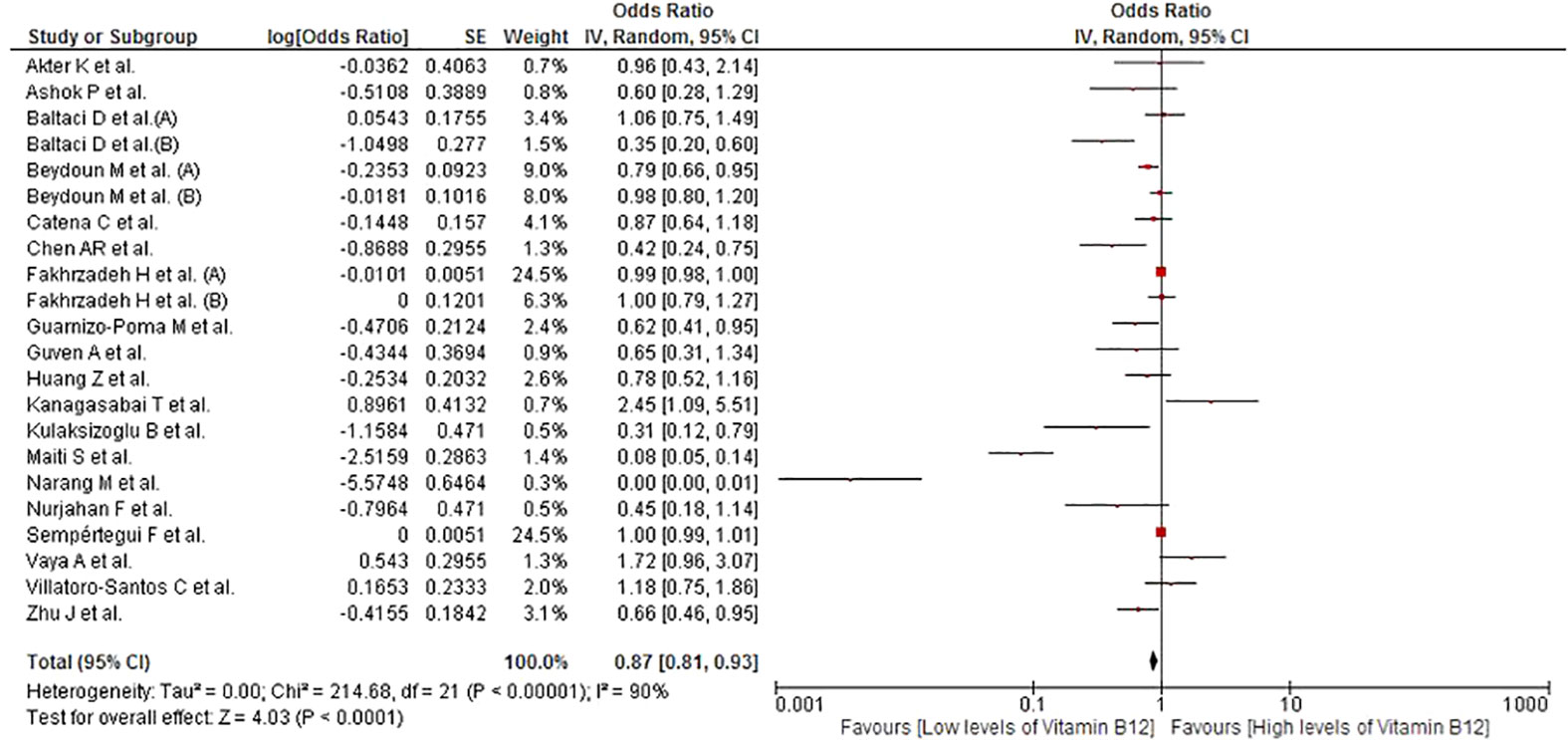
Figure 2 Association between vitamin B12 and MetS.
3.4 Association between folate levels and MetS
This association was evaluated in 20 studies involving a total of 15,869 participants. No significant association was found between folate levels and MetS (OR = 0.83; 95% CI: 0.66–1.03; p = 0.09; I2 = 90%) (Figure 3). Given the high heterogeneity, subgroup analyses by continent (Supplementary Figure S6), sex (Supplementary Figure S7), assay method (Supplementary Figure S8), and MetS diagnostic criteria (Supplementary Figure S9) were performed. In the subgroup of women, higher folate levels were significantly associated with the risk of MetS (OR = 1.35; 95% CI: 1.13–1.60; p < 0.01; I2 = 5%). In the subgroup of AHA/NHLBI diagnostic criteria, higher folate levels were inversely associated with MetS (OR = 0.36; 95% CI: 0.16–0.81; p = 0.01; I2 = 96%). In the sensitivity analysis (Supplementary Figure S10), after removing studies at high risk of bias, there was no significant association and the heterogeneity remained high (OR = 0.78; 95% CI: 0.59–1.03; p = 0.08; I2 = 92%).
