 Samuel Linière1
Samuel Linière1 Mathieu Nacher2
Mathieu Nacher2 Kinan Drak Alsibai3Mayka Mergeayfabre2Nezha Hafsi4
Kinan Drak Alsibai3Mayka Mergeayfabre2Nezha Hafsi4 Aurelie Charpin2Caroline Misslin-Tritsch5Jean-François Carod6Jean Markens Aurelus4
Aurelie Charpin2Caroline Misslin-Tritsch5Jean-François Carod6Jean Markens Aurelus4 Bertrand De Toffol7André Ntoutoum4
Bertrand De Toffol7André Ntoutoum4 John Bukasa Kakamba4
John Bukasa Kakamba4 Magalie Demar8,9Jeannie Helene-Pelage10
Magalie Demar8,9Jeannie Helene-Pelage10 Antoine Adenis2
Antoine Adenis2 Nadia Sabbah2,4*
Nadia Sabbah2,4*- 1Department of General Medicine, Cayenne Hospital Center, Cayenne, French Guiana
- 2Clinical Investigation Center Antilles French Guiana (CIC INSERM 1424) Cayenne Hospital Center, Cayenne, French Guiana
- 3Department of Pathology and Center of Biological Resources (CRB Amazonie), Cayenne Hospital Center, Cayenne, French Guiana
- 4Department of Endocrinology and Metabolic Diseases, Cayenne Hospital Center, Cayenne, French Guiana
- 5Department of General Medicine, Ouest Guyanais Hospital Center, Saint-Laurent, French Guiana
- 6Laboratory of Biology, Ouest, Guyanais Hospital Center, Saint Laurent, French Guiana
- 7Department of Neurology, Cayenne Hospital Center, Cayenne, French Guiana
- 8Laboratory of Parasitology-Mycology (LHUPM), Cayenne Hospital Center, Cayenne, French Guiana
- 9EA3593, Amazon Ecosystems and Tropical Diseases, University of Guiana, Cayenne, French Guiana
- 10Department of General Medicine, University of the French West Indies and Guiana, Pointe-à-Pitre, Guadeloupe
Aims: The social parameters of an individual impact the incidence of cardiovascular diseases. French Guiana, an overseas French territory with a lower standard of living than France, has a prevalence of diabetes mellitus that is twice that of mainland France. In this context we aimed to study the relation between precariousness, diabetes complications and glycemic control.
Methods: A multicenter prospective cohort was initiated since May 2019. 1243 patients were included and their outcomes and history were compared between the precarious and non-precarious based on their EPICES score, a score that measures social isolation and precariousness.
Results: 73.3% of the sample was considered precarious. Retinopathy was significantly more frequent among the deprived. There were no significant differences for other macro or microvascular complications.There was a significant difference in Glycated Haemoglobin between the precarious and non-precarious groups (8.3% (67 mmol/l) vs 8.8% (73mmol/l)). After adjusting for potential confounders, precariousness was no longer associated with poor glycemic control; the independent factors significantly associated with poor glycemic control were: not being fluent in French, having creole or portugese as mother language, and not having any insurance.
Conclusions: Precariousness is a risk factor for retinal complications in patients with diabetes mellitus in French Guiana. In this chronic disease, the universal healthcare system alleviates health inequalities for many, but not all, diabetic complications.Translation and cultural mediation may further reduce health inequalities in this multicultural territory where a substantial proportion of the population is not fluent in French.
Introduction
The relationship between health and an individual’s social parameters has received renewed attention in recent years. In 2012, the World Health Organization’s regional council for Europe included in its “Health 2020” project the reduction of social inequalities in health as the main strategic and political objective (1). France is one of the Western European countries where social inequalities in health are the highest despite an improvement in the average standard of living (2).
It is now widely demonstrated that material and social deprivation in the general population is inversely related to health status (3). Indeed, in socially deprived populations, there is an increase in mortality (4). Thisis largely linked to an increase in the incidence of cancers (5)cardio vascular diseases and their risk factors (6).
Diabetes, which is increasing in incidence (7), is one of the major cardiovascular risk factors. Several publications describe the influence of social class on the mortality rate of diabetes (8) has a direct consequence of poor glycemic control and increased complications in vulnerable population (9).
To highlight these causal relationships, several indicators have been proposed to represent socio-economic status (10), the socio-occupational category (4), income (6) or the level of education (9). However, these inequality indicators do not assess the socio-economic status of an individual in all its dimensions (11). To define more precisely the link between the social parameters of an individual and his health, the concept of precariousness, defined in 1987 by Joseph Wresinski, seems to be more appropriate (12). This global dimension is similar to that used in the Anglo-Saxon literature by Peter Townsend in his terms of « material and social deprivation » (13).French Guiana is an overseas territory located at more than 7090Km from mainland France, it is one of the largest French territories with 90% of its 84000km2 covered by primary Amazonian forest. Remote populations are isolated because the road infrastructure is poor and means of transportation are rare. The population includes more than thirty ethnic groups and is culturally diverse. With the highest GDP per capita in Latin America it attracts numerous immigrants, notably from northern Brazil, Suriname, Guyana, and Haiti. Overall, 29% of the population is of foreign origin, and for adults it is nearly half of the population. The health system is that of France with universal health coverage, notably allowing the poorest to receive free health care, including undocumented immigrants.
All social indicators show that the standard of living in the overseas territories, and in particular in French Guiana, is lower than in mainland France (14).For example, the unemployment rate in French Guiana was 16.1% in 2020 compared to 7.8% in mainland France and the poverty level was 53% compared to 14% (14). At the same time, in these territories, there is a higher prevalence of cardiovascular disease (15) and diabetes (16).
