
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 12 April 2023
Sec. Pediatric Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1172823
This article is part of the Research Topic Thyroid Nodules and Tumors in Childhood View all 10 articles
 Dominika Januś1,2*
Dominika Januś1,2* Monika Kujdowicz3,4
Monika Kujdowicz3,4 Małgorzata Wójcik1,2
Małgorzata Wójcik1,2 Anna Taczanowska-Niemczuk5,6Aleksandra Kiszka-Wiłkojć5,6
Anna Taczanowska-Niemczuk5,6Aleksandra Kiszka-Wiłkojć5,6 Wojciech Górecki5,6
Wojciech Górecki5,6 Jerzy B. Starzyk1,2
Jerzy B. Starzyk1,2Background: Follicular cell-derived thyroid carcinoma represents the vast majority of paediatric thyroid cancers (TCs). Papillary thyroid carcinoma (PTC) accounts for over 90% of all childhood TC cases, and its incidence in paediatric patients is increasing. The objective of this follow-up study was to present the outcome of ultrasound (US) and laboratory monitoring of paediatric patients with autoimmune thyroiditis (AIT) prior to the development of PTC.
Patients and methods: This prospective study included 180 children and adolescents (132 females; 73.3%) with a suspicion of thyroid disorder referred to the Outpatient Endocrine Department. The patients were divided into four groups: 1) 28 patients with a mean age of 10.7 [standard deviation (SD), 3.1] y, in whom PTC was detected during the active surveillance of AIT [AIT(+), PTC(+) follow up (F)]; 2) 18 patients with a mean age of 12.8 (SD, 3.4) y, in whom PTC and AIT were detected upon admission (A) [AIT(+), PTC(+) A]; 3) 45 patients with a mean age of 13.0 (SD, 3.4) y, in whom PTC was detected upon admission and AIT was excluded [AIT(-), PTC(+) A]; and 4) an age- and sex-matched control group of 89 patients with AIT and with a mean age of 9.4 (SD, 3.0) y. The analysis included clinical, US, and laboratory assessment results of children on admission (groups 1–4) and during follow-up (groups 1 and 4) in the Paediatric Endocrine Outpatient Department.
Results: Upon admission of those in group 1, the US evaluation revealed a hypoechogenic thyroid gland in 12 and an irregular normoechogenic gland in 16 patients. US monitoring revealed an increase in thyroid echogenicity and an increased irregularity of the thyroid structure during the follow-up period of all of the patients from group 1. Such changes were not noticed in group 4. PTC was diagnosed at the mean time of 3.6 y (3 mo–9 y) since AIT confirmation in group 1. The mean maximum PTC diameter as per the US was significantly smaller in group 1 than in groups 2 and 3 [13.2 (10.8) mm vs. 22.2 (12.8) and 22.05 (15.4) mm]. Fewer patients in group 1 were referred to 131I than in groups 2 and 3 (71.4% vs. 94.4 and 93.3%). Interestingly, significant differences were observed in the thyroglobulin antibody (TgAb)/thyroid peroxidase antibody (TPOAb) ratio between groups 2 and 3, as opposed to group 4, at the beginning of observation [15.3 (27.6) and 3.5 (8.8] vs. 0.77 (1.9)]. In group 1, after the follow-up, an increase in the TgAb/TPOAb ratio was observed [1.2 (9.8) to 5.2 (13.5)]. There were no significant differences between groups 1–3 in labeling index Ki67, lymph nodes metastasis, extrathyroidal extension, and angioinvasion. There were no associations between thyroid-stimulating hormone, TgAb, and the extent of the disease.
Conclusion: The use of thyroid US focused on the search for developing tumours in the routine follow-up of patients with AIT may not only help in the early detection of thyroid malignancies that are not clinically apparent but may also influence the invasiveness of oncological therapy and reduce the future side effects of 131I therapy. We propose that the repeat evaluation of TPOAb and TgAb warrants further exploration as a strategy to determine TC susceptibility in paediatric patients with AIT in larger multicentre studies.
Follicular cell-derived thyroid carcinoma represents the vast majority of paediatric thyroid cancers (TCs) (1). Papillary thyroid carcinoma (PTC) accounts for over 90% of all childhood TC cases (2). The most recent statistical data presented by Siegel et al. estimate that TC accounts for 12% of cancers in adolescents and 2%, in children below 14 y of age (3). TC ranks the fourth most common type of cancer in adolescents and the seventh most common in children in the United States (3). According to the data of the Polish National Cancer Registry, new cases of TC in patients below 19 y of age constitute 2.3% of all TCs diagnosed, every second solid neoplasm in girls, and every eighth solid neoplasm in boys (2).
The prevalence of chronic autoimmune thyroiditis (AIT) has been assessed as up to 2% in children and almost 10% in adolescents, depending on the populations studied (4, 5). The disease has female sex predominance, and although it can be diagnosed from infancy, its peak is observed after puberty (6). AIT is responsible for approximately 55–65% of all pediatric euthyroid goiters (7, 8). In 1955, Dailey et al. suggested for the first time that AIT might be considered a premalignant lesion, as chronic inflammation contributes to the development of cancer in many tissues (9–12). Chronic autoimmune inflammation of the thyroid may cause functional and/or structural thyroid disorders leading to an estimated one-third of patients to develop a nodular rebuilding of the thyroid gland (13–20).
In the paediatric population, the incidence of thyroid nodules is lower (0.5–2%) than in those with AIT (3.5–31.5%) (13–23). In recent years, there has been an increase in the coincidental occurrence of AIT and PTC in children and adolescents (7, 14, 16, 23). According to the current paediatric guidelines, neck US in children with autoimmune thyroid disease (AITD) should be performed at least annually (2, 24).The practicality of this approach was presented by our group in the study evaluating parenchymal changes in the thyroid gland with diffuse AIT in children prior to the development of PTC (25). In 2022, Siegel et al. in Cancer Statistics revealed that in the adult population in the United States, after decades of increase, TC incidence rates have now been declining partly because of recent changes in clinical practice designed to reduce overdetection. However, in a more recent analysis in 2023, Huang et al. found that the incidence rate of TC increased in most countries among individuals irrespective of age groups (3, 26). Additionally, the incidence rate increased in populations aged <40 y in several countries, including Poland (26). Because the presentation of PTC in children is more severe than in adults, the extent of surgery is larger, and therapy also includes 131I therapy, leading to potential future therapeutic side effects. On the other hand, overall survival in children is excellent (24, 27, 28). Therefore, it is important to focus the research on the early detection of malignancies with the aim to reduce future side effects of oncological therapy for PTC in children with long life-expectancy (24, 27, 28).
The present study provides an expansion of previous work from our centre related to the monitoring of patients with thyroid disorders (25). The aim of this study was to prospectively present the outcome of US follow-up in children with AITD who developed PTC and to characterize the US and laboratory variables prior to the development of PTC that might be useful in selecting the PTC risk group within the large population of paediatric patients with AIT.
This prospective study included 180 children and adolescents (132 females; 73.3%) referred to the Outpatient Endocrine Department. The patients were recruited since 2010 till 2023. Patients were divided into four groups: 1) 28 patients with a mean age of 10.7 [standard deviation (SD), 3.1] y, in whom PTC was detected during the active surveillance of AIT [AIT(+), PTC(+) follow up (F)]; 2) 18 patients with a mean age of 12.8 (SD, 3.4) y, in whom PTC and AIT were detected upon admission (A) [AIT(+), PTC(+) A]; 3) 45 patients with a mean age of 13.0 (SD, 3.4) y, in whom PTC was detected upon admission and AIT was excluded [AIT (–), PTC(+) A]; and 4) an age- and sex-matched control group of 89 patients with AIT and with a mean age of 9.4 (SD, 3.0) y.
The prospective analysis of medical records included the evaluations of thyroid function status, US, and cytological and histopathological variables in patients with PTC. All hormonal and immune assessments were routinely performed at the Department of Biochemistry at the University Children’s Hospital in Krakow, Poland and were determined using a single fasting blood sample. Thyroid-stimulating hormone (TSH), fT3, and fT4 levels were measured using immunochemistry with an ADVIA Centaur machine, and thyroid peroxidase antibody (TPOAb), thyroglobulin antibody (TgAb), and thyroid hormone receptor antibody (TRAb) levels were assessed using the radioimmunoassay method with a Brams machine. TSH, fT3, fT4, TPOAb, and TgAb assessments were performed upon admission to the Department (on first visit) and prior to therapy with levothyroxine or antithyroid methimazole when it was needed. TPOAb and TgAb were additionally examined if US analysis revealed a nodule (prior to surgery). TRAb was controlled only in patients with thyrotoxicosis. TSH, fT3, and fT4 were controlled routinely every 3, 4, and 6 mo in all of the patients. Either TPOAb or TgAb were assessed in all patients. Most of the patients underwent all of the assessments of TPOAb and TgAb. In group 1, TPOAb and TgAb were both assessed in 23 of the 28 patients. In group 2, TPOAb was assessed in all 18 and TgAb, in 10 of the 18 patients. In group 3, TPOAb was assessed in 33 and TgAb, in 25 of the 45 patients. In group 4, TPOAb was assessed in 85 and TgAb, in 69 of the 89 patients. Therefore the TgAb/TPOAb ratio could only be assessed in all 23 patients in group 1, 10 out of 18 patients in group 2, 23 out of 45 patients in group 3, and 66 out of 89 patients in group 4.
