
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 14 March 2023
Sec. Neuroendocrine Science
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1046690
This article is part of the Research TopicEarly Biomarkers in the Investigation of Peripheral and Central Diabetic NeuropathyView all 8 articles
 Zoltan Kender1,2*†
Zoltan Kender1,2*† Johann M. E. Jende3†
Johann M. E. Jende3† Felix T. Kurz3,4
Felix T. Kurz3,4 Dimitrios Tsilingiris1,2†Lukas Schimpfle1
Dimitrios Tsilingiris1,2†Lukas Schimpfle1 Alba Sulaj1,2†
Alba Sulaj1,2† Ekaterina von Rauchhaupt1,2
Ekaterina von Rauchhaupt1,2 Hannelore Bartl1Christoph Mooshage3Jens Göpfert5†
Hannelore Bartl1Christoph Mooshage3Jens Göpfert5† Peter Nawroth1,2,6†Stephan Herzig2,6,7
Peter Nawroth1,2,6†Stephan Herzig2,6,7 Julia Szendroedi1,2,6†
Julia Szendroedi1,2,6† Martin Bendszus3
Martin Bendszus3 Stefan Kopf1,2†
Stefan Kopf1,2†Background: Diabetic sensorimotor polyneuropathy (DSPN) is one of the most prevalent and poorly understood diabetic microvascular complications. Recent studies have found that fractional anisotropy (FA), a marker for microstructural nerve integrity, is a sensitive parameter for the structural and functional nerve damage in DSPN. The aim of this study was to investigate the significance of proximal sciatic nerve’s FA on different distal nerve fiber deficits of the upper and lower limbs and its correlation with the neuroaxonal biomarker, neurofilament light chain protein (NfL).
Materials and methods: Sixty-nine patients with type 2 diabetes (T2DM) and 30 healthy controls underwent detailed clinical and electrophysiological assessments, complete quantitative sensory testing (QST), and diffusion-weighted magnetic resonance neurography of the sciatic nerve. NfL was measured in the serum of healthy controls and patients with T2DM. Multivariate models were used to adjust for confounders of microvascular damage.
Results: Patients with DSPN showed a 17% lower sciatic microstructural integrity compared to healthy controls (p<0.001). FA correlated with tibial and peroneal motor nerve conduction velocity (NCV) (r=0.6; p<0.001 and r=0.6; p<0.001) and sural sensory NCV (r=0.50; p<0.001). Participants with reduced sciatic nerve´s FA showed a loss of function of mechanical and thermal sensation of upper (r=0.3; p<0.01 and r=0.3; p<0.01) and lower (r=0.5; p<0.001 and r=0.3; p=<0.01) limbs and reduced functional performance of upper limbs (Purdue Pegboard Test for dominant hand; r=0.4; p<0.001). Increased levels of NfL and urinary albumin-creatinine ratio (ACR) were associated with loss of sciatic nerve´s FA (r=-0.5; p<0.001 and r= -0.3, p= 0.001). Of note, there was no correlation between sciatic FA and neuropathic symptoms or pain.
Conclusion: This is the first study showing that microstructural nerve integrity is associated with damage of different nerve fiber types and a neuroaxonal biomarker in DSPN. Furthermore, these findings show that proximal nerve damage is related to distal nerve function even before clinical symptoms occur. The microstructure of the proximal sciatic nerve and is also associated with functional nerve fiber deficits of the upper and lower limbs, suggesting that diabetic neuropathy involves structural changes of peripheral nerves of upper limbs too.
Diabetic sensorimotor peripheral neuropathy (DSPN) affects more than half of patients with diabetes mellitus (DM) (1), resulting in increased morbidity and mortality, reduced quality of life and constitutes a considerable economic burden for health care systems (2, 3). In DSPN, structural and functional changes are observed in the whole spectrum of peripheral nervous system components including myelinated and unmyelinated nerve fibers. Even though preclinical and clinical studies have identified several underlying molecular mechanisms contributing to the pathophysiology of DSPN, the pathogenesis of DSPN remains to be elucidated (4, 5). Moreover, promising data from therapeutic applications in animal models have not yielded meaningful results in clinical trials. In addition, owing to the frequent lack of symptoms, the condition remains typically undiagnosed until later stages. Although DSPN typically predominantly affects the lower extremities, recent studies have shown that loss of sensorimotor functions of the upper limb are also frequent, but often remain underdiagnosed in patients with DM (6, 7). Contrary to the progression of clinical symptoms, previous studies on magnetic resonance neurography (MRN) showed predominantly proximally localized nerve damage in DSPN, but its relevance on different nerve fiber functions remained unclear (8–10). Validated diagnostic measures such as electrophysiological testing (EPT) and quantitative sensory testing (QST) can be used in the early detection of subclinical and asymptomatic DSPN (4, 11). These require a high degree of expertise, are time-consuming and expensive, and therefore are used mostly in the research setting. Notably, QST is considered to be a subjective method. Consequently, there is an obvious need for the establishment of objective and non-invasive methods or biomarkers that allow early detection of nerve fiber damage, to gain a better understanding of the underlying pathomechanisms and natural course of DSPN and evaluate new therapeutic options. Ideally, such methods should accurately and reproducibly detect DSPN and its progression.
Magnetic resonance neurography (MRN) can visualize and characterize peripheral nerve structures including internal fascicular patterns. Previous studies have shown that MRN is able to detect and localize peripheral nerve lesions (12, 13). Surprisingly, MRN studies revealed a proximal predominance of nerve lesions in DSPN (9). Diffusion tensor imaging (DTI) is a well-established method to measure microstructural integrity of peripheral and central nerve fibers used quantitative measures such as fractional anisotropy (FA) (14, 15). Recent studies have shown a good diagnostic accuracy of DTI for the detection of DSPN diagnosed by clinical symptoms and signs in patients with type 1 and type 2 diabetes (10, 16). In an experimental model, DTI was used to assess axonal regeneration after sciatic nerve crush (17). However, the relation of nerve fiber integrity assessed by DTI to the various nerve fiber functions of upper and lower extremities and axonal damage has not been evaluated. The prevalence of microstructural changes in patients with asymptomatic preclinical DSPN is yet unclear.
Currently, no blood-based or urine-based biomarkers for DSPN with diagnostic and predictive capacity are available for routine clinical use. Neurofilaments are neuronal proteins which levels increase in in blood and cerebrospinal fluid following axonal damage and as such, they constitute attractive candidate biomarkers in various neurodegenerative conditions (18, 19). Neurofilament light chain (NfL) is a cytoplasmatic protein with high expression in myelinated axons (20). Its role as a biomarker has been described in different neurodegenerative diseases, such as multiple sclerosis, Alzheimer disease and motoneuron diseases (19). Some preclinical and clinical studies showed an association of NfL and peripheral nerve diseases, especially in inflammatory and toxic nerve damage (21–24). One prior study showed associations between NfL and altered nerve function, especially hyperalgesia in patients with type 2 diabetes (T2DM) (25). However, the role of NfL in DSPN remained unclear.
The aim of this study was to investigate the association of extensively assessed nerve function parameters with the microstructure of the sciatic nerve as assessed from MRN (FA) and the neuroaxonal biomarker NfL in order to evaluate the role of proximal nerve damage in different nerve fiber functions and to better understand the pathophysiological background of nerve damage in DSPN. We hypothesized that the FA of sciatic nerve is associated with (i) a marker of axonal damage and (ii) loss of different nerve fiber functions of the upper and lower limb, (iii) even in patients with preclinical symptomatic DSPN.
Participants were assessed from outpatient facilities of Heidelberg University Hospital between June 2017 and August 2020. Patients with diabetes were diagnosed according to the guidelines of the German Diabetes Association (26). Healthy control subjects had to perform an oral glucose tolerance test. Overall exclusion criteria were age <18, type 1 diabetes, pregnancy, and any contraindications for MR imaging. Individuals with known neurological diseases or neuropathy-associated risk factors such as Parkinson’s disease, multiple sclerosis, lumbar surgery or disc extrusion, entrapment syndromes, alcohol abuse, hypovitaminosis, malignant or infectious diseases were excluded. All participants gave written informed consent. The study was is conducted according to the Declaration of Helsinki (2013), approved by the local ethics committee of the University of Heidelberg (local ethics number S-383/2016, clinicaltrials.gov identifier NCT03022721).
All participants underwent assessment of detailed medical history and anthropometric measurements. Blood was drawn and urine was taken under fasting conditions in the morning to measure HbA1c, lipid profile, albumin/creatinine ratio, and glomerular filtration rate (GFR). To estimate GFR the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula was used (27).
All participants underwent a routine clinical examination including the neuropathy deficit score (NDS) and neuropathy symptom score (NSS) (11, 28).
The fine motor functions of the hands and manual dexterity were tested using a Purdue Pegboard Test (Model 32020; Lafayette Instrument Co., Lafayette, Indiana USA), as previously described (6, 29).