Glycemic control of the patient with diabetes is key to prevent the risk of complications (17). However, few studies have simultaneously evaluated the link between precariousness, diabetes complications and glycemic control of the patient with diabetes and none has yet been conducted in the overseas French territories, which combine poor populations and a French health system. The main objective of the study was to evaluate the influence of precariousness on the complications of diabetes and on glycemic control.
Materials and Methods
The CODIAM cohort (Cohort of Diabetes in French Amazonia) is a prospective cohort study conducted in French Guiana since May 2019 describing the epidemiological, clinical and biological aspects of different types of diabetes. It is a multicenter study conducted at the André Rosemon Hospital in Cayenne and the West Guianese Hospital in Saint-Laurent-du-Maroni, French Guiana, between May 2019 and June 2021. Given the number of different potential outcomes there was no predetermined sample size calculation. The aim was to include as many patients as possible to describe our population and to have the greatest possible power to identify trends.
Overall, 1243 participants with diabetes mellitus were included in the CODIAM cohort. Diabetes was defined as an increase in fasting plasma blood glucose greater than or equal to 126 mg/dL (or 7 mmol/L) on two occasions and/or a blood glucose level taken at any time of day greater than or equal to 200mg/dL (or 11 mmol/L) on two occasions.
Inclusion Criteria
Patients over 18 years of age, with a confirmed diagnosis of diabetes and signed consent.
Exclusion Criteria
Patients who were minors, under guardianship, did not sign consent, refused to participate, were deprived of liberty, in acute life-threatening situations, with gestational diabetes, or during pregnancy and post partum (less than 6 months) were excluded.
Data Collection
Patients were included (first measure -V1) during consultations atthe Endocrinology Diabetology Nutrition department of Cayenne Hospital and the General Medicine department of Saint-Laurent-du-Maroni Hospital between May 2019 and June 2021. They were also recruited during hospitalizations in one of the medical or surgical departments of Cayenne hospital who requested an expertise in diabetology. Various data (social and demographic characteristics, medical and surgical history, examination data, and biological results, including basic diabetes monitoring parameters)were collected from included patients.
Evaluation of Precariousness
The EPICES (Evaluation of Precariousness and Inequalities in Health in Health Examination Centers) score was initially developed from a 42-variable questionnaire selected from the major Townsend and Wresinski studies. These included traditional socioeconomic determinants such as education, income, and occupation, but also take into account questions about family structure and housing, social benefits, and leisure activities. After the creators of the score conducted factor analysis of the 42 variables and multiple regression of the “social precarity gradient,” they selected a subset of 11 binary questions (Appendix 1). These 11 questions are the ones that are used to compute the score.Each question has a regression coefficient, the score varies from 0 (no precariousness) to 100 (maximum precariousness).The definition of deprivation state is defined as a score ≥ 30.17, a threshold which was established in a large cohort study carried out by Centre technique d’appui et de formation des centresd’examens de santé (Technical Centre of Support and Training for Health Centres) (18, 19).
The micro and macro vascular complications of diabetes (retinopathy, nephropathy, neuropathy, coronary artery disease (angina pectoris pectoris or myocardial infarction), transient ischemic attack or stroke, obliterative arteriopathy of the lower limbs)werecompared between precarious and non precarious. Indicators of glycemic control and associated clinical data of the patient with diabetes were compared between precarious and non precarious individuals.Infections classically attributable to diabetes (cutaneous, urinary tract, pulmonary, osteoarticular) were also compared between precarious and non precarious groups.
Statistical Analysis
Statistical analysis was performed using STATA software ®(STATA-CORP®, StataCorp LLC 4905 Lakeway Drive College Station, Texas 77845-4512 USA). A descriptive analysis of the study population and clinical data was performed. Quantitative data are expressed as mean and standard deviation and qualitative variables were expressed as frequencies and percentages. Comparisons of quantitative variables between precarious and non precarious patients were made using Student’s t-tests. The cross-tabulation of qualitative variables with the binary precariousness variable used the Chi-2 test to test for statistically significant differences. Glycated hemoglobin concentration was used as a dependent variable and other independent explanatory variables were included in a multiple linear regression model. The significance level was 5%.
Regulatory and Ethical Aspects
All included patients were informed of the anonymous use of their data for the research. In accordance with the French Data Protection Act and the General Data Protection Regulation, the data processing was subject to a data protection impact analysis, an entry in the hospital’s data processing register and a declaration of compliance MR003. The protocol was approved by the Comité de Protection des Personnes Sud-Est de Clermont-Ferrand (Nos ref: 2020/CE 05). All patients provided written informed consent for participation and publication of anonymized study results.
Results
Sociodemographic, Clinical and Biological Characteristics of the Population
1243 patients were included in the CODIAM cohort during the study period, 1018 responded to the EPICES score questions. 751 patients, i.e. 73.3% of the sample, had an EPICES score > 30.17 and were thus considered as precarious (Table 1). In the precarious population, there were more women (57.3%) than men. The non-precarious population was significantly older (59.1 ± 12.2 vs 56.0 ± 12.7 years) than the precarious population (Table 2). The meanduration of diabetes was identical at 9.3 ± 9.3 years in non precarious population and 9.3 ± 9.1 years in precarious population. Regarding the clinical examination, the group of people in precarious situations were significantly shorter by 4 cm.
