 Shenghui Ge
Shenghui Ge Mengge Yang
Mengge Yang Wenfeng Gong
Wenfeng Gong Wenzhe Chen
Wenzhe Chen Jianjun Dong
Jianjun Dong Lin Liao
Lin Liao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Endocrinol., 05 August 2022
Sec. Clinical Diabetes
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.917819
This article is part of the Research TopicClinical Aspects of Different Forms of Diabetes in Children and AdolescentsView all 9 articles
Background: Maturity-onset diabetes of the young 5 (MODY5), a rare diabetes syndrome of young adults, is associated with variants in hepatocyte nuclear factor 1B (HNF1B) gene.
Case Presentation: We reported a case of MODY5, which presented with diabetic ketosis, multiple renal cysts, and hypokalemia. In this case, the HNF1B score was estimated as 13 and a heterozygous variant of HNF1B in exon 4 (c.826C>T, p.Arg276*) was identified through Sanger sequencing.
Conclusions: Multiple renal cysts and youth-onset diabetes are common manifestations in patients with HNF1B mutations, and insufficient insulin secretion may be a potential cause of diabetic ketosis in MODY5.
Diabetes, as an early adverse factor in many other diseases, has attracted widespread attention, and there is growing evidence that diabetes is a heterogeneous disease affected by genetic and environmental influences. With the maturity of genetic testing technology, single-gene defect diabetes has been continuously discovered, especially maturity-onset diabetes of the young (MODY). Currently, at least 14 genes have been confirmed to be involved in the pathogenesis of MODY, including GCK, HNF1A, HNF1B, HNF4A, PDX1, NEUROD-1, KLF-11, CEL, PAX4, INS, BLK, ABCC8, KCNJ11, and APPL1 (1). Maturity-onset diabetes of the young 5 (MODY5) is expected to account for less than 5% of MODY, which is mainly related to HNF1B gene variation (2). However, there is a large heterogeneity in its clinical manifestations. Therefore, it is necessary for us to expand on the clinical phenotype of MODY5 so that clinicians can better identify this disease. In this report, we describe a MODY5 patient with diabetic ketosis, which provides a basis for the supplement of the MODY5 phenotype.
A 26-year-old Chinese woman was admitted to our hospital, with symptoms of thirst, easy hunger, and polyuria for half a year. She had no nausea, vomiting, diarrhea, abdominal pain, or blurred vision. The patient was 156 cm in height, 37.6 kg in weight, and 15.5 kg/m2 in body mass index (BMI). Physical examination revealed no abnormalities except rapid pulse rate and malnutrition. Laboratory investigations revealed a random blood glucose (RBG) level of 28.9 mmol/L and glycated hemoglobin (HbA1c) value of 17.40%. The erythrocyte sedimentation rate (ESR) level was 10 mm/h and c-reactive protein was less than 3.11 mg/L, both within the normal range. Urine ketone bodies were positive and urine sugar was strongly positive. Therefore, the patient was diagnosed with diabetic ketosis and treated with insulin at a dose of 0.48 U/kg*d as a tentative pharmacotherapy. The patient’s hyperglycemia gradually improved and urine ketones were negative. After that, we performed the relevant examination for the patient (Tables 1 and 2). The results showed that her fasting glucose (FBG) level was 9.08 mmol/L and serum C-peptide and insulin levels were 0.31 nmol/L and 2.03 uIU/mL, and 2-hour postprandial blood glucose level was 9.75 mmol/L and 2-hour postprandial serum C-peptide and 2-hour postprandial insulin levels were 0.26 nmol/L and 1.40 uIU/mL. The patient’s insulin resistance index HOMA-IR was estimated as 0.82. Serum creatinine and esti mated glomerularfiltrationrate (eGFR) were 57.00 umol/L and 129.23, respectively. Serum potassium level was low and serum magnesium level was at the lower limit of normal. As shown in Figure 1, ultra-sonographic examination of the abdomen revealed multiple cysts in both kidneys, the echogenicity of the liver parenchyma was enlarged, and no obvious abnormality was detected in other organs. To determine the pathogenesis of her diabetes, further tests were performed (Table 1). Anti-GAD, anti-IAA and anti-ICA antibodies, unique to type 1 diabetes, were all negative. The patient’s insulin secretion was insufficient, so insulin subcutaneous pump was used and the dose was maintained at 0.38 U/kg*d.
