
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 23 May 2023
Sec. Cancer Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1156680
This article is part of the Research Topic Endocrine Aspects of Gynaecological Cancers View all 9 articles
 Cylia Dahmani1Patrick Caron1
Cylia Dahmani1Patrick Caron1 David Simonyan2
David Simonyan2 Véronique Turcotte1Jean Grégoire3Marie Plante3
Véronique Turcotte1Jean Grégoire3Marie Plante3 Chantal Guillemette1,4*
Chantal Guillemette1,4*Context: Recent evidence support that androgens play an important role in the etiology of endometrial cancer (EC). Adrenal-derived 11-oxygenated androgens are highly potent agonists of the androgen receptor (AR), comparable to testosterone (T) and dihydrotestosterone (DHT) that have not been studied in the context of EC.
Methodology: We studied a cohort of 272 newly diagnosed postmenopausal EC cases undergoing surgical treatment. Circulating concentrations of seven 11-oxygenated androgens including precursors, potent androgens and their metabolites were established in serum samples collected before and 1 month after surgery using a validated liquid chromatography tandem mass spectrometry method (LC-MS/MS). Free (unconjugated) and total (free + sulfate and glucuronide conjugates following enzymatic hydrolysis) were analyzed in relation to clinicopathological features, recurrence and disease-free survival (DFS).
Results: Levels of 11-oxygenated androgens were weakly correlated to those of canonical androgens such as testosterone (T) and dihydrotestosterone (DHT), with no evidence of their association with clinicopathological features. Levels of 11-oxygenated androgens declined after surgery but remained higher in overweight and obese compared to normal weight cases. Higher levels of preoperative free 11-ketoandrosterone (11KAST) were associated with an increased risk of recurrence (Hazard ratio (HR) of 2.99 (95%CI=1.09-8.18); P=0.03). Postoperative free 11β-hydroxyandrosterone (11OHAST) levels were adversely associated with recurrence and DFS (HR = 3.23 (1.11-9.40); P=0.03 and 3.27 (1.34-8.00); P=0.009, respectively).
Conclusion: 11-oxygenated androgen metabolites emerge as potential prognostic markers of EC.
Endometrial cancer (EC) is the most common gynecological cancer in the Western world, predominantly affecting postmenopausal women (1). The majority of cases is diagnosed at an early stage and presents a favorable prognosis. Hysterectomy is the first line treatment for cases with localized tumors, however, a subset of patients experience recurrence. EC is a hormone-dependent cancer, in which sex steroid hormones, and particularly estrogens, play a major role.
Studies ascertained the relationships between circulating adrenal precursors, androgens and/or estrogens as well as germline variations in steroid-related biosynthesis pathways with the risk of EC (2). However, knowledge remains limited regarding the relation between circulating steroid levels and prognosis for EC patients. One study of 246 EC cases showed that higher preoperative serum levels of the estrogen precursor estrone-sulfate (E1-S) and estradiol (E2) metabolites were associated with recurrence after hysterectomy and shorter overall survival (3). Another study evidenced that lower plasma levels of androstenedione (A4), the precursor of E1, were associated with aggressive tumor characteristics and poor survival in 100 EC cases (4). In a limited series of 19 EC cases with shorter survival that died within 3 years after diagnosis, lower preoperative levels of E1-S as well as the adrenal derived androgen precursor dehydroepiandrosterone (DHEA) and its sulfated derivative DHEA-S were observed, compared to 19 EC cases with prolonged survival, with no evidence of differences for E2 between groups (5). After menopause, the adrenal glands secrete DHEA and A4 as the main precursors of potent androgen (AR) and estrogen (ER) receptor ligands, and their levels decline with age (6). Aromatization of androgens to estrogens is very active in the adipose tissues and as a result, body mass index (BMI) is directly correlated with E1 and E2 levels in postmenopausal women (3). Levels of androgens such as testosterone (T) and dihydrotestosterone (DHT) have also been shown to increase in EC cases, both in endometrioid and non-endometrioid diseases (3, 7). In addition to their aromatization to estrogens in multiple sites including adipose and uterine tissues (8–11), androgens and AR signaling pathway may play different roles in EC (12–14). Both oncogenic and tumor suppressive roles have been reported along with variable AR expression levels depending on the stage of disease (15, 16). In EC cell models, evidence suggests interference with the progestin signaling, promotion of cell proliferation and drug resistance, although with inconsistent results (17–20). These findings reinforce the need to examine whether additional androgens and AR-ligands influence EC prognosis.
Recent studies showed that circulating levels of non-canonical 11-oxygenated androgens originating primarily in the adrenal gland do not decline with age (21, 22). Their biosynthesis arises from the precursor 11β-hydroxyandrostenedione (11OHA4) and 11-ketoandrostenedione (11KA4) to produce 11-ketotestosterone (11KT), 11β-hydroxytestosterone (11OHT) and 11-ketodihydrotestosterone (11KDHT) with androgenic activity, representing additional AR ligands (23, 24). Their metabolites 11-ketoandrosterone (11KAST) and mainly 11β-hydroxyandrosterone (11OHAST) are also abundant in circulation of healthy men and women (21). In a recent publication that measured all seven of them using a validated mass spectrometry (MS) assay (21), 11-oxygenated androgens were associated with poor prognosis in a cohort of 1793 men with localized prostate cancer undergoing prostatectomy (25). Other studies using either non validated and validated assays (discussed in reference 21), reported few of these non-canonical 11-oxygenated androgens in a number of other clinical conditions, including androgen excess conditions, Cushing’s syndrome and congenital adrenal hyperplasia, all using validated MS methods (24, 26–29).
In this study, we sought to provide a detailed assessment of both free and total circulating levels of 11-oxygenated androgens in EC cases, measured in preoperative and postoperative blood specimens by MS, and establish their link with canonical androgens, BMI, poor prognostic features, recurrence and disease-free survival (DFS) after surgery. We studied a prospective cohort of 272 postmenopausal EC cases undergoing hysterectomy. Data exposed that circulating 11-oxygenated androgen metabolites are linked to adverse outcomes in EC cases, independent of established prognostic features, suggesting their role in EC progression.
All patients were recruited at The Hôtel-Dieu de Québec Hospital (Québec City, Canada), between 2002 and 2013. To be included in the study, women had to be postmenopausal, undergoing surgery for EC (hysterectomy and bilateral salpingo-oophorectomy), and not having taken hormone-replacement therapy (HRT) in the three weeks prior to surgery. Demographic information and anthropometric data were collected through a nurse-administered questionnaire, including HRT. A pathologist assessed histopathological characteristics of each hysterectomy specimen. The assembling and review of medical records was performed by one of the treating gynecologic oncologists (JG). Blood sampling were performed early morning the day of surgery and approximately one month later as part of a follow-up appointment. This cohort has also been described in more details previously (3). All participants provided a written informed consent for their participation in the study and the use of their specimens, and the protocol was evaluated and approved by the local Ethical Research Committee (CHUQc-UL #2012-993).
Quantification of circulating 11-oxygenated androgens was performed using a recently validated liquid chromatography tandem mass spectrometry (LC-MS/MS) assay using deuterated steroids as internal standard, as described in our previous work (21). Briefly, we used 200 µl of serum to quantify 11OHA4, 11KA4, 11OHT, 11KT, 11KDHT, 11OHAST and 11KAST, analyzed in a blinded fashion. Sample preparation consisted of a liquid-liquid extraction followed by chemical hydroxylamine derivatization (21). Prior to extraction, an enzymatic hydrolysis treatment was performed using β-glucuronidase/sulfatase overnight at 37C° to measure total 11-oxygenated androgens, corresponding to the sum of unconjugated and conjugated forms (sulfates + glucuronides) of steroids, as described (21). For measurement of free or unconjugated 11-oxygenated androgens, this hydrolysis step was omitted. Quality controls were included in each run, and coefficients of variation for each metabolite were <10%. Lower limits of quantification were 10 pg/mL and 20 pg/mL for free (unconjugated) and total (unconjugated and conjugated) fractions, respectively. Levels of canonical steroids assessed by LC-MS/MS were available from our previous study of the same EC cohort (3).