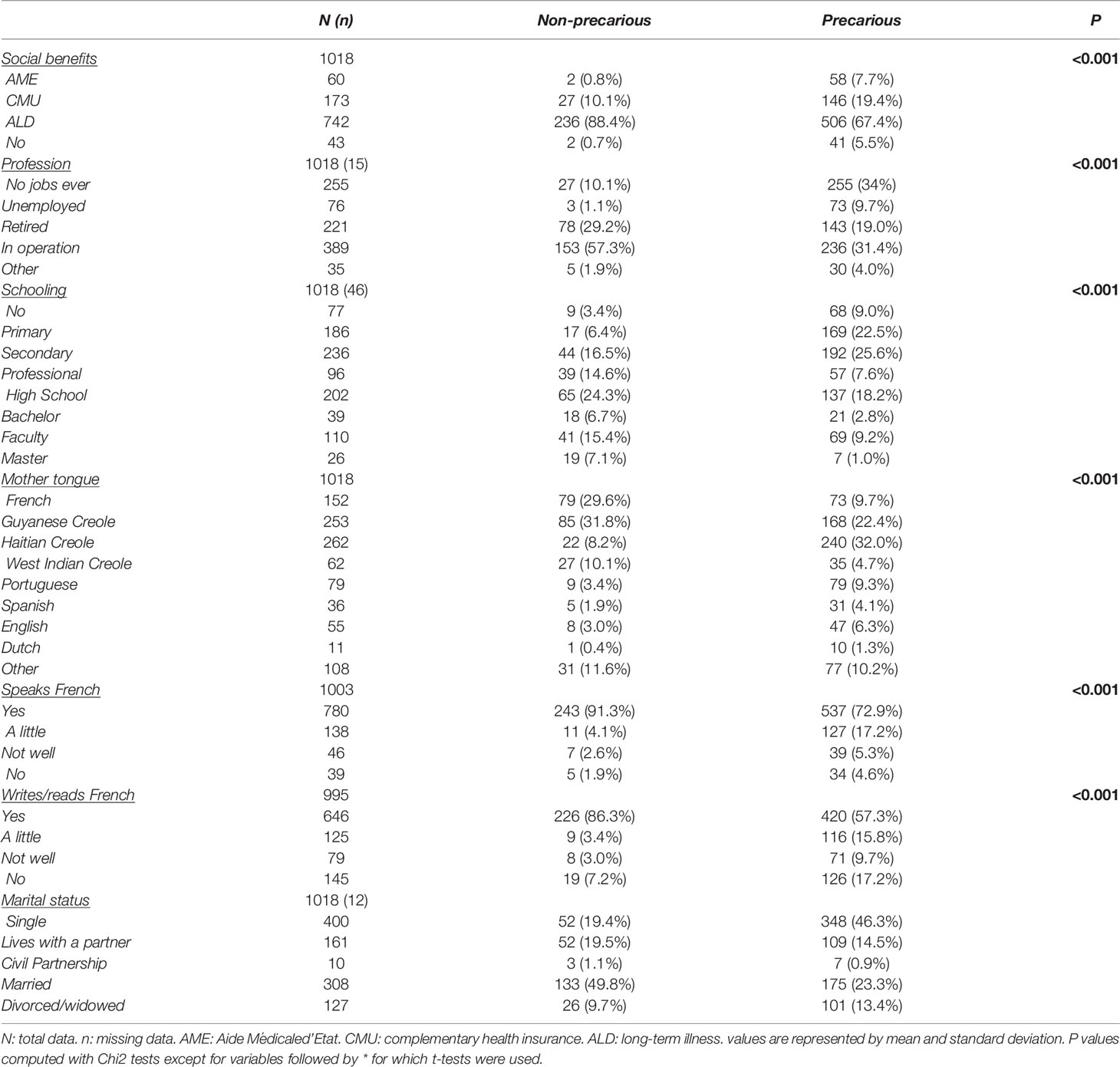
Table 1 Sociodemographic characteristics of the study population according to Precariousness.
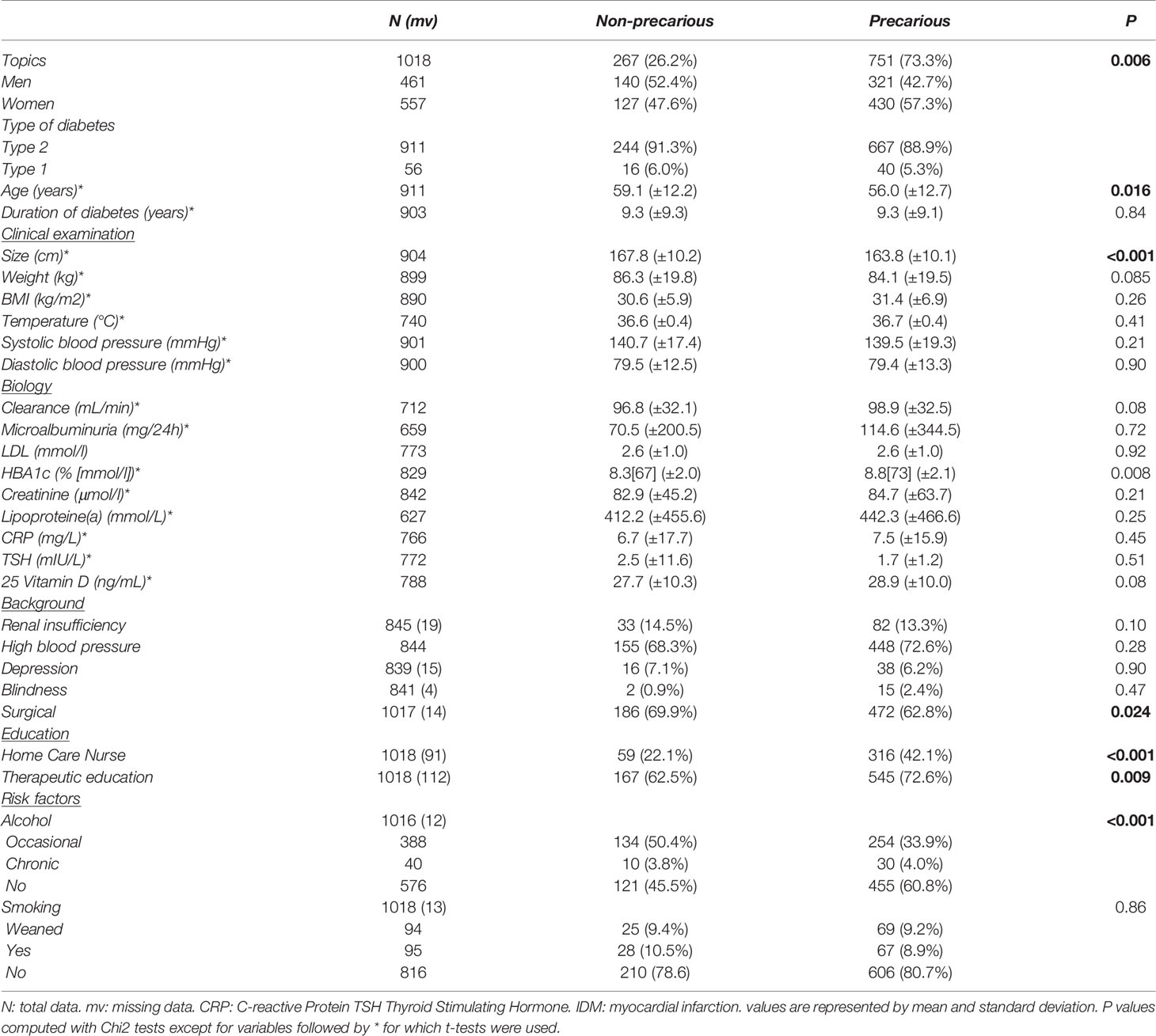
Table 2 Medical characteristics of the study population according to precariousness.
Biologically, the precarious subjects had a 0.5% higher Glycated Haemoglobin level than the non precarious. The vitamin D level was higher in the precarious group, but this failed to reach statistical significance. No significant difference was found for the rest of the variables.
Unsurprisingly, patients in the precarious group were significantly more likely to benefit from the PUMA, AME (Table 1) (guarantees any person working or residing in France in a stable and regular manner: Uninterrupted residence in France for more than 3 months a right to coverage of his or her health expenses on a personal basis and continuously throughout life) and/or CMUc health insurance regimens designed for the poor.
The population without a professional activity was significantly more important in the precarious group (Table 1), while the population with aprofessional activity was more important in the non precarious group. The level of education was inversely proportional to precariousness. The precarious population had significantly more difficulty speaking, reading and writing French and less than 10% considered French as their mother tongue.