The EPT using the Viking IV electromyography system (Nicolet, Middleton, Wisconsin, USA) of the right leg includes distal motor latencies of the tibial and peroneal nerve, compound motor and sensory action potentials (CMAPs and SNAPs, respectively) and nerve conduction velocities (NCV) of the tibial, peroneal and sural nerves; all tests were done by the same trained technician (30). Participants without recordable sural NCV and SNAP were assigned the lowest measured NVC, and a SNAP of 0. Additionally, EPT of the sensory and motor component on the median and ulnar nerves were performed in 6 control subjects and 38 patients with type 2 diabetes (31). Skin temperature was at least 32°C throughout the examination.
We defined DSPN according to following criteria:1) a score of ≥ 3 in NSS or NDS (a higher score was chosen); 2) Abnormal results of nerve conduction studies in at least two different nerves (28, 32, 33).
QST was performed on one foot and one hand according to the protocol of the German Research Network on Neuropathic Pain (DFNS), as previously published (34). Complete QST can determine neuropathic deficits and hyperalgesia with the following parameters: cold detection threshold (CDT); warm detection threshold (WDT); thermal sensory limen (TSL); cold pain threshold (CPT); heat pain threshold (HPT); pressure pain threshold (PPT); mechanical pain threshold (MPT); mechanical pain sensitivity (MPS); wind-up ratio (WUR); mechanical detection threshold (MDT); vibration detection threshold (VDT); dynamic mechanical allodynia (DMA); and paradoxical heat sensation (PHS) (11, 34). CDT, WDT, and TSL reflect thermal detection of small fibers (Aδ and C fibers), while CPT, HPT, PPT, and particularly MPS, and MPT represent nociceptive sensation of small fibers (Aδ and C fibers). MDT and VDT reflect tactile sensation (mechanical detection) of larger Aβ fibers (12).
MRN examinations were performed of the right tight using a 3-Tesla MR-scanner (Magnetom TIM-TRIO, Siemens Healthcare, Erlangen, Germany) with a 15-channel transmit-receive extremity coil in all participants, as previously described (8, 33). MRN sequences were centered in all participants on the sciatic nerve’s bifurcation to ensure that the anatomic region visualized by MRN was comparable in all participants. MRIs were acquired from the following sequences:
1) Axial high resolution T2-weighted turbo spin echo (TSE) 2D sequence with spectral fat saturation, and the following parameters: relaxation time (TR) = 5970 ms, echo time (TE) = 55ms, field of view (FOV) = 160 x 160 mm2, matrix size = 512 x 512, slice thickness = 4 mm, interslice gap = 0.79mm, voxel size = 0.3 x 0.3 x 4.0 mm3, 24 slices, 24 acquired images.
2) Axial fat-suppressed, diffusion-weighted 2-dimensional echo-planar sequence with the following parameters: TR = 5100 ms; TE=92.8 ms; b = 0 and 1000 s/mm2; directions = 20; field of view 160 x 160 mm2; matrix size 128 x 128; slice thickness 4 mm; voxel size 1.3 x 1.3 x 4 mm3; no interslice gap, 3 averages, 24 slices, 1512 acquired images.
Nordic BRAINEX software, a Food and Drug Administration (FDA) approved processing software was used to process and analyze images with automated calculation and reconstruction of nerve fiber tracts in DTI (35, 36).. We followed the DTI module instructions for Nordic BRANEX (Nordic Neuro Lab, Bergen, Norway). T2-weighted and diffusion weighted sequences were analyzed by two trained neuroradiologists with 7 and 8 years of experience in MRN imaging, respectively. Both were blinded to clinical and demographic patient data. Based on previous studies on DTI of the sciatic nerve, the nerve was automatically segmented with a threshold of > 0.1 for the nerve’s FA. The average FA was calculated automatically (36).
Serum blood samples were collected from all participants and centrifuged within 1 hour and stored at −80°C. NfL was measured within 4 years after collection of serum samples. For analysis of the concentration of NfL in serum samples a Simoa immunoassay (Quanterix, Billerica, MA, USA) was used, as previously described (25). For this study samples were analyzed in two independent assay runs on two different days using the same kit lots on a Simoa HD-X analyzer (Quanterix). Sample concentrations were calculated based on individual standard curves for each assay run using the Simoa HD-X Software (Version 3.1.2011.30002, Quanterix). The quality control (QC) samples provided by the kit manufacturer were included in both assay-runs and met the acceptance range specified with the kit. The inter-run coefficient of variation (CV) of the two levels of QCs was 6.4 and 11.9%.
Data sets of continuous variables were tested for normal distribution using the Kolmogorov-Smirnov test. Descriptive statistics are expressed as absolute numbers and percentages (n, %), means ± standard deviations or medians [25, 75 interquartile range] for categorical, normally, and non-normally distributed continuous data, respectively. One-way-ANOVA or the Kruskal-Wallis non-parametric test were used for comparisons across the three subgroups regarding normally and non-normally distributed continuous variables, respectively. In case of significant differences, post-hoc pairwise comparisons with Bonferroni correction were applied. was used to compare means of normally distributed variables, A chi-squared test was applied to compare categorical data. The Pearson correlation coefficient was used to examine the association of DTI (dependent variable) with factors pertinent to peripheral nerve function (independent variable). In order to ascertain the independence of observed correlations, multivariable linear regression models were used with inclusion of multiple potential confounders as covariates. The normality of regression residuals was tested through the Kolmogorov-Smirnov test and residual Q-Q plots and histograms was deemed adequate. For all tests the level of significance was defined at p<0.05. SPSS Version 23.0 (IBM-SPSS, Chicago, IL, USA) was used for statistics, and GraphPad Prism 7 for illustrating figures (GraphPad Software Inc. La Jolla, CA; USA).
The study cohort consisted of 99 participants, 30 with normal glucose tolerance, 40 with T2DM without DSPN and 29 with T2DM with DSPN. There were no differences in sex distribution, BMI, eGFR, and high-sensitive C-reactive protein levels. Patients with T2DM and DSPN were slightly older than healthy controls. Participants with T2DM were slightly older than controls (62.9 vs. 57.5 years, p=0.010), chiefly due to the difference between those with T2DM and DSPN versus healthy controls (63.7 vs. 57.5 years, p=0.038 in post-hoc comparison). There were no differences in age, sex, diabetes duration, statin use and established cardiovascular disease (CVD) between the subgroups of participants with T2DM with and without DSPN. As expected, participants with T2DM showed higher fasting plasma glucose, HbA1c and triglycerides compared to control subjects. Neuropathy scores were found to be highest among those with T2DM and DSPN compared to the other two groups and comparable between glucose tolerant controls and T2DM patients without DSPN (Table 1).
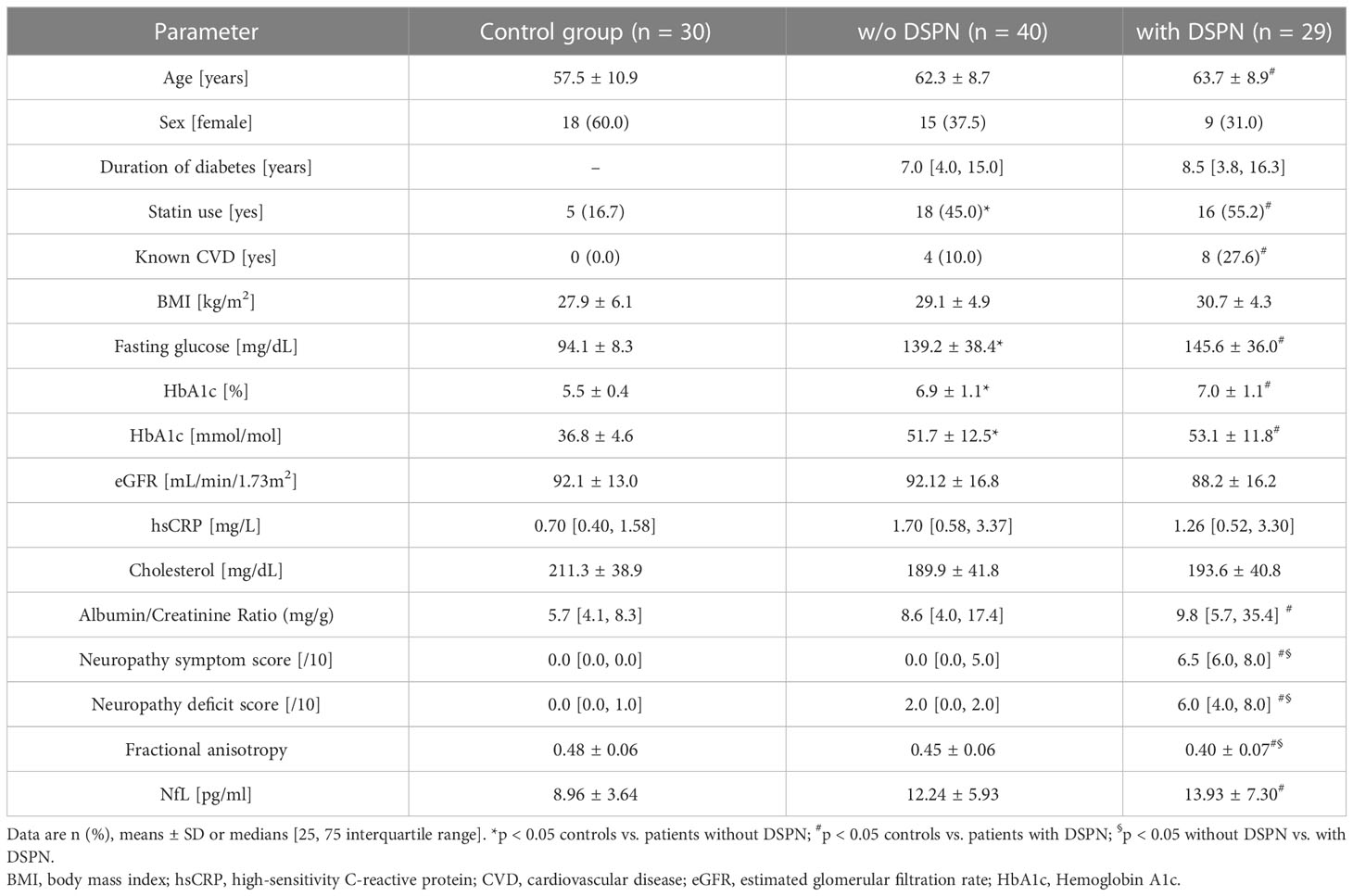
Table 1 Clinical characteristics of study participants.