Data were described as means, SD, confidence intervals (CI 95%), medians, and ranges, and categorical variables as frequencies and percentages. Categorical data were compared by Chi-square (χ2) tests or Fisher’s exact tests. Logarithmic transformation (with natural log values) was used for statistics to normalize skewed distribution of 11-oxygenated concentrations. Differences in 11-oxygenated androgen levels between groups were assessed using the analysis of covariance (ANCOVA). In pairwise comparisons of more than two groups, the Tukey-Kramer post hoc test was used. Variations in repeated measures of 11-oxygenated androgens between paired blood samples collected early morning were available for 186 cases (e.g. matched preoperative and postoperative samples) and analyzed using Wilcoxon signed rank test, as performed in our previous study similar in scope (3). Spearman correlations were estimated between steroids. The association between circulating 11-oxygenated androgens levels and outcomes (recurrence and survival) was estimated by univariable analyses using Kaplan-Meier and survival differences between groups compared with log-rank test. Multivariable analyses were performed by using Cox proportional-hazard models (HR). The statistical model was adjusted for age, BMI, histological type, myometrial invasion and SHBG levels, as performed in our previous study (3). Covariables were also specified in the legends of figures and tables. DFS was defined as the time from date of primary treatment (surgery) to the time of cancer recurrence/death. Two-sided P value less than 0.05 were considered statistically significant. Because of exploratory nature of study, all finding were considered hypothesis generating, adjustment for multiple testing correction was not performed. All statistical analyses were performed using SAS Statistical Software v.9.2. and graphs with GraphPad v.9.3.1.
A prospective cohort of 272 postmenopausal women newly diagnosed with EC and all treated by hysterectomy was studied (Figure 1). The mean follow-up time was 60.5 months after hysterectomy and included thirty patients that experienced recurrence (11%). Serum samples were available prior to and after surgery for most cases, as indicated in Figure 1. Clinical features are depicted in Table 1. Cases were mostly type I adenocarcinoma (82%) and with 18% type II (histologically characterized by serous, clear cell, mucinous, or mixed carcinomas). Adverse histological features including myoinvasive tumors, the presence of metastatic node and lymph-vascular space invasion, were associated with DFS and recurrence but not BMI (Table 2). Poor prognosis based on preoperative risk classification was categorized as low (type I low grade G1 and G2) and high (type I high grade G3 and type II) risk groups, with most relapse cases occurring in the high-risk group (Table 2).

Figure 1 Flow chart of the study cohort and available serum specimens.

Table 1 Clinicopathological features of endometrial cancer (EC) cases undergoing hysterectomy.
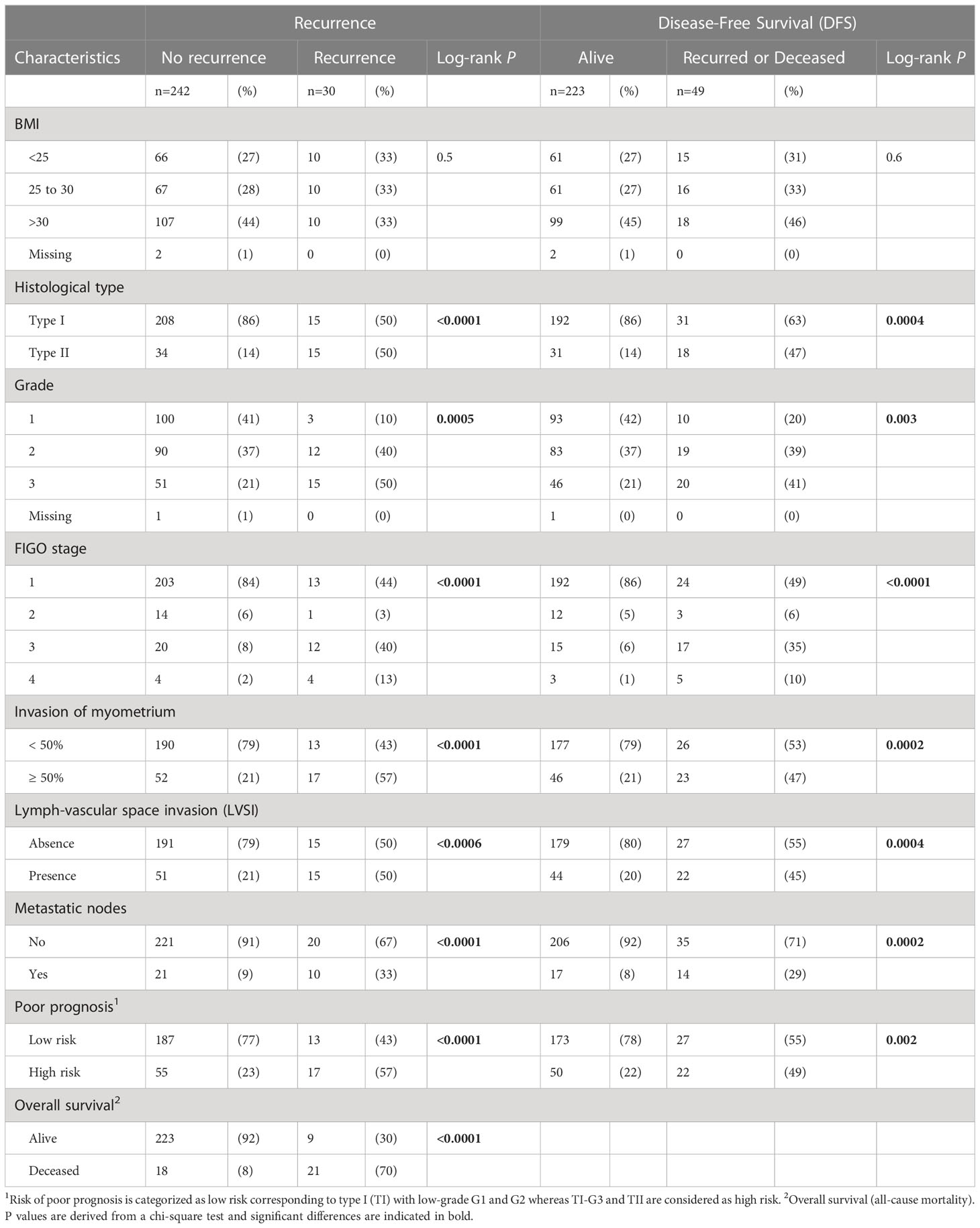
Table 2 Clinicopathological features of EC cases undergoing surgery for curative intent in relation to recurrence and survival.
Seven 11-oxygenated androgens were measured by MS in serum samples collected early morning, the day of surgery and one month after. Steroids measured included two 11-oxygenated precursors (11OHA4 and 11KA4), full agonists 11KT and 11KDHT, partial agonist 11OHT, and their metabolites 11OHAST and 11KAST (Figure 2). For each steroid, free (unconjugated) and total (free + conjugated) 11-oxygenated androgens were reported. The majority of 11-oxygenated androgens were detected above LLOQ, except free 11KAST detected in 49% preoperative (130/263) and 31% postoperative (70/224) serums (Table 3). When limited to 186 cases with paired preoperative and postoperative specimens, similar observations were noted. Another exception is the AR agonist 11KDHT that was detected in 13% preoperative serums (34/263) as total 11KDHT, and not detected above LLOQ for free/unconjugated 11KDHT. In cases with detectable total 11KDHT, we also observed higher free preoperative 11OHAST compared to cases with no detectable 11KDHT (median levels of 115 vs 92 pg/ml; P = 0.018), whereas levels of 11KAST were not significantly different. The unconjugated adrenal precursor 11OHA4 was the predominant 11-oxygenated androgen in circulation of EC cases before surgery, representing 73% of all measured 11-oxygenated androgens while free 11OHT and 11KT represented 16% (Figure 3A). The levels of the free metabolites 11OHAST and 11KAST were less abundant (4% of all measured 11-oxygenated androgens). When assessing the total fraction comprising free and conjugated steroids, levels of the most abundant total 11OHAST represented 83% of all 11-oxygenated androgens measured. In postoperative serums, a similar distribution of 11-oxygenated androgens was observed (Figure 3B). Compared to preoperative levels of free 11-oxgenated androgens, those assessed after surgery for the same cases were reduced by 11 to 33% (P < 0.001) (Table 4; Figure 4), a finding replicated in the analysis of all samples.
