
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 08 September 2022
Sec. Neuroendocrine Science
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.920680
This article is part of the Research TopicAdvances and Perspectives in NeuroplacentologyView all 8 articles
 Rachel L. Leon1*
Rachel L. Leon1* Vinay Kalvacherla2
Vinay Kalvacherla2 Michelle Machie Andrews1
Michelle Machie Andrews1 Jennifer M. Thomas1
Jennifer M. Thomas1 Imran N. Mir1
Imran N. Mir1 Lina F. Chalak1
Lina F. Chalak1Objective: To determine the birth prevalence of perinatal stroke in term born infants at our high-volume delivery center and assess the frequency of both gross and histologic placental pathologies associated with perinatal stroke using the Amsterdam Placental Workshop Group Consensus Statement guidelines and definitions.
Study Design: A single-center retrospective cohort study spanning 2010-2020.
Results: There were 129,759 live births at Parkland Hospital during the study period and a total of 18 term born infants leading to a birth prevalence of 1 in 6,829 infants. Perinatal risk factors were found in all but one patient, and 74% presented with seizures. Pathologic placental examination was available in 56% of the cohort and only one patient had normal placental examination. Acute histologic chorioamnionitis was described in five placentas (50%) and an additional two had isolated umbilical and/or chorionic plate vasculitis with or without funisitis compared to a rate of 28% with acute inflammation in a Control group. Chronic inflammation in the form of villitis of unknown etiology was described in three of the acutely inflamed placentas and was high-grade in each of those while none of the placentas from our Control group showed evidence of any chronic lesion.
Conclusion: Both acute and chronic placental inflammation are common in perinatal stroke; placental examination should be considered an essential component to the diagnostic workup.
Perinatal stroke is defined as cerebrovascular injury occurring between 20 weeks gestational age until the 28th postnatal day. Perinatal stroke affects an estimated 1 in 2,300 to 1 in 5,000 term born infants (1–3). In broad terms, perinatal stroke comprises several entities including arterial ischemic stroke (AIS), cerebral sinovenous thrombosis (CSVT), and intracranial hemorrhage (ICH). Perinatal AIS is the most common form of stroke in term neonates and is a leading cause of hemiplegia in pediatric patients (4, 5). Perinatal AIS is characterized by imaging findings of parenchymal infarct in a specific arterial territory, and outcomes vary widely depending on timing of injury, lesion size, and location (6–8). Perinatal CSVT is less common entity most frequently affecting the sagittal and/or lateral sinus (9–11).
Numerous risk factors have been associated with perinatal stroke (12–20), which can be divided into maternal, fetal, and neonatal complications. Suspected maternal risk factors include preeclampsia and prothrombotic disorders, while fetal risk factors include intrauterine growth restriction, prolonged rupture of membranes, and congenital heart disease. Neonatal factors associated with perinatal stroke involve birth asphyxia, infection, and hematologic disorders. Despite numerous studies attempting to define risk factors for perinatal stroke, the etiology of the injury remains unclear in most cases. Some experts hypothesize that for AIS, a thromboembolus may originate from the placenta, enter fetal circulation, and cross the patent foramen ovale to result in cerebral artery obstruction (21), but no studies to date have confirmed this mechanism (22, 23). As much as 30% of neonatal AIS is multifocal, even in the absence of congenital cardiac disease (4), and recurrence postnatally is exceedingly rare, supporting this hypothesis of a placental origin of thromboembolism. The connection of the placenta to CSVT and ICH is less clear, but may be associated with chronic placental inflammation, a type of pathology linked to other neurologic morbidities (24, 25). Overall, there is a paucity of existing evidence directly linking placental disease to neonatal stroke.
The objective of this study was to determine the birth prevalence of perinatal stroke in term born infants at our high-volume delivery center, describe the clinical factors associated with perinatal stroke in our cohort, and assess the frequency of both gross and histologic placental pathologies associated with perinatal stroke using the Amsterdam Placental Workshop Group Consensus Statement guidelines and definitions. We hypothesized that perinatal stroke would be associated with acute inflammation of the placenta, maternal pregnancy complications, fetal congenital heart disease, and birth asphyxia.
This single-center retrospective cohort study was approved by the Institutional Review Board at University of Texas Southwestern Medical Center. All infants born at Parkland Hospital between 2010-2020 with a diagnosis of stroke were evaluated for inclusion in the study. Control placentas were collected as part of a separate prospective study, previously reported (26) with inclusion criteria of gestational age of at least 37 weeks, singleton pregnancy without diagnosis of fetal anomalies or fetal growth restriction, and no history of fetal asphyxia.
Demographic information was collected on both mother and infant including maternal age, gestational age at birth, infant sex, race, and ethnicity. Maternal pregnancy complications, fetal diagnoses, and birth characteristics were collected and percentiles for anthropometric data (27). Specific factors affecting risk for placental pathology were collected including maternal gravida status, maternal diabetes mellitus (DM; both gestational and pre-gestational), any form of maternal hypertension, and presence of placenta accreta spectrum disease.
In general, the approach to selection of placentas for pathologic examination include any maternal or fetal pregnancy complication, or any abnormality during labor or delivery including the need for advanced neonatal resuscitation. The standardized approach of our institution to placental pathology has been previously described (24). In summary, gross examination includes assessment of the umbilical cord, membranes, and placental disc. The trimmed placental weight is measured after removal of umbilical cord, fetal membranes, and non-adherent blood clots. Gross pathologies include placental size abnormalities [small for gestational age (SGA), <10th percentile; and large for gestational age (LGA), >90th percentile], umbilical cord anomalies, and aberrant placental disc shapes. To determine histopathology, placental discs are sectioned at 1-2 cm intervals and representative sections of parenchyma, as well as umbilical cord and fetal membranes, are examined. Lesions identified during sectioning are also examined. Based on the Amsterdam criteria (28), histopathologic abnormalities were divided into the following subcategories:
1. Acute histologic chorioamnionitis (AHC), further categorized as maternal inflammatory response (MIR) and fetal inflammatory response (FIR), also classified by stages and grades.