No significant differences were shown in chronic alcohol use and active smoking (Table 2).
Finally, the precarious group was significantly more likely to benefit from a home care nurse and to participate in therapeutic education sessions.
Complications
Retinopathy and infections were significantly greater in the precarious group than in the non precarious group. No significant difference was shown fornephropathy, but there was an increase in microalbuminuria in the precarious group without alteration of renal function (Table 3).
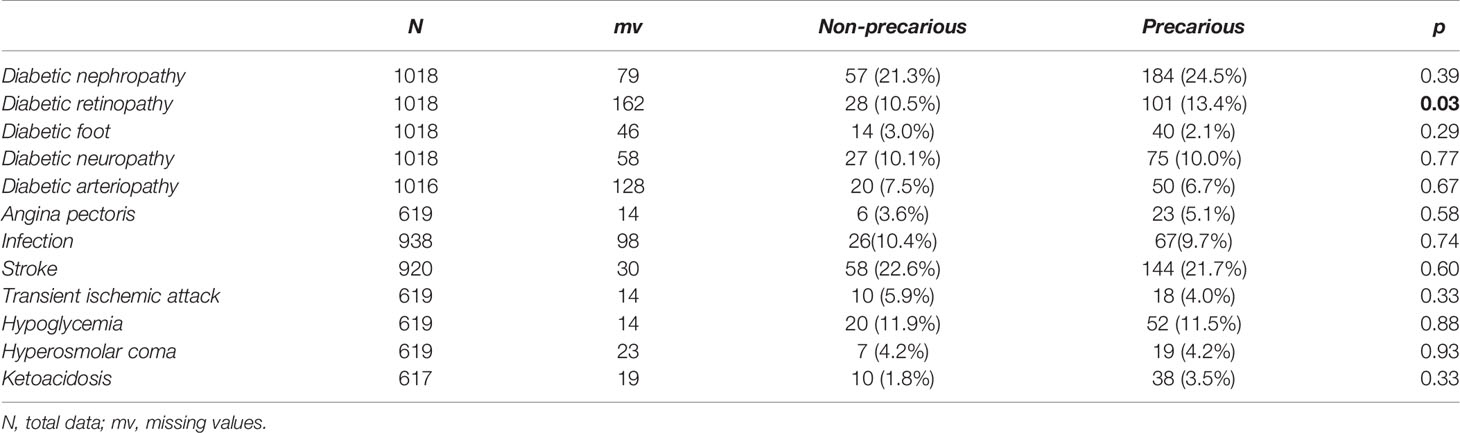
Table 3 Complications of the patient with diabetes according to precariousness.
Multiple Linear Regression Model of Glycated Hemoglobin Concentration
After adjusting for potential confounders, precariousness was no longer associated with glycated hemoglobin concentration. The variables that remained independently associated with a significant increase in the concentration of glycated hemoglobin were: being poorly fluent in French (+1.2% than fluent), having as a mother language Haitian creole (+0.6% relative to French), Guianese creole (+0.6% relative to French), Antilles creole (+0.7% relative to French) and portugese (+0.9% relative to French), and not having any health insurance (+1.5% relative to Full ALD insurance for diabetes) (Table 4).