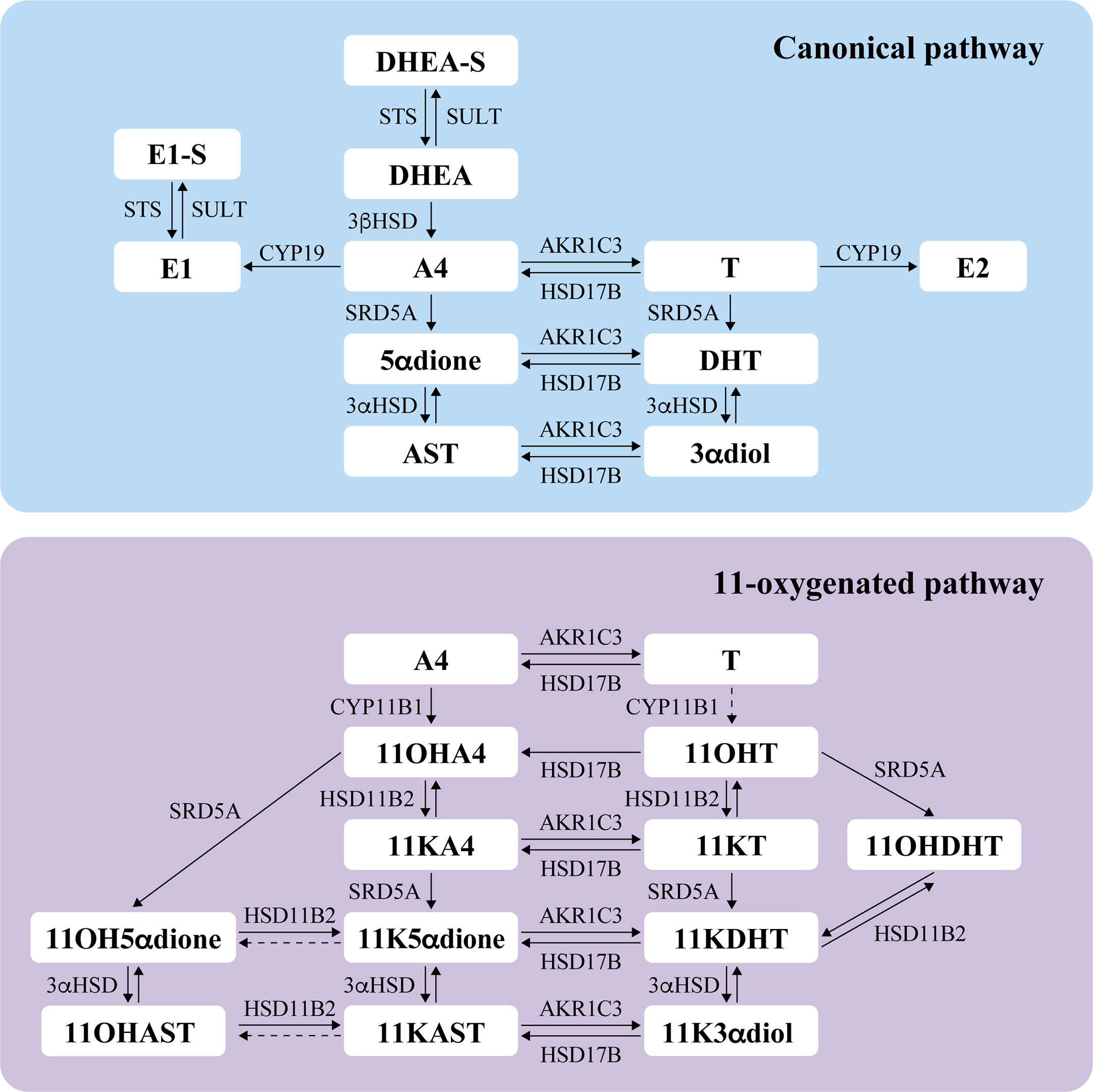
Figure 2 Schematic overview of steroidogenesis depicting the canonical and 11-oxygenated androgen pathways, based on data from the literature (23, 24, 29–38). Steroids assessed in this study are indicated in bold. The dotted arrow between T and 11OHT indicates an unfavorable reaction; A4 is the preferred substrate of CYP11B1 compared to T (30). The dotted arrows for the conversion of 11KAST to 11OHAST and 11K5αdione to 11OH5αdione represent biotransformation inconsistently reported in the literature (33, 34, 36, 39). DHEA, dehydroepiandrosterone; DHEA-S, dehydroepiandrosterone sulfate; A4, androstenedione; 5αdione, 5α-androstanedione; AST, androsterone; T, testosterone; DHT, 5α-dihydrotestosterone; 3αdiol, 5α-androstane-3α,17β-diol; E1, estrone; E1-S, estrone sulfate; E2, estradiol; 11OHA4, 11-hydroxyandrostenedione; 11KA4, 11-keto-androstenedione; 11OHT, 11-hydroxytestosterone; 11KT, 11-keto-testosterone; 11OHDHT, 11-hydroxydihydrotestosterone; 11KDHT, 11-keto-dihydrotestosterone; 11OH5αdione, 11β-hydroxy-5α-androstanedione; 11K5αdione, 11-keto-5α-androstanedione; 11OHAST, 11-hydroxyandrosterone; 11KAST, 11-keto-androsterone; 11K3αdiol, 11-keto-5α-androstane-3α,17β-diol. STS, steroid sulfatase; SULT, sulfotransferase; 3βHSD, 3β–hydroxysteroid dehydrogenase; SRD5A, 5α reductase; 3αHSD, 3α-hydroxysteroid dehydrogenase; AKR1C3, aldo-keto reductase family 1 member C3 (also known as 17β-hydroxysteroid dehydrogenase type 5); HSD17B, 17β-hydroxysteroid dehydrogenase; CYP19, aromatase; CYP11B1, cytochrome P450 11β-hydroxylase member 1; HSD11B2, 11β-hydroxysteroid dehydrogenase type 2.
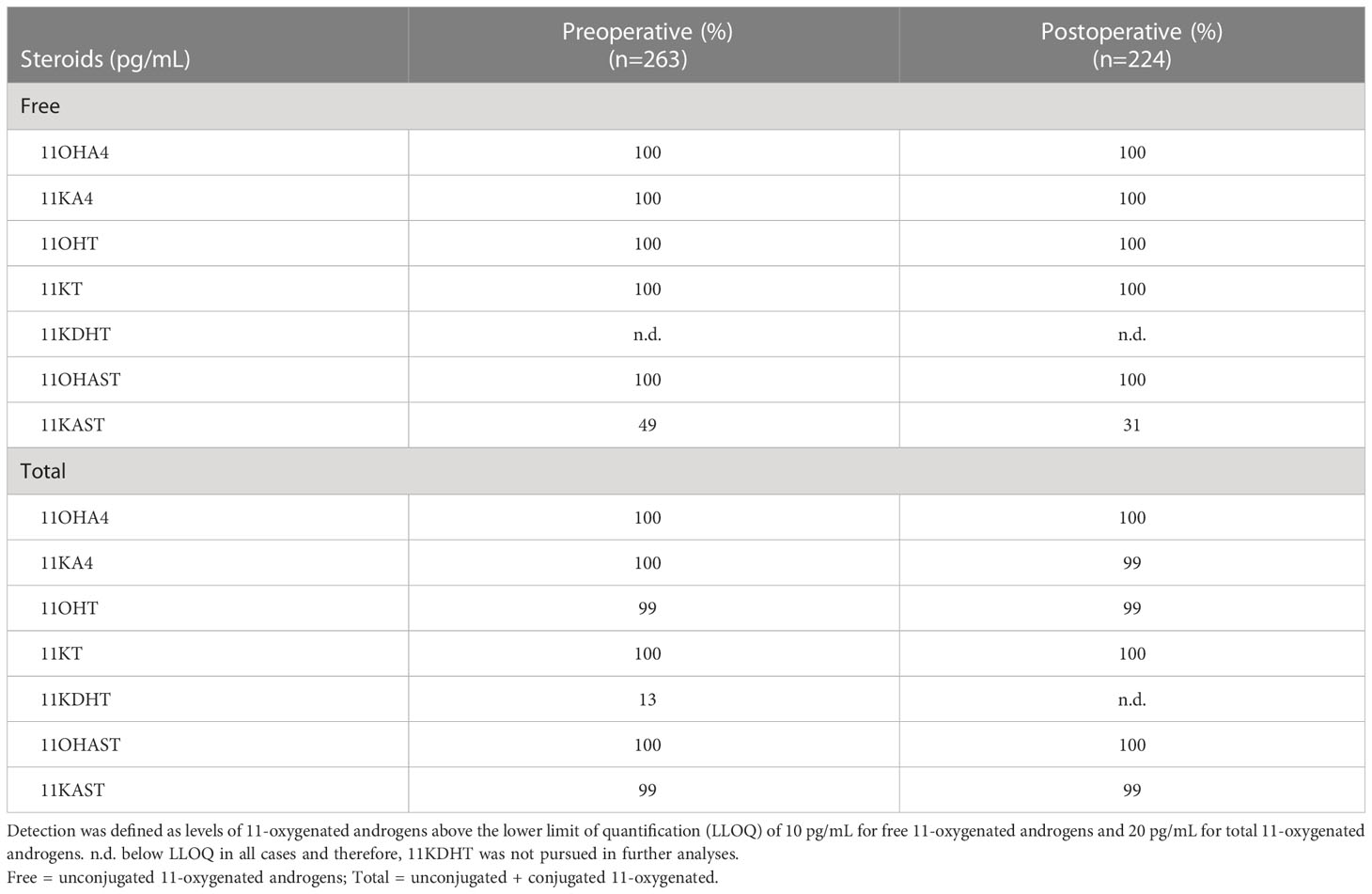
Table 3 Percent of detection (%) of 11-oxygenated androgens measured by mass spectrometry in preoperative and postoperative serums of endometrial cancer cases.
