 Antonio Mercorio
Antonio Mercorio Pierluigi Giampaolino
Pierluigi Giampaolino Andrea Romano
Andrea Romano Patrick Dällenbach
Patrick Dällenbach Nicola Pluchino
Nicola Pluchino- 1Department of Pediatrics Gynecology and Obstetrics, Division of Gynecology, Geneva University Hospitals, Geneva, Switzerland
- 2Department of Public Health, School of Medicine, University of Naples Federico II, Naples, Italy
- 3Obstetrics and Gynaecology Department, GROW - School for Oncology and Reproduction, Maastricht University, Maastricht, Netherlands
Endometriosis is a chronic, multifactorial, estrogen-dependent disease. The abnormal endocrine microenvironment of endometriosis lesions is considered a main feature and multiple enzymatic pathways leading to local increased synthesis of estrogens have been identified. However, the relevance of intracrinology in clinical practice is still lacking. Medline, Embase, Scopus database were systematically searched for studies reporting on local estrogens metabolism of endometriotic lesions. The main enzymatic pathways involved in the intracrinology of endometriosis such as aromatase (CYP19A1), 17β-hydroxysteroid dehydrogenase (HSD17B) type 1, type 2 and type 5, steroid sulfatase (STS), estrogen sulfotransferase (SULT1E1) were assessed with a critical perspective on their role in disease endocrine phenotyping, drug resistance and as therapeutic targets. Overall, studies heterogeneity and missing clinical data affect the interpretation of the clinical role of these enzymes. Although the use of some drugs such as aromatase inhibitors has been proposed in clinical practice for two decades, their potential clinical value is still under investigation as well as their modality of administration. A closer look at new, more realistic drug targets is provided and discussed. Altered expression of these key enzymes in the lesions have far reaching implication in the development of new drugs aimed at decreasing local estrogenic activity with a minimal effect on gonadal function; however, given the complexity of the evaluation of the expression of the enzymes, multiple aspects still remains to be clarified.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022311329, identifier CRD42022311329.
Introduction
Endometriosis is described by the presence of endometrial-like tissue outside the uterus. It is defined as an estrogen-dependent, inflammatory, and chronic disease, often associated with pelvic pain and subfertility/infertility. The etiology remains uncertain and seems to be related to a complex interplay between family of genes associated with the immune system functioning, sex steroid hormone pathways (neuro)inflammation and environmental risk factors (1).
The estrogen-dependent nature of endometriosis is well known and clinically highlighted by the relapse of the disease in premenopausal women post discontinuation of anti-gonadotropic therapy, as well as in postmenopausal women following the administration of estrogen replacement therapy (2–4) Estrogens show direct cellular antiapoptotic and proliferative effects on the endometriosis lesion as well as promote the pro-inflammatory microenvironment, leading to the chronic nature of the disease (2).. Recent genomics, transcriptomics, and proteomics data, show that endometriosis tissue has a different hormonal environment (5). Increased estrogenic responsiveness, based on the aberrant number and ratio of ERalpha/ER beta (6), abnormal estrogen signaling, progesterone resistance have provided evidence that estrogen effects in normal endometrium do not fully replicate their action on endometriosis (7). Moreover, several studies have shown that endometriotic lesion represents a microenvironment where a multistep enzymatic process leads to an altered metabolism of DHEA or other androgen precursors into bioactive estrogens (Table 1). This mechanism which was called “intracrinology” was primarily defined by Fernand Labrie (8) as the combination of steroids that exhibit their action in the same cell without any pericellular space secretion. More recently, the term has been extended to the tissue microenvironment as the capacity to regulate tissue steroid concentrations from circulating precursors (9, 10).
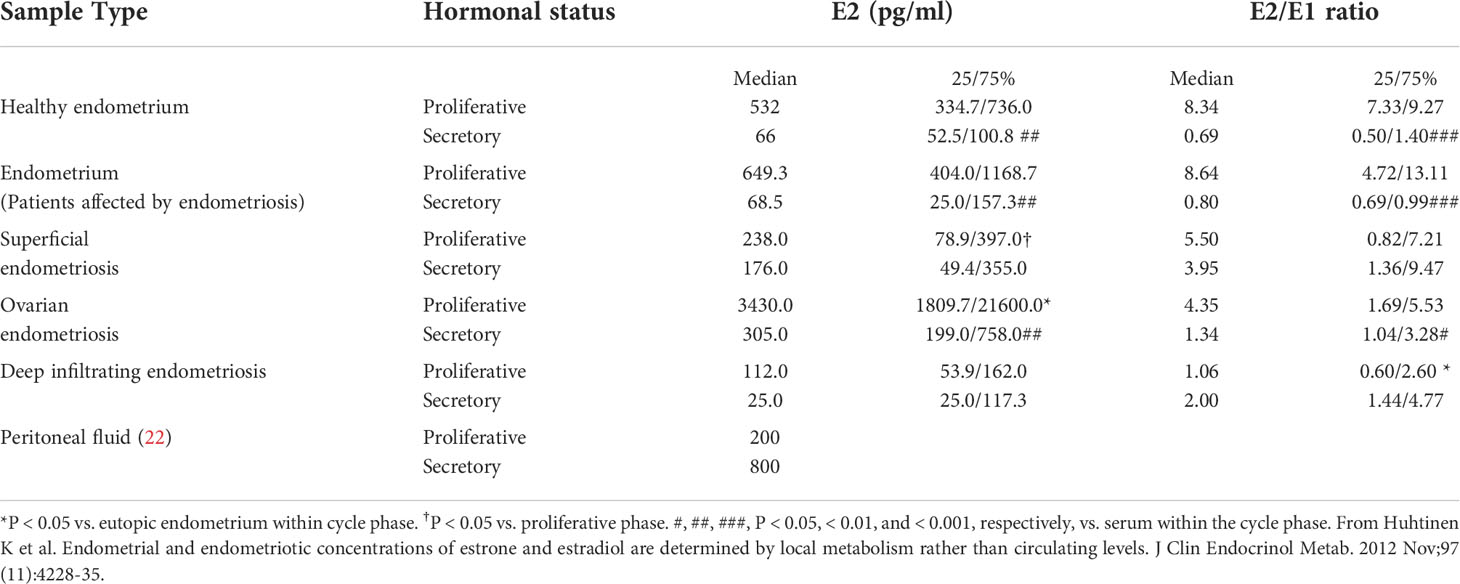
Table 1 Estrogen concentrations in women with and without endometriosis.
The ability of peripheral tissues to use blood precursors and generate steroids has been quite well characterized for tissue remodeling and critical phases such as implantation, early pregnancy development and menstruation (11, 12).The evidence that intracrinology might play a role in the aberrant endocrine environment of endometriosis (13) have far-reaching implications for disease physiopathology, molecular characterization, and drug targeting. Although a large body of evidence in the last ten years supports the view that that endometriosis is a heterogeneous disease, molecular and endocrine clustering processes are just beginning to be understood. The macroscopic appearance of the disease poorly correlates with painful symptoms. Hormonal signatures have the potential to optimize disease characterization and management in the clinical setting. The present article aims to review the available literature investigating the association of intracrinology of endometriosis with clinical features of the disease. Current and ongoing clinical studies targeting intracrinology will be critically reviewed.
Materials and methods
Search strategy
Following protocol registration with PROSPERO (Registration number CRD42022311329) a systematic review was conducted according to Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines. No approval from the Institutional Research Ethics Committee was sought owing to the nature of this work. The following search query was submitted throug Medline, Embase and Scoups database: (“oestrogen”[All Fields] OR ′′estrogens”[MeSH Terms] AND (′′metabolism”[All Fields] OR ′′metabolism”[MeSH Terms] OR ′′metabolic networks and pathways”[MeSH Terms] AND (“endometriosis”[MeSH Terms] OR (“endometriosis”[All Fields]). In addition, Embase and Medline were searched with broader terms: endometriosis AND estrogen metabolism AND steroid sulfatase; endometriosis AND estrogen metabolism AND 17beta hydroxysteroid dehydrogenase; endometriosis AND estrogen metabolism AND estrogen sulfotransferase.
Study selection
We limited the search to publications in English and excluded article published earlier than 1995. Potentially eligible studies were retrieved in full text for the assessment of their eligibility. Study selection was conducted independently by two reviewers (AM and NP) with disagreement resolved by consensus. We included all studies that satisfied the following eligibility criteria, i) They were human based studies. Studies on animal models and in vitro studies investigating human tissue derived cell lines were excluded, ii) They presented original research data, iii) Participants had endometriosis confirmed by histology. In order to highlight the association of the enzymes involved in the intracrinology of endometriosis and the clinical features of the disease, we decided to focus preferentially on their protein expressions levels which reflects gene function more directly than mRNA and is more directly related to phenotype; however, due to the paucity of data present in literature this focused analysis was possible only for the “aromatase” enzyme.
Data extraction and analysis
A standardized critical appraisal and data extraction tool was generated using criteria from CASP (Critical Appraisal Skills Programme) and statements, PRISMA, STARD (Standards for Reporting Diagnostic accuracy studies) and STROBE (Strengthening The Reporting of Observational Studies in Epidemiology) as appropriate. Two reviewers independently appraised the articles and extracted data (AM and NP).
Risk of bias
To reduce selection bias, the abstracts and full text papers were evaluated by masking the authors as far as possible and by basing decisions regarding relevance and eligibility on the independent appraisal by two reviewers. Bias in studies included was assessed independently by the two reviewers.
Results
Study selection
Total articles retrieved after duplicated removal were 1023. Analysis of the titles and abstract led to the removal of 949 papers, including repeated hits and articles based on disease other than endometriosis or full text in English not available. Out of the 74 articles remained for full-text analysis, 28 were excluded because they did not provide original results (i.e. reviews) or they referred to preclinical data. References in the selected articles were controlled for missing inclusions and six articles were included manually (Figure 1). In the end a total of 40 articles were included in this systematic review.