AIT was diagnosed based on the typical features of chronic AIT seen during thyroid US assessment as previously described, on increased TPOAb and/or TgAb and/or TRAb antibodies levels, and after histopathological confirmation in all of the patients after thyroidectomy (groups 1 and 2) (16, 25). In group 4 the diagnosis of AIT was based on positive TPOAb and/or TgAb and ultrasound.
Thyroid US was performed on all of the patients at the time of thyroid dysfunction diagnosis and annually since then. US of the thyroid gland was performed at the University Children’s Hospital by paediatric endocrinologists and surgeons with experience in paediatric US (DJ and AT >20 y and AKW and MW >15 y). Thyroid US was performed using a high-resolution Voluson 730 GE Medical System (8- to 12-MHz linear-array transducer), Philips Epiq5 (L12-5 linear transducer), Philips iE22 (L11-3 linear transducer), and Samsung HS40 (LA3-16AD transducer). The US examination was performed in the longitudinal and transversal planes. Normal thyroid parenchyma (normoechogenic background) was defined as demonstrating homogenous echogenicity and relative hyperechogenicity compared with the adjacent sternohyoid, sternothyroid, omohyoid, and sternocleidomastoid muscles as described previously (16, 25). The analysis included US features of the thyroid gland according to the EU-TIRADS PL 2022 classification (Polish update of EU-TIRADS 2017) and of the lymph nodes (29, 30).
The patients presenting a nodule containing suspicious features, such as hypoechogenicity, a hyperechogenic ‘border’ between a nodule and thyroid parenchyma, poorly defined margins, irregular shape, microcalcifications, solid composition, presence of chaotic vascularity as detected via Doppler flow, and/or pathological lymph nodes were referred to paediatric oncologic surgeons for fine needle aspiration biopsy (FNAB).
FNAB results were classified according to Bethesda criteria (31). In the patients with PTC, total thyroidectomy with a histopathological verification of the lateral and central lymph nodes was performed. Histopathological evaluation was performed in the Department of Pathology of University Children’s Hospital in Krakow.
The hematoxylin and eosin (HE)-stained tissue slides (deparafinnated, cut with 3.5-um thickness) were scanned with the NanoZoomer SQ Hamamatsu (x400 magnification) after a routine diagnosis of thyroid nodules. The pictures were taken from the scans, with the scale placed on the bottom left.
This study was approved by the relevant institutional review board (The Bioethics Committee of the Jagiellonian University; opinion number:1072.6120.288.2021). Written informed consent was obtained from all of the participants and/or their parents. Written informed consent was obtained from the individual(s) and minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
We summarised baseline and demographic characteristics using descriptive statistics. Categorical variables were expressed as percentages. We assessed the distribution of continuous variables using the Shapiro-Wilks test and described continuous variables using mean and SD when appropriate. We used the non-parametric Kruskal-Wallis and U-Mann Whitney tests to compare the groups of patients. For the assessment of correlations, we used the Spearmann test. A two-tailed p<0.05 was considered statistically significant. All of the analysis were performed with STATISTICA, version 13 (TIBCO Software Inc., Palo Alto, CA 94304 United States).
Clinical, hormonal and histopathological assessment of the patients in the four groups are presented in Table 1 and Table 2.
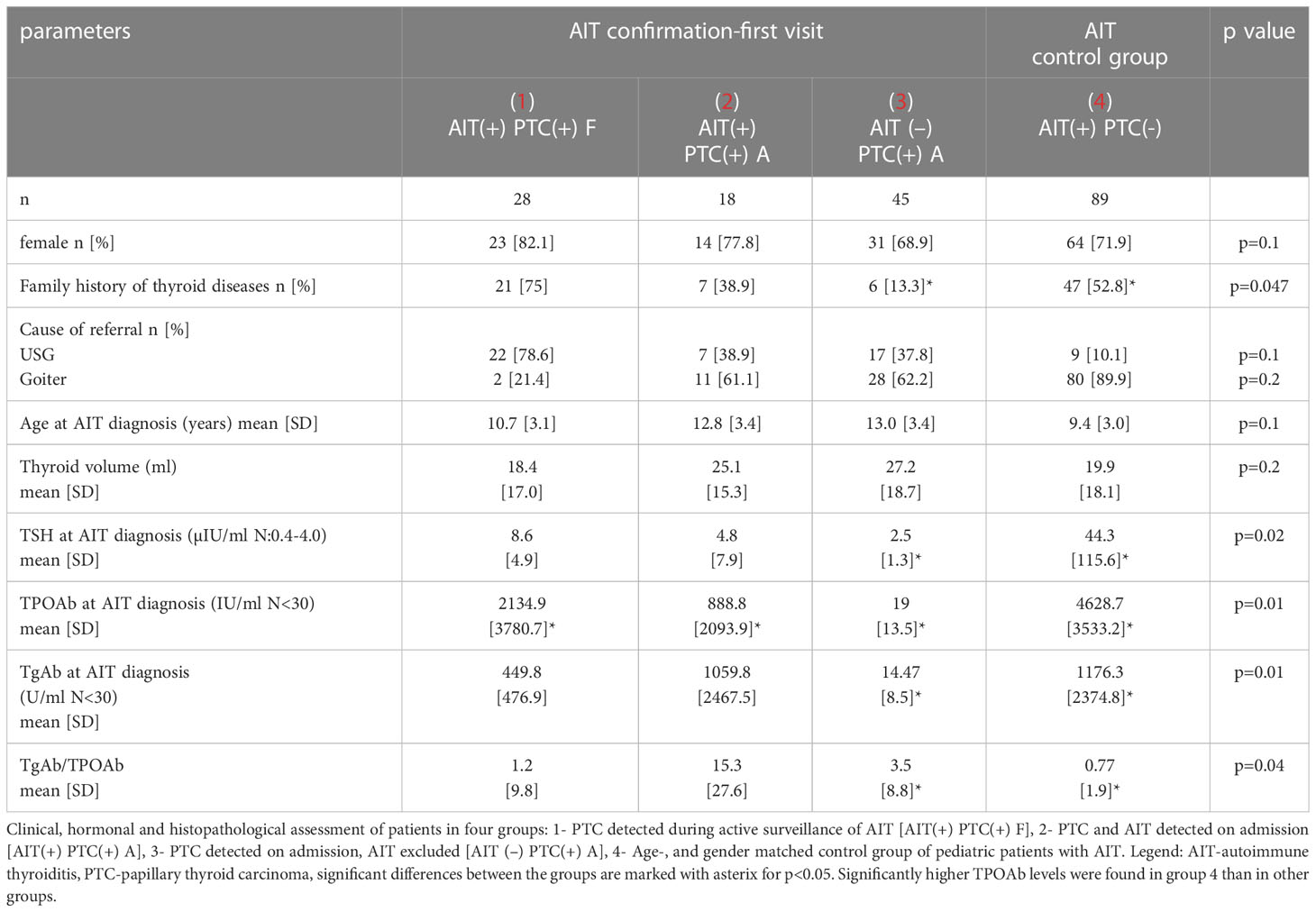
Table 1 AIT-confirmation –first visit.
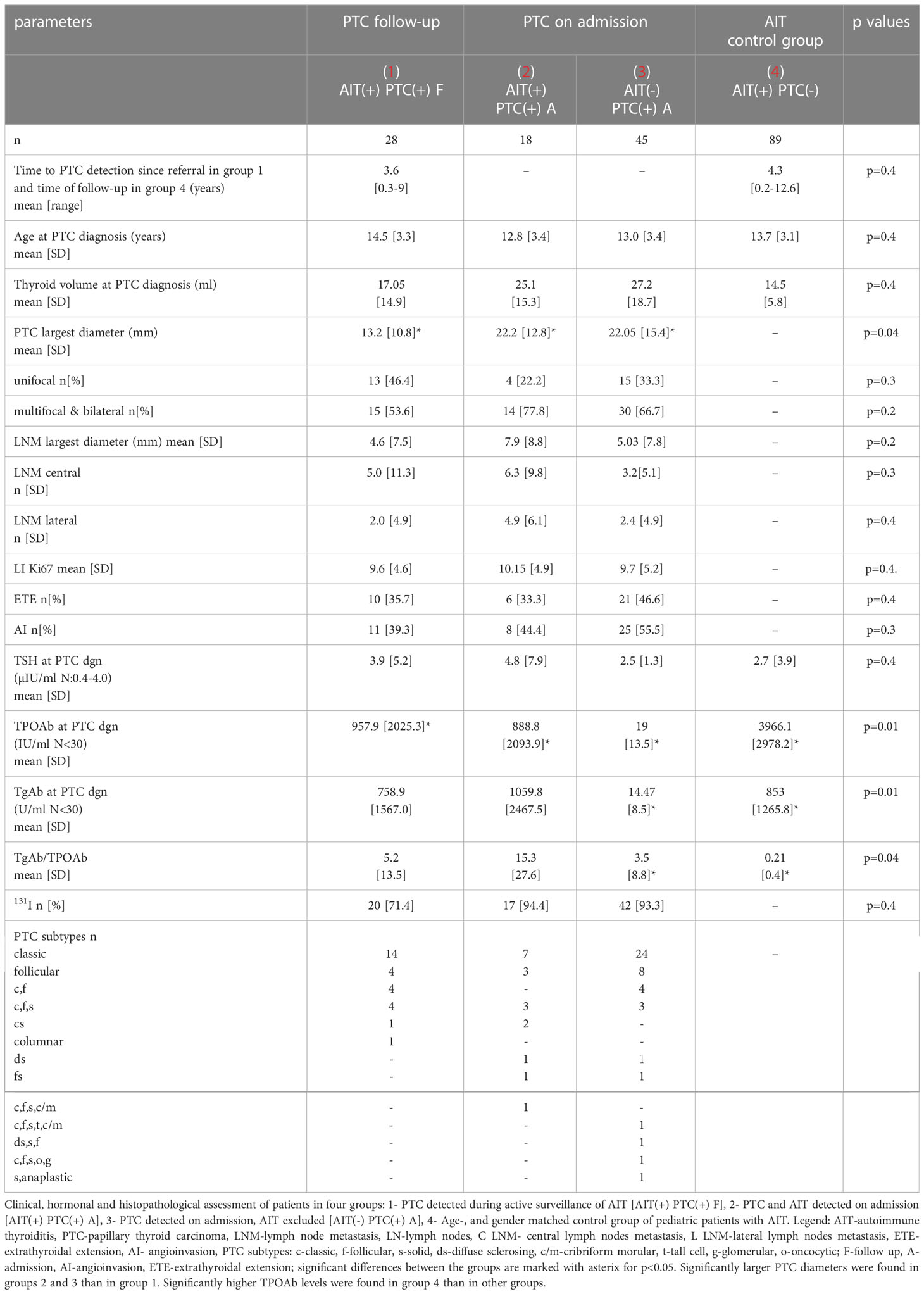
Table 2 PTC diagnosis.