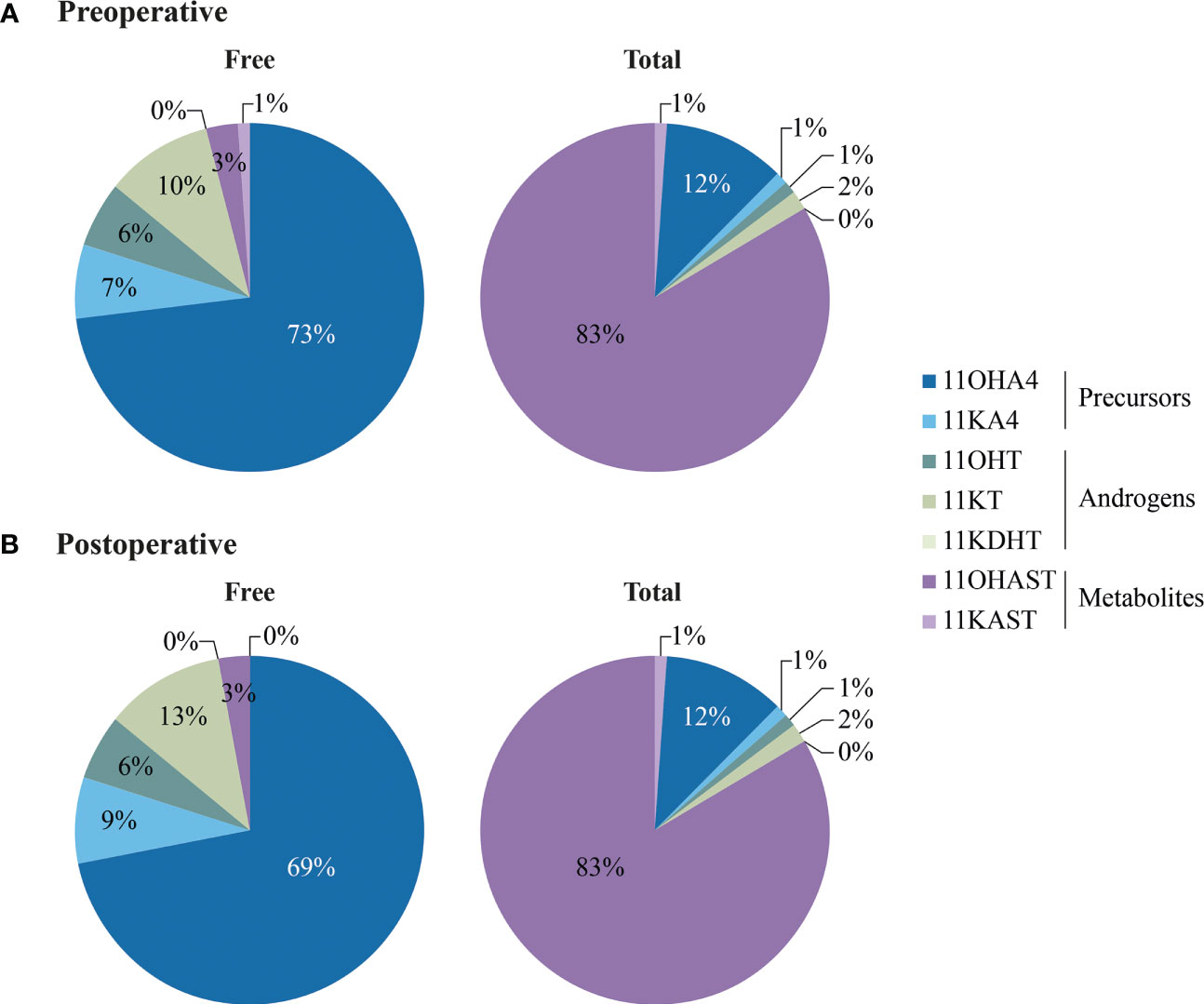
Figure 3 Pie charts showing the distribution of free (unconjugated) and total (unconjugated+ conjugated) 11-oxygenated androgens in preoperative (A) and postoperative (B) serums of EC cases. Steroid concentrations are presented in Table 4.
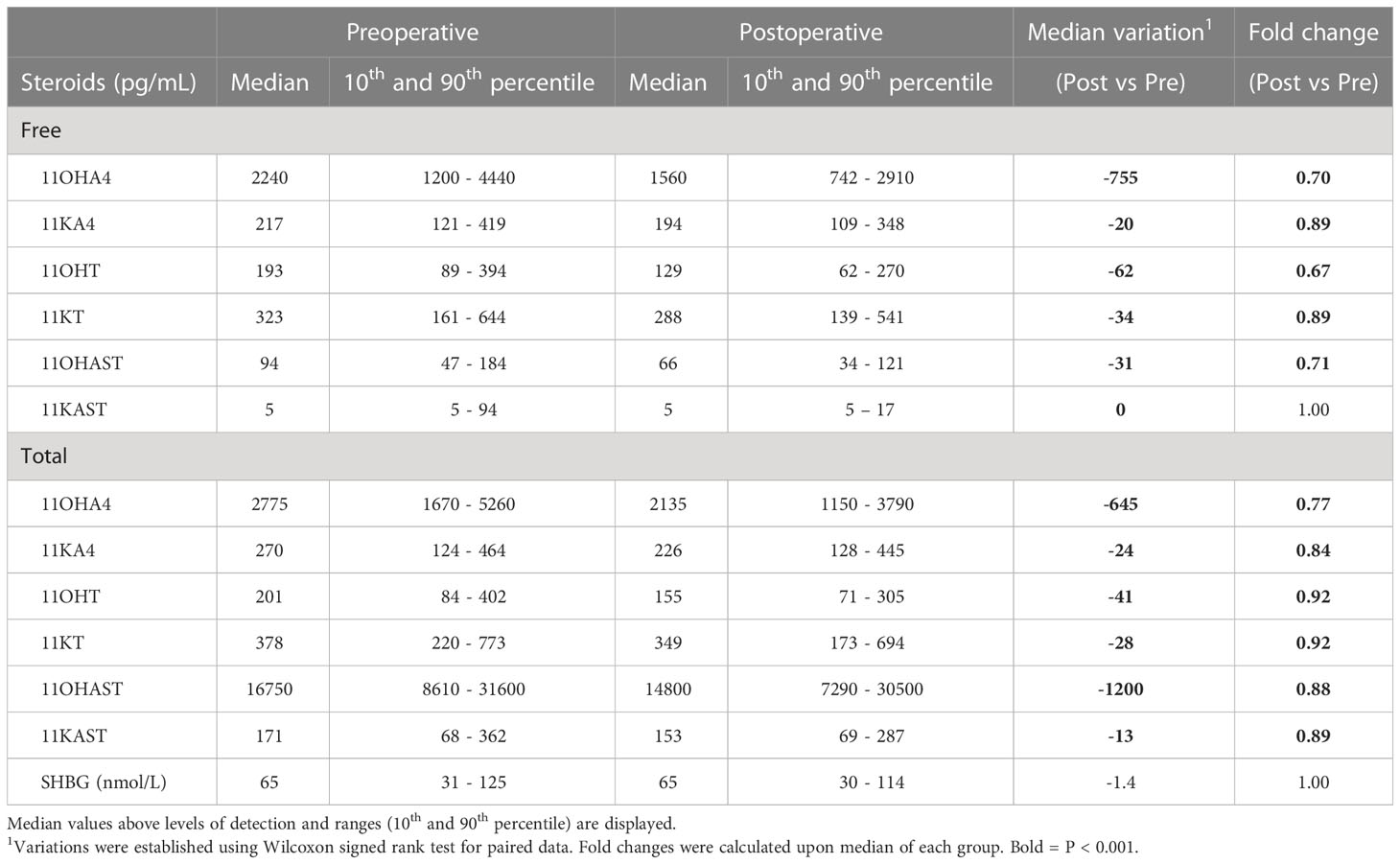
Table 4 Comparison of median (10th and 90th percentile) levels of steroids in paired preoperative and postoperative serums from 186 endometrial cancer cases.