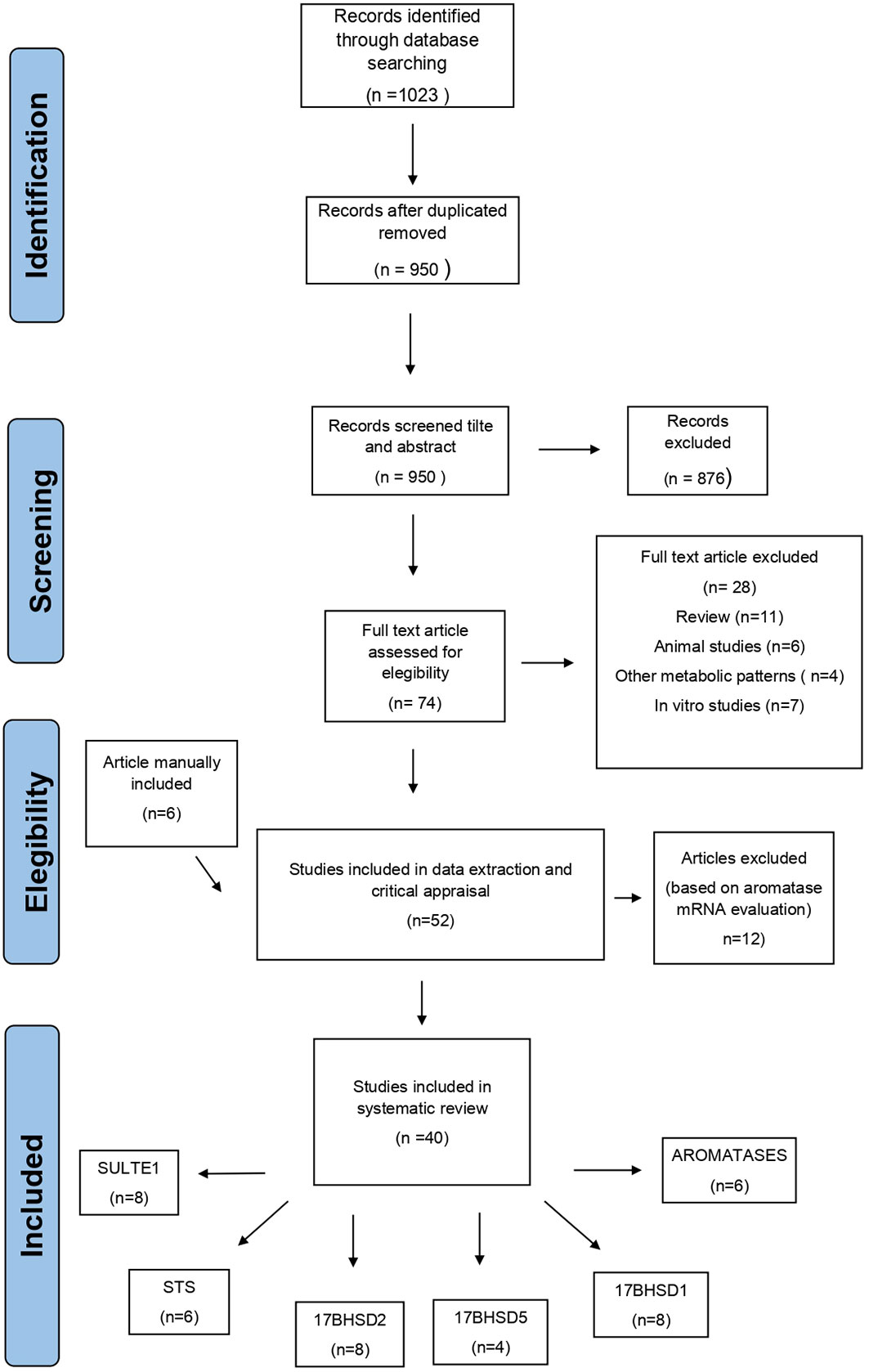
Figure 1 Flow diagram of the systematic search strategy on published studies reporting about the expression of the enzymes involved in the intracrinology of endometriosis.
Characteristics of the included studies
In the following sections, studies evaluating the expressions of the enzymes controlling the synthesis/inactivation of estrogens in endometriosis are examined with respect to clinical stage of disease, severity of symptoms and disease localization. Analysis of targeted enzyme therapy and current hormonal treatments effect on intracrinology regulation are provided. Four are the principal pathways that have received more attention and that likely contribute more than others to aberrant endocrine regulation: aromatase,17β-hydroxysteroid dehydrogenase, sulfatase and sulfotransferase (Figure 2).
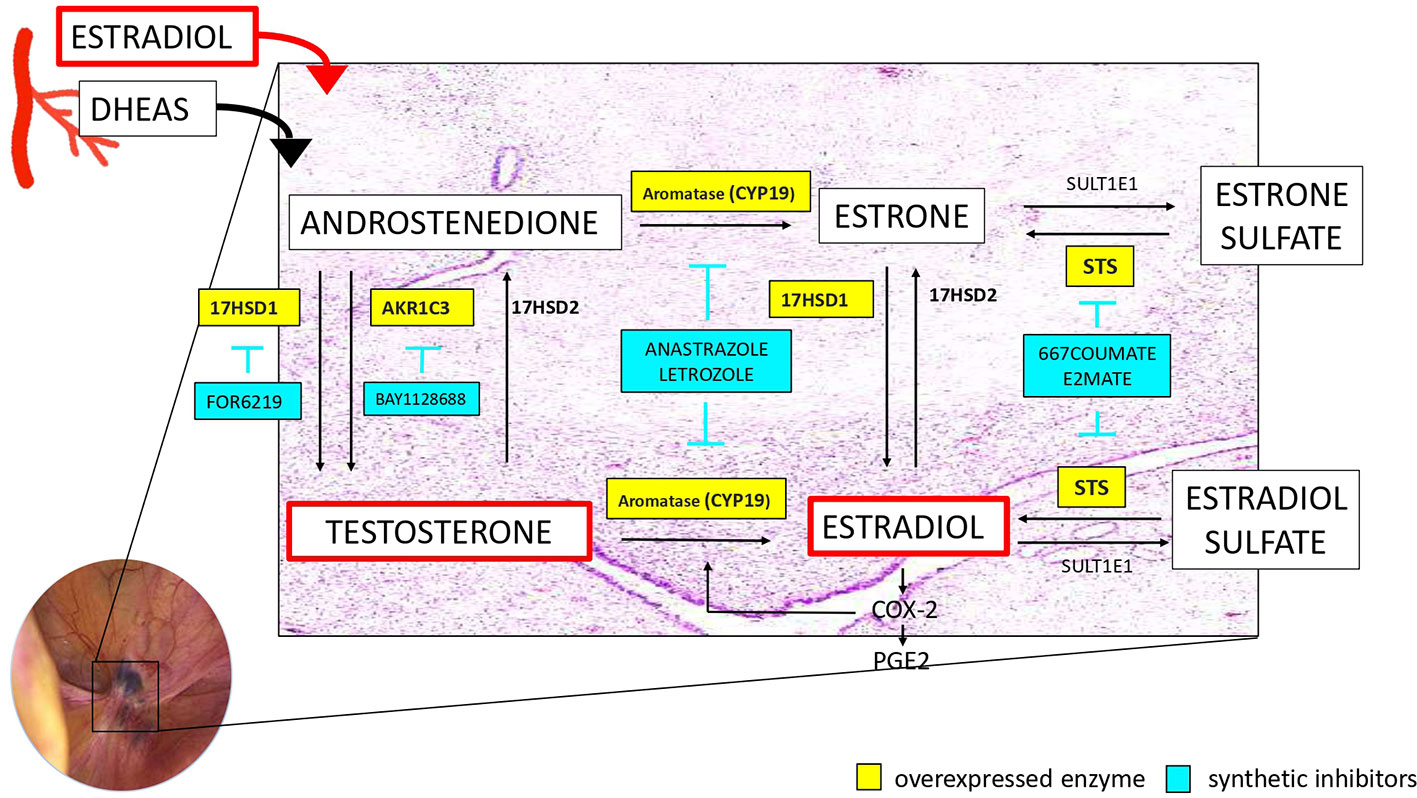
Figure 2 Schematic representation of the intracrine estrogen metabolism with the additional data on the overexpressed enzymes and their synthetic inhibitors.
Aromatase
Aromatase has been extensively investigated in endometriosis. However, findings are still conflicting. Aromatase is encoded by the CYP19A1 gene, a member of the cytochrome P450 superfamily, which consists of monooxygenases that catalyze several reactions involved in steroidogenesis. It is physiologically expressed in growing ovarian follicles by granulosa cells, promoting the conversion of androstenedione (A4) and testosterone (T) to estrone (E1) and estradiol (E2), respectively. In the last ten years, it has been proposed that endometriotic tissue features different aromatase expression compared to normal endometrium, which is responsible for the local production of estradiol and in turn stimulates the production of the cyclooxygenase type 2 (COX-2) enzyme, resulting in elevated levels of prostaglandin E2 (PGE2), which is a potent stimulator of aromatase activity in endometriosis (14). Nevertheless, it should be taken into account that immunohistochemistry is a semi-quantitative method which does not consent the actual “quantification” and cannot determine the activity of an enzyme but only detect its presence. This positive feedback produces a local, continuous stream of estrogen and PGE2 in endometriotic tissue, supporting a loop between a hyperestrogenic environment, inflammation and cell proliferation (15, 16). In vitro and in vivo studies clearly show the expression of aromatase in stromal and epithelial cells within endometriotic lesions. In vitro, mechanistic models support its crucial role. However, the full picture of endometriotic aromatase in the clinical setting has not been fully clarified.
Aromatase expression in human tissue
To date, most investigations have been performed at the mRNA level or using Western blotting. There is a paucity of data utilizing tissue staining techniques, and the results are conflicting. Although mRNA expression is informative of protein expression, mRNA copies do not necessarily reflect the level of functional protein: posttranscriptional and posttranslational regulation induces functionally important changes that cannot be seen at the mRNA level (17). Therefore, we focus mainly on protein expression, which reflects gene function more directly than mRNA and is more directly related to phenotype (Table 2). Based on our research criteria, only six studies evaluated aromatase expression at the protein level using immunohistochemistry. The level of staining differs among studies in relation to the type of endometriosis, number of positive patients and correlation with clinical symptoms.