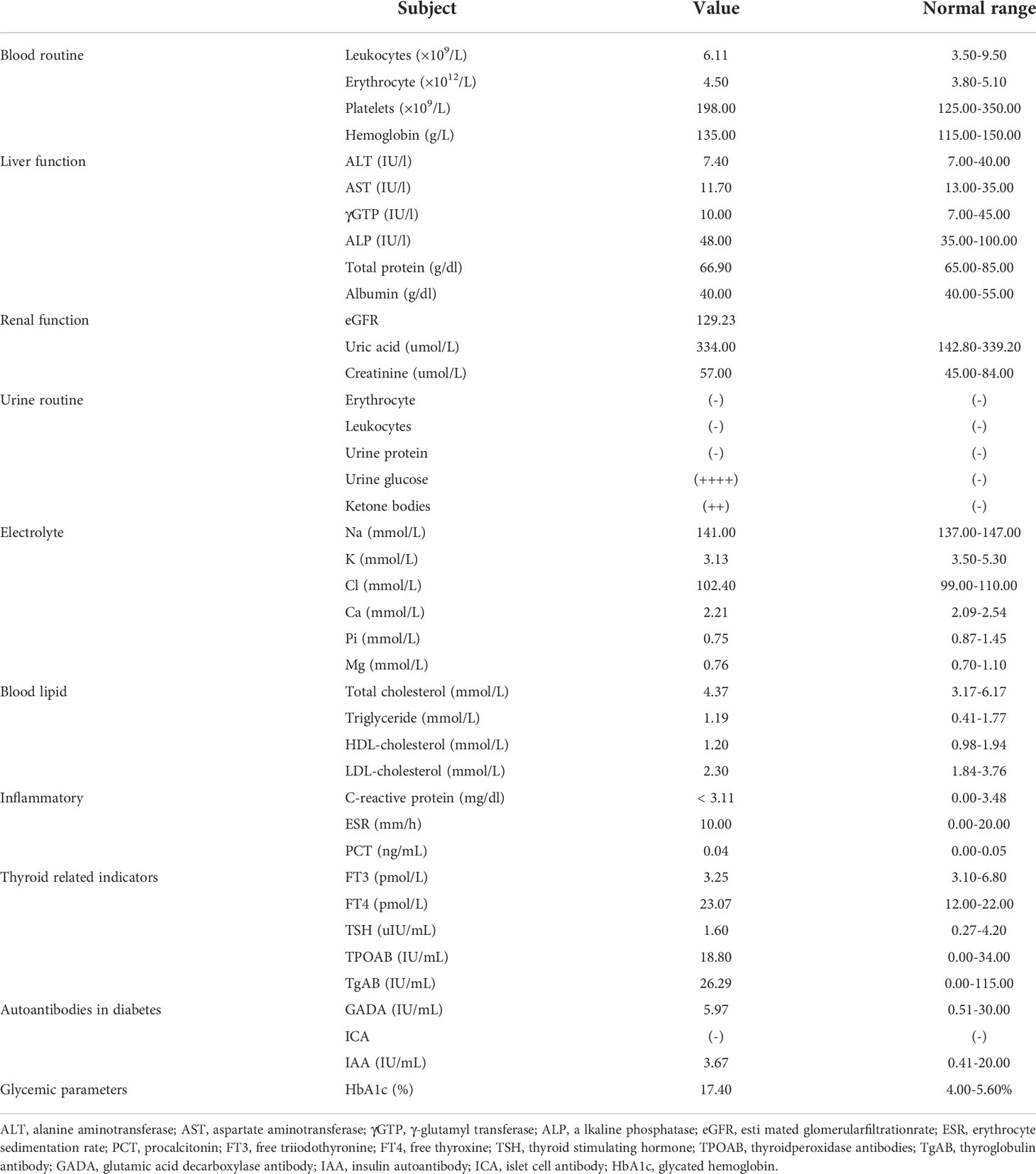
Table 1 Laboratory examinations at the time of admission.