2. Villitis of unknown origin (VUE) including low grade, high grade, and villitis with avascular villi.
3. Maternal vascular malperfusion (MVM), which encompasses maternal vascular lesions (e.g. decidual arteriopathy, mural hypertrophy, incomplete transformation of spiral arteries, and decidual necrosis), infarcts, hemorrhage or hematoma, thrombi (involving >5% of parenchyma), villous changes (e.g. chorangiosis, syncytial knots, distal villous hypoplasia, and accelerated villous maturation), and placental hypoplasia.
4. Fetal vascular malperfusion (FVM) further divided into two patterns, a) segmental FVM, indicating thrombotic occlusion of chorionic or stem villous vessels, or stem vessel obliteration, and b) global FVM, characterized by partially obstructed umbilical blood flow accompanied by venous ectasia, intramural fibrin deposition in large vessels, and/or small foci of avascular or karyorrhectic villi.
5. Other inflammatory lesions such as chronic deciduitis with plasma cells, massive chronic intervillositis, perivillous fibrin, and histiocytic intervillositis; and, delayed villous maturation, and villous edema.
6. Abnormalities in placental size – either small for gestational age (<10th percentile, SGA) or large for gestational age (>90th percentile, LGA).
Maternal and infant patient characteristics as well as placental pathologies were analyzed with descriptive statistics. Values are presented as mean ± standard deviation or median (interquartile range) where appropriate.
Between 2010 and 2020, there were 129,759 live births at Parkland Hospital and a total of 19 infants born at ≥37 weeks gestational age diagnosed with stroke or presumed perinatal stroke during the study period, giving a perinatal stroke birth prevalence of 1 in 6,829 live births. In our cohort from this community safety-net hospital, 84% of our patient cohort was Hispanic. Of the 19 stroke patients, 53% were female, their median gestational age at birth was 39 6/7 (29, 30), and median Apgar scores were 8 (4, 8) and 9 (7, 9) at one and five minutes (Table 1). Seizure was the presenting symptom in 74% of the cohort. The average age at onset of symptoms was 1.5 days (2.5 hours, 2.8 days) for those diagnosed in the neonatal period.
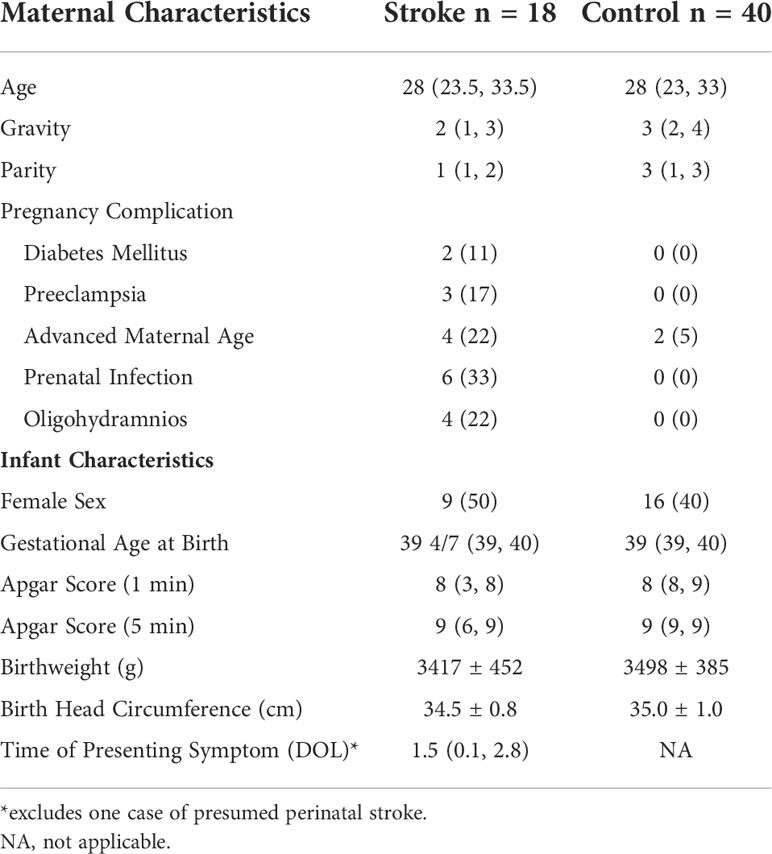
Table 1 Maternal and infant patient characteristics.
In our patient cohort, 13 had AIS, four had hemorrhagic stroke, and two were diagnosed with CSVT (Table 2). Of the patients with AIS, six were left-sided, four were right-sided, and three were bilateral. AIS was multifocal in eight patients and most commonly occurred in the distribution of the MCA. Hemorrhagic stroke presented on the left side in three patients and on the right in one patient. In addition to parenchymal hemorrhage, there was associated IVH in two patients. CSVT affected the dorsal aspect of intracerebral veins and vein of Galen in one patient and the deep medullary veins in the other patient. Neither of these patients had concomitant IVH. One or more perinatal risk factor was present in nearly every patient with maternal infectious concerns the leading maternal risk factor (occurring in 6 maternal patients) (Table 3). Maternal preeclampsia was diagnosed in three patients and diabetes mellitus in two. Meconium-stained amniotic fluid was common in our cohort occurring in 12 patients. In addition, non-reassuring fetal heart tones (defined as Category II or III fetal heart rate tracings) occurred in seven patients and delivery room resuscitation was required in nine patients that had stroke. A total of five stroke patients were diagnosed with hypoxic-ischemic encephalopathy and six patients had congenital heart disease, which was primarily ASD with or without VSD. Clinical chorioamnionitis was diagnosed in four patients, but histologic evidence of acute inflammation was more common, as described with placental findings.
