 Kento Ikegawa
Kento Ikegawa Yukihiro Hasegawa
Yukihiro Hasegawa
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol. , 17 October 2022
Sec. Pediatric Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.967857
This article is part of the Research Topic Update on Hypogonadism in Turner Syndrome View all 7 articles
Turner syndrome (TS), the most common type of X chromosomal disorder, has various, clinical manifestations. Among these, primary hypogonadism, which may lead to osteoporosis, is a life-long health issue. A high prevalence of fractures associated with osteoporosis is a major problem in patients with TS, where it may be 1.4-2.2 times higher than in healthy individuals and increases with age.
Among the risk factors associated with fractures in TS, hypogonadism is arguably the most important. Estrogen deficiency due to hypogonadism leads to low bone mineral density (BMD), resulting in a high prevalence of bone fractures. Estrogen replacement therapy (ERT) in patients with TS reportedly improved their BMD. However, other causes of low BMD may exist, given that this condition begins in the prepubertal period in patients with TS.
Most previous studies have reported low BMD in patients with TS using dual-energy X-ray absorptiometry (DXA), but this method has some limitations. Areal BMD values assessed by DXA were influenced by bone size and short stature, resulting in an underestimation of BMD. Currently, volumetric BMD values may be accurately obtained using peripheral quantitative computed tomography (pQCT). pQCT, high-resolution pQCT, and the trabecular bone score can also be used to evaluate bone quality, including bone geometry and microarchitecture, in TS.
The present review discusses the high fracture risk, role of estrogen deficiency in low BMD, advantages and disadvantages of various bone assessment methods, and characteristics of bone quality in TS.
Turner syndrome (TS) is a congenital disorder resulting from partial or complete loss of one X-chromosome and has a prevalence of approximately one in 2000 live births (1). Patients with TS have various symptoms, such as short stature, hypogonadism, cardiac malformation, and fractures, although their clinical phenotype varies depending on their karyotype (1, 2). A high fracture risk is especially problematic for patients with TS because the prevalence of fractures can be as high as 30.5-32.2% (3–5).
Numerous, previous studies and reviews have reported the characteristics of fractures in TS (2, 3, 6), which are caused by estrogen deficiency, a high risk of falling, X chromosomal abnormalities, and comorbidities of TS (6, 7). In particular low bone mineral density (BMD) stemming from estrogen deficiency is associated with an increased risk of fractures. BMD was higher in patients with TS with a spontaneous menstrual cycle than in those with primary hypogonadism (8–12). Indeed, estrogen replacement therapy (ERT) has been found to improve BMD in TS (13).
Dual-energy X-ray absorptiometry (DXA) is often used to assess BMD in TS but it is crucial to understand its limitations. Areal BMD (aBMD) values obtained using DXA are influenced by bone size and short stature, resulting in an underestimation of BMD (14, 15). This limitation of DXA has implications for patients with TS, most of whom have short stature. In recent years, quantitative computed tomography (QCT) has come to be used more often to assess volumetric BMD (vBMD) (16–19).
Bone quality, including bone geometry and microarchitecture, contribute to increasing or decreasing the risk of fractures independently of BMD (20). Bone quality in TS is currently evaluated using peripheral QCT (pQCT), high-resolution pQCT (HR-pQCT), and the trabecular bone score (TBS).
The present review aims to summarize the high fracture risk, role of estrogen deficiency in low BMD, advantages and disadvantages of various bone assessment methods, and characteristics of bone quality while focusing on TS.
Patients with Turner syndrome (TS) have a 30.5-32.2% prevalence of fractures (3–5). Population databases show that the risk of fractures is 1.4-2.2 times higher in patients with TS than in healthy individuals (21, 22). The high fracture risk in these patients has its onset in childhood (21, 23) and increases with age (24, 25). The odds ratio (OR) of the fracture rate between patients with TS and healthy subjects was 1.99 for those younger than age 45 years and 19.26 for those older than 45 years (24). In general, the occurrence of a fracture depends on bone strength and the frequency, type and severity of trauma. Bone strength is determined by bone density and bone quality, including the microarchitecture of cortical and trabecular bone and bone geometry (26). All these factors may contribute to increasing the risk of fractures in patients with TS.
While numerous, previous studies have demonstrated a high fracture risk in patients with TS, some have denied any significant difference from the fracture risk in the general population. Ross et al. compared past fractures in 78 patients with TS aged 4-13 years with the annual fracture rate in healthy children and reported that the total, annual fracture rate did not differ significantly between these groups (27). Another report demonstrated that the total fracture rate in 267 adult patients with TS (30.5%) did not differ significantly from the epidemiological data showing a rate of 32-44% (4). These reports were possibly biased because the data on the fracture rate in patients with TS and healthy controls were collected in different regions and at different times. The impact of the role of ERT on fractures is not entirely clear although its impact on BMD has been studied.
A major contributor to fractures in TS is the loss of bone density associated with estrogen deficiency. Estrogen suppresses osteoclasts, and estrogen deficiency weakens this suppression, resulting in osteoclast activation and loss of BMD (28). Estrogen deficiency also contributes to decreased intestinal calcium absorption and increased urinary calcium loss, which occurs when parathyroid hormone secretion decreases in response to elevated serum calcium resulting from bone resorption (29).
Elevated follicle-stimulating hormone (FSH) is also associated with decreased BMD in TS patients (6). FSH decreases bone density by directly binding to FSH receptors on osteoclasts and indirectly by promoting the production of TNF-α, which in turn promotes the production of osteoclasts (30, 31). Sun et al. demonstrated that neither FSHβ nor FSH receptor null mice had decreased BMD despite having severe hypogonadism (30). Furthermore, they demonstrated that BMD increased in haploinsufficient FSHβ+ mice with normal ovarian function, suggesting that FSH directly affects bone loss (30). Many patients with TS have a high FSH level from the neonatal period or early childhood (32), and it is possible that a high FSH level is related in some way to decreased BMD.