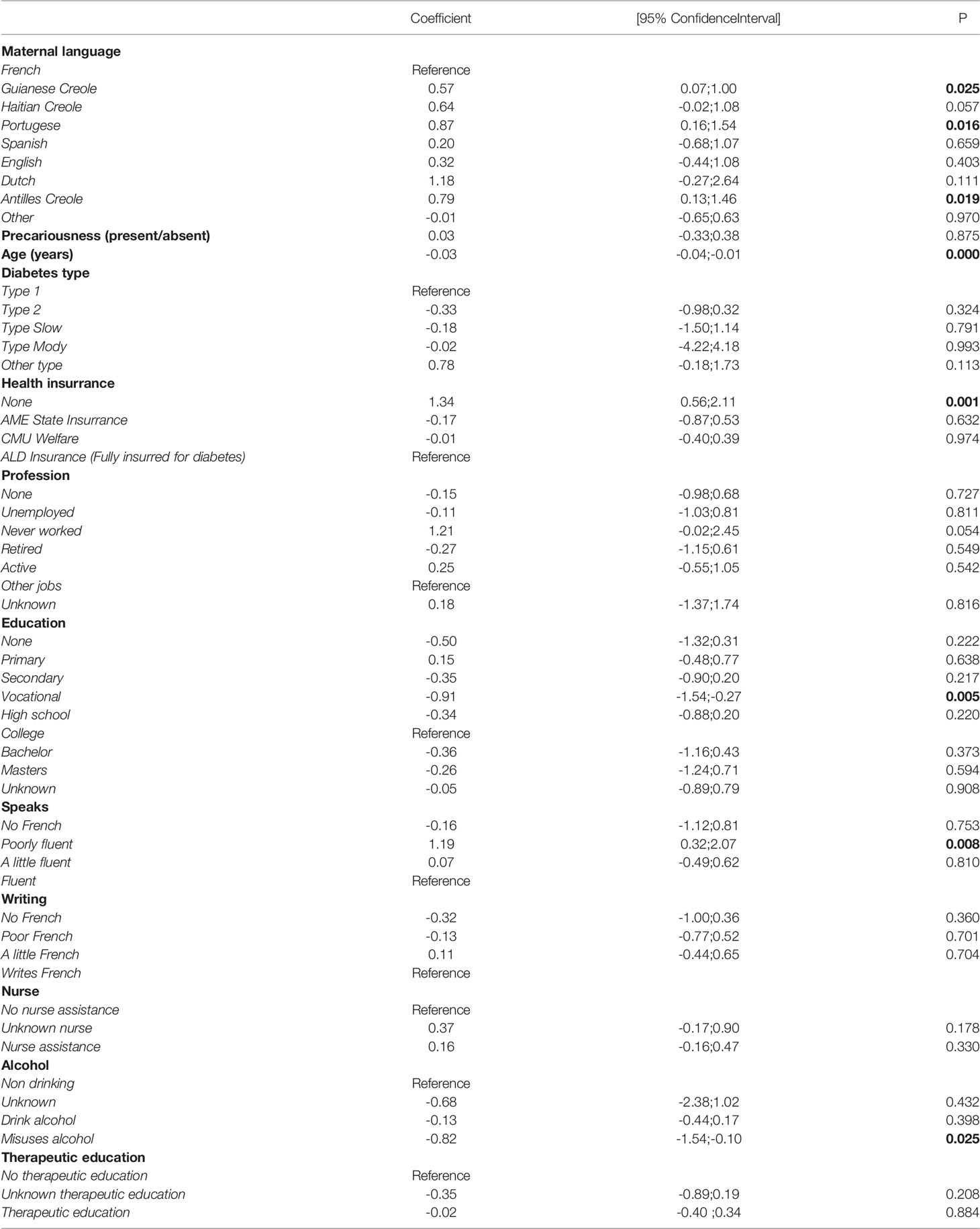
Table 4 Multiple linear regression model of glycated hemoglobin concentration and demographic and socioeconomic independent variables. .
Discussion
This work showed the association of precariousness with glycemic imbalance and retinal complications in patients with diabetes mellitus. However, apart from these significant results, the negative results may be even more striking: indeed, counter to our initial expectations, for most macro and microvascular complications there were no significant differences between precarious and non precarious patients. Furthermore, after adjusting for potential confounders precariousness was no longer associated with glycated hemoglobin concentration; the variables that remained independently associated with a significant increase in the concentration of glycated hemoglobin were: being poorly fluent in French, not having any health insurance, having creole or portugese as a mother language. Not understanding what the health professionals say and not being insurred are known obstacles to glycemic control: Management of diabetes requires interactive communication between the patient and the physician and shared decision making (20). Indeed, greater efficiency in health behaviors, health literacy allow for better glycemic control (21, 22). The mother language variable, which was adjusted for insurance and fluency, suggests other complementary explanations: cultural or genetic differences that may also influence glycemic control. Studies have indeed shown that ethnic minorities often have poor glycemic control (23). These differences are thought to be related to different biological functions related to insulin resistance, hyperinsulinemia, beta cell function and fat metabolism (24). It may have seemed surprising to find, after adjustments, no relation of having a home nurse or therapeutic education with glycemic control. However, the relation between glycated hemoglobin and these 2 variables actually goes both ways: although the interventions improve glycemic control, doctors prescribe a home nurse and more therapeutic education when glycemic control is poor.
Overall, the results suggest that for this chronic disease, once it is diagnosed, the universal health system eventually rectifies social inequalities in health in the long run leading to few differences between the precarious and non precarious, Hence, precarious patients were significantly more likely to have a home nurse than the non precarious (42.1% vs 22.1%) and more therapeutic education (81% vs 72%) to try to compensate for patient difficulties.