The mean FA values were lower among those with T2DM and DSPN compared with the other two groups (0.40 vs. 0.48 and 0.45 for T2DM with DSPN vs. controls and T2DM without DSPN, respectively, p-ANOVA < 0.001 Figure 1). Mean NfL concentration gradually increased across healthy, T2DM without and with DSPN (8.96 vs. 12.24 vs. 13.93, respectively p-ANOVA= 0.008).
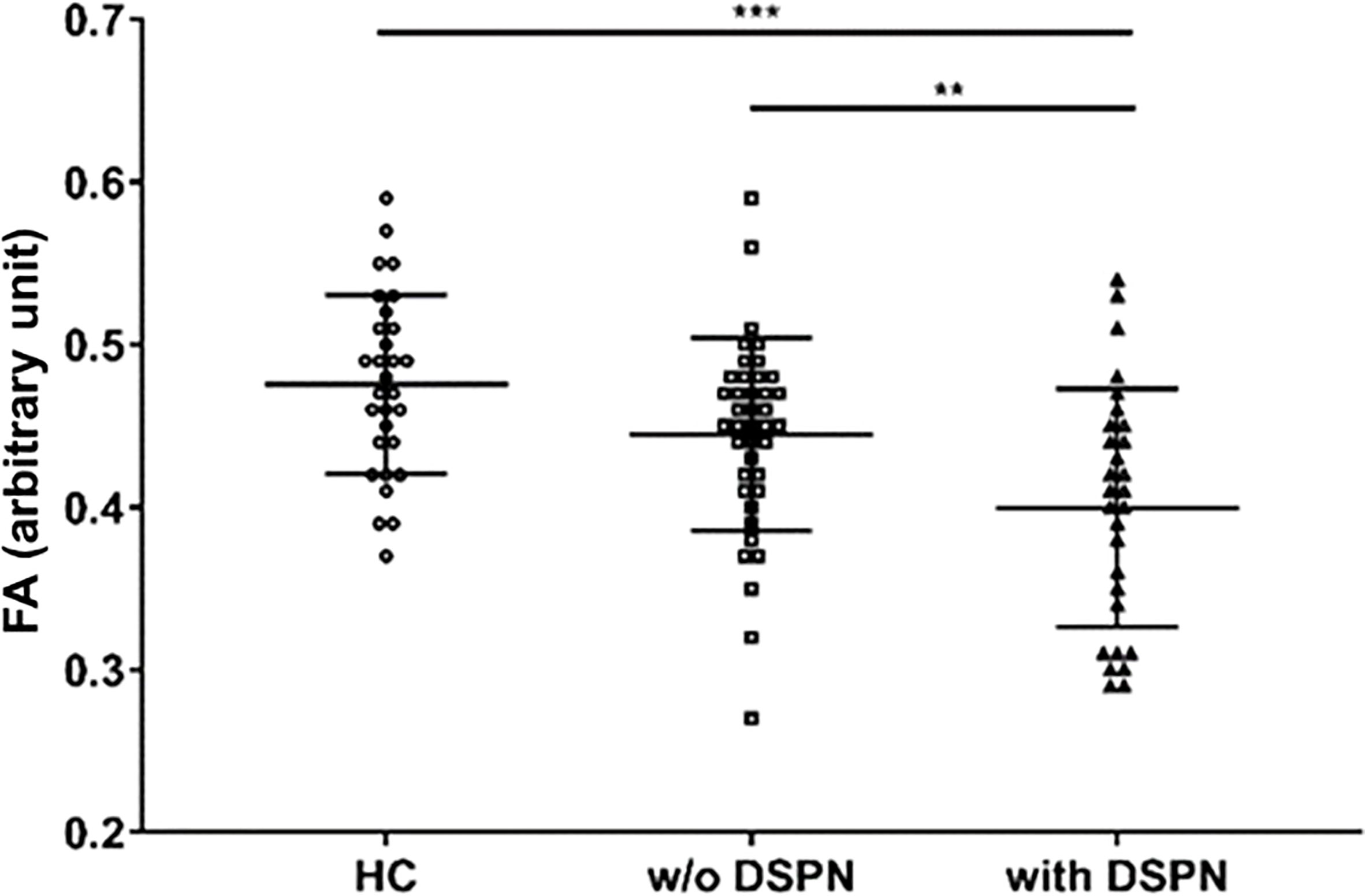
Figure 1 Quantification of sciatic nerve’s fractional anisotropy in control participants (n=30), participants with type 2 diabetes without DSPN (n=40), and participants with type 2 diabetes and DSPN (n=29). FA, fractional anisotropy; HC, healthy control; DSPN, Diabetic sensorimotor polyneuropathy. **p<0.01; ***p<0.001.
As a next step, the associations between the FA of the sciatic nerve and neuropathic deficits of the lower limbs were investigated. In total, the findings were suggestive of a robust association of FA values to an impaired peripheral sensory and motor nerve status (Table 2). In univariable analysis, FA showed negative correlations with clinical neuropathy scores (NSS and NDS, r= -0.517, p<0.001 and r=-0.034, p=0.001, respectively) as well as tibial and peroneal distal motor latencies, and positive with tibial and peroneal motor NCVs and amplitudes, as well as sural sensory NCVs and amplitudes(p<0.001 for all parameters). With the exception of neuropathy symptom score, these findings remained essentially unchanged in two multivariable regression models adjusted for various parameters which may have confounded the observed associations (model 1 adjusted for age, sex, body mass index (BMI) and waist–hip ratio (WHR), model 2 additionally for HbA1c, eGFR, total cholesterol, statin use and manifest CVD). Of note, no significant effects of HbA1c on the tested values were noted in the adjusted models (data not shown).