Bone fragility in TS is caused not only by decreased BMD but also decreased bone quality, including changes in bone geometry and microarchitecture. An increase in the total bone area, low cortical bone thickness in the radius, and small vertebrae and femurs have been reported in patients with TS (17–20, 33) (Table 1). The characteristics of radial bone in TS may be caused by a deletion of entire coding regions in the SHOX gene (SHOX-del) (33). The microarchitecture is affected by remodeling, a process of bone formation mediated by osteoblasts, and bone resorption mediated by osteoclasts (7). Remodeling in TS shows an imbalance between these processes, with bone resorption being more pronounced than bone formation (36), resulting in poor trabecular microarchitecture (35).
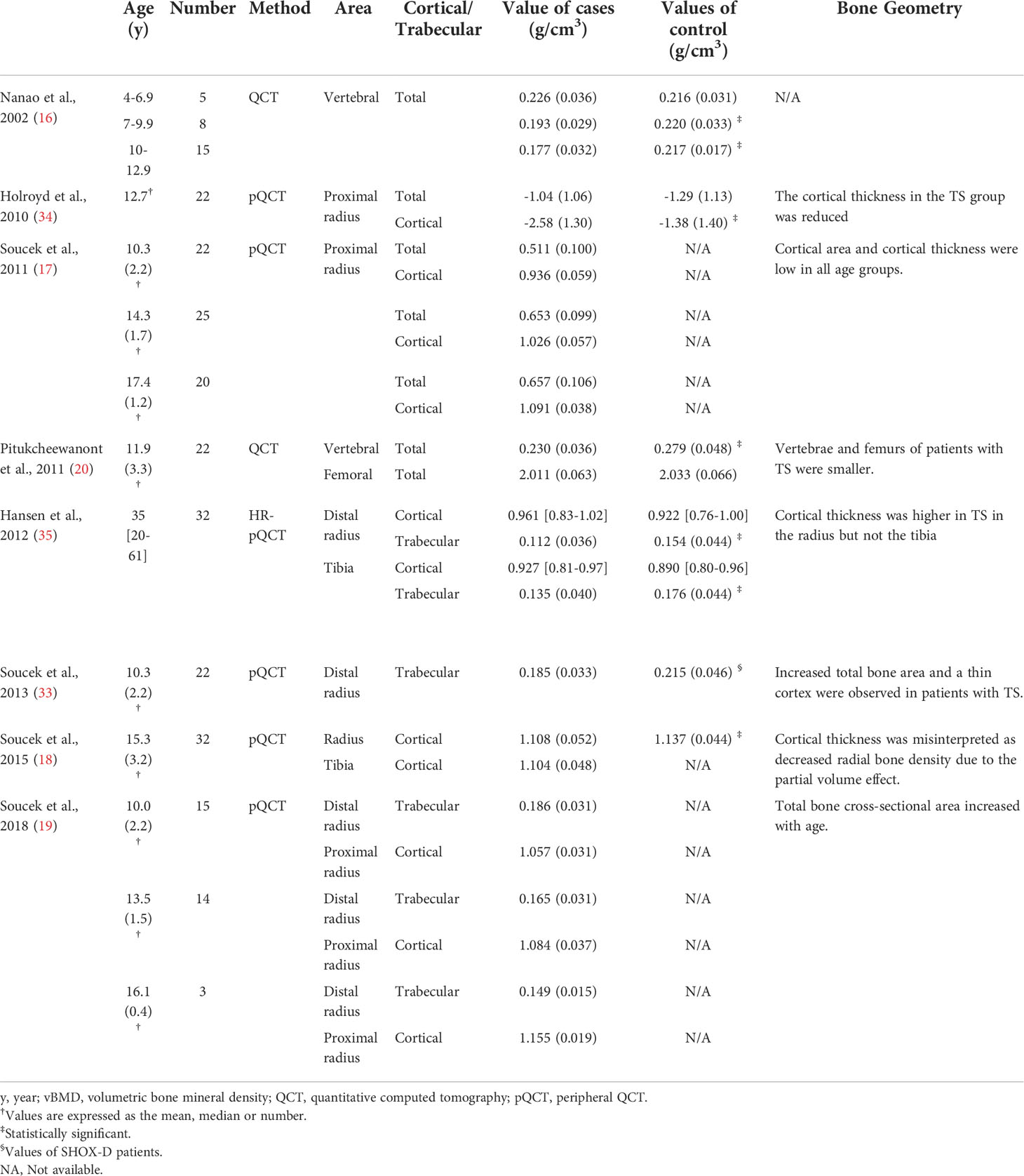
Table 1 Bone density and quality in TS according to QCT, pQCT, and HR-pQCT.
The most obvious cause of fractures in patients with TS is hypogonadism. ERT reportedly decreased the fracture rate in patients with hypogonadism (14). Patients with primary amenorrhea caused by some other diseases besides TS had a significantly higher fracture prevalence than healthy controls (33% vs 5%) (37), suggesting that hypogonadism was one of the significant clinical risk factors associated with fractures. Gravholt et al. published two manuscripts on the fracture rate in patients with TS, demonstrating the importance of ERT for fracture risk reduction in these patients. In the first study, they used the Danish Population Database to show that the relative risk (95% confidence interval [CI]) of fractures in patients with TS was 2.16 (1.50-3.00) compared to the general population (21). Their second study, which employed a similar method, demonstrated that the hazard ratio (95% CI) for fractures in patients with TS was 1.35 (1.04-1.75) (22). The higher fracture risk found in the first study was the result of a difference in the percentage of subjects receiving ERT between the two studies; in the former study, almost none of the patients had received ERT while in the second study, 83% had, indicating the efficacy of ERT. Although some studies have investigated the relationship between BMD and the timing and dosage of ERT as described below, no reports have hitherto directly investigated the relationship between these ERT-related factors and the frequency of fractures.
A higher risk of falling associated with hearing impairment also contributes to the high fracture rate in patients with TS. Several, previous studies reported an association between hearing impairment and the fracture rate (4, 5). Hearing impairment leads to impaired speech perception and spatial orientation, increasing the risk of falling resulting in forearm fractures (4). This type of fracture is common in patients with TS, whose annual, childhood incidence of wrist fractures was significantly higher than in healthy children (9.1/1000 vs 3.5/1000, p < 0.003) (27).