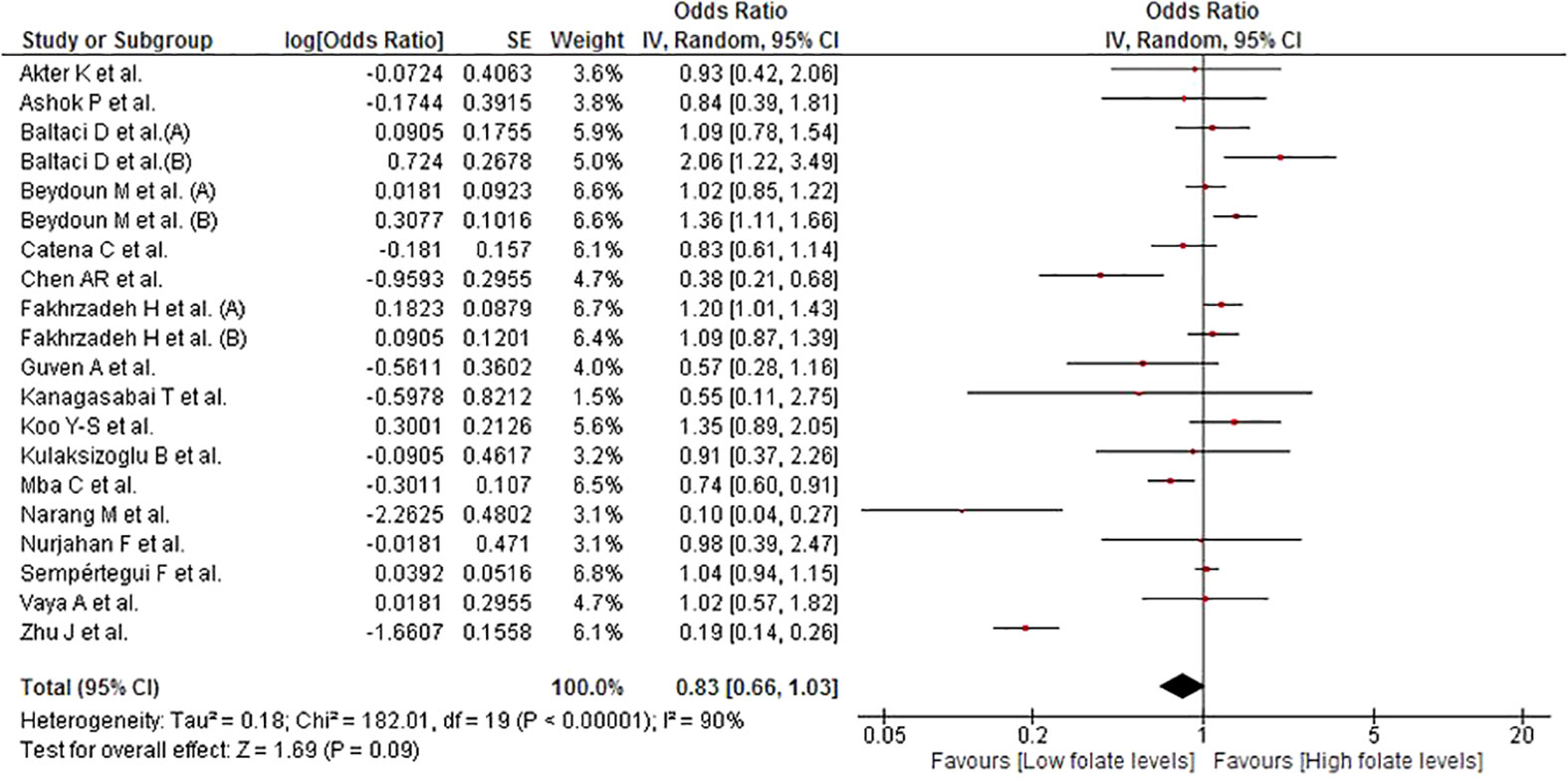
Figure 3 Association between folate and MetS.
3.5 Association between homocysteine levels and MetS
This association was evaluated in 61 studies involving a total of 81,888 participants. Higher Hcy levels were associated with MetS (OR = 1.19; 95% CI: 1.14–1.24; p < 0.01; I2 = 90%) (Figure 4). Owing to the high heterogeneity, subgroup analysis according to continents (Supplementary Figure S11), sex (Supplementary Figure S12), assay method (Supplementary Figure S13), and MetS diagnostic criteria (Supplementary Figure S14) were conducted. All the subgroups exhibited statistically significant associations, except for the subgroup that used the HPLC method to quantify the Hcy levels. On sensitivity analysis (Supplementary Figure S15), the association remained significant after eliminating the studies at high risk of bias (OR = 1.21; 95% CI: 1.16–1.26; p < 0.01); yet, there was high heterogeneity (I2 = 90%).

Figure 4 Association between homocysteine and Mets.
3.6 Publication bias
Begg test revealed no significant influence of publication bias on the association of vitamin B12 and folate with MetS (Begg test <0.1). Nonetheless, the association between Hcy and MetS was corrected using the trim-and-fill method (OR = 1.031; 95% CI: 1.025–1.036) (Supplementary Figure S16).
4 Discussion
This systematic review and subsequent meta-analysis separately evaluated the association between vitamin B12, folate, or Hcy level and MetS. Higher vitamin B12 levels were inversely associated with MetS. Contrarily, higher Hcy levels were associated with MetS. The first association was driven mostly by studies from the Asian continent, while the latter showed no differences in the subgroup analyses. On the other hand, there was no association between folate levels and MetS; however, on subgroup analysis, folate levels showed an association with MetS in women. Overall, this systematic review and meta-analysis may facilitate an in-depth understanding of these associations.
The interaction between vitamin B12 and MetS is complex and not completely understood. Studies have shown that deficiency of folate, vitamin B6, and vitamin B12 can cause dyslipidemia, vascular endothelial dysfunction, glucose intolerance, and insulin resistance through oxidative stress (18). Their deficiency leads to systemic inflammation and impaired nitric oxide synthesis, all of which are implicated in the pathophysiology of MetS (18). Vitamin B12 is an essential hydrosoluble vitamin that plays an important role in DNA methylation as well as amino acid and lipid homeostasis through the regulation of one-carbon metabolism (25). Low levels of vitamin B12 can interfere with DNA synthesis and cellular inflammation, and increase fat and Hcy synthesis (25).
An increase in the binding of vitamin B12 to haptocorrins secondary to their increased plasma levels, especially for transcobalamin (TCB) I and III, which are the main haptocorrins, leads to a potential decline in their attachment to TCB II and, therefore, alters their delivery to cells (103). This phenomenon can cause a functional vitamin B12 deficiency with an increase in Hcy and/or methylmalonic acid levels, even though the initial abnormality is not a vitamin B12 deficiency (103). This is relevant, since vitamin B12 is essential for facilitating energy, lipid, and carbohydrate metabolism in humans, mainly by counteracting hyperhomocysteinemia (18, 104).
Mammalian cells exhibit two different vitamin B12-dependent reactions: the conversion of methylmalonyl coenzyme A to succinyl coenzyme and the methylation of Hcy to methionine (25). Therefore, vitamin B12 deficiency results in elevated serum levels of Hcy and methylmalonic acid, which serve as biochemical markers of vitamin B12 status. Therefore, methylmalonic acid accumulates in patients with B12 deficiency, which is associated with lipogenesis and insulin resistance (25). Although there are multiple pathogenic mechanisms of MetS, insulin resistance is one of the most important underlying causes.
The underlying mechanism of the association between insulin resistance and the MetS is not fully understood, but some metabolic pathways have been proposed. Insulin resistance causes an increase in circulating glucose leading to increased insulin secretion (25). Consequently, glucose transporter types 1-3 (GLUT1-3), which are insulin-independent and found in neurons, renal cells, and red blood cells, are exposed to large amounts of glucose, leading to glucotoxicity (105). Persistent insulin resistance exhausts the ability of pancreatic beta cells to provide the required amounts of insulin, further disrupting glucose homeostasis (106). Additionally, there is an increase in the synthesis of triglycerides and very low-density lipoproteins that contribute to the failure of the GLUT4 transporter (106, 107). According to the portal theory of MetS, free fatty acids are released from the accumulated visceral fat (25). These free fatty acids affect the activity of phosphoinositide-3-kinase, reducing its function and aggravating insulin resistance (106). In addition, they contribute to endothelial damage by producing reactive oxygen species, along with the hyperinsulinemia state and cytokines produced by adipose tissue (25).