Table 2 Expression (protein levels), enzymatic activity of aromatase in endometriotic lesions and correlation with disease characteristics, eutopic and healty endometrium.
In two cohorts of mixed lesions (ovary, peritoneal and deep implants), positive immunohistochemical expression of aromatase was found in only 38/62 women (61.3% of patients with histologically confirmed endometriosis) (21) and in 32/35 patients with mild to moderate endometriosis according to the revised American Fertility Society (AFS) classification (18). These patients showed multiple endometriomas, frequently bilateral, and more moderate-to-severe chronic pelvic pain. Eutopic endometrium often stained aromatase in endometriosis patients (18, 21), being detectable by IHC in 66/92 patients but also in the endometrium of 13/14 (95%) patients with severe dysmenorrhea but free from endometriosis. Interesting in asymptomatic women (control group) aromatase expression was not detected (18). This finding suggests that functional endometrial changes leading to an increase in aromatase expression may therefore precede the development of endometriosis and have a positive correlation with dysmenorrhea severity.
In a recent study, patients experiencing moderate to severe deep dyspareunia showed higher epithelial aromatase in deep lesions involving the pouch of the Douglas than patients experiencing absence to mild dyspareunia (8). However, in 209 samples of mixed-type endometriosis (peritoneal, ovarian and rectovaginal lesions), aromatase expression was not detected in either ectopic or eutopic endometrial tissue, although there was no mention of pain symptoms (23) or even stage of disease (20).
Unfortunately, conflicting data and methodological concerns affect the interpretation of the role of this enzyme in endometriotic implants, and consistent proof of aromatase expression is still lacking. Some of the variations in the reported patterns of expression may relate to the use of different antibodies, analysis of eutopic endometrium at different stages of the cycle, the type of lesion or the inflammatory status. Moreover, fragments of ovarian tissue may be included in the histological sections of specimens of ovarian endometriosis, affecting the accuracy of the evaluation.
Aromatase inhibitors (AIs)
Despite the paucity of human data, aromatase blockade has been proposed as a treatment for endometriosis since its first successful use in a postmenopausal woman with aggressive and refractory endometriosis (24). Thereafter, different studies, published over the last twenty years, have evaluated the efficacy of AI treatment alone or combined with other hormonal therapies. Selective third-generation AIs, letrozole and anastrozole, have been found to have better efficacy and tolerability than earlier agents (25). Seven clinical trials have compared the use of these drugs with other treatments for endometriosis (Table 3). Aromatase inhibitors, whenever given in combination with progestins, GnRHa or administered alone, showed greater results in terms of pain reduction than conventional hormonal treatments. Anastrozole (1 mg/day), administered in conjunction with goserelin for 6 months in patients with severe baseline endometriosis (rASRM score >40), showed greater improvement in pain Total Pelvic Symptom Score (TPSS) than patients using goserelin alone (ΔTPSS-P baseline -24 months PMT 5.0 vs. 3.3 p<0.0001) (26). The efficacy of AIs combined with norethisterone acetate (NETA) (letrozole 2.5 mg/day plus norethisterone acetate 2.5 mg/day) versus NETA alone (2.5 mg/day) has been specifically evaluated in rectovaginal endometriosis (27). Significantly lower dyspareunia and chronic pelvic pain were reported in the group receiving the double drug regimen after 3 months. Letrozole was also investigated as single molecule in a randomized clinical trial based demonstrating the lowest mean chronic pelvic pain at 5 months compared to danazol (600 mg/day) and placebo. No data, however, are available regarding the stage, type, and localization of disease (28). Four additional studies investigating more than 200 patients showed comparable results in terms of pain reduction between AIs vs. GnRHa or AI plus NETA vs. NETA alone or AI plus GnRH (29–32), making less clear the clinical added value of AI over conventional, first-line, treatments. The onset of recurrence of symptoms during follow-up was always comparable among all studies. Adding AI to current hormonal treatment does not offer advantages over the single drug, as control group. Only one study, showed a longer interval before recurrence of symptoms during the 24-month follow-up: recurrence was registered in only 3/40 (8%) of patients in the combined arm (AI + goserelin) compared to 14/40 (35%) in the goserelin-only arm (26). Regarding side effects, AIs in association with progestins did not seem to have a more detrimental impact than progestin alone in two trials (30, 32). However, in Ferrero et al., a high incidence of adverse events in patients taking letrozole plus norethisterone acetate was registered (two patients interrupted the treatment because of severe joint pain, others had severe migraine attacks, myalgia and breakthrough bleeding) (27). As a consequence, “global degree satisfaction” was not different among groups despite a better pain reduction in patients receiving AI plus progestins. When AI was associated with GnRHa, a higher rate of side effects was found, and Ferrero et al. were forced to end the study preterm due to the high incidence of adverse effects (arthralgia, decreased libido, hot flashes) (30). This supports the hypothesis that cotreatment with progestins is more accepted than cotreatment with gonadotropin-releasing hormone analogs. In terms of bone mineral density, no significant change were reported when AIs were combined with NETA (27). In contrast, when associated with GnRH, AIs resulted in a significant decrease in the mineral bone density at 6 months (26, 30); however, none of these patients fell into the category of osteopenia and, furthermore, this reduction was not confirmed at 2 years of treatment withdrawal (26).
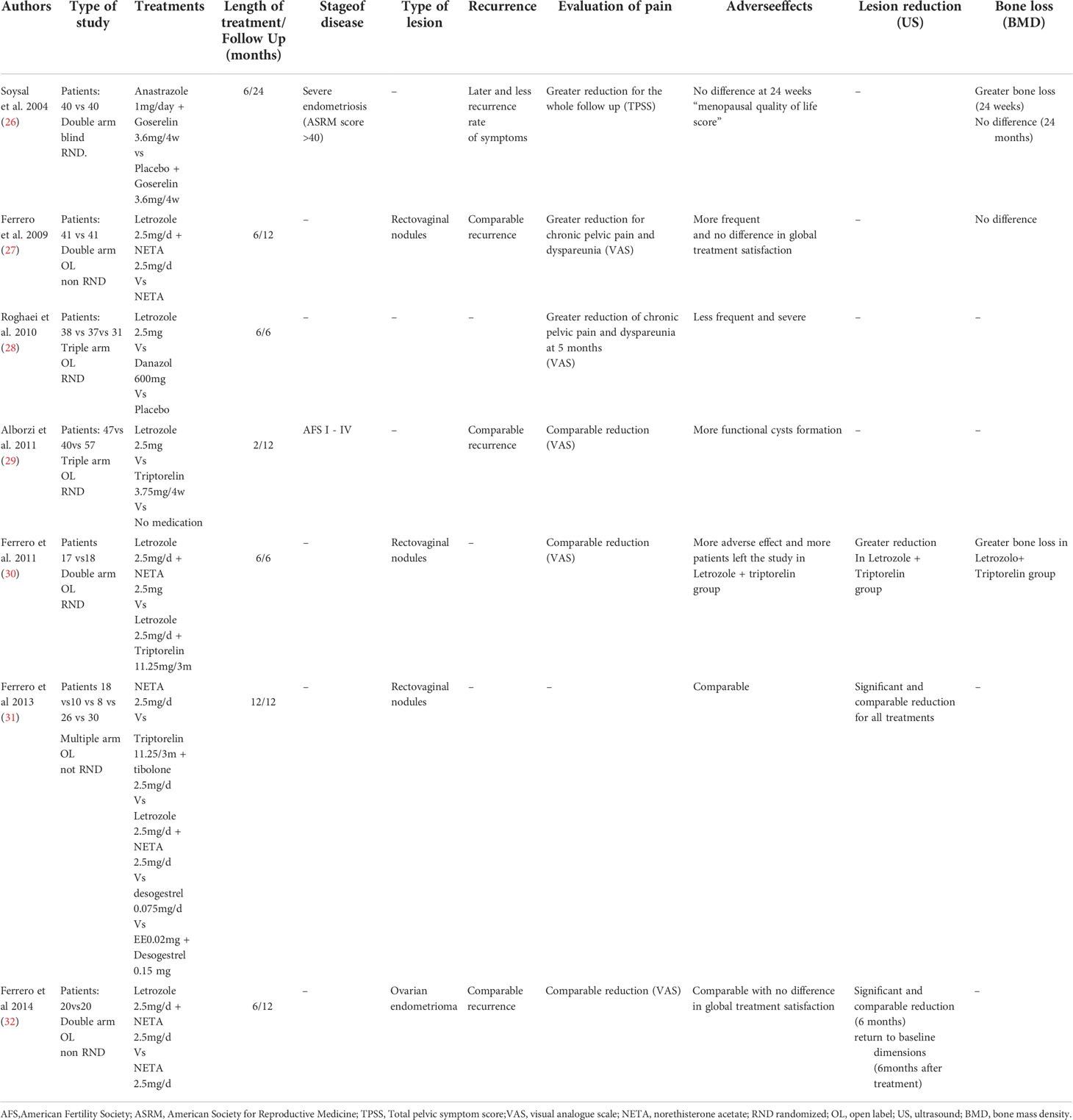
Table 3 Clinical trials comparing AIs (alone or combined) with other treatments in women with endometriosis.
Three trials evaluated whether AIs were superior to other hormonal treatments for the regression of endometriosis lesions (30–32). The combination of letrozole plus NETA showed a greater reduction in endometrioma at 6 months of treatment than the administration of Neta alone (-74.4± 4.2% vs. -46.8±3.8%). Regrettably, no patients reported a complete regression of cysts, and endometriomas usually regrew after treatment discontinuation (32). Two studies confirm the reduction of the size of rectovaginal lesions (30, 31). In a multiple arms trial, letrozole 2.5 mg/d + NETA 2.5 mg/d was compared with other first-line regimens and no difference of volume reduction was recorded (31). When letrozole is administered in combination with triptorelin demonstrated a significant reduction in the volume of the endometriotic nodules after 6 months (16.1 cm3 ± 10.0% vs. 10.2 cm3 ± 6.3%; p = 0.048) in comparison to NETA alone (30).
