 Taner Bayraktaroğlu
Taner Bayraktaroğlu Figen Barut
Figen Barut Güldeniz Karadeniz Çakmak
Güldeniz Karadeniz Çakmak- 1Divison of Endocrinology and Metabolism, Department of Internal Medicine, Zonguldak, Türkiye
- 2Department of Pathology, Faculty of Medicine, Zonguldak, Türkiye
- 3Department of General Surgery, Faculty of Medicine, Zonguldak Bulent Ecevit University, Zonguldak, Türkiye
Editorial on the Research Topic
Subclassification of AUS/FLUS category for thyroid nodules: trials and evidence-based clinical management
Introduction
This Research Topic aims to include original research articles, reviews, systematic reviews, meta-analyses, on themes related to the “atypia of undetermined significance/follicular lesion of undetermined significance” (AUS/FLUS) category regarding Bethesda System for Reporting Thyroid Cytopathology (BSRTC) (1–4). The fırst article of this Research Topic concluded that the malignancy rate of thyroid nodules with AUS/FLUS cytology was comparable irrespective of the presence of underlying chronic lymphocytic thyroiditis (CLT) (Cho et al.). In an other study, risk stratification w recommended for patients with Bethesda category III (AUS/FLUS) nodules with a size under 1 cm. Nodules with a size over 1 cm harboring WT-BRAF or those under 1 cm harboring BRAF V600E mutation was regarded as moderate risk, and molecular testing should be recommended. However, those with a size over 1 cm harboring BRAF V600E mutation should be regarded as high risk, and a diagnostic surgery should be recommended (Zha et al.) In addition, malignant disease was common in Bethesda category III nodules, and surgical treatment was strongly indicated in the presence of male sex, aspect ratio>1, microcalcification, and BRAFV600E mutation (Liu et al.).
Fine needle aspiration cytology is the gold standard method for the differential diagnosis of thyroid nodules, though 25–30% of which are classified as indeterminate in categories III or IV of the Bethesda System for Reporting Thyroid Cytopathology (1, 2). The reported confirmation rate of the malignancy in surgical specimens is up to 40% for indeterminate nodules which means most of the patients may be subjected to unnecessary surgical interventions (5).