Table 2 Fasting and 2-hour postprandial metabolic indicators.
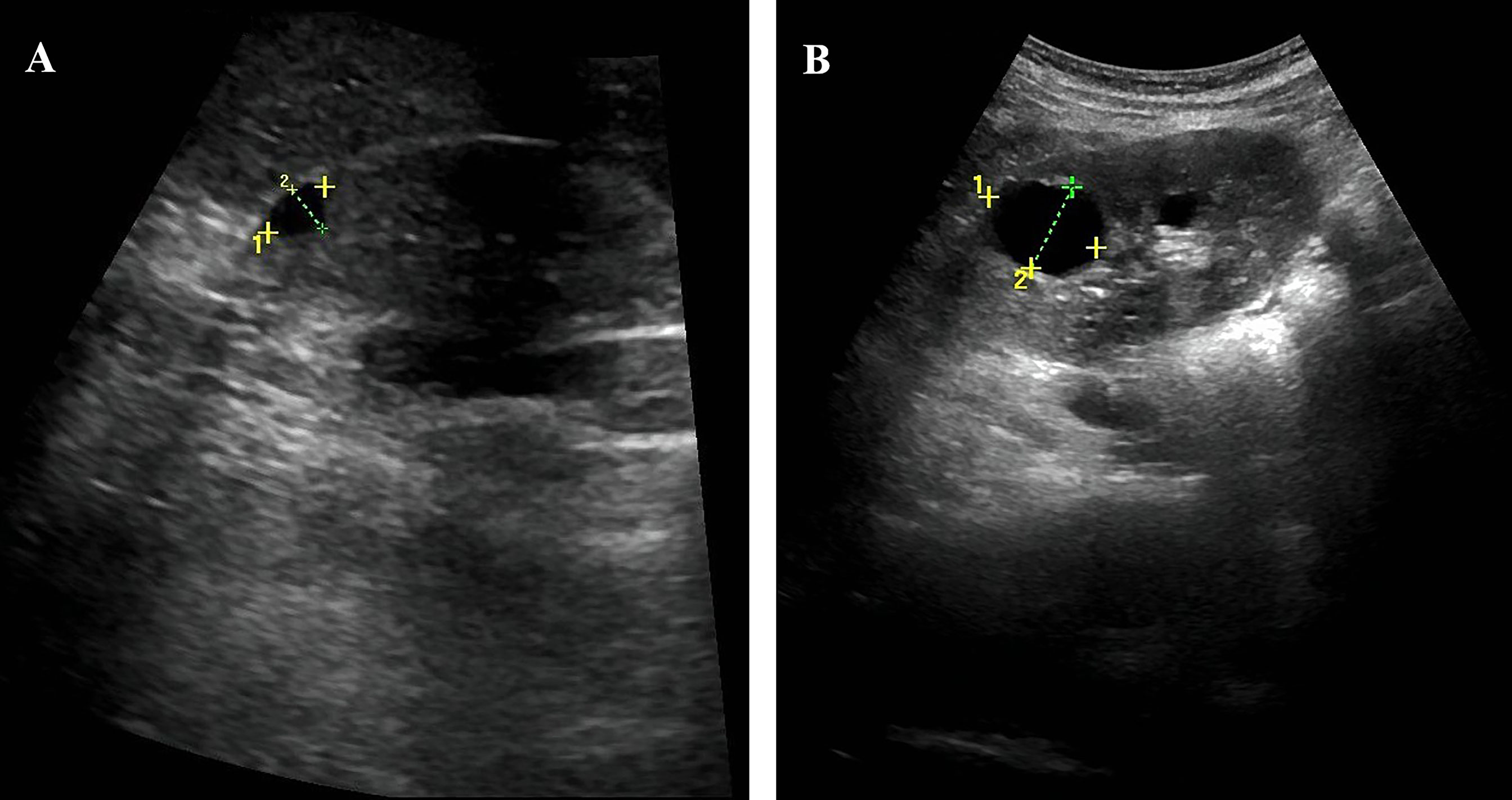
Figure 1 Abdominal ultrasound showed the patient’s kidneys. (A) The patient has multiple cysts in the right kidney, the largest cyst (9*6mm). (B) The patient has multiple cysts in the left kidney, the largest cyst (25*19mm).