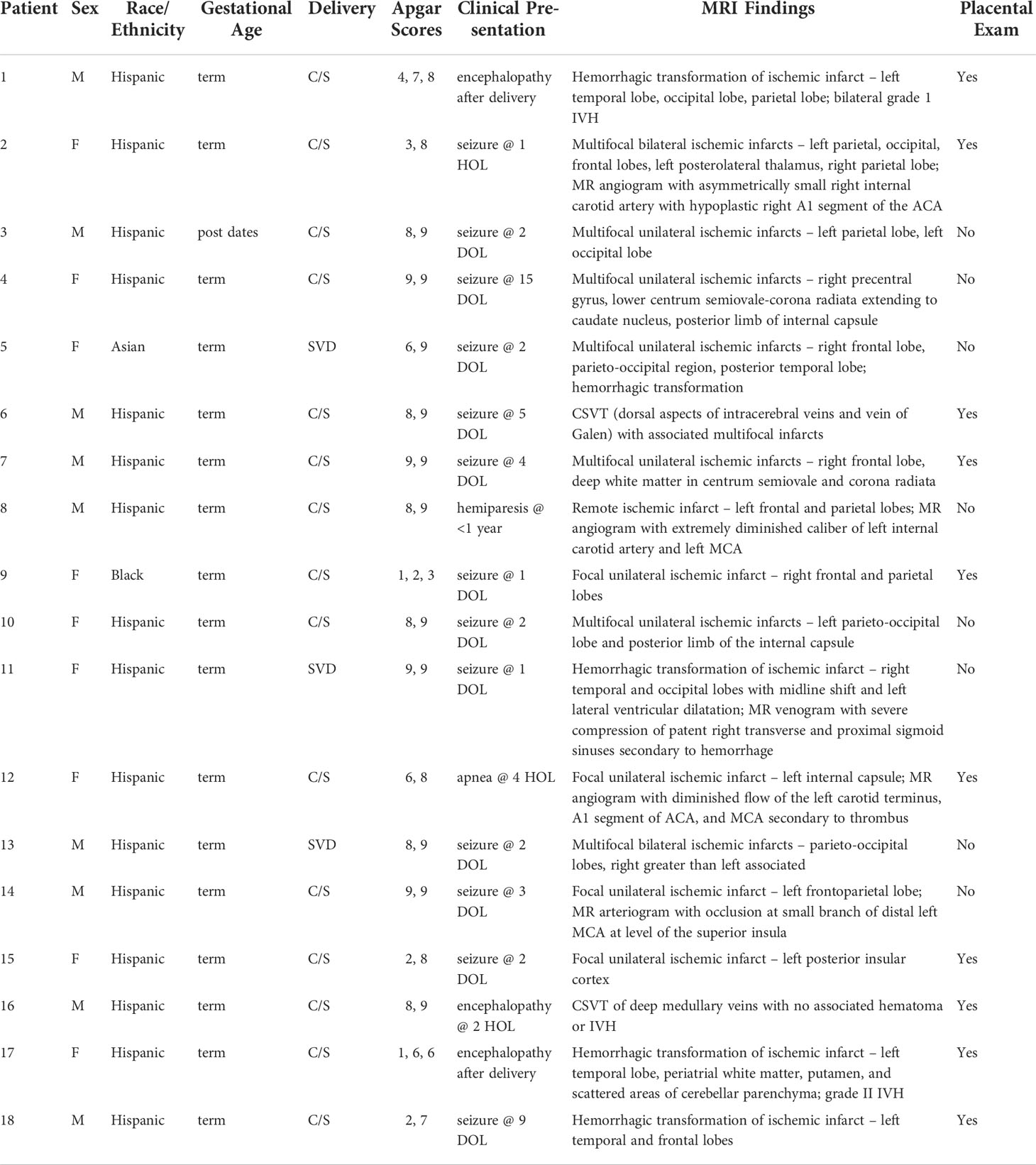
Table 2 Detailed clinical information .