Females predominated in all of the groups. However, a female sex prevalence was more visible in the AIT groups (Table 1).
Interestingly, in group 1, there were more cases with a positive family history of thyroid disorders (nodular goiter, AIT, and PTC) than in groups with PTC detected upon admission. In group 3, this percentage was only 13.3%, and it may explain why these patients presented with a more advanced disease stage upon the first referral (Table 1).
The causes of referral were as follows: in group 1, there were abnormal US features of the thyroid gland in over 70% of the patients, whereas goiter dominated in groups 2 to 4 (Table 1)
There were no significant differences in age upon admission between the groups (Table 1).
At AIT diagnosis, the mean thyroid volume was above the reference ranges for Polish patients and, according to WHO reference ranges, in all groups (32, 33). However, in groups 2 and 3, this was not statistically significantly bigger than in the other groups (Table 1).
There were significant differences between TSH, TPOAb, and TgAb between group 4 and the other groups as there were more cases of overt hypothyroidism in this group (Table 1).
In group 1, TSH ranged from 0-26, in group 2 from 0-6.2, in group 3 from 0.7-5.1, and in group 4 from 0-692.3 µIU/ml.
Hypothyroid patients from three groups started receiving levothyroxine: 22 patients in group 1 (4 with overt hypothyroidism and 18 with subclinical hypothyroidism), 4 patients in group 2 (all with subclinical hypothyroidism) and 60 patients in group 4 (55 with overt hypothyroidism and 5 with subclinical hypothyroidism).
Prior to surgery, three patients from group 2 were treated with the antithyroid drug methimazole due to thyreotoxicosis.
Interestingly, the TgAb/TPOAb ratio was significantly lower in group 4 [0.77 (1.9)] versus group 3 [3.5 (8.8)] and not significantly different versus group 2 [15.3 (27.6)] (Table 1).
PTC was diagnosed at the mean time of 3.6 y (3 mo to 9 y) from AIT confirmation in group 1 (Table 2).
Significantly larger PTC diameters were found in groups 2 and 3 than in group 1 (Table 2). However, the localization of lesions (unifocal or multifocal and bilateral), number of lymph nodes with central or lateral PTC metastasis [lymph nodes metastasis (LNM)], maximum length of the largest metastatic lymph node, labelling index Ki67, extrathyroidal extension, and angioinvasion were similar in all groups 1-3 (Table 2).
After follow-up we have seen a decrease of mean TSH in group 1 and 4, however the mean thyroid volume decreased more in group 4 than in group 1. The mean (SD) TSH levels in group 1 and 2 were close to upper normal range and in the middle of the normal range in group 4.
TPOAb was significantly higher in group 4 than in the other groups. Interestingly, the TgAb/TPOAb ratio was significantly lower in group 4 [0.21 (0.4)] than in groups 3 [3.5 (8.8)] and 1 [5.2 (13.5)] (Table 2). This observation can be explained by a decrease of TPOAb level and increase in TgAb titers as seen in some children in group 1, whereas in the AIT group, we observed a decrease in both TPOAb and TgAb levels. Unfortunately, our small sample size enabled a more detailed analysis.
Histological assessment revealed more aggressive subtypes of PTC in group 2 and mostly in group 3: tall cells, diffuse sclerosing, and solid and more mixed subtypes, including the solid/anaplastic subtype (Table 2).
In group 1, only 71.4% were referred for 131I therapy. Meanwhile, this percentage was higher in group 2 (94.4%) and group 3 (93.3%) (Table 2).
US and corresponding histopathological features of the thyroid gland from representative patients from group 1 are presented in Figures 1–3.
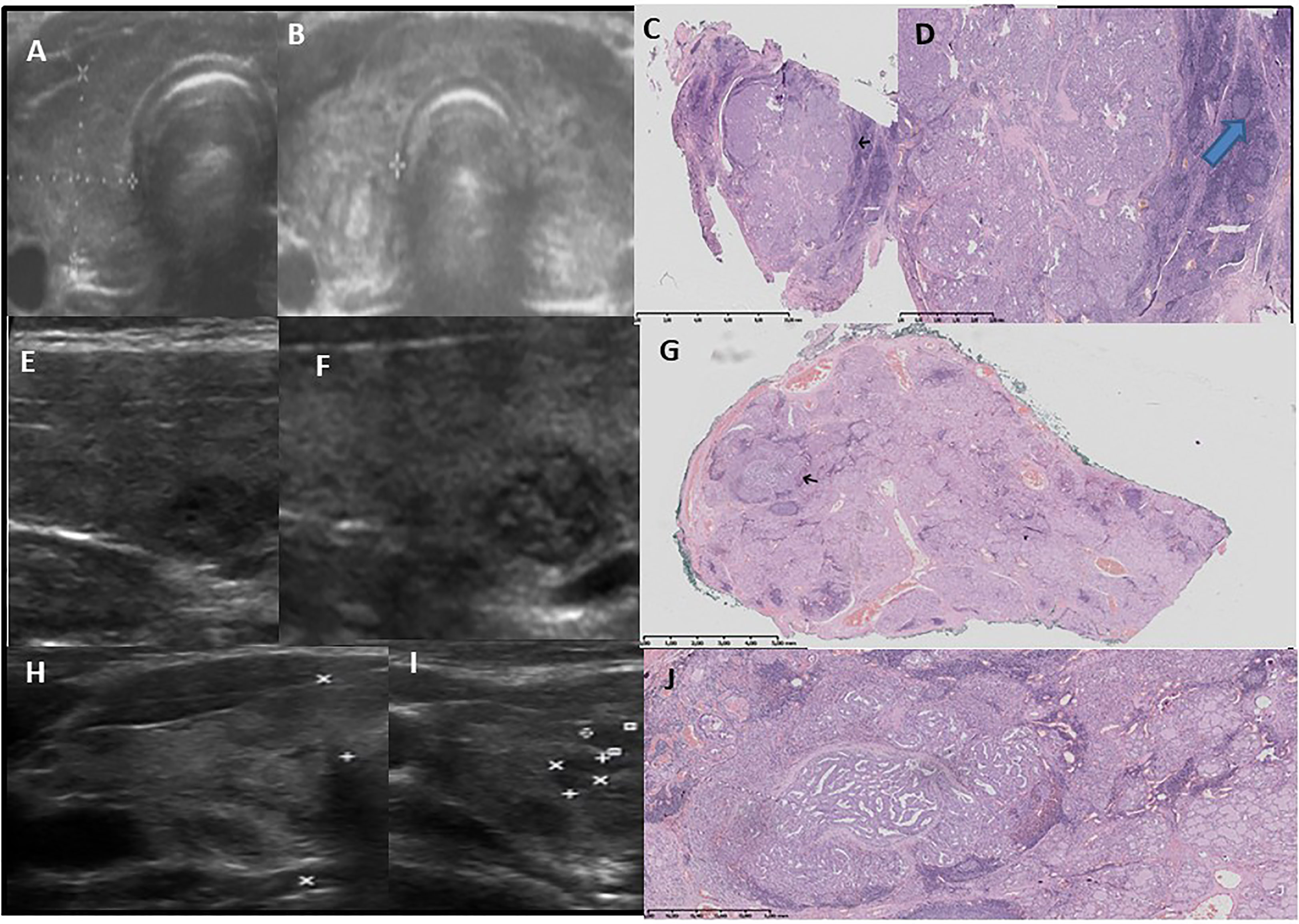
Figure 1 Pattern 1 - a lobulated nodule on US seen as few small malignant lesions- separated by fibrosis and surrounded by lymphocytic inflammation in histology. Ultrasound -pathology correlations. 1st row (A–D): Development of lobulated nodule with nodular hyperechogenic solid composition after 5 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Increase in background echogenicity is visible. Female patient, age 17 years old, classic PTC, 10 mm, multifocal, bilateral (A)-before, (B)-after.(C) Lobulated tumour radiates from a central scar, pushing into thyroid H&E x1, (D) thin fibrotic capsule partially visible. Outside the tumour chronic lymphocytic infiltration with formation of germinal centers, fibrosis is visible H&E ×10, black arrow – tumour, blue arrow – germinal center in lymphocytic inflammation. 2nd and 3rd row (E–J): Development of lobulated nodule with nodular hyperchogenic solid composition after 4 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Female patient, 18 years old, with classic, follicular PTC, 5 mm, multifocal, bilateral (E, H) -before, (F, I)-after). (G) Lobulated tumour with fibrotic layers inside, pushing into thyroid H&E x1, black arrow – tumour. (J) light-pink fibrotic capsule is partially visible in a small, central compartment with purely papillary composition. Tumour invades capsule and the outer part of whole cancer has more compact papillary-follicular composition surrounded by a dark-blue lymphocyte inflammation. The pink, thin, long fibrosis is present in non-tumoural thyroid. Angioinvasion (+). H&E ×20.