Given the scarcity of ophtalmologists in French Guiana, the increased proportion of patients with diabetic retinopathy among the precarious possibly reflects the particular difficulty to accessthe specialty for precarious populations (25). In French Guiana, only 19% of patients with diabetes had their eyes checked at least once every two years (26).
We did not find any significant difference between the two groups concerning diabetic nephropathy, unlike some authors (27) but similarly to others (28). We did not find any significant difference in angina pectoris or stroke, which differs from the literature (29, 30), probably because of the small number of events but perhaps also because the imperfect but universal healthcare system manages to provide primary care to the disfavored groups thus erasing the risk difference with the non-precarious.
In our population of patients with diabetes, a massive 73.3% of subjects were precarious. Precarious patients were older and more likely to be female than non precarious patients, presumably because with time and age, persons acquire greater social capital and resources whereas for single women, caring for children is costly. Comparative studies carried out in mainland France on a diabetic population using the same score to define precariousness show a prevalence ranging from 6.9% to 46% (19). In French Guiana, the prevalence of precariousness in a population witha stroke was 69% (31). In the United States, inequality among Afro-American, Hispanic or Asian ethnic minorities have been highlighted (32). The underlying mechanisms arein part explained by different lifestyles, particularly in terms of culture, understanding of the disease, and access to care, which can be very variable between health systems (33).
The EPICES score is regularly used in epidemiological studies dealing with the relationship between an individual’s socioeconomic factors and health status (34). It has been compared with the Anglo-Saxon indicators of Townsend and Carstairs and has shown equivalent results for the measurement of material and social deprivation (35). One study highlighted its capacity to measure precariousness in a multidimensional way and its robustness in the detection of precarious patients (36). Furthermore, a recent study comparing French Guiana to mainland France (37) showed no major difference between the two for the detection of precariousness and the EPICES score.
The strength of our study lies is that it allowed us to obtain a diverse sample of the French Guianese population and thus to limit selection bias. The weaknesses of the study lie mainly in the short duration of the follow-up of the cohort and future work will focus on the follow-up of the cohort over 24 months.
Furthermore, although the reduction of health inequalities have been a priority in many countries, to our knowledge, our work is one of few that has compared the occurrence of clinical events in a population with diabetes between the precarious and non precarious.
In conclusion, although there was a link between precariousness and the risk of retinopathy in precarious patients, this work highlights the fact there were no other significant differences between precarious and non precarious patients regarding micro or macrovascular complications of diabetes. Our health system may have difficulties in reaching some populations, however for chronic diseases such as diabetes, once patients are in the health care system, it seems to be fairly effective in erasing differences between the precarious and the non precarious. One of the weakest points of the French health system operating in the multicultural and multilingual context of French Guiana is the lack of translators and cultural mediators to cover the quasi-constant needs. The present results suggest this may be an area where gains could be made. There is still room for expanding the reach of the universal health system and mobile teams are being set up to go to isolated areas, therapeutic education modules are being strengthened in the departments with cultural and linguistic adaptation, and health mediators to improve glycemic control.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by ref: 2020/CE 05. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
Conceptualization: SL, MN, MM, AA, NS. Data curation: SL, MN, KD, MM, NH, AC, JA, AN, JK, AA, NS. Formal analysis: SL, MN, NS. Investigation: SL, MN, NH, MM, AC, CM-T, J-FC, JA, AA, NS. Resources: SL, MN, KD, MM, NH, AC, CMT, J-FC, JA, MD, KD AN, AA, NS. Supervision: MN, AA, NS. Validation: SL, MM, NH, MM, AC, CM-T, J-FC, JA, BD, KD JH-P, AN, JK, MD, AA, NS. Visualization: SL, MM, NH, KD, MM, AC, CM-T, J-FC, JA, BD, MD, JH-P, AN, AA, NS. Manuscript writing: SL, MN, KD, AA, NS. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.937156/full#supplementary-material
Abbreviations
CODIAM, Cohort of Diabetes in French Amazonia; EPICES, Evaluation of Precariousness and Inequalities in Health in Health Examination Centers; AME, state medical aid; ALD, Long-term care insurance; PUMA, universal health protection; CMU-c, complementary universal health coverage; HbA1c, Glycated Haemoglobin.