Other reasons for the high fracture risk in patients with TS includes X chromosomal abnormalities (7, 38). SHOX-del, which is observed in almost all patients with TS, may be the one of the most important factors. Altered bone shape and microarchitecture, observed in many patients with TS, possibly stem from SHOX-del (39). Children with SHOX deficiency (SHOX-D) had an increased total bone area (Z-score = 1.5 ± 1.4, p = 0.001) and thin cortex (Z-score = -2.0 ± 1.2, p < 0.001) than healthy subjects (33). Similar results were observed in patients with TS (33) (Table 1). Although no studies have as of yet examined the higher fracture rate associated with SHOX-D, the previously mentioned differences in bone characteristics may contribute to the higher fracture rate in patients with TS. Other genes associated with fractures in TS include bone morphogenetic protein 2 (BMP2), which is involved in bone mineralization; insulin-like growth factor 2 (IGF2), which is involved in bone repair and formation; and secreted frizzled-related protein 1 (sFRP1), which plays an important role in Wnt signaling (40–42). Genome-wide methylation analysis profiling has shown that these genes are not located on the X chromosome but are downregulated in 45, X cells (43).
Comorbidities of TS, such as obesity, diabetes, inflammatory bowel disease (IBD), and thyroid disorder affect bone health (7, 38). Obesity activates both osteoblast and osteoclast functions (44), and epidemiological data show that obesity increases the fracture risk (45). A systematic review demonstrated that the relative risk (95% CI) of any type of fracture in patients with diabetes mellitus was 1.5 (1.3-1.8) (46). A population study reported an increased fracture risk associated with thyrotoxicosis (47), and a review article reported that patients with IBD had an increased fracture risk (48). However, the nature of the association of thyrotoxicosis and IBD with the fracture rate is still unknown (7).
Patients with TS have low bone mineral density (BMD), which is one of the causes of the high prevalence of fractures (5). An association between BMD and the fracture risk was has been observed both in healthy individuals and patients with TS (5, 49). A cohort study of 124, healthy, subadult females indicated that the fracture risk was significantly higher in healthy subjects with a low total volumetric BMD (vBMD) of the distal radius (odds ratio (OR): 1.71) (49). An interview of 177 adult patients with TS demonstrated that an increased risk of fractures was independently associated with low vertebral BMD as measured by dual-energy X-ray absorptiometry (DXA) (OR: 3.2; 95% CI: 1.0-10.5) (5). Based on these results, BMD is now often used as a surrogate outcome to predict the risk of fractures although other factors, such as bone microarchitecture, bone geometry, and the high risk of trauma owning to hearing impairment described above, are also potential risk factors.
One of the most significant causes of low BMD in patients with TS is estrogen deficiency, a well-established finding of this syndrome, as well as postmenopausal osteoporosis (7, 50, 51). Several facts indicate the importance of estrogen for BMD in patients with TS. First, BMD was higher in patients with TS with a spontaneous menstrual cycle, which occurs in 6% of patients with TS (25, 52), than in those with primary hypogonadism (8–12). Second, the later ERT is initiated, the lower the resulting BMD is (13, 53). Third, the BMD Z-score was lower in adolescence than in early childhood (8), suggesting that BMD did not increase as much during adolescence in these patients as in healthy individuals, who are typically exposed to estrogen. In this study, the mean starting age for ERT was 13.5 (range 7.1-21.3) years, or later than the currently recommended age. Therefore, the BMD Z score might not have decreased in these patients if ERT had been started at the appropriate age.
ERT is known to improve BMD in patients with TS, a finding which was borne out by our own study (54), which compared the BMD Z-score measured by DXA before and after cyclic estrogen and progesterone therapy (Kaufmann therapy) in 18 patients with TS and found an increase in the BMD Z-score after the start of therapy (54). To the best of our knowledge, no other study has compared BMD before and after Kaufmann therapy in the same subjects.
ERT is effective in increasing BMD, but the increase is insufficient and needs to be improved. BMD was higher in patients with TS with a spontaneous menstrual cycle than in those with primary hypogonadism even if they received ERT (8–12), suggesting that there is room for improvement in the conventional ERT. In these reports, the mean starting age of ERT was 13.5-20.2 years, and the mean age of menarche onset was 14.7-17.8 years (8–11). Since BMD is known to increase more with earlier ERT initiation (13), patients with TS may achieve long-term BMD if they begin ERT around the recently recommended age of 11-12 years.
Low BMD in patients with TS reportedly begins before pubertal ages (16, 55), suggesting that hypogonadism might not be the only cause. Nanao et al. measured bone density in the lumbar spine using QCT, which mainly represents trabecular BMD, in 21 subadult females with TS and 20, healthy, age- and sex-matched controls (16). The study demonstrated lower BMD in the patients with TS than in the healthy controls in the prepubertal period (16). The authors also observed a gradual decline in vertebral vBMD before prepubertal age (16) (Table 1). Hogler et al. published a study supporting these findings, demonstrating that the decrease in vertebral vBMD in patients with TS occurred before pubertal age (55). One, possible explanation of these findings of low trabecular BMD is the low level of estrogen secretion before pubertal age.
The optimal timing of the start of estrogen replacement therapy for TS is uncertain (10, 54). Saito et al. demonstrated that age at ERT initiation was significantly related to BMD as measured by DXA (53). Another study demonstrated that height, age, and cortical thickness-adjusted cortical vBMD as measured by pQCT was positively correlated to the duration of ERT (17). Recent guidelines recommend that estrogen replacement begin between ages 11 and 12 years and be increased to the adult dosage over 2-3 years (25, 56) although the evidence in terms of BMD is pending.
Furthermore, the optimal, initial dosage and the criteria for increasing the dosage have not been established. One, previous report demonstrated that a high oral 17B-estradiol dosage (4 mg/day) did not affect BMD significantly in adult patients with TS (57). Our previous report demonstrated that BMD in patients with TS who began ethinyl estradiol therapy at an ultra-low dosage (1-5 ng/kg/day) was no different from that of their counterparts receiving classical conjugated estrogen (12). A recent study recommended 3-7 µg/day for transdermal E2 or 0.25 mg/day for 17β oral E2 as the pubertal initiation dose (25) although this recommendation is not evidence-based.