Due to the presence of young-onset diabetes, low BMI, multiple renal cysts in both kidneys, insulin secretion dysfunction, and negative diabetes-related antibodies, we suspected the patient to be MODY5 and the HNF1B score was estimated as 13 (Table S1) (3). To further establish definitive diagnosis, genomic DNA was isolated from peripheral blood of the patient, and DNA sequence analysis of the HNF1B gene revealed a heterozygous point mutation (c.826C>T) in 4 exon, leading to a nonsense change of amino acids 276, which changed the amino acid position 276 of the encoded protein from Arg to stop codon (Figure 2). Therefore, the result indicated that our patient was MODY5. This mutation has been reported previously (Table 3).
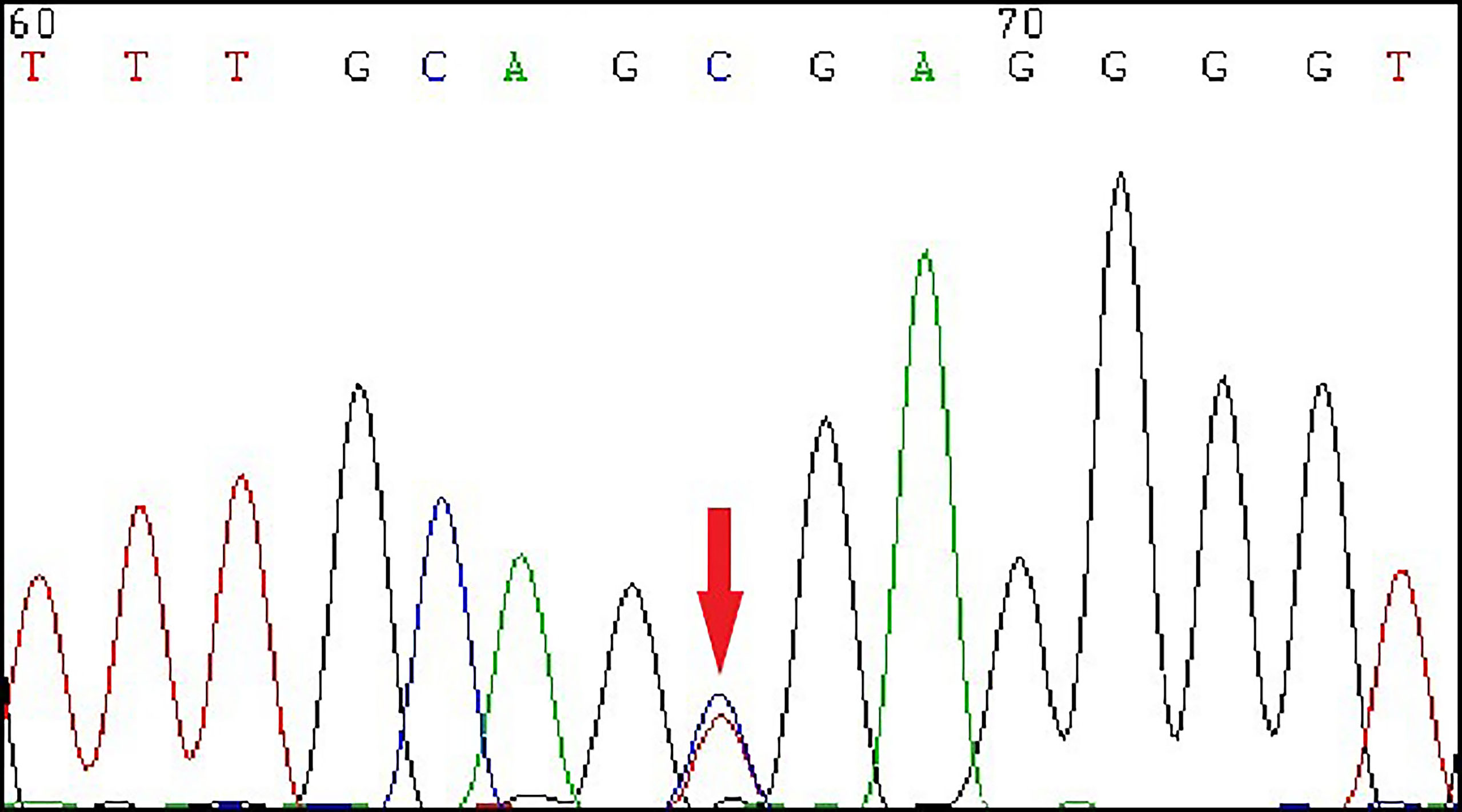
Figure 2 The Sanger sequencing showed a heterozygous mutation of HNF1B gene in exon 4 (c.826C>T, p.Arg276*) of the patient.
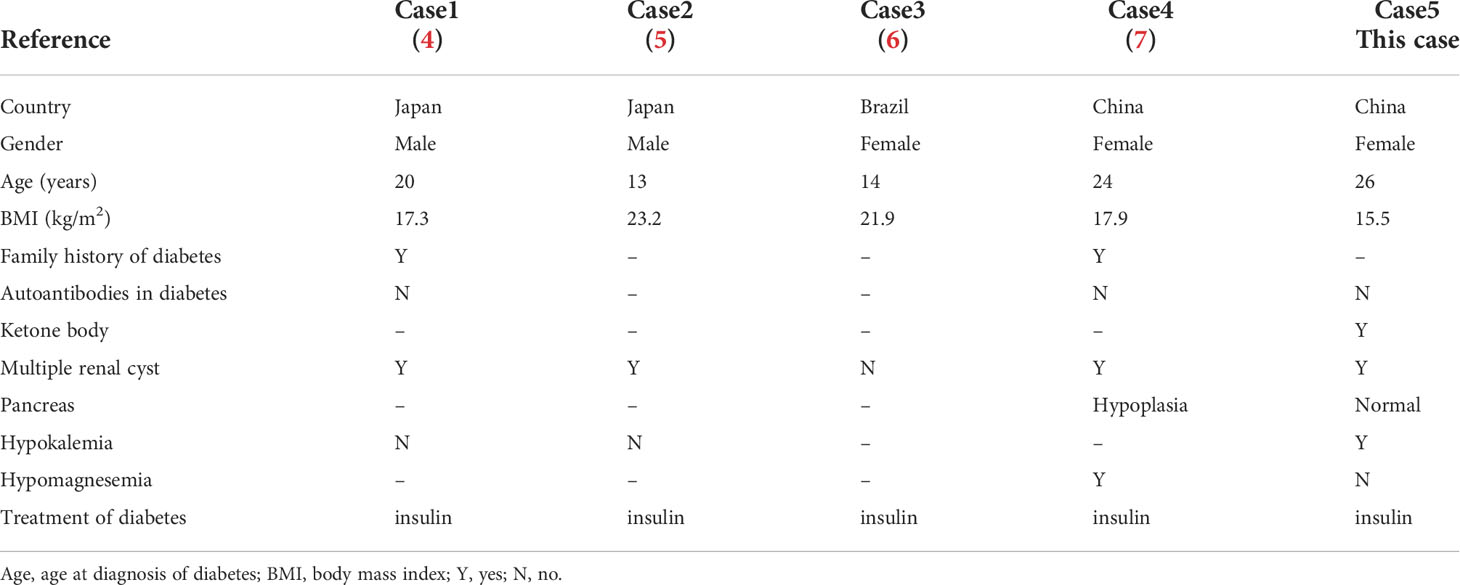
Table 3 Cases of HNF1B mutation (c.826C>T, p.Arg276*) in literature.