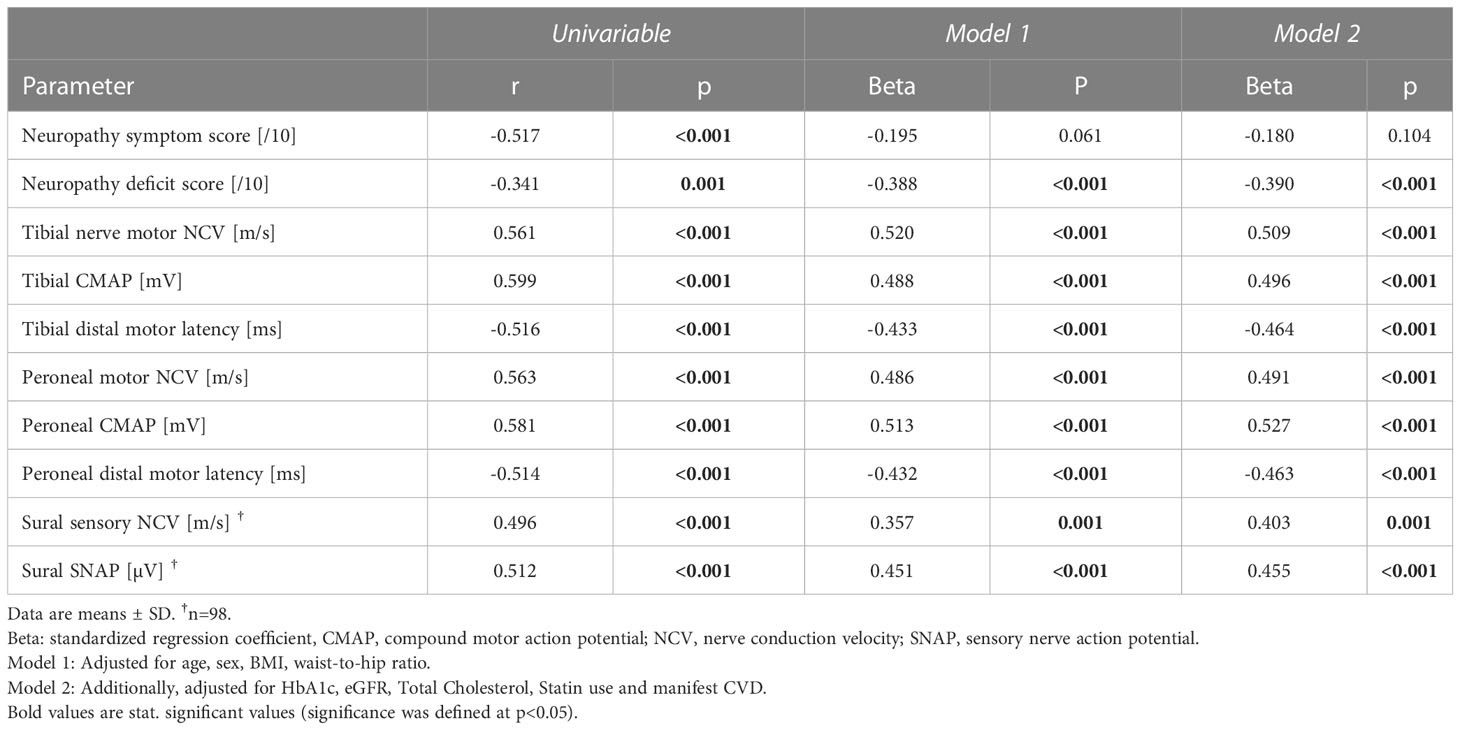
Table 2 Correlations of sciatic nerve´s FA (dependent variable) with appropriate clinical parameters and nerve conduction studies of the lower limb participants (independent variables) for all study participants.
Table 3 shows the associations of sciatic nerves’ FA with neuropathic deficits of the upper limb. Higher FA values were independently associated with increased sensory and motor NCV of the median (r= 0.545, p<0.001 and r=0.434, p=0.004) and ulnar nerves (r=0.431, p=0.003 and r=0.541, p<0.001) as well as CMAP of the ulnar nerve (r= 0.452, p=0.002) and SNAP of the median and ulnar nerves (r=0.516 and r= 0.522, p<0.001). Higher FA values were associated with higher fine motor dexterity in all four domains of the Purdue Pegboard Test in univariable analysis. In the adjusted models however, this correlation remained significant for the dominant hand only (p=0.01).
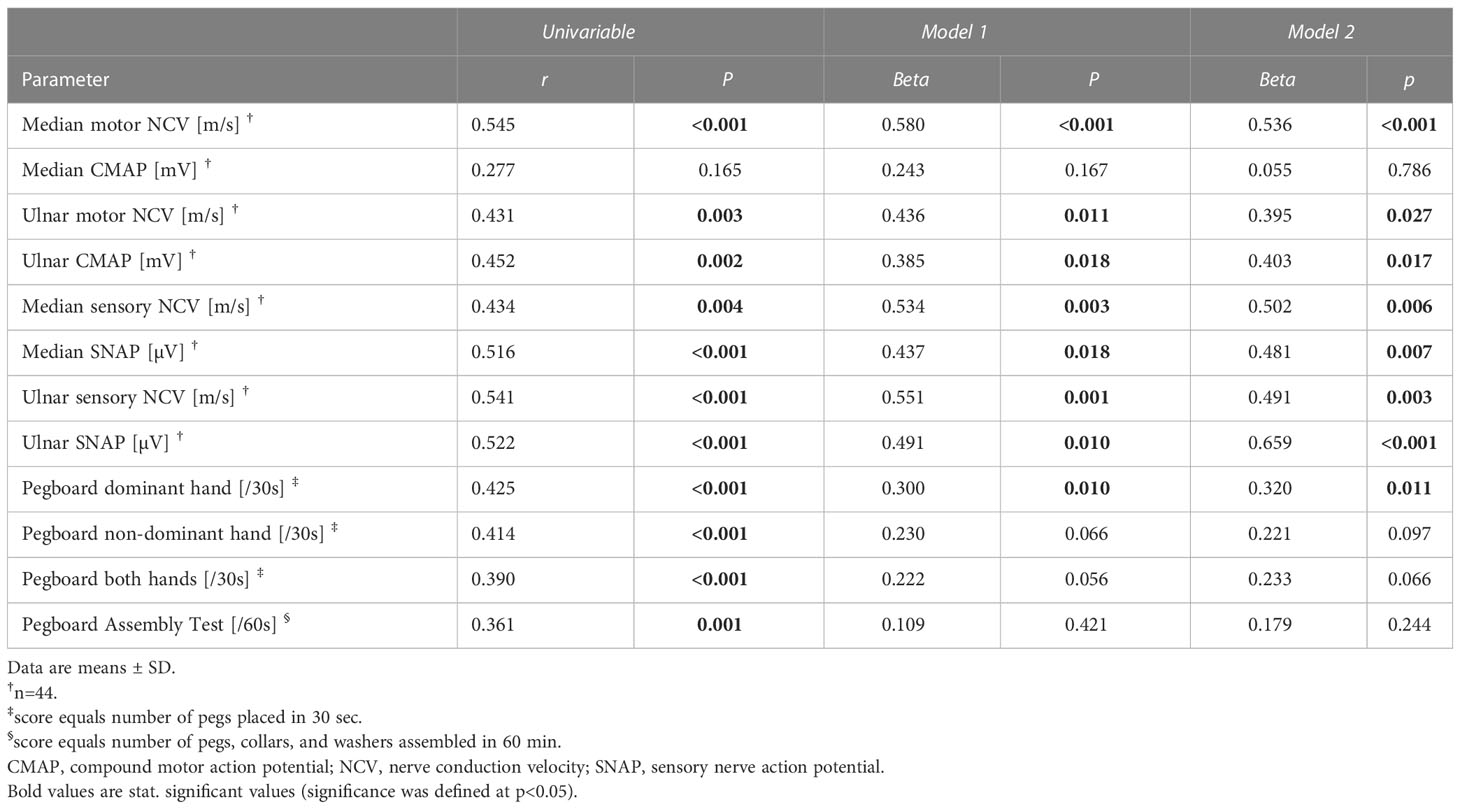
Table 3 Correlations of sciatic nerve´s FA (dependent variable) with nerve conduction studies and functional parameters of the upper limb participants (independent variables) for all study participants.
In the lower extremity, FA exhibited positive and independent associations most prominently with QST domains indicative of medium (mechanical pain threshold and mechanical pain sensitivity) and large (mechanical detection threshold and vibration detection threshold) fiber functional status. Regarding small fiber indices, a significant and independent association was noted with the cold pain threshold (r=0.301, p=0.004 in univariable analysis) (Table 4A). After grouping individual QST domains into compound scores on a functional basis, FA was shown to positively correlate with the compound z-scores of thermal and mechanical detections (r=0.26, p=0.008 and r=0.536, p<0.001) as well mechanical pain (r=0.379, p=0.001) on the feet measured by quantitative sensory testing (QST). In multivariable regression analysis, the associations with mechanical detection and pain remained constant, while the association with thermal detection was marginally non-significant (Table 4A).