Bethesda category III namely, atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS) represents the gray zone in thyroid cytopathology for which the decision making process might be even harder either for patient or the physician. (Figure 1). The terms “indeterminate” and “atypical” may be interpreted differently by different medical professionals and institutions, leading to confusion in diagnostic and therapeutic management of thyroid nodules. This can lead to variation in patient care and outcomes. Therefore, it’s important to have standardized guidelines and criteria for the interpretation and management of thyroid nodules to ensure consistency and accuracy in diagnosis and treatment (6, 7, Liu et al.; Zha et al.).
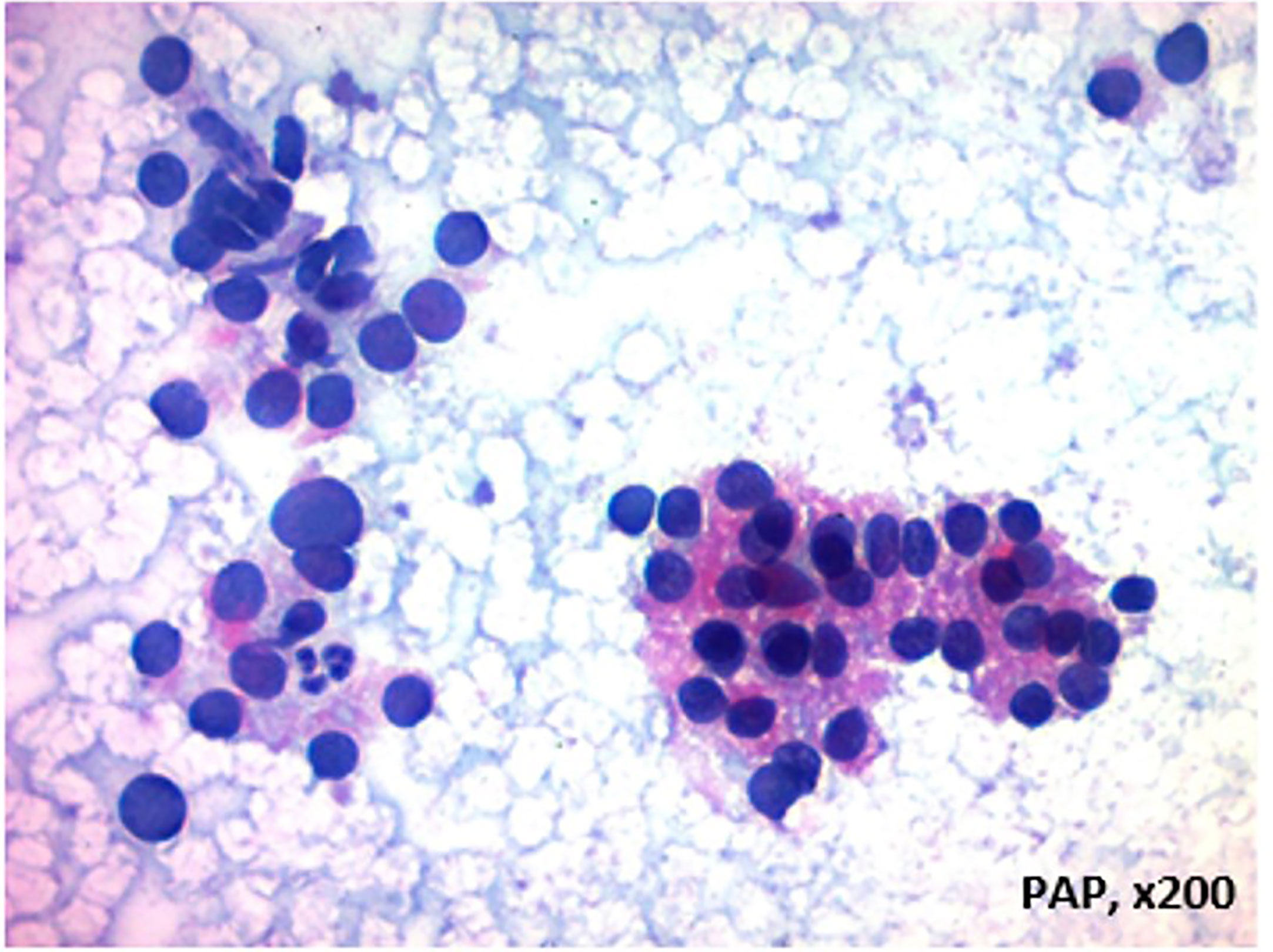
Figure 1 Thyroid epithelial cells that form a three-dimensional cell layer with few microfollicule-like structures and exhibit hyperchromasia and pleomorphism in some areas, AUS/Bethesda III Category author (It was used from FB's archive and permisssion).
The risk of malignancy associated with AUS/FLUS
The risk of malignancy (ROM) associated with different subgroups remains unresolved; ROM for AUS/FLUS varies greatly among medical centers (8, 9, Cho et al.; Zha et al.). Subclassification of AUS/FLUS might be helpful in identifying nodules with a high ROM in this category and improving the management of such nodules. The AUS subcategory indicates a higher risk of malignancy than the FLUS subcategory. To resolve some of these problems, recent studies of the malignancy risk in AUS/FLUS suggest a two- tier subclassification of the AUS/FLUS category (2, 5):
1-Low cellularity with predominant microfollicular architecture and absence of colloid,
2-Nuclear features not characteristic of benign lesions (nuclear atypia) attributable to strict criteria for the evaluation of cancer probability.