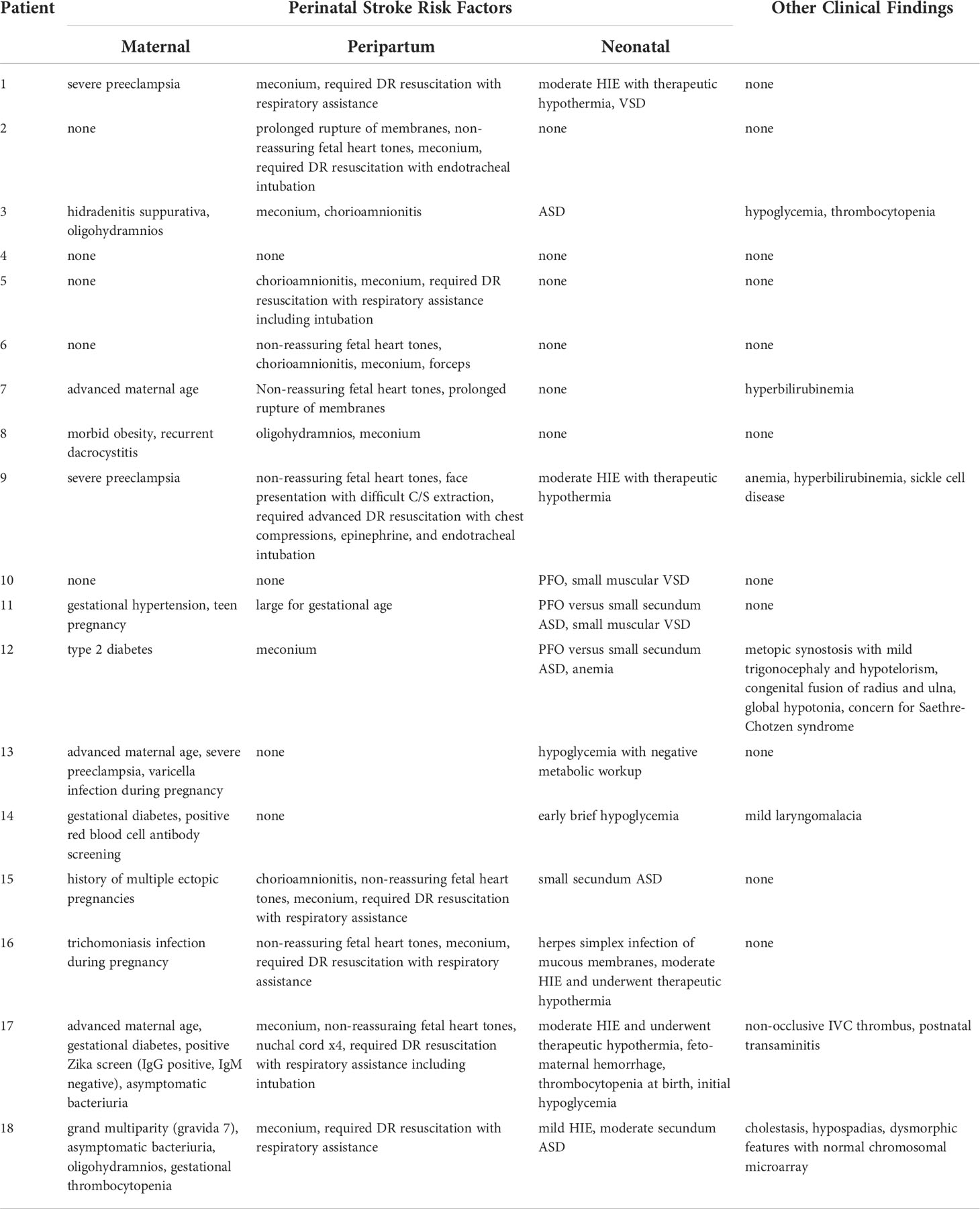
Table 3 Stroke risk factors.
Ten of our patients with stroke had placental pathologic examination performed (53%), and results are summarized in Table 4. Only one of these placentas had no gross or histologic abnormalities compared to 29 (72.5%) of Control placentas with no abnormalities. Three placentas in our Stroke cohort were found to be SGA and one was LGA while no size abnormalities were present in the Control group. One placenta from a neonate with stroke had borderline hypercoiled umbilical cord and none of the placentas had abnormalities of disc shape. Similarly, no cord insertion abnormalities were reported in either group. All but one placenta in the Stroke group had gross and/or histologic evidence of meconium staining while only four placentas in the Control group had evidence of meconium. Acute inflammatory lesions were highly prevalent in the Stroke cohort with five placentas diagnosed with acute histologic chorioamnionitis, all with Maternal Inflammatory Response (MIR) Stage 2, and nearly all Grade 1. Fetal Inflammatory Response (FIR) was present in six placentas: isolated FIR Stage 2, Grade 1 without MIR in one placenta; Stage 2, Grade 1 in four placentas; Stage 1, Grade 1 in one placenta; and Stage 3, Grade 2 in one placenta. Only one placenta from the Stroke group with MIR did not demonstrate associated FIR. Acute inflammation was the only lesions in the Control placentas, and MIR was present in 11 (28%) with six of those showing associated FIR. In the Stroke group, chronic inflammation in the form of VUE was described in three of the acutely inflamed placentas and was high-grade in each of those. No placentas had VUE with avascular villitis. MVM was described in four placentas from neonates with stroke, with three showing placental hypoplasia and one with extensive thrombosis, infarcts comprising >5% of the parenchyma, and diffuse fibrin. FVM was found in none of the study placentas. Chronic deciduitis with plasma cells occurred in two placentas from the Stroke group. Delayed villous maturation and villous edema were not present in any placentas.