References
1. Marmot M, Allen J, Bell R, Bloomer E, Goldblatt P. Consortium for the European Review of Social Determinants of Health and the Health Divide (2012) WHO European Review of Social Determinants of Health and the Health Divide. Lancet Lond Engl 380(9846):1011–29. doi: 10.1016/S0140-6736(12)61228-8
2. Mackenbach JP, Stirbu I, Roskam A-JR, Schaap MM, Menvielle G, Leinsalu M, et al. Socioeconomic Inequalities in Health in 22 European Countries. N Engl J Med (2008) 358(23):2468–81. doi: 10.1056/NEJMsa0707519
3. Power C, Matthews S. Origins of Health Inequalities in a National Population Sample. Lancet Lond Engl (1997) 350(9091):1584–9. doi: 10.1016/S0140-6736(97)07474-6
4. Stringhini S, Dugravot A, Shipley M, Goldberg M, Zins M, Kivimäki M, et al. Health Behaviours, Socioeconomic Status, and Mortality: Further Analyses of the British Whitehall II and the French GAZEL Prospective Cohorts. PloS Med (2011) 8(2):e1000419. doi: 10.1371/journal.pmed.1000419
5. Ward E, Jemal A, Cokkinides V, Singh GK, Cardinez C, Ghafoor A, et al. Cancer Disparities by Race/Ethnicity and Socioeconomic Status. CA Cancer J Clin (2004) 54(2):78–93. doi: 10.3322/canjclin.54.2.78
6. Rosengren A, Smyth A, Rangarajan S, Ramasundarahettige C, Bangdiwala SI, AlHabib KF, et al. Socioeconomic Status and Risk of Cardiovascular Disease in 20 Low-Income, Middle-Income, and High-Income Countries: The Prospective Urban Rural Epidemiologic (PURE) Study. Lancet Glob Health (2019) 7(6):e748–60. doi: 10.1016/S2214-109X(19)30045-2
7. Abraham TM, Pencina KM, Pencina MJ, Fox CS. Trends in Diabetes Incidence: The Framingham Heart Study. Diabetes Care (2015) 38(3):482–7. doi: 10.2337/dc14-1432
8. Roper NA, Bilous RW, Kelly WF, Unwin NC, Connolly VM. Excess Mortality in a Population With Diabetes and the Impact of Material Deprivation: Longitudinal, Population Based Study. BMJ (2001) 322(7299):1389–93. doi: 10.1136/bmj.322.7299.1389
9. Robinson N, Lloyd CE, Stevens LK. Social Deprivation and Mortality in Adults With Diabetes Mellitus. Diabetes Med J Br Diabetes Assoc (1998) 15(3):205–12. doi: 10.1002/(SICI)1096-9136(199803)15:3<205::AID-DIA519>3.0.CO;2-
10. Krieger N, Williams DR, Moss NE. Measuring Social Class in US Public Health Research: Concepts, Methodologies, and Guidelines. Annu Rev Public Health (1997) 18:341–78. doi: 10.1146/annurev.publhealth.18.1.341
11. Brown AF, Ettner SL, Piette J, Weinberger M, Gregg E, Shapiro MF, et al. Socioeconomic Position and Health Among Persons With Diabetes Mellitus: A Conceptual Framework and Review of the Literature. Epidemiol Rev (2004) 26:63–77. doi: 10.1093/epirev/mxh002
12. Rapport Wresinski CES 1987 (2006). Joseph Wresinski. Available at: https://www.joseph-wresinski.org/fr/grande-pauvrete-et-precarite/ (Accessed 18 Jan 2021). FR.
14. Niveaux De Vie Et Pauvreté En Guyane En 2017 : La Moitié Des Guyanais Vivent Sous Le Seuil De Pauvreté - Insee Analyses Guyane - 46 . Available at: https://www.insee.fr/fr/statistiques/4623886 (Accessed 4 Feb 2022).
15. Atallah A, Atallah V, Daigre J-L, Boissin J-L, Kangambega P, Larifla L, et al. [High Blood Pressure and Obesity: Disparities Among Four French Overseas Territories]. Ann Cardiol Angeiol (Paris) (2014) 63(3):155–62. doi: 10.1016/j.ancard.2014.05.008
16. Sabbah N, Massicard M, Mathieu N. Specificities of the Diabetic Population in French Guiana: The Health Barometer Survey. Curr Diabetes Rev (2021) 18(1):e012821190876. doi: 10.2174/1573399817666210129103506
17. UK Prospective Diabetes Study (UKPDS) Group. Intensive Blood-Glucose Control With Sulphonylureas or Insulin Compared With Conventional Treatment and Risk of Complications in Patients With Type 2 Diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet Lond Engl (1998) 352(9131):837–53.
18. Sass C, Moulin JJ, Gueguen R, Abric L, Dauphinot V, Dupre C, et al. Le Score Épices : Un Score Individuel De Précarité. Construction Du Score Et Mesure Des Relations Avec Des Données De Santé, Dans Une Population De 197 389 Personnes. (2006), Score Épic Un Score Individ Précarité Constr Score Mes Relat Avec Données Santé Dans Une Popul 197 389 Pers., Paris France, Santé Publique France
19. Bihan H, Ramentol M, Fysekidis M, Auclair C, Gerbaud L, Desbiez F, et al. Screening for Deprivation Using the EPICES Score: A Tool for Detecting Patients at High Risk of Diabetic Complications and Poor Quality of Life. Diabetes Metab (2012) 38(1):82–5. doi: 10.1016/j.diabet.2011.10.004
20. Chatterjee S, Davies MJ, Heller S, Speight J, Snoek FJ, Khunti K. Diabetes Structured Self-Management Education Programmes: A Narrative Review and Current Innovations. Lancet Diabetes Endocrinol (2018) 6(2):130–42. doi: 10.1016/S2213-8587(17)30239-5
21. Aljasem LI, Peyrot M, Wissow L, Rubin RR. The Impact of Barriers and Self-Efficacy on Self-Care Behaviors in Type 2 Diabetes. Diabetes Educ (2001) 27(3):393–404. doi: 10.1177/014572170102700309
22. Schillinger D, Barton LR, Karter AJ, Wang F, Adler N. Does Literacy Mediate the Relationship Between Education and Health Outcomes? A Study of a Low-Income Population With Diabetes. Public Health Rep Wash DC (20061974) 121(3):245–54. doi: 10.1177/003335490612100305