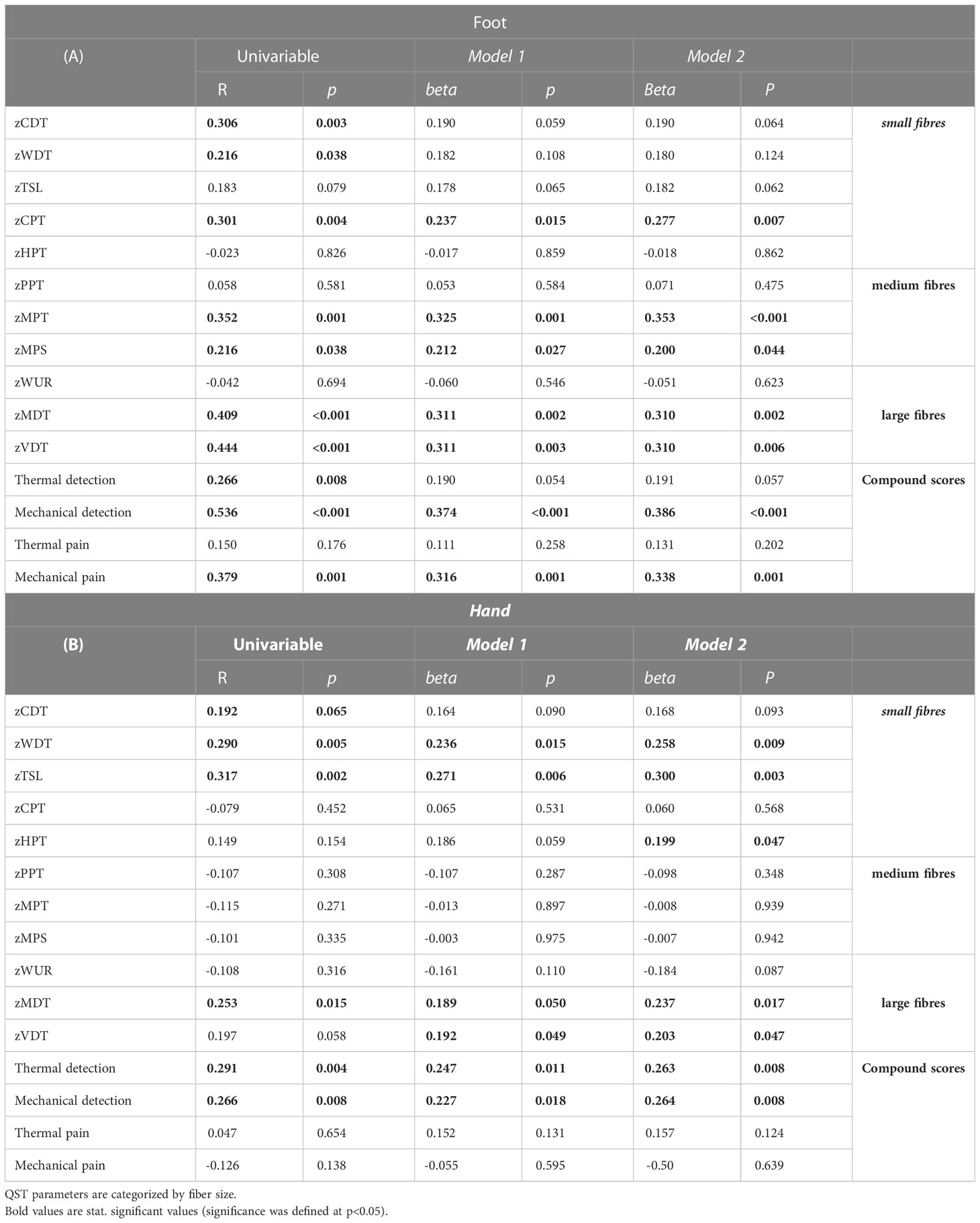
Table 4 Correlations of sciatic nerve´s FA (dependent variable) with z-scores of QST parameters and compound z-scores of the feet and hands in all participants (independent variables).
Regarding the hand sciatic FA showed positive associations with small (warm detection threshold and thermal sensory limen) and large fiber functions (mechanical detection threshold and vibration detection threshold). Likewise, there were independent positive correlations between FA and compound z-scores of thermal and mechanical detections of the hand (r=0.291, p=0.004 and r=0.266, p=0.008) (Table 4B).
In order to test the hypothesis that sciatic nerve FA values may reflect peripheral sensory axonal damage in the lower extremity, we investigated the association between FA and circulating levels of axonal biomarker NfL, using a similar modelling approach as above. There was a negative correlation between the two parameters, which remained unaffected in multivariable analysis (r=-0.244, p=0.003) (Figure 2A). Representative sciatic nerve fiber tracts from an individual with decreased FA and increased NfL and from a healthy individual with normal FA and NfL are depicted in Figures 2B, C.
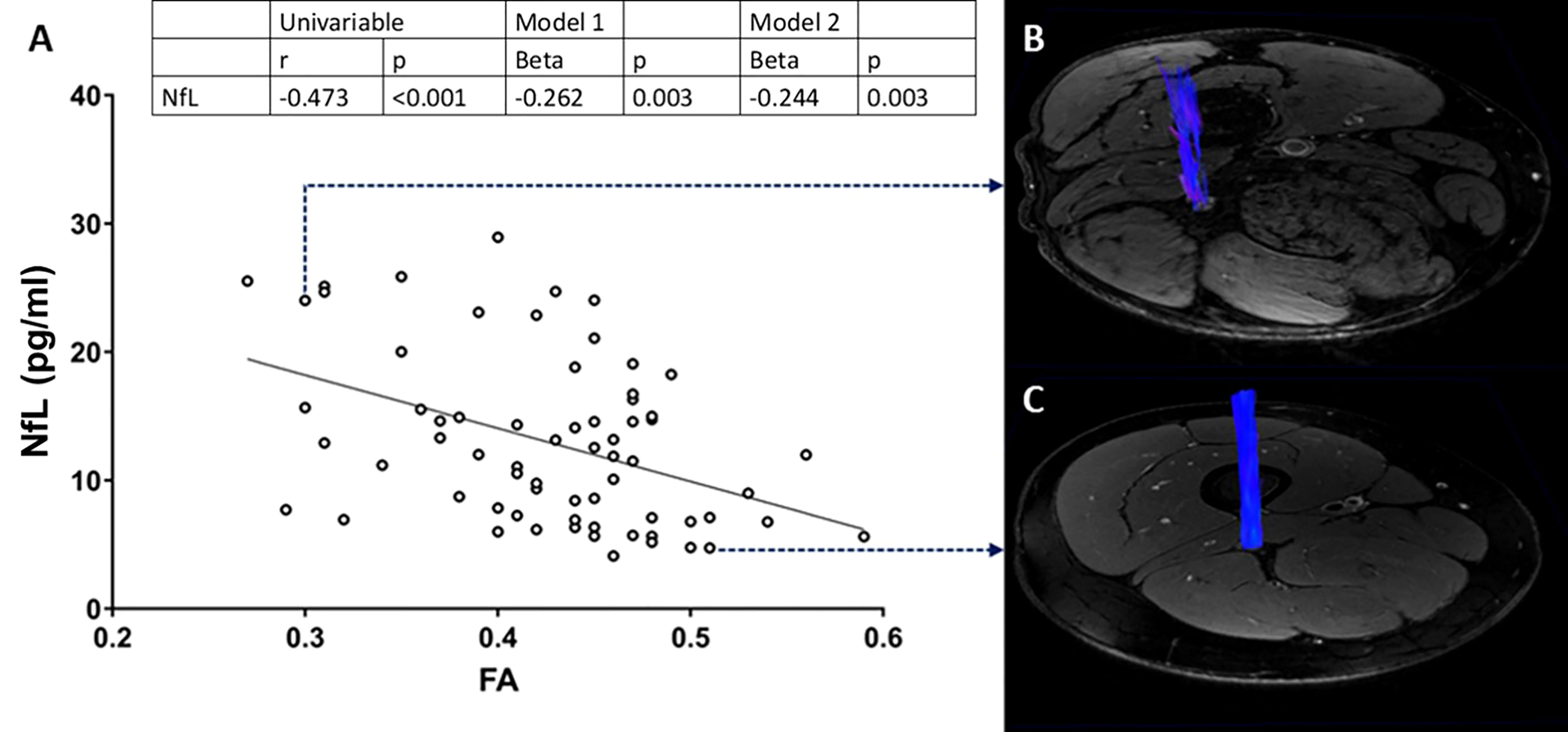
Figure 2 Correlation analysis of FA on the sciatic nerve with plasma NfL (A). Reconstructed, 3D fiber track of the right sciatic nerve of a patient with decreased FA and increased NfL (B), and a heathy control (C). FA, fractional anisotropy; NfL, neurofilament light chain protein.
As an additional step, the relationship between FA and albumin-to-creatinine ratio (ACR), a surrogate of microvascular damage, was examined. Due to its extremely skewed distribution the log-transformed ACR values were used in the analysis. There was a negative correlation between FA and log-transformed ACR (r=-0.347, p= 0.001), which remained unaffected in multivariable analysis (beta=-0.251, p=0.011, beta=-0.250 p=0.015 in models 1 and 2, respectively).
When both NfL and logACR, NDS and NSS were included as independent variables in a fully adjusted multivariable model (as in model 2 previously), NDS (beta= -0.300, p=0.018) and NfL (beta= -0.390, p=0.014) but not ACR were independent predictors of FA. The effects of other included variables were non-significant (Table 5).