Despite this plausibility, there are discrepancies on whether levels of vitamin B12 or a diet rich in vitamin B12 reduce the risk of MetS as opposed to other components of the vitamin B complex. These discrepancies may be partially attributable to differences between the studies with respect to methodology, clinical features, and ethnic composition of the study population (18). Although this study does not solve these questions, it provides evidence of the potential linkage between vitamin B12 levels and MetS (18). Therefore, randomized studies assessing the potential beneficial effect of vitamin B12 supplementation are needed. Long-term vitamin B12 supplementation has been shown to reduce weight gain in overweight or obese people (19). In the present study, a stronger association was observed in the studies conducted in the Asian continent, which suggests that ethnic, dietetic, or genetic factors may influence this association (108, 109). Hence, future studies should control for these potential effect modifiers. It is necessary to emphasize that a large percentage of studies included in this review were conducted in Asian countries, where deficiencies of other micronutrients, such as vitamin A or D, have also been described (110, 111). These micronutrient deficiencies were also shown to be associated with MetS (112, 113). Thus, our systematic review does not allow us to discern whether our findings, despite being biologically plausible, are independent of these associations.
We observed no association between endogenous folate levels and MetS, which is not consistent with some studies of folate supplementation. Nevertheless, in the subgroup analysis by sex, folate deficiency showed an association with MetS among women. Sex-based differences in the effect of progression of metabolic risk factors on the development of diabetes have been reported (114). Further studies are required to unravel the underlying causes of this difference. On the other hand, folic acid supplementation has been shown toimprove clinical and laboratory outcomes. In a randomized clinical trial enrolling obese women with polycystic ovary syndrome, folic acid supplementation improved metabolic profiles (115). Similarly, in another trial, both men and women exhibited improved insulin resistance and endothelial dysfunction as well as decreasing Hcy levels after treatment with folic acid and vitamin B12 (116). A systematic review of randomized trials found beneficial effects of folic acid on inflammatory markers–such as hs-CRP, IL-6, and TNF-α–in patients with MetS. Indeed, low levels of folate, like vitamin B12, can interfere with DNA synthesis, increase cellular inflammation, and elevate fat and Hcy synthesis (25).
Several studies have documented the association between Hcy and MetS (62, 64), and Hcy has even been proposed as a marker (40). Increased levels of Hcy were shown to be associated with cardiovascular death (64), stroke (117), and obesity (118). Nonetheless, it is important to note that the high levels of Hcy in patients with MetS could be iatrogenic, as most hypolipidemic, antidiabetic, and antihypertensive drugs raise circulating Hcy levels (119). The biological plausibility of these associations relies on various biological effects secondary to hyperhomocysteinemia, such as vascular damage, oxidative stress-induced DNA damage, neuronal apoptosis, cellular cytotoxicity, and endothelial nitric oxide production, which could trigger MetS (55, 120). Moreover, since Hcy metabolism is regulated by vitamin B6, folate, and vitamin B12, the effect of Hcy may also be partly mediated by variations in these vitamins (19). On the other hand, the reported sex-based differences are not fully understood but some authors hypothesize that estrogen status is inversely associated with total circulating Hcy level, independent of nutritional status and muscle mass (121). Dietary factors may also explain the differences reported in subgroup analysis by continent (122).
The differences in the levels of the macromolecules studied suggest the potential therapeutic role of supplementation of these macromolecules. Several clinical trials and observational studies have studied folic acid and vitamin B12 supplementation for the management of MetS and control of Hcy levels (18, 123, 124), as well as other cardiovascular outcomes (115, 125), with apparently positive results. Thus, this evidence needs to be synthesized in future studies.
4.1 Limitations
Some limitations of this study should be considered while interpreting the findings. First, the lack of data prevented a meta-analysis of the sensitivity, specificity, and optimal cut-off points of these variables. Moreover, we did not compare the pooled mean levels of the macromolecules between participants with and without MetS. Second, high statistical heterogeneity was found due to methodological and clinical differences between studies, which only decreased in some subgroups. Third, the studies had not adjusted the marker levels for potential confounding factors, such as lifestyle, diet quality, sociodemographic conditions, and comorbidities. Given the observational nature of the included studies, the study findings should be interpreted as exploratory. Fourth, a large proportion of studies included in our meta-analysis were conducted in Asia; thus, it would be worthwhile to conduct further research on this topic in other geographic regions. Fifth, given that most of the included studies were of cross-sectional design and the nature of the exposure and outcome variable, there is a risk of retro-causality. Nonetheless, this study has several strengths. A large number of studies and participants were included. Moreover, several subgroups were analyzed. To the best of our knowledge, this is the first systematic review and meta-analysis assessing the association between vitamin B12, Hcy, or folate and MetS.
5 Conclusion
Higher vitamin B12 levels were inversely associated with MetS. Further studies are required to assess the pathways underlying this association.