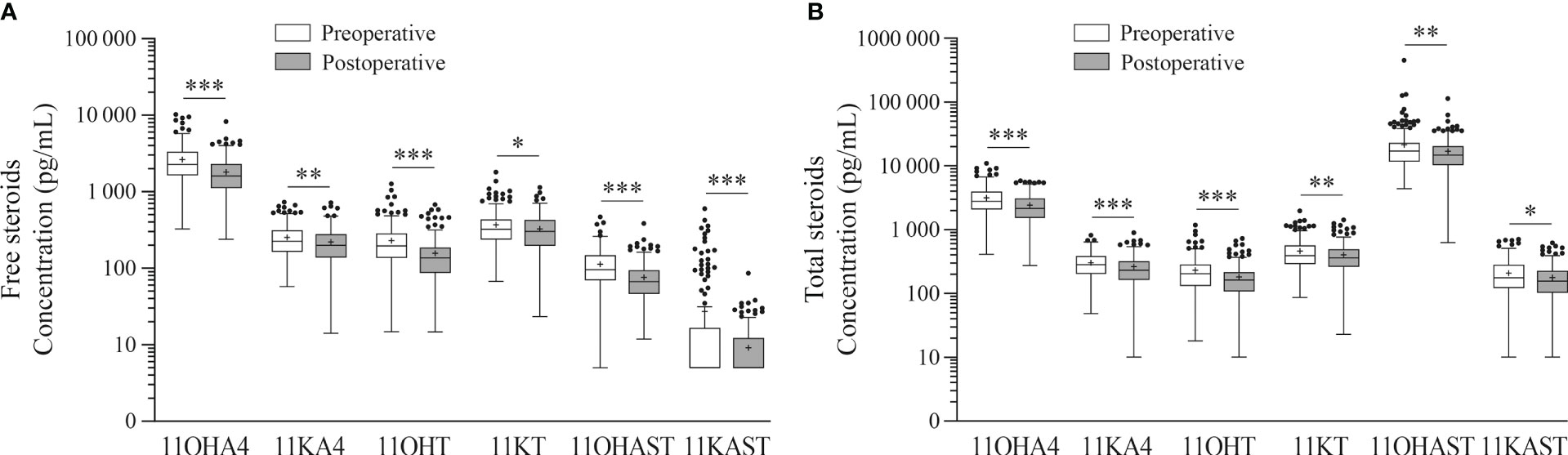
Figure 4 Comparison between preoperative and postoperative circulating levels of 11-oxygenated androgens. Free (unconjugated) (A) and total (free + conjugated (sulfates + glucuronides)) (B) 11-oxygenated androgens are depicted. Preoperative (white boxes) and postoperative (gray boxes) 11-oxygenated steroids were measured in serums from paired preoperative and postoperative paired samples of 186 EC cases. Box plot depicts 25-75 percentile and whiskers with the median are shown as solid lines and mean shown as +. Levels of 11-oxygenated androgens were log transformed and adjusted for age and BMI for statistics. * P< 0.05. ** P< 0.01. *** P< 0.001.
Levels of free 11-oxygenated androgens were weakly correlated to BMI (r ≤ 0.25), except for 11OHT that displayed slightly higher correlation values (r = 0.38 and 0.35 for preoperative and postoperative levels, respectively (P < 0.001) (Supplementary Table 1). Using BMI categories, we also noted that levels of preoperative 11-oxygenated androgens and most particularly 11OHT, were higher for overweight (1.1 to 2.1-fold; BMI 25 to 29.9 kg/m2; P < 0.05) and obese EC cases (1.2 to 2.1-fold; BMI > 30 kg/m2; P < 0.05), compared to those with normal weight (BMI <25 kg/m2) (Supplementary Table 2). After surgery, most 11-oxygenated androgens remained individually higher for overweight (1.1-1.5-fold; BMI 25 to 29.9 kg/m2; P < 0.05) and obese EC cases (1.2 to 1.6-fold; BMI > 30 kg/m2; P < 0.05), compared to those with normal weight (BMI <25 kg/m2) (Supplementary Table 3).
Preoperative levels of 11-oxygenated androgens were strongly correlated (Figure 5A). The strongest correlations were observed for precursors 11OHA4 and 11KA4 and the androgenic 11OHT and 11KT (r = 0.61-0.77; P < 0.001). Levels of 11OHAST and 11KAST metabolites displayed weak to moderate correlations with the 11-oxygenated precursors and the androgenic 11KT (r = 0.28-0.49; P < 0.001). These correlations remained significant after surgery, although they were weaker between precursors and 11-oxygenated androgens metabolites (Figure 5B). We further assessed the relationships between levels of 11-oxygenated androgens and canonical steroids measured in our previous study of the same cohort, including abundant precursor derived from the adrenal gland such as DHEA (3). In preoperative serums, levels of 11-oxygenated androgens were weakly to moderately correlated to those of canonical adrenal precursors DHEA and A4 (r = 0.25 to 0.48; P < 0.05). The strongest correlations were noted between A4 and 11OHA4 (r = 0.65; P < 0.001) and 11KA4 (r = 0.51; P < 0.001). The canonical AR ligands T and DHT displayed modest correlations with the AR agonist 11KT (r = 0.36 and 0.33, respectively; P < 0.001). Furthermore, estrone (E1) and estradiol (E2) were correlated to partial AR agonist 11OHT in both preoperative (r = 0.57 and 0.53, respectively; P < 0.001) and postoperative (r = 0.63 and 0.65, respectively; P < 0.001) serums. Following surgery, strongest correlations were observed between the AR agonist 11KT and levels of A4, T, E1 and E2 (r values ranging from 0.48 to 0.52, respectively; P < 0.001) (Figure 5B).
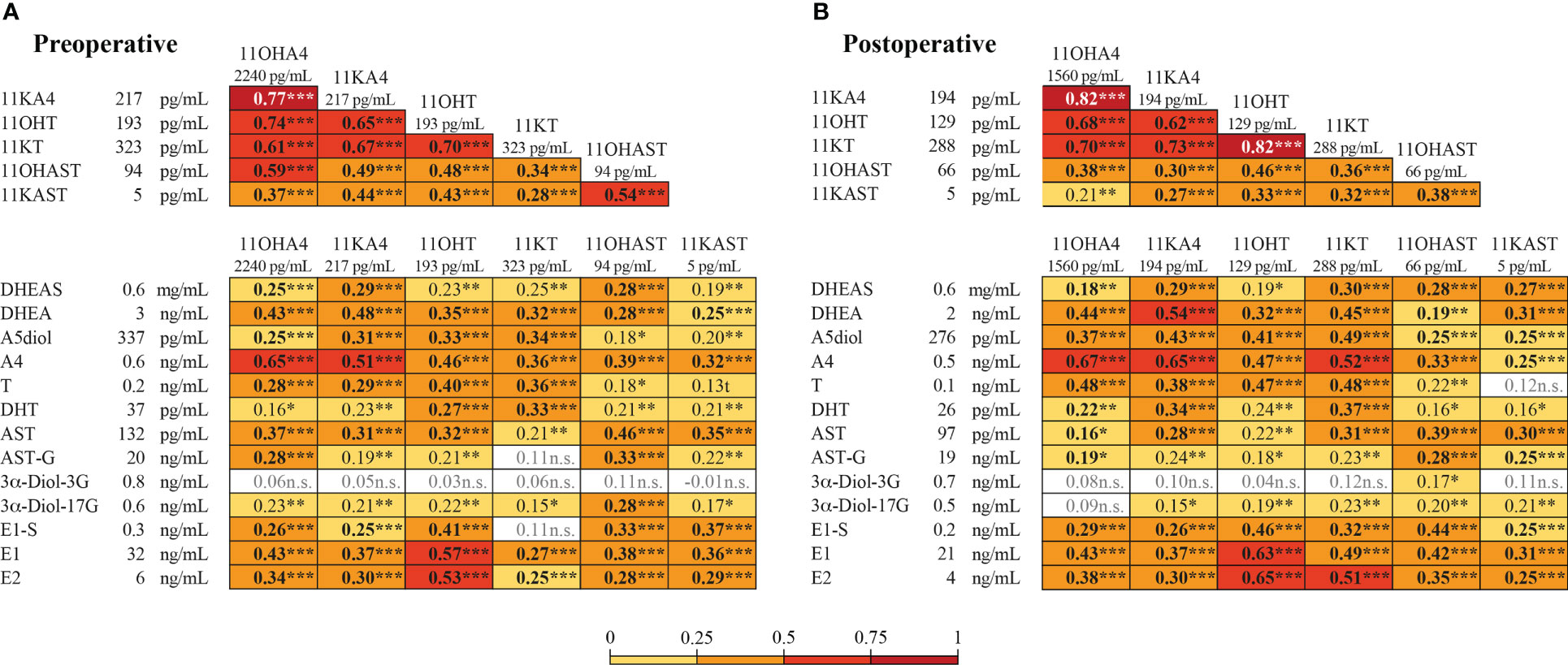
Figure 5 Correlation between preoperative and postoperative levels of 11-oxygenated androgens and canonical steroids in paired preoperative and postoperative samples from 186 EC cases. Heatmap of free 11-oxygenated androgens and canonical steroids in preoperative (A) and postoperative (B) serums. Spearman r values are shown in the box. Significant correlations are shaded as per the colors in the key. Levels of 11-oxygenated steroids (this study) and of canonical steroids (previously reported (3)) are given on the side of heatmaps. Significant data (P< 0.05) are indicated in bold. * P< 0.05. ** P< 0.01. *** P< 0.001.
