 Guicun Yang1,2
Guicun Yang1,2 Yan Zhao
Yan Zhao
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 21 September 2023
Sec. Developmental Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1048615
This article is part of the Research Topic Endocrine and Metabolic Effects on Maternal-fetal and Neonatal Outcomes View all 28 articles
Background: Fat-soluble vitamins, including vitamins A, D and E, play an important role in the regulation of glucose and lipid metabolism, and may affect infant birth weight. Evidence on the association of birthweight with fat-soluble vitamins is controversial. Therefore, this study aims is to determine the associations of birthweight with vitamin A, D, and E concentrations in cord blood.
Methods: A total of 199 mother–infant pairs were enrolled in the study. According to gestational age and birth weight, the mother–infant pairs were divided into small for gestational age (SGA), appropriate for gestational age (AGA), and large for gestational age (LGA). The Vitamin A, D, and E concentrations in serum were measured by high-performance liquid chromatography tandem-mass spectrometry.
Results: The concentrations of vitamin A in the SGA group were significantly lower than those in the AGA and LGA groups. The concentrations of vitamin E in the SGA group were significantly higher than those in the AGA and LGA groups. However, no significant differences were observed in vitamin D among the three groups. Being male (β = 0.317, p < 0.001) and birth weight (β = 0.229, p = 0.014) were positively correlated with the levels of vitamin A. Birth weight (β = -0.213, p= 0.026) was correlated with lower levels of vitamin E. No correlation was found between influencing Factors and the levels of vitamin D (p> 0.05). After adjusting for gestational age, sex, mother’s age, delivery mode, pre-pregnancy BMI, and weight gain during pregnancy, the levels of cord blood vitamin A were positively correlated with birth weight (p=0.012).
Conclusion: The infant’s birth weight is associated with the levels of cord blood vitamins A and E. The dysregulation of vitamins A and E in infants may be a risk factor for fetal growth and future metabolic diseases.
Birth weight (BW) is important to the health of the fetus, and it also predicts the subsequent development of the child. There are two types of extreme birth weight according to the gestational age and sex-specific (1): large for gestational age (LGA) and small for gestational age (SGA), and both of them increase the risk of cardiovascular disease, diabetes, and obesity later in life (2, 3). However, the mechanisms underlying the extreme birth weight and subsequent metabolic dysfunction are not well understood.
Maternal nutrition is important for fetal development and maternal health. Fat-soluble vitamins, including vitamins A, D and E, play an essential role in the regulation of glucose and lipid metabolism. Vitamin A and Vitamin D can affect obesity, cardiovascular disease, insulin resistance and type 2 diabetes (4, 5). While recent literature has found new mechanistic insights into the vitamin E derivatives in cardiovascular disease regulation (6). Vitamin E improves lipid metabolism in mice with nonalcoholic fatty liver through Nrf2/CES1 signaling pathway (7). Optimal maternal nutrition is a major factor in regulating fetal development and its lifelong consequences (8). The cord blood concentration of fat-soluble vitamins may influence the intrauterine environment, and may be associated with birth weight and lifelong metabolic dysfunction.
Evidence on the association of birthweight with fat-soluble vitamins is controversial. Recent studies have shown that premature low birth weight (LBW) infants have significantly lower cord blood vitamin A levels, and vitamin A levels in LBW infants correlate with their birth weight (9). However, Enfu Tao et al. found that cord blood vitamin A concentration in late preterm infants was not associated with birth weight (10). Some meta-analysis relating to vitamin revealed that maternal vitamin D deficiency increased the risk of SGA (OR=1.588, 95% CI 1.138-2.216) (11) and LBW (OR=2.39, 95% CI 1.25-4.57) (12). However, in the current literature, the difference in neonatal anthropometric measurements was not found between infants born to normal and vitamin D deficient mothers (13). Vitamin E was found to be positively associated with birth weight and reduced the risk of SGA (14). And one finding had been reported that high levels of vitamin E were associated with macrosomia (15).
Understanding fat-soluble vitamins in low and high birth-weight infants may provide new insights into metabolic mechanisms in newborns and help prevent subsequent metabolic diseases. This study aims to determine associations between birthweight and vitamin A, E, and D concentrations in cord blood.
Cord blood samples were collected from 199 newborns in the Department of Obstetrics of Chongqing Maternal and Child Health Hospital between June 2021 and December 2021. Inclusion criteria were singleton pregnancy, live, term birth (37–42 weeks), aged 18–42 years, no smoking and drinking history. Women with pregnancy complications, such as gestational hypertension, preeclampsia, cancer, or asthma were excluded. According to birth weight and gestational age (GA), a total of 199 mother–infant pairs were divided into SGA group (63), AGA (appropriate for gestational age) group (87), LGA group (49). Informed written consent was obtained. This study was approved by the Ethics Committee of our hospital.
Data were collected from our hospital’s electronic information system, including pre-pregnancy weight, maternal height, gestational weight gain, sociodemographic information, delivery and neonatal outcomes (GA, newborn sex, birth weight, birth length). Baby weight and birth length were measured immediately after birth. Neonatal cord blood was collected during delivery. As soon as the samples were collected, they were sent without delay to the hospital laboratory, centrifuged, and frozen at -80°C until fat-soluble vitamin levels were analyzed.
The samples were analyzed at the Neonatal Screening Center, Chongqing Health Center for Women and Children. The Vitamin A, D and E concentrations in serum were measured by high-performance liquid chromatography tandem-mass spectrometry (HPLCMS/MS) using a Waters UPLC Xevo TQS (Waters Corporation, Milford, MA, USA) described by Hao Liu et al. (16). Briefly, QCs, standards, and plasma samples were added into the corresponding wells of 96-wells plates. Protein was precipitated by adding isotopic IS in a 35:1 (v/v) mixture of methanol: isopropanol, then hexane was added to each well for extraction. The Vitamin A, D and E in serum was separated by HPLC on a Shimadzu Waters BEH C18μm 1.7 2.1*50mm column and quantitated by MS.
Birth weight was measured immediately after delivery by midwives using electronic scales to the nearest 10 g. According to the birth weight curve of newborns in China, infants with birth weight less than the 10th percentile and greater than the 90th percentile for gestational age and sex were divided into SGA and LGA (17). Prepregnancy BMI was calculated by dividing self-reported weight in kilograms by height in meters squared. Gestational weight gain was calculated from prenatal weight and pre-pregnancy weight. Babies born between 37-42 weeks of pregnancy were defined as term birth. The GA was confirmed through the use of ultrasound before week 20 of gestation.
All analyses were done with SPSS version 25.0. Data are presented as mean ± standard deviation (SD) for continuous variables, medians and interquartile range for skewed distributions, and counts (percentages) for categorical variables. Comparisons among subjects in the SGA, AGA, and LGA groups were made using One-way ANOVA. Multivariate linear regression models were used to estimate the influencing factors on vitamins A, D, and E in cord blood and birth weight after adjusting for confounders. Associations between fat-soluble vitamins and neonatal birth weight adjusted for confounders were evaluated by partial correlation analysis. The confounders considered were mode of delivery, GA, maternal age, pre-pregnancy BMI, and sex of the infants. A p-value <0.05 was considered statistically significant.
Table 1 shows baseline characteristics of mothers and birth outcomes. This study enrolled a total of 199 mother-infant pairs, including 63 in the SGA group, 87 in the AGA group and 49 in the LGA group. Statistically significant differences were found in maternal age (P=0.005), delivery mode (P<0.001), gestational age (P=0.005), birth weight (P<0.001), birth length (P<0.001), and weight gain (P<0.001) among the three groups. Women with LGA babies were less likely to deliver spontaneously, and have higher weight gain during pregnancy and prepregnancy BMI than SGA and AGA groups.
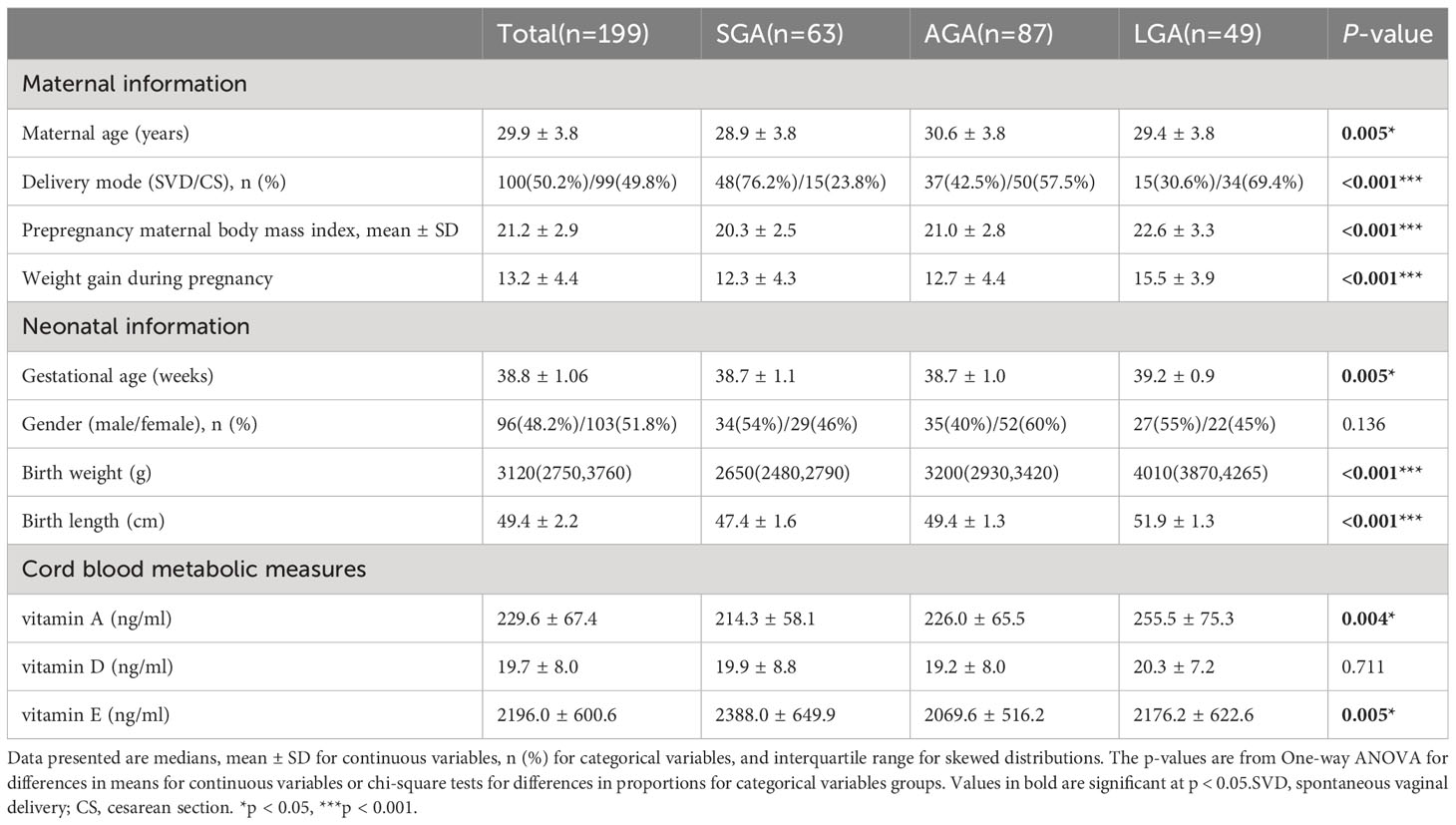
Table 1 Baseline characteristics of the mother–infant pairs in the three groups.
Statistically significant differences were found in cord blood vitamin A and E concentrations among the groups; No significant differences were observed in vitamin D. The concentrations of vitamin A in the SGA group were significantly lower than those in the AGA and LGA group; however, the concentrations of vitamin E in the SGA group were significantly higher than those in the AGA and LGA group (Table 1).
GA, spontaneous vaginal delivery (SVD), weight gain during pregnancy, pre-pregnancy BMI, Vitamin A, and Vitamin E were associated with birth weight. GA (β = 0.480, p<0.001), Pre-pregnancy BMI (β = 0.260, p<0.001), Weight gain during pregnancy (β = 0.248, p<0.001), Vitamin A (β = 0.146, p=0.009) and being SVD (β = 0.277, p<0.001) were positively correlated with the birth weight, while Vitamin E (β = −0.135, p = 0.015) negatively correlated with the birth weight (Table 2).
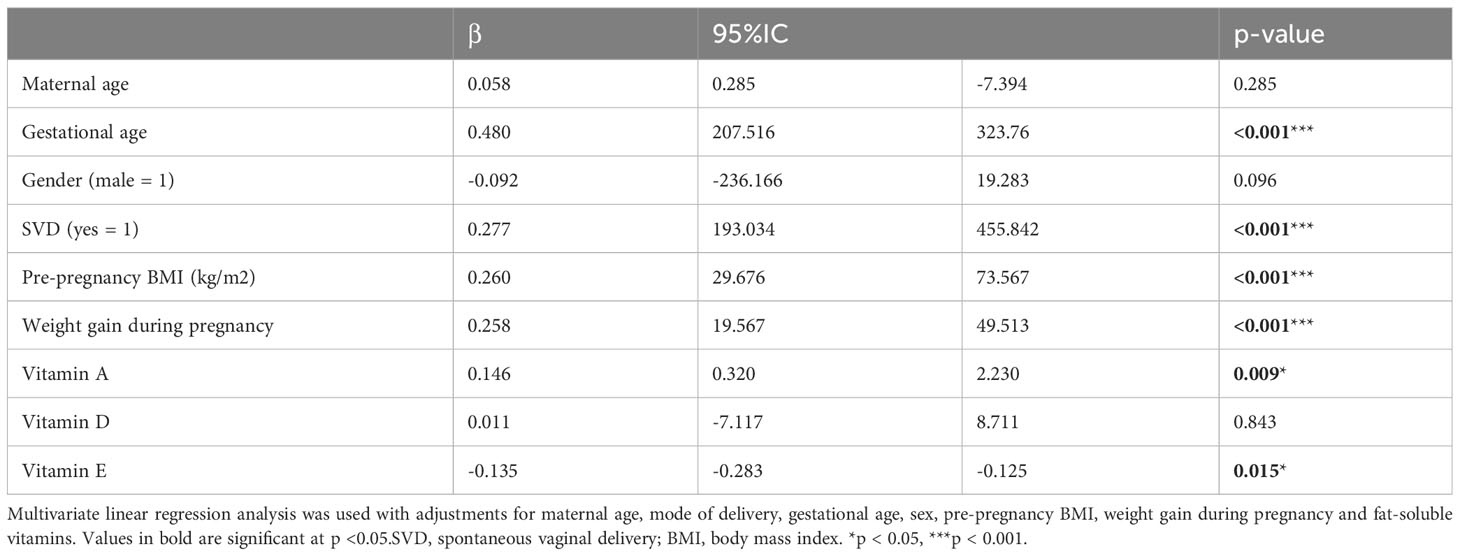
Table 2 Multivariate linear regression analysis of the influencing factors on birth weight.
Sex and birth weight were associated with the levels of vitamin A in umbilical cord blood. Being male (β = 0.317, p < 0.001) and birth weight (β = 0.229, p = 0.014) were positively correlated with the levels of vitamin A. Birth weight (β = -0.213, p= 0.026) was correlated with lower levels of vitamin E. No correlation was found between influencing Factors and the levels of vitamin D (p> 0.05) (Table 3).
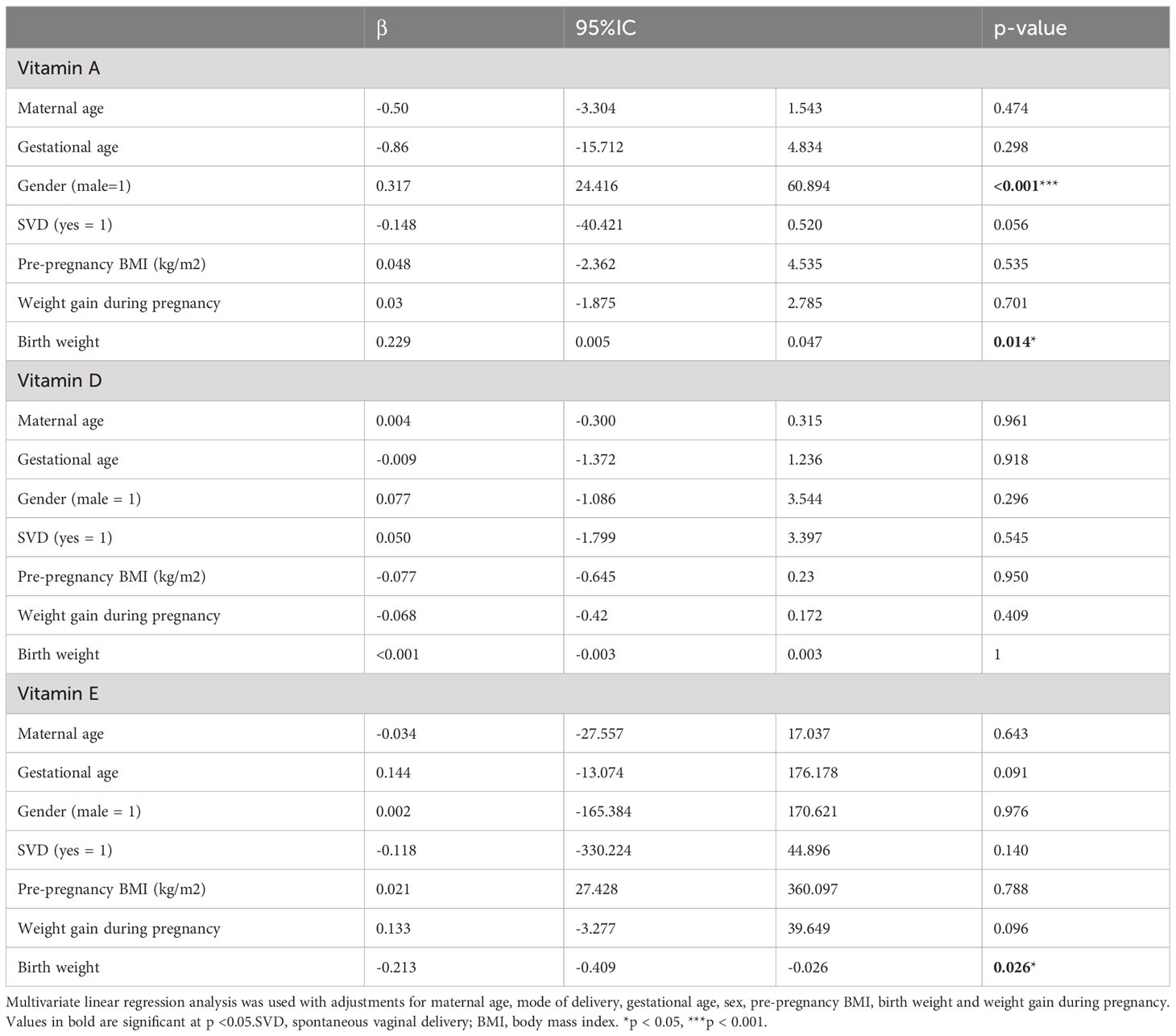
Table 3 Multivariate linear regression analysis of the influencing factors for the levels vitamin A, vitamin D, and vitamin E in cord blood.
The partial correlation coefficients between fat-soluble vitamins and newborn birth weight are shown in Table 4. After adjusting for delivery mode, GA, mother’s age, sex, pre-pregnancy BMI, pregnancy weight gain and other factors, the cord blood vitamin A level i was positively correlated with body weight (p=0.012). However, no statistically significant association was found between vitamin D or vitamin E level and birth weight.

Table 4 Relationship between the levels of vitamins A, D and E and infant birth weight.
Our study demonstrates the relationship between the levels of cord blood fat-soluble vitamins and the BW. We found that the cord blood vitamin A level was positively correlated with the infant BW, while the vitamin E level was negatively correlated with BW. When compared with those of AGA and LGA, the vitamin A level was substantially lower in SGA, whereas the vitamin E level was significantly higher. However, we found no significant association between cord blood vitamin D serum level with birth weight.
Vitamin A is critical to ensure proper embryonic development and is involved in several metabolic pathways (18). Observational studies have found that cord blood and maternal vitamin A levels were significantly correlated with birth weight and length (19–22). The largest study investigating untargeted metabolic profiles showed that cord blood vitamin A levels were associated with birthweight (23), after controlling for hereditary factors such as parental size. Indeed, the vitamin A supplementation study in Human Immunodeficiency Virus–Infected Women have indicated that maternal vitamin A supplementation increase birth weight and neonatal growth, and decreases anemia (24). In our study, we found that the cord blood vitamin A concentrations were associated with birth weight, which is consistent with previous research findings. This finding suggests that there might be a role of vitamin A in determining birth weight and underscores the importance of vitamin A nutrition in fetal growth. However, some studies have shown that maternal vitamin A concentrations were not associated with birth weight (10, 25). The reasons behind these discrepancies might be partly due to different study participants. In our study, the Mother–Infant Pairs were all healthy and born full term, therefore, the effects of premature birth, infection, and maternal disease on vitamin A were excluded.
Here, we also discovered that SGA infants exhibit lower concentrations of cord blood vitamin A compared to AGA infants. As some studies have found that umbilical cord blood vitamin A serum concentration is significantly correlated with maternal vitamin A status (21, 26), SGA infants may be born from vitamin A deficient mothers. Unfortunately, we did not measure serum vitamin A levels in pregnant mothers. We further observed that LGA infants had higher concentrations of cord blood vitamin A compared with AGA infants. As maternal nutritional status has a key role on fetal growth (27), this result suggested that maintaining a high concentration of vitamin A during pregnancy may not be good for fetal growth.
In this study, we found no significant association between cord blood vitamin D serum levels with birth weight, which does not agree with the findings of previous studies (11, 12, 28). A meta-analysis of observational studies has shown that vitamin D deficiency during pregnancy is associated with a higher risk of low birth weight (12). While a Brazilian cohort study found that higher concentrations of vitamin D during the first, second, and third trimesters increase the risk of preterm birth (28). A meta-analysis has suggested that vitamin D deficiency is associated with an increased risk of SGA (11). However, in our study, we found no association between cord blood vitamin D levels and SGA. Three limitations may have biased the result, particularly the fact that our study subjects were full-term infants, excluding preterm infants. The second limitation the plasma we tested came from cord blood, which does not signify the entire course of pregnancy. The third limitation was the relatively small sample size. In light of the conflicting data from studies, larger-sample studies are required to further confirm the effects of vitamin D on birth weight.
Vitamin E is a regulator of glucose and lipid metabolism and vitamin E deficiency causes metabolic dysregulation in the early stages of development. Therefore, cord blood vitamin E serum levels may influence infant birth weight. Several studies have demonstrated that vitamin E deficiency was found in VLBW infants (29, 30). While a Chinese observational study has indicated that vitamin E concentrations were positively related to increased fetal growth, and a positive association between vitamin E and macrosomia (15). In our study, we found that vitamin E was inversely related to birth weight. The results of this study indicate that the findings are different from what has been previously reported by other researchers. The possible influence factors were the different gestational ages of study participants and the source of the blood. And in another study, vitamin E concentrations were related to decreased risk of SGA births, and an increased risk of LGA (14). Here, we found that cord blood vitamin E concentrations were significantly higher in SGA than those in AGA and LGA. These findings suggest that vitamin E levels may affect on birth weight, but it is still controversial. Further studies are needed to investigate the relationship and mechanism between vitamin E and birth weight.
The strengths of this research include not only comparing the levels of fat-soluble vitamins in umbilical cord blood, but also dividing infants into subgroups based on their GA and BW. One limitation of the present study is the small number of participants from only one hospital in China, thus, it may not be sufficient in power to be generalizable. In the future, a large number of multicenter studies are needed.
In conclusion, this study found that a lower concentration of vitamin A in cord blood was associated with a higher risk of SGA and a lower risk of LGA. Additionally, excessive concentration of vitamin E in cord blood was found to be associated with SGA. Since the vitamin status of newborns is mostly dependent on that of their mothers, women are recommended to avoid having high concentrations of vitamin A and E during pregnancy. Nonetheless, further prospective studies are needed to explore these associations in different populations and to understand the mechanism linking vitamin A and E to infant birth weight.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the ethics committee of Chongqing Health Center for Women and Children. The patients/participants provided their written informed consent to participate in this study.
YZ and GY conceived the study. GY performed the data analysis and wrote the manuscript. HL contributed to manuscript preparation. NW and LS helped with data analysis. All the authors contributed to the manuscript and approved the submitted version.
This study was supported by the Chongqing medical scientific research project (Joint project of Chongqing Health Commission and Science and Technology Bureau) (2021MSXM211) and Maternal and infant nutrition and health research project(2021FY012).
We wish to thank the assistance provided by members of the Department of Children Healthcare and Neonatal Screening Center of Chongqing Health Center for Women and Children. We also thank all the mothers who provided samples.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
SGA, small for gestational age; LGA, large for gestational age; AGA, appropriate for gestational age group; LBW, low birth weight; GA, gestational age; CS, cesarean section; BMI, Body Mass Index; BW, Birth weight; SD, standard deviation.
1. Grantz KL, Hediger ML, Liu D, Buck Louis GM. Fetal growth standards: the NICHD fetal growth study approach in context with INTERGROWTH-21st and the World Health Organization Multicentre Growth Reference Study. Am J Obstet Gynecol (2018) 218(2S):S641–S655 e28. doi: 10.1016/j.ajog.2017.11.593
2. Hong YH, Chung S. Small for gestational age and obesity related comorbidities. Ann Pediatr Endocrinol Metab (2018) 23(1):4–8. doi: 10.6065/apem.2018.23.1.4
3. Hong YH, Lee JE. Large for gestational age and obesity-related comorbidities. J Obes Metab Syndr (2021) 30(2):124–31. doi: 10.7570/jomes20130
4. Blaner WS. Vitamin A signaling and homeostasis in obesity, diabetes, and metabolic disorders. Pharmacol Ther (2019) 197:153–78. doi: 10.1016/j.pharmthera.2019.01.006
5. Wimalawansa SJ. Associations of vitamin D with insulin resistance, obesity, type 2 diabetes, and metabolic syndrome. J Steroid Biochem Mol Biol (2018) 175:177–89. doi: 10.1016/j.jsbmb.2016.09.017
6. Sozen E, Demirel T, Ozer NK, Vitamin E. Regulatory role in the cardiovascular system. IUBMB Life (2019) 71(4):507–15. doi: 10.1002/iub.2020
7. He W, Xu Y, Ren X, Xiang D, Lei K, Zhang C, et al. Vitamin E ameliorates lipid metabolism in mice with nonalcoholic fatty liver disease via Nrf2/CES1 signaling pathway. Dig Dis Sci (2019) 64(11):3182–91. doi: 10.1007/s10620-019-05657-9
8. Naik VD, Lee J, Wu G, Washburn S, Ramadoss J. Effects of nutrition and gestational alcohol consumption on fetal growth and development. Nutr Rev (2022) 80(6):1568–79. doi: 10.1093/nutrit/nuab119
9. Adhikari KM, Somani BL, Kalra S, Mathai SS, Arora MM. Umbilical cord blood plasma vitamin A levels in low birth weight (LBW) babies. Med J Armed Forces India (2011) 67(2):142–6. doi: 10.1016/S0377-1237(11)60013-0
10. Tao E, Chen C, Chen Y, Cai L, Yuan T. The relationship between umbilical cord blood vitamin A levels and late preterm infant morbidities: a prospective cohort study. Eur J Pediatr (2021) 180(3):791–7. doi: 10.1007/s00431-020-03787-1
11. Chen Y, Zhu B, Wu X, Li S, Tao F. Association between maternal vitamin 297 D deficiency and small for gestational age: evidence from a meta-analysis of prospective cohort studies. 298 BMJ Open (2017) 7:e016404. doi: 10.1136/bmjopen-2017-016404
12. Fang K, He Y, Mu M, Liu K. Maternal vitamin D deficiency during pregnancy and low birth weight: a systematic review and meta-analysis. J Matern Fetal Neonatal Med (2021) 34(7):1167–73. doi: 10.1080/14767058.2019.1623780
13. Wierzejska R, Jarosz M, Kleminska-Nowak M, Tomaszewska M, Sawicki W, Bachanek M, et al. Maternal and cord blood vitamin D status and anthropometric measurements in term newborns at birth. Front Endocrinol (Lausanne) (2018) 9:9. doi: 10.3389/fendo.2018.00009
14. Scholl TO, Chen X, Sims M, Stein TP. Vitamin E: maternal concentrations are associated with fetal growth. Am J Clin Nutr (2006) 84(6):1442–8. doi: 10.1093/ajcn/84.6.1442
15. Yang W, Jiao M, Xi L, Han N, Luo S, Xu X, et al. The association between maternal fat-soluble vitamin concentrations during pregnancy and infant birth weight in China. Br J Nutr (2020) 125(9):1058–66. doi: 10.1017/S0007114520003347
16. Liu H, Wang DJ, Wan KX, Zhang J, Yuan ZJ, Yu CW, et al. Simultaneous quantification of fat-soluble vitamins A, 25-hydroxylvitamin D and vitamin E in plasma from children using liquid chromatography coupled to Orbitrap mass spectrometry. J Chromatogr B Analyt Technol BioMed Life Sci (2021) 1177:122795. doi: 10.1016/j.jchromb.2021.122795
17. P. Capital Institute of, G, Coordinating Study Group of Nine Cities on the Physical, C. Development of. [Growth standard curves of birth weight, length and head circumference of Chinese newborns of different gestation]. Zhonghua Er Ke Za Zhi (2020) 58(9):738–46. doi: 10.3760/cma.j.cn112140-20200316-00242
18. de Souza Mesquita LM, Mennitti LV, de Rosso VV, Pisani LP. The role of vitamin A and its pro-vitamin carotenoids in fetal and neonatal programming: gaps in knowledge and metabolic pathways. Nutr Rev (2021) 79(1):76–87. doi: 10.1093/nutrit/nuaa075
19. Mezzano J, Namirembe G, Ausman LM, Marino-Costello E, Shrestha R, Erhardt J, et al. Effects of iron and vitamin A levels on pregnant women and birth outcomes: complex relationships untangled using a birth cohort study in Uganda. Matern Child Health J (2022) 26(7):1516–28. doi: 10.1007/s10995-022-03387-5
20. Neves PAR, Castro MC, Oliveira CVR, Malta MB, Lourenco BH, Cardoso MA, et al. Effect of Vitamin A status during pregnancy on maternal anemia and newborn birth weight: results from a cohort study in the Western Brazilian Amazon. Eur J Nutr (2020) 59(1):45–56. doi: 10.1007/s00394-018-1880-1
21. Gazala E, Sarov B, Hershkovitz E, Edvardson S, Sklan D, Katz M, et al. Retinol concentration in maternal and cord serum: its relation to birth weight in healthy mother–infant pairs. Early Hum Dev (2003) 71(1):19–28. doi: 10.1016/S0378-3782(02)00096-8
22. Raksha S, Shah M, Rajalakshmi R. Vitamin A status of the newborn in relation to gestational age, body weight, and maternal nutritional status. Am J Clin Nutr (1984) 40:794–800. doi: 10.1093/ajcn/40.4.794
23. Robinson O, Keski-Rahkonen P, Chatzi L, Kogevinas M, Nawrot T, Pizzi C, et al. Cord blood metabolic signatures of birth weight: A population-based study. J Proteome Res (2018) 17(3):1235–47. doi: 10.1021/acs.jproteome.7b00846
24. Kumwenda N, Miotti PG, Taha TE, Broadhead R, Biggar RJ, Jackson JB. Antenatal vitamin A supplementation increases birth weight and decreases anemia among infants born to human immunodeficiency virus–infected women in Malawi. Clin Infect Dis (2002) 35:618–24. doi: 10.1086/342297
25. Christian P, Klemm R, Shamim AA, Ali H, Rashid M, Shaikh S, et al. Effects of vitamin A and beta-carotene supplementation on birth size and length of gestation in rural Bangladesh: a cluster-randomized trial. Am J Clin Nutr (2013) 97(1):188–94. doi: 10.3945/ajcn.112.042275
26. Bezerra DS, Ribeiro KDS, Lima MSR, Pires Medeiros JF, da Silva A, Dimenstein R, et al. Retinol status and associated factors in mother-newborn pairs. J Hum Nutr Diet (2020) 33(2):222–31. doi: 10.1111/jhn.12707
27. Moreno-Fernandez J, Ochoa JJ, Lopez-Frias M, Diaz-Castro J. Impact of early nutrition, physical activity and sleep on the fetal programming of disease in the pregnancy: A narrative review. Nutrients (2020) 12(12):1–18. doi: 10.3390/nu12123900
28. Benaim C, Carrilho TRB, Farias DR, Kac G. Vitamin D during pregnancy and its association with birth outcomes: a Brazilian cohort study. Eur J Clin Nutr (2021) 75(3):489–500. doi: 10.1038/s41430-020-00733-0
29. Kositamongkol S, Suthutvoravut U, Chongviriyaphan N, Feungpean B, Nuntnarumit P. Vitamin A and E status in very low birth weight infants. J Perinatol (2011) 31(7):471–6. doi: 10.1038/jp.2010.155
Keywords: vitamin A, vitamin D, vitamin E, fat-soluble vitamin, umbilical cord blood, birth weight
Citation: Yang G, wang N, Liu H, Si L and Zhao Y (2023) The association between umbilical cord blood fat-soluble vitamin concentrations and infant birth weight. Front. Endocrinol. 14:1048615. doi: 10.3389/fendo.2023.1048615
Received: 19 September 2022; Accepted: 04 September 2023;
Published: 21 September 2023.
Edited by:
Jeff M. P. Holly, University of Bristol, United KingdomReviewed by:
Ihsan Erol Özçil, American University of Cyprus, CyprusCopyright © 2023 Yang, wang, Liu, Si and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yan Zhao, MjkxNjQ5NzgxNUBxcS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.