Author contributions
JU-B: Conceptualization, Methodology, Investigation, Formal analysis, and Writing - Original Draft. EH-B: Methodology, Investigation, Formal analysis, and Writing - Original Draft. EA-B: Methodology, Investigation, Formal analysis, and Writing - Original Draft. AA-k-C: Methodology, Investigation, Formal analysis, and Writing - Original Draft. JC-G: Methodology, Investigation, Formal analysis, and Writing - Original Draft. PH-A: Investigation, Writing - Original Draft, Visualization and Supervision. VB-Z: Conceptualization, Methodology, Writing - Review & Editing, Visualization, and Supervision. All authors contributed to the article and approved the submitted version.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1221259/full#supplementary-material
References
1. Eckel RH, Alberti KG, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet (2010) 375(9710):181–3. doi: 10.1016/S0140-6736(09)61794-3
2. Mongraw-Chaffin M, Foster MC, Anderson CAM, Burke GL, Haq N, Kalyani RR, et al. Metabolically healthy obesity, transition to metabolic syndrome, and cardiovascular risk. J Am Coll Cardiol (2018) 71(17):1857–65. doi: 10.1016/j.jacc.2018.02.055
3. Zhang F, Liu L, Zhang C, Ji S, Mei Z, Li T. Association of metabolic syndrome and its components with risk of stroke recurrence and mortality: A meta-analysis. Neurology (2021) 97(7):e695–705. doi: 10.1212/WNL.0000000000012415
4. Ulloque-Badaracco JR, Hernandez-Bustamante EA, Alarcon-Braga EA, Mosquera-Rojas MD, Campos-Aspajo A, Salazar-Valdivia FE, et al. Atherogenic index of plasma and coronary artery disease: A systematic review. Open Med (Wars) (2022) 17(1):1915–26. doi: 10.1515/med-2022-0590
5. Wu SH, Liu Z, Ho SC. Metabolic syndrome and all-cause mortality: a meta-analysis of prospective cohort studies. Eur J Epidemiol (2010) 25(6):375–84. doi: 10.1007/s10654-010-9459-z
6. Fahed G, Aoun L, Bou Zerdan M, Allam S, Bou Zerdan M, Bouferraa Y, et al. Metabolic syndrome: updates on pathophysiology and management in 2021. Int J Mol Sci (2022) 23(2):786. doi: 10.3390/ijms23020786
7. Yang C, Jia X, Wang Y, Fan J, Zhao C, Yang Y, et al. Trends and influence factors in the prevalence, intervention, and control of metabolic syndrome among US adults, 1999-2018. BMC Geriatr (2022) 22(1):979. doi: 10.1186/s12877-022-03672-6
8. Rojas-Martínez R, Aguilar-Salinas CA, Romero-Martínez M, Castro-Porras L, Gómez-Velasco D, Mehta R. Trends in the prevalence of metabolic syndrome and its components in Mexican adults, 2006-2018. Salud Publica Mex (2021) 63(6, Nov-Dic):713–24. doi: 10.21149/12835
9. Stančáková A, Laakso M. Genetics of metabolic syndrome. Rev Endocr Metab Disord (2014) 15(4):243–52. doi: 10.1007/s11154-014-9293-9
10. Zhang D, Liu X, Liu Y, Sun X, Wang B, Ren Y, et al. Leisure-time physical activity and incident metabolic syndrome: a systematic review and dose-response meta-analysis of cohort studies. Metabolism (2017) 75:36–44. doi: 10.1016/j.metabol.2017.08.001
11. Dibaba DT, Xun P, Fly AD, Yokota K, He K. Dietary magnesium intake and risk of metabolic syndrome: a meta-analysis. Diabetes Med (2014) 31(11):1301–9. doi: 10.1111/dme.12537
12. Ju SY, Choi WS, Ock SM, Kim CM, Kim DH. Dietary magnesium intake and metabolic syndrome in the adult population: dose-response meta-analysis and meta-regression. Nutrients (2014) 6(12):6005–19. doi: 10.3390/nu6126005
13. Wei B, Liu Y, Lin X, Fang Y, Cui J, Wan J. Dietary fiber intake and risk of metabolic syndrome: A meta-analysis of observational studies. Clin Nutr (2018) 37(6(A)):1935–42. doi: 10.1016/j.clnu.2017.10.019
14. Guo H, Ding J, Liu Q, Li Y, Liang J, Zhang Y. Vitamin C and metabolic syndrome: A meta-analysis of observational studies. Front Nutr (2021) 8:728880. doi: 10.3389/fnut.2021.728880
15. Theik NWY, Raji OE, Shenwai P, Shah R, Kalluri SR, Bhutta TH, et al. Relationship and effects of vitamin D on metabolic syndrome: A systematic review. Cureus (2021) 13(8):e17419. doi: 10.7759/cureus.17419
16. Beydoun MA, Chen X, Jha K, Beydoun HA, Zonderman AB, Canas JA. Carotenoids, vitamin A, and their association with the metabolic syndrome: a systematic review and meta-analysis. Nutr Rev (2019) 77(1):32–45. doi: 10.1093/nutrit/nuy044
17. Ulloque-Badaracco JR, Al-Kassab-Córdova A, Hernandez-Bustamante EA, Alarcon-Braga EA, Huayta-Cortez M, Carballo-Tello XL, et al. Association of apolipoproteins and lipoprotein(a) with metabolic syndrome: a systematic review and meta-analysis. Lipids Health Dis (2023) 22(1):98. doi: 10.1186/s12944-023-01860-w
18. Zhu J, Chen C, Lu L, Shikany JM, D’Alton ME, Kahe K. Folate, vitamin B6, and vitamin B12 status in association with metabolic syndrome incidence. JAMA Netw Open (2023) 6(1):e2250621. doi: 10.1001/jamanetworkopen.2022.50621
19. Thomas-Valdés S, Tostes MDGV, Anunciação PC, da Silva BP, Sant’Ana HMP. Association between vitamin deficiency and metabolic disorders related to obesity. Crit Rev Food Sci Nutr (2017) 57(15):3332–43. doi: 10.1080/10408398.2015.1117413
20. Benites-Zapata VA, Ignacio-Cconchoy FL, Ulloque-Badaracco JR, Hernandez-Bustamante EA, Alarcón-Braga EA, Al-Kassab-Córdova A, et al. Vitamin B12 levels in thyroid disorders: A systematic review and meta-analysis. Front Endocrinol (2023) 14:1070592. doi: 10.3389/fendo.2023.1070592
21. Yahn GB, Abato JE, Jadavji NM. Role of vitamin B12 deficiency in ischemic stroke risk and outcome. Neural Regener Res (2021) 16(3):470–4. doi: 10.4103/1673-5374.291381
22. Katsimardou A, Stavropoulos K, Imprialos K, Doumas M, Athyros VG. Hypertension and hyperhomocysteinemia as risk factors for chronic kidney disease: A dangerous duo? J Clin Hypertens (Greenwich) (2019) 21(10):1578–9. doi: 10.1111/jch.13676
23. Wolffenbuttel BHR, Heiner-Fokkema MR, Green R, Gans ROB. Relationship between serum B12 concentrations and mortality: experience in NHANES. BMC Med (2020) 18(1):307. doi: 10.1186/s12916-020-01771-y
24. Wu Y, Li S, Wang W, Zhang D. Associations of dietary vitamin B1, vitamin B2, niacin, vitamin B6, vitamin B12 and folate equivalent intakes with metabolic syndrome. Int J Food Sci Nutr (2020) 71(6):738–49. doi: 10.1080/09637486.2020.1719390
25. Ashok T, Puttam H, Tarnate VCA, Jhaveri S, Avanthika C, Trejo Treviño AG, et al. Role of vitamin B12 and folate in metabolic syndrome. Cureus (2021) 13(10):e18521. doi: 10.7759/cureus.18521
26. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ (2009) 339:b2700. doi: 10.1136/bmj.b2700
27. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ (2017) 358:j4008. doi: 10.1136/bmj.j4008
28. McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol (2016) 75:40–6. doi: 10.1016/j.jclinepi.2016.01.021
29. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app forsystematic reviews. Syst Rev (2016) 5(1):210. doi: 10.1186/s13643-016-0384-4
30. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2021). Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
31. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics (1994) 50(4):1088–101. doi: 10.2307/2533446
32. Duval S, Tweedie R. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. J Am Stat Assoc (2000) 95(449):89–98. doi: 10.1080/01621459.2000.10473905
33. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol (2005) 5(1):13. doi: 10.1186/1471-2288-5-13
34. Chinn S. A simple method for converting an odds ratio to effect size for use in meta-analysis. Stat Med (2000) 19(22):3127–31. doi: 10.1002/1097-0258(20001130)19:22%3C3127::AID-SIM784%3E3.0.CO;2-M
35. Narang M, Singh M, Dange S. Serum homocysteine, vitamin B12 and folic acid levels in patients with metabolic syndrome. J Assoc Physicians India (2016) 64(7):22–6.