None of the 11-oxygenated androgens, including for preoperative total 11KDHT or free 11KAST detected in a subset of cases, were significantly associated with clinicopathological features, including histological type, grade, stage, myometrial and lymph-vascular space invasion (not shown). Cases with type II EC presented lower levels of postoperative potent androgens 11KT (by 27%; P = 0.005) and 11OHT (by 22%; P = 0.03), whereas no differences were seen for cases diagnosed with type I (Supplementary Table 4). Lower levels of free 11KT (17%; P = 0.04) were also observed for postoperative serums of cases in the high-risk group, compared to those in the low risk group (Supplementary Figure 1).
In Kaplan-Meier analyses, a shorter time to recurrence was significant for EC cases with higher preoperative free 11KAST (P = 0.005) and 11OHAST (P = 0.04) (Supplementary Figure 2A-C). In multivariable analyses with the fully adjusted model, an increased risk of recurrence was observed for free 11OHAST measured before surgery (HR = 2.24 (0.89-5.60; P = 0.09) that reached significance for levels measured after surgery (HR = 2.99 (95% CI=1.09-8.18; P = 0.03) (Figure 6, Supplementary Table 5). A significant increased risk of recurrence was also observed for preoperative levels of free 11KAST detected at significantly lower levels than 11OHAST, with an HR value of 3.23 (95% CI = 1.11-9.40; P = 0.03), but was not significant after surgery, potentially due to a significant proportion of cases for which 11KAST remained undetectable (Figure 6). Kaplan-Meier revealed that high postoperative levels of free 11OHAST were associated with poorer DFS (P = 0.02), which remained significant in multivariable analyses (HR=3.27 (95 CI%=1.34-8.00; P = 0.009) (Supplementary Figure 2D, Supplementary Table 6). For total preoperative 11KDHT, despite the low number of cases with detectable levels (n=34), a trend towards a higher risk of poorer DFS was observed in multivariable analyses (HR = 2.20 (0.99-4.87; P=0.05), with no relationship to recurrence.
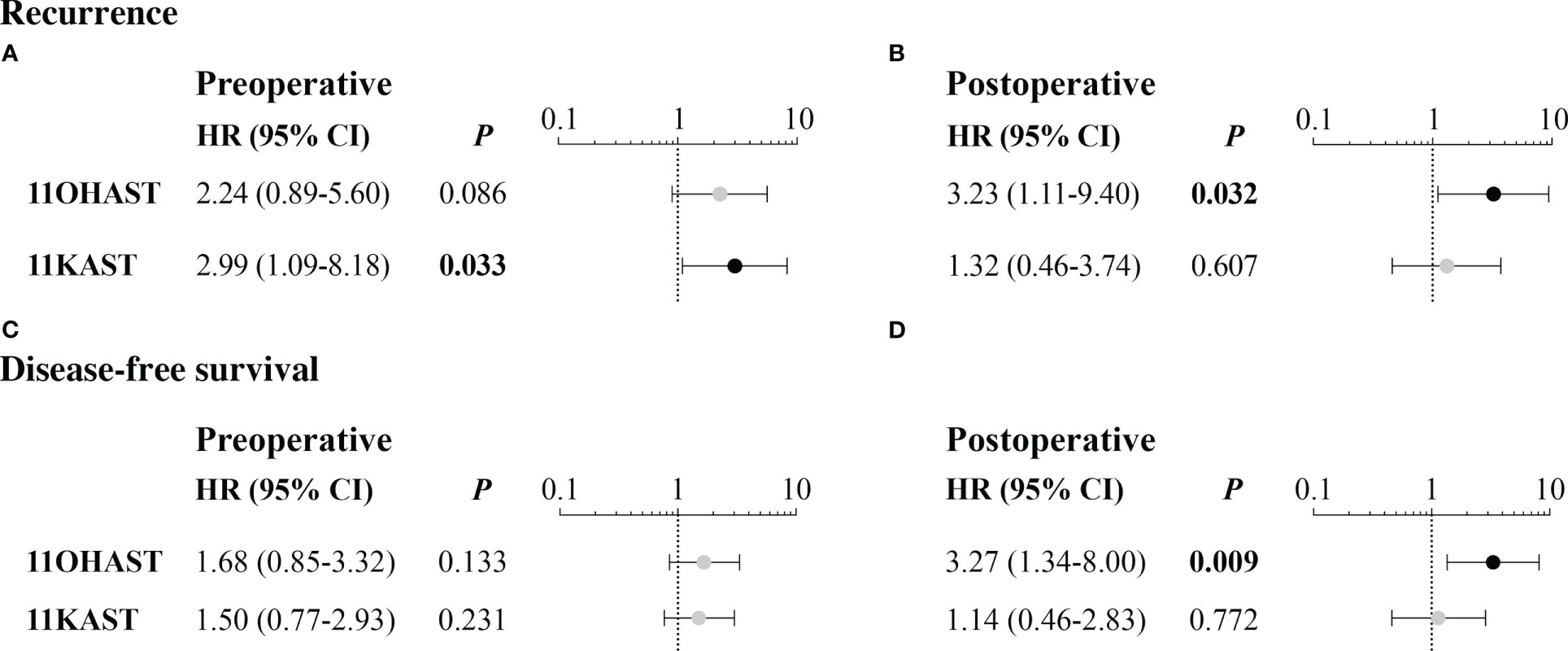
Figure 6 Risk of recurrence and disease-free survival in relation to free preoperative and postoperative levels of 11-oxygenated androgens. Hazard ratios (HR) were calculated using Cox regression for all available follow-up and comparing hormone categories separated upon median, with adjustment for age, BMI, histological type and myometrial invasion and SHBG levels, and as performed for canonical steroids in a previous report (3). Only significant relationships are depicted for recurrence (A, B) and disease-free survival (C, D) whereas all results of these analyses are presented in Supplementary Tables 5, 6.
This study provides the first comprehensive profiling of free and total circulating 11-oxygenated androgens in postmenopausal women diagnosed with EC undergoing surgical treatment. The main observation relates to their link to an increased risk of recurrence and poorer DFS, suggesting that exposition to this novel class of androgens may sustain EC progression and serve as prognostic indicators and support the relevance of profiling these additional AR ligands. Findings contrast with those of our previous study focused on canonical androgens such as T and DHT that did not demonstrate a relationship with clinical outcomes, despite higher T and DHT levels measured in circulation of EC cases compared to healthy donors (3). We also provide evidence that circulating levels of 11-oxygenated androgens weakly correlate to known prognostic factors, further supporting their independent prognostic significance.