Management AUS/FLUS - trials and evidence-based outcomes
The rates of malignancy among this category have varied widely, ranging from 6 – 48% among selected subsets of the patient’s undergoing surgery. In this context, ultrasound (US) classifications, allowing a better classification of malignant nodules, have developed worldwide. Among them, the European Thyroid Association guidelines introduced in 2017, a US classification for thyroid nodules, the EU-TIRADS, which was confirmed to be a highly sensitive system and is widely used among European Countries (10, 11). The American College of Radiology (ACR) recommended the Thyroid Imaging Reporting and Data System (TI-RADS) as a classification system. ACR TI-RADS predicts the probability of malignancy in thyroid nodules using a scoring system (TR1-TR5) based on multiple ultrasound characteristics and nodule size (12). Various scoring systems have been developed to combine ultrasound findings with clinical information to more accurately predict the risk of malignancy in thyroid nodules (13, 14). Moreover, upon the improved knowledge on the genetic characterization of thyroid cancer (TC), several studies focused on the molecular evaluation of nodules to optimize the management of cytological indeterminate nodules (15–19), as recommended in current guidelines (20, 21).
The available molecular diagnostic tools are classified into two different categories: ‘rule-out’ methods, which have the purpose to reduce the avoidable treatment of benign nodules, and ‘rule-in’ approaches that aim to optimize surgical management (total thyroidectomy or diagnostic lobectomy). Among the rule-in methods, the last version of ThyroSeq (TSv3) can identify more than 12,000 hotspot mutations and more than 120 fusions, while the rule out Afrma Genomic Sequencing Classifier (GSC) analyzes the expression profiles of 1115 genes and detects single nucleotide variants and fusions. Additional approaches for molecular testing include the analysis of miRNAs expression (22). Although both GSC and TSv3 have been demonstrated to be considerably more cost-effective than diagnostic lobectomy (23). However, the main limitation of these molecular tests is their high cost (25) which largely restricts their application in clinical practice, especially in European Countries.
Customized 5-7 genes rule-in panels have been set up to analyze the most frequent genetic alterations found in TC (22). A developed PTC-MA assay able to evaluate in an extremely cost-effective manner, a total of 24 genetic alterations including point mutations and fusions frequently found in TC (25–27). Afirma, ThyroSeq, and ThyGenX/ThyGeNEXT with ThyraMIR are covered by Medicare and many health insurance plans, including BlueCross/BlueShield in the United States, (28, 29). In the 2017 European Thyroid Association guideline (27), the authors concluded that there may be benefit to considering genetic panels that include BRAF, RET/PTC, PZX8/PPARG, NTRK, and RAS mutations for nodules of indeterminate cytology, but they did not recommend the routine use of the Afirma GEC to exclude malignancies because validation studies in the form of long-term outcome data are lacking (28).