The heterogeneity of the current literature limits the evaluation of the potential advantages provided by the use of AIs for the treatment of endometriosis as well as the assessment of side effects: severity and type of the disease are often underreported, and follow-up of pain symptoms is not long enough to make consistent conclusions regarding their implementation in clinical practice. Based on current recommendations, AIs should be now offered only in case of surgical and other hormonal therapies failure (33). To minimize the impact on systemic estrogen levels, administration of an aromatase inhibitor (AI) via an intravaginal ring (IVR) has been proposed. This approach offers the advantage of providing sustained and controlled drug release and requires a lower dose to achieve equivalent pharmacodynamic efficacy compared to oral administration (it avoids the first-pass effect of the liver) (34). Phase I and Phase II studies on an IVR containing a combination of anastrazole and levonorgestrel gave reassuring results in terms of safety and tolerability at different doses as well as contraceptive efficacy (35, 36). However, the clinical effect of this combination is still unknown. A pilot study demonstrated modest efficacy following administration of vaginal anastrozole (0.25 mg/d) for 6 months offered to 10 women suffering from rectovaginal endometriosis: although a small, statistically significant improvement in dysmenorrhea was observed, chronic pelvic pain, dyspareunia and rectovaginal lesion size remained unchanged. The inefficacy of the therapy could be attributed to inadequate dose exposure given the absence of a reduction in circulating E2 (37). Endometriosis-targeted inhibition of local aromatase, despite its promising potential, has recently been discredited, using a new chick embryo allantoic membrane (CAM) model incorporating xenografted human endometriosis cysts: in this recent study was shown that topical treatment with anastrozole reduced the size of the lesions, corroborating the presence of aromatase activity in endometriotic tissue. However, when systemic estrogens reached the grafted endometriotic tissue, the effect of the local inhibition of aromatase by anastrozole was blunted. This finding supports the speculation that endometriosis aromatase cannot be a drug target without the inhibition of systemic estrogen synthesis (38).
17β-Hydroxysteroid dehydrogenase (HSD17B)
17β-Hydroxysteroid dehydrogenase (HSD17B) isozymes are a group of alcohol oxidoreductases, of which several isoforms are expressed in human tissues. Of particular interest is the activity of HSD17B1, which is responsible for the production of testosterone (T) and 17 beta estradiol (E2) from weak androstenedione (A4) and estrone (E1), respectively, and HSD17B2, which, in contrast, catalyzes the opposite reaction, metabolizing E2 to the less active E1. These pathways are believed to be involved in the abnormal ratio E2/E1 in the ectopic endometrium. Interesting data on the activity of these enzymes in endometriosis comes from Delvoux et al: in this study, endometriotic tissues of 14 women affected by moderate to severe endometriosis (endometrioma, deep infiltrative and superficial peritoneal endometriosis) showed a marked increase in HSD17B1 activity, leading to higher estradiol (E2) production than normal endometrial tissue (23). Conversely, the activity of the enzymes responsible for the oxidation of 17-estradiol into the less active estrone was significantly lower. Therefore, the net balance between oxidization and reduction favored the production of 17-beta E2 in ectopic tissues compared with endometrial tissues of healthy patients.
HSD17B1 expression in human tissue
Despite this premise, discordant results arise from studies evaluating HSD17B1 expression (Table 4). At the protein level, there was no evidence of HSD17B1 hyperexpression in endometriosis tissue (41, 45). In 14 samples of rectovaginal endometriosis, HSD17B1 protein levels were found to be even lower than those in normal endometrium. This result diverges from HSD17B1 mRNA level, which was higher than in controls, raising the hypothesis that the expression of the HSD17B1 gene may therefore not necessarily reflect changes at the functional protein level (41). Delvoux et al. and found a greater than 6000-fold increase in HSD17B1 mRNA expression in endometriosis (Stade IV rASRM, mixed lesions) compared to eutopic tissue (46). In addition, inhibition of HSD17B1 by a specific inhibitor (3-[15b-estronyl]-N-(5-methyl-thiazol-2-yl)-propionamide) was achieved, decreasing the production of 17-estradiol by at least 85% in 70% of patient biopsies tested ex-vivo. Three additional studies (a total of 101 patients were evaluated), upregulation of the HSD17B1 enzyme was confirmed only in ovarian endometriosis (42–44). Interestingly, data from two studies (39, 45) are in contrast with the abovementioned results and no difference of HSD17B1mRNA between endometriosis (each type) and controls (eutopic endometrium in patients without endometriosis) were detected.
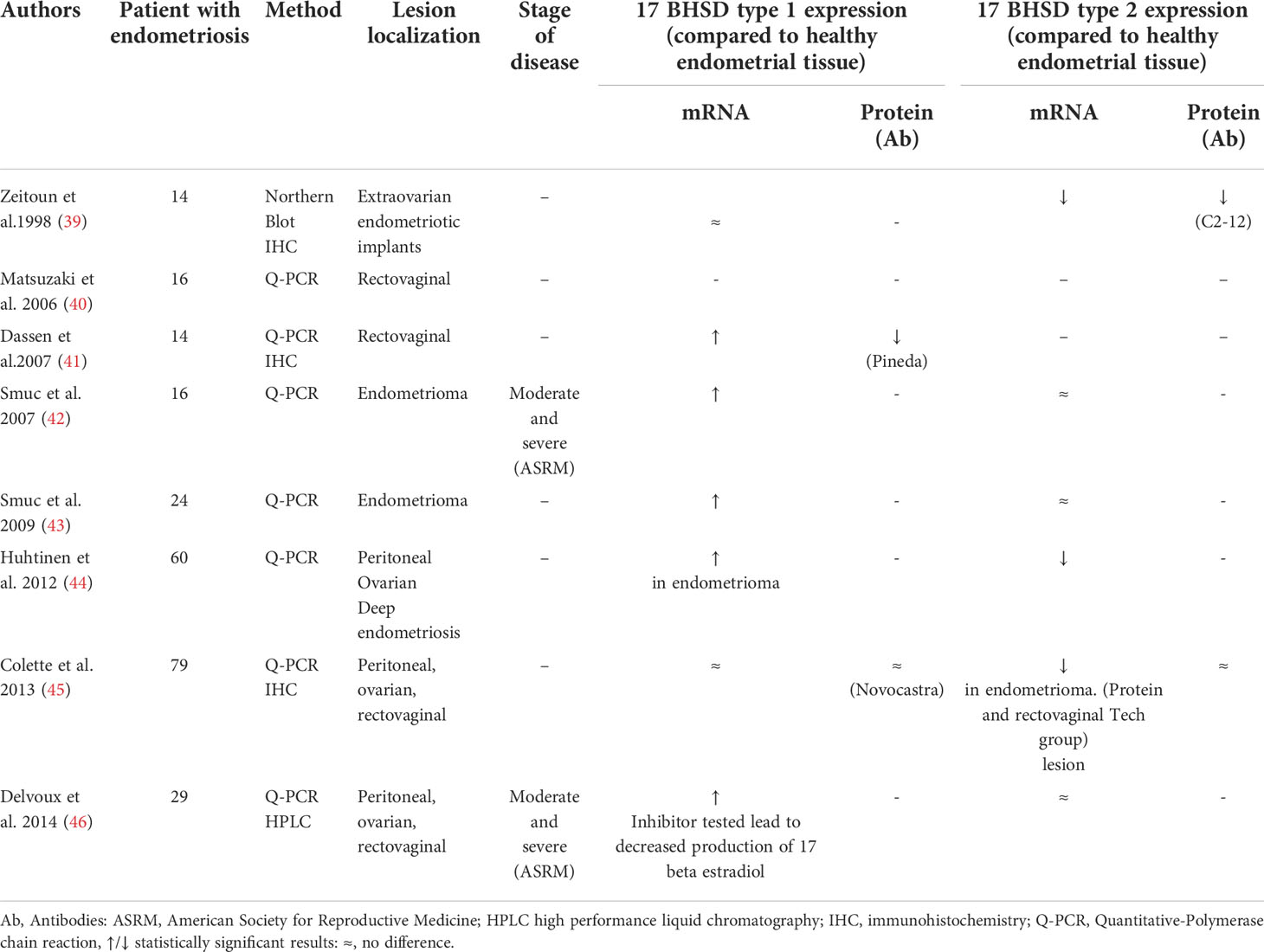
Table 4 17BHSD type 1, type 2 mRNA and protein expression in endometriotic tissue.
HSD17B2 expression on human tissue
The HSD17B2 enzyme is involved in the oxidative reaction and is responsible for the metabolization of potent E2 to the less active E1. The evaluation of HSD17B2 at the protein level is scanty and based only on two studies with conflicting results (39, 42–46), showing lower expression (39) or no changes (45) in endometriotic tissues (mixed lesions). Concerning mRNA expression, HSD17B2 appeared to be reduced in all types of endometriotic lesions compared to controls (39, 44, 46). Deep endometriosis shows undetectable levels of HSD17B2 mRNA type 2 in 50% of patients (8/16), and low levels were found in the remaining patients (40). In the study of Colette et al., where the protein level did not differ between samples, lower mRNA expression in rectovaginal and ovarian lesions but not in superficial peritoneal lesions was observed (45). Surprisingly, in endometrioma tissues evaluated by Smuc et al. (42, 43), no statistically significant difference was found with respect to healthy patients.
The heterogeneity, in terms of the method used to evaluate mRNA and protein expression, of the abovementioned studies prevent a proper comparison. Moreover, from a clinical perspective, given the lack of data regarding the stage of disease (only Delvoux et al. specified the characteristics of their patients) and the correlation with the severity of symptoms, it is difficult to estimate which patient can really benefit from future targeted enzyme therapy.