Diet and exercise habits may also contribute to low BMD in patients with TS. The serum vitamin D level was shown to be lower in patients with TS, which may be a contributing cause of lower BMD (38, 58). Physical activity is also reportedly associated with high BMD in patients with TS (59). Thus, an appropriate diet with sufficient vitamin D and exercise are important for bone health, especially in TS (7, 11).
One of the most common methods of assessing BMD is DXA, a low-dose x-ray technology that measures the attenuation of x-ray beams as they pass through tissues of varying density (15). The recommended measurement sites are the lumbar spine, distal radius, proximal femur, or the whole body for adults, and the lumbar spine or total body less head (TBLH) for children (60, 61). The lumbar spine and TBLH consist mainly of trabecular bone, and the distal radius, proximal femur, and whole body consist primarily of cortical bone (60). DXA is rapid, safe, widely available, and use comparatively lower levels of radiation (15). However, in general, DXA can only measure aBMD, which is expressed in g/cm2, but not vBMD, which is expressed in g/cm3. This limitation may cause the values to be skewed by short stature and bone size (14, 15). Although there are various methods of using by DXA to assess vBMD, they are generally only theoretical (15). An exception is the method described by Kroger et al., which uses the cylindrical shape of bone to calculate the vBMD using the following formula: vBMD = aBMD*[4/(π *width of vertebral)] (60, 62). This method has been validated for use in children aged 6-19 years (60).
QCT, which is generally a method of evaluating the lumbar spine or proximal femur using computed tomography (CT), allow us to directly measure the vBMD (in g/cm3) (15, 63). Therefore, QCT can provide the true BMD value independently of short stature and bone size. Furthermore, this method can be used to evaluate cortical and trabecular bone separately (15, 63). However, one of the disadvantages of QCT is that patients are exposed to high doses of radiation (15, 63).
pQCT is a technique for evaluating radial and tibial BMD using the smaller, less expensive peripheral CT scan (15, 63). This method can assess vBMD using a lower radiation dose (64). HR-pQCT can accurately assess cortical BMD with less partial volume effect (15, 18), and also can measure bone microstructure by using indicators, such as cortical porosity, trabecular number, and trabecular spacing, to produce an assessment of bone quality (65).
TBS is an indirect method of measuring the trabecular microarchitecture based on DXA data (66, 67). TBS is calculated as the sum of the squared gray-level differences between pixels at a specific distance (66, 67). The better the trabecular microarchitecture, the more gray-level variation of small amplitude there is, which leads to increasing the TBS score (67). This method is easy, cost-effective, and involves lower levels of radiation exposure. The disadvantage of TBS is the lack of reference data (66).
The methods described above are used to assess BMD or bone quality in patients with TS. Numerous, previous studies have diagnosed low BMD in patients with TS using DXA, but this method has limitations, especially when used in patients with TS (7, 14). Bakalov et al. demonstrated the aBMD value on DXA was influenced by bone size and short stature, resulting in an underestimation of BMD in patients with TS (14). They demonstrated that a difference in the BMD values for the femoral neck between patients with TS and age-matched, healthy, adult females decreased after adjusting for bone size (14).
Several reports have assessed the vBMD in patients with TS using either DXA or QCT (16, 38). Gravholt et al. assessed the vBMD of the lumbar vertebrae in patients with TS using DXA (38), which reconstructs the vertebrae using four scans to allow a three-dimensional view. Nanao et al. measured the vBMD of the lumbar vertebrae in patients with TS using QCT, which can directly provide three-dimensional assessment of BMD, and demonstrated that the vBMD had already decreased during the prepubertal period (16). These methods can reduce the distorting effect of bone size and short stature on BMD assessments (15).
Recently, pQCT, which measures radial bone density and involves less radiation exposure than QCT, has come into use (17, 19) (Table 1). Several studies used pQCT to show that the cortical BMD in patients with TS during and after puberty was lower than in healthy, adult females (17, 34, 68). However, Soucek et al. demonstrated that the cortical BMD on pQCT did not decrease in patients with TS and that the decline in cortical BMD in TS reported previously was due to the partial volume effect described mentioned above (18), which skews assessments of the cortical BMD, particularly in patients with a cortical thickness < 2.0 mm (63, 69). A previous study using HR-pQCT, which is less affected by the partial volume effect, reported no difference in cortical BMD between patients with TS and control subjects (35).
Bone quality contributes to increased or decreased risk of fractures independently of BMD (26). Recent studies have described bone quality in TS, including bone geometry and microarchitecture.
Bone geometry assessments using QCT and pQCT demonstrated that the total bone area increased, and cortical thickness decreased, in TS (Table 1). Soucek et al. demonstrated that the total bone area Z-score (SD) and cortical thickness Z-score (SD) of the proximal radius in prepubertal patients with TS was 0.9 (1.5) and -0.7 (1.2), respectively (33). These findings were more pronounced in patients with SHOX-D (33), suggesting that SHOX-del is a major contributor to altered bone geometry in TS. One of the hypotheses advanced to explain the smaller changes in bone geometry seen in TS than in SHOX-D holds that low serum estrogen might suppress changes in bone geometry (33). Since there are many unknowns regarding the relationship between estrogen and bone geometry, future studies are needed to explore this issue.
Microarchitecture is another important factor determining bone quality and is associated with resistance to fractures (70). A previous study used HR-pQCT to demonstrate weakened trabecular microarchitecture in TS. Hansen et al. compared the radial bone microarchitecture in adult patients with TS and healthy controls using HR-QCT and found that cortical porosity was lower in TS patients (0.58 [0.10-2.27]% versus 1.14 [0.27-2.92]%; p<0.0001) (35). Their study demonstrated a lower trabecular value (1.42 [0.42-2.15] mm-1 versus 1.92 [1.77-2.07] mm-1; p<0.0001) and higher trabecular spacing (0.65 [0.40-2.28] mm versus 0.44 [0.36-1.9] mm) (35). The TBS, an indirect method of measuring trabecular microarchitecture, is also considered a useful predictor of fractures (71). The TBS is calculated using data from DXA, is less burdensome to patients, and involves less radiation exposure than other methods of evaluating bone microarchitecture, such as HR-pQCT (53, 71). Two, previous studies demonstrated an association between the TBS and fracture history, vertebral and femoral neck BMD, and age in patients with TS (53, 71) (Table 2).