The thyroid risk score (TRS) system was developed to further enhance the sensitivity and specificity of the molecular tool. It is based on the combination of clinical, ultrasound, cytological, and molecular criteria (Table 1) (27).
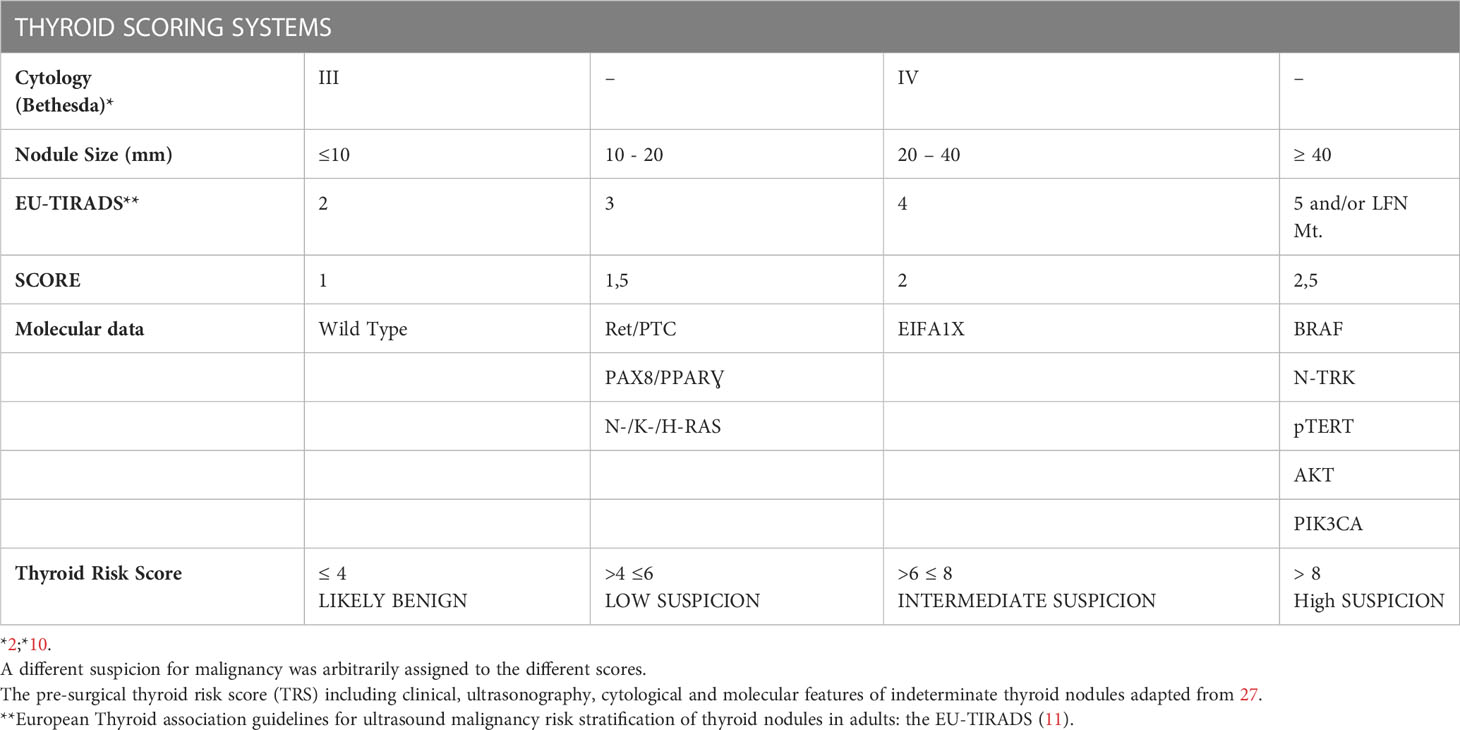
Table 1 Thyroid Scoring Systems.
The indication to surgery was based on the following parameters (27):
– Risk score ≥6
– Large goiters with compression independently from the risk score
– Presence of at least one genetic mutation. It is worth noting that all mutated cases were ultimately found to harbor a risk score ≥6.
Though 14 point mutations and 11 fusions have been tested, only seven genetic alterations were found (in the HRAS, NRAS, BRAF, TERT, EIF1AX, PAX8, RET genes), which are likely to be the more frequently represented in the indeterminate samples. The rate of follicular thyroid carcinomas (FTCs) included (8%) is even higher than that reported in large validation case series (30–32).
Perspectives
This Research Topic perspectives include original research articles, reviews, meta-analyses, on themes related to the AUS/FLUS. Thyroid nodules with indeterminate cytology are one of the most important challenges for the endocrinologist and surgeon. The definitive diagnosis of these nodules requires a histological evaluation after surgery, which represents an overtreatment, and a considerable waste of resources for the national healthcare systems and patients facing potential complications in most benign cases (60–80% of total indeterminate nodules). Ultrasound risk evaluation and molecular testing have been shown to be useful tools in guiding the clinical management of thyroid nodules with indeterminate cytology. However, ultrasound risk evaluation may be limited in its specificity, and molecular testing may be limited by its high cost. Therefore, these tools should be used in conjunction with other clinical and laboratory evaluations to optimize patient care. These parameters have been almost always considered as separate tools for the presurgical differential diagnosis of indeterminate nodules.
A combined score including different parameters, previously validated as diagnostic tools, generated to increase the preoperative accuracy is important. In particular, ‘thyroid risk score’ (TRS), ACR TI-RADS prediction system, the EU-TIRADS scoring and the Bethesda classification, characterized by a high sensitivity (12, 33, 34).
We hope that the reader will find in this Research Topic a useful reference for the current literature in the emerging field of BETHESDA III category as AUS/FLUS.