HSD17B5 expression on human tissue
Worth of mention for its ability to influence multiple signaling pathways in endometriosis is 17β-hydroxysteroid dehydrogenase type 5 (17BHSD5) also known as AKR1C3. This steroidogenic enzyme can function as a PGF2α synthases, increasing the concentration of prostaglandins in peritoneal fluid (47), and catalyze the reduction of progesterone to the less active 20α-hydroxyprogesterone, leading to a defective progesterone action and contributing to the progesterone-resistant state (48). Concerning its roles in androgen and estrogen biosynthesis it has a very high catalytic efficiency for the conversion of androstenedione to testosterone which may finally act as a substrate for aromatase, having thus an indirect role in estradiol formation (49). In term of protein levels using IHC, two studies reported, the presence of AKR1C3 in endometriomas (43) and peritoneal endometriotic lesions (50). However, when scoring of AKR1C3 staining was performed, no significant differences in endometriosis lesions (ovarian endometriomas) compared to the endometrium of control patients were revealed (47, 51). Data provided on mRNA levels in endometriotic tissue are even more discordant. In a study evaluating 24 samples of ovarian endometrioma mRNA reported a higher expression respect to controls (43), whereas in a study reporting the analysis of 31 ovarian endometrioma only a slight difference was observed (51). Furthermore no data on pain symptoms or endometriosis stage are reported, making difficult further comparison. Interesting results from a study where peritoneal endometriosis samples were classified according to menstrual cycle phase (50): increased expression of AKR1C3 was observed in women with disease stages I–II and during the proliferative phase of the menstrual cycle. However, when all type of endo are analyzed together, only minor differences of mRNA expression (44) were detected. As consequence, further evidence to confirm the clinical relevance of AKR1C3 as a target in endometriosis are then needed.
HSD17B inhibitors
Some inhibitors of HSD17B1 were developed in the past to target the biosynthesis of bioactive E2 in breast cancer (52). However, only a few compounds have been applied in vivo (53). Differences between enzymes in humans and other species are one of the main reasons that preclinical in vivo evaluation has been hindered.
A novel HSD17B1 inhibitor, FOR-6219, recently successfully completed a Phase 1a study in which the safety, tolerability, and pharmacokinetics of single and multiple ascending doses in 36 healthy postmenopausal women were investigated (NCT03709420). In Phase 1b, 36 premenopausal healthy women were investigated to expand the safety data and explore secondary outcome measures; interestingly, these women continued to experience normal ovulatory menstrual cycles (Report No.: NCT03709420. Available from: https://clinicaltrials.gov/ct2/show/NCT03709420).
Forendo Pharma is now planning a Phase 2 program including endometriosis patients in the US (available from: https://forendo.com/forendo-pharma-successfully-completes-phase-1-studies-of-for-6219-in-endometriosis-aiming-to-advance-program-into-phase-2-clinical-studies/). A steroidal inhibitor of AKR1C3, BAY1128688, was tested in a phase I clinical trial (NCT02434640) to investigate its safety, tolerability and pharmacokinetics in healthy women, and it appeared to be well tolerated up to a high dose of 60 mg twice per day. In a phase II clinical trial (NCT03373422) designed to evaluate the reduction of pain and the incidence of adverse events, it was planned to treat symptomatic women with endometriosis over a 12-week treatment period. Unfortunately, the trial was stopped in advance due to hepatotoxicity. A recent review, however, concluded that hepatotoxic effects can be compound-related, and AKR1C3 should not be precluded as a potential target (48). The development of other drugs targeting this enzyme is ongoing.
Sulfatase and sulfotransferase
Sulfatase (STS) is an enzyme involved in another critical alternative pathway that contributes to the increased bioavailability of regionally active estrogens. Hydrolysis transforms dehydroepiandrosterone sulfate (DHEA-S), estrone sulfate (E1S), the most abundant circulating estrogen metabolite, and estradiol sulfate (E2S) into their bioactive metabolites (DHEA, E1 and E2, respectively). Despite its potential pivotal roles in local estrogen formation, data on metabolic activity of this enzyme are not very conclusive. An analysis of 27 peritoneal endometriosis implants showed lower overall STS activity in ectopic endometrium than in eutopic endometrium (54). The authors attributed this to the relatively lower enzyme activity levels in endometriotic lesions from patients with minimal to mild disease, and indeed, with further analysis, they observed that STS activity in endometriosis implants correlates with the severity of this disease, and a significantly higher activity of STS was found in patients with moderate to severe disease with respect to controls, indicating that women with severe endometriosis may be particularly amenable to STS inhibitor therapy. However, Delvoux et al. did not find a difference in terms of STS enzyme activity between ectopic and eutopic endometrial tissue despite the analysis being provided in women affected by moderate to severe endometriosis from all three types of endometriosis (23).
Sulfatase expression on human tissue
To date, evidence on the expression of STS in endometriosis has remained relatively contradictory (Table 5). Only two studies evaluated STS at the protein level (41, 45), reporting no difference between cases and controls. STS mRNA expression was greater in superficial, ovarian and deep-infiltrating lesions (no significant differences were found between these two types of lesions) of endometriosis samples than in eutopic endometrium of subjects without endometriosis (43, 45, 56). Conflicting findings have been published by from Dassen et al., that, evaluated 14 women with rectovaginal endometriosis and did not observe any differences between STS mRNA levels of endometriosis and healthy tissues (P, 0.05) (41).
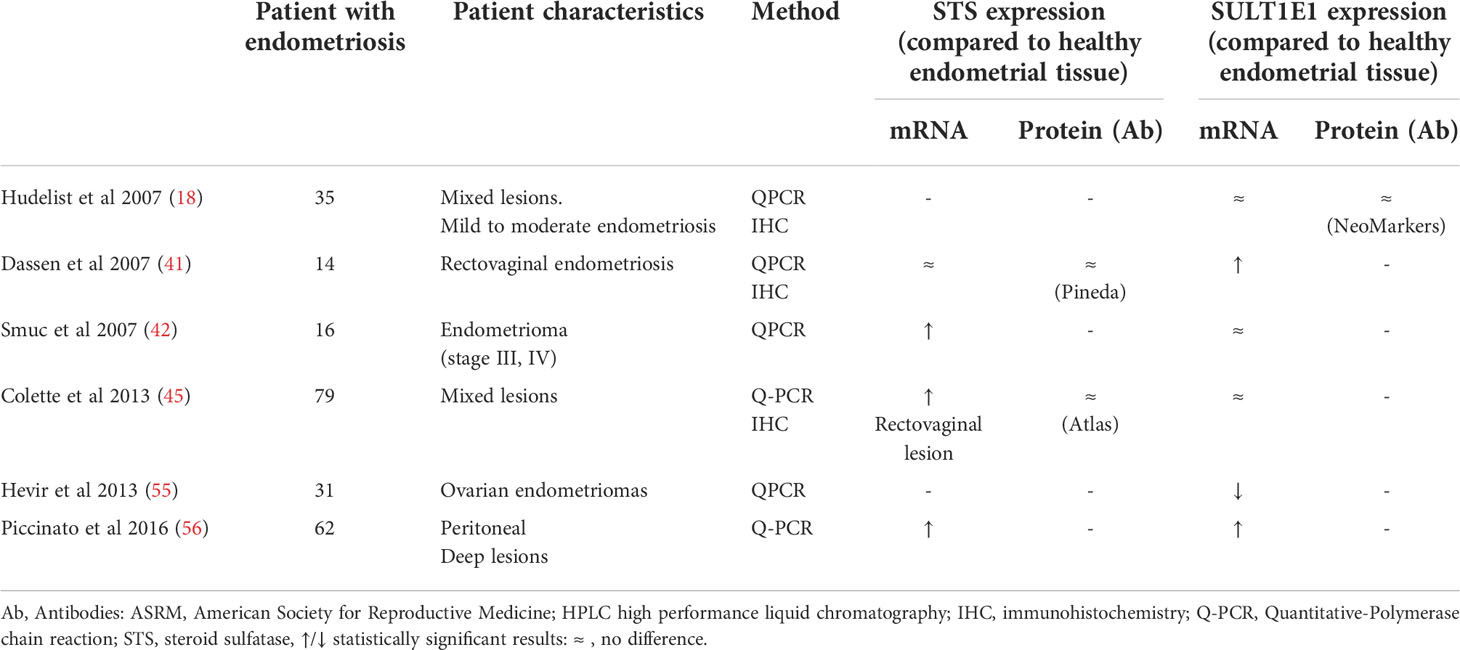
Table 5 STS and SULT1E1 mRNA, protein expression in endometriotic tissue.
Sulfotransferase expression in human tissue
Estrone sulfotransferase (SULT1E1), in contrast to STS, antagonizes the action of STS by sulfating estrone into esterone sulfate, thus converting estrogens into less active metabolites. However, the expression of this enzyme in endometriosis lesions demonstrated a contradictory pattern. The evaluation of patients with mild and moderate endometriosis shows no significant differences between the expression levels of SULT1E1 protein in uterine and ectopic samples in comparison to the endometrium of healthy women (18). In endometrioma samples, Hevir et al. found that SULT1E1 mRNA levels were significantly decreased compared to controls (55), whereas Smuc et al. registered no significant difference in its expression (42). Colette et al. showed that in rectovaginal endometriosis, although no difference was encountered in SULT1E1 mRNA expression, there was a high ratio between STS and SULT1E1, giving rise to the view that in endometriosis lesions, the sulfatase pathway is overactive (45). Interestingly, two studies reported a higher expression of SULT1E1 in endometriotic lesions than in normal endometrium: rectovaginal endometriosis lesions (41) and superficial peritoneal lesions (56) showed higher expression of EST compared to the control and had a positive correlation with STS expression. If STS abounds over SULT1E1, the increased net production of estradiol in endometriosis is the directed consequence; in this way, sufficient sulfated estrogens can be continuously hydrolyzed (desulfated) and sulfated in situ, maintaining a highly local estrogenic milieu.