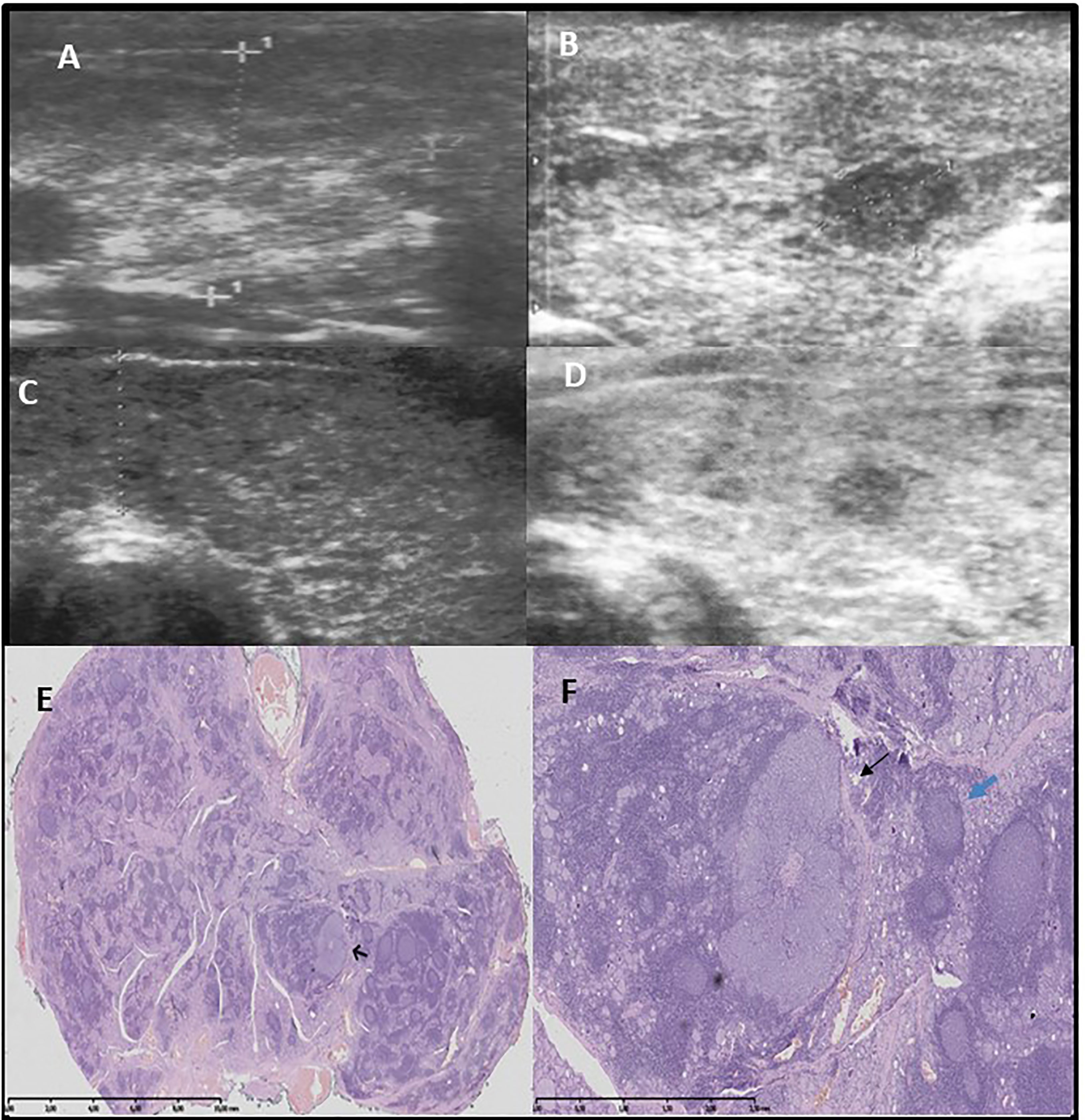
Figure 2 Pattern 3 - hypoechogenic nodule, histologically unencapsulated and with irregular margin. Row (A, B): Development of hypoechogenic lesion surrounded by hyperechogenic fibrotic parenchyma after 1 9/12 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Female patient 11 years old, classic PTC, 6.7 mm, unilateral (A) before, (B) after Row (C–F): Development of hypoechogenic lesion surrounded by hyperechogenic fibrotic parenchyma after 4 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Female patient 17.5 years old, classic, follicular PTC, multifocal, bilateral (C) before, (D) after, (E)The thyroid with AITD and goiter seen as a mixture of normal thyroid with colloid production, intense lymphocytic infiltration, as well as oblong and irregular fibrotic bands. In one large area of intense lymphocytic infiltration an irregular demarcated tumour is present (black arrow). H&E x1, (F)irregular classic PTC with lymphocytic background adhere on the right to fibrotic band (black arrow). The tumour is surrounded by large lymphocytic aggregation on the left. In the central part of the tumour, small, irregular, oval area of fibrosis is seen. H&E x10, blue arrow germinal center.
Upon admission, in group 1, the US evaluation revealed a hypoechogenic thyroid gland in 12 and irregular normoechogenic gland in 16 patients. US monitoring showed an increase in thyroid echogenicity during the follow-up period in all of the patients in group 1; an increasing irregularity of the thyroid structure was also seen. Such changes were not noticed in the patients in group 4 with hypoechoic thyroid glands typical for diffuse thyroiditis during the study period. In groups 2 and 3, with PTC detected upon admission, the US of the thyroid gland represented nodular rebuilding in all of the patients at the background of irregular normoechogenicity of the thyroid gland.
The malignant lesion was hypoechoic in all of the patients, though we observed three US patterns. The first was seen in 18 out of 28 patients in group 1, 10 out of 18 patients in group 2, and all 45 in group 3; here, we noted the nodular, lobulated composition of the lesion (Figure 1). Histopathological assessment revealed small malignant lesions separated by fibrosis (Figure 1). The second pattern was seen in only seven patients only in group 1. The lesion was circumscribed by a hyperechogenic layer, which was histopathologically confirmed to be fibrosis with psammoma bodies (Figure 3). This pattern was characteristic in patients with diffuse thyroiditis and hypoechoic parenchyma with hyperechogenic layers of fibrosis seen in the background. The third pattern included hypoechogenic nodules later described by pathologists to be lesions with spiculated, irregular margins surrounded by fibrotic parenchyma with multiple areas of lymphocytic infiltration in patients with goiter. This pattern was seen in 3 out of 28 patients in group 1 and 8 out of 18 patients in group 2 (Figure 2).