In conclusion, this Research Topic provides multidisciplinary;
• Bethesda System for Reporting Thyroid Cytopathology (BSRTC)
• The “atypia of undetermined significance/follicular lesion of undetermined significance” (AUS/FLUS) category
• Diagnostic categories and evidence-based clinical management.
• Presurgical differential diagnosis of indeterminate nodules
• Thyroid risk score’ (TRS),
• The EU-TIRADS scoring, Ultrasound risk evaluation
• The risk of malignancy (ROM) for AUS/FLUS
• Validated as diagnostic tools, generated to increase the preoperative accuracy
• BRAF molecular testing for the stratification of ROM into high-risk and low-risk AUS cases;
• Morphological subcategorization, based on atypia qualifiers and molecular testing, potential improvement of malignancy risk stratification of AUS/FLUS patients;
• Different qualifiers of AUS/FLUS thyroid FNA e.g. BRAF, RAS, RET/PTC, and PAX8/PPARg alterations
• Hybrid molecular and morphological subcategorization systems in improving the malignancy risk stratification of thyroid FNA samples diagnosed as AUS/FLUS.
We welcome original research, reviews, perspective, and thought-provoking opinion to this Research Topic.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication. TB, FB and GKÇ contributed to conception and design of the article. TB wrote the first draft of the manuscript. FB prepared and added a AUS/FLUS Figure in the text. All authors contributed to manuscript revision, read, and approved the submitted version.
Acknowledgments
We deeply thank all the authors and reviewers who have participated in this Research Topic.
Conflict of interest
The authors declare that the research was conducted in the absence of any personal, commercial, financial, and professional affiliations or relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nardi F, Basolo F, Crescenzi A, Fadda G, Frasoldati A, Orlandi F, et al. Italian Consensus for the classification and reporting of thyroid cytology. J endocrinological Invest (2014) 37(6):593–9. doi: 10.1007/s40618-014-0062-0
2. Cibas ES, Ali SZ. The 2017 Bethesda system for reporting thyroid cytopathology. Thyroid (2017) 27(11):1341–6. doi: 10.1089/thy.2017.0500
3. Cibas ES, Ali SZ. The Bethesda system for reporting thyroid cytopathology. Thyroid (2009) 19(11):1159–65. doi: 10.1089/thy.2009.0274
4. Cibas ES, Ali SZ, NCI Thyroid FNA State of the Science Conference. The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol (2009) 132(5):658–65. doi: 10.1309/AJCPPHLWMI3JV4LA
5. Ho AS, Sarti EE, Jain KS, Wang H, Nixon IJ, Shaha AR, et al. Malignancy rate in thyroid nodules classified as Bethesda category III (AUS/FLUS). Thyroid (2014) 24(5):832–9. doi: 10.1089/thy.2013.0317
6. Redman R, Yoder BJ, Massoll NA. Perceptions of diagnostic terminology and cytopathologic reporting of fine-needle aspiration biopsies of thyroid nodules: a survey of clinicians and pathologists. Thyroid (2006) 16(10):1003–8. doi: 10.1089/thy.2006.16.1003
7. Somma J, Schlecht NF, Fink D, Khader SN, Smith RV, Cajigas A. Thyroid fine needle aspiration cytology: follicular lesions and the gray zone. Acta cytologica (2010) 54(2):123–31. doi: 10.1159/000324996
8. Zhao H, Guo H, Zhao L, Cao J, Sun Y, Wang C, et al. Subclassification of the Bethesda category III (AUS/FLUS): a study of thyroid FNA cytology based on ThinPrep slides from the national cancer center in China. Cancer cytopathology (2021) 129(8):642–8. doi: 10.1002/cncy.22417