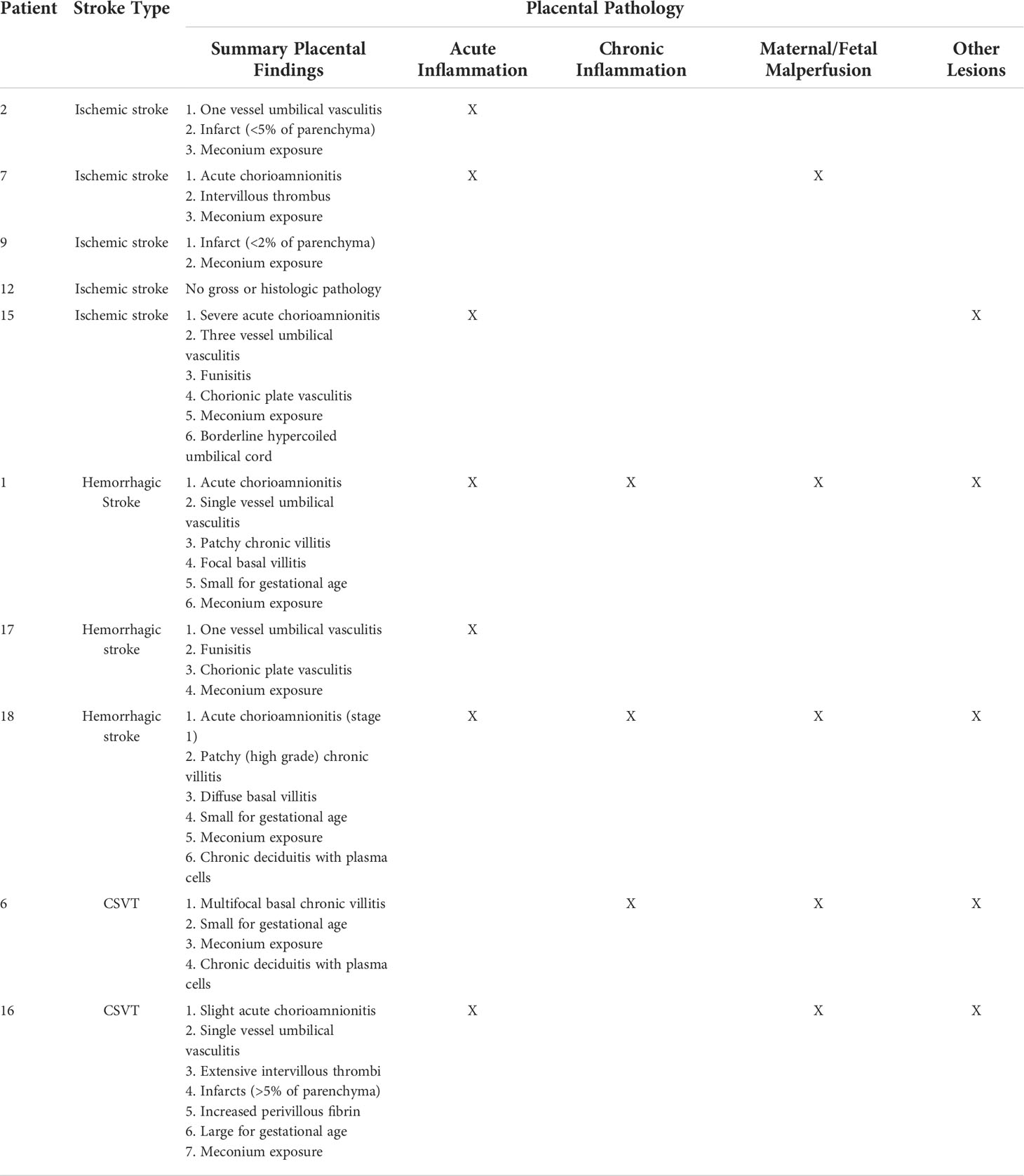
Table 4 Placental gross and histopathologic findings.
In this single-center cohort study we demonstrated that 1) pathologic placental lesions often accompany perinatal stroke, particularly acute and chronic inflammatory conditions, and 2) placental examination is frequently missed in the clinical investigation to determine stroke etiology, even in centers with robust guidelines for placental pathology practices. Nevertheless, placental examination in 53% of our perinatal stroke cohort is significantly higher than prior studies where rates of placental examination for neonates diagnosed with stroke ranged from 6-13% (31). The most likely explanation for the low rate of placental pathology in these cases is the delayed onset of symptoms and diagnosis of perinatal stroke, by which time the placenta may have already been discarded.
Perinatal stroke is an infrequent but important cause of both immediate and long-term morbidity in neonates. Our single-center data show an overall birth prevalence of perinatal stroke of 1 in 6,829 over a 10-year period at our high-volume delivery center, which differs from other reports and indicates that some patients may have gone undiagnosed during postnatal hospital stay. Furthermore, our report includes only one case of presumed perinatal stroke, which likely contributes to the difference we report in birth prevalence of perinatal stroke compared to other studies (1, 18, 32, 33). Since our NICU readmits patients from home for a limited range of indications only within the first week after birth, these results exclude many patients who are later diagnosed due to seizures, early handedness, hemiparesis, or delayed achievement of developmental milestones. This brings attention to the fact that perinatal stroke diagnosis requires a high level of clinical suspicion and for many patients, may go undetected until later. Presumed perinatal stroke accounts for a significant number of perinatal stroke cases and typically presents before one-year of age (3, 34).
While numerous studies have outlined risk factors associated with perinatal stroke (12, 15, 21, 34, 35), the exact etiology remains unknown and is likely multifactorial, including maternal, peripartum, and neonatal factors. Nearly all our patients had one or more perinatal risk factor(s) and seizures were the most frequent presenting symptom in our cohort, as has been previously reported (5). In a meta-analysis of eight studies including 550 cases of neonatal AIS, maternal preeclampsia imparted a significantly increased risk of neonatal AIS (36). In our small cohort, preeclampsia was less prevalent than maternal infectious concerns which ranged from asymptomatic bacteriuria to hidradenitis suppurativa. In addition, clinical chorioamnionitis was diagnosed in 60% of the maternal patients in our cohort. In prior reports, inflammatory conditions including chorioamnionitis have been prominent risk factors for perinatal stroke (31).