After her discharge, insulin subcutaneous pump was used with the basal dosage 2.0 units/d and bolus 4.0, 5.8 and 2.5 units before breakfast, lunch and dinner. She tested her blood glucose frequently. Her levels of fasting glucose were around 4 to 6 mmol/L, post prandial 7 to 10 mmol/L, and the recent HbA1c was 5.1%.
MODY5 is a rare disease characterized by multiple cysts of both kidneys, pancreatic dysplasia, hypomagnesemia, and diabetes in young adults, usually caused by mutations in HNF1B. While this was first reported by Horikawa in 1997, now several 100 mutations have been identified (8, 9). The HNF1B is expressed in the pancreas, liver, and kidney, and plays an important role in the development of multiple tissues (10–12). MODY5 can be classified into 2 entities according to the genetic defect type: patients with a gene deletion and patients with a gene mutation. Patients with HNF1B mutations had a poorer renal prognosis than those with a gene deletion (13).
In our patient, heterozygous point mutation (c.826C>T, p.Arg276*) occurred in exon 4 and diabetic ketosis was the first manifestation. This was the first report of diabetic ketosis in patient with HNF1B mutation (c.826C>T, p.Arg276*). The occurrence of diabetic ketosis might be related to insufficient insulin secretion, which was different from type 1 diabetes in that diabetes-related autoantibodies were negative. While previous reports suggested that pancreatic hypoplasia was often the cause of insufficient insulin secretion in MODY5 patients (14), no overt pancreatic hypoplasia was presented in our patient, suggesting a possible non-pancreatic volume-dependent dysfunction. Notably, although the serum C-peptide levels were below the normal range, it did not reach deficiency. Insulin secretion was still preserved, and if this process persisted, MODY should be suggestive (15). Furthermore, there was no corresponding increase in postprandial C-peptide levels. A possible explanation was that HNF1B mutations might cause dysfunction of the GLUT-2 signaling pathway, resulting in insufficient glucose-stimulated insulin secretion (4). As the effect accumulated, the patient eventually developed diabetic ketosis. However, diabetic ketosis had not been reported in previous cases of HNF1B mutation (c.826C>T, p.Arg276*), and the possible reasons were as follows: First, there was obvious heterogeneity in MODY5 patients, and the clinical manifestations were different among different patients. Second, diabetic ketosis was a rare manifestation of MODY5 (16), which might not have received much attention in previous studies. Finally, there might be a cumulative effect in the development of diabetes and diabetic ketosis, which occurred when the disturbance of glucose metabolism caused by the mutation reached a certain level.
The patient presented with typical polycystic kidney manifestations, which was consistent with previous reports (13). Although studies have shown that patients with the mutation might have worse kidney damage than those with the gene deletion (13), kidney damage was not presented in this patient. Hypokalemia was also presented in this patient, and previous studies have shown that hypokalemia occurs in approximately half of adults with HNF1B mutations (17). HNF1B can directly regulate the transcription of genes related to renal K+ processing and can regulate the transcription of K+ channel proteins (12). Dysregulation of multiple transporters might contribute to hypokalemia. In addition, hypomagnesemia was also a common presentation in MODY5 patients, often due to renal magnesium loss (18). The degree of hypomagnesemia varied across age groups in patients with HNF1B mutations, and previous studies have shown that hypomagnesemia develops with increasing age (19). Therefore, although the patient’s current serum magnesium was within the normal range, regular monitoring of serum electrolytes was still necessary.