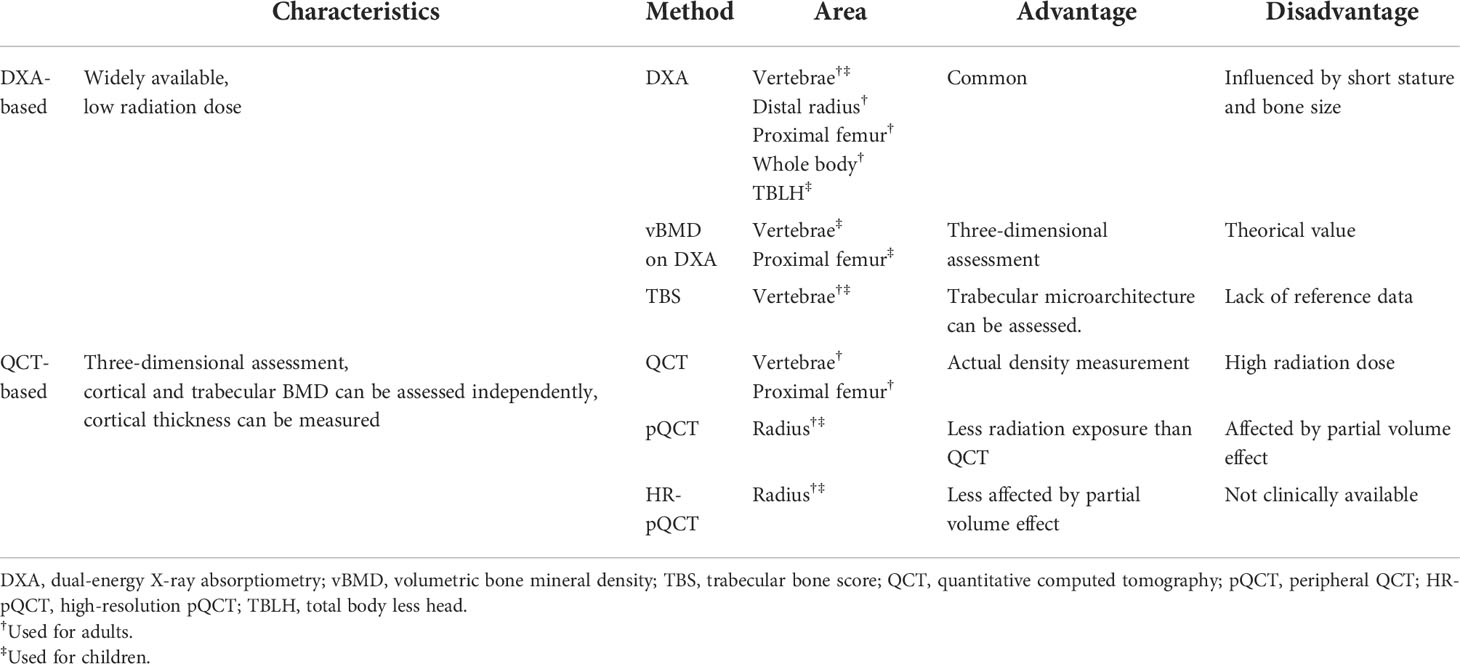
Table 2 Advantages and disadvantages of bone assessment methods in patients with TS.
Further research is needed to evaluate bone quality, including bone geometry and microarchitecture, and more studies using pQCT, HR-pQCT, and the TBS rather than only DXA are needed to identify the best method and predictor of the fracture risk in patients with TS.
YH planned the review. KI searched previous studies and wrote the first draft of the manuscript. YH revised the manuscript. All authors contributed to the article and approved the submitted version.
YH received a grant from the Japan Agency for Medical Research and Development (AMED 22ek01099464s0403).
We are indebted to Mr. James R. Valera for his assistance with editing this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gravholt CH, Viuff MH, Brun S, Stochholm K, Andersen NH. Turner syndrome: mechanisms and management. Nat Rev Endocrinol (2019) 15(10):601–14. doi: 10.1038/s41574-019-0224-4
2. Augoulea A, Zachou G, Lambrinoudaki I. Turner syndrome and osteoporosis. Maturitas. (2019) 130:41–9. doi: 10.1016/j.maturitas.2019.09.010
3. Bakalov VK, Bondy CA. Fracture risk and bone mineral density in turner syndrome. Rev Endocr Metab Disord (2008) 9:145–51. doi: 10.1007/s11154-008-9076-2
4. Cardona Attard C, Cameron-Pimblett A, Puri D, Elliot J, Wilson JC, Talaulikar VS, et al. Fracture rate in women with oestrogen deficiency - comparison of turner syndrome and premature ovarian insufficiency. Clin Endocrinol (2019) 91:743–9. doi: 10.1111/cen.14110
5. Han TS, Cadge B, Conway GS. Hearing impairment and low bone mineral density increase the risk of bone fractures in women with turner’s syndrome. Clin Endocrinol (2006) 65:643–7. doi: 10.1111/j.1365-2265.2006.02643.x
6. Chiarito M, Brunetti G, D’Amato G, Faienza MF. Monitoring and maintaining bone health in patients with turner syndrome. Expert Rev Endocrinol Metab (2020) 15(6):431–8. doi: 10.1080/17446651.2020.1834846
7. Faienza MF, Ventura A, Colucci S, Cavallo L, Grano M, Brunetti G. Bone fragility in turner syndrome: Mechanisms and prevention strategies. Front Endocrinol (2016) 7:34. doi: 10.3389/fendo.2016.00034
8. Costa AM, Lemos-Marini SH, Baptista MT, Morcillo AM, Maciel-Guerra AT, Guerra G Jr. Bone mineralization in turner syndrome: A transverse study of the determinant factors in 58 patients. J Bone Miner Metab (2002) 20:294–7. doi: 10.1007/s007740200042
9. Nishigaki S, Itonaga T, Hasegawa Y, Kawai M. Starting age of oestrogen-progestin therapy is negatively associated with bone mineral density in young adults with turner syndrome independent of age and body mass index. Clin Endocrinol (2021) 95:84–91. doi: 10.1111/cen.14484
10. Nakamura T, Tsuburai T, Tokinaga A, Nakajima I, Kitayama R, Imai Y, et al. Efficacy of estrogen replacement therapy (ERT) on uterine growth and acquisition of bone mass in patients with turner syndrome. Endocr J (2015) 62:965–70. doi: 10.1507/endocrj.EJ15-0172
11. Carrascosa A, Gussinyé M, Terradas P, Yeste D, Audí L, Vicens-Calvet E. Spontaneous, but not induced, puberty permits adequate bone mass acquisition in adolescent turner syndrome patients. J Bone Miner Res (2000) 15:2005–10. doi: 10.1359/jbmr.2000.15.10.2005
12. Hasegawa Y, Ariyasu D, Izawa M, Igaki-Miyamoto J, Fukuma M, Hatano M, et al. Gradually increasing ethinyl estradiol for turner syndrome may produce good final height but not ideal BMD. Endocr J (2017) 64:221–7. doi: 10.1507/endocrj.EJ16-0170
13. Cameron-Pimblett A, Davies MC, Burt E, Talaulikar VS, La Rosa C, King TFJ, et al. Effects of estrogen therapies on outcomes in turner syndrome: Assessment of induction of puberty and adult estrogen use. J Clin Endocrinol Metab (2019) 104(7):2820–6. doi: 10.1210/jc.2018-02137
14. Bakalov VK, Chen ML, Baron J, Hanton LB, Reynolds JC, Stratakis CA, et al. Bone mineral density and fractures in turner syndrome. Am J Med (2003) 115:259–64. doi: 10.1016/s0002-9343(03)00364-4
15. Di Iorgi N, Maruca K, Patti G, Mora S. Update on bone density measurements and their interpretation in children and adolescents. Best Pract Res Clin Endocrinol Metab (2018) 32:477–98. doi: 10.1016/j.beem.2018.06.002