Our understanding of the role of the placenta in perinatal AIS has evolved in recent years with new evidence emerging that there are high rates of multiple placental histopathologies in perinatal stroke, particularly AIS (37, 38). Our cohort confirms those findings with 90% of stroke patients having at least one placental abnormality. This is similarly high to the rate of placental lesions in a cohort of patients we recently studied with congenital heart disease (78%) (39). Placental inflammatory conditions seem to play a prominent role in perinatal stroke pathophysiology (38), and our cohort has similar findings with 80% showing acute and/or chronic inflammation of the placenta. These inflammatory processes may contribute to formation of emboli of placental origin that reach the fetal cerebrovasculature through the PFO (38, 40). Further evidence supporting a placental origin of emboli are that an estimated 30% of neonatal stroke is multifocal, even in the absence of CHD and the recurrence of AIS postnatally is exceedingly rare (4). Infarcts were multifocal in 42% of our cohort and to our knowledge, none of the cohort experienced stroke recurrence, although our study is limited by the information available in the medical records. Our study was also limited by the small number in our cohort, the potential for ascertainment bias in the placentas sent for pathologic examination, and the limited outcome data available. Similarly, nearly half of the cohort did not have placental pathologic examination performed, which underscores the selection bias involved in placentas sent for pathology, although our center has a culture of commonly sending placentas to pathology for any indication related to maternal or fetal pregnancy or peripartum risk factors such as pregnancy complications (e.g. maternal diabetes mellitus, fetal growth restriction), or abnormalities during labor or delivery (e.g. perinatal asphyxia, placental abruption).
The suspected pathophysiology of AIS supports the clinical practice of placental pathologic examination in all cases of perinatal stroke (1, 29, 30); however, this retrospective approach is inadequate to change clinical outcomes or prevalence of perinatal stroke. New technologies are required to change perinatal stroke care from a focus on diagnosis and recovery, to one of prevention. This will require creative utilization of what we already know as well as development of new technologies. Recent studies have focused on identifying inflammatory biomarker signatures in patients at-risk for perinatal stroke (41), which may improve the ability to detect perinatal stroke early and allow initiation of supportive therapies sooner. Some experts have recommended more widespread use of neuroimaging in neonates with risk factors for stroke (42), but clear algorithms are still lacking to define which neonates are at highest risk. Placental pathology may provide input into a stroke risk stratification algorithm, but the timeframe required for placental examination will be a limiting factor until new techniques are developed that can offer real-time, clinically-relevant information. In order to establish preventative strategies, advanced methods of in utero assessment are needed, such as the many emerging methods in advanced placental magnetic resonance imaging (43–46).
Inflammatory conditions including maternal infection and fetal asphyxia are often present in patients with perinatal stroke. Placental pathologic examination has a high yield of abnormal findings and should be considered integral to the diagnostic workup in all neonates with perinatal stroke. Imaging or blood biomarkers may eventually play a role in assessing those at risk for perinatal stroke in order to employ timely and effective interventions.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by University of Texas Southwestern Medical Center Institutional Review Board. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Concept: LC, IM, RL. Data Curation: LC, IM. Investigation and Analysis: RL, VK, MA, JT. Drafting, Revising: RL, VK, MA, JT, IM, LC. Final Approval: RL, VK, MA, JT, IM, LC.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ferriero DM, Fullerton HJ, Bernard TJ, Billinghurst L, Daniels SR, DeBaun MR, et al. Management of stroke in neonates and children: A scientific statement from the American heart Association/American stroke association. Stroke (2019) 50(3):e51–96. doi: 10.1161/STR.0000000000000183
2. Hoffman JL, Mack GK, Minich LL, Benedict SL, Heywood M, Stoddard GJ, et al. Failure to impact prevalence of arterial ischemic stroke in pediatric cardiac patients over three decades. Congenital Heart disease (2011) 6(3):211–8. doi: 10.1111/j.1747-0803.2011.00510.x
3. van der Aa NE, Benders MJ, Groenendaal F, de Vries LS. Neonatal stroke: a review of the current evidence on epidemiology, pathogenesis, diagnostics and therapeutic options. Acta paediatrica (2014) 103(4):356–64. doi: 10.1111/apa.12555
4. Kirton A, Armstrong-Wells J, Chang T, Deveber G, Rivkin MJ, Hernandez M, et al. Symptomatic neonatal arterial ischemic stroke: the international pediatric stroke study. Pediatrics (2011) 128(6):e1402–10. doi: 10.1542/peds.2011-1148