Insulin was the main recommended treatment agent for MODY5 patients, especially when HNF1B mutation (c.826C>T, p.Arg276*) occurred. Although some patients might be independent of insulin in the early stage (5), it should be noted that this mutation might lead to potential insulin secretion defects. Therefore, when MODY5 was suspected, pancreatic function should be evaluated and inappropriate drug should be avoided.
In conclusion, we report a MODY5 patient with onset of diabetic ketosis in whom we identified a nonsense mutation at exon 4 of the HNF1B gene. Multiple renal cysts and youth-onset diabetes are common manifestations in patients with HNF1B mutations, and insufficient insulin secretion might be a potential cause of diabetic ketosis in MODY5. Our findings provide a new complement to the phenotype of MODY5 and bring more attention to patients with diabetic ketosis.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
SG: Data extraction, Data analysis, Essay writing, and Paper submission. MY, WG and WC: Data extraction. JD and LL: Critical revision and Paper submission. All authors contributed to the article and approved the submitted version.
This work was funded by the National Natural Science Foundation of China (82170847).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.917819/full#supplementary-material
1. Urakami T. Maturity-onset diabetes of the young (Mody): Current perspectives on diagnosis and treatment. Diabetes Metab Syndrome Obes Targets Ther (2019) 12:1047–56. doi: 10.2147/dmso.S179793
2. Firdous P, Nissar K, Ali S, Ganai BA, Shabir U, Hassan T, et al. Genetic testing of maturity-onset diabetes of the young current status and future perspectives. Front Endocrinol (2018) 9:253. doi: 10.3389/fendo.2018.00253
3. Faguer S, Chassaing N, Bandin F, Prouheze C, Garnier A, Casemayou A, et al. The Hnf1b score is a simple tool to select patients for Hnf1b gene analysis. Kidney Int (2014) 86(5):1007–15. doi: 10.1038/ki.2014.202
4. Fujimoto K, Sasaki T, Hiki Y, Nemoto M, Utsunomiya Y, Yokoo T, et al. In vitro and pathological investigations of Mody5 with the R276x-Hnf1beta (Tcf2) mutation. Endocrine J (2007) 54(5):757–64. doi: 10.1507/endocrj.k07-051
5. Furuta H, Furuta M, Sanke T, Ekawa K, Hanabusa T, Nishi M, et al. Nonsense and missense mutations in the human hepatocyte nuclear factor-1 beta gene (Tcf2) and their relation to type 2 diabetes in Japanese. J Clin Endocrinol Metab (2002) 87(8):3859–63. doi: 10.1210/jcem.87.8.8776
6. Abreu GM, Tarantino RM, da Fonseca ACP, Andrade J, de Souza RB, Soares C, et al. Identification of variants responsible for monogenic forms of diabetes in Brazil. Front Endocrinol (2022) 13:827325. doi: 10.3389/fendo.2022.827325
7. Zhao SL, Long Q, Liu SP, Qin TT, Jin P. A case report of young adult-onset diabetes mellitus type 5 caused by p.R276* mutation in hepatocyte nuclear factor 1b gene. Chin J Diabetes (2021) 29(1):63–6. doi: 10.3969/j.issn.1006-6187.2021.01.012
8. Horikawa Y, Iwasaki N, Hara M, Furuta H, Hinokio Y, Cockburn BN, et al. Mutation in hepatocyte nuclear factor-1 beta gene (Tcf2) associated with mody. Nat Genet (1997) 17(4):384–5. doi: 10.1038/ng1297-384