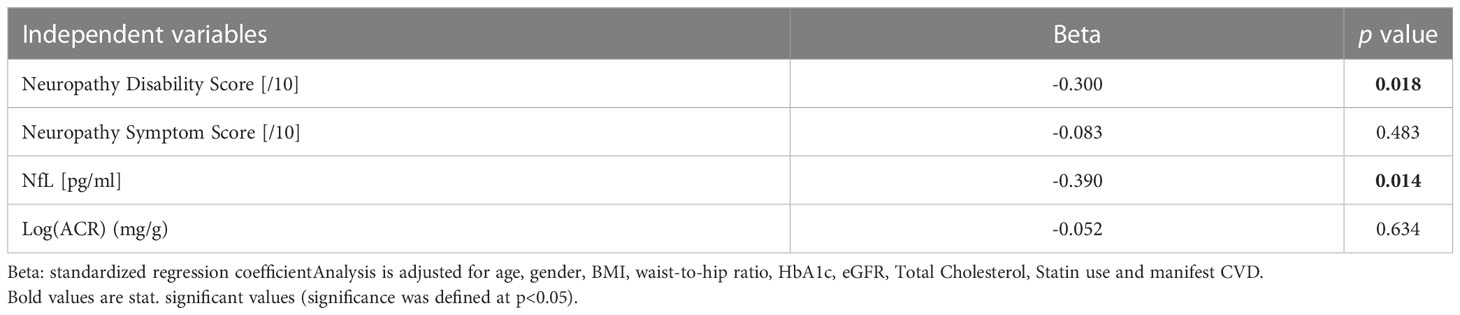
Table 5 Linear regression analysis for FA (dependent variable) of the sciatic nerve in all participants.
The results of this cross-sectional study in well characterized patients with T2DM showed associations between sciatic nerve integrity as assessed from FA measured by MRN based DTI and peripheral sensory as well as motor nerve status of upper and lower limbs. To our knowledge, this study is the first to demonstrate that sciatic nerve´s FA reflects sensory loss of small, medium, and large fibers even in early stages of DSPN. Since MRN itself cannot differentiate between different nerve fiber types, the ascertained associations with alterations in different fiber functions aid to a better understanding of peripheral nerve’s FA. In line with the initial hypothesis, we found an association between reduced nerve integrity and higher serum NfL, a biomarker of axonal damage. The observed associations were independent of age, sex and other covariables, and comprised asymptomatic patients with preclinical DSPN, strengthening the notion that changes in sciatic nerve´s microstructure play an important role in the development of DSPN.
Previous studies on magnetic resonance neurography in DSPN have focused on standard imaging protocols based on morphological sequences or T2-weighted sequences (9, 37). However, with a lack of microstructural specificity. DTI is a functional magnetic resonance imaging (MRI) technique, which can visualize microstructural changes in the central and peripheral nerve system at the anatomical level of nerve fascicles (38–40). FA reflects the directional orientation of water molecules within the nerve tissue and the anisotropy of peripheral nerves (40). Recent studies have demonstrated a reduction in FA for the sciatic and tibial nerves in patients with clinically overt DSPN (10, 16, 33, 41). These studies showed an association between FA and large and medium myelinated fiber dysfunction evident by nerve conduction studies (NCS). However, these studies have not detected small fiber functions. The most sensitive clinical method for the detection and characterization of peripheral nerve fiber functional deficits is complete quantitative sensory testing (QST), which includes the estimation of thermal and mechanical detection and pain thresholds (11, 34, 42). QST has not yet been used to evaluate the clinical relevance of FA. A recent study showed that T2-weighted lesions in the sciatic nerve may be associated with a decline in medium and large fiber functions in DSPN (12). To our knowledge, our study is the first to show that DTI can detect more widespread nerve fascicle lesions, including those affecting unmyelinated medium and small fibers, as evidenced by changes in individual sensation thresholds (Table 4). This is of clinical importance, since route tests like neuropathy scores and NCS cannot detect unmyelinated fiber functions which serve clinically relevant functions such as pain and the regulation of microvascular blood flow. In the current study we unraveled positive and independent associations between FA and mechanical detection and pain thresholds of the foot and thermal and mechanical detection thresholds of the hands. Notably, in multivariable analysis FA showed no association with neuropathic symptoms assessed by NSS. This finding is very important since it may demonstrate that proximal nerve damage is related to distal nerve function even before clinical symptoms appear.
The pathophysiological background of the lesions detected by MRN is yet unclear. Notably, electrophysiological testing showed strong associations of sciatic nerve´s FA with NCV, an indicator of myelin damage, and even more robust with SNAP, an indicator of axonal loss. While fiber loss is considered more prominent than myelin damage in DSPN (43), both types of nerve fiber damage have previously been described in DSPN (44). In models of injury of the centrals nervous system, decreased FA is associated with the degree of axon degeneration (45–47). Axonal injury is a severe complication of DSPN and can lead to loss of sensory and motor function of peripheral nerves. An independent association of sciatic nerve´s FA with serum NfL, a known biomarker of axonal damage, was also noted. These findings support the concept that structural nerve changes in DSPN visualized with DTI are causally related to injured microstructural integrity in DSPN caused in part by axonal damage (16, 48).
Furthermore, FA showed an independent negative association with ACR, a surrogate of microvascular disease in DM, but not with glycemia as indexed by HbA1c. Several studies have shown limited effect of glycemia on the course of DSPN, indicating that other risk factors such as microvascular damage may contribute to reduced nerve tissue integrity due to the degeneration of axons and Schwann cells in DSPN (49). A previous study on QST also showed an association between DSPN and albuminuria (11). However, this correlation in current study is modest, and in a fully adjusted multivariable model including NfL and NDS, ACR did not remain an independent predictor of nerve integrity. This supports the hypothesis that changes of FA might be more specific to the restriction of intra-axonal diffusion caused by injured microstructure and axonal damage, rather than being confounded by concomitant perturbations of systemic microvascular damage in DSPN.
To our knowledge this is the first study demonstrating that sciatic nerve integrity reflects a widespread sensorimotor loss including small fiber functions not only of the lower, but also of upper extremities. This may harbor implications regarding the natural course of nerve damage in DSPN. The finding that proximal microstructural damage of the sciatic nerve shows independent associations with indices of peripheral nerve fiber damage also of the upper limb suggests that in DSPN may be viewed as a systemic condition affecting the entire peripheral nervous system. This is in line with results from a previous study showing a substantial prevalence of upper limb neuropathy in patients with T2DM (6). A further implication would include FA of the sciatic nerve as a surrogate of peripheral nervous system status as a whole, in the frame of early preclinical stages of DSPN.
Our study is limited by its cross-sectional design, which precludes any definite conclusions on the predictive value of the sciatic nerve’s FA to be drawn. However, FA also related to nerve function deficits in asymptomatic patients with DSPN, suggesting a role of microstructural changes of proximal nerves in the pathophysiology of diabetic neuropathy. Another limitation is that only a subset of MRN patients underwent NCS of the upper limb. However, to date no data is available on the relation of sciatic FA with upper limbs nerve function in patients with and without DSPN. Furthermore, DTI metrics might be influenced by the technical setup, sequence specifications and the accuracy of the software. To date, differences between DTI techniques have been assessed only in few studies which showed comparable DTI measurements across different MR imaging platforms (50, 51). It should be also noted, that systematic errors during the automated reconstruction process may impact the FA values, however the algorithm used by BRAINEX is a widely used for DTI reconstruction (52). The present study has several strengths. We included a relatively high number of well characterized patients with and without DSPN. These subgroups are very similar regarding demographic and clinical profiles. We used not only electrophysiological testing, but a complete QST to assess all nerve fiber functions, including small fiber functions and hypersensitivity. The statistical analysis was adjusted carefully for several covariates in different models.
In summary, this study demonstrates that the sciatic nerve´s microstructure is related to Nfl, a marker of axonal damage and impaired function of different nerve fiber types in DSPN. In addition, these findings show that proximal nerve damage is related to distal nerve function even before clinical symptoms occur. The sciatic nerve´s microstructure is also associated with functional deficits of the upper and lower limbs, suggesting that upper and lower limbs are simultaneously affected by nerve damage in DSPN. Further longitudinal studies are needed to detect the predictive value of the sciatic nerve’s FA for the natural course of DSPN.
The datasets presented in this article are not readily available because they are subject to national data protection laws and restrictions imposed by the ethics committee to ensure the privacy of study participants. Datasets are available from the corresponding author upon reasonable request for research purpose after anonymization and approval by the local ethics committee. Requests to access the datasets should be directed to zoltan.kender@med.uni-heidelberg.de.
The studies involving human participants were reviewed and approved by Ethikkommission der medizinischen Fakultät Heidelberg. The patients/participants provided their written informed consent to participate in this study.