5. Elgendy MM, Puthuraya S, LoPiccolo C, Liu W, Aly H, Karnati S. Neonatal stroke: Clinical characteristics and neurodevelopmental outcomes. Pediatr neonatology (2022) 63(1):41–7. doi: 10.1016/j.pedneo.2021.06.017
6. Chabrier S, Peyric E, Drutel L, Deron J, Kossorotoff M, Dinomais M, et al. Multimodal outcome at 7 years of age after neonatal arterial ischemic stroke. J pediatrics (2016) 172:156–61.e3. doi: 10.1016/j.jpeds.2016.01.069
7. Darteyre S, Renaud C, Vuillerot C, Presles E, Kossorotoff M, Dinomais M, et al. Quality of life and functional outcome in early school-aged children after neonatal stroke: a prospective cohort study. Eur J paediatric Neurol EJPN Off J Eur Paediatric Neurol Society (2014) 18(3):347–53. doi: 10.1016/j.ejpn.2014.01.006
8. Dinomais M, Hertz-Pannier L, Groeschel S, Chabrier S, Delion M, Husson B, et al. Long term motor function after neonatal stroke: Lesion localization above all. Hum Brain mapping (2015) 36(12):4793–807. doi: 10.1002/hbm.22950
9. deVeber G, Andrew M, Adams C, Bjornson B, Booth F, Buckley DJ, et al. Cerebral sinovenous thrombosis in children. New Engl J Med (2001) 345(6):417–23. doi: 10.1056/NEJM200108093450604
10. Fitzgerald KC, Williams LS, Garg BP, Carvalho KS, Golomb MR. Cerebral sinovenous thrombosis in the neonate. Arch neurol. (2006) 63(3):405–9. doi: 10.1001/archneur.63.3.405
11. Grunt S, Wingeier K, Wehrli E, Boltshauser E, Capone A, Fluss J, et al. Cerebral sinus venous thrombosis in Swiss children. Dev Med Child neurol. (2010) 52(12):1145–50. doi: 10.1111/j.1469-8749.2010.03722.x
12. Benders MJ, Groenendaal F, Uiterwaal CS, Nikkels PG, Bruinse HW, Nievelstein RA, et al. Maternal and infant characteristics associated with perinatal arterial stroke in the preterm infant. Stroke (2007) 38(6):1759–65. doi: 10.1161/STROKEAHA.106.479311
13. Bruno CJ, Beslow LA, Witmer CM, Vossough A, Jordan LC, Zelonis S, et al. Haemorrhagic stroke in term and late preterm neonates. Arch Dis childhood Fetal neonatal edition (2014) 99(1):F48–53. doi: 10.1136/archdischild-2013-304068
14. Chen J, Zimmerman RA, Jarvik GP, Nord AS, Clancy RR, Wernovsky G, et al. Perioperative stroke in infants undergoing open heart operations for congenital heart disease. Ann Thorac surgery (2009) 88(3):823–9. doi: 10.1016/j.athoracsur.2009.03.030
15. Curry CJ, Bhullar S, Holmes J, Delozier CD, Roeder ER, Hutchison HT. Risk factors for perinatal arterial stroke: a study of 60 mother-child pairs. Pediatr neurol (2007) 37(2):99–107. doi: 10.1016/j.pediatrneurol.2007.04.007
16. Gunther G, Junker R, Strater R, Schobess R, Kurnik K, Heller C, et al. Symptomatic ischemic stroke in full-term neonates : role of acquired and genetic prothrombotic risk factors. Stroke (2000) 31(10):2437–41. doi: 10.1161/01.STR.31.10.2437
17. Laugesaar R, Kolk A, Tomberg T, Metsvaht T, Lintrop M, Varendi H, et al. Acutely and retrospectively diagnosed perinatal stroke: a population-based study. Stroke (2007) 38(8):2234–40. doi: 10.1161/STROKEAHA.107.483743
18. Raju TN, Nelson KB, Ferriero D, Lynch JK, Participants N-NPSW. Ischemic perinatal stroke: summary of a workshop sponsored by the national institute of child health and human development and the national institute of neurological disorders and stroke. Pediatrics (2007) 120(3):609–16. doi: 10.1542/peds.2007-0336
19. Tan M, Deveber G, Shroff M, Moharir M, Pontigon AM, Widjaja E, et al. Sagittal sinus compression is associated with neonatal cerebral sinovenous thrombosis. Pediatrics (2011) 128(2):e429–35. doi: 10.1542/peds.2010-3896
20. Armstrong-Wells J, Ferriero DM. Diagnosis and acute management of perinatal arterial ischemic stroke. Neurol Clin practice (2014) 4(5):378–85. doi: 10.1212/CPJ.0000000000000077
21. Chabrier S, Saliba E, Nguyen The Tich S, Charollais A, Varlet MN, Tardy B, et al. Obstetrical and neonatal characteristics vary with birthweight in a cohort of 100 term newborns with symptomatic arterial ischemic stroke. Eur J paediatric Neurol EJPN Off J Eur Paediatric Neurol Society (2010) 14(3):206–13. doi: 10.1016/j.ejpn.2009.05.004
22. Dunbar M, Kirton A. Perinatal stroke: mechanisms, management, and outcomes of early cerebrovascular brain injury. Lancet Child Adolesc Health (2018) 2(9):666–76. doi: 10.1016/S2352-4642(18)30173-1
23. Fluss J, Dinomais M, Chabrier S. Perinatal stroke syndromes: Similarities and diversities in aetiology, outcome and management. Eur J paediatric Neurol EJPN Off J Eur Paediatric Neurol Society (2019) 23(3):368–83. doi: 10.1016/j.ejpn.2019.02.013
24. Mir IN, Chalak LF, Brown LS, Johnson-Welch S, Heyne R, Rosenfeld CR, et al. Impact of multiple placental pathologies on neonatal death, bronchopulmonary dysplasia, and neurodevelopmental impairment in preterm infants. Pediatr Res (2020) 87(5):885–91. doi: 10.1038/s41390-019-0715-y
25. Leon RL, Mir IN, Herrera CL, Sharma K, Spong CY, Twickler DM, et al. Neuroplacentology in congenital heart disease: placental connections to neurodevelopmental outcomes. Pediatr Res (2022) 91(4):787–94. doi: 10.1038/s41390-021-01521-7