9. Çubuk H, Yalçın Çapan Ö. A review of functional characterization of single amino acid change mutations in hnf transcription factors in mody pathogenesis. Protein J (2021) 40(3):348–60. doi: 10.1007/s10930-021-09991-8
10. Barbacci E, Reber M, Ott MO, Breillat C, Huetz F, Cereghini S. Variant hepatocyte nuclear factor 1 is required for visceral endoderm specification. Dev (Cambridge England) (1999) 126(21):4795–805. doi: 10.1242/dev.126.21.4795
11. Chan SC, Zhang Y, Shao A, Avdulov S, Herrera J, Aboudehen K, et al. Mechanism of fibrosis in Hnf1b-related autosomal dominant tubulointerstitial kidney disease. J Am Soc Nephrol JASN (2018) 29(10):2493–509. doi: 10.1681/asn.2018040437
12. Ferrè S, Igarashi P. New insights into the role of hnf-1β in kidney (Patho)Physiology. Pediatr Nephrol (Berlin Germany) (2019) 34(8):1325–35. doi: 10.1007/s00467-018-3990-7
13. Dubois-Laforgue D, Cornu E, Saint-Martin C, Coste J, Bellanné-Chantelot C, Timsit J. Response to comment on dubois-laforgue et al. diabetes, associated clinical spectrum, long-term prognosis, and Genotype/Phenotype correlations in 201 adult patients with hepatocyte nuclear factor 1b (Hnf1b) molecular defects. Diabetes Care (2017) 40:1436–43. doi: 10.2337/dci17-0048
14. Haldorsen IS, Vesterhus M, Raeder H, Jensen DK, Søvik O, Molven A, et al. Lack of pancreatic body and tail in Hnf1b mutation carriers. Diabetic Med J Br Diabetic Assoc (2008) 25(7):782–7. doi: 10.1111/j.1464-5491.2008.02460.x
15. Jones AG, Hattersley AT. The clinical utility of c-peptide measurement in the care of patients with diabetes. Diabetic Med J Br Diabetic Assoc (2013) 30(7):803–17. doi: 10.1111/dme.12159
16. Haaland WC, Scaduto DI, Maldonado MR, Mansouri DL, Nalini R, Iyer D, et al. A-Beta-Subtype of ketosis-prone diabetes is not predominantly a monogenic diabetic syndrome. Diabetes Care (2009) 32(5):873–7. doi: 10.2337/dc08-1529
17. Faguer S, Decramer S, Chassaing N, Bellanné-Chantelot C, Calvas P, Beaufils S, et al. Diagnosis, management, and prognosis of Hnf1b nephropathy in adulthood. Kidney Int (2011) 80(7):768–76. doi: 10.1038/ki.2011.225
18. Ferrè S, Veenstra GJ, Bouwmeester R, Hoenderop JG, Bindels RJ. Hnf-1b specifically regulates the transcription of the Γa-subunit of the Na+/K+-atpase. Biochem Biophys Res Commun (2011) 404(1):284–90. doi: 10.1016/j.bbrc.2010.11.108
Keywords: MODY5, HNF1B, case, mutation, diagnosis, renal cysts and diabetes syndrome
Citation: Ge S, Yang M, Gong W, Chen W, Dong J and Liao L (2022) Case Report: A case of HNF1B mutation patient with first presentation of diabetic ketosis. Front. Endocrinol. 13:917819. doi: 10.3389/fendo.2022.917819
Received: 11 April 2022; Accepted: 19 July 2022;
Published: 05 August 2022.
Edited by:
Stefano Zucchini, Sant’Orsola-Malpighi Polyclinic, ItalyReviewed by:
Sarah Alam, NMC Specialty Hospital, United Arab EmiratesCopyright © 2022 Ge, Yang, Gong, Chen, Dong and Liao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lin Liao, bGlhb2xpbkBzZHUuZWR1LmNu; Jianjun Dong, ZG9uZ2ppYW5qdW5Ac2R1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.