In postmenopausal women with EC, the adrenal precursor 11OHA4 was the predominant unconjugated 11-oxygenated androgen (median range 2.24 ng/ml or 7.41 nM) in preoperative serums, with levels comparable to those of DHEA observed in the same cohort (median levels of 2.62 ng/mL or 9.10 nM) (3). However, circulating levels of 11KDHT remained undetectable in circulation before and after surgery for most women, with only 13% of EC cases displaying detectable total 11KDHT in preoperative samples, preventing us to fully appreciate its association with disease characteristics and outcome. The 11OHT and 11KT with androgenic activity were detected at a median range of 193–223 pg/mL (0.74 nM) comparable to those of T (240 pg/mL or 0.83 nM) previously reported in the same EC cohort (3). This observation supports similar concentrations of circulating canonical and non-canonical androgens in postmenopausal women. No study evaluated 11-oxygenated metabolites 11KAST and 11OHAST in postmenopausal women, preventing us to compare levels across cohorts. Their higher levels and particularly those of the abundant 11OHAST were associated with an increased risk of relapse after surgery and shorter DFS. A recent study reported minimal or no androgenic bioactivity for these 11-oxygenated metabolites (40). In multivariate model adjusted for age, BMI and known prognostic variables, higher postoperative levels of 11OHAST were significantly associated with adverse outcomes and may reflect an enhanced conversion of 11-oxygenated AR agonists by peripheral tissues and/or residual and disseminated tumoral cells, favoring EC progression and relapse. In support, cases presenting higher total preoperative levels of the most potent 11KDHT agonist presented a 2.2-fold higher risk of poorer DFS that did not reached significance (P = 0.05). However, this finding should be interpreted with caution due to the low number of patients.
The levels of all 11-oxygenated androgens significantly declined one month after surgery, supporting that EC tumors and/or uterus and the surrounding organs removed by hysterectomy, meaningfully contribute to the activation of adrenal 11-oxygenated androgens. This is sustained by lower circulating levels of the 11KT with high androgenic potency in postoperative serums of type II cases and those in the high-risk category with poorer prognosis, compared to preoperative levels. Furthermore, previous reports showed that the main enzymes involved in the biotransformation of 11-oxygenated androgens are expressed in EC tumors, such as SRD5A, HSD11B2 and AKR1C3 (13, 41, 42). Levels of 11-oxygenated androgens were increased in obese and overweight compared to normal weight cases but were weakly linked to BMI (r ≤ 0.25), except for 11OHT which displayed a moderate association (r ~0.35). We also observed that the levels of 11OHT remained superior after surgery, suggesting that the adipose tissue may contribute and consistent with the expression of HSD11B1 involved in the conversion of 11KT to 11OHT (23).
Strengths of this study include measurement of a novel class of non-canonical androgens with a robust validated bioanalytical method based on mass spectrometry, comparison of their levels to those of canonical androgens assessed in the same cohort also measured by mass spectrometry, and investigations of their link with clinical outcomes based on a large cohort of newly diagnosed postmenopausal EC cases undergoing hysterectomy with extended follow-up, detailed clinicopathological parameters, and not using HRT. These findings are however limited by the small number of recurrent cases whereas no adjustments for multiple testing were performed given the exploratory nature of our investigation. A replication of our findings is warranted. At the tissue levels, measures of these novel androgens in EC tumors collected at surgery would help investigate whether circulatory levels reflect tissue steroid levels. These data will also help support their prognostic potential. Nonetheless, we hope that these initial findings will prompt other groups to investigate 11OHAST and 11KAST with more depth by adding these inactive 11-oxygenated metabolites to their analysis of the steroidome in EC and other clinical conditions, and using validated methods.
The findings that higher levels of 11-oxygenated androgen metabolites, 11OHAST and/or 11KAST measured before and after hysterectomy, were linked to an increased risk of recurrence and poorer DFS, provide insights for future research investigating the role of 11-oxygenated androgens in EC cancer, as they might serve as prognostic indicators. Further research is necessary to understand the effect of excess adrenal 11-oxygenated androgens in promoting EC progression.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by CHU de Québec - Université Laval ethics committee. The patients/participants provided their written informed consent to participate in this study.
Study concept and design: CG. Patient recruitment and clinical data: MP, JG. Conducted experiments and mass spectrometry: PC, VT. Statistical analyses: CD, DS, CG. Drafting of the manuscript: CD, CG. Critical revision of the manuscript for important intellectual content: All authors. Obtaining funding: CG. All authors contributed to the article and approved the submitted version.
The Canadian Institutes of Health Research (CIHR FRN-167269) and The Canada Research Chair Program supported this work. CD received a scholarship from Cancer Research Center (CRC) – Université Laval. CG holds a Canada Research Chair in Pharmacogenomics.
We would like to acknowledge and thank all study participants and the efforts of research staff that made this study possible. We would also like to express our gratitude to one of the study participants and her family for a donation to the Fondation du CHU de Québec that made possible part of this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1156680/full#supplementary-material
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics. CA: A Cancer J Clin (2022) 72:7–33. doi: 10.3322/caac.21708
2. Anh NH, Long NP, Kim SJ, Min JE, Yoon SJ, Kim HM, et al. Steroidomics for the prevention, assessment, and management of cancers: a systematic review and functional analysis. Metabolites (2019) 9. doi: 10.3390/metabo9100199
3. Audet-Delage Y, Gregoire J, Caron P, Turcotte V, Plante M, Ayotte P, et al. Estradiol metabolites as biomarkers of endometrial cancer prognosis after surgery. J Steroid Biochem Mol Biol (2018) 178:45–54. doi: 10.1016/j.jsbmb.2017.10.021
4. Forsse D, Tangen IL, Fasmer KE, Halle MK, Viste K, Almas B, et al. Blood steroid levels predict survival in endometrial cancer and reflect tumor estrogen signaling. Gynecol Oncol (2020) 156:400–06. doi: 10.1016/j.ygyno.2019.11.123
5. Tangen IL, Fasmer KE, Konings GF, Jochems A, Delvoux B, Xanthoulea S, et al. Blood steroids are associated with prognosis and fat distribution in endometrial cancer. Gynecol Oncol (2019) 152:46–52. doi: 10.1016/j.ygyno.2018.10.024
6. Labrie F. All sex steroids are made intracellularly in peripheral tissues by the mechanisms of intracrinology after menopause. J Steroid Biochem Mol Biol (2015) 145:133–8. doi: 10.1016/j.jsbmb.2014.06.001
7. Tanaka S, Miki Y, Hashimoto C, Takagi K, Doe Z, Li B, et al. The role of 5alpha-reductase type 1 associated with intratumoral dihydrotestosterone concentrations in human endometrial carcinoma. Mol Cell Endocrinol (2015) 401:56–64. doi: 10.1016/j.mce.2014.11.022
8. Gibson DA, Simitsidellis I, Collins F, Saunders. Androgens PTK. Oestrogens and endometrium: a fine balance between perfection and pathology. J Endocrinol (2020) 246:R75–93. doi: 10.1530/JOE-20-0106
9. Rizner TL. Estrogen biosynthesis, phase I and phase II metabolism, and action in endometrial cancer. Mol Cell Endocrinol (2013) 381:124–39. doi: 10.1016/j.mce.2013.07.026