36. Guven A, Inanc F, Kilinc M, Ekerbicer H. Plasma homocysteine and lipoprotein (a) levels in Turkish patients with metabolic syndrome. Heart Vessels (2005) 20(6):290–5. doi: 10.1007/s00380-004-0822-4
37. Catena C, Colussi G, Nait F, Capobianco F, Sechi LA. Elevated homocysteine levels are associated with the metabolic syndrome and cardiovascular events in hypertensive patients. Am J Hypertens (2015) 28(7):943–50. doi: 10.1093/ajh/hpu248
38. Vayá A, Carmona P, Badia N, Pérez R, Hernandez Mijares A, Corella D. Homocysteine levels and the metabolic syndrome in a Mediterranean population: a case-control study. Clin Hemorheol Microcirc (2011) 47(1):59–66. doi: 10.3233/CH-2010-1366
39. Sempértegui F, Estrella B, Tucker KL, Hamer DH, Narvaez X, Sempértegui M, et al. Metabolic syndrome in the elderly living in marginal peri-urban communities in Quito, Ecuador. Public Health Nutr (2011) 14(5):758–67. doi: 10.1017/S1368980010002636
40. Sreckovic B, Sreckovic VD, Soldatovic I, Colak E, Sumarac-Dumanovic M, Janeski H, et al. Homocysteine is a marker for metabolic syndrome and atherosclerosis. Diabetes Metab Syndr (2017) 11(3):179–82. doi: 10.1016/j.dsx.2016.08.026
41. Loprinzi PD, Cardinal BJ. Interrelationships among physical activity, depression, homocysteine, and metabolic syndrome with special considerations by sex. Prev Med (2012) 54(6):388–92. doi: 10.1016/j.ypmed.2012.03.016
42. Fakhrzadeh H, Mirarefin M, Sharifi F, Ghotbi S, Rezaei Hemami M, Mohammad Amoli M, et al. Association of methylene tetrahydrofolate reductase gene Polymorphism.;C677t with Metabolic Syndrome in an Iranian Population: Tehran Homocysteine Survey. Iran J Diabetes Lipid Disord (2009) 8:37–46.
43. Nurjahan F, Shumi MB, Begum S. Relationship of lung function with homocysteine, vitamin B12 and folic acid level in metabolic syndrome: lung function in metabolic syndrome. Bangladesh Med Res Counc Bull (2022) 47(2):175–80. doi: 10.3329/bmrcb.v47i2.57776
44. Akter K, Akter H, Nurjahan F, Sultana S, Begum S. Vitamin B12, folic acid and homocysteine Levels in female metabolic syndrome patients and their relationship with heart rate variability. J Bangladesh Soc Physiol (2021) 16(1):24–32. doi: 10.3329/jbsp.v16i1.54349
45. Hajer GR, van der Graaf Y, Olijhoek JK, Verhaar MC, Visseren FL. Levels of homocysteine are increased in metabolic syndrome patients but are not associated with an increased cardiovascular risk, in contrast to patients without the metabolic syndrome. Heart (2007) 93(2):216–20. doi: 10.1136/hrt.2006.093971
46. Azarpazhooh MR, Andalibi MSS, Hackam DG, Spence JD. Interaction of smoking, hyperhomocysteinemia, and metabolic syndrome with carotid atherosclerosis: A cross-sectional study in 972 non-diabetic patients. Nutrition (2020) 79-80:110874. doi: 10.1016/j.nut.2020.110874
47. Kang JY, Park IK, Lee JY, Sung SH, Chang YK, Park YK, et al. Use of serum homocysteine to predict cardiovascular disease in Korean men with or without metabolic syndrome. J Korean Med Sci (2012) 27(5):500–5. doi: 10.3346/jkms.2012.27.5.500
48. Wang J, Xu L, Xia H, Li Y, Tang S. Association of MTHFR C677T gene polymorphism with metabolic syndrome in a Chinese population: a case-control study. J Int Med Res (2018) 46(7):2658–69. doi: 10.1177/0300060518768969
49. Fakhrzadeh H, Ebrahimpour P, Pourebrahim R, Heshmat R, Larijani B. Homocysteine levels and its correlation to metabolic syndrome in 25-64 years old residents of the Tehran Medical University Population Lab. ijdld (2004) 4(2):71–8.
50. Srećković B, Soldatovic I, Colak E, Mrdovic I, Sumarac-Dumanovic M, Janeski H, et al. Homocysteine is the confounding factor of metabolic syndrome-confirmed by siMS score. Drug Metab Pers Ther (2018) 33(2):99–103. doi: 10.1515/dmpt-2017-0013
51. Beydoun MA, Shroff MR, Chen X, Beydoun HA, Wang Y, Zonderman AB. Serum antioxidant status is associated with metabolic syndrome among U.S. adults in recent national surveys. J Nutr (2011) 141(5):903–13. doi: 10.3945/jn.110.136580
52. Garcin JM, Cremades S, Garcia-Hejl C, Bordier L, Dupuy O, Mayaudon H, et al. Is hyperhomocysteinemia an additional risk factor of the metabolic syndrome? Metab Syndr Relat Disord (2006) 4(3):185–95. doi: 10.1089/met.2006.4.185
53. Nabipour I, Ebrahimi A, Jafari SM, Vahdat K, Assadi M, Movahed A, et al. The metabolic syndrome is not associated with homocysteinemia: the Persian Gulf Healthy Heart Study. J Endocrinol Invest (2009) 32(5):406–10. doi: 10.1007/BF03346476
54. Wang X, Ye P, Cao R, Yang X, Xiao W, Zhang Y, et al. The association of homocysteine with metabolic syndrome in a community-dwelling population: homocysteine might be concomitant with metabolic syndrome. PloS One (2014) 9(11):e113148. doi: 10.1371/journal.pone.0113148
55. Lee HS, In S, Park T. The homocysteine and metabolic syndrome: A Mendelian randomization study. Nutrients (2021) 13(7):2440. doi: 10.3390/nu13072440
56. Rhee EJ, Hwang ST, Lee WY, Yoon JH, Kim BJ, Kim BS, et al. Relationship between metabolic syndrome categorized by newly recommended by International Diabetes Federation criteria with plasma homocysteine concentration. Endocr J (2007) 54(6):995–1002. doi: 10.1507/endocrj.k07e-018
57. Balcioğlu AS, Durakoğlugil ME, Ciçek D, Bal UA, Boyaci B, Müderrisoğlu H. Epicardial adipose tissue thickness and plasma homocysteine in patients with metabolic syndrome and normal coronary arteries. Diabetol Metab Syndr (2014) 6:62. doi: 10.1186/1758-5996-6-62
58. Shih YL, Shih CC, Huang TC, Chen JY. The relationship between elevated homocysteine and metabolic syndrome in a community-dwelling middle-aged and elderly population in Taiwan. Biomedicines (2023) 11(2):378. doi: 10.3390/biomedicines11020378
59. Feng SQ, Ye P, Luo LM, Xiao WK, Xu RY, Wu HM. [Relationship between serum homocysteine and metabolic syndrome: a cross-sectional study]. Zhonghua Liu Xing Bing Xue Za Zhi (2012) 33(3):256–9.