23. Heidemann DL, Joseph NA, Kuchipudi A, Perkins DW, Drake S. Racial and Economic Disparities in Diabetes in a Large Primary Care Patient Population. Ethn Dis (2016) 26(1):85–90. doi: 10.18865/ed.26.1.85
24. Golden SH, Brown A, Cauley JA, Chin MH, Gary-Webb TL, Kim C, et al. Health Disparities in Endocrine Disorders: Biological, Clinical, and Nonclinical Factors–an Endocrine Society Scientific Statement. J Clin Endocrinol Metab (2012) 97(9):E1579–1639. doi: 10.1210/jc.2012-2043
25. Zhang X, Beckles GL, Chou C-F, Saaddine JB, Wilson MR, Lee PP, et al. Socioeconomic Disparity in Use of Eye Care Services Among US Adults With Age-Related Eye Diseases: National Health Interview Survey, 2002 and 2008. JAMA Ophthalmol (2013) 131(9):1198–206. doi: 10.1001/jamaophthalmol.2013.4694
26. Sudre C, Duplan H, Bukasakakamba J, Nacher M, Peyre-Costa P, Sabbah N. Diabetes Care in French Guiana: The Gap Between National Guidelines and Reality. Front Endocrinol (2021) 12:789391. doi: 10.3389/fendo.2021.789391
27. Nicolucci A, Carinci F, Ciampi A. Stratifying Patients at Risk of Diabetic Complications: An Integrated Look at Clinical, Socioeconomic, and Care-Related Factors. SID-AMD Italian Study Group for the Implementation of the St. Vincent Declaration. Diabetes Care (1998) 21(9):1439–44. doi: 10.2337/diacare.21.9.1439
28. Bihan H, Laurent S, Sass C, Nguyen G, Huot C, Moulin JJ, et al. Association Among Individual Deprivation, Glycemic Control, and Diabetes Complications: The EPICES Score. Diabetes Care (2005) 28(11):2680–5. doi: 10.2337/diacare.28.11.2680
29. Booth GL, Bishara P, Lipscombe LL, Shah BR, Feig DS, Bhattacharyya O, et al. Universal Drug Coverage and Socioeconomic Disparities in Major Diabetes Outcomes. Diabetes Care (2012) 35(11):2257–64. doi: 10.2337/dc12-0364
30. Larrañaga I, Arteagoitia JM, Rodriguez JL, Gonzalez F, Esnaola S, Piniés JA, et al. Socio-Economic Inequalities in the Prevalence of Type 2 Diabetes, Cardiovascular Risk Factors and Chronic Diabetic Complications in the Basque Country, Spain. Diabetes Med J Br Diabetes Assoc (2005) 22(8):1047–53. doi: 10.1111/j.1464-5491.2005.01598.x
31. Béjot Y, Guilloteau A, Joux J, Lannuzel A, Mimeau E, Mislin-Tritsch C, et al. Social Deprivation and Stroke Severity on Admission: A French Cohort Study in Burgundy and the West Indies - Guyana Region. Eur J Neurol (2017) 24(5):694–702. doi: 10.1111/ene.13271
32. Williams DR, Priest N, Anderson NB. Understanding Associations Among Race, Socioeconomic Status, and Health: Patterns and Prospects. Health Psychol Off J Div Health Psychol Am Psychol Assoc (2016) 35(4):407–11. doi: 10.1037/hea0000242
33. Ford ES, Merritt RK, Heath GW, Powell KE, Washburn RA, Kriska A, et al. Physical Activity Behaviors in Lower and Higher Socioeconomic Status Populations. Am J Epidemiol (1991) 133(12):1246–56. doi: 10.1093/oxfordjournals.aje.a115836
34. Le Floch A-C, Eisinger F, D’Incan E, Rey J, Charbonnier A, Caymaris L, et al. Socioeconomic Deprivation is Associated With Decreased Survival in Patients With Acute Myeloid Leukemia. Cancer Epidemiol (2020) 66:101699. doi: 10.1016/j.canep.2020.101699
35. Labbe E, Blanquet M, Gerbaud L, Poirier G, Sass C, Vendittelli F, et al. A New Reliable Index to Measure Individual Deprivation: The EPICES Score. Eur J Public Health (2015) 25(4):604–9. doi: 10.1093/eurpub/cku231
36. Sass C, Guéguen R, Moulin JJ, Abric L, Dauphinot V, Dupré C, et al. [Comparison of the Individual Deprivation Index of the French Health Examination Centres and the Administrative Definition of Deprivation]. Sante Publique Vandoeuvre–Nancy Fr (2006) 18(4):513–22. doi: 10.3917/spub.064.0513
37. Guilloteau A, Binquet C, Bourredjem A, Fournel I, Lalanne-Mistrih ML, Nacher M, et al. Social Deprivation Among Socio-Economic Contrasted French Areas: Using Item Response Theory Analysis to Assess Differential Item Functioning of the EPICES Questionnaire in Stroke Patients. PloS One (2020) 15(4):e0230661. doi: 10.1371/journal.pone.0230661
Keywords: precariousness, diabetes, retinopathy, infections, stroke
Citation: Linière S, Nacher M, Drak Alsibai K, Mergeayfabre M, Hafsi N, Charpin A, Misslin-Tritsch C, Carod J-F, Aurelus JM, De Toffol B, Ntoutoum A, Kakamba JB, Demar M, Helene-Pelage J, Adenis A and Sabbah N (2022) Precariousness, Diabetes Control and Complications in French Guiana. Front. Endocrinol. 13:937156. doi: 10.3389/fendo.2022.937156
Received: 05 May 2022; Accepted: 20 June 2022;
Published: 22 July 2022.
Edited by:
Junping Wen, Fujian Provincial Hospital, ChinaReviewed by:
Nigusie Gashaye Shita, Debre Markos University, EthiopiaLouis POTIER, Assistance Publique Hopitaux De Paris, France
Copyright © 2022 Linière, Nacher, Drak Alsibai, Mergeayfabre, Hafsi, Charpin, Misslin-Tritsch, Carod, Aurelus, De Toffol, Ntoutoum, Kakamba, Demar, Helene-Pelage, Adenis and Sabbah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nadia Sabbah, bmFkaWEuc2FiYmFoQGNoLWNheWVubmUuZnI=; orcid.org/0000-0002-7789-6728