 Felipe Aguiar Pupo Seabra Malta
Felipe Aguiar Pupo Seabra Malta Daniela Caetano Gonçalves
Daniela Caetano Gonçalves- 1Postgraduate Program in Nutrition, Universidade Federal de São Paulo (UNIFESP), São Paulo, Brazil
- 2Department of Biosciences, Universidade Federal de São Paulo (UNIFESP), São Paulo, Brazil
Background: Progressive, involuntary weight and lean mass loss in cancer are linked to cachexia, a prevalent syndrome in gastrointestinal malignancies that impacts quality of life, survival and postoperative complications. Its pathophysiology is complex and believed to involve proinflammatory cytokine-mediated systemic inflammation resulting from tumor-host interaction, oxidative stress, abnormal metabolism and neuroendocrine changes. Therapeutic options for cachexia remain extremely limited, highlighting the need for clinical research targeting new interventions. Thus, this study primarily assesses the effects of grape-seed flour (GSF), rich in polyphenols and fibers, for attenuating perioperative weight loss in colorectal cancer.
Methods: This is a dual-center, triple-masked, placebo-controlled, parallel-group, phase II, randomized clinical trial designed to investigate GSF supplementation in subjects with pre- or cachexia associated with colorectal cancer during the perioperative period. Eighty-two participants will receive 8g of GSF or cornstarch (control) for 8 weeks. Assessments are scheduled around surgery: pre-intervention (4 weeks prior), day before, first week after, and post-intervention (4 weeks later). The primary endpoint is the difference in body weight mean change from baseline to week 8. The secondary endpoints describe the harms from 8-week supplementation and assess its superiority to improve body composition, post-surgical complications, quality of life, anorexia, fatigue, gastrointestinal symptoms, and handgrip strength. The study will also explore its effects on gut bacteria activity and composition, systemic inflammation, and muscle metabolism.
Discussion: The current trial addresses a gap within the field of cancer cachexia, specifically focusing on the potential role of a nutritional intervention during the acute treatment phase. GSF is expected to modulate inflammation and oxidative stress, both involved in muscle and intestinal dysfunction. The research findings hold substantial implications for enhancing the understanding about cachexia pathophysiology and may offer a new clinical approach to managing cachexia at a critical point in treatment, directly impacting clinical outcomes.
Trial registration: The Brazilian Registry of Clinical Trials (ReBEC), RBR-5p6nv8b; UTN: U1111-1285-9594. Prospectively registered on February 07, 2023.
Introduction
Background and rationale
Involuntary and progressive weight loss is common in some cancers like head and neck, lung, and gastrointestinal tract cancer (1). This phenomenon is credited to cachexia, a complex metabolic syndrome characterized by an ongoing loss of muscle mass, accompanied or not by loss of fat mass, that leads to progressive functional impairment (2). Cachexia can affect up to 80% of individuals with advanced malignancy and is believed to directly cause 20% of cancer-related deaths (3). These statistics are particularly alarming given the high global cancer incidence, with 19.3 million new cases per year, and mortality, accounting for 10 million deaths annually, ranking as the second leading cause of death (4).
Cancer cachexia is a multifactorial syndrome thought to be caused by the proinflammatory cytokine-mediated systemic inflammation resulting from tumor-host interaction, oxidative stress, abnormal metabolism, neuroendocrine changes, gut dysbiosis, and tumor-secreted catabolic factors (5–8). Besides weight loss, patients with cachexia often experience muscle failure (9), anorexia (2), fatigue and decreased quality of life (10), leading to reduced survival (11), prolonged hospital stay (12), increased morbidity, lower resistance to treatment (13), and greater postoperative risks (14).
The extent of weight loss in cachexia is influenced by the treatment, type and stage of cancer. This loss amounts to a minimum of 5% of the individual’s usual weight within six months (or 2% in cases accompanied by sarcopenia or low muscularity) (2), and averages a 10 to 15% total reduction from pre-diagnosis weight during the first year post-diagnosis (15–17). Furthermore, patients with cachexia have significantly higher death rates, ranging from 1.26 to 1.82 times those observed in patients with cancer but without cachexia (18–20), emphasizing the relevance of this condition and its impact on patient outcomes.
Cancer cachexia cannot be fully reversed by nutritional support, and thus far, the effectiveness of most interventions has been disappointing, failing to meet regulatory requirements, with the exception of anarmorelin’s approval in Japan for some cases (21). Despite these challenges, in recent decades significant research and development efforts have been focused on potential interventions, mainly nutritional, exercise-based or pharmacological. Nutritional strategies, such as dietary counseling or nutraceutical-based, offer the benefit of minimal risk of harm to patients, facilitating their implementation in research (22).
By definition, the nutraceuticals category includes food products and dietary supplements that contain one or more compounds capable of exerting a positive clinical effect on a particular syndrome/disease (23, 24). In cancer cachexia, nutraceuticals with anti-inflammatory and antioxidant properties, mostly sources of omega-3 or polyphenols, are amongst the most researched. Experimental studies suggest they can reduce weight and lean mass loss (25, 26), decrease systemic inflammation, inhibit proteolysis, and increase muscle protein synthesis (27–30). However, when translated to clinical context, the results are heterogeneous (31, 32), possibly because of the small number of trials, different designs, and insufficient methodological quality.
In this scenario, clinical efficacy trials are fundamental for guiding basic research and establishing intervention options for pragmatic trials. Grape seed-based supplements contain substantial amounts of insoluble fiber and polyphenols, particularly proanthocyanidins (33, 34). In experimental models, they have demonstrated nutraceutical potential by promoting a range of positive effects, including the ability to attenuate oxidative stress (35–37), modulate gut microbiota composition (38) and preserve muscle mass (39–41). In human studies, grape seed supplementation improved biomarkers, promoted clinical benefits (42, 43), and exhibited safety even at high doses (44–46).
Therefore, to address these literature gaps concerning the clinical potential of nutraceuticals, this study will investigate grape seed flour (GSF) supplementation effects on cachexia associated with colorectal cancer in the perioperative context. The choice of colorectal cancer was motivated by the high prevalence of cachexia in this cancer (47), which is the third most common in the world (48). Likewise, the perioperative phase holds significant importance during treatment, as it represents a critical moment characterized by substantial weight and muscle mass loss, which can predict unfavorable clinical consequences (49–52).
So, given polyphenols’ systemic antioxidant and anti-inflammatory action, as well as their ability to promote gut health in conjunction with dietary fiber, we hypothesize that GSF supplementation may attenuate weight and fat-free mass loss during the perioperative period, thereby improving patients’ post-surgical clinical response.
Objectives
The primary objective of this study is to assess the superiority of an 8-week supplementation of grape seed flour (8g/day) against placebo for attenuate mean weight loss in patients with pre- or cachexia associated with colorectal cancer during the perioperative period (primary tumor resection), regardless of treatment switching, discontinuation, or extent of supplementation adherence.
The secondary objectives are:
• To evaluate the superiority of an 8-week supplementation of GSF against placebo in patients with pre- or cachexia associated with colorectal cancer during perioperative period (primary tumor resection), regardless of treatment switching, discontinuation, or extent of supplementation adherence, to:
○ reduce the deterioration of fat-free mass, muscle strength, quality of life, anorexia, fatigue, and gastrointestinal symptoms;
○ improve post-surgical recovery.
• To describe the eight-week intervention-related harms.
Estimands
The international regulatory guidance ICH E9 (R1) Statistical Principles for Clinical Trials: Addendum: Estimands and Sensitivity Analysis in Clinical Trials proposed a structured framework to align planning, design, conduct, analysis and interpretation of clinical trials (53). The estimand should provide a clear and precise description of the treatment effect of interest that aims to answer a clinical question posed by a specific clinical trial objective. Through five attributes, the framework guides the development of an estimator (statistical methods) to produce a clinically meaningful estimate (numerical result). Its use facilitates comprehension and communication with different stakeholders, making it highly recommended for implementation in trial protocols (54, 55).
Primary estimand (estimand A)
• Treatment condition: Grape seed flour supplementation versus placebo supplementation (cornstarch), including the effects of treatment discontinuation, switching, and different levels of supplement adherence.
• Target population: adult participants with pre- or cachexia associated with colorectal cancer during perioperative period (primary tumor curative resection), as defined by inclusion and exclusion criteria.
• Endpoint: body weight change from baseline (V1) to week 8 (V4).
• Intercurrent events and strategies to address them: treatment discontinuation, arm switching, intake of additional fiber/antioxidant supplementation, and low adherence will be handled by the treatment policy strategy, which includes these effects in the analysis. Participants’ death, disease-related or not, will be handled by Principal Stratum, excluding those participants from the analysis data set. Further intercurrent events (ICE) are not currently anticipated.
• Population-level summary measure: The difference in mean difference change from baseline to week eight in body weight (kg).
Secondary and exploratory estimands
Secondary and exploratory estimands are detailed elsewhere (see in Supplementary Table 2).
Trial design
This is a phase-2 proof-of-concept, randomized, triple-masked (participant, researcher, and clinical staff), parallel-group, placebo-controlled, dual-center, superiority clinical trial designed to assess the effects of 8-week grape seed flour supplementation in subjects with pre- or cachexia associated with colorectal cancer during perioperative period. Eighty two subjects will be randomized 1:1 through a minimization method, using center, sex and cachexia degree as stratification factors. Participants will face a pre- and post-surgery treatment phase, each lasting 28 days. A 60-day follow-up period will be added to observe postoperative complications. The enrollment is planned to stop as the target sample size is reached and the study to end at the last assessment of the eighty-second participant. The study design is presented in Figure 1.
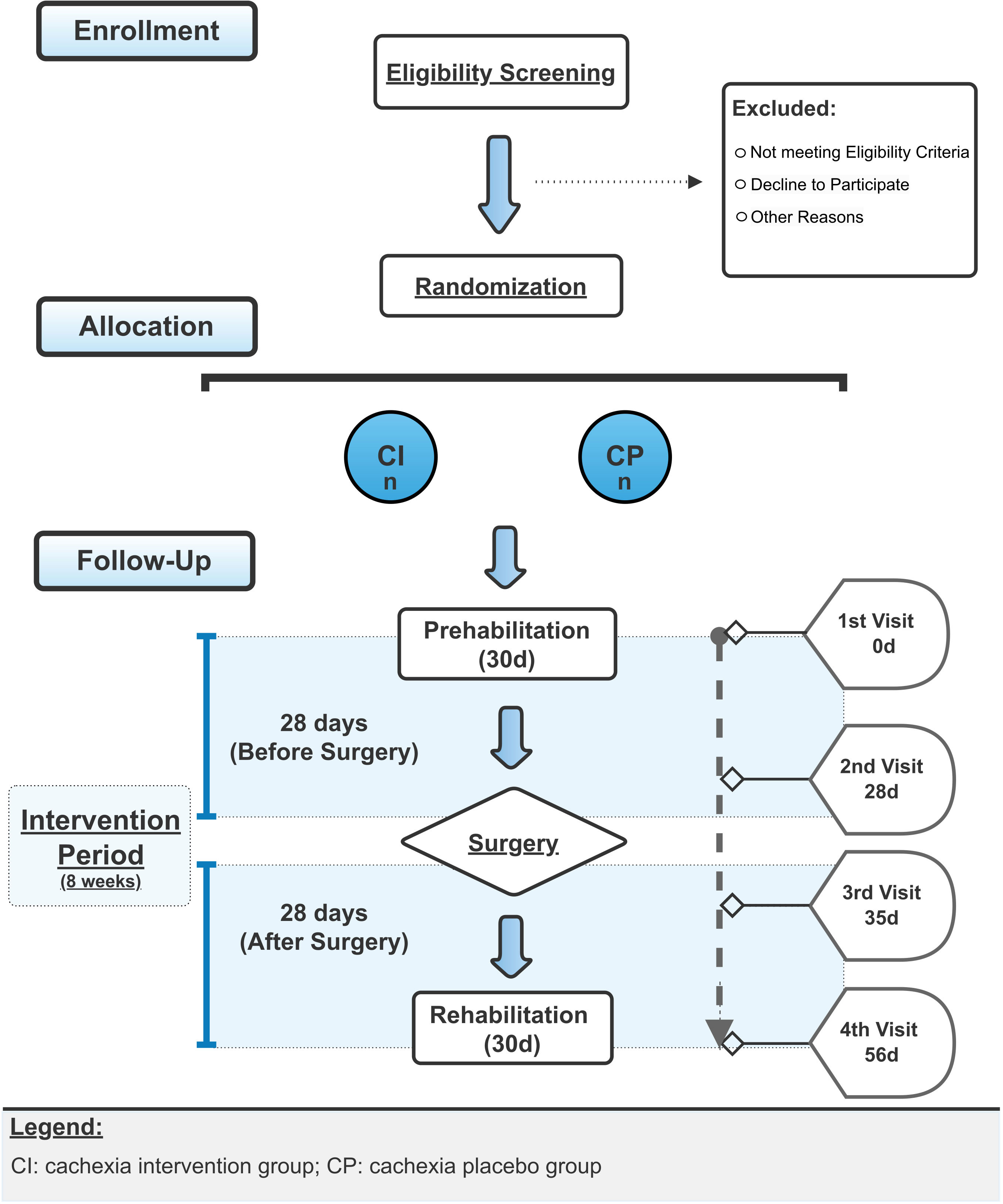
Figure 1 Study Design Flowchart.
Recommendations from SPIRIT 2013 Statement (Standard Protocol Items: Recommendations for Interventional Trials) were used as complementary tool to improve trial design completeness and the quality of protocol report (Supplementary Table 3) (56). In addition, the PRECIS-2 (PRagmatic Explanatory Continuum Indicator Summary) tool was used during the design of the trial to align the methodological choices with the study objectives, as well as to provide a visual framework that helps to locate study purpose on the explanatory-pragmatic continuum (Figure 2). The scoring rationale for each PRECIS-2 domain is displayed in the Supplementary Table 4 (57).
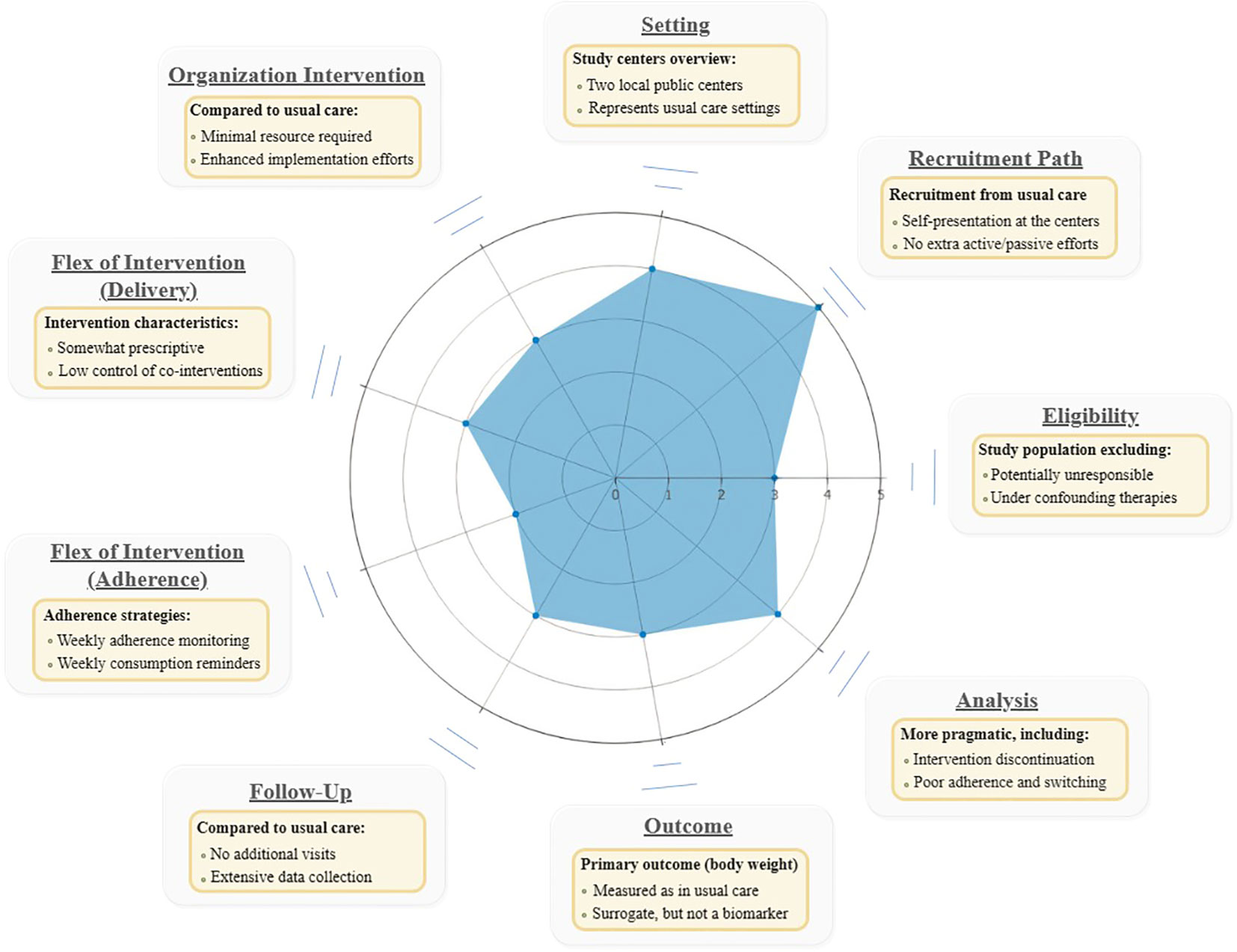
Figure 2 PRECIS-2 Wheel.
Methods
Study setting
The study will be conducted at two tertiary referral centers (metropolitan urban area of 1.9 million people) (58) - Hospital Guilherme Álvaro; and Irmandade da Santa Casa da Misericórdia de Santos. These centers belong to the Brazilian Unified National Health System (SUS) and provide free-of-charge surgical treatment to people diagnosed with colorectal cancer. Patients screening, enrollment, allocation and baseline assessment will occur at colorectal surgical outpatients clinics of the hospitals. Participants will be followed up weekly by telephone/internet up to the day before surgery, when the research team will assess them at the surgical wards and Intensive Care Units until the moment of hospital discharge. The last two face-to-face assessments will be carried out on the seventh and thirtieth day after surgery at the same hospitals outpatient clinics cited before.
Eligibility criteria
To be included participants must have a diagnosis of colorectal cancer, be scheduled for elective curative surgery for primary tumor resection (laparotomy or laparoscopy) without neoadjuvant therapy, and fulfill the following criteria:
● Histopathological diagnosis of colorectal carcinoma.
● Tumor staging according to Union for International Cancer Control (UICC) (59).
● Adults (age between 40 and 90 years).
● Cachexia or pre-cachexia (2011 Fearon Consensus definition) (2).
● Signed informed consent.
Exclusion criteria are as follows:
● Confirmed distant metastasis.
● Radio/Chemotherapy treatment in the last 3 months.
● Body Mass Index (BMI) greater than 40 kg/m².
● History of liver function impairment (Child-Pugh-Turcotte score B and C) (60).
● History of chronic kidney disease (KDIGO 2012 definition) (61).
● HIV positive with AIDS-related complications.
● Hypersensitivity to trial supplement.
● Continuous supplementation of polyphenols or pre/probiotics in the last 3 months.
● Inflammatory bowel diseases (IBD) or chronic inflammatory processes unrelated to cachexia, such as autoimmune disorders.
● Pregnancy or breastfeeding.
Interventions
Participants assigned to the intervention arm will receive a daily dose of approximately 8g of grape seed flour (Econatura, Rio Grande do Sul, Brazil) offered in 12 gelatin capsules of similar weight. The prescribed dosing is four capsules three times per day, distributed in the morning, afternoon and evening. In case of forgetting to consume the capsules of one period, the recommendation is to take them together with the capsules of the next period of the day.
The choice of an inactive comparator (placebo-only) as the unique control group is ethically supported by the clinical equipoise principle in situations where genuine therapeutic uncertainty within the clinical community to a certain condition coexists with the absence of a scientifically proven effective treatment (62), which is exactly the case for cancer cachexia (22, 63). Cornstarch, a product made from cereal endosperm, characterized by a very low content of dietary fiber and phytochemicals (64), was chosen as a filler for placebo inert pills.
Capsules from both arms possess the same physical presentation (color, form and weight) and will be delivered to participants in equally, indistinguishable, opaque, sealed, alphanumeric coded containers All study participants will receive the same instructions for consumption, including to not change their usual diet and exercise habits during the trial.
Pill count should be done weekly by participants and reported for calculation of the adherence rate (number of capsules consumed divided by the amount expected for the period). Adherence will also be verified by counting returned unconsumed capsules at the end of the pre- and post-surgery periods, in which participants must return the containers where supplements were dispensed. To enhance adherence, participants will be advised to take the capsules with the main meals (breakfast, lunch and dinner). In addition, weekly consumption reminders will be sent through telephone or messaging application, and at each study visit they will be personally reminded of the importance of proper capsule consumption for the study objectives.
Discontinuation of supplementation is planned in the following cases: very low adherence (defined by two consecutive weeks with consumption under 25% of expected); participant’s wish to withdraw; and in cases of serious adverse events possibly related to the intervention. As an exception, in cases of transient poor gastrointestinal tolerability or swallowing difficulties, which may occur during the first week after surgery, the reduced weekly capsule intake will not be considered in the calculation to determine very low adherence.
Lastly, the only trial concomitant care restriction is to not allow additional consumption of other fiber-rich or prebiotics/probiotics supplements.
Outcomes
The primary outcome is the change in the mean body weight measured in kilograms from pre-intervention (baseline) to post-intervention (week 8). The secondary and exploratory outcomes are detailed in Table 1.

Table 1 Secondary and Exploratory Outcomes.
Participant timeline
The timeline for enrollment, allocation, study visits, assessments, and others are presented in Table 2.
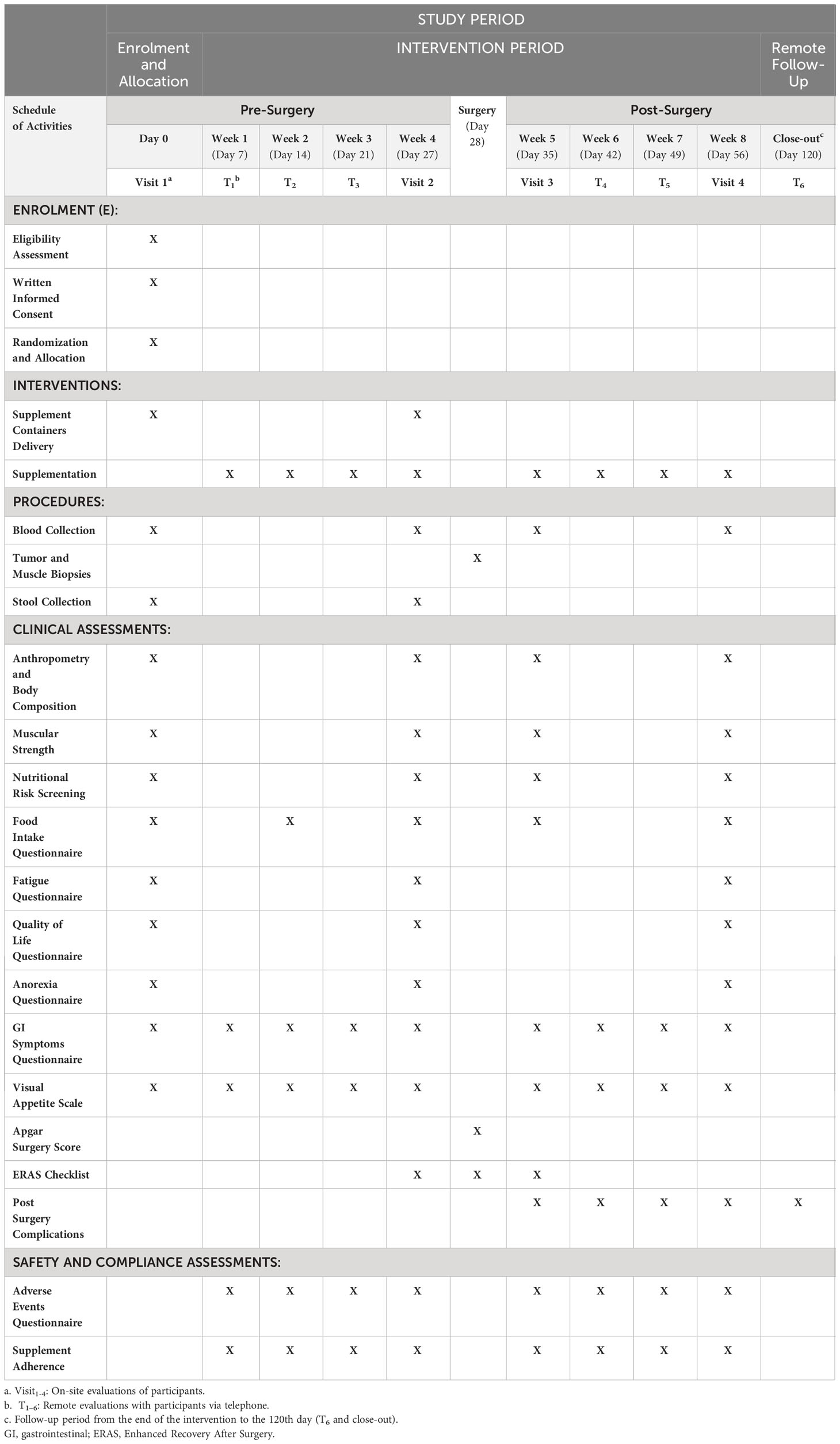
Table 2 Schedule of Enrolment, Interventions, and Assessments (SPIRIT figure).
Sample size
To determine the sample size, a search in MEDLINE was performed via PubMed (December, 2022) to locate studies that provided data of central tendency and dispersion of human longitudinal body weight behavior in the perioperative context of colorectal malign tumor resection. The search strategy combined thesaurus terms and synonyms related to weight loss, colorectal surgery and neoplasms. An additional hand search in Google Scholar was made. Four studies that reported the body weight at the preoperative period and 30-40 days post-surgery were selected for inclusion (65–68) (Supplementary Figures 1A, B).
The choice of the smallest effect size of interest (SESOI) (69) was based on the cancer-associated weight loss grading, which indicates that weight losses greater than 2.5% of the body weight are clinically important (70). So, a random-effects meta-analysis was performed to combine the effect sizes between the real scenario of the included studies and a hypothetical one where the relative change-from-baseline body weight mean was 2% (Supplementary Figure 1C). A sample size of 41 per group (82 in total) will be required to test the primary outcome of interest of the Estimand A. The calculation was based on a mixed model for repeated measures with a general correlation structure (71). The calculations assumed a group allocation of 1:1, alpha of 0.05, 80% power, four assessment points, a between-groups effect size of Cohen’s d = 0.65 at post-intervention, a compound symmetry correlation matrix (rho = 0.5), and attrition rates of 3%, 6% and 10% between assessment points.
Recruitment
Patients who receive from the surgical oncology team an indication for curative colorectal tumor resection without neoadjuvant therapy will be referred to the research staff for active recruitment and pre-screening of eligibility criteria. Recruitment will occur at the same center immediately after the clinical visit in which the surgery is confirmed. These potential participants will come to one of the study’s two tertiary surgery centers either from primary/secondary care referral or on their own behalf. No additional recruitment strategies (active or passive) or extra efforts will be employed.
Allocation
Participants who meet the eligibility criteria and declare consent to participate will be assigned (1:1) to the intervention or control group using the minimisation method, which reduces the probability of imbalances in important covariate at baseline. This adaptive restricted randomization will be implemented with the help of the R package Minirand (72). The first assignment will be completely at random and the subsequents will favor the least imbalance between groups, with a random component of 20% to avoid a deterministic assignment. If a tie occurs in the resulting imbalances, the randomization will be completely random. The following covariate factors will be used in the minimisation algorithm: center (2 levels), sex (2 levels) and cachexia degree (2 levels).
For the purpose of allocation concealment and study masking, an unordered list of 82 random alphanumeric codes containing two letters and three numbers will be created. An independent assistant who is not part of the study will randomly split this list into two password-protected lists of equal length with the help of R software (73). One list containing the codes corresponding to the placebo group bottles, and the other containing the codes corresponding to the intervention bottles. It is important to note that access to these lists by study staff access is strictly prohibited. At the time of assignment, minimisation program will return, according to the software-determined assignment, a code randomly selected from one of these two lists instead of the assigned arm (intervention or control) as answer. The drawn code will automatically be removed from the list before subsequent assignments are made. These codes will also identify participants throughout the study.
No previous allocation sequence will be generated as the assignment will be carried out in real time through the minimisation program. The unidentifiable codes will be stamped on the supplement bottles in advance, in order to preserve allocation concealment. To this end, the bottles will be identical, opaque and sealed. The research staff responsible for allocation won’t have access to the participants’ covariate matrix utilized in the minimisation algorithm, and as they will be masked throughout study, they won’t be aware of previous assignments, decreasing the predictability of upcoming allocations.
Masking
Participants, researchers, hospital clinical staff and data analysts will be blinded until the end of the analysis. To preserve masking throughout the study, several actions will be implemented: both groups will receive physically identical supplement containers and capsules; The participants’ assigned study arm will not be revealed, as their identification is a unique random alphanumeric code; the study arms will be designated in the statistical dataset as “A” and “B” to prevent treatment identification; and true group assignments will only be revealed after data analysis has been completed according to the statistical plan.
The intentional unmasking of participants is allowed only in the investigation of serious adverse events, and carried out immediately by a third-party personnel who is not involved in the screening, enrollment, randomization, and data collection steps. Any code breaks should be documented and reported to regulatory entities.
Data collection
Biospecimen collection
Muscle Biopsy will be collected from the rectus abdominis by sharp dissection during the initial phase of the tumor resection surgery. The main specimen of approximately 1g will be wrapped in saline-moistened gauze and divided into samples to be promptly placed in pre-labelled cryovials for snap-frozen. The samples will be transported to the laboratory within a period of no longer than 4 hours in a styrofoam container with dry ice. The specimen will be maintained at the sponsor’s biorepository under -80°C until the analysis. For electron microscopy, a small piece (~50-100mg) will immediately be separated from the main specimen and placed in a histology cassette for fixation in a 10% neutral buffered formalin solution at room temperature (74–76).
Tumor Biopsy collection will follow a Standard Operating Procedure (SOP) to ensure sampling quality and reproducibility (77–79). Biopsies will be collected from the viable surplus resected surgical specimen and paired with uninvolved tissue removed during surgery — a distant healthy colorectal mucosa (preferred) or with perilesional uninvolved mucosa. Representative parts of the tumor will be sampled (central, periphery and midpoint) (80), avoiding areas with obvious necrosis or hemorrhage, within approximately 30 minutes after specimen excision. Samples of about 1 cm³ will be placed in pre-labelled histology cassettes for fixation or in cryovials to snap-frozen for 20 seconds. The cryovials will be transported in a container with dry ice for storage in the sponsor’s biorepository at -80°C freezers until analysis.
Blood collection will be performed via peripheral venipuncture by a qualified phlebotomist according to the best practices (81). Samples will be collected in two vacutainer tubes: 10 ml in a lavender-top containing K3-ethylenediaminetetraacetic acid (EDTA); and 7.5 ml in a yellow-top with serum separator. The tubes will be gently inverted 8 times to ensure proper mixing and then kept at a temperature below 4°C until transportation to the laboratory. Subsequently, samples will be centrifuged and stored in the biorepository at -80°C. The entire process must be completed within four hours of blood collection (82).
Anthropometric measures
Prior to the measures, participants will be requested to remove all accessories, footwear and any upper-body outerwear garment. The body mass will be measured using a portable calibrated weighing scale with a maximum capacity of 150 kilograms and precision of 100 grams. Height will be measured with a coupled stadiometer that has an accuracy of 0.01 meters (MIC-200 PPA, Micheletti, São Paulo, Brasil). Body mass index (BMI) will be calculated by the ratio of weight in kilograms to the squared height in meters.
Body circumferences (mid-arm, hip, abdominal (83) and maximum calf (84) will be measured using an inelastic tape measure with a precision of 0.1 centimeters, following established protocols that have been referenced. In addition, triceps skinfold (83) will be assessed in triplicate using a Lange® skinfold caliper (Beta Technology, Santa Cruz, California, USA). The mean of the measurements will be reported.
To minimize potential interrater variability, anthropometric measurements of each participant will be performed by the same trained researcher whenever possible, ensuring greater consistency in the measurement process.
Body composition
Bioimpedance analysis (BIA) will be used as the main method to estimate body composition using a calibrated Biodynamics BIA 450 Bioimpedance Analyzer (Biodynamics Corporation, Shoreline, WA), which is a whole-body, single-frequency, tetrapolar device. Absolute fat and fat-free mass will be obtained as a function of reactance (Xc) and resistance (R) values by Schols equation (85). This equation has shown superiority for estimating body composition in subjects with colorectal cancer when using a whole-body device (86). Phase angle (PhA) will be expressed in degrees, obtained by the arctangent of (Xc/R).
The assessment protocol requires removal of metallic body accessories, absence of edema, 24 hours abstinence from alcohol and diuretic medications; no intense physical activity in the last 8 hours; four hours of fasting; bladder voiding thirty minutes before the evaluation; and five minutes of rest before the assessment. The test will be performed with the participant placed on a non-conductive bench in supine position. Arms and legs must be extended and abducted within a 30–45° angle from the trunk. A pair of adhesive sensor pad electrodes will be positioned on the dorsal surfaces of the right wrist and another on the right ankle. The average of three repeated measurements will be reported (87, 88).
Computed Tomography (CT) body composition assessment will be explored in a subset of study participants who are requested by hospital staff to undergo CT imaging for disease diagnosis or follow-up as part of their clinical routine evaluation. Lumbar muscle cross-sectional area (MCSA) and intermuscular (IAT), visceral (VAT), and subcutaneous adipose tissue (SAT) will be quantified based on a single transversal slice at third lumbar vertebra (L3) with the semi-automated software SliceOmatic 5.0 (TomoVision, Montreal, Canadá). Total adipose tissue (TAT) will be calculated as the sum of the aforementioned adipose depots. Whole-body free fat mass will be estimated from lumbar MSCA (89). The mean radiation attenuation value of the MSCA will be used to determine skeletal muscle radiodensity (SMD) (90). A trained member of the research team, blinded to participant information and study arm, will analyze the images. For the purpose of quality control, a random subset of the images will be assessed by other two researchers to check interrater reliability.
Muscle strength
Handgrip strength will be assessed using the protocol described by The American Society of Hand Therapists (91) (Valdes, MacDermid, and Solomon, 2015). Tests will be performed in triplicate with 15-second intervals between each measurement using a Jamar® 5030J1 hydraulic hand dynamometer (Patterson Medical, Warrenville, IL, USA). The subjects must be seated with shoulders adducted, elbow flexed at 90 degrees, and forearm in a neutral position. Using the non-dominant hand, they should perform the maximum handgrip upon receiving voice prompts until the maximum value is reached. The final value, expressed in kilograms, is the arithmetic mean of the attempts.
Fatigue
The Brazilian Portuguese validated version of the fatigue subscale from Functional Assessment of Cancer Therapy (FACIT-F) questionnaire will be used to assess cancer-related fatigue (92, 93). This questionnaire is based on the participants’ experiences over the last 7 days and has 13 items scored on a Likert scale, with a minimum total score of 0 and a maximum of 52 points. Final scores lower than 34 indicate fatigue and are used as a parameter in the diagnosis of cancer cachexia (94). The FACIT-F will be filled out by the participants.
Food intake
Assessment of participants’ food intake will be conducted by trained researchers using the USDA’s (United States Department of Agriculture) 24-hour dietary recall Five-Pass Automated Multiple-Pass Method (AMPM) (95, 96). This interviewer-administered recall assesses the food intake of the previous day and can be done in person or by telephone (97). The method comprises five sequential steps: quick listing of consumed foods; forgotten foods; time and occasion of consumption; detail cycle; and final review. A food model booklet with three-dimensional pictures of food and kitchenware will be used to support answers (98). Calculation of dietary polyphenols content will be performed using the Phenol-Explorer database (99), while energy, macro- and micronutrients will be determined using the NutrabemPro software (100), which incorporates USDA (101) and TACO (Tabela Brasileira de Composição de Alimentos) (102) food composition tables. To estimate the means of usual intake at each study time point, two-day recalls (mid-week and weekend) will be combined using the Multiple Source Method (MSM) (103). The first recall for each participant will be realized in person, while subsequent recalls will be conducted via telephone to minimize participant burden.
Anorexia
Anorexia will be assessed by the appetite Visual Analog Scale (VAS). The VAS result for anorexia is obtained by measuring the distance, in millimeters, from the 0 mm point (“I had no appetite at all”) to the point marked by the subject on a line whose maximum value is 100mm (“My appetite was very good”). Values equal to or lower than 70 indicate anorexia (104).
Additionally, to evaluate the severity of anorexia symptoms, an adapted version of the conceptual subscale of food aversion from the cachexia questionnaire of the European Organization for Research and Treatment of Cancer (QLQ-CAX24) to Brazilian Portuguese (Supplementary Table 5) will be used. This scale divides anorexia symptoms into five questions, which address: pleasantness of food taste/texture; desire to put off a meal because of its smell/quantity; and early satiety (105). Both instruments are filled out by the participants based on their experiences regarding their appetite over the last 7 days.
Malnutrition risk screening
The 3-Minute Nutrition Screening (3-MinNS) (106), version adapted to Brazilian Portuguese, will be applied by the research team to assess malnutrition risk. This tool, of quick and easy applicability, had the best sensitivity and specificity among 18 other tools for malnutrition assessment according to a recent systematic review (107). Its score is composed of items ranging from 0 to 3 that assess: weight loss, food consumption, and loss of muscle mass. A final score greater than or equal to 3 indicates nutritional risk; 3-4 points indicates risk of moderate malnutrition; and 5-9 risk of severe malnutrition.
Quality of life
Quality of life must be measured using the official Portuguese version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core (EORTC QLQ-C30). This questionnaire is a multidimensional, self-administered instrument that measures the quality of life in cancer patients through 30 items that address functional, symptomatic and global health status aspects in the preceding 7 days (108). Global health questions are scored on a scale ranging from 1 to 7, while all other questions follow a four-point Likert scale.
Supplementing the QLQ-C30, the EORTC QLQ-CAX24 questionnaire will be applied. It was specifically developed to assess the impact of cancer cachexia through five multi-item scales (food aversion, concern about food and weight loss, difficulty eating, loss of control, and physical decline) and by four other single items (105).
Comorbidity load
Participants’ comorbidity load will be assessed at baseline using the Updated Charlson Comorbidity Index (uCCI) (109) through an adapted questionnaire (110). This index lists twelve comorbidities with weights ranging from 1 to 6. The final score is calculated by the summing of the weights and has a minimum value of 0 and a maximum of 28, but as in this study the scores referring to solid tumors and metastasis will not be computed, the maximum score will be 18. The uCCI is shown to be methodologically valid and reliable for clinical research (111), and has demonstrated prognostic validity for mortality in short-term longitudinal studies and a positive association with 30-day mortality in colorectal surgery (112).
Postoperative complications
The most frequent and general post-surgical complications will be defined according to the European Perioperative Clinical Outcome (EPCO) definitions (113). The degree of severity of each complication will be rated on a scale of 1 to 5 using the Clavien-Dindo scale (114), which is effective in assessing the negative impact of post-colorectal resection complications; and as mild, moderate, or severe according to criteria standardized by the European Society of Intensive Care Medicine - European Society of Anaesthesiology (ESICM - ESA) task force (115). The Comprehensive Complication Index (CCI) (116) will be used to summarize in a single continuous measure the overall morbidity in the post-operative period, combining all postoperative complications, each one scored using the Clavien-Dindo scale, resulting in a final score that ranges from 0 to 100.
Pre-, intra-, and post-operative parameters
Total surgical time, technique (laparotomy vs laparoscopy), surgical conversion rate, and Surgical Apgar Score (SAS) (116) will be collected at surgery. The SAS, which produces a maximum score of 10 points based on three intraoperative variables (heart rate; mean arterial pressure; and estimated blood loss), is able to predict the risk of post-surgical complications and 30-day mortality, including from colorectal resections (117).
In addition, during the first 30 postoperative days, the following variables will be prospectively collected from medical records: length of stay (number of days between surgery and hospital discharge), ICU (Intensive Care Unit) length of stay (total days between ICU admission and discharge to medical clinic), time to evacuation (number of days until first bowel movement), readmission rate (relative frequency of readmitted patients after discharge), and reoperation rate (relative frequency of reoperations). Mortality rate (relative frequency of deaths) will be collected over 90 days, as recommended (113), and rates for 30 and 90 days will be reported.
To assess the general quality of perioperative care, we will assess the compliance with the Enhanced Recovery After Surgery (ERAS) colorectal protocol (118), which has been negatively associated with postoperative complications (119, 120). To do this, a checklist was created with the 25 ERAS recommendation items and their descriptions. Each participant’s care will be described based on the degree to which the items were implemented, individually categorized as non-adherence, partial adherence, or complete adherence (Supplementary Table 6). The total and item-specific relative frequencies of these categories will be summarized for study groups and participant centers.
Gastrointestinal symptoms
The Brazilian Portuguese translated version (121) of the Gastrointestinal Symptom Rating Scale (GSRS) (122, 123) will be used to assess the participants’ perception of gastrointestinal symptoms, which may be compromised to some degree because of the cancer itself, the tumor site, and/or the perioperative context. This tool, which has already been used in similar settings (124, 125), evaluates in a seven-point Likert scale fifteen questions that address: abdominal pain, gastroesophageal reflux, diarrhea, indigestion and constipation.
Muscle mRNA expression
For total RNA (RNAtot) isolation, muscle tissue samples will be lysed and homogenized in TRIzol™ Reagent (Invitrogen, Carlstad, USA) according to manufacturer’s protocol. Briefly, RNAtot precipitate will be washed in 75% ethanol and then resuspended in RNase-free water. Total nucleic acid content and sample purity will be determined by spectrophotometry at 260 and 280 nm. Next, reverse transcription of RNAtot will be performed using M-MLV Reverse Transcriptase (Invitrogen, Carlstad, USA), oligo (dT) primer, and a dNTP mix. Forward and reverse primers for the atrogenes (TRIM63, FBXO32, CAPN3, CTSB, CTSL), mito-genes (FIS1, MFN2, TFAM, PPARGC1A) and GADPH will be designed according to the NCBI RefSeq (126) sequences using Primer-BLAST (127). qRT-PCR will be performed for amplification and quantification of mRNA expression using SYBR Green Supermix (Bio-Rad Laboratories, Hercules, CA, USA). The relative fold change expression will be the final result using glyceraldehyde 3-phosphate dehydrogenase (GAPDH) as a housekeeping gene.
Muscle total protein carbonylation
Concentration of carbonylated proteins in muscle tissue will be determined according to the protocol provided in the Protein Carbonyl Content Assay MAK094 kit (Merck KGaA, Darmstadt, Germany). Briefly, to the diluted muscle sample (protein concentration of 10 mg/mL) will be added 100μL of DNPH Solution. After vortexing and incubating for 10 minutes at room temperature, 30 uL of trichloroacetic acid will be added per sample, then centrifuged at 13,000 x g for 2 minutes to remove the supernatant. Each pellet will receive an ice-cold acetone bath (-20°C) for free DNPH removal, and then 200 microlitres of guanidine solution will be added to resolubilize proteins. The absorbance will be measured at 375 nm in a multiwell plate. A volume of 5μl from these final samples will be used to perform bicinchoninic acid (BCA) assay to measure protein concentration using bovine serum albumin (BSA) as standard curve. The final concentration of the carbonylated proteins will be reported as nmol carbonyl/mg protein.
Muscle lipid peroxidation
Briefly, following MAK085 kit instructions (Merck KGaA, Darmstadt, Germany), samples of muscle tissue will be homogenized on ice with MDA Lysis Buffer and centrifuged (13,000 x g for 10 min) to remove insoluble material. The supernatant will be incubated with thiobarbituric acid solution at 95°C for 60 minutes. After cooling in ice bath, the absorbance of the resulting reaction mixture sample will be measured using a spectrophotometer at 532 nm. The malondialdehyde (MDA) concentration will be reported in nmol/mL.
Muscle mitochondrial morphology
Muscle samples will be cut into 2 mm slices, fixed immediately in 10% neutral buffered formalin (NBF), embedded in Spurr resin, and then sectioned using an ultramicrotome. Scanning Transmission Electron Microscopy (STEM) will be used to provide high magnification and high-resolution images of the tissue. By means of the software ImageJ (128), intermyofibrillar mitochondrial area will be determined from the resulting STEM images.
Muscle apoptosis and inflammation
Multiplex bead-based flow cytometry assay will be used to measure multiple molecules, such as muscle apoptosis proteins, cytokines, chemokines and myokines, using the following kits: 48-669MAG (for the measurement of Akt, BAD, Bcl-2, p53, JNK, caspase-8, caspase-9), HCYTMAG-60K-PX29 (for EGF, G-CSF, GM-CSF, IFN-α2, IFN-γ, IL-1α, IL-1β,IL-1ra, IL-2, IL-3, IL-4, IL-5, IL-6,IL-7, IL-8, IL-10, IL-12p40, IL-12p70, IL-13, IL-15, IL-17A, IP-10, MCP-1, MIP-1α, MIP-1β, TNF-α, TNF-β, VEGF, Eotaxin/CCL11), and HMYOMAG-56K (for Apelin, BDNF, EPO,FABP3, FGF-21, Factalkine/CX3CL1, IL-6, IL-15, Irisin, LIF, Myostatin/GDF8, OSM, Osteocrin/Muclin, SPARC) (Merck-Millipore, St. Charles, Missouri, USA).
Muscle tissue samples will be homogenized in ice-cold lysis buffer containing proteases inhibitors. The diluted sample lysates will then be mixed with the beads and assay-specific buffer in a 1:1:1 ratio, and added to the wells for incubation and washing cycle. Afterwards, detection antibodies will be mixed, incubated and removed before analysis in Magpix® (Life Technologies, Grand Island, NY, USA). The total protein concentration of the 1:4 phosphate-buffered saline (PBS) diluted lysate will be determined by BCA assay using BSA as standard curve.
Systemic inflammation
The quantification of C-reactive protein (CRP) and albumin levels in the serum will be performed using immunoturbidimetry and colorimetry, respectively. In addition, the Glasgow Prognostic Score (GPS) (129) will be provided as an inflammatory indicator. The quantities of lymphocytes, neutrophils and platelets will be obtained from automated cell counters to calculate neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR). Finally, cytokines will be quantified from plasma with the HCYTMAG-60K-PX29 (Merck-Millipore, St. Charles, Missouri, USA) kit, employing the aforementioned method.
Fecal microbiota composition and metabolites
Individuals will collect feces from the first bowel movement of the day at home. The collection will occur with the help of a sterile toilet seat cover (ColOff®, São Paulo, Brasil). Participants will be instructed to sanitize their hands with 70% alcohol before collecting aliquots from different parts of the fecal sample using a sterile plastic scoop (130, 131). The stool will then be transferred to a sterile vial and placed in a Styrofoam box for storage in the household freezer (-16°C) (132) for a maximum period of 4 weeks. To ensure temperature preservation, the material will be shipped to the laboratory along with sterile frozen gel packs as cooling agents. The Bristol classification will be performed before homogenization and subsampling of the stool. Samples will be maintained for up to 6 months in -80°C ultra freezers (133).
Short-Chain Fatty Acids (SCFA) quantification will be conducted using liquid chromatography–mass spectrometry (LC-MS) and the SBR00030 kit (Merck KGaA, Darmstadt, Germany) according to the kit instructions. Briefly, acetone will be added to the sample, and the mixture will be centrifuged. The supernatant will be transferred to a vial and combined with 2,3,4,5,6-Pentafluorobenzyl bromide (PFB-Br) for incubation at a warm temperature. The final derivatized sample will be analyzed using a calibration curve generated from a standard curve calibrated with an SCFA mix. The concentrations of fecal acetate, butyrate and propionate will be expressed in µmol/g.
Sequence analysis and taxonomic profiling of fecal microbiota will be carried out using 16S rRNA Next Generation Sequencing (NGS). DNA extraction will be performed using the Fast DNA Stool Mini Kit (Qiagen, Hilden, Germany) following the manufacturer’s protocol. The concentration, yield, and purity of the DNA will be determined by fluorometry, while DNA length by pulsed-field gel electrophoresis (PFGE). Amplification of the V3-V4 region will be performed on a PCR system using the GoTaq® Hot Start Colorless Master Mix kit (Promega, Madison, WI, USA) and a universal primer. The resulting PCR products will be purified using the magnetic bead-based system PCRClean DX C-1003-450 (Aline Biosciences, Woburn, MA, USA). Library will be constructed using Nextera XT DNA Library Prep (Illumina, California, USA) kit according to the manufacturer’s protocol steps.
After quantification, normalization and pooling, the library will be loaded onto an Illumina MiSeq sequencer (San Diego, CA, USA) to generate FASTQ reads. The raw paired-end FASTQ reads will be merged and filtered using the QIIME 2 (Quantitative Insights Into Microbial Ecology) (134) - Deblur (135) pipeline (136). Taxonomic classification will be undertaken by the q2-feature-classifier (137) plugin using the naive Bayes machine-learning classifier method. Sample ecological alpha and beta diversity will be explored using the q2-diversity plugin.
Participants compliance
Participant compliance in longitudinal cancer studies is a recurring problem and attrition rates typically range from 10 to 30% of the initial sample (138). Thus, some strategies to increase trial retention will be implemented, such as: scheduling study visits on the same days as standard care visits; training assessors to improve data collection time and reduce participant burden; maintaining clear and empathetic communication with participants throughout the study, stressing the importance of following trial instructions; using frequent reminder emails and phone calls to reduce absenteeism during data collection and study visits; allowing participants to ask questions about study procedures via messaging application on weekdays; and attempting to locate participants who miss a scheduled visit (139).
Nevertheless, if participants express a desire to discontinue treatment, we will request permission to continue collecting data from them, once these data are valuable for the study inferences (140). Lastly, we will document any unavoidable losses to follow-up and present them in a flowchart with the corresponding causes and moments of dropout.
Data management
All data will be entered electronically by investigators at the trial site or remotely by the participants using the electronic case report forms (eCRFs) and the Research Electronic Data Capture (REDCap) software (141, 142), supported by the Federal University of São Paulo (UNIFESP). REDCap is a HIPAA-compliant (Health Insurance Portability and Accountability Act) (143) web-based software platform with an intuitive interface for data capture that allows for the implementation of strategies that facilitate data management and decrease the likelihood of errors during data input, such as: accurate date stamping, real-time monitoring of response rates, review for missing data, offline data collection, data field validation, and mandatory response fields.
Data accuracy and completeness will be monitored weekly to assess the integrity of the data. To ensure data security, access to view and modify participants’ data is protected by a strong password that only the principal investigator and the first author will have access to. A monthly backup will be made on a password-protected physical device (USB flash drive), which will be kept locked at the principal investigator room. After publication, the full dataset will be available at the Open Science Framework repository under a Creative Commons Attribution-NonCommercial-ShareAlike (CC BY-NC-SA) license, while maintaining the anonymity and confidentiality of individual participants. Data will be retained for at least 10 years after study completion.
Data monitoring
In accordance with the guidelines from the Food and Drug Administration (FDA) and European Medicines Agency (EMA) on Data Monitoring Committees (DMCs) (144, 145), a DMC will not be established for this study because this is a short-term, modest-sized study whose intervention offers low risk to participants (38). For the same reasons, no interim analysis is planned.
Statistical methods
Baseline variables will be summarized separately for the control and intervention groups using the mean and standard deviation for continuous variables, and relative frequency for categorical variables. Endpoint summarization and statistical analysis will be performed using the Full Analysis Set (FAS), which includes all randomized subjects and data collected after treatment discontinuation. The exception is for safety outcomes, which will be analyzed using the Safety Set. This set includes all participants according to the treatment they actually received for at least one day (intervention or comparator supplement).
The primary estimand (Estimand A) analysis will be based on FAS to assess the treatment superiority in attenuating the body weight change from baseline (V1) to week 8 (V4), regardless of treatment switching, discontinuation or adherence. This estimand will be estimated using a linear mixed model for repeated measurements (MMRM) method with a compound symmetry correlation matrix (rho = 0.5). All available body weight data, regardless of the occurrence of intercurrent events (ICEs), will be used (treatment policy strategy). For this estimand, missing data from participants who were lost to follow-up will be imputed by jump to reference (J2R) method, assuming a Missing Not At Random (MNAR) mechanism. The analysis model assumes a normal distribution and includes time, group, and their interaction as fixed factors, and baseline weight (kg) as a covariate (standard model). The mean difference and the 95% confidence interval will be presented with the two-sided p-value and the observed effect size.
The secondary estimand (Estimand B) will assess the efficacy of the supplement superiority in attenuating the change in body weight from baseline to week 8 in a hypothetical scenario in which no participant has low adherence levels or interrupts the intervention for any reasons other than adverse events, excluding of intake of additional fiber/antioxidant supplements, irrespective of the assigned group (hybrid hypothetical estimand). The aforementioned standard statistical model will be used to generate the estimate. To deal with ICEs, the following strategies will be implemented:
● The group variable will be defined according to the intervention participants actually received (As Treated);
● Data values after treatment interruption due to AEs will be imputed using the J2R method, for interruptions for other reasons than AEs, a Missing At Random (MAR) mechanism will be assumed for the MMRM analysis (Hypothetical strategy).
● Data from participants with low adherence (total consumption lower than 70% of the expected) will be set as missing after the first day of the two consecutive weeks of supplementation less than 70% of expected up to the end of the study (right censoring) for MMRM analysis (Hypothetical strategy).
● Participants who experience death, disease-related or not, or consume additional fiber/antioxidant supplement will be excluded from the analysis data set (Principal Stratum).
Sensitivity analysis will be conducted to explore the robustness of the results from the main estimator (standard model). The model will be tested using different missing data imputation techniques (146), correlation structures and distributions other than normal. A Generalized Linear Mixed Models (GLMM) will be used for this set of analyses, and the performance of the models will be compared using metrics such as Residual Standard Error (RSE) and Aikaike’s Information Criteria (AIC). Individual subjects will be included as a random effect in the model, and adjustments will be made for covariates such as BMI, cachexia stage, Charlson Comorbidity Index and Surgical Apgar Scale. Data analysis and visualization will be performed using the open-source free software R (73) and lmer (147) and ggplot2 (148) packages.
Adverse events and harms
As defined by the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 (149), an adverse event (AE) is any unfavorable and unintended sign, symptom or disease that is temporally associated with the use of a medical treatment or procedure that may or may not be considered related to the treatment on procedure. A serious adverse event (SAEs) is one that is life-threatening or results in death, hospitalization (initial or prolonged) or disability/permanent damage (150). All AEs will be documented in the eCRF and listed separately according to the System Organ Class (SOC). The severity of each event will be graded from 1 to 5 according to CTCAE, and its causality will be classified as unlikely, possible, probable, or definitively related. The causality of each AE will be discussed with the hospital’s surgical and clinical staff. In the event of an SAEs, the research team will immediately notify all the ethics committees involved in the study.
AEs will be monitored on a weekly basis at visits or via online questionnaires using the Patient-Reported Outcomes version of the CTCAE (PRO-CTCAE™) (151). During these evaluations, participants will report and classify AEs according to frequency and severity. The following symptoms will be evaluated: rash, acne, headache, insomnia, and anxiety, as well as an open field for other symptoms. Study staff will also be available at any time (phone or messaging application) for participants to report AEs.
Descriptive statistics will be used to summarize all reported AEs by study arm, SOC, CTCAE term, and severity. There will be no formal hypothesis testing for safety outcomes.
Auditing
There are no planned audit on-site visits. However, to ensure compliance with Good Clinical Practice (150) and guarantee the quality of the trial, the sponsor and/or regulatory authorities may have access to study-related records and visit the study site at any time to verify procedures. The study investigators will submit biannual reports to the sponsor and hospital ethical committees detailing the status of the study and ongoing procedures for independent audit.
Ethics and dissemination
Research ethics approval
This trial will be conducted in compliance with this protocol and the ethical principles outlined in the Helsinki Declaration (63) and International Council for Harmonization Guidelines for Good Clinical Practice (ICH-GCP E6) (144) in order to protect participants’ safety and rights. The study has received ethical approval from the Federal University of São Paulos’ Research Ethics Committee (CAAE number: 39368320.5.0000.5505), the Hospital Guilherme Álvaro Research Ethics Committee (CAAE number: 39368320.5.3001.5448), and the Irmandade da Santa Casa da Misericórdia de Santos Research Ethics Committee (CAAE number: 39368320.5.3001.0139). All participants must provide written informed consent before engaging in any study procedure.
Protocol amendments
Modifications to procedures that impact the conduct of the study will require mandatory protocol amendments, which must first be approved by all of the aforementioned Research Ethics Committees before being implemented. These amendments will be made public in trial registries.
Consent
The trial researchers, by having a conversation, will provide potential participants with general information about the study and its objectives, and allow time for participants to ask any questions they may have. They will be informed that it is their right to refuse participation or withdraw their consent at any time and for any reason during the study. After the initial conversation, the consent form (Supplementary Document 1) will be provided for the patients to read. Those who agree to the form must sign the document consenting to their participation in the study. In addition, participants will have the option to consent to the storage of biological specimens (rectus abdominis muscle and tumor tissues) for potential use in ancillary studies, which will require additional consent and ethical approval before being utilized.
Confidentiality
All participants’ data (CRF, eCRF and laboratory specimens) will be de-identified to protect their confidentiality by attributing a random alphanumeric identification code randomly selected from a previously generated list to each participant. Physical documents containing personal identifiers, such as consent forms, will be kept key-locked at the principal investigator’s main office, to which access is restricted to authorized persons. Password-protected access to electronic databases is limited to the principal investigator and first author only, but may be requested for auditing.
Access to data
Data access is restricted to the principal investigator and first author.
Ancillary and post-trial care
In agreement with the Declaration of Helsinki (63), participants who are still in need will have access to the intervention if its superiority is demonstrated at the end of the study. No additional post-trial care will be provided, as all recruited participants are already within a public health system with broad access to adequate clinical care. No ancillary care during the trial will be provided to participants.
Dissemination policy
The research team will publish study results in an internationally relevant, peer-reviewed scientific journal, regardless of the direction and magnitude of the findings. After publication, participants who expressed intent at study enrollment will receive by email the original report and a special document with the study results written in accessible, non-scientific language. It is important to remark that exploratory endpoints can be published as separate manuscripts, always citing the trial registration number and this protocol.
The Authorship declarations of the articles resulting from this study will adhere to the International Committee of Medical Journal Editors (ICMJE) recommendations on Authorship and Contribution.
Discussion
Cancer patients who develop cachexia during the course of their disease are more likely to experience reduced survival, quality of life deterioration, and complications at acute treatment moments, such as in the perioperative and chemotherapy periods. Currently, the literature on nutritional interventions, mainly on omega-3 fatty acids, amino acids, (e.g. leucine and β-hydroxy-beta-methyl butyrate) and rich-protein oral nutritional supplements, offers limited evidence about their efficacy and does not support their recommendation (31, 32, 152). This protocol describes the rationale, design, and methods implemented in the reported clinical trial to properly answer its main objective: to determine if grape seed flour can attenuate the weight loss during the perioperative period in patients with colorectal cancer cachexia.
Loss of muscle mass in cancer cachexia stems from several immuno-metabolic alterations, such as those caused by systemic inflammation and oxidative stress (6, 153, 154), which can lead to activation of nuclear factor kappa B (NF-κB) and subsequent stimulation of the calpain (155–158), autophagic-lysosomal (159–161) and ubiquitin-proteasome proteolytic pathways (162–164). The disruption of oxidative balance is also believed to impair protein synthesis by inhibiting the anabolic Akt-mTOR pathway (165–167), causing mitochondrial dysfunction (159) and reducing the proliferation and differentiation of muscle satellite cells (168, 169). Therefore, grape seed flour emerges as an intervention in cachexia due to the potential demonstrated in the preclinical setting that its polyphenols can reduce oxidative stress (40) and inflammation (39), counteracting muscle breakdown by inhibition of NF-κB and atrogin-1 expression (41, 170), as well as averting mitochondrial dysfunction (40, 171, 172).
Strengths
To the best of our knowledge, this is the first clinical trial to investigate the effects of a dietary fiber- and polyphenol-rich supplement in patients with pre- or cachexia associated with cancer during the perioperative period (173), a critical moment in treatment when there are often acute changes in body composition that can predict clinical outcomes. The inclusion of restrictive eligibility criteria, such as type of cancer and less advanced stages of cachexia, and the use of covariates at the time of randomization, helps to create a more homogeneous sample and increase balance between groups, improving the internal validity of the study. The secondary outcomes of the study will be evaluated using validated, widespread methods in the surgical-oncology area, and are of particular interest to patients, as they include both clinical outcomes and patient-reported outcomes.
Furthermore, an exploratory analysis will be carried out to gain valuable insights into the mechanisms of action of the intervention and to advance our understanding of cancer cachexia’s pathophysiology, with a specific emphasis on the mechanisms that orchestrate muscle depletion, which remain largely uncertain (174). This analysis will involve the assessment of different immunological, metabolic, muscular and intestinal health-related biomarkers in the clinical context. Such an approach is demanded in the field of cachexia and can significantly contribute to the understanding of the interconnected elements that constitute the whole picture of cancer cachexia (175–177).
Limitations
Although the predictive relationship between weight loss and negative clinical consequences is broadly accepted (70), one of the main limitations of the study is precisely that the primary endpoint is a surrogate outcome (178). Clinical outcomes like overall survival or postoperative complication rate are fundamental in oncology, but require a longer follow-up and larger sample sizes (179, 180), incompatible with the research funding. The use of only two participating centers is compatible with the clinical phase but reduces the generalizability of study results when compared to multicenter international clinical trials (181). Lastly, supplement’s pharmacokinetic and bioavailability will not be evaluated, and compliance with the intervention will only be assessed by the weekly consumption rate reported by the participants and by counting the returned capsules at the end of the two intervention periods, rather than through the use of biomarkers.
Ethics statement
The study was approved by the Federal University of São Paulos’ Research Ethics Committee (CAAE number: 39368320.5.0000.5505), the Hospital Guilherme Álvaro Research Ethics Committee (CAAE number: 39368320.5.3001.5448), and the Irmandade da Santa Casa da Misericórdia de Santos Research Ethics Committee (CAAE number: 39368320.5.3001.0139). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FM contributed to the manuscript writing. All authors contributed to the study conception and design, revised the manuscript, and approved the final version submitted.
Funding
This project is supported by the São Paulo Research Foundation (FAPESP) through a Regular Research Grant (Process Number: 2019/19988-2). FM received a PhD scholarship from the Coordination of Superior Level Staff Improvement (CAPES) - Finance Code 001. The grape seed flour supplement was donated by Econatura (Garibaldi, Rio Grande do Sul, Brazil).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1146479/full#supplementary-material
References
1. Vagnildhaug OM, Brunelli C, Hjermstad MJ, Strasser F, Baracos V, Wilcock A, et al. A prospective study examining cachexia predictors in patients with incurable cancer. BMC Palliat Care (2019) 18(1):46. doi: 10.1186/s12904-019-0429-2
2. Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol (2011) 12(5):489–95. doi: 10.1016/S1470-2045(10)70218-7
3. Tan BH, Fearon KC. Cachexia: prevalence and impact in medicine. Curr Opin Internal Med (2008) 7(5):441–8. doi: 10.1097/MCI.0b013e328315510b
4. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
5. Porporato PE. Understanding cachexia as a cancer metabolism syndrome. Oncogenesis (2016) 5(2):e200–0. doi: 10.1038/oncsis.2016.3
6. Argilés JM, Busquets S, Stemmler B, López-Soriano FJ. Cancer cachexia: understanding the molecular basis. Nat Rev Cancer (2014) 14(11):754–62. doi: 10.1038/nrc3829
8. Bindels LB, Neyrinck AM, Loumaye A, Catry E, Walgrave H, Cherbuy C, et al. Increased gut permeability in cancer cachexia: mechanisms and clinical relevance. Oncotarget (2018) 9(26):18224–38. doi: 10.18632/oncotarget.24804
9. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing (2019) 48(4):601–1. doi: 10.1093/ageing/afz046
10. Wallengren O, Lundholm K, Bosaeus I. Diagnostic criteria of cancer cachexia: relation to quality of life, exercise capacity and survival in unselected palliative care patients. Support Care Cancer (2013) 21(6):1569–77. doi: 10.1007/s00520-012-1697-z
11. Martin L, Birdsell L, Macdonald N, Reiman T, Clandinin MT, McCargar LJ, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol (2013) 31(12):1539–47. doi: 10.1200/JCO.2012.45.2722
12. Fukuta A, Saito T, Murata S, Makiura D, Inoue J, Okumura M, et al. Impact of preoperative cachexia on postoperative length of stay in elderly patients with gastrointestinal cancer. Nutrition (2019) 58:65–8. doi: 10.1016/j.nut.2018.06.022
13. Ross PJ, Ashley S, Norton A, Priest K, Waters JS, Eisen T, et al. Do patients with weight loss have a worse outcome when undergoing chemotherapy for lung cancers? Br J Cancer (2004) 90(10):1905–11. doi: 10.1038/sj.bjc.6601781
14. Mason MC, Garcia JM, Sansgiry S, Walder A, Berger DH, Anaya DA. Preoperative cancer cachexia and short-term outcomes following surgery. J Surg Res (2016) 205(2):398–406. doi: 10.1016/j.jss.2016.06.07
15. Hakozaki T, Nolin-Lapalme A, Kogawa M, Okuma Y, Nakamura S, Moreau-Amaru D, et al. Cancer cachexia among patients with advanced non-small-cell lung cancer on immunotherapy: An observational study with exploratory gut microbiota analysis. Cancers (2022) 14(21):5405. doi: 10.3390/cancers14215405
16. Gilmore LA, Olaechea S, Gilmore BW, Gannavarapu BS, Alvarez CM, Ahn C, et al. A preponderance of gastrointestinal cancer patients transition into Cachexia syndrome. J Cachexia Sarcopenia Muscle (2022) 13(6):2920–31. doi: 10.1002/jcsm.13086
17. Lerner L, Hayes TG, Tao N, Krieger B, Feng B, Wu Z, et al. Plasma growth differentiation factor 15 is associated with weight loss and mortality in cancer patients. J Cachexia Sarcopenia Muscle (2015) 6(4):317–24. doi: 10.1002/jcsm.12033
18. Gannavarapu BS, Lau SKM, Carter K, Cannon NA, Gao A, Ahn C, et al. Prevalence and survival impact of pretreatment cancer-associated weight loss: A tool for guiding early palliative care. J Oncol Pract (2018) 14(4):e238–e250. doi: 10.1200/jop.2017.025221
19. Rich NE, Phen S, Desai N, Mittal S, Yopp AC, Yang JD, et al. Cachexia is prevalent in patients with hepatocellular carcinoma and associated with worse prognosis. Clin Gastroenterol Hepatol (2022) 20(5):e1157–e1169. doi: 10.1016/j.cgh.2021.09.022
20. Vanhoutte G, van de Wiel M, Wouters K, Sels M, Bartolomeeussen L, De Keersmaecker S, et al. Cachexia in cancer: What is in the definition? BMJ Open Gastroenterol (2016) 3(1). doi: 10.1136/bmjgast-2016-000097
21. Wakabayashi H, Arai H, Inui A. The regulatory approval of anamorelin for treatment of cachexia in patients with non-small cell lung cancer, gastric cancer, pancreatic cancer, and colorectal cancer in Japan: Facts and numbers. J Cachexia Sarcopenia Muscle (2020) 12(1):14–6. doi: 10.1002/jcsm.12675
22. Roeland EJ, Bohlke K, Baracos VE, Bruera E, Del Fabbro E, Dixon S, et al. Management of cancer cachexia: ASCO guideline. J Clin Oncol (2020) 38(21):2438–53.1. doi: 10.1200/jco.20.00611
23. Kalra EK. Nutraceutical-definition and introduction. AAPS PharmSci (2003) 5(3):27–8. doi: 10.1208/ps050325
24. Frank J, Fukagawa NK, Bilia AR, Johnson EJ, Kwon O, Prakash V, et al. Terms and nomenclature used for plant-derived components in nutrition and related research: Efforts toward harmonization. Nutr Rev (2019) 78(6):451–8. doi: 10.1093/nutrit/nuz081
25. Park B, You S, Cho WC, Choi J-Y, Lee MS. A systematic review of herbal medicines for the treatment of cancer cachexia in animal models. J Zhejiang University-SCIENCE B (2019) 20(1):9–22. doi: 10.1631/jzus.b1800171
26. Freitas RDS, Campos MM. Protective effects of omega-3 fatty acids in cancer-related complications. Nutrients (2019) 11(5):1–23. doi: 10.3390/nu11050945
27. Francaux M, Deldicque L. Using polyphenol derivatives to prevent muscle wasting. Curr Opin Clin Nutr Metab Care (2018) 21(3):159–63. doi: 10.1097/MCO.0000000000000455
28. You JS, Park MN, Song W, Lee YS. Dietary fish oil alleviates soleus atrophy during immobilization in association with Akt signaling to p70s6k and E3 ubiquitin ligases in rats. Appl Physiol Nutr Metab (2010) 35(3):310–8. doi: 10.1139/H10-022
29. Whitehouse AS, Smith HJ, Drake JL, Tisdale MJ. Mechanism of attenuation of skeletal muscle protein catabolism in cancer cachexia by eicosapentaenoic acid. Cancer Res (2001) 61(9):598–602. Available at: https://aacrjournals.org/cancerres/article/61/9/3604/508735/Mechanism-of-Attenuation-of-Skeletal-Muscle
30. Gorjao R, Momesso dos Santos CM, Duarte Afonso Serdan T, Sousa Diniz VL, Alba-Loureiro TC, Cury-Boaventura MF, et al. New insights on the regulation of cancer cachexia by N-3 polyunsaturated fatty acids. Pharmacol Ther (2019) 196:117–34. doi: 10.1016/j.pharmthera.2018.12.001
31. Dewey A, Baughan C, Dean TP, Higgins B, Johnson I. Eicosapentaenoic acid (EPA, an omega-3 fatty acid from fish oils) for the treatment of Cancer cachexia. Cochrane Database Systematic Rev (2007) 2017(12):1–36. doi: 10.1002/14651858.cd004597.pub2
32. Mochamat, Cuhls H, Marinova M, Kaasa S, Stieber C, Conrad R, et al. A systematic review on the role of vitamins, minerals, proteins, and other supplements for the treatment of cachexia in cancer: a European Palliative Care Research Centre cachexia project. J Cachexia Sarcopenia Muscle (2017) 8(1):25–39. doi: 10.1002/jcsm.12127
33. Shi J, Yu J, Pohorly JE, Kakuda Y. Polyphenolics in grape seeds—biochemistry and functionality. J Medicinal Food (2003) 6(4):291–9. doi: 10.1089/109662003772519831
34. Costa GN, Tonon RV, Mellinger-Silva C, Galdeano MC, Iacomini M, Santiago MC, et al. Grape seed pomace as a valuable source of antioxidant fibers. J Sci Food Agric (2019) 99(10):4593–601. doi: 10.1002/jsfa.9698
35. Décordé K, Teissèdre PL, Sutra T, Ventura E, Cristol JP, Rouanet JM. Chardonnay grape seed procyanidin extract supplementation prevents high-fat diet-induced obesity in hamsters by improving adipokine imbalance and oxidative stress markers. Mol Nutr Food Res (2009) 53(5):659–66. doi: 10.1002/mnfr.200800165
36. Ding Y, Dai X, Jiang Y, Zhang Z, Bao L, Li Y, et al. Grape seed proanthocyanidin extracts alleviate oxidative stress and ER stress in skeletal muscle of low-dose streptozotocin- and high-carbohydrate/high-fat diet-induced diabetic rats. Mol Nutr Food Res (2013) 57(2):365–9. doi: 10.1002/mnfr.201200463
37. Seo K-H, Bartley GE, Tam C, Kim H-S, Kim D-H, Chon J-W, et al. Chardonnay grape seed flour ameliorates hepatic steatosis and insulin resistance via altered hepatic gene expression for oxidative stress, inflammation, and lipid and ceramide synthesis in diet-induced obese mice. PloS One (2016) 11(12):e0167680. doi: 10.1371/journal.pone.0167680
38. Seo K-H, Kim D-H, Jeong D, Yokoyama W, Kim H. Chardonnay grape seed flour supplemented diets alter intestinal microbiota in diet-induced obese mice. J Food Biochem (2017) 41(5):1–9. doi: 10.1111/jfbc.12396
39. Myburgh KH, Kruger MJ, Smith C. Accelerated skeletal muscle recovery after in vivo polyphenol administration. J Nutr Biochem (2012) 23(9):1072–9. doi: 10.1016/j.jnutbio.2011.05.014
40. Lambert K, Coisy-Quivy M, Bisbal C, Sirvent P, Hugon G, Mercier J, et al. Grape polyphenols supplementation reduces muscle atrophy in a mouse model of chronic inflammation. Nutrition (2015) 31(10):1275–83. doi: 10.1016/j.nut.2015.04.022
41. Wang B, Yang G, Liang X, Zhu M, Du M. Grape seed extract prevents skeletal muscle wasting in interleukin 10 knockout mice. BMC Complement Altern Med (2014) 14(1):2–8. doi: 10.1186/1472-6882-14-162
42. Park E, Edirisinghe I, Choy YY, Waterhouse A, Burton-Freeman B. Effects of grape seed extract beverage on blood pressure and metabolic indices in individuals with pre-hypertension: a randomised, double-blinded, two-arm, parallel, placebo-controlled trial. Br J Nutr (2015) 115(2):226–38. doi: 10.1017/s0007114515004328
43. Razavi SM, Gholamin S, Eskandari A, Mohsenian N, Ghorbanihaghjo A, Delazar A, et al. Red grape seed extract improves lipid profiles and decreases oxidized low-density lipoprotein in patients with mild hyperlipidemia. J Med Food (2013) 16(3):255–8. doi: 10.1089/jmf.2012.2408
44. Sano A. Safety Assessment of 4-week oral intake of proanthocyanidin-rich grape seed extract in healthy subjects. Food Chem Toxicol (2017) 108:519–23. doi: 10.1016/j.fct.2016.11.021
45. Bejaoui W, Mahmoudi M, Charradi K, Abbes-Belhadj M, Boukhalfa H, Ben-Attia M, et al. Preventive and healing effect of high dosing grape seed flour on CKD patients of various stages and aetiologies. Biomarkers (2022) 27(8):795–801. doi: 10.1080/1354750X.2022.2125580
46. Bitting RL, Tooze JA, Isom S, Petty WJ, Grant SC, Desnoyers RJ, et al. Phase I study of muscadine grape extract for patients with advanced cancer. Am J Clin Oncol (2021) 44(6):239–46. doi: 10.1097/COC.0000000000000814
47. Baracos VE, Martin L, Korc M, Guttridge DC, Fearon KCH. Cancer-associated cachexia. Nat Rev Dis Primers (2018) 4(1):1–18. doi: 10.1038/nrdp.2017.105
48. Wild CP, Weiderpass E, Stewart BW. World cancer report: cancer research for cancer prevention. Lyon, France: International Agency for Research on Cancer (2020). Available at: http://publications.iarc.fr/586.
49. Huang DD, Wang SL, Zhuang CL, Zheng BS, Lu JX, Chen FF, et al. Sarcopenia, as defined by low muscle mass, strength and physical performance, predicts complications after surgery for colorectal cancer. Colorectal Dis (2015) 17(11):256–64. doi: 10.1111/codi.13067
50. Lieffers JR, Bathe OF, Fassbender K, Winget M, Baracos VE. Sarcopenia is associated with postoperative infection and delayed recovery from colorectal cancer resection surgery. Br J Cancer (2012) 107(6):931–6. doi: 10.1038/bjc.2012.350
51. Vergara-Fernandez O, Trejo-Avila M, Salgado-Nesme N. Sarcopenia in patients with colorectal cancer: A comprehensive review. World J Clin Cases (2020) 8(7):1188–202. doi: 10.12998/wjcc.v8.i7.1188
52. Sun G, Li Y, Peng Y, Lu D, Zhang F, Cui X, et al. Can sarcopenia be a predictor of prognosis for patients with non-metastatic colorectal cancer? A systematic review and meta-analysis. Int J Colorectal Dis (2018) 33(10):1419–27. doi: 10.1007/s00384-018-3128-1
53. International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. Addendum on estimands and sensitivity analysis in clinical trials to the Guideline on Statistical Principles for Clinical Trials (2019). Available at: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e9-r1-addendum-estimands-sensitivity-analysis-clinical-trials-guideline-statistical-principles_en.pdf.
54. Kahan BC, Morris TP, White IR, Carpenter J, Cro S. Estimands in published protocols of randomised trials: urgent improvement needed. Trials (2021) 22(1):686. doi: 10.1186/s13063-021-05644-4
55. Lynggaard H, Bell J, Lösch C, Besseghir A, Rantell K, Schoder V, et al. Principles and recommendations for incorporating estimands into clinical study protocol templates. Trials (2022) 23(1):685. doi: 10.1186/s13063-022-06515-2
56. Chan AW, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin JA, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ (2013) 346:e7586. doi: 10.1136/bmj.e7586
57. Loudon K, Treweek S, Sullivan F, Donnan P, Thorpe KE, Zwarenstein M. The PRECIS-2 tool: designing trials that are fit for purpose. BMJ (2015) 350:h2147. doi: 10.1136/bmj.h2147
58. Instituto Brasileiro de Geografia e Estatística — IBGE. Censo Demográfico de 2022. Rio de Janeiro: IBGE (2022). Available at: https://cidades.ibge.gov.br/.
59. Brierley JD, Gospodarowicz MK, Wittekind C. TNM classification of Malignant tumours. Chichester, West Sussex, UK: John Wiley & Sons, Inc (2017).
61. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl (2013) 3(1):1–150. doi: 10.1038/kisup.2012.64
62. Freedman B. Equipoise and the ethics of clinical research. N Engl J Med (1987) 317(3):141–5. doi: 10.1056/NEJM198707163170304
63. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA (2013) 310(20):2191–4. doi: 10.1001/jama.2013.281053
64. Bach Knudsen KE, Nørskov NP, Bolvig AK, Hedemann MS, Laerke HN. Dietary fibers and associated phytochemicals in cereals. Mol Nutr Food Res (2017) 61(7). doi: 10.1002/mnfr.201600518
65. Norager CB, Jensen MB, Madsen MR, Qvist N, Laurberg S. Effect of darbepoetin alfa on physical function in patients undergoing surgery for colorectal cancer. A randomized, double-blind, placebo-controlled study. Oncology (2006) 71(3-4):212–20. doi: 10.1159/000106071
66. Suen M, Liew A, Turner JD, Khatri S, Lin Y, Raso KL, et al. Short-term multimodal prehabilitation improves functional capacity for colorectal cancer patients prior to surgery. Asia Pac J Clin Oncol (2022) 18(2):e103–10. doi: 10.1111/ajco.13564
67. Han SR, Bae JH, Lee CS, Al-Sawat A, Park SJ, Lee HJ, et al. Serial measurements of body composition using bioelectrical impedance and clinical usefulness of phase angle in colorectal cancer. Nutr Clin Pract (2022) 37(1):153–66. doi: 10.1002/ncp.10754
68. Houborg KB, Jensen MB, Hessov I, Laurberg S. Little effect of physical training on body composition and nutritional intake following colorectal surgery–a randomised placebo-controlled trial. Eur J Clin Nutr (2005) 59(8):969–77. doi: 10.1038/sj.ejcn.1602198
69. Lakens D. Performing high-powered studies efficiently with sequential analyses. Eur J Soc Psychol (2014) 44(7):701–10. doi: 10.1002/ejsp.2023
70. Martin L, Senesse P, Gioulbasanis I, Antoun S, Bozzetti F, Deans C, et al. Diagnostic criteria for the classification of cancer-associated weight loss. J Clin Oncol (2015) 33(1):90–9. doi: 10.1200/JCO.2014.56.1894
71. Lu K, Luo X, Chen P-Y. Sample Size Estimation for repeated measures analysis in randomized clinical trials with missing data. Int J Biostatistics (2008) 4(1):1–16. doi: 10.2202/1557-4679.1098
72. Jin M, Polis A, Hartzel J. Algorithms for minimization randomization and the implementation with an R package. Commun Stat - Simulation Computation (2019) 50(10):3077–87. doi: 10.1080/03610918.2019.1619765
73. The R project for statistical computing. Available at: https://www.R-project.org/.
74. Meng H, Janssen PML, Grange RW, Yang L, Beggs AH, Swanson LC, et al. Tissue triage and freezing for models of skeletal muscle disease. J Vis Exp (2014) 89:1–8. doi: 10.3791/51586
75. Joyce NC, Oskarsson B, Jin LW. Muscle biopsy evaluation in neuromuscular disorders. Phys Med Rehabil Clin N Am (2012) 3):609–31. doi: 10.1016/j.pmr.2012.06.006
76. Anoveros-Barrera A, Bhullar AS, Stretch C, Esfandiari N, Dunichand-Hoedl AR, Martins KJB, et al. Clinical and biological characterization of skeletal muscle tissue biopsies of surgical cancer patients. J Cachexia Sarcopenia Muscle (2019) 10(6):1356–77. doi: 10.1002/jcsm.12466
77. Mager SR, Oomen MHA, Morente MM, Ratcliffe C, Knox K, Kerr DJ, et al. Standard operating procedure for the collection of fresh frozen tissue samples. Eur J Cancer (2007) 43(5):828–34. doi: 10.1016/j.ejca.2007.01.002
78. National Cancer Institute (NCI) of the National Institute of Health (NIH). Snap-freezing of post-surgical tissue biospecimens (2014). Available at: https://biospecimens.cancer.gov/global/pdfs/NCI_BEBP_Snap-freezing_of_Post-surgical_Tissue_Biospecimens.pdf.
79. Engel KB, Vaught J, Moore HM. National Cancer Institute Biospecimen Evidence-Based Practices: a novel approach to pre-analytical standardization. Biopreserv Biobank (2014) 12(2):148–50. doi: 10.1089/bio.2013.0091
80. Jones L, Craig C. Tissue handling for molecular pathology. The Bulletin of The Royal College of Pathologists (2017) 180:327–32.
81. World Health Organization. WHO guidelines on drawing blood: best practices in phlebotomy. World Health Organization, Geneva (2010) p. 1–125. Available at: https://www.euro.who.int/:data/assets/pdf_file/0005/268790/WHO-guidelines-on-drawing-blood-best-practices-in-phlebotomy-Eng.pdf.
82. Tuck MK, Chan DW, Chia D, Godwin AK, Grizzle WE, Krueger KE, et al. Standard operating procedures for serum and plasma collection: early detection research network consensus statement standard operating procedure integration working group. J Proteome Res (2009) 8(1):113–7. doi: 10.1021/pr800545q
83. United States Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES), 1999-2000. Inter-university Consortium for Political and Social Research [distributor], (2012). doi: 10.3886/ICPSR25501.v4
84. Lohman TJ, Roache AF, Martorell R. Anthropometric standardization reference manual. Med Sci Sports Exercise (1992) 24(8):952. doi: 10.1249/00005768-199208000-00020
85. Steiner MC, Barton RL, Singh SJ, Morgan MDL. Bedside methods versus dual energy X-ray absorptiometry for body composition measurement in COPD. Eur Respir J (2002) 19(4):626–31. doi: 10.1183/09031936.02.00279602
86. Ræder H, Kværner AS, Henriksen C, Florholmen G, Henriksen HB, Bøhn SK, et al. Validity of bioelectrical impedance analysis in estimation of fat-free mass in colorectal cancer patients. Clin Nutr (2018) 37(1):292–300. doi: 10.1016/j.clnu.2016.12.028
87. Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Manuel Gómez J, et al. Bioelectrical impedance analysis—part II: Utilization in clinical practice. Clin Nutr (2004) 23(6):1430–53. doi: 10.1016/j.clnu.2004.09.012
88. Brantlov S, Jødal L, Lange A, Rittig S, Ward LC. Standardisation of bioelectrical impedance analysis for the estimation of body composition in healthy paediatric populations: a systematic review. J Med Eng Technol (2017) 41(6):460–79. doi: 10.1080/03091902.2017.1333165
89. Mourtzakis M, Prado CMM, Lieffers JR, Reiman T, McCargar LJ, Baracos VE. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab (2008) 33(5):997–1006. doi: 10.1139/H08-075
90. Xiao J, Caan BJ, Cespedes Feliciano EM, Meyerhardt JA, Peng PD, Baracos VE, et al. Association of low muscle mass and low muscle radiodensity with morbidity and mortality for colon cancer surgery. JAMA Surg (2020) 155(10):942–9. doi: 10.1001/jamasurg.2020.2497
91. MacDermid J, Solomon G, Valdes K eds. Clinical assessment recommendations. American Society of Hand Therapists, Mount Laurel, N. J. (2015).
92. Ishikawa NM, Thuler LCS, Giglio AG, Baldotto CS da R, de Andrade CJC, Derchain SFM. Validation of the Portuguese version of functional assessment of cancer therapy-fatigue (FACT-F) in Brazilian cancer patients. Support Care Cancer (2010) 18(4):481–90. doi: 10.1007/s00520-009-0697-0
93. Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E. Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. J Pain Symptom Manage (1997) 13(2):63–74. doi: 10.1016/S0885-3924(96)00274-6
94. Van Belle S, Paridaens R, Evers G, Kerger J, Bron D, Foubert J, et al. Comparison of proposed diagnostic criteria with FACT-F and VAS for cancer-related fatigue: proposal for use as a screening tool. Support Care Cancer (2005) 13(4):246–54. doi: 10.1007/s00520-004-0734-y
95. Centers for Disease Control and Prevention. National health and nutrition examination survey (Nhanes): phone follow-up dietary interviewer procedures manual. CreateSpace (2002). p. 365.
96. Steinfeldt L, Anand J, Murayi T. Food reporting patterns in the USDA automated multiple-pass method. Proc Food Science (2013) 2:145–56. doi: 10.1016/j.profoo.2013.04.022
97. Casey PH, Goolsby SL, Lensing SY, Perloff BP, Bogle ML. The use of telephone interview methodology to obtain 24-hour dietary recalls. J Am Diet Assoc (1999) 99(11):1406–11. doi: 10.1016/S0002-8223(99)00340-5
98. Crispim SP, Fisberg RM, Lobo M, Steluti J. Manual fotográfico de quantificação alimentar. Curitiba: Universidade Federal do Paraná (2017).
99. Rothwell JA, Perez-Jimenez J, Neveu V, Medina-Remon A, M’Hiri N, Garcia-Lobato P, et al. Phenol-explorer 3.0: A major update of the phenol-explorer database to incorporate data on the effects of food processing on polyphenol content. Database (2013) 2013(0):1–8. doi: 10.1093/database/bat070
100. Caivano S, Domene SM. NutrabemPro [computer program on the Internet]. Brasil: Universidade Federal de São Paulo. (2009). Available at: https://nutrabem.unifesp.br/.
101. US Department of Agriculture, Agricultural Research Service, Nutrient Data Laboratory. USDA National Nutrient Database for Standard Reference, Release 28 (Slightly revised). Version Current: May 2016 (2016). Internet: http://www.ars.usda.gov/ba/bhnrc/ndl
102. Núcleo de Estudos e Pesquisas em Alimentação – NEPA. Tabela Brasileira de Composição de Alimentos (TACO). Campinas, Brasil: NEPA - UNICAMP (2011).
103. Harttig U, Haubrock J, Knüppel S, Boeing H. EFCOVAL Consortium. The MSM program: web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur J Clin Nutr (2011) 65 Suppl 1:S87–91. doi: 10.1038/ejcn.2011.92
104. Blauwhoff-Buskermolen S, Ruijgrok C, Ostelo RW, de Vet HCW, Verheul HMW, de van der Schueren MAE, et al. The assessment of anorexia in patients with cancer: cut-off values for the FAACT-A/CS and the VAS for appetite. Support Care Cancer (2016) 24(2):661–6. doi: 10.1007/s00520-015-2826-2
105. Wheelwright SJ, Hopkinson JB, Darlington AS, Fitzsimmons DF, Fayers P, Balstad TR, et al. Development of the EORTC QLQ-CAX24, A questionnaire for cancer patients with cachexia. J Pain Symptom Manage (2017) 53(2):232–42. doi: 10.1016/j.jpainsymman.2016.09.010
106. Lim SL, Tong CY, Ang E, Lee EJC, Loke WC, Chen Y, et al. Development and validation of 3-Minute Nutrition Screening (3-MinNS) tool for acute hospital patients in Singapore. Asia Pac J Clin Nutr (2009) 18(3):395–403. Available at: https://apjcn.nhri.org.tw/issue/2009-3/
107. Miller J, Wells L, Nwulu U, Currow D, Johnson MJ, Skipworth RJE. Validated screening tools for the assessment of cachexia, sarcopenia, and malnutrition: a systematic review. Am J Clin Nutr. (2018) 108(6):1196–208. doi: 10.1093/ajcn/nqy244
108. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst (1993) 85(5):365–76. doi: 10.1093/jnci/85.5.365
109. Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol (2011) 173(6):676–82. doi: 10.1093/aje/kwq433
110. Katz JN, Chang LC, Sangha O, Fossel AH, Bates DW. Can comorbidity be measured by questionnaire rather than medical record review? Med Care (1996) 34(1):73–84. doi: 10.1097/00005650-199601000-00006
111. de Groot V, Beckerman H, Lankhorst G, Bouter L. How to measure comorbidity: A critical review of available methods. J Clin Epidemiol (2004) 57(3):323. doi: 10.1016/j.jclinepi.2003.09.002
112. Niemeläinen S, Huhtala H, Ehrlich A, Kössi J, Jämsen E, Hyöty M. Risk factors of short-term survival in the aged in elective colon cancer surgery: a population-based study. Int J Colorectal Dis (2020) 35(2):307–15. doi: 10.1007/s00384-019-03488-8
113. Jammer I, Wickboldt N, Sander M, Smith A, Schultz MJ, Pelosi P, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol (2015) 32(2):88–105. doi: 10.1097/EJA.0000000000000118
114. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg (2004) 240(2):205–13. doi: 10.1097/01.sla.0000133083.54934.ae
115. Slankamenac K, Graf R, Barkun J, Puhan MA, Clavien PA. The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann Surg (2013) 258(1):1–7. doi: 10.1097/SLA.0b013e318296c732
116. Gawande AA, Kwaan MR, Regenbogen SE, Lipsitz SA, Zinner MJ. An Apgar score for surgery. J Am Coll Surg (2007) 204(2):201–8. doi: 10.1016/j.jamcollsurg.2006.11.011
117. Regenbogen SE, Bordeianou L, Hutter MM, Gawande AA. The intraoperative Surgical Apgar Score predicts postdischarge complications after colon and rectal resection. Surgery (2010) 148(3):559–66. doi: 10.1016/j.surg.2010.01.015
118. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS) society recommendations: 2018. World J Surg (2019) 43(3):659–95. doi: 10.1007/s00268-018-4844-y
119. Ripollés-Melchor J, Abad-Motos A, Díez-Remesal Y, Aseguinolaza-Pagola M, Padin-Barreiro L, Sánchez-Martín R, et al. Association between use of enhanced recovery after surgery protocol and postoperative complications in total hip and knee arthroplasty in the postoperative outcomes within enhanced recovery after surgery protocol in elective total hip and knee arthroplasty study (POWER2). JAMA Surg (2020) 155(4):e196024. doi: 10.1001/jamasurg.2019.6024
120. Ni X, Jia D, Chen Y, Wang L, Suo J. Is the enhanced recovery after surgery (ERAS) program effective and safe in laparoscopic colorectal cancer surgery? A meta-analysis of randomized controlled trials. J Gastrointest Surg (2019) 23(7):1502–12. doi: 10.1007/s11605-019-04170-8
121. Souza GS, Sardá FAH, Giuntini EB, Gumbrevicius I, de Morais MB, de Menezes EW. Translation and validation of the Brazilian portuguese version of the gastrointestinal symptom rating scale (Gsrs) questionnaire. Arq Gastroenterol (2016) 53(3):146–51. doi: 10.1590/S0004-28032016000300005
122. Revicki DA, Wood M, Wiklund I, Crawley J. Reliability and validity of the Gastrointestinal Symptom Rating Scale in patients with gastroesophageal reflux disease. Qual Life Res (1998) 7(1):75–83. doi: 10.1023/A:1008841022998
123. Svedlund J, Sjödin I, Dotevall G. GSRS–a clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig Dis Sci (1988) 33(2):129–34. doi: 10.1007/BF01535722
124. Tanabe H, Higurashi T, Takatsu T, Misawa N, Yoshihara T, Goto S, et al. Effects of colorectal endoscopic submucosal dissection on postoperative abdominal symptoms: a prospective observational study. Surg Endosc (2022) 36(1):314–20. doi: 10.1007/s00464-020-08278-w
125. Li Z, Ma Y, Liu G, Fang M, Xue Y. Proximal gastrectomy with gastric tube reconstruction or jejunal interposition reconstruction in upper-third gastric cancer: which offers better short-term surgical outcomes? BMC Surg (2021) 21(1):249. doi: 10.1186/s12893-021-01239-7
126. O’Leary NA, Wright MW, Brister JR, Ciufo S, Haddad D, McVeigh R, et al. Reference sequence (RefSeq) database at NCBI: current status, taxonomic expansion, and functional annotation. Nucleic Acids Res (2016) 44(D1):D733–45. doi: 10.1093/nar/gkv1189
127. Ye J, Coulouris G, Zaretskaya I, Cutcutache I, Rozen S, Madden TL. Primer-BLAST: a tool to design target-specific primers for polymerase chain reaction. BMC Bioinf (2012) 13:134. doi: 10.1186/1471-2105-13-134
128. Schneider CA, Rasband WS, Eliceiri KW. NIH Image to ImageJ: 25 years of image analysis. Nat Methods (2012) 9(7):671–5. doi: 10.1038/nmeth.2089
129. McMillan DC. The systemic inflammation-based Glasgow prognostic score: A decade of experience in patients with cancer. Cancer Treat Rev (2013) 39(5):534–40. doi: 10.1016/j.ctrv.2012.08.003
130. Hogue SR, Gomez MF, da Silva WV, Pierce CM. A customized at-home stool collection protocol for use in microbiome studies conducted in cancer patient populations. Microb Ecol (2019) 78(4):1030–4. doi: 10.1007/s00248-019-01346-2
131. Liang Y, Dong T, Chen M, He L, Wang T, Liu X, et al. Systematic analysis of impact of sampling regions and storage methods on fecal gut microbiome and metabolome profiles. mSphere (2020) 5(1):1–13. doi: 10.1128/mSphere.00763-19
132. Wu W-K, Chen C-C, Panyod S, Chen R-A, Wu M-S, Sheen L-Y, et al. Optimization of fecal sample processing for microbiome study — the journey from bathroom to bench. J Formosan Med Assoc (2019) 118(2):545–55. doi: 10.1016/j.jfma.2018.02.005
133. Su W, Du Y, Lian F, Wu H, Zhang X, Yang W, et al. Standards for collection, preservation, and transportation of fecal samples in TCM clinical trials. Front Cell Infection Microbiol (2022) 12:783682. doi: 10.3389/fcimb.2022.783682
134. Bolyen E, Rideout JR, Dillon MR, Bokulich NA, Abnet CC, Al-Ghalith GA, et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat Biotechnol (2019) 37(8):852–7. doi: 10.1038/s41587-019-0209-9
135. Amir A, McDonald D, Navas-Molina JA, Kopylova E, Morton JT, Zech Xu Z, et al. Deblur rapidly resolves single-nucleotide community sequence patterns. mSystems (2017) 2(2):1–7. doi: 10.1128/mSystems.00191-16
136. Prodan A, Tremaroli V, Brolin H, Zwinderman AH, Nieuwdorp M, Levin E. Comparing bioinformatic pipelines for Microbial 16S rrna amplicon sequencing. PloS One (2020) 15(1):1–19. doi: 10.1371/journal.pone.0227434
137. Bokulich NA, Kaehler BD, Rideout JR, Dillon M, Bolyen E, Knight R, et al. Optimizing taxonomic classification of marker-gene amplicon sequences with QIIME 2’s q2-feature-classifier plugin. Microbiome (2018) 6(1):90. doi: 10.1186/s40168-018-0470-z
138. Le-Rademacher JG, Storrick EM, Jatoi A. Remarks on the design and analyses of longitudinal studies for cancer patients with anorexia and weight loss. J Cachexia Sarcopenia Muscle (2019) 10(6):1175–82. doi: 10.1002/jcsm.12480
139. National Research Council (US) Panel on Handling Missing Data in Clinical Trials. The prevention and treatment of missing data in clinical trials. Washington (DC): National Academies Press (US) (2010). doi: 10.17226/12955.
140. Little RJ, D’Agostino R, Cohen ML, Dickersin K, Emerson SS, Farrar JT, et al. The prevention and treatment of missing data in clinical trials. N Engl J Med (2012) 367(14):1355–60. doi: 10.1056/NEJMsr1203730
141. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al. The redcap consortium: Building an international community of Software Platform Partners. J Biomed Informatics (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
142. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J BioMed Inform (2009) 42(2):377–81. doi: 10.1016/j.jbi.2008.08.010
143. United States. Health Insurance Portability and Accountability Act of 1996. Public Law 104-191. US Statut Large (1996) 110:1936–2103.
144. Ellenberg SS, Siegel JP. “FDA and Clinical Trial Data Monitoring Committees,” In: DeMets DL, Furberg CD, Friedman LM, editors. Data Monitoring in Clinical Trials: A Case Studies Approach. New York, NY: Springer US (2006). p. 39–49. doi: 10.1007/0-387-30107-0_3
145. Committee for Medicinal Products for Human Use, Efficacy Working Party, Committee for Release for Consultation. Committee for Medicinal Products for Human use (CHMP) guideline on data monitoring committees. Stat Med (2006) 25(10):1639–45. doi: 10.1002/sim.2585
146. Cro S, Morris TP, Kenward MG, Carpenter JR. Sensitivity analysis for clinical trials with missing continuous outcome data using controlled multiple imputation: A practical guide. Stat Med (2020) 39(21):2815–42. doi: 10.1002/sim.8569
147. Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Software (2015) 67(1):1–48. doi: 10.18637/jss.v067.i01
148. Wickham H. ggplot2: elegant graphics for data analysis. Springer, New York (2016). p. 260. https://ggplot2.tidyverse.org
149. U.S. Department Of Health And Human Services. Common terminology criteria for adverse events (CTCAE) version 5.0. National Cancer Institute, National Institutes of Health, U.S. Department of Health and Human Services (2017).
150. International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use - ICH. ICH Harmonised Guideline Integrated Addendum to ICH E6(R1): Guideline for Good Clinical Practice ICH E6(R2). (2016). Available at: https://ichgcp.net/.
151. Basch E, Reeve BB, Mitchell SA, Clauser SB, Minasian LM, Dueck AC, et al. Development of the National Cancer Institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst (2014) 106(9):1–11. doi: 10.1093/jnci/dju244
152. Braha A, Albai A, Timar B, Şerban N, Sorin S, Roman D, et al. Nutritional interventions to improve cachexia outcomes in cancer—a systematic review. Medicina (2022) 58(7):966. doi: 10.3390/medicina58070966
153. Ábrigo J, Elorza AA, Riedel CA, Vilos C, Simon F, Cabrera D, et al. Role of oxidative stress as key regulator of muscle wasting during Cachexia. Oxid Med Cell Longevity (2018) 2018:1–17. doi: 10.1155/2018/2063179
154. Puig-Vilanova E, Rodriguez DA, Lloreta J, Ausin P, Pascual-Guardia S, Broquetas J, et al. Oxidative stress, redox signaling pathways, and autophagy in cachectic muscles of male patients with advanced COPD and lung cancer. Free Radical Biol Med (2015) 79:91–108. doi: 10.1016/j.freeradbiomed.2014.11.006
155. Smith IJ, Aversa Z, Hasselgren P-O, Pacelli F, Rosa F, Doglietto GB, et al. Calpain activity is increased in skeletal muscle from gastric cancer patients with no or minimal weight loss. Muscle Nerve (2011) 43(3):410–4. doi: 10.1002/mus.21893
156. Toledo M, Busquets Sílvia, Penna F, Zhou X, Marmonti E, Betancourt A, et al. Complete reversal of muscle wasting in experimental cancer cachexia: Additive effects of activin type II receptor inhibition and β-2 agonist. Int J Cancer (2015) 138(8):2021–9. doi: 10.1002/ijc.29930
157. Lin X, Chen S. Calpain inhibitors ameliorate muscle wasting in a cachectic mouse model bearing CT26 colorectal adenocarcinoma. Oncol Rep (2017) 37(3):1601–10. doi: 10.3892/or.2017.5396
158. Pin F, Minero VG, Penna F, Muscaritoli M, De Tullio R, Baccino FM, et al. Interference with ca2+-dependent proteolysis does not alter the course of muscle wasting in experimental cancer cachexia. Front Physiol (2017) 8. doi: 10.3389/fphys.2017.00213
159. Penna F, Ballarò R, Martinez-Cristobal P, Sala D, Sebastian D, Busquets S, et al. Autophagy exacerbates muscle wasting in cancer cachexia and impairs mitochondrial function. J Mol Biol (2019) 431(15):2674–86. doi: 10.1016/j.jmb.2019.05.032
160. Pigna E, Berardi E, Aulino P, Rizzuto E, Zampieri S, Carraro U, et al. Aerobic exercise and pharmacological treatments counteract cachexia by modulating autophagy in colon cancer. Sci Rep (2016) 6(1):1–14. doi: 10.1038/srep26991
161. Johns N, Hatakeyama S, Stephens NA, Degen M, Degen S, Frieauff W, et al. Clinical classification of cancer cachexia: phenotypic correlates in human skeletal muscle. PloS One (2014) 9(1):e83618–8. doi: 10.1371/journal.pone.0083618
162. Sandri M. Protein breakdown in muscle wasting: role of autophagy-lysosome and ubiquitin-proteasome. Int J Biochem Cell Biol (2013) 45(10):2121–9. doi: 10.1016/j.biocel.2013.04.023
163. Argilés JM, López-Soriano FJ, Busquets S. Mediators of cachexia in cancer patients. Nutrition (2019) 66:11–5. doi: 10.1016/j.nut.2019.03.012
164. Zhang Y, Wang J, Wang X, Gao T, Tian H, Zhou D, et al. The autophagic-lysosomal and ubiquitin proteasome systems are simultaneously activated in the skeletal muscle of gastric cancer patients with cachexia. Am J Clin Nutr (2020) 111(3):570–9. doi: 10.1093/ajcn/nqz347
165. Arthur PG, Grounds MD, Shavlakadze T. Oxidative stress as a therapeutic target during muscle wasting: considering the complex interactions. Curr Opin Clin Nutr Metab Care (2008) 11(4):408–16. doi: 10.1097/MCO.0b013e328302f3fe
166. Op den Kamp CM, Langen RC, Snepvangers FJ, de Theije CC, Schellekens JM, Laugs F, et al. Nuclear transcription factor κ B activation and protein turnover adaptations in skeletal muscle of patients with progressive stages of lung cancer cachexia. Am J Clin Nutr (2013) 98(3):738–48. doi: 10.3945/ajcn.113.058388
167. Murton AJ, Maddocks M, Stephens FB, Marimuthu K, England R, Wilcock A. Consequences of late-stage non–small-cell lung cancer cachexia on muscle metabolic processes. Clin Lung Cancer (2017) 18(1):e1–11. doi: 10.1016/j.cllc.2016.06.003
168. Kozakowska M, Pietraszek-Gremplewicz K, Jozkowicz A, Dulak J. The role of oxidative stress in skeletal muscle injury and regeneration: focus on antioxidant enzymes. J Muscle Res Cell Motil (2015) 6):377–93. doi: 10.1007/s10974-015-9438-9
169. Le Moal E, Pialoux V, Juban G, Groussard C, Zouhal H, Chazaud B, et al. Redox control of skeletal muscle regeneration. Antioxid Redox Signal (2017) 27(5):276–310. doi: 10.1089/ars.2016.6782
170. Levolger S, van den Engel S, Ambagtsheer G, IJzermans JNM, de Bruin RWF. Quercetin supplementation attenuates muscle wasting in cancer-associated cachexia in mice. Nutr Healthy Aging (2021) 6(1):35–47. doi: 10.3233/NHA-200084
171. Kunz H, Port JD, Kaufman KR, Jatoi A, Hart CR, Gries KJ, et al. Skeletal muscle mitochondrial dysfunction and muscle and whole body functional deficits in cancer patients with weight loss. J Appl Physiol (2022) 132(2):388–401. doi: 10.1152/japplphysiol.00746.2021
172. VanderVeen BN, Cardaci TD, Cunningham P, McDonald SJ, Bullard BM, Fan D, et al. Quercetin improved muscle mass and mitochondrial content in a murine model of cancer and chemotherapy-induced cachexia. Nutrients (2022) 15(1):102–2. doi: 10.3390/nu15010102
173. Orsso CE, Montes-Ibarra M, Findlay M, van der Meij BS, de van der Schueren MAE, Landi F, et al. Mapping ongoing nutrition intervention trials in muscle, sarcopenia, and cachexia: a scoping review of future research. J Cachexia Sarcopenia Muscle (2022) 13(3):1442–59. doi: 10.1002/jcsm.12954
174. Martin A, Gallot YS, Freyssenet D. Molecular mechanisms of cancer cachexia-related loss of skeletal muscle mass: data analysis from preclinical and clinical studies. J Cachexia Sarcopenia Muscle (2023) 14(3):1150–67. doi: 10.1002/jcsm.13073
175. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 8. Rating the quality of evidence–indirectness. J Clin Epidemiol (2011) 64(12):1303–10. doi: 10.1016/j.jclinepi.2011.04.014
176. Ziemons J, Smidt ML, Damink SO, Rensen SS. Gut microbiota and metabolic aspects of cancer cachexia. Best Pract Res Clin Endocrinol Metab (2021) 35(3):101508. doi: 10.1016/j.beem.2021.101508
177. McGovern J, Dolan RD, Skipworth RJ, Laird BJ, McMillan DC. Cancer cachexia: a nutritional or a systemic inflammatory syndrome? Br J Cancer (2022) 127(3):379–82. doi: 10.1038/s41416-022-01826-2
178. Dolly A, Dumas J, Servais S. Cancer cachexia and skeletal muscle atrophy in clinical studies: what do we really know? J Cachexia Sarcopenia Muscle (2020) 11(6):1413–1428. doi: 10.1002/jcsm.12633
179. Fleming TR, Powers JH. Biomarkers and surrogate endpoints in clinical trials. Stat Med (2012) 31(25):2973–84. doi: 10.1002/sim.5403
180. Fleming TR, DeMets DL. Surrogate end points in clinical trials: are we being misled? Ann Intern Med (1996) 125(7):605–13. doi: 10.7326/0003-4819-125-7-199610010-00011
Keywords: dietary fiber, dietary supplements, inflammation, neoplasms, malnutrition, polyphenols, body composition, surgery
Citation: Malta FAPS and Gonçalves DC (2024) A triple-masked, two-center, randomized parallel clinical trial to assess the superiority of eight weeks of grape seed flour supplementation against placebo for weight loss attenuation during perioperative period in patients with cachexia associated with colorectal cancer: a study protocol. Front. Endocrinol. 14:1146479. doi: 10.3389/fendo.2023.1146479
Received: 17 January 2023; Accepted: 07 December 2023;
Published: 19 January 2024.
Edited by:
Seema Parte, Stanford University, United StatesReviewed by:
Haruka Amitani, Kagoshima University, JapanZheng Ruan, Nanchang University, China
Alkhair Idris, Ahfad University for Women, Sudan
Copyright © 2024 Malta and Gonçalves. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniela Caetano Gonçalves, ZGFuaWVsYS5jYWV0YW5vQHVuaWZlc3AuYnI=