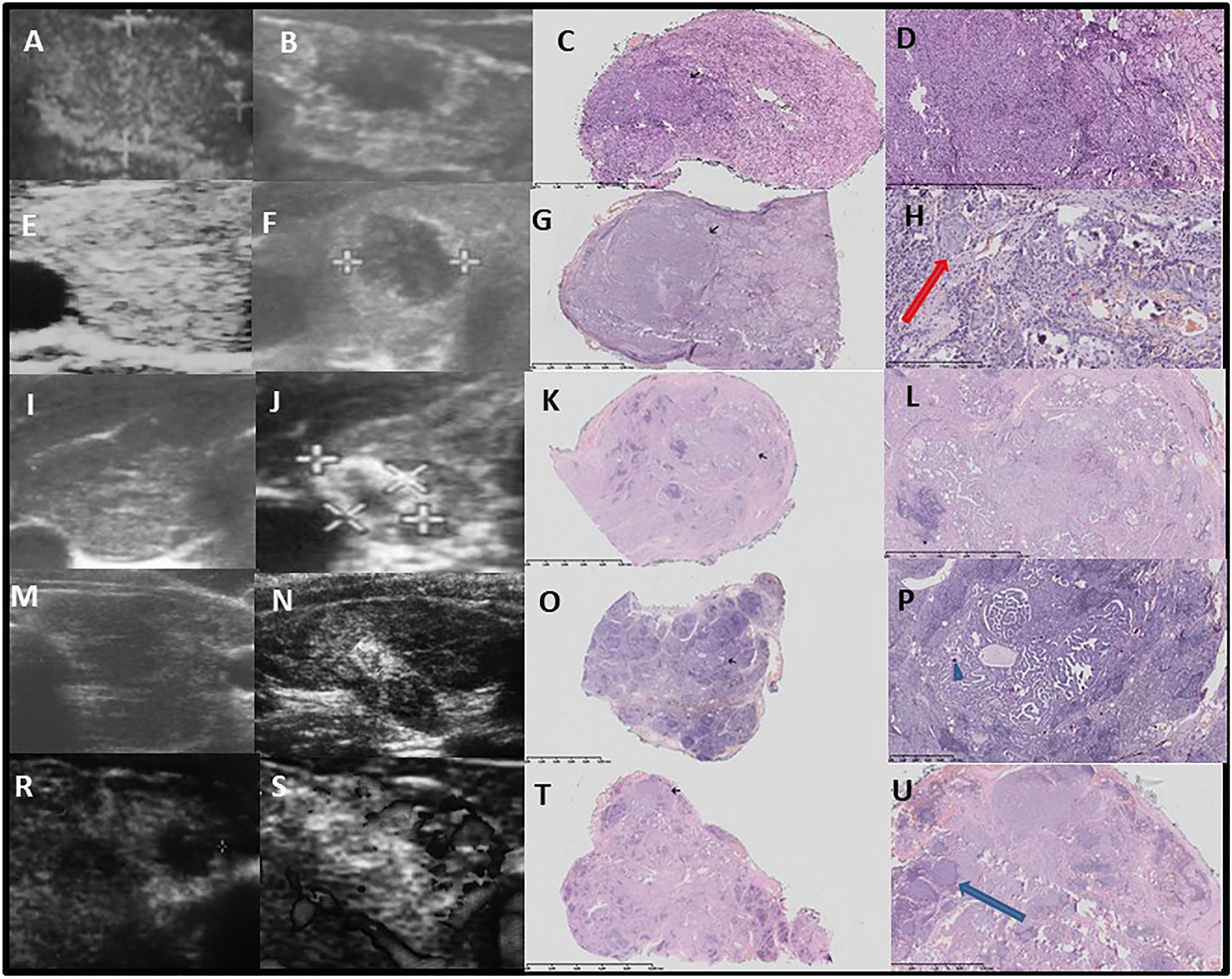
Figure 3 Pattern 2 – well circumscribed hypoechogenic lesion surrounded by a hyperechogenic thick layer and further, hypoechogenic parenchyma with hyperechogenic fibrosis. Thick layer is histologically seen as a tumour surrounded by fibrosis and psammoma bodies, and with diffuse thyroiditis in the background. Ultrasound -pathology correlations. Row (A–D): Development of hypoechogenic nodule surrounded by hyperechogenic fibrotic layer after 4 7/12 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Female patient, 14 years old, classic, follicular, solid PTC, 7 mm and 2 mm, multifocal, bilateral (A)-before, (B)-after. (C) The tumour infiltrates into surrounding thyroid on histology, correlated with blurred margin on ultrasound, no angioinvasion H&E x1, black arrow – tumour. (D) thin fibrotic capsule around classic PTC subtype is visible (upper part of the tumour). Outside the tumour chronic lymphocytic infiltration (dark blue) and fibrosis with few psammoma bodies (small, purple bodies which generate oblong artefacts resembling jagged tissues) is visible H&E ×40. Row (E–H): Development of hypoechogenic nodule surrounded by hyperechogenic fibrotic layer after 4 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Female patient, 13 years old, classic, follicular, solid PTC, 9 mm, unilateral (E) before, (F) after. (G) The ‘mushroom-shaped’ tumour, predominantly papillary in upper part, and follicular and solid in lower part which infiltrates into surrounding thyroid (histology) what correlates with blurred margin on ultrasound. Angioinvasion is present. Inside the solid part of the tumour oblong, irregular fibrosis and desmoplasia are visible. Tumour infiltrates its capsule (a thin capsule is seen in upper part of the tumour, which in this part is quite well demarcated and oval). H&E x1, black arrow – tumour. (H) High magnification of the PTC enriched with multiple psammoma bodies and a foci of squamous epithelial metaplasia (red arrow). H&E ×100. Row (I–L): Development of hypoechogenic nodule surrounded by hyperechogenic fibrotic layer on the background of hypoechoic thyroid, after 4 11/12 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Female patient, 17.5 years old, classic, follicular, solid PTC, 9.8 mm, multifocal, bilateral (I) before, (J) after). (K) The tumour is infiltrating into surrounding thyroid on histology, angioinvasion is absent. H&E ×1, black arrow - tumour. (L) a biphasic (central – dense and solid, while outer – papillary and follicular) tumour infiltrates its capsule (herein a thin capsule demarcate upper part of the tumour). Outside the tumour chronic lymphocytic infiltration and irregular fibrosis is visible H&E ×10. Row (M–P): Development of hypoechogenic nodule surrounded by hyperechogenic fibrotic layer on the background of hypoechoic thyroid, after 2 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Female patient, 8.8 years old, classic PTC, 6.7 mm, unilateral (M)-before, (N)-after). (O)-The tumour is not encapsulated and infiltrates the thyroid. Outside and inside the tumour massive lymphocytic infiltration with formation of germinal centres. H&E x1, black arrow – tumour. (P)-Papillary tumour with a few psammoma bodies (blue arrowhead) and fibrosis (surrounds the lower part and sides of the tumour as well as occurs between lymphocytic infiltration), H&E x40. Row (R–U): Development of hypoechogenic nodule surrounded by hyperechogenic fibrotic layer after 4 years since the confirmation of autoimmune thyroiditis and first thyroid ultrasound. Female patient 17 years old, follicular PTC, 10 mm, multifocal, bilateral (R) before, (S) after). (T) Extensive fibrosis and lymphocytic infiltration of thyroid with less fibrosis in a tumour. H&E x1, black arrow – tumour. (U) Follicular tumour interspersed with thin bands of fibrous tissue. A few small psammoma bodies (which give oblong artefacts) are seen in lower part of the tumour. Lymphocytic germinal centers within the tumour (blue arrow) H&E x40.
We found that the majority of detected nodules showed a fast growth rate over time, with volumes that doubled or even tripled within 2–8 mo of observation before FNAB was performed. This pattern of growth has already been described in our previous report (25).
After FNAB based on the Bethesda criteria was conducted, total thyroidectomy with lymph node dissection where appropriate was performed in all of the patients (31). The recurrences were observed only in group 3, in five patients who were subsequently subjected to lateral lymph node dissection.
There was no correlation between the PTC subtype and the pattern of a nodule seen on US, though our sample may have been too small to observe the differences.
A histopathological assessment revealed that the malignant lesions were not encapsulated. Fibrotic capsules, if partially visible, were infiltrated by the branches of the lesions. In all of the patients, the lymphocytic infiltration around the tumor was visible. In patients with a normoechoic background, the infiltration was less advanced in the surrounding thyroid tissue than in patients with a hypoechoic background, where massive inflammation with germinal centres infiltrated by tumors was visible (Figures 1–3).
There were no correlations between TSH, TgAb, and the extent of the disease. The only determined associations involving the extent of the disease were with age and PTC nodule diameter. The patients’ ages correlated negatively with PTC mm (r: -0.3, p=0.01), LNM mm (r: -0.38, p=0.048), number of central and lateral LNM (r: -0.36; r: -0.32, p=0.01), extrathyroidal extension (ETE) (r: -0.37, p=0.01), and angioinvasion (AI) (r: -0.3, p=0.02). Negative correlations were found between thyroid peroxidase (TPO) and PTC mm (r: -0.29, p=0.011) and AI (r: -0.26, p=0.011). The diameter of PTC in mm correlated positively with LNM mm (r: 0.39, p=0.02), number of central and lateral LNM (r: 0.29; r: 0.36, p=0.01), LI Ki67 (r: 0.32, p=0.012), ETE (r: 0.36, p=0.01), and AI (r: 0.3, p=0.02).The TgAb/TPOAb ratio correlated with AI (r: 0.26, p=0.01).
In the present follow-up study thyroid malignancies were detected early via US before they were clinically apparent. A surgical work-up of all of the patients confirmed malignancies, and there were no surgical complications and unnecessary surgeries. We found that the majority of detected nodules showed a fast growth rate over time, with volume that doubled or even tripled within 2–8 mo of observation before FNAB was performed. This pattern of growth has already been described in our previous report (25).
In the present study, we observed that paediatric PTC is fast-growing and aggressive as even with the regular monitoring and detection of small lesions after thyroidectomy, over 70% of children in group 1 were referred for 131I therapy due to multifocality and bilaterality and LNM, a known observation in paediatrics (2, 6, 13, 24). However, this percentage was over 90% in other groups; thus, active surveillance might reduce the need for 131I therapy. Additionally, the diameter of the nodules was significantly lower in the actively surveilled group. Interestingly, we observed more aggressive and mixed PTC subtypes in groups detected upon admission (referred with goiter or nodules already found during US assessment). Furthermore, the percentage of those with a family history of thyroid disorders was much smaller in group 2 and especially in group 3 than in group 1; therefore, the children in these groups were referred relatively late to endocrinologists. The poor awareness of thyroid diseases by parents without familiarity with thyroid problems could impact late referrals. This finding is not surprising, but it may underline the need for a thorough check-up of family thyroid history in paediatric patients, as well as thyroid US checks in cases of neck goiter even if this history is negative.