Sulfatase inhibitors
Based on the aforementioned data, STS can be considered an attractive molecular target with potential therapeutic value in endometriosis, and targeting this enzyme may benefit patients with resistance to other hormonal treatments. Purohit et al. tested a recent irreversible STS inhibitor, 667COUMATE (also called Irosustat), which was already assessed in postmenopausal women with metastatic breast cancer. It proved to be very effective at inhibiting STS activity in endometriotic cell lysates, reducing enzyme activity by 99% in both eutopic and ectopic endometrial tissue samples (54). Another inhibitor, estradiol-3-O-sufamate (E2MATE), also encoding PGL2001, was proven to effectively inhibit STS activity when tested in vitro on endometrial fragments of ten patients affected by benign pathologic conditions other than endometriosis (STS activity inhibition after 24 h of culture: 66.5 + 10.3%, P, 0.001). Endometriosis was then induced in mice to evaluate the inhibition in vivo of this enzyme. After twenty-one days of therapy, lesion sizes were found to be significantly decreased (control mice: 44.5 ±30.2 mm2; 1 mg/kg-treated mice: 26.3±20.1 mm2; 0.5 mg/kg treated mice: 22.8±15.3 mm2) (57). As an additional benefit, progesterone (PR) expression in endometriotic lesions was found to be increased, and the absence of an effect on circulating estradiol levels opens up new perspectives in endometriosis treatment. E2MATE was then evaluated in a phase I double-blind study (58).Given that the majority of estrogens are produced in the ovaries, the authors focused their evaluation on a combination STS-I plus progestin in order to reduce both the local and ovarian estrogen production. Twenty-four healthy volunteer women were randomized to E2MATE (4 mg/week), NETA or the combination E2MATE+NETA. Treatment lasted 4 weeks with a 12-week follow-up. E2MATE associated with NETA showed a synergistic effect: the mean percentage of STS inhibition in the endometrium was 91% and 96% in the PGL2001 and PGL2001 plus NETA groups, respectively, compared to 42% in the NETA group, and due to its potent irreversible binding and long half-life one month after stopping treatment, the percentage inhibition remained high at 88% and 93% in the PGL2001 and PGL2001 plus NETA groups, respectively, with no inhibition seen in the NETA group. Treatment was well tolerated, with no relevant differences between the treatment regimens in terms of adverse events, and no impact on circulating estradiol levels was registered compared to the NETA groups. E2MATE and NETA have been further studied in endometriosis patients in a phase II study (NCT01631981, available at: https://clinicaltrials.gov/ct2/show/NCT01631981), although at present, no results are publicly available. An interesting recent development is the establishment of multiple designed ligands that effectively inhibit both STS and HSD17B1 (59).Such dual inhibitors can further decrease intracellular E2 levels more efficiently than selective inhibitors of HSD17B1 and may therefore be a superior therapeutic strategy for endometriosis.
Effect of current hormonal treatments on intracrinology regulation
Current first-line hormonal treatments in endometriosis (oral contraceptives and progestins) were originally developed using the normal endometrium as the main experimental tissue to investigate their reproductive effects and were adopted only afterwards for the treatment of endometriosis-associated pain. There are several patients for whom current first-line hormonal treatments for endometriosis do not provide enough or a sustained solution to pain. A recent review demonstrated that the median proportion of women with no decrease in pain was 11% to 19%; when the therapy ended, 5% to 59% had persistent pain; and in the follow-up, 17% to 34% felt recurrence of pain symptoms (60). The recent evidence that women, despite the hypogonatrophic effect obtained from combined oral contraceptives (COCs), have increased hormone levels in endometriosis implants compared to controls (61) highlights the crucial role of intracrinology as a mechanism of endometriosis development and drug resistance. There are only a few available research studies that have investigated the influence of the commonly used therapy against the enzymes involved in the intracrinology of the endometriosis. Few are based on progestins, and no research studies have investigated the effects of COC. Most studies, in addition, have been conducted in vitro using immortalized cells, limiting a realistic interpretation of the results. Dienogest (DNG), a synthetic progestin largely employed for therapy, has received the greatest attention. DNG has been shown to repress aromatase expression in human immortalized endometrial epithelial cells and primary cultured endometriotic stromal cells (SCs) (62, 63). Moreover, DNG has been shown to inhibit HSD17B1 expression and enzymes in cultured ovarian endometrioma cells, whereas no effect has been demonstrated on HSD17B2, HSD17B7, HSD17B12, steroid sulfatase (STS), and estrogen sulfotransferase (EST) activity (64). There are few details with respect to GnRH agonist and antagonist effects on endometrial intracrinology. While GnRH agonists have been shown to decrease serum E2 levels by approximately 97%, intracrinological changes in endometriosis lesions are not known. Even if GnRH agonists are responsible for decreasing tissue inflammation and angiogenesis and increasing apoptosis in endometriosis (65), 14% (0-20%) of patients did not show improvement of symptoms, and nearly one-third of patients who received GnRH analog treatment postsurgery experienced pain symptoms when medical treatment ended (60). Interestingly, one-year therapy with a GnRH analog decreases the adrenal DHEA-S combination by only 16%, leaving open the possibility of its metabolism in peripheral tissue and eventually inducing resistance to treatments (66). GnRH agonists have been shown to reduce aromatase cytochrome P450 expression in at least eutopic endometrium from patients with endometriosis (67) and hinder E1 sulfatase expression in endometrioma (68). Recently, GnRH antagonists have been augmented in the armamentarium of gynecologists to cure endometriosis and resolve the side effects of GnRH agonists based on the “estrogen threshold hypothesis,” where estrogen may be regulated to a level that is enough to reduce pain without causing clinical hypoestrogenic effects. Elagolix did not fully repress ovulation at doses of 150 and 200 mg/day, 56% of women had proliferative endometrium after 6 months of therapy at a dose of 150 mg, and 61% had normal dormant or least stimulated endometrium at a dose of 200 mg. Even if the majority of patients were satisfied with this therapy, as many as 40% of patients indicated unsatisfactory improvement of pain symptoms (69). On the basis of the complexity of the intracrinology of endometriosis and the fact that GnRH antagonists have no direct effect on the endometrium, we can then hypothesize that the intracrine features of endometriosis may represent a mechanism creating an incomplete response to symptoms of pain in 30-35% of patients
Discussion
The study of intracrinology in endometriosis highlights important limitations in the current knowledge of the disease, from its developmental and initial phases to the macroscopic appearance of advanced deep nodules. It is clear that the current macroscopic classification is insufficient to properly characterize heterogeneous lesions. A closer look at endocrine aspects of lesions may shed new light on disease features, enabling precision medicine in endometriosis care. However, current methodological limitations (i.e., number of patients enrolled in the studies) or appropriateness of investigations (i.e., contamination of endometrioma cysts with ovarian cortex) has limited the implementation of endocrine phenotyping in daily practice. Furthermore, the accurate evaluation of the expression of these enzymes is a complex task; for instance, concerning aromatase protein expression, some authors argued that what was believed to be aromatase protein in a previous study was mainly endogenous biotic labeling or iron deposits (20). Even if various enzymatic pathways are aberrantly regulated in endometriosis, the recognition of which enzymatic pathways are more critical for promoting the hyperestrogenic environment is less clear. This is important for the development of new drugs aimed at decreasing local estrogenic activity with a minimal effect on gonadal activity.
Strengths and limitations
The strength of this review lies in the evaluation of intracrinology of endometriosis from a clinical prospective. The main limitation was that heterogeneity of the studies included and a lack a particular model to investigate the role of local modulation of these enzymatic pathways.
Conclusion and new perspectives
Unbalanced intracrinology is a critical feature of endometriosis implants and a complex mechanism that supports local hyperestrogenism partially independent from gonadal function. This has far-reaching implications in clinical practice, since all available therapies induce a reduction in gonadal activity as main mechanism of action. Recently, the development of harmonization initiatives, such as EPHect, Endometriosis Phenome and Biobanking Harmonisation Project, has represented a new systematic approach to stratify predefined outcomes in endometriosis research with family history, symptoms, clinical examination, dynamic imaging/pain reporting, surgical staging, and systemic or tissue biomarkers. From a clinical perspective, current knowledge of intracrinology in endometriosis in the actual classification of the disease has identified that endometriosis lesions on the ovary are likely the most endocrine active and responsive to steroids. As a result, they are characterized by a higher incidence of recurrence following surgical excision. In addition, enzymatic pathways expressed in endometriosis are likely consequences of epigenetic changes and inflammation signals. Again, a closer look at intracrinology could facilitate lesion phenotyping and estimate the aggressiveness of the disease. However, current methodological limitations and heterogeneity in the evaluation of mRNA and protein expression make it hard to draw definitive conclusions. In certain cases, contradictory results can be explained by the close proximity of healthy tissue to the endometriotic lesion, influencing the results obtained by the whole tissue specimens and highlighting the need for a careful histopathological characterization of the specimens studied (laser capture microdissection may therefore be envisaged to fully isolate endometriotic glands). Moreover, a large number of studies miss correlations with the severity of symptoms, stage and localization of disease, making it difficult to estimate which patient can benefit the best from future targeted enzyme therapy. Although AIs are not realistically useful in clinical practice, intracrinology offers interesting new drug targets that can incorporate many of the above ambitious features. Some molecules are already in the pipeline of the pharma industry in the next 10 years. In conclusion, intracrinology of endometriosis is relevant in clinical practice as a major main endometriosis developmental feature, a basis for phonotypical characterization, a potential mechanism of drug resistance and a source of new therapeutic targets.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
AM and NP undertook the searches, data extraction and drafted the manuscript. NP, AM, PG, PD, and AR participated in data analysis and interpretation, preparation of. the manuscript and critically revising the paper. NP and AR conceived the idea of the manuscript. All authors approved the final version of the manuscript.