16. Nanao K, Tsuchiya Y, Kotoh S, Hasegawa Y. Low vertebral cancellous bone density in peripubertal girls with turner’s syndrome and boys with hypogonadism. J Pediatr Endocrinol Metab (2002) 15:1537–42. doi: 10.1515/jpem.2002.15.9.1537
17. Soucek O, Lebl J, Snajderova M, Kolouskova S, Rocek M, Hlavka Z, et al. Bone geometry and volumetric bone mineral density in girls with turner syndrome of different pubertal stages. Clin Endocrinol (2011) 74:445–52. doi: 10.1111/j.1365-2265.2010.03955.x
18. Soucek O, Schonau E, Lebl J, Sumnik Z. Artificially low cortical bone mineral density in turner syndrome is due to the partial volume effect. Osteoporos Int (2015) 26:1213–8. doi: 10.1007/s00198-014-2901-4
19. Soucek O, Schonau E, Lebl J, Willnecker J, Hlavka Z, Sumnik Z. A 6-year follow-up of fracture incidence and volumetric bone mineral density development in girls with turner syndrome. J Clin Endocrinol Metab (2018) 103:1188–97. doi: 10.1210/jc.2017-02381
20. Pitukcheewanont P, Numbenjapon N, Safani D, Rossmiller S, Gilsanz V, Costin G. Bone size and density measurements in prepubertal children with turner syndrome prior to growth hormone therapy. Osteoporos Int (2011) 22(6):1709–15. doi: 10.1007/s00198-010-1375-2
21. Gravholt CH, Juul S, Naeraa RW, Hansen J. Morbidity in turner syndrome. J Clin Epidemiol (1998) 51:147–58. doi: 10.1016/s0895-4356(97)00237-0
22. Gravholt CH, Vestergaard P, Hermann AP, Mosekilde L, Brixen K, Christiansen JS. Increased fracture rates in turner’s syndrome: a nationwide questionnaire survey. Clin Endocrinol (2003) 59:89–96. doi: 10.1046/j.1365-2265.2003.01807.x
23. Bercu BB, Kramer SS, Bode HH. A useful radiologic sign for the diagnosis of turner’s syndrome. Pediatrics (1976) 58:737–9. doi: 10.1542/peds.58.5.737
24. Landin-Wilhelmsen K, Bryman I, Windh M, Wilhelmsen L. Osteoporosis and fractures in turner syndrome-importance of growth promoting and oestrogen therapy. Clin Endocrinol (1999) 51:497–502. doi: 10.1046/j.1365-2265.1999.00841.x
25. Gravholt CH, Andersen NH, Conway GS, Dekkers OM, Geffner ME, Klein KO, et al. Clinical practice guidelines for the care of girls and women with turner syndrome: proceedings from the 2016 Cincinnati international turner syndrome meeting. Eur J Endocrinol (2017) 177:G1–G70. doi: 10.1530/EJE-17-0430
26. Fonseca H, Moreira-Goncalves D, Coriolano HJ, Duarte JA. Bone quality: The determinants of bone strength and fragility. Sports Med (2014) 44:37–53. doi: 10.1007/s40279-013-0100-7
27. Ross JL, Long LM, Feuillan P, Cassorla F, Cutler GB Jr. Normal bone density of the wrist and spine and increased wrist fractures in girls with turner’s syndrome. J Clin Endocrinol Metab (1991) 73:355–9. doi: 10.1210/jcem-73-2-355
28. Armas LA, Recker RR. Pathophysiology of osteoporosis: New mechanistic insights. Endocrinol Metab Clin North Am (2012) 41(3):475–86. doi: 10.1016/j.ecl.2012.04.006
29. Heaney RP, Recker RR, Saville PD. Nutrition classics. the journal of laboratory and clinical medicine, volume 92, 1978: Menopausal changes in calcium balance performance. Nutr Rev (1983) 41(3):86–9. doi: 10.1111/j.1753-4887.1983.tb07709.x
30. Sun L, Peng Y, Sharrow AC, Iqbal J, Zhang Z, Papachristou DJ, et al. FSH directly regulates bone mass. Cell. (2006) 125(2):247–60. doi: 10.1016/j.cell.2006.01.051
31. Iqbal J, Sun L, Kumar TR, Blair HC, Zaidi M. Follicle-stimulating hormone stimulates TNF production from immune cells to enhance osteoblast and osteoclast formation. Proc Natl Acad Sci U.S.A. (2006) 103(40):14925–30. doi: 10.1073/pnas.0606805103
32. Carpini S, Carvalho AB, de Lemos-Marini SHV, Guerra-Junior G, Maciel-Guerra AT. FSH may be a useful tool to allow early diagnosis of turner syndrome. BMC Endocr Disord (2018) 18(1):8. doi: 10.1186/s12902-018-0236-4
33. Soucek O, Zapletalova J, Zemkova D, Snajderova M, Novotna D, Hirschfeldova K, et al. Prepubertal girls with turner syndrome and children with isolated SHOX deficiency have similar bone geometry at the radius. J Clin Endocrinol Metab (2013) 98:1241–7. doi: 10.1210/jc.2013-1113
34. Holroyd CR, Davies JH, Taylor P, Jameson K, Rivett C, Cooper C, et al. Reduced cortical bone density with normal trabecular bone density in girls with turner syndrome. Osteoporos Int (2010) 21:2093–9. doi: 10.1007/s00198-010-1170-0