This study is an expansion of our previous work presenting the follow-up of patients with AIT who did not appear to have nodules on the first US check-up, which was performed during the first referral visit, but who later developed nodules, as seen during subsequent visits (25). The patterns observed and described in our previous work and presented to all members of our team enabled an increase in the detection of PTC in our departments. In the present study, the mean time to PTC detection was 3.6 y. These data are consistent with those of the Italian study by Rizzo et al., demonstrating that the lag time between AIT diagnosis and PTC detection was approximately 5 years (34). The increase in the number of thyroid nodules during follow-up, but not PTC, has also been reported by Radetti et al. in a large study of paediatric patients with AIT (13). This difference could be related to the small size bias in our group of selected patients.
The US evaluation of thyroid nodules detected during follow-up revealed three patterns of a nodule. To our knowledge, this is the first study describing different patterns of a developing nodule in paediatric patients. The first, which was more common, was of a lesion with a nodular, lobulated, solid composition. The second was of a lesion circumscribed by a hyperechogenic layer, which was histopathologically confirmed to be fibrosis with psammoma bodies. This pattern was characteristically seen in patients with diffuse thyroiditis and hypoechogenic parenchyma with hyperechogenic layers of fibrosis seen in the background. The third pattern included hypoechogenic nodules later described by pathologists as lesions with spiculated, irregular margins surrounded by fibrotic parenchyma in patients with goiter. These observations require much larger groups of paediatric patients in multicentre studies for confirmation and the determination of molecular associations.
A histopathological assessment revealed that malignant lesions were not encapsulated. Fibrotic capsules, if partially visible, were infiltrated by the branches of the lesions. This was in contrast to usually encapsulated PTC nodules in adults (24, 27). In all of the patients, the lymphocytic infiltration around the tumour was visible. However, in patients with a normoechoic background, it was less advanced in the surrounding thyroid tissue than in patients with a hypoechoic background, where massive lymphocytic infiltration, with the formation of germinal centres within the tumour, was visible.
Oppenheimer et al. found that the subset of patients with nodular AIT who had normal background parenchyma is a particularly interesting group to consider in further research and proposed that these patients may not carry a preexisting clinical diagnosis of AIT (22). Therefore, it was suggested by other research groups that an autoimmune reaction might be secondary to developing PTC (35–38). In a study by Paparodis et al., patients with less destructive AIT were described to have a higher risk for differentiated TC than were patients with a clear destructive AIT (21). However, in our study, we were able to notice the formation of a nodule on a hypoechoic background in several patients. As reported by Lee et al., a sonographic AIT diagnosis is made based on the hypoechogenicity and heterogenicity of the thyroid gland (7). Thyroidal parenchymal stiffness takes place in patients with AIT due to the lymphocytic infiltration, fibrosis, and follicular destruction in the thyroid gland during the disease process. This can be seen on US as increased parenchymal echogenicity with time (39, 40). We suggest that we should search for lesions that are circumscribed by a fibrotic layer in these paediatric patients.
Another point of interest in this study is the observation that although all hypothyroid patients in group 1 received levothyroxine treatment and presented decreased thyroid volumes and TSH levels, this therapy failed to provide any protection from nodule development. However, in the group 1 that developed AIT we have not seen similar decrease of mean thyroid volume as in AIT control group 4. Corrias et al. and Mussa et al. presented that progressive increase in nodule diameter under levothyroxine therapy is a factor which seems to be significantly associated with the risk of malignancy, an observation reported also by other researchers (13, 14, 25, 41).
After follow-up we have seen a decrease of mean TSH in group 1 and 4. The mean TSH levels in group 1 were close to upper normal range and in the middle of the normal range in group 4. Mussa et al. and Zirilli et al. presented that persistently elevated TSH levels play an independent role as predictors of the likelihood of TC, in children and in adults (41, 42). Interestingly Mussa et al. presented that serum TSH in the upper normal range was consistently associated wih thyroid cancer in children (41). It has to be emphasized that there are no current guidelines related to the level of TSH suppression in AIT treatment in children, as a possible TC prevention, and our study was not designed to provide them. Recent studies presented however, that TSH suppressive therapy for TC is associated with increased cardiovascular risk and has a negative impact on cognition in children (43–45), therefore in our AIT patients we aimed at TSH within the normal range.
An interesting observation was related to the TPOAb and TgAb assessments. TgAb is generally used as a prognostic marker of PTC only after total thyroidectomy, but its preoperative value in patients with PTC with concomitant AIT is still unclear (46). The role of thyroid antibodies in inducing malignant transformation of the thyroid tissue, regional lymph node invasion, and even long-term disease-free survival is controversial (47–51). Jia et al. and Kim et al. have reported for the first time that positive serum TgAb is an independent predictive marker for thyroid malignancy in patients diagnosed with thyroid nodules, regardless of the presence of AIT (52, 53). Interestingly, in our study, the TgAb/TPOAb ratio was significantly lower in children with AIT than in children in whom PTC was diagnosed upon admission, independently with regards to AIT. However, in patients with PTC who were not diagnosed with AIT, both TgAb and TPOAb levels were below the lower norm. Interestingly, in the group that was actively surveilled, the TgAb/TPOAb ratio increased since the beginning of the observation period and was higher than in patients with AIT. This observation can be explained by a decrease of TPOAb level and increase in TgAb titers as seen in some children in this group, whereas in the AIT group, we observed a decrease in both TPOAb and TgAb levels.
Recent studies by Hosseini et al. and Grani et al. have also suggested the use of preoperative TgAb levels as a marker for PTC (54, 55). The causal relationship between AIT and PTC is not yet clear, and it is uncertain whether TgAb is generated by the same pathological process in both AIT and PTC. It was found that the pattern of Tg recognition differs in patients with and without AITD (35, 56, 57). The Tg epitopic regions in patients without AITD were more variable than in those with AITD. Moreover, the pattern of recognition of TgAb in patients with both PTC and AIT was more similar to that observed in those with AIT, as compared to patients with PTC (35, 56, 57).
Min et al. observed an association between high serum TgAb levels and C LNM in patients with PTC and AIT, suggesting that it can be useful in predicting LNM in these patients (51). Similarly to our observation in paediatric patients that the TgAb/TPOAb ratio is associated with angioinvasion, Min et al. identified that the TgAb/TPOAb ratio were significantly associated with the extent of the disease once the ratio index was higher than 2 in adult patients (51). Unfortunately, a small sample size precluded a more detailed analysis in our study; therefore, multicentre paediatric research is necessary to confirm this observation.
Xu et al. have reported that larger PTC lesions and LNM were significantly associated with higher TgAb, and an increasing preoperative TgAb level of up to 2000 IU/mL was associated with shorter recurrence-free survival (46). According to Li et al., although preoperative positive TPOAb and TgAb are independent predictive markers for PTC, they are also associated with milder clinicopathological features of PTC (58). In our study, however, we found that AIT was observed in 50% of operated children, but we could not confirm the association of AIT with the PTC stage in relation to LNM or ETE. The only association involving the extent of the disease was found in relation to the age, tumour diameter, and TPOAb, similarly as observed in other recent paediatric studies (59–61). In paediatric patients, Huang et al. found that preoperative positive TgAb and TPOAb were protective factors for recurrence in younger age groups but not in older patients (62).
Unlike adults, children with differentiated TC may present with more advanced disease and have a higher local recurrence and distant metastases, even though their prognosis is favourable with overall 10-y survival rates of over 90% (24). Children have a longer posttreatment life expectancy and, thus, have more time for recurrence or potential treatment side-effects to manifest (1). Recent studies also confirmed that 131I therapy is associated with an increased risk for the development of second malignancies as well as with an increase in overall mortality for patients with PTC, especially for those who were treated in childhood (63). On the other hand, inadequate treatment of the initial cancer is linked to recurrent or persistent disease, and subsequent surgeries are much more difficult and prone to complications (1). Therefore, PTC prognostics is at present an area of intense research in the field of oncology (53).
Several limitations existed in our study. Due to the rarity of PTC incidence in young patients, our sample was small and had no power to establish statistical significance. Additionally, not all of the patients had repeated all of the tests, which influenced the result.
However, strengths included the fact that at the time of writing, the authors are clinical doctors and are involved in the diagnostic and therapeutic process. Additionally, patterns of nodule recognition described by our group are of practical value in every day US practices. Similarly to adult studies, we found that the preoperative TgAb/TPOAb ratio could likely serve as a novel prognostic factor for predicting PTC in children, though this needs confirmation in multicentre studies.
The use of thyroid US focused on the search for developing tumours in the routine follow-up of patients with AIT may not only help in the early detection of thyroid malignancies that are not clinically apparent but may also influence the invasiveness of oncological therapy and reduce the future side effects of 131I therapy. We propose that the repeat evaluation of TPOAb and TgAb warrants further exploration as a strategy to determine TC susceptibility in paediatric patients with AIT in larger multicentre studies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was approved by the relevant institutional review board (The Bioethics Committee of the Jagiellonian University; opinion number:1072.6120.288.2021). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Study design: DJ. Study conduct: DJ, AT-N, AK-W, MK, MW, WG. Data collection: DJ, MK, AT-N, AK-W, MW. Data analysis: DJ, MW, MK. Data interpretation: DJ, MW, MK, AT-N, AK-W. Drafting manuscript: DJ, MW. Revising manuscript content: DJ, MW, WG, JS. Approving final version of manuscript: DJ, MW, JS, WG. DJ takes responsibility for the integrity of the data analysis.