Funding
Open access funding was provided by the University of Geneva.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zhang Y, Ma NY. Environmental risk factors for endometriosis: An umbrella review of a meta-analysis of 354 observational studies with over 5 million populations. Front Med (Lausanne). (2021) 8:680833. doi: 10.3389/fmed.2021.680833
2. Zondervan KT, Becker CM, Koga K, Missmer SA, Taylor RN, Vigano P. Endometriosis. Nat Rev Dis Primers. (2018) 4(1):9. doi: 10.1038/s41572-018-0008-5
3. Vercellini P, Vigano P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol (2014) 10(5):261–75. doi: 10.1038/nrendo.2013.255
4. Chantalat E, Valera MC, Vaysse C, Noirrit E, Rusidze M, Weyl A, et al. Estrogen receptors and endometriosis. Int J Mol Sci (2020) 21(8):2815. doi: 10.3390/ijms21082815
6. Pluchino N, Mamillapalli R, Wenger JM, Ramyead L, Drakopoulos P, Tille JC, et al. Estrogen receptor-α immunoreactivity predicts symptom severity and pain recurrence in deep endometriosis. Fertil Steril. (2020) 113(6):1224–31. doi: 10.1016/j.fertnstert.2020.01.036
7. Colgrave EM, Bittinger S, Healey M, Dior UP, Rogers PAW, Keast JR, et al. Superficial peritoneal endometriotic lesions are histologically diverse and rarely demonstrate menstrual cycle synchronicity with matched eutopic endometrium. Hum Reprod (2020) 3512:2701–14. doi: 10.1093/humrep/deaa249
8. Labrie F. Intracrinology. Mol Cell Endocrinol (1991) 78(3):C113–8. doi: 10.1016/0303-7207(91)90116-A
9. Pluchino N, Drakopoulos P, Bianchi-Demicheli F, Wenger JM, Petignat P, Genazzani AR. Neurobiology of DHEA and effects on sexuality, mood and cognition. J Steroid Biochem Mol Biol (2015) 145:273–80. doi: 10.1016/j.jsbmb.2014.04.012
10. Labrie F. Intracrinology and menopause: the science describing the cell-specific intracellular formation of estrogens and androgens from DHEA and their strictly local action and inactivation in peripheral tissues. Menopause (New York NY) (2019) 26(2):220–24. doi: 10.1097/GME.0000000000001177
11. L Gibson DA, Simitsidellis I, Collins F, Saunders PTK. Endometrial intracrinology: Oestrogens, androgens and endometrial disorders. Int J Mol Sci (2018) 19:3276. doi: 10.3390/ijms19103276
12. Cornel KMC, MY B, Kruitwagen RPFM, Romano A. Local estrogen metabolism (intracrinology) in endometrial cancer: A systematic review. Mol Cell Endocrinol (2019) 489:45–65. doi: 10.1016/j.mce.2018.10.004
13. Konings G, Brentjens L, Delvoux B, Linnanen T, Cornel K, Koskimies P, et al. Intracrine regulation of estrogen and other sex steroid levels in endometrium and non-gynecological tissues; pathology, physiology, and drug discovery. Front Pharmacol (2018) 9:940. doi: 10.3389/fphar.2018.00940
14. Noble LS, Takayama K, Zeitoun KM, Putman JM, Johns DA, Hinshelwood MM, et al. Bulun, prostaglandin E2 stimulates aromatase expression in endometriosis-derived stromal cells. J Clin Endocrinol Metab (1997) 822:600–6. doi: 10.1210/jcem.82.2.3783
15. Noble LS, Takayama K, Zeitoun KM, Putman JM, Johns DA, Hinshel- wood MM, et al. Prostaglandin E2 stimulates aromatase expression in endometriosis-derived stromal cells. J Clin Endocrinol Metab (1997) 82:600–6. doi: 10.1210/jc.82.2.600
16. Attar E, Bulun SE. Aromatase and other steroidogenic genes in endometriosis: translational aspects. Hum Reprod (2006) 12:49–56. doi: 10.1093/humupd/dmi034
17. Buccitelli C, Selbach M. mRNAs, proteins and the emerging principles of gene expression control. Nat Rev Genet (2020) 21:630–44. doi: 10.1038/s41576-020-0258-4
18. Hudelist G, Czerwenka K, Keckstein J, Haas C, Fink-Retter A, Gschwantler-Kaulich D, et al. Expression of aromatase and estrogen sulfotransferase in eutopic and ectopic endometrium: evidence for unbalanced estradiol production in endometriosis. Reprod Sci (2007) 14(8):798–805. doi: 10.1177/1933719107309120
19. Acién P, Velasco I, Gutiérrez M, Martínez-Beltrán M. Aromatase expression in endometriotic tissues and its relationship to clinical and analytical findings. Fertil Steril (2007) 88(1):32–8. doi: 10.1016/j.fertnstert.2006.11.188
20. Colette S, Lousse JC, Defrère S, Curaba M, Heilier JF, Van Langendonckt A, et al. Absence of aromatase protein and mRNA expression in endometriosis. Hum Reprod (2009) 24(9):2133–41. doi: 10.1093/humrep/dep199
21. Maia H Jr, Haddad C, Casoy J. Correlation between aromatase expression in the eutopic endometrium of symptomatic patients and the presence of endometriosis. Int J Womens Health (2012) 4:61–5. doi: 10.2147/IJWH.S29154
22. Koninckx PR, Ussia A, Adamyan L, Gomel V, Martin DC. Peritoneal fluid progesterone and progesterone resistance in superficial endometriosis lesions. Hum Reprod (2022) 37(2):203–11. doi: 10.1093/humrep/deab258
23. Delvoux B, Groothuis P, D'Hooghe T, Kyama C, Dunselman G, Romano A. Increased production of 17beta-estradiol in endometriosis lesions is the result of impaired metabolism. J Clin Endocrinol Metab (2009) 94(3):876–83. doi: 10.1210/jc.2008-2218
24. Takayama K, Zeitoun K, Gunby RT, Sasano H, Carr BR, Bulun SE. Treatment of severe postmenopausal endometriosis with an aromatase inhibitor. Fertil Steril. (1998) 69(4):709–13. doi: 10.1016/S0015-0282(98)00022-3
25. Pavone ME, Bulun SE. Aromatase inhibitors for the treat- ment of endometriosis [Review]. Fertil Steril. (2012) 98(6):1370–9. doi: 10.1016/j.fertnstert.2012.08.053
26. Soysal S, Soysal ME, Ozer S, Gul N. Gezgin T: The effects of post-surgicaladministration of goserelin plus anastrozole compared to goserelin alone in patients with severe endometriosis: a prospective randomized trial. Hum Reprod (2004) 19:160–7. doi: 10.1093/humrep/deh035
27. Ferrero S, Camerini G, Seracchioli R, Ragni N, Venturini PL, Remorgida V. Letrozole combined with norethisterone acetate compared with norethisterone acetate alone in the treatment of pain symptoms caused by endometriosis. Hum Reprod (2009) 2412:3033–41. doi: 10.1093/humrep/dep302
28. Roghaei MA, Tehrany HG, Taherian A, Koleini N. Effects of letrozole compared with danazol on patients with confirmed endometriosis: A randomized clinical trial. IJFS (2010) 4:67–72. Available at: https://www.sid.ir/en/journal/viewpaper.aspx?id=176450
29. Alborzi S, Hamedi B, Omidvar A, Dehbashi S, Alborzi S, Alborzi M. A comparison of the effect of short-term aromatase inhibitor (letrozole) and GnRH agonist (triptorelin) versus case control on pregnancy rate and symptom and sign recurrence after laparoscopic treatment of endometriosis. Arch Gynecol Obstet (2011) 284(1):105–10. doi: 10.1007/s00404-010-1599-6
30. Ferrero S, Venturini PL, Gillott DJ, Remorgida V. Letrozole and norethisterone acetate versus letrozole and triptorelin in the treatment of endometriosis related pain symptoms: a randomized controlled trial. Reprod Biol Endocrinol (2011) 9:88. doi: 10.1186/1477-7827-9-88
31. Ferrero S, Leone Roberti Maggiore U, Scala C, Di Luca M, PL V, Remorgida V. Changes in the size of rectovaginal endometriotic nodules infiltrating the rectum during hormonal therapies. Arch Gynecol Obstet. (2013) 287(3):447–53. doi: 10.1007/s00404-012-2581-2
32. Ferrero S, Remorgida V, Venturini PL, Leone Roberti Maggiore U, et al. Norethisterone acetate versus norethisterone acetatecombined with letrozole for the treatment of ovarian endometriotic cysts: a patient preference study. Eur JObstet Gynecol Reprod Biol (2014) 174:117–22. doi: 10.1016/j.ejogrb.2013.11.030
33. Dunselman GA, Vermeulen N, Becker C, Calhaz-Jorge C, D'Hooghe T, De Bie B, et al. European Society of human reproduction and embryology. ESHRE guideline: management of women with endometriosis. Hum Reprod (2014) 29(3):400–12. doi: 10.1093/humrep/det457
34. Hussain A, Ahsan F. The vagina as a route for systemic drug delivery. J Control Release (2005) 103(2):301–13. doi: 10.1016/j.jconrel.2004.11.034
35. Schultze-Mosgau MH, Waellnitz K, Nave R, Klein S, Kraetzschmar J, Rautenberg T, et al. Pharmacokinetics, pharmacodynamics, safety and tolerability of an intravaginal ring releasing anastrozole and levonorgestrel in healthy premenopausal women: a phase 1 randomized controlled trial. Hum Reprod (2016) 318:1713–22. doi: 10.1093/humrep/dew145
36. Nave R, Mellinger U, Klein S, Höchel J, Schmitz H., et al. Absence of drug-drug-interaction of anastrozole on levonorgestrel delivered simultaneously by an intravaginal ring: results of a phase 2 trial. J Clin Pharmacol (2019) 59(7):1022–8. doi: 10.1002/jcph.1396
37. Hefler LA, Grimm C, van Trotsenburg M, Nagele F. Role of the vaginally administered aromatase inhibitor anastrozole in women with rectovaginal endometriosis: a pilot study. Fertil Steril. (2005) 84(4):1033–6. doi: 10.1016/j.fertnstert.2005.04.059
