
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 08 July 2022
Sec. Pediatric Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.909201
This article is part of the Research Topic Childhood Obesity: Prevention, Management and New Insight in Pathophysiology View all 14 articles
 Rocío Escartín1
Rocío Escartín1 Maria Font1José Miguel González-Clemente2Joan Vendrell3,4Assumpta Caixàs2
Maria Font1José Miguel González-Clemente2Joan Vendrell3,4Assumpta Caixàs2 Raquel Corripio1*
Raquel Corripio1*Objective: Obesity is characterized by a low-grade inflammatory state in adipose tissue. Tumor Necrosis Factor Weak Inducer of Apoptosis (TWEAK) and Cluster of Differentiation 163 (CD163) are cytokines potentially involved in the pathogenesis of obesity. Little is known about them in children. The aim of this study was to observe serum levels of TWEAK and CD163 in prepubertal children with obesity compared to lean, and to evaluate its changes after a 2-year intervention program in children with obesity.
Methods: Case-control study with a prospective follow-up of cases for 2 years in a referral pediatric endocrine outpatient centre. Seventy-three prepubertal children with obesity, and forty-seven age- and gender-matched lean controls were studied. Sixty-two cases finished the program. Anthropometric parameters, Homeostatic Model Assessment for Insulin Resistance (HOMA-IR), lipid profile, and concentrations of TWEAK and CD163 were determined. Children with obesity were re-evaluated after a 2-year intervention program consisting of diet and exercise. Weight loss was considered if z-score Body Mass Index (BMI) decreased at least 0.5 Standard Deviations (SD).
Results: We observed higher CD163 levels in children with obesity compared to controls. No significant differences were observed in TWEAK and CD163/TWEAK ratio at baseline. After the 2-year intervention program, TWEAK levels were higher and CD163/TWEAK ratio was lower in children with weight loss than those without weight loss. CD163 decreased in both groups.
Conclusion: TWEAK and CD163 seem to have a role in the pathogenesis of obesity in prepubertal children.
The prevalence of childhood obesity has increased dramatically in recent decades, becoming a global public health problem (1). Pathological conditions associated with obesity, such as diabetes, hyperlipidemia, or hypertension (2), have been observed mainly in adults. As the prevalence of childhood obesity increases, these conditions are becoming more common among infants and teenagers (3–8).
Obesity is associated with a chronic inflammatory state in adipose tissue (9–11). In this context, we can observe altered levels of molecules involved in the regulation of inflammation, called cytokines (12–14).
Research on cytokines has increased during the last years in order to identify risk and protective factors of cardiovascular disease and to generate potential target treatments (15, 16).
Tumor Necrosis Factor Weak Inducer of Apoptosis (TWEAK), also known as Tumor Necrosis Factor (TNF) ligand superfamily member 12, is a cytokine involved in multiple biological functions (12, 17, 18). It seems to play a protective role in the regulation of obesity and insulin resistance (15, 19, 20). It was observed that serum levels of soluble TWEAK are lower in adults with severe obesity, and they increase in these patients after a significant weight loss (21).
Cluster of Differentiation 163 (CD163) is a macrophage-specific protein that increases in the context of inflammation (22). In vitro, it has been identified as a scavenger receptor of TWEAK, promoting its degradation (23). Serum levels of CD163 are higher in obesity and insulin resistance, being a strong predictor of type 2 diabetes in adults (24). In cardiovascular diseases, a high CD163/TWEAK ratio was found (25).
Little is known about TWEAK and CD163 in children. The main objective of the study was to evaluate if a significant weight loss in children with obesity may induce changes in these parameters after a 2-year lifestyle intervention program. In addition, the investigation aimed to evaluate serum levels of TWEAK, CD163, and CD163/TWEAK ratio in prepubertal children with obesity compared to lean children.