We would like to thank Editage (www.editage.com) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Koney N, Mahmood S, Gannon A, Finkelstein MS, Mody T. Pediatric thyroid cancer: Imaging and therapy update. Curr Radiol Rep (2017) 5:48. doi: 10.1007/s40134-017-0247-3
2. Niedziela M, Handkiewicz-Junak D, Małecka-Tendera E, Czarniecka A, Dedecjus M, Lange D, et al. Diagnostics and treatment of differentiated thyroid carcinoma in children–guidelines of polish national societies. Endokrynol Pol (2016) 67:628–42. doi: 10.5603/EP.2016.0072
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin (2022) 72(1):7–33. doi: 10.3322/caac.21708
4. Zdraveska N, Kocova M. Hashimoto thyroiditis in childhood–review of the epidemiology, genetic susceptibility and clinical aspects of the disease. Maced J Med Sci (2012) 15:336–45.
5. Zois C, Stavrou I, Kalogera C, Svarna E, Dimoliatis I, Seferiadis K, et al. High prevalence of autoimmune thyroiditis in school children after elimination of iodine deficiency in northwestern Greece. Thyroid (2003) 13:485–9. doi: 10.1089/105072503322021151
6. Radetti G, Gottardi E, Bona G, Corrias A, Salardi S, Loche S. The natural history of euthyroid hashimoto’s thyroiditis in children. J Pediatr (2006) 149:827–32. doi: 10.1016/j.jpeds.2006.08.045
7. Lee SJ, Lim GY, Kim JY, Chung MH. Diagnostic performance of thyroid ultrasonography screening in pediatric patients with a hypothyroid, hyperthyroid or euthyroid goiter. Pediatr Radiol (2016) 46:104–11. doi: 10.1007/s00247-015-3435-4
8. Janus D, Wojcik M, Kalicka-Kasperczyk A, Drabik G, Wyrobek L, Wedrychowicz A, et al. Novel insights in ultrasound evaluation of thyroid gland in children with papillary thyroid carcinoma. Neuro Endocrinol Lett (2017) 38:367–74.
9. Dailey ME, Lindsay S, Skahen R. Relation of thyroid neoplasms to hashimoto disease of the thyroid gland. AMA Arch Surg (1955) 70:291–7. doi: 10.1001/archsurg.1955.01270080137023
10. Balkwill F, Mantovani A. Inflammation and cancer: Back to virchow? Lancet (2001) 357(9255):539–45. doi: 10.1016/S0140-6736(00)04046-0
11. Grivennikov SI. Inflammation and colorectal cancer: Colitis-associated neoplasia. Semin Immunopathol (2013) 35(2):229–44. doi: 10.1007/s00281-012-0352-6
12. Fung J, Lai C-L, Yuen M-F. Hepatitis b and c virus-related carcinogenesis. Clin Microbiol Infect (2009) 15(11):964–70. doi: 10.1111/j.1469-0691.2009.03035.x
13. Radetti G, Loche S, D'Antonio V, Salerno M, Guzzetti C, Aversa T, et al. Influence of hashimoto thyroiditis on the development of thyroid nodules and cancer in children and adolescents. J Endocr Soc (2019) 3(3):607–16. doi: 10.1210/js.2018-00287
14. Corrias A, Cassio A, Weber G, Mussa A, Wasniewska M, Rapa A, et al. Study group for thyroid diseases of Italian society for pediatric endocrinology and diabetology (SIEDP/ISPED). thyroid nodules and cancer in children and adolescents affected by autoimmune thyroiditis. Arch Pediatr Adolesc Med (2008) 162(6):526–31. doi: 10.1001/archpedi.162.6.526
15. Keskin M, Savas-Erdeve S, Aycan Z. Co-Existence of thyroid nodule and thyroid cancer in children and adolescents with hashimoto thyroiditis: A single-center study. Horm Res Paediatr (2016) 85(3):181–7. doi: 10.1159/000443143
16. Januś D, Wójcik M, Drabik G, Wyrobek Ł, Starzyk JB. Ultrasound variants of autoimmune thyroiditis in children and adolescents and their clinical implication in relation to papillary thyroid carcinoma development. J Endocrinol Invest (2018) 41(3):371–80. doi: 10.1007/s40618-017-0758-z
17. Aghini-Lombardi F, Antonangeli L, Martino E, Vitti P, Maccherini D, Leoli F, et al. The spectrum of thyroid disorders in an iodine-deficient community: the pescopagano survey. J Clin Endocrinol Metab (1999) 84(2):561–6. doi: 10.1210/jcem.84.2.5508
18. Rallison ML, Dobyns BM, Keating FR Jr, Rall JE, Tyler FH. Thyroid nodularity in children. JAMA (1975) 233(10):1069–72. doi: 10.1001/jama.1975.03260100039017
19. Suzuki S, Suzuki S, Fukushima T, Midorikawa S, Shimura H, Matsuzuka T, et al. Comprehensive survey results of childhood thyroid ultrasound examinations in fukushima in the first four years after the fukushima daiichi nuclear power plant accident. Thyroid (2016) 26(6):843–51. doi: 10.1089/thy.2015.0564
20. Avula S, Daneman A, Navarro OM, Moineddin R, Urbach S, Daneman D. Incidental thyroid abnormalities identified on neck US for non-thyroid disorders. Pediatr Radiol (2010) 40(11):1774–80. doi: 10.1007/s00247-010-1684-9
21. Paparodis R, Imam S, Todorova-Koteva K, Staii A, Jaume JC. Hashimoto’s thyroiditis pathology and risk for thyroid cancer. Thyroid (2014) 24(7):1107–14. doi: 10.1089/thy.2013.0588
22. Oppenheimer DC, Giampoli E, Montoya S, Patel S, Dogra V. Sonographic features of nodular hashimoto thyroiditis. Ultrasound Q (2016) 32:271–6. doi: 10.1097/RUQ.0000000000000228
23. Tamimi DM. The association between chronic lymphocytic thyroiditis and thyroid tumours. Int J Surg Pathol (2002) 10:141–6. doi: 10.1177/106689690201000207
24. Lebbink CA, Links TP, Czarniecka A, Dias RP, Elisei R, Izatt L, et al. European Thyroid association guidelines for the management of pediatric thyroid nodules and differentiated thyroid carcinoma. Eur Thyroid J (2022) 11(6):e220146. doi: 10.1530/ETJ-22-0146
25. Januś D, Wójcik M, Taczanowska A, Sołtysiak P, Wędrychowicz A, Roztoczyńska D, et al. Follow-up of parenchymal changes in the thyroid gland with diffuse autoimmune thyroiditis in children prior to the development of papillary thyroid carcinoma. J Endocrinol Invest (2019) 42(3):261–70. doi: 10.1007/s40618-018-0909-x
26. Huang J, Ngai CH, Deng Y, Pun CN, Lok V, Zhang L, et al. NCD research group, global health, association of pacific rim universities (APRU). incidence and mortality of thyroid cancer in 50 countries: a joinpoint regression analysis of global trends. Endocrine (2023) 6. doi: 10.1007/s12020-022-03274-7
27. Jung CK, Bychkov A, Kakudo K. Update from the 2022 world health organization classification of thyroid tumours: A standardized diagnostic approach. Endocrinol Metab (Seoul) (2022) 37(5):703–18. doi: 10.3803/EnM.2022.1553
28. Dinauer CA, Breuer C, Rivkees SA. Differentiated thyroid cancer in children: diagnosis and management. Curr Opin Oncol (2008) 20(1):59–65. doi: 10.1097/CCO.0b013e3282f30220
29. Jarząb B, Dedecjus M, Lewiński A, Adamczewski Z, Bakuła-Zalewska E, Bałdys-Waligórska A, et al. Diagnosis and treatment of thyroid cancer in adult patients - recommendations of polish scientific societies and the national oncological strategy. 2022 update. Endokrynol Pol (2022) 73(2):173–300. doi: 10.5603/EP.a2022.0028
30. Russ G, Bonnema SJ, Erdogan MF, Durante C, Ngu R, Leenhardt L. European Thyroid association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: The EU-TIRADS. Eur Thyroid J (2017) 6(5):225–37. doi: 10.1159/000478927
31. Cibas ES, Ali SZ. The Bethesda system for reporting thyroid cytopathology. Thyroid (2009) 19:1159–65. doi: 10.1089/thy.2009.0274
32. Szybiński Z, Trofimiuk-Müldner M, Buziak-Bereza M, Walczycka L, Hubalewska-Dydejczyk A. Reference values for thyroid volume established by ultrasound in polish school children. Endokrynol Pol (2012) 63:104–9.
33. World health organization and international council for control of iodine deficiency disorders recommended normative values for thyroid volume in children aged 6–15 years. Bull World Health Organ (1997) 75:95–7.