60. Vigna L, Vassalle C, Tirelli AS, Gori F, Tomaino L, Sabatino L, et al. Gender-related association between uric acid, homocysteine, γ-glutamyltransferase, inflammatory biomarkers and metabolic syndrome in subjects affected by obesity. biomark Med (2017) 11(10). doi: 10.2217/bmm-2017-0072
61. Butkowski EG, Al-Aubaidy HA, Jelinek HF. Interaction of homocysteine, glutathione and 8-hydroxy-2′-deoxyguanosine in metabolic syndrome progression. Clin Biochem (2017) 50(3):116–20. doi: 10.1016/j.clinbiochem.2016.10.006
62. Agoşton-Coldea L, Mocan T, Dobie L, Mărginean A, Lupu S. The association between homocysteine level and metabolic syndrome in patients of prior myocardial infarction. Rom J Intern Med (2010) 48(2):151–8.
63. Saeed A, Al Shehri M, Al Saleb A, Othman F, Al Hazmi M, Al Amri F, et al. The association between plasma homocysteine level and metabolic syndrome. A record-based study of Saudi patients attending King Abdulaziz Medical City in Riyadh, Saudi Arabia. Saudi Med J (2020) 41(9):947–54. doi: 10.15537/smj.2020.9.25273
64. Liu C, Liu L, Wang Y, Chen X, Liu J, Peng S, et al. Hyperhomocysteinemia increases risk of metabolic syndrome and cardiovascular death in an elderly Chinese community population of a 7-year follow-up study. Front Cardiovasc Med (2021) 8:811670. doi: 10.3389/fcvm.2021.811670
65. Kim SH, Lee JW, Im JA, Hwang HJ. Monocyte chemoattractant protein-1 is related to metabolic syndrome and homocysteine in subjects without clinically significant atherosclerotic cardiovascular disease. Scand J Clin Lab Investig (2011) 71(1):1–6. doi: 10.3109/00365513.2010.519047
66. Yoon KS, Choi HJ, Im JA, Yoon JH, Kim SH. Association between metabolic syndrome and plasma homocysteine among Korean adults. J Korean Acad Fam Med (2008) 29(7):499–505.
67. Orluwene CG, Mommoh MO. Plasma total homocysteine, high-sensitivity C-reactive protein and thyroid function in metabolic syndrome patients. Niger Postgrad Med J (2013) 20(4):286–90. doi: 10.4103/1117-1936.164606
68. Nayak BS, Pinto Pereira LM, Seemungal T, Davis G, Teelucksingh S, Jagessar A, et al. Relationship of fasting total homocysteine, high sensitivity C-reactive protein and features of the metabolic syndrome in Trinidadian subjects. Arch Physiol Biochem (2013) 119(1):22–6. doi: 10.3109/13813455.2012.735245
69. Cankurtaran M, Halil M, Yavuz BB, Dagli N, Oyan B, Ariogul S. Prevalence and correlates of metabolic syndrome (MS) in older adults. Arch Gerontol Geriatr (2006) 42(1):35–45. doi: 10.1016/j.archger.2005.05.004
70. Herman WA, Krzoska A, Łacka K, Bugaj R, Dorszewska J. [Evaluation of the relationships between plasma homocysteine level and selected low-grade inflammation indices according to the prevalence of metabolic syndrome in men]. Pol Merkur Lekarski (2013) 34(204):320–4.
71. Alihanoglu YI, Yildiz BS, Özcan EE, Kilic ID, Kuru DS, Taskoylu O, et al. Impaired coronary blood flow may be related to elevated homocysteine levels in patients with metabolic syndrome. Wien Klin Wochenschr (2015) 127(21-22):864–70. doi: 10.1007/s00508-015-0854-z
72. Shin K-A. Association between Obesity factors and homocysteine Levels with the Metabolic Syndrome. Korean J Clin Lab Sci (2012) 44:147–54.
73. Khan RJ, Gebreab SY, Sims M, Riestra P, Xu R, Davis SK. Prevalence, associated factors and heritabilities of metabolic syndrome and its individual components in African Americans: the Jackson Heart Study. BMJ (Open) (2015) 5(10):e008675. doi: 10.1136/bmjopen-2015-008675
74. Al-Daghri NM. Hyperhomocysteinemia, coronary heart disease, and diabetes mellitus as predicted by various definitions for metabolic syndrome in a hypertensive Saudi population. Saudi Med J (2007) 28(3):339–46.
75. Huang Z, Tan A, Zhang H, Gao Y, Lu Z, Wu C, et al. Relationship between serum homocysteine and metabolic syndrome in middle-aged men in Fangchenggang City. Mod Med J China (2019) 7:9–12.
76. Yue CHI, Ling-li T, Ting YU. Clinical significance of detection of homocysteine and cystatin C in patients with metabolic syndrome. Labeled Immunoassays Clin Med (2012) 19(1):25–7.
77. Di Cianni G, Lencioni C, Volpe L, Ghio A, Cuccuru I, Pellegrini G, et al. C-reactive protein and metabolic syndrome in women with previous gestational diabetes. Diabetes Metab Res Rev (2007) 23(2):135–40. doi: 10.1002/dmrr.661
78. Sung SH, Kim NH, Hong SP, Lee JK, Choi SJ. Associations of metabolic syndrome with total testosterone and homocysteine levels in male Korean workers. Endocrinol Metab (Seoul) (2019) 34(2):158–68. doi: 10.3803/EnM.2019.34.2.158
79. Bauduceau B, Baigts F, Bordier L, Burnat P, Ceppa F, Dumenil V, et al. Epidemiology of the metabolic syndrome in 2045 French military personnel (EPIMIL study). Diabetes Metab (2005) 31(4 Pt. 1):353–9. doi: 10.1016/s1262-3636(07)70204-5
80. Panagiotakos DB, Pitsavos C, Chrysohoou C, Skoumas J, Tousoulis D, Toutouza M, et al. Impact of lifestyle habits on the prevalence of the metabolic syndrome among Greek adults from the Attica study. Am Heart J (2004) 147(1):106–12. doi: 10.1016/s0002-8703(03)00442-3
81. Prasad M, Flowers E, Divakaruni M, Molina C, Mathur A, Assimes TL, et al. The relationship of lipoprotein(a), C-reactive protein and homocysteine with metabolic syndrome in South Asians. J Indian Coll Cardiol (2014) 4(4):208–13. doi: 10.1016/j.jicc.2014.08.004
82. Shin Y-R, Lee J-W, Lee S-Y, Yun Y-J, Jeong H-Y, Kim K-M, et al. Correlation between metabolic syndrome and plasma homocysteine level in patients with silent lacunar infarction. J Intern Korean. Med (2012) 33(3):243–56.