35. Hansen S, Brixen K, Gravholt CH. Compromised trabecular microarchitecture and lower finite element estimates of radius and tibia bone strength in adults with turner syndrome: a cross-sectional study using high-resolution-pQCT. J Bone Miner Res (2012) 27:1794–803. doi: 10.1002/jbmr.1624
36. Faienza MF, Brunetti G, Ventura A, Piacente L, Messina MF, De Luca F, et al. Mechanisms of enhanced osteoclastogenesis in girls and young women with turner’s syndrome. Bone. (2015) 81:228–36. doi: 10.1016/j.bone.2015.07.021
37. Davies MC, Gulekli B, Jacobs HS. Osteoporosis in turner’s syndrome and other forms of primary amenorrhoea. Clin Endocrinol (1995) 43:741–6. doi: 10.1111/j.1365-2265.1995.tb00544.x
38. Gravholt CH, Lauridsen AL, Brixen K, Mosekilde L, Heickendorff L, Christiansen JS. Marked disproportionality in bone size and mineral, and distinct abnormalities in bone markers and calcitropic hormones in adult turner syndrome: A cross-sectional study. J Clin Endocrinol Metab (2002) 87:2798–808. doi: 10.1210/jcem.87.6.8598
39. Frederiksen AL, Hansen S, Brixen K, Frost M. Increased cortical area and thickness in the distal radius in subjects with SHOX-gene mutation. Bone (2014) 69:23–9. doi: 10.1016/j.bone.2014.09.001
40. Bodine PV, Zhao W, Kharode YP, Bex FJ, Lambert AJ, Goad MB, et al. The wnt antagonist secreted frizzled-related protein-1 is a negative regulator of trabecular bone formation in adult mice. Mol Endocrinol (2004) 18(5):1222–37. doi: 10.1210/me.2003-0498
41. Chen L, Jiang W, Huang J, He BC, Zuo GW, Zhang W, et al. Insulin-like growth factor 2 (IGF-2) potentiates BMP-9-induced osteogenic differentiation and bone formation. J Bone Miner Res (2010) 25(11):2447–59. doi: 10.1002/jbmr.133
42. Marrony S, Bassilana F, Seuwen K, Keller H. Bone morphogenetic protein 2 induces placental growth factor in mesenchymal stem cells. Bone. (2003) 33(3):426–33. doi: 10.1016/s8756-3282(03)00195-9
43. Alvarez-Nava F, Lanes R. Epigenetics in turner syndrome. Clin Epigenetics. (2018) 10:45. doi: 10.1186/s13148-018-0477-0
44. Gonnelli S, Caffarelli C, Nuti R. Obesity and fracture risk. Clin cases mineral Bone metabolism: Off J Ital Soc Osteoporosis Mineral Metabolism Skeletal Dis (2014) 11:9–14. doi: 10.11138/ccmbm/2014.11.1.009
45. Hsu YH, Venners SA, Terwedow HA, Feng Y, Niu T, Li Z, et al. Relation of body composition, fat mass, and serum lipids to osteoporotic fractures and bone mineral density in Chinese men and women. Am J Clin Nutr (2006) 83:146–54. doi: 10.1093/ajcn/83.1.146
46. Bai J, Gao Q, Wang C, Dai J. Diabetes mellitus and risk of low-energy fracture: a meta-analysis. Aging Clin Exp Res (2020) 32:2173–86. doi: 10.1007/s40520-019-01417-x
47. Williams GR, Bassett JHD. Thyroid diseases and bone health. J Endocrinol Invest (2018) 41:99–109. doi: 10.1007/s40618-017-0753-4
48. Targownik LE, Bernstein CN, Leslie WD. Inflammatory bowel disease and the risk of osteoporosis and fracture. Maturitas (2013) 76:315–9. doi: 10.1016/j.maturitas.2013.09.009
49. Chevalley T, Bonjour JP, van Rietbergen B, Rizzoli R, Ferrari S. Fractures in healthy females followed from childhood to early adulthood are associated with later menarcheal age and with impaired bone microstructure at peak bone mass. J Clin Endocrinol Metab (2012) 97:4174–81. doi: 10.1210/jc.2012-2561
50. Eastell R, O’Neill TW, Hofbauer LC, Langdahl B, Reid IR, Gold DT, et al. Postmenopausal osteoporosis. Nat Rev Dis Primers (2016) 2:16069. doi: 10.1038/nrdp.2016.69
51. Li L, Wang Z. Ovarian aging and osteoporosis. Adv Exp Med Biol (2018) 1086:199–215. doi: 10.1007/978-981-13-1117-8_13
52. Pasquino AM, Passeri F, Pucarelli I, Segni M, Municchi G. Spontaneous pubertal development in turner’s syndrome. Italian study group for turner’s syndrome. J Clin Endocrinol Metab (1997) 82:1810–3. doi: 10.1210/jcem.82.6.3970
53. Saito S, Koga E, Okada Y, Tsuburai T, Yoshikata H, Miyagi E, et al. Effects of age at estrogen replacement therapy initiation on trabecular bone score in Japanese adults with turner syndrome. Osteoporos Int (2021) 32:671–80. doi: 10.1007/s00198-020-05652-1
54. Itonaga T, Koga E, Nishigaki S, Kawai M, Sakakibara H, Hasegawa Y. A retrospective multicenter study of bone mineral density in adolescents and adults with turner syndrome in Japan. Endocr J (2020) 67:1023–8. doi: 10.1507/endocrj.EJ20-0083