ZK: Conceptualization (lead); Data curation (equal); Formal analysis (lead); Investigation (equal); Methodology (equal); Visualization (lead); Project administration (equal); Writing-original draft (lead). JJ: Data curation (equal); Methodology (equal); Writing-review and editing (equal). FK: Data curation (equal); Methodology (equal); Writing-review and editing (equal). DT: Data curation (supporting); Investigation (equal); Formal analysis (equal), Writing-review and editing (equal). LS: Data curation (equal); Methodology (equal); Writing-review and editing (equal). AS: Data curation (supporting); Investigation (equal); Writing-review and editing (equal). ER: Data curation (equal); Methodology (equal); Writing-review and editing (equal). HB: Data curation (equal); Methodology (equal); Writing-review and editing (equal). CM: Data curation (equal); Methodology (equal); Writing-review and editing (equal). JG: Data curation (equal); Methodology (equal); Writing-review and editing (equal). PN: Conceptualization (equal); Data curation (equal); Formal analysis (equal); Funding acquisition (equal); Methodology (equal); Supervision (lead); Writing-review and editing (equal) SH: Data curation (supporting); Formal analysis (supporting); Writing-review and editing (equal). JS: Data curation (supporting); Formal analysis (supporting); Writing-review and editing (equal). MB: Data curation (supporting); Writing-review and editing (equal). SK: Conceptualization (equal); Data curation (equal); Formal analysis (equal); Funding acquisition (equal); Investigation (supporting); Methodology (equal); Project administration (lead); Resources (equal); Software (equal); Supervision (lead); Validation (equal); Visualization (equal); Writing-original draft (equal); Writing-review and editing (equal). All authors contributed to the article and approved the submitted version.
This study was supported by the Federal Ministry for Research (BMBF)/German Center for Diabetes Research (DZD e.V.) and by the German Research Foundation in the Collaborative Research Center 1158 and Collaborative Research Center 1118, and the International Foundation for Research in Paraplegia.
The authors would like to thank all participants for their voluntary contribution. For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme “Open Access Publikationskosten” as well as by Heidelberg University. Preliminary data of this study were presented as an abstract at the 58th Annual Meeting of the European Association for the Study of Diabetes in 2022.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, et al. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: the Rochester diabetic neuropathy study. Neurology (1993) 43(4):817–24. doi: 10.1212/WNL.43.4.817
2. Davies M, Brophy S, Williams R, Taylor A. The prevalence, severity, and impact of painful diabetic peripheral neuropathy in type 2 diabetes. Diabetes Care (2006) 29(7):1518–22. doi: 10.2337/dc05-2228
3. Mehra M, Merchant S, Gupta S, Potluri RC. Diabetic peripheral neuropathy: resource utilization and burden of illness. J Med Econ (2014) 17(9):637–45. doi: 10.3111/13696998.2014.928639
4. Pop-Busui R, Boulton AJ, Feldman EL, Bril V, Freeman R, Malik RA, et al. Diabetic neuropathy: A position statement by the American diabetes association. Diabetes Care (2017) 40(1):136–54. doi: 10.2337/dc16-2042
5. Sloan G, Selvarajah D, Tesfaye S. Pathogenesis, diagnosis and clinical management of diabetic sensorimotor peripheral neuropathy. Nat Rev Endocrinol (2021) 17(7):400–20. doi: 10.1038/s41574-021-00496-z
6. Kender Z, Groener JB, Jende JME, Kurz FT, Fleming T, Sulaj A, et al. Diabetic neuropathy is a generalized phenomenon with impact on hand functional performance and quality of life. Eur J Neurol (2022) 29(10):3081–91. doi: 10.1111/ene.15446
7. Yang CJ, Hsu HY, Lu CH, Chao YL, Chiu HY, Kuo LC. Do we underestimate influences of diabetic mononeuropathy or polyneuropathy on hand functional performance and life quality? J Diabetes Investig (2018) 9(1):179–85. doi: 10.1111/jdi.12649
8. Jende JME, Kender Z, Mooshage C, Groener JB, Alvarez-Ramos L, Kollmer J, et al. Diffusion tensor imaging of the sciatic nerve as a surrogate marker for nerve functionality of the upper and lower limb in patients with diabetes and prediabetes. Front Neurosci (2021) 15:642589. doi: 10.3389/fnins.2021.642589
9. Pham M, Oikonomou D, Hornung B, Weiler M, Heiland S, Baumer P, et al. Magnetic resonance neurography detects diabetic neuropathy early and with proximal predominance. Ann Neurol (2015) 78(6):939–48. doi: 10.1002/ana.24524
10. Vaeggemose M, Pham M, Ringgaard S, Tankisi H, Ejskjaer N, Heiland S, et al. Diffusion tensor imaging MR neurography for the detection of polyneuropathy in type 1 diabetes. J Magn Reson Imaging. (2017) 45(4):1125–34. doi: 10.1002/jmri.25415
11. Kopf S, Groener JB, Kender Z, Fleming T, Bischoff S, Jende J, et al. Deep phenotyping neuropathy: An underestimated complication in patients with pre-diabetes and type 2 diabetes associated with albuminuria. Diabetes Res Clin Pract (2018) 146:191–201. doi: 10.1016/j.diabres.2018.10.020
12. Groener JB, Jende JME, Kurz FT, Kender Z, Treede RD, Schuh-Hofer S, et al. Understanding diabetic neuropathy-from subclinical nerve lesions to severe nerve fiber deficits: A cross-sectional study in patients with type 2 diabetes and healthy control subjects. Diabetes (2020) 69(3):436–47. doi: 10.2337/db19-0197
13. Jende JME, Groener JB, Kender Z, Rother C, Hahn A, Hilgenfeld T, et al. Structural nerve remodeling at 3-T MR neurography differs between painful and painless diabetic polyneuropathy in type 1 or 2 diabetes. Radiology (2020) 294(2):405–14. doi: 10.1148/radiol.2019191347
14. Kronlage M, Schwehr V, Schwarz D, Godel T, Uhlmann L, Heiland S, et al. Peripheral nerve diffusion tensor imaging (DTI): normal values and demographic determinants in a cohort of 60 healthy individuals. Eur Radiol (2018) 28(5):1801–8. doi: 10.1007/s00330-017-5134-z
15. Preisner F, Baumer P, Wehrstein M, Friedmann-Bette B, Hackbusch M, Heiland S, et al. Peripheral nerve diffusion tensor imaging : Interreader and test-retest reliability as quantified by the standard error of measurement. Clin Neuroradiol (2020) 30(4):679–89. doi: 10.1007/s00062-019-00859-0
16. Vaeggemose M, Haakma W, Pham M, Ringgaard S, Tankisi H, Ejskjaer N, et al. Diffusion tensor imaging MR neurography detects polyneuropathy in type 2 diabetes. J Diabetes Complications. (2020) 34(2):107439. doi: 10.1016/j.jdiacomp.2019.107439
17. Lehmann HC, Zhang J, Mori S, Sheikh KA. Diffusion tensor imaging to assess axonal regeneration in peripheral nerves. Exp Neurol (2010) 223(1):238–44. doi: 10.1016/j.expneurol.2009.10.012
18. Gaetani L, Blennow K, Calabresi P, Di Filippo M, Parnetti L, Zetterberg H. Neurofilament light chain as a biomarker in neurological disorders. J Neurol Neurosurg Psychiatry (2019) 90(8):870–81. doi: 10.1136/jnnp-2018-320106
19. Olsson B, Portelius E, Cullen NC, Sandelius A, Zetterberg H, Andreasson U, et al. Association of cerebrospinal fluid neurofilament light protein levels with cognition in patients with dementia, motor neuron disease, and movement disorders. JAMA Neurol (2019) 76(3):318–25. doi: 10.1001/jamaneurol.2018.3746
20. Disanto G, Barro C, Benkert P, Naegelin Y, Schadelin S, Giardiello A, et al. Serum neurofilament light: A biomarker of neuronal damage in multiple sclerosis. Ann Neurol (2017) 81(6):857–70. doi: 10.1002/ana.24954
21. Bischof A, Manigold T, Barro C, Heijnen I, Berger CT, Derfuss T, et al. Serum neurofilament light chain: a biomarker of neuronal injury in vasculitic neuropathy. Ann Rheum Dis (2018) 77(7):1093–4. doi: 10.1136/annrheumdis-2017-212045
22. Fukami Y, Iijima M, Koike H, Yamada S, Hashizume A, Katsuno M. Association of serum neurofilament light chain levels with clinicopathology of chronic inflammatory demyelinating polyneuropathy, including NF155 reactive patients. J Neurol (2021) 268(10):3835–44. doi: 10.1007/s00415-021-10537-2