26. Mir IN, Chalak LF, Liao J, Johnson-Welch S, Brown LS, Longoria C, et al. Fetal-placental crosstalk occurs through fetal cytokine synthesis and placental clearance. Placenta (2018) 69:1–8. doi: 10.1016/j.placenta.2018.07.006
27. Fenton TR, Kim JH. A systematic review and meta-analysis to revise the fenton growth chart for preterm infants. BMC Pediatr (2013) 13:59. doi: 10.1186/1471-2431-13-59
28. Khong TY, Mooney EE, Ariel I, Balmus NC, Boyd TK, Brundler MA, et al. Sampling and definitions of placental lesions: Amsterdam placental workshop group consensus statement. Arch Pathol Lab Med (2016) 140(7):698–713. doi: 10.5858/arpa.2015-0225-CC
29. Govaert P, Smith L, Dudink J. Diagnostic management of neonatal stroke. Semin fetal neonatal Med (2009) 14(5):323–8. doi: 10.1016/j.siny.2009.07.007
30. Langston C, Kaplan C, Macpherson T, Manci E, Peevy K, Clark B, et al. Practice guideline for examination of the placenta: developed by the placental pathology practice guideline development task force of the college of American pathologists. Arch Pathol Lab Med (1997) 121(5):449–76. Available at: https://www.proquest.com/scholarly-journals/practice-guideline-examination-placenta/docview/211920353/se-2
31. Roy B, Arbuckle S, Walker K, Morgan C, Galea C, Badawi N, et al. The role of the placenta in perinatal stroke: A systematic review. J Child neurol. (2020) 35(11):773–83. doi: 10.1177/0883073820929214
32. Whitaker EE, Cipolla MJ. Perinatal stroke. Handb Clin Neurol (2020) 171:313–26. doi: 10.1016/B978-0-444-64239-4.00016-3
33. Dunbar M, Mineyko A, Hill M, Hodge J, Floer A, Kirton A. Population based birth prevalence of disease-specific perinatal stroke. Pediatrics (2020) 146(5):e2020013201. doi: 10.1542/peds.2020-013201
34. Wu YW, March WM, Croen LA, Grether JK, Escobar GJ, Newman TB. Perinatal stroke in children with motor impairment: a population-based study. Pediatrics (2004) 114(3):612–9. doi: 10.1542/peds.2004-0385
35. Sorg AL, von Kries R, Klemme M, Gerstl L, Weinberger R, Beyerlein A, et al. Risk factors for perinatal arterial ischaemic stroke: a large case-control study. Dev Med Child neurol. (2020) 62(4):513–20. doi: 10.1111/dmcn.14347
36. Luo L, Chen D, Qu Y, Wu J, Li X, Mu D. Association between hypoxia and perinatal arterial ischemic stroke: a meta-analysis. PLoS One (2014) 9(2):e90106. doi: 10.1371/journal.pone.0090106
37. Elbers J, Viero S, MacGregor D, DeVeber G, Moore AM. Placental pathology in neonatal stroke. Pediatrics (2011) 127(3):e722–9. doi: 10.1542/peds.2010-1490
38. Chabrier S, Sebire G. Perinatal inflammation and placental programming of neonatal stroke. Dev Med Child neurol. (2020) 62(4):413–4. doi: 10.1111/dmcn.14375
39. Leon RL, Sharma K, Mir IN, Herrera CL, Brown SL, Spong CY, et al. Placental vascular malperfusion lesions in fetal congenital heart disease. Am J Obstet Gynecol (2022) S0002-9378(22):00389–1. doi: 10.1016/j.ajog.2022.05.038
40. Fernandez-Lopez D, Natarajan N, Ashwal S, Vexler ZS. Mechanisms of perinatal arterial ischemic stroke. J Cereb Blood Flow Metab Off J Int Soc Cereb Blood Flow Metab (2014) 34(6):921–32. doi: 10.1038/jcbfm.2014.41
41. Mineyko A, Nettel-Aguirre A, de Jesus P, Benseler S, Yusuf K, Narendran A, et al. Association of neonatal inflammatory markers and perinatal stroke subtypes. Neurology (2020) 95(9):e1163–e73. doi: 10.1212/WNL.0000000000010309
42. Xia Q, Yang Z, Xie Y, Zhu Y, Yang Z, Hei M, et al. The incidence and characteristics of perinatal stroke in Beijing: A multicenter study. Front Public Health (2022) 10:783153. doi: 10.3389/fpubh.2022.783153
43. Leon RL, Brown BP, Persohn SA, Norris CD, Steinhardt NP, Lin C, et al. Intravoxel incoherent motion MR imaging analysis for diagnosis of placenta accrete spectrum disorders: A pilot feasibility study. Magn Reson Imaging (2021) 80:26–32. doi: 10.1016/j.mri.2021.03.007
44. Leon RL, Li KT, Brown BP. A retrospective segmentation analysis of placental volume by magnetic resonance imaging from first trimester to term gestation. Pediatr radiol (2018) 48(13):1936–44. doi: 10.1007/s00247-018-4213-x
45. Schlatterer SD, Murnick J, Jacobs M, White L, Donofrio MT, Limperopoulos C. Placental pathology and neuroimaging correlates in neonates with congenital heart disease. Sci Rep (2019) 9(1):4137. doi: 10.1038/s41598-019-40894-y
Keywords: perinatal stroke, placenta, chorioamnionitis, villitis, perinatal asphyxia, vascular malperfusion, neonatal brain, neonatal seizure
Citation: Leon RL, Kalvacherla V, Andrews MM, Thomas JM, Mir IN and Chalak LF (2022) Placental pathologic lesions associated with stroke in term neonates. Front. Endocrinol. 13:920680. doi: 10.3389/fendo.2022.920680
Received: 14 April 2022; Accepted: 17 August 2022;
Published: 08 September 2022.
Edited by:
Ben Nephew, Worcester Polytechnic Institute, United StatesReviewed by:
Philip Katzman, University of Rochester Medical Center, United StatesCopyright © 2022 Leon, Kalvacherla, Andrews, Thomas, Mir and Chalak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rachel L. Leon, UmFjaGVsLkxlb25AVVRTb3V0aHdlc3Rlcm4uZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.