10. Segawa T, Shozu M, Murakami K, Kasai T, Shinohara K, Nomura K, et al. Aromatase expression in stromal cells of endometrioid endometrial cancer correlates with poor survival. Clin Cancer Res (2005) 11:2188–94. doi: 10.1158/1078-0432.CCR-04-1859
11. Siiteri PK. Adipose tissue as a source of hormones. Am J Clin Nutr (1987) 45:277–82. doi: 10.1093/ajcn/45.1.277
12. Simitsidellis I, Saunders PTK, Gibson. Androgens DA. And endometrium: new insights and new targets. Mol Cell Endocrinol (2018) 465:48–60. doi: 10.1016/j.mce.2017.09.022
13. Gjorgoska M, Rizner TL. Integration of androgen hormones in endometrial cancer biology. Trends Endocrinol Metab (2022) 33:639–51. doi: 10.1016/j.tem.2022.06.001
14. Lv M, Yu J, Huang Y, Ma J, Xiang J, Wang Y, et al. Androgen signaling in uterine diseases: new insights and new targets. Biomolecules (2022) 12. doi: 10.3390/biom12111624
15. Wu X, Zhong X, Huo X, Zhang J, Yang X, Zhang Y. The clinicopathological significance and prognostic value of androgen receptor in endometrial carcinoma: a meta-analysis. Front Oncol (2022) 12:905809. doi: 10.3389/fonc.2022.905809
16. Zang H, Sahlin L, Masironi B, Hirschberg AL. Effects of testosterone and estrogen treatment on the distribution of sex hormone receptors in the endometrium of postmenopausal women. Menopause (2008) 15:233–9. doi: 10.1097/gme.0b013e318148bb99
17. Chen L, Chang WC, Hung YC, Chang YY, Bao BY, Huang HC, et al. Androgen receptor increases CD133 expression and progenitor-like population that associate with cisplatin resistance in endometrial cancer cell line. Reprod Sci (2014) 21:386–94. doi: 10.1177/1933719113497281
18. Hackenberg R, Beck S, Filmer A, Hushmand Nia A, Kunzmann R, Koch M, et al. Androgen responsiveness of the new human endometrial cancer cell line MFE-296. Int J Cancer (1994) 57:117–22. doi: 10.1002/ijc.2910570121
19. Qiu M, Bao W, Wang J, Yang T, He X, Liao Y, et al. FOXA1 promotes tumor cell proliferation through AR involving the notch pathway in endometrial cancer. BMC Cancer (2014) 14:78. doi: 10.1186/1471-2407-14-78
20. Tuckerman EM, Okon MA, Li T, Laird SM. Do androgens have a direct effect on endometrial function? an in vitro study. Fertil Steril (2000) 74:771–9. doi: 10.1016/S0015-0282(00)00711-1
21. Caron P, Turcotte V, Guillemette C. A quantitative analysis of total and free 11-oxygenated androgens and its application to human serum and plasma specimens using liquid-chromatography tandem mass spectrometry. J Chromatogr A (2021) 1650:462228. doi: 10.1016/j.chroma.2021.462228
22. Nanba AT, Rege J, Ren J, Auchus RJ, Rainey WE, Turcu AF. 11-oxygenated C19 steroids do not decline with age in women. J Clin Endocrinol Metab (2019) 104:2615–22. doi: 10.1210/jc.2018-02527
23. Storbeck KH, Bloem LM, Africander D, Schloms L, Swart P, Swart AC. 11beta-hydroxydihydrotestosterone and 11-ketodihydrotestosterone, novel C19 steroids with androgenic activity: a putative role in castration resistant prostate cancer? Mol Cell Endocrinol (2013) 377:135–46. doi: 10.1016/j.mce.2013.07.006
24. Turcu AF, Rege J, Auchus RJ, Rainey WE. 11-oxygenated androgens in health and disease. Nat Rev Endocrinol (2020) 16:284–96. doi: 10.1038/s41574-020-0336-x
25. Dahmani C, Caron P, Simonyan D, Lacombe L, Aprikian A, Saad F, et al. Preoperative circulating 11-oxygenated androgens are associated with metastasis-free survival in localized prostate cancer. J Urol (2023) 209:337–46. doi: 10.1097/JU.0000000000003049
26. Auer MK, Paizoni L, Neuner M, Lottspeich C, Schmidt H, Bidlingmaier M, et al. 11-oxygenated androgens and their relation to hypothalamus-pituitary-gonadal-axis disturbances in adults with congenital adrenal hyperplasia. J Steroid Biochem Mol Biol (2021) 212:105921. doi: 10.1016/j.jsbmb.2021.105921
27. Bacila I, Adaway J, Hawley J, Mahdi S, Krone R, Patel L, et al. Measurement of salivary adrenal-specific androgens as biomarkers of therapy control in 21-hydroxylase deficiency. J Clin Endocrinol Metab (2019) 104:6417–29. doi: 10.1210/jc.2019-00031
28. Kamrath C, Wettstaedt L, Boettcher C, Hartmann MF, Wudy SA. Androgen excess is due to elevated 11-oxygenated androgens in treated children with congenital adrenal hyperplasia. J Steroid Biochem Mol Biol (2018) 178:221–28. doi: 10.1016/j.jsbmb.2017.12.016
29. Nowotny HF, Braun L, Vogel F, Bidlingmaier M, Reincke M, Tschaidse L, et al. 11-oxygenated C19 steroids are the predominant androgens responsible for hyperandrogenemia in cushing's disease. Eur J Endocrinol (2022) 187:663–73. doi: 10.1530/EJE-22-0320
30. Barbier ID, Gent R, Toit TD, Swart AC. Androstenedione is the preferred substrate for cytochrome P450 11β-hydroxylase leading to the production of 11β-hydroxyandrostenedione in the adrenal gland. J Endocr Soc (2021) 5:A65. doi: 10.1210/jendso/bvab048.132
31. Barnard L, Gent R, van Rooyen D, Swart AC. Adrenal C11-oxy C(21) steroids contribute to the C11-oxy C(19) steroid pool via the backdoor pathway in the biosynthesis and metabolism of 21-deoxycortisol and 21-deoxycortisone. J Steroid Biochem Mol Biol (2017) 174:86–95. doi: 10.1016/j.jsbmb.2017.07.034
32. Barnard M, Mostaghel EA, Auchus RJ, Storbeck KH. The role of adrenal derived androgens in castration resistant prostate cancer. J Steroid Biochem Mol Biol (2020) 197:105506. doi: 10.1016/j.jsbmb.2019.105506
33. Barnard M, Quanson JL, Mostaghel E, Pretorius E, Snoep JL, Storbeck KH. 11-oxygenated androgen precursors are the preferred substrates for aldo-keto reductase 1C3 (AKR1C3): implications for castration resistant prostate cancer. J Steroid Biochem Mol Biol (2018) 183:192–201. doi: 10.1016/j.jsbmb.2018.06.013
34. du Toit T, Swart AC. The 11beta-hydroxyandrostenedione pathway and C11-oxy C21 backdoor pathway are active in benign prostatic hyperplasia yielding 11keto-testosterone and 11keto-progesterone. J Steroid Biochem Mol Biol (2020) 196:105497. doi: 10.1016/j.jsbmb.2019.105497
35. Mostaghel EA. Beyond T and DHT - novel steroid derivatives capable of wild type androgen receptor activation. Int J Biol Sci (2014) 10:602–13. doi: 10.7150/ijbs.8844
36. Pretorius E, Africander DJ, Vlok M, Perkins MS, Quanson J, Storbeck KH. 11-ketotestosterone and 11-ketodihydrotestosterone in castration resistant prostate cancer: potent androgens which can no longer be ignored. PloS One (2016) 11:e0159867. doi: 10.1371/journal.pone.0159867
37. Storbeck KH. A commentary on the origins of 11-ketotestosterone. Eur J Endocrinol (2022) 187:C5–8. doi: 10.1530/EJE-22-0820
38. Storbeck KH, Mostaghel EA. Canonical and noncanonical androgen metabolism and activity. Adv Exp Med Biol (2019) 1210:239–77. doi: 10.1007/978-3-030-32656-2_11
39. Pretorius E, Arlt W, Storbeck KH. A new dawn for androgens: novel lessons from 11-oxygenated C19 steroids. Mol Cell Endocrinol (2017) 441:76–85. doi: 10.1016/j.mce.2016.08.014
40. Handelsman DJ, Cooper ER, Heather AK. Bioactivity of 11 keto and hydroxy androgens in yeast and mammalian host cells. J Steroid Biochem Mol Biol (2022) 218:106049. doi: 10.1016/j.jsbmb.2021.106049
41. Ito K, Suzuki T, Akahira J, Moriya T, Kaneko C, Utsunomiya H, et al. Expression of androgen receptor and 5alpha-reductases in the human normal endometrium and its disorders. Int J Cancer (2002) 99:652–7. doi: 10.1002/ijc.10394
Keywords: endometrial cancer (EC), 11-oxygenated androgens, mass spectrometry - LC-MS/MS, recurrence, survival
Citation: Dahmani C, Caron P, Simonyan D, Turcotte V, Grégoire J, Plante M and Guillemette C (2023) Circulating adrenal 11-oxygenated androgens are associated with clinical outcome in endometrial cancer. Front. Endocrinol. 14:1156680. doi: 10.3389/fendo.2023.1156680
Received: 01 February 2023; Accepted: 10 May 2023;
Published: 23 May 2023.
Edited by:
Maria Magdalena Montt-Guevara, University of Pisa, ItalyReviewed by:
Yoshitaka Imamichi, Fukui Prefectural University, JapanCopyright © 2023 Dahmani, Caron, Simonyan, Turcotte, Grégoire, Plante and Guillemette. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chantal Guillemette, Y2hhbnRhbC5ndWlsbGVtZXR0ZUBjcmNodWRlcXVlYmVjLnVsYXZhbC5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.