38. Pluchino N, Poppi G, Yart L, Marci R, Wenger JM, Tille JC, et al. Effect of local aromatase inhibition in endometriosis using a new chick embryo chorioallantoic membrane model. J Cell Mol Med (2019) 23(8):5808–12. doi: 10.1111/jcmm.14372
39. Zeitoun K, Takayama K, Sasano H, Suzuki T, Moghrabi N, Andersson S. Deficient 17-hydroxysteroid dehydrogenase type 2 expression in endometriosis: failure to metabolize 17-estradiol. J Clin Endocrinol Metab (1998) 83:4474–80. doi: 10.1210/jc.83.12.4474
40. Matsuzaki S, Canis M, Pouly JL, Dechelotte PJ, Mage G. Analysis of aro-matase and 17-hydroxysteroid dehydroganse type 2 messenger ribonucleicacid expression in deep endometriosis and eutopic endometrium using lasercapture microdissection. Fertil Steril (2006) 85:308–13. doi: 10.1016/j.fertnstert.2005.08.017
41. Dassen H, Pundayeera C, Kamps R, Delvoux B, Van Langendonckt A, Donnez J, et al. Estrogen metabolizingenzymes in endometrium and endometriosis. Hum Reprod (2007) 22:3148–58. doi: 10.1093/humrep/dem310
42. Smuc T, Pucelj MR, Sinkovec J, Husen B, Thole H, Lanisnik Rizner T. Expression analysis of the genes involved in estradiol and progesterone action in human ovarian endometriosis. Gynecol Endocrinol (2007) 23(2):105–11. doi: 10.1080/09513590601152219
43. Smuc T, Hevir N, Ribic-Pucelj M, Husen B, Thole H, Rizner TL. Disturbed estrogen and progesterone action in ovarian endometriosis. Mol Cell Endocrinol (2009) 301(1-2):59–64. doi: 10.1016/j.mce.2008.07.020
44. Huhtinen K, Desai R, Ståhle M, Salminen A, Handelsman DJ, Perheentupa A, et al. Endometrial and endometriotic concentrations of estrone and estradiol are determined by local metabolism rather than circulating levels. J Clin Endocrinol Metab (2012) 97(11):4228–35. doi: 10.1210/jc.2012-1154
45. Colette S, Defrère S, Van Kerk O, Van Langendonckt A, Dolmans MM, Donnez J. Differential expression of steroidogenic enzymes according to endometriosis type. Fertil Steril. (2013) 100(6):1642–9. doi: 10.1016/j.fertnstert.2013.08.003
46. Delvoux B, D'Hooghe T, Kyama C, Koskimies P, RJ H, GA D, et al. Inhibition of type 1 17beta-hydroxysteroid dehydrogenase impairs the synthesis of 17beta-estradiol in endometriosis lesions. J Clin Endocrinol Metab (2014) 99(1):276–84. doi: 10.1210/jc.2013-2851
47. Sinreih M, Anko M, Kene NH, Kocbek V, Rižner TL. Expression of AKR1B1, AKR1C3 and other genes of prostaglandin F2α biosynthesis and action in ovarian endometriosis tissue and in model cell lines, chem. Biol Interact (2015) 234:320–31. doi: 10.1016/j.cbi.2014.11.009
48. Rižner TL, Penning TM. Aldo-keto reductase 1C3-assessment as a new target for the treatment of endometriosis. Pharmacol Res (2020) 152:104446. doi: 10.1016/j.phrs.2019.104446
49. Sharma KK, Lindqvist A, Zhou XJ, Auchus RJ, Penning TM, Andersson S. Deoxycorticosterone inactivation by AKR1C3 in human mineralocorticoid target tissues, mol. Cell Endocrinol (2006) 248(1-2):79–86. doi: 10.1016/j.mce.2005.10.024
50. Rakhila H, Carli C, Daris M, Lemyre M, Leboeuf M, Akoum A. Identification of multiple and distinct defects in prostaglandin biosynthetic pathways in eutopic and ectopic endometrium of women with endometriosis, fertil. Steril (2013) 100(6):1650–9. doi: 10.1016/j.fertnstert.2013.08.016
51. Hevir N, Vouk K, Sinkovec J, Ribič-Pucelj M, Rižner TL. Aldo-keto reductases AKR1C1, AKR1C2 and AKR1C3 may enhance progesterone metabolism in ovarian endometriosis, chem. Biol Interact (2011) 191(1-3):217–26. doi: 10.1016/j.cbi.2011.01.003
52. Poirier D. Contribution to the development of inhibitors of 17β-hydroxysteroid dehydrogenase types 1 and 7: key tools for studying and treating estrogen-dependent diseases. J Steroid Biochem Mol Biol (2011) 125(1-2):83–94. doi: 10.1016/j.jsbmb.2010.12.007
53. Day JM, Tutill HJ, Purohit A, Reed MJ. Design and validation of specific inhibitors of 17-hydroxysteroid dehydrogenases for therapeutic application in breast and prostate cancer, and in endometriosis. Endocr Relat Cancer. (2008) 15:665–92. doi: 10.1677/ERC-08-0042
54. Purohit A, Fusi L, Brosens J, Woo LWL, Potter BVL, MJ R. Inhibition of steroid sulphatase activity in endometriotic implants by 667 COUMATE: a potential new therapy. Hum Reprod (2008) 232:290–7. doi: 10.1093/humrep/dem308
55. Hevir N, Ribič-Pucelj M, Lanišnik Rižner T. Disturbed balance between phase I and II metabolizing enzymes in ovarian endometriosis: a source of excessive hydroxy-estrogens and ROS? Mol Cell Endocrinol (2013) 367(1-2):74–84. doi: 10.1016/j.mce.2012.12.019
56. Piccinato CA, Neme RM, Torres N, Sanches LR, Derogis P, Brudniewski HF, et al. Effects of steroid hormone on estrogen sulfotransferase and on steroid sulfatase expression in endometriosis tissue and stromal cells. J Steroid Biochem Mol Biol (2016) 158:117–26. doi: 10.1016/j.jsbmb.2015.12.025
57. Colette S, Defrere S, Lousse JC, Van Langendonckt A, Gotteland JP, Loumaye E, et al. Inhibition of steroid sulfatase decreases endometriosis in an in vivo murine model. Hum Reprod (2011) 26:1362–70. doi: 10.1093/humrep/der079
58. Pohl O, Bestel E, Gotteland JP. Synergistic effects of E2MATE and norethindrone acetate on steroid sulfatase inhibition: a randomized phase I proof-of-principle clinical study in women of reproductive age. Reprod Sci (2014) 21(10):1256–65. doi: 10.1177/1933719114522526
59. Salah M, Abdelsamie AS, Frotscher M. First dual inhibitors of steroid sulfatase (STS) and 17β-hydroxysteroid dehydrogenase type 1 (17β-HSD1): Designed multiple ligands as novel potential therapeutics for estrogen-dependent diseases. J Med Chem (2017) 60(9):4086–92. doi: 10.1021/acs.jmedchem.7b00062
60. Becker CM, Gattrell WT, Gude K, Singh SS. Reevaluating response and failure of medical treatment of endometriosis: a systematic review. Fertility Sterility (2017) 108(1):125–36. doi: 10.1016/j.fertnstert.2017.05.004
61. Attar E, Bulun SE. Aromatase and other steroidogenic genes in endometriosis: translational aspects. Hum Reprod (2006) 12:49–56. doi: 10.1093/humupd/dmi034
62. Yamanaka K, Xu B, Suganuma I, Kusuki I, Mita S, Shimizu Y, et al. Dienogest inhibits aromatase and cyclooxygenase-2 expression and prostaglandin E2 productionin human endometriotic stromal cells in spheroid culture. Fertility Sterility (2012) 97:477–82. doi: 10.1016/j.fertnstert.2011.11.005
63. Shimizu Y, Mita S, Takeuchi T, Notsu T, Mizuguchi K, Kyo S. Dienogest, a synthetic progestin, inhibits prostaglandin E2 production and aromatase expression by human endometrial epithelial cells in a spheroid culture system. Steroids (2011) 76(1-2):60–7. doi: 10.1016/j.steroids.2010.08.010
64. Mori T, Ito F, Matsushima H, Takaoka O, Koshiba A, Tanaka Y, et al. Dienogest reduces HSD17beta1 expression and activity in endometriosis. J Endocrinol (2015) 225(2):69–76. doi: 10.1530/JOE-15-0052
65. Khan KN, Kitajima M, Hiraki K, Fujishita A, Sekine I, Ishimaru T, et al. Changes in tissue inflammation, angiogenesis and apoptosis in endometriosis, adenomyosis and uterine myoma after GnRH agonist therapy. Hum Reprod (2010) 25(3):642–53. doi: 10.1093/humrep/dep437
66. Miyazawa Y, Sekine Y, Syuto T, Nomura M, Koike H, Matsui H, et al. A gonadotropin-releasing hormone antagonist reduces serum adrenal androgen levels in prostate cancer patients. BMC Urol (2017) 17(1):70. doi: 10.1186/s12894-017-0261-z
67. Ishihara H, Kitawaki J, Kado N, Koshiba H, Fushiki S, Honjo H. Gonadotropin-releasing hormone agonist and danazol normalize aromatase cytochrome P450 expression in eutopic endometrium from women with endometriosis, adenomyosis, or leiomyomas. Fertil Steril (2003) 79 Suppl 1:735–42. doi: 10.1016/S0015-0282(02)04813-6
68. Maitoko K, Sasaki H. Gonadotropin-releasing hormone agonist inhibits estrone sulfatase expression of cystic endometriosis in the ovary. Fertil Steril. (2004) 82(2):322–6. doi: 10.1016/j.fertnstert.2003.12.044
Keywords: endometriosis, estrogen, metabolism, pelvic pain, endometrium
Citation: Mercorio A, Giampaolino P, Romano A, Dällenbach P and Pluchino N (2022) Is intracrinology of endometriosis relevant in clinical practice? A systematic review on estrogen metabolism. Front. Endocrinol. 13:950866. doi: 10.3389/fendo.2022.950866
Received: 23 May 2022; Accepted: 24 August 2022;
Published: 20 September 2022.
Edited by:
Mainak Dutta, Birla Institute of Technology and Science, United Arab EmiratesReviewed by:
Philippa Saunders, University of Edinburgh, United KingdomArnab Banerjee, Birla Institute of Technology and Science, India
Koninckx R. Philippe, KU Leuven, Belgium
Copyright © 2022 Mercorio, Giampaolino, Romano, Dällenbach and Pluchino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicola Pluchino, Tmljb2xhLlBsdWNoaW5vQGhjdWdlLmNo