9. Kroll-Wheeler L, Cantley R, Pang JC, Soles BS, Smola B, Jing X, et al. An institutional experience: a retrospective analysis of the effect of transitioning from follicular lesion of undetermined significance to atypia of undetermined significance with subclassified atypia on interobserver concordance, rates of neoplasia, and rates of malignancy. Diagn cytopathology (2021) 49(1):31–8. doi: 10.1002/dc.24611
10. Russ G, Bonnema SJ, Erdogan MF, Durante C, Ngu R, Leenhardt L. European Thyroid association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: the EU-TIRADS. Eur Thyroid J (2017) 6(5):225–37. doi: 10.1159/000478927
11. Yoon JH, Lee HS, Kim EK, Moon HJ, Park VY, Kwak JY. Pattern-based vs. score-based guidelines using ultrasound features have different strengths in risk stratification of thyroid nodules. Eur Radiol (2020) 30(7):3793–802. doi: 10.1007/s00330-020-06722-y
12. Grant EG, Tessler FN, Hoang JK, Langer JE, Beland MD, Berland LL, et al. Thyroid ultrasound reporting lexicon: white paper of the ACR thyroid imaging, reporting and data system (TIRADS) committee. J Am Coll Radiol JACR (2015) 12(12 Pt A):1272–9. doi: 10.1016/j.jacr.2015.07.011
13. Ianni F, Campanella P, Rota CA, Prete A, Castellino L, Pontecorvi A, et al. A meta-analysis-derived proposal for a clinical, ultrasonographic, and cytological scoring system to evaluate thyroid nodules: the ‘CUT’ score. Endocrine (2016) 52:313–21. doi: 10.1007/s12020-015-0785-5
14. Cozzolino A, Pozza C, Pofi R, Sbardella E, Faggiano A, Isidori AM, et al. Predictors of malignancy in high-risk indeterminate (TIR3B) cytopathology thyroid nodules. J endocrinological Invest (2020) 43(8):1115–23. doi: 10.1007/s40618-020-01200-0
15. Alexander EK, Kennedy GC, Baloch ZW, Cibas ES, Chudova D, Diggans J, et al. Preoperative diagnosis of benign thyroid nodules with indeterminate cytology. New Engl J Med (2012) 367(8):705–15. doi: 10.1056/NEJMoa1203208
16. Duick DS, Klopper JP, Diggans JC, Friedman L, Kennedy GC, Lanman RB, et al. The impact of benign gene expression classifier test results on the endocrinologist-patient decision to operate on patients with thyroid nodules with indeterminate fine-needle aspiration cytopathology. Thyroid (2012) 22(10):996–1001. doi: 10.1089/thy.2012.0180
17. McIver B, Castro MR, Morris JC, Bernet V, Smallridge R, Henry M, et al. An independent study of a gene expression classifier (Afirma) in the evaluation of cytologically indeterminate thyroid nodules. J Clin Endocrinol Metab (2014) 99(11):4069–77. doi: 10.1210/jc.2013-3584
18. Nikiforov YE, Carty SE, Chiosea SI, Coyne C, Duvvuri U, Ferris RL, et al. Highly accurate diagnosis of cancer in thyroid nodules with follicular neoplasm/suspicious for a follicular neoplasm cytology by ThyroSeq v2 next-generation sequencing assay. Cancer (2014) 120(23):3627–34. doi: 10.1002/cncr.29038
19. Nikiforov YE. Role of molecular markers in thyroid nodule management: then and now. Endocrine Pract (2017) 23(8):979–88. doi: 10.4158/EP171805.RA
20. Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, Hegedüs L, et al. American Association of clinical endocrinologists, American college of endocrinology, and associazione Medici endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules–2016 update. Endocrine Pract (2016) 22(5):622–39. doi: 10.4158/EP161208.GL
21. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid (2016) 26(1):1–133. doi: 10.1089/thy.2015.0020
22. Muzza M, Colombo C, Pogliaghi G, Karapanou O, Fugazzola L. Molecular markers for the classification of cytologically indeterminate thyroid nodules. J endocrinological Invest (2020) 43(6):703–16. doi: 10.1007/s40618-019-01164-w
23. Nicholson KJ, Roberts MS, McCoy KL, Carty SE, Yip L. Molecular testing versus diagnostic lobectomy in Bethesda III/IV thyroid nodules: a cost-effectiveness analysis. Thyroid (2019) 29(9):1237–43. doi: 10.1089/thy.2018.0779
24. Sciacchitano S, Lavra L, Ulivieri A, Magi F, De Francesco GP, Bellotti C, et al. Comparative analysis of diagnostic performance, feasibility and cost of different test-methods for thyroid nodules with indeterminate cytology. Oncotarget (2017) 8(30):49421–42. doi: 10.18632/oncotarget.17220
25. Pesenti C, Muzza M, Colombo C, Proverbio MC, Farè C, Ferrero S, et al. MassARRAY-based simultaneous detection of hotspot somatic mutations and recurrent fusion genes in papillary thyroid carcinoma: the PTC-MA assay. Endocrine (2018) 61(1):36–41. doi: 10.1007/s12020-017-1483-2
26. Colombo C, Muzza M, Proverbio MC, Tosi D, Soranna D, Pesenti C, et al. Impact of mutation density and heterogeneity on papillary thyroid cancer clinical features and remission probability. Thyroid (2019) 29(2):237–51. doi: 10.1089/thy.2018.0339
27. Colombo C, Muzza M, Pogliaghi G, Palazzo S, Vannucchi G, Vicentini L, et al. The thyroid risk score (TRS) for nodules with indeterminate cytology. Endocrine-related Cancer (2021) 28(4):225–35. doi: 10.1530/ERC-20-0511
28. Paschke R, Cantara S, Crescenzi A, Jarzab B, Musholt TJ, Sobrinho Simoes M. European Thyroid association guidelines regarding thyroid nodule molecular fine-needle aspiration cytology diagnostics. Eur Thyroid J (2017) 6(3):115–29. doi: 10.1159/000468519
29. ThyroSeq. Insurance coverage and CPT code [Internet]. Atlanta (GA): ThyroSeq; (2017). Available from: https://thyroseq.com/physicians/test-ordering/insurance-coverage. Accessed at 01.05.2023.
30. Nikiforova MN, Mercurio S, Wald AI, Barbi de Moura M, Callenberg K, Santana-Santos L, et al. Analytical performance of the ThyroSeq v3 genomic classifier for cancer diagnosis in thyroid nodules. Cancer (2018) 124(8):1682–90. doi: 10.1002/cncr.31245
31. Patel KN, Angell TE, Babiarz J, Barth NM, Blevins T, Duh QY, et al. Performance of a genomic sequencing classifier for the preoperative diagnosis of cytologically indeterminate thyroid nodules. JAMA Surg (2018) 153(9):817–24. doi: 10.1001/jamasurg.2018.1153
32. Steward DL, Carty SE, Sippel RS, Yang SP, Sosa JA, Sipos JA, et al. Performance of a multigene genomic classifier in thyroid nodules with indeterminate cytology: a prospective blinded multicenter study. JAMA Oncol (2019) 5(2):204–12. doi: 10.1001/jamaoncol.2018.4616
33. Kim PH, Suh CH, Baek JH, Chung SR, Choi YJ, Lee JH. Diagnostic performance of four ultrasound risk stratification systems: a systematic review and meta-analysis. Thyroid (2020) 30(8):1159–68. doi: 10.1089/thy.2019.0812
Keywords: Bethesda System for Reporting Thyroid Cytopathology, Atypia of Undetermined Significance/Follicular Lesion of Undetermined Significance, AUS/FLUS, Thyroid Nodules, Fine Needle Aspiration Cytology
Citation: Bayraktaroğlu T, Barut F and Çakmak GK (2023) Editorial: Subclassification of AUS/FLUS category for thyroid nodules: trials and evidence-based clinical management. Front. Endocrinol. 14:1209776. doi: 10.3389/fendo.2023.1209776
Received: 21 April 2023; Accepted: 23 May 2023;
Published: 13 June 2023.
Edited and Reviewed by:
Terry Francis Davies, Icahn School of Medicine at Mount Sinai, United StatesCopyright © 2023 Bayraktaroğlu, Barut and Çakmak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Taner Bayraktaroğlu, YmF5dGFuZXJAeWFob28uY29t