55. Hogler W, Briody J, Moore B, Garnett S, Lu PW, Cowell CT. Importance of estrogen on bone health in turner syndrome: A cross-sectional and longitudinal study using dual-energy X-ray absorptiometry. J Clin Endocrinol Metab (2004) 89:193–9. doi: 10.1210/jc.2003-030799
56. Donaldson M, Kristrom B, Ankarberg-Lindgren C, Verlinde S, van Alfen-van der Velden J, Gawlik A, et al. Optimal pubertal induction in girls with turner syndrome using either oral or transdermal estradiol: A proposed modern strategy. Horm Res Paediatr (2019) 91:153–63. doi: 10.1159/000500050
57. Cleemann L, Holm K, Kobbernagel H, Kristensen B, Skouby SO, Jensen AK, et al. Dosage of estradiol, bone and body composition in turner syndrome: A 5-year randomized controlled clinical trial. Eur J Endocrinol (2017) 176:233–42. doi: 10.1530/EJE-16-0582
58. Cleemann L, Hjerrild BE, Lauridsen AL, Heickendorff L, Christiansen JS, Mosekilde L, et al. Long-term hormone replacement therapy preserves bone mineral density in turner syndrome. Eur J Endocrinol (2009) 161:251–7. doi: 10.1530/EJE-09-0020
59. Naeraa RW, Brixen K, Hansen RM, Hasling C, Mosekilde L, Andresen JH, et al. Skeletal size and bone mineral content in turner’s syndrome: Relation to karyotype, estrogen treatment, physical fitness, and bone turnover. Calcif Tissue Int (1991) 49:77–83. doi: 10.1007/bf02565125
60. Wasserman H, O’Donnell JM, Gordon CM. Use of dual energy X-ray absorptiometry in pediatric patients. Bone. (2017) 104:84–90. doi: 10.1016/j.bone.2016.12.008
61. Crabtree NJ, Arabi A, Bachrach LK, Fewtrell M, El-Hajj Fuleihan G, Kecskemethy HH, et al. Dual-energy X-ray absorptiometry interpretation and reporting in children and adolescents: the revised 2013 ISCD pediatric official positions. J Clin Densitom. (2014) 17(2):225–42. doi: 10.1016/j.jocd.2014.01.003
62. Kröger H, Kotaniemi A, Vainio P, Alhava E. Bone densitometry of the spine and femur in children by dual-energy x-ray absorptiometry. Bone Miner. (1992) 17(1):75–85. doi: 10.1016/0169-6009(92)90712-m
63. Lewiecki EM. Imaging technologies for assessment of skeletal health in men. Curr osteoporosis Rep (2013) 11(1):1–10. doi: 10.1007/s11914-012-0128-x
64. Müller A, Rüegsegger E, Rüegsegger P. Peripheral QCT: A low-risk procedure to identify women predisposed to osteoporosis. Phys Med Biol (1989) 34(6):741–9. doi: 10.1088/0031-9155/34/6/009
65. Burrows M, Liu D, McKay H. High-resolution peripheral QCT imaging of bone micro-structure in adolescents. Osteoporos Int (2010) 21(3):515–20. doi: 10.1007/s00198-009-0913-2
66. Kong SH, Hong N, Kim JW, Kim DY, Kim JH. Application of the trabecular bone score in clinical practice. J Bone Metab (2021) 28(2):101–13. doi: 10.11005/jbm.2021.28.2.101
67. Silva BC, Leslie WD. Trabecular bone score: A new DXA-derived measurement for fracture risk assessment. Endocrinol Metab Clin North Am (2017) 46(1):153–80. doi: 10.1016/j.ecl.2016.09.005
68. Bechtold S, Rauch F, Noelle V, Donhauser S, Neu CM, Schoenau E, et al. Musculoskeletal analyses of the forearm in young women with turner syndrome: A study using peripheral quantitative computed tomography. J Clin Endocrinol Metab (2001) 86:5819–23. doi: 10.1210/jcem.86.12.8063
69. Binkley TL, Specker BL. pQCT measurement of bone parameters in young children. J Clin Densitom (2000) 3:9–14. doi: 10.1385/jcd:3:1:009
70. Brandi ML. Microarchitecture, the key to bone quality. Rheumatol (Oxford) (2009) 48 Suppl 4:iv3–8. doi: 10.1093/rheumatology/kep273
Keywords: Turner syndrome, fracture, hypogonadism, BMD, QCT, TBS
Citation: Ikegawa K and Hasegawa Y (2022) Fracture risk, underlying pathophysiology, and bone quality assessment in patients with Turner syndrome. Front. Endocrinol. 13:967857. doi: 10.3389/fendo.2022.967857
Received: 13 June 2022; Accepted: 29 September 2022;
Published: 17 October 2022.
Edited by:
Giacomina Brunetti, University of Bari Aldo Moro, ItalyReviewed by:
Sheng Guo, Shanghai Jiao Tong University, ChinaCopyright © 2022 Ikegawa and Hasegawa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kento Ikegawa, aWtlZ2F3YWtlbnRvNzIxQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.