34. Rizzo M, Sindoni A, Talamo Rossi R, Bonaffini O, Panetta S, Scisca C, et al. Annual increase in the frequency of papillary thyroid carcinoma as diagnosed by fine-needle aspiration at a cytology unit in Sicily. Horm. (Athens) (2013) 12:46–57. doi: 10.1007/BF03401286
35. Latrofa F, Ricci D, Grasso L, Vitti P, Masserini L, Basolo F, et al. Characterization of thyroglobulin epitopes in patients with autoimmune and non-autoimmune thyroid diseases using recombinant human monoclonal thyroglobulin autoantibodies. J Clin Endocrinol Metab (2008) 93:591–6. doi: 10.1210/jc.2007-1199
36. Ehlers M, Schott M. Hashimoto’s thyroiditis and papillary thyroid cancer: are they immunologically linked? Trends Endocrinol Metab (2014) 25:656–64. doi: 10.1016/j.tem.2014.09.001
37. Anderson L, Middleton WD, Teefey SA, Reading CC, Langer JE, Desser T, et al. Hashimoto thyroiditis: part 1, sonographic analysis of the nodular form of hashimoto thyroiditis. AJR Am J Roentgenol (2010) 195:208–15. doi: 10.2214/AJR.09.2459
38. Imam S, Paparodis R, Sharma D, Jaume JC. Lymphocytic profiling in thyroid cancer provides clues for failure of tumour immunity. Endocr Relat Cancer (2014) 21:505–16. doi: 10.1530/ERC-13-0436
39. Yoshida A, Adachi T, Noguchi T, Urabe K, Onoyama S, Okamura Y, et al. Echographic findings and histological feature of the thyroid: a reverse relationship between the level of echo-amplitude and lymphocytic infiltration. Endocrinol Jpn (1985) 32:681–90. doi: 10.1507/endocrj1954.32.681
40. Marcocci C, Vitti P, Cetani F, Catalano F, Concetti R, Pinchera A. Thyroid ultrasonography helps to identify patients with lymphocytic thyroiditis who are prone to develop hypothyroidism. J Clin Endocrinol Metab (1991) 72:209–13. doi: 10.1210/jcem-72-1-209
41. Mussa A, De Andrea M, Motta M, Mormile A, Palestini N, Corrias A. Predictors of malignancy in children with thyroid nodules. J Pediatr (2015) 167:886–92. doi: 10.1016/j.jpeds.2015.06.026
42. Zirilli G, Salzano G, Corica D, Pajno GB, Mignosa C, Pepe G, et al. Thyrotropin serum levels and coexistence with hashimoto's thyroiditis as predictors of malignancy in children with thyroid nodules. Ital J Pediatr (2019) 45(1):96. doi: 10.1186/s13052-019-0693-z
43. Yang X, Guo N, Gao X, Liang J, Fan X, Zhao Y. Meta-analysis of TSH suppression therapy and the risk of cardiovascular events after thyroid cancer surgery. Front Endocrinol (Lausanne) (2022) 22:991876. doi: 10.3389/fendo.2022.991876
44. Links TP, van der Boom T, Zandee WT, Lefrandt JD. Cardiovascular effects of overt and subclinical hyperthyroidism: focus on differentiated thyroid cancer. Endocr Connect (2021) 10(1):R43–51. doi: 10.1530/EC-20-0539
45. Wu T, Flowers JW, Tudiver F, Wilson JL, Punyasavatsut N. Subclinical thyroid disorders and cognitive performance among adolescents in the united states. BMC Pediatr (2006) 19:6. doi: 10.1186/1471-2431-6-12
46. Xu S, Huang H, Qian J, Wang X, Xu Z, Liu S, et al. Prognostic value of the preoperative and early trends in postoperative serum thyroglobulin antibody levels among patients with papillary thyroid carcinoma and concomitant hashimoto’s thyroiditis. Endocrine (2022) 19. doi: 10.1007/s12020-022-03283-6
47. Song E, Jeon MJ, Park S, Kim M, Oh HS, Song DE, et al. Influence of coexistent hashimoto’s thyroiditis on the extent of cervical lymph node dissection and prognosis in papillary thyroid carcinoma. Clin Endocrinol (Oxf) (2018) 88(1):123–35. doi: 10.1111/cen.13475
48. Marotta V, Sciammarella C, Chiofalo MG, Gambardella C, Bellevicine C, Grasso M, et al. Hashimoto’s thyroiditis predicts outcome in intrathyroidal papillary thyroid cancer. Endocr Relat Cancer (2017) 24(9):485–93. doi: 10.1530/ERC-17-0085
49. Graceffa G, Patrone R, Vieni S, Campanella S, Calamia S, Laise I, et al. Association between hashimoto’s thyroiditis and papillary thyroid carcinoma: A retrospective analysis of 305 patients. BMC Endocr Disord (2019). doi: 10.1186/s12902-019-0351-x
50. Ralli M, Angeletti D, Fiore M, D’Aguanno V, Lambiase A, Artico M, et al. Hashimoto’s thyroiditis: An update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation. Autoimmun Rev (2020) 19(10):102649. doi: 10.1016/j.autrev.2020.102649
51. Min Y, Huang Y, Wei M, Wei X, Chen H, Wang X, et al. Preoperatively predicting the central lymph node metastasis for papillary thyroid cancer patients with hashimoto’s thyroiditis. Front Endocrinol (Lausanne) (2021) 22:713475. doi: 10.3389/fendo.2021.713475
52. Kim ES, Lim DJ, Baek KH, Lee JM, Kim MK, Kwon HS, et al. Thyroglobulin antibody is associated with increased cancer risk in thyroid nodules. Thyroid (2010) 20:885–91. doi: 10.1089/thy.2009.0384
53. Jia X, Pang P, Wang L, Zhao L, Jiang L, Song Y, et al. Clinical analysis of preoperative anti-thyroglobulin antibody in papillary thyroid cancer between 2011 and 2015 in Beijing, China: A retrospective study. Front Endocrinol (Lausanne) (2020) 15:452. doi: 10.3389/fendo.2020.00452
54. Grani G, Calvanese A, Carbotta G, D’Alessandri M, Nesca A, Bianchini M, et al. Thyroid autoimmunity and risk of malignancy in thyroid nodules submitted to fine-needle aspiration cytology. Head Neck (2015) 37:260–4. doi: 10.1002/hed.23587
55. Hosseini S, Payne RJ, Zawawi F, Mlynarek A, Hier MP, Tamilia M, et al. Can preoperative thyroglobulin antibody levels be used as a marker for well differentiated thyroid cancer? J Otolaryngol Head Neck Surg (2016) 45:31. doi: 10.1186/s40463-016-0143-5
56. Lupoli GA, Okosieme OE, Evans C, Clark PM, Pickett AJ, Premawardhana LD, et al. Prognostic significance of thyroglobulin antibody epitopes in differentiated thyroid cancer. J Clin Endocrinol Metab (2015) 100:100–8. doi: 10.1210/jc.2014-2725
57. Okosieme OE, Evans C, Moss L, Parkes AB, Premawardhana LD, Lazarus JH. Thyroglobulin antibodies in serum of patients with differentiated thyroid cancer: relationship between epitope specificities and thyroglobulin recovery. Clin Chem (2005) 51:729–34. doi: 10.1373/clinchem.2004.0445
58. Li L, Shan T, Sun X, Lv B, Chen B, Liu N, et al. Positive thyroid peroxidase antibody and thyroglobulin antibody are associated with better clinicopathologic features of papillary thyroid cancer. Endocr Pract (2021) 27(4):306–11. doi: 10.1016/j.eprac.2020.10.017
59. Thiesmeyer JW, Egan CE, Greenberg JA, Beninato T, Zarnegar R, Fahey Iii TJ, et al. Prepubertal children with papillary thyroid carcinoma present with more invasive disease than adolescents and young adults. Thyroid (2022) 9. doi: 10.1089/thy.2022.0098
60. He Y, Li H, Wang K, Wang J, Zhu Y, Ni S, et al. Fourteen years old as the best age cutoff to differentiate prepubertal from pubertal papillary thyroid carcinoma.s. Head Neck (2023) 45(1):85–94. doi: 10.1002/hed.27208
61. Keefe G, Culbreath K, Cherella CE, Smith JR, Zendejas B, Shamberger RC, et al. Autoimmune thyroiditis and risk of malignancy in children with thyroid nodules. Thyroid (2022) 32(9):1109–17. doi: 10.1089/thy.2022.0241
62. Huang D, Zhi J, Zhang J, Qin X, Zhao J, Zheng X, et al. Relationship between thyroid autoantibodies and recurrence of papillary thyroid carcinoma in children and adolescents. Front Oncol (2022) 8:883591. doi: 10.3389/fonc.2022.883591
Keywords: autoimmune thyroiditis, papillary thyroid carcinoma, ultrasonography of thyroid gland, TgAb/TPOAb ratio, hypoechogenic thyroid nodules
Citation: Januś D, Kujdowicz M, Wójcik M, Taczanowska-Niemczuk A, Kiszka-Wiłkojć A, Górecki W and Starzyk JB (2023) Ultrasound evolution of parenchymal changes in the thyroid gland with autoimmune thyroiditis in children prior to the development of papillary thyroid carcinoma – a follow-up study. Front. Endocrinol. 14:1172823. doi: 10.3389/fendo.2023.1172823
Received: 23 February 2023; Accepted: 29 March 2023;
Published: 12 April 2023.
Edited by:
Malgorzata Gabriela Wasniewska, University of Messina, ItalyReviewed by:
Domenico Corica, University of Messina, ItalyCopyright © 2023 Januś, Kujdowicz, Wójcik, Taczanowska-Niemczuk, Kiszka-Wiłkojć, Górecki and Starzyk. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dominika Januś, ZG9taW5pa2EuamFudXNAdWouZWR1LnBs
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.