83. Mohorko N, Petelin A, Jurdana M, Biolo G, Jenko-Pražnikar Z. Elevated serum levels of cysteine and tyrosine: early biomarkers in asymptomatic adults at increased risk of developing metabolic syndrome. BioMed Res Int (2015) 2015:418681. doi: 10.1155/2015/418681
84. Yu S, Chen Y, Yang H, Guo X, Zheng L, Sun Y. Hyperhomocysteinemia accompany with metabolic syndrome increase the risk of left ventricular hypertrophy in rural Chinese. BMC Cardiovasc Disord (2020) 20(1):44. doi: 10.1186/s12872-020-01350-2
85. Hu F, Yu S, Li J, Zhou W, Wang T, Huang X, et al. Association between hyperhomocysteinemia combined with metabolic syndrome and higher prevalence of stroke in Chinese adults who have elevated blood pressure. Med Sci Monit (2022) 28:e934100. doi: 10.12659/MSM.934100
86. Baltaci D, Kutlucan A, Turker Y, Yilmaz A, Karacam S, Deler H, et al. Association of vitamin B12 with obesity, overweight, insulin resistance and metabolic syndrome, and body fat composition; primary care-based study. Med Glas (Zenica) (2013) 10(2):203–10.
87. Chen AR, Zhang HG, Wang ZP, Fu SJ, Yang PQ, Ren JG, et al. C-reactive protein, vitamin B12 and C677T polymorphism of N-5,10-methylenetetrahydrofolate reductase gene are related to insulin resistance and risk factors for metabolic syndrome in Chinese population. Clin Invest Med (2010) 33(5):E290–7. doi: 10.25011/cim.v33i5.14354
88. Kulaksizoglu B, Kulaksizoglu S. Correlation of metabolic syndrome with serum BDNF, vitamin B12 and folate in schizophrenic patients. Res J Pharm Biol Chem Sci (2016) 7(6):3142–51.
89. Kanagasabai T, Alkhalaqi K, Churilla JR, Ardern CI. The association between metabolic syndrome and serum concentrations of micronutrients, inflammation, and oxidative stress outside of the clinical reference ranges: A cross-sectional study. Metab Syndr Relat Disord (2019) 17(1):29–36. doi: 10.1089/met.2018.0080
90. Guarnizo-Poma M, Urrunaga-Pastor D, Montero-Suyo C, Lazaro-Alcantara H, Paico-Palacios S, Pantoja-Torres B, et al. Association between serum vitamin B12 levels and metabolic syndrome in a euthyroid population. Diabetes Metab Syndr (2018) 12(6):943–8. doi: 10.1016/j.dsx.2018.05.022
91. Koo YS, Lee YJ, Park JM. Inverse association of serum folate level with metabolic syndrome and its components in Korean premenopausal women: findings of the 2016-2018 Korean national health nutrition examination survey. Nutrients (2022) 14(4):880. doi: 10.3390/nu14040880
92. Mba CM, Koulman A, Forouhi NG, Imamura F, Assah F, Mbanya JC, et al. Associations of serum folate and Holotranscobalamin with cardiometabolic risk factors in rural and urban Cameroon. Nutrients (2021) 14(1):178. doi: 10.3390/nu14010178
93. Villatoro-Santos CR, Ramirez-Zea M, Villamor E, Nine Mesoamerican Countries Metabolic Syndrome (NiMeCoMeS) Study Group. B-vitamins and metabolic syndrome in Mesoamerican children and their adult parents. Public Health Nutr (2021) 24(14):4537–45. doi: 10.1017/S1368980020003936
94. Ashok P, Godbole G, Salunkhe A. Association of homocysteine with metabolic syndrome risk factors in postmenopausal women. Natl J Physiol Pharm Pharmacol (2022) 12(8):1176–81. doi: 10.5455/njppp.2022.12.114006202104012022
95. Maiti S, Lochan Das K. Estimation of serum vitamin B12 levels in metabolic syndrome patients: a tertiary hospital based study in Eastern part of India. Int J Inf Res Rev (2015) 2(9):1137–41.
96. Shu-heng CUI, Qi Z, Na W, Yue Z, Yun QIU, Xiao-yan Z, et al. Association between metabolic syndrome and its components with hyperhomocysteinemia in community population. Chin J Dis Control Prev (2020) 9:1003–8.
97. Xiang L, Shuhong L, Lin L. Association of serum homocysteine levels with metabolic syndrome and its components in adults. Chin J Clin Nutr (2016) 24(3):139–43.
98. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation (2005) 112(17):2735–52. doi: 10.1161/CIRCULATIONAHA.105.169404
99. Jia W, Weng J, Zhu D, Ji L, Lu J, Zhou Z, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev (2019) 35(6):e3158. doi: 10.1002/dmrr.3158
100. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment Panel III). JAMA (2001) 285(19):2486–97. doi: 10.1001/jama.285.19.2486
101. Alberti KG, Zimmet P, Shaw J. Metabolic syndrome–a new world-wide definition. A consensus statement from the International Diabetes Federation. Diabetes Med (2006) 23(5):469–80. doi: 10.1111/j.1464-5491.2006.01858.x
102. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabetes Med (1998) 15(7):539–53. doi: 10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
103. Andrès E, Serraj K, Zhu J, Vermorken AJ. The pathophysiology of elevated vitamin B12 in clinical practice. Qjm (2013) 106(6):505–15. doi: 10.1093/qjmed/hct051
104. Mabasa L, Samodien E, Sangweni NF, Pheiffer C, Louw J, Johnson R. In utero one-carbon metabolism interplay and metabolic syndrome in cardiovascular disease risk reduction. Mol Nutr Food Res (2020) 64(4):e1900377. doi: 10.1002/mnfr.201900377
105. Langouche L, Van den Berghe G. Glucose metabolism and insulin therapy. Crit Care Clin (2006) 22(1):119–29. doi: 10.1016/j.ccc.2005.09.005
106. Avramoglu RK, Basciano H, Adeli K. Lipid and lipoprotein dysregulation in insulin resistant states. Clin Chim Acta (2006) 368(1-2):1–19. doi: 10.1016/j.cca.2005.12.026
107. Matsuzawa Y, Funahashi T, Nakamura T. The concept of metabolic syndrome: contribution of visceral fat accumulation and its molecular mechanism. J Atheroscler Thromb (2011) 18(8):629–39. doi: 10.5551/jat.7922
108. Sobczyńska-Malefora A, Katayev A, Steed D, O’Logbon J, Crook M, Harrington DJ. Age- and ethnicity-related reference intervals for serum vitamin B12(12). Clin Biochem (2023) 111:66–71. doi: 10.1016/j.clinbiochem.2022.10.007
109. Surendran S, Jayashri R, Drysdale L, Bodhini D, Lakshmipriya N, Shanthi Rani CS, et al. Evidence for the association between FTO gene variants and vitamin B12 concentrations in an Asian Indian population. Genes Nutr (2019) 14:26. doi: 10.1186/s12263-019-0649-3
110. Lee PC, Ganguly S, Dixon JB, Tan HC, Lim CH, Tham KW. Nutritional deficiencies in severe obesity: a multiethnic Asian cohort. Obes Surg (2019) 29(1):166–71. doi: 10.1007/s11695-018-3494-3
111. Hsu WC, de Juras AR, Hu SC. Prevalence and determinants of multiple forms of malnutrition among adults with different body mass index: A population-based survey in the Philippines. BioMed Res Int (2023) 2023:3182289. doi: 10.1155/2023/3182289
112. Melguizo-Rodríguez L, Costela-Ruiz VJ, García-Recio E, De Luna-Bertos E, Ruiz C, Illescas-Montes R. Role of vitamin D in the metabolic syndrome. Nutrients (2021) 13(3):830. doi: 10.3390/nu13030830
113. Zhang T, Sun P, Geng Q, Fan H, Gong Y, Hu Y, et al. Disrupted spermatogenesis in a metabolic syndrome model: the role of vitamin A metabolism in the gut–testis axis. Gut (2022) 71(1):78–87. doi: 10.1136/gutjnl-2020-323347
114. Yoshida Y, Chen Z, Baudier RL, Krousel-Wood M, Anderson AH, Fonseca VA, et al. Sex differences in the progression of metabolic risk factors in diabetes development. JAMA Netw Open (2022) 5(7):e2222070. doi: 10.1001/jamanetworkopen.2022.22070
115. Asemi Z, KaraMali M, Esmaillzadeh A. Metabolic response to folate supplementation in overweight women with polycystic ovary syndrome: a randomized double-blind placebo-controlled clinical trial. Mol Nutr Food Res (2014) 58(7):1465–73. doi: 10.1002/mnfr.201400033
116. Setola E, Monti LD, Galluccio E, Palloshi A, Fragasso G, Paroni R, et al. Insulin resistance and endothelial function are improved after folate and vitamin B12 therapy in patients with metabolic syndrome: relationship between homocysteine levels and hyperinsulinemia. Eur J Endocrinol (2004) 151(4):483–9. doi: 10.1530/eje.0.1510483
117. Rabelo NN, Telles JPM, Pipek LZ, Farias Vidigal Nascimento R, de Gusmão RC, Teixeira MJ, et al. Homocysteine is associated with higher risks of ischemic stroke: A systematic review and meta-analysis. PloS One (2022) 17(10):e0276087. doi: 10.1371/journal.pone.0276087
118. Wang J, You D, Wang H, Yang Y, Zhang D, Lv J, et al. Association between homocysteine and obesity: A meta-analysis. J Evid Based Med (2021) 14(3):208–17. doi: 10.1111/jebm.12412
119. Ntaios G, Savopoulos C, Chatzopoulos S, Mikhailidis D, Hatzitolios A. Iatrogenic hyperhomocysteinemia in patients with metabolic syndrome: a systematic review and metaanalysis. Atherosclerosis (2011) 214(1):11–9. doi: 10.1016/j.atherosclerosis.2010.08.045
120. Kim J, Kim H, Roh H, Kwon Y. Causes of hyperhomocysteinemia and its pathological significance. Arch Pharm Res (2018) 41(4):372–83. doi: 10.1007/s12272-018-1016-4
121. Nakhai Pour HR, Grobbee DE, Muller M, Emmelot-Vonk M, van der Schouw YT. Serum sex hormone and plasma homocysteine levels in middle-aged and elderly men. Eur J Endocrinol (2006) 155(6):887–93. doi: 10.1530/eje.1.02303
122. Gao X, Bermudez OI, Tucker KL. Plasma C-reactive protein and homocysteine concentrations are related to frequent fruit and vegetable intake in Hispanic and non-Hispanic white elders. J Nutr (2004) 134(4):913–8. doi: 10.1093/jn/134.4.913
123. Benito P, Caballero J, Moreno J, Gutiérrez-Alcántara C, Muñoz C, Rojo G, et al. Effects of milk enriched with omega-3 fatty acid, oleic acid and folic acid in patients with metabolic syndrome. Clin Nutr (2006) 25(4):581–7. doi: 10.1016/j.clnu.2005.12.006
124. Maruyama K, Eshak E S, Kinuta M, Nagao M, Cui R, Imano H, et al. Association between vitamin B group supplementation with changes in % flow-mediated dilatation and plasma homocysteine levels: a randomized controlled trial. J Clin Biochem Nutr (2019) 64(3):243–9. doi: 10.3164/jcbn.17-56
Keywords: metabolic syndrome, folate, vitamin B12, homocysteine, meta-analysis
Citation: Ulloque-Badaracco JR, Hernandez-Bustamante EA, Alarcon-Braga EA, Al-kassab-Córdova A, Cabrera-Guzmán JC, Herrera-Añazco P and Benites-Zapata VA (2023) Vitamin B12, folate, and homocysteine in metabolic syndrome: a systematic review and meta-analysis. Front. Endocrinol. 14:1221259. doi: 10.3389/fendo.2023.1221259
Received: 12 May 2023; Accepted: 22 August 2023;
Published: 13 September 2023.
Edited by:
Roger Gutiérrez-Juárez, National Autonomous University of Mexico, MexicoReviewed by:
Rosaura Leis, University of Santiago de Compostela, SpainZoran Gluvic, University of Belgrade, Serbia
Copyright © 2023 Ulloque-Badaracco, Hernandez-Bustamante, Alarcon-Braga, Al-kassab-Córdova, Cabrera-Guzmán, Herrera-Añazco and Benites-Zapata. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente A. Benites-Zapata, dmJlbml0ZXNAdXNpbC5lZHUucGU=