23. Huehnchen P, Schinke C, Bangemann N, Dordevic AD, Kern J, Maierhof SK, et al. Neurofilament proteins as a potential biomarker in chemotherapy-induced polyneuropathy. JCI Insight (2022) 7(6):e154395. doi: 10.1172/jci.insight.154395
24. Meregalli C, Fumagalli G, Alberti P, Canta A, Carozzi VA, Chiorazzi A, et al. Neurofilament light chain as disease biomarker in a rodent model of chemotherapy induced peripheral neuropathy. Exp Neurol (2018) 307:129–32. doi: 10.1016/j.expneurol.2018.06.005
25. Morgenstern J, Groener JB, Jende JME, Kurz FT, Strom A, Gopfert J, et al. Neuron-specific biomarkers predict hypo- and hyperalgesia in individuals with diabetic peripheral neuropathy. Diabetologia (2021) 64(12):2843–55. doi: 10.1007/s00125-021-05557-6
26. Schleicher E, Gerdes C, Petersmann A, Muller-Wieland D, Muller UA, Freckmann G, et al. Definition, classification and diagnosis of diabetes mellitus. Exp Clin Endocrinol Diabetes (2022) 130(S 01):S1–8. doi: 10.1055/a-1624-2897
27. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med (2009) 150(9):604–12. doi: 10.7326/0003-4819-150-9-200905050-00006
28. Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen PH. A multicentre study of the prevalence of diabetic peripheral neuropathy in the united kingdom hospital clinic population. Diabetologia (1993) 36(2):150–4. doi: 10.1007/BF00400697
29. Tiffin J, Asher EJ. The purdue pegboard; norms and studies of reliability and validity. J Appl Psychol (1948) 32(3):234–47. doi: 10.1037/h0061266
30. Gibbons CH, Freeman R, Veves A. Diabetic neuropathy: a cross-sectional study of the relationships among tests of neurophysiology. Diabetes Care (2010) 33(12):2629–34. doi: 10.2337/dc10-0763
31. Gazioglu S, Boz C, Cakmak VA. Electrodiagnosis of carpal tunnel syndrome in patients with diabetic polyneuropathy. Clin Neurophysiol (2011) 122(7):1463–9. doi: 10.1016/j.clinph.2010.11.021
32. Dyck PJ, Albers JW, Andersen H, Arezzo JC, Biessels GJ, Bril V, et al. Diabetic polyneuropathies: update on research definition, diagnostic criteria and estimation of severity. Diabetes Metab Res Rev (2011) 27(7):620–8. doi: 10.1002/dmrr.1226
33. Jende JME, Groener JB, Kender Z, Hahn A, Morgenstern J, Heiland S, et al. Troponin T parallels structural nerve damage in type 2 diabetes: A cross-sectional study using magnetic resonance neurography. Diabetes (2020) 69(4):713–23. doi: 10.2337/db19-1094
34. Rolke R, Baron R, Maier C, Tolle TR, Treede RD, Beyer A, et al. Quantitative sensory testing in the German research network on neuropathic pain (DFNS): standardized protocol and reference values. Pain (2006) 123(3):231–43. doi: 10.1016/j.pain.2006.01.041
35. O'Donnell LJ, Suter Y, Rigolo L, Kahali P, Zhang F, Norton I, et al. Automated white matter fiber tract identification in patients with brain tumors. NeuroImage Clin (2017) 13:138–53. doi: 10.1016/j.nicl.2016.11.023
36. Christidi F, Karavasilis E, Samiotis K, Bisdas S, Papanikolaou N. Fiber tracking: A qualitative and quantitative comparison between four different software tools on the reconstruction of major white matter tracts. Eur J Radiol Open (2016) 3:153–61. doi: 10.1016/j.ejro.2016.06.002
37. Jende JME, Groener JB, Oikonomou D, Heiland S, Kopf S, Pham M, et al. Diabetic neuropathy differs between type 1 and type 2 diabetes: Insights from magnetic resonance neurography. Ann Neurol (2018) 83(3):588–98. doi: 10.1002/ana.25182
38. Fox RJ, Cronin T, Lin J, Wang X, Sakaie K, Ontaneda D, et al. Measuring myelin repair and axonal loss with diffusion tensor imaging. AJNR Am J Neuroradiol (2011) 32(1):85–91. doi: 10.3174/ajnr.A2238
39. Kim B, Srinivasan A, Sabb B, Feldman EL, Pop-Busui R. Diffusion tensor imaging of the sural nerve in normal controls. Clin Imaging. (2014) 38(5):648–54. doi: 10.1016/j.clinimag.2014.04.008
40. Baumer P, Pham M, Ruetters M, Heiland S, Heckel A, Radbruch A, et al. Peripheral neuropathy: detection with diffusion-tensor imaging. Radiology (2014) 273(1):185–93. doi: 10.1148/radiol.14132837
41. Vaeggemose M, Pham M, Ringgaard S, Tankisi H, Ejskjaer N, Heiland S, et al. Magnetic resonance neurography visualizes abnormalities in sciatic and tibial nerves in patients with type 1 diabetes and neuropathy. Diabetes (2017) 66(7):1779–88. doi: 10.2337/db16-1049
42. Maier C, Baron R, Tolle TR, Binder A, Birbaumer N, Birklein F, et al. Quantitative sensory testing in the German research network on neuropathic pain (DFNS): somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Pain (2010) 150(3):439–50. doi: 10.1016/j.pain.2010.05.002
43. Dyck PJ, Lais A, Karnes JL, O'Brien P, Rizza R. Fiber loss is primary and multifocal in sural nerves in diabetic polyneuropathy. Ann Neurol (1986) 19(5):425–39. doi: 10.1002/ana.410190503
44. Pasnoor M, Dimachkie MM, Kluding P, Barohn RJ. Diabetic neuropathy part 1: overview and symmetric phenotypes. Neurol Clin (2013) 31(2):425–45. doi: 10.1016/j.ncl.2013.02.004
45. Kim JH, Loy DN, Liang HF, Trinkaus K, Schmidt RE, Song SK. Noninvasive diffusion tensor imaging of evolving white matter pathology in a mouse model of acute spinal cord injury. Magn Reson Med (2007) 58(2):253–60. doi: 10.1002/mrm.21316
46. Sun SW, Liang HF, Schmidt RE, Cross AH, Song SK. Selective vulnerability of cerebral white matter in a murine model of multiple sclerosis detected using diffusion tensor imaging. Neurobiol Dis (2007) 28(1):30–8. doi: 10.1016/j.nbd.2007.06.011
47. Song SK, Sun SW, Ju WK, Lin SJ, Cross AH, Neufeld AH. Diffusion tensor imaging detects and differentiates axon and myelin degeneration in mouse optic nerve after retinal ischemia. Neuroimage (2003) 20(3):1714–22. doi: 10.1016/j.neuroimage.2003.07.005
48. Breckwoldt MO, Stock C, Xia A, Heckel A, Bendszus M, Pham M, et al. Diffusion tensor imaging adds diagnostic accuracy in magnetic resonance neurography. Invest Radiol (2015) 50(8):498–504. doi: 10.1097/RLI.0000000000000156
49. Callaghan BC, Little AA, Feldman EL, Hughes RA. Enhanced glucose control for preventing and treating diabetic neuropathy. Cochrane Database Syst Rev (2012) 6(6):CD007543. doi: 10.1002/14651858.CD007543.pub2
50. Fox RJ, Sakaie K, Lee JC, Debbins JP, Liu Y, Arnold DL, et al. A validation study of multicenter diffusion tensor imaging: reliability of fractional anisotropy and diffusivity values. AJNR Am J Neuroradiol (2012) 33(4):695–700. doi: 10.3174/ajnr.A2844
51. Manoliu A, Ho M, Nanz D, Piccirelli M, Dappa E, Klarhofer M, et al. Diffusion tensor imaging of lumbar nerve roots: Comparison between fast readout-segmented and selective-excitation acquisitions. Invest Radiol (2016) 51(8):499–504. doi: 10.1097/RLI.0000000000000260
Keywords: magnetic resonance neurography, diffusion tensor imaging, fractional anisotropy, diabetic neuropathy, quantitative sensory testing, neurofilament light chain protein
Citation: Kender Z, Jende JME, Kurz FT, Tsilingiris D, Schimpfle L, Sulaj A, von Rauchhaupt E, Bartl H, Mooshage C, Göpfert J, Nawroth P, Herzig S, Szendroedi J, Bendszus M and Kopf S (2023) Sciatic nerve fractional anisotropy and neurofilament light chain protein are related to sensorimotor deficit of the upper and lower limbs in patients with type 2 diabetes. Front. Endocrinol. 14:1046690. doi: 10.3389/fendo.2023.1046690
Received: 16 September 2022; Accepted: 06 February 2023;
Published: 14 March 2023.
Edited by:
Solomon Tesfaye, Sheffield Teaching Hospitals NHS Foundation Trust, United KingdomReviewed by:
Uazman Alam, University of Liverpool, United KingdomCopyright © 2023 Kender, Jende, Kurz, Tsilingiris, Schimpfle, Sulaj, von Rauchhaupt, Bartl, Mooshage, Göpfert, Nawroth, Herzig, Szendroedi, Bendszus and Kopf. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zoltan Kender, em9sdGFuLmtlbmRlckBtZWQudW5pLWhlaWRlbGJlcmcuZGU=
†ORCID: Zoltan Kender, orcid.org/0000-0003-0745-1587
Dimitrios Tsilingiris, orcid.org/0000-0002-6864-4289
Johann M. E. Jende, orcid.org/0000-0002-1387-9304
Alba Sulaj, orcid.org/0000-0002-6051-6696
Jens Göpfert, orcid.org/0000-0003-3525-3684
Peter Nawroth, orcid.org/0000-0002-6134-7804
Julia Szendroedi, orcid.org/0000-0002-5185-8168
Stefan Kopf, orcid.org/0000-0002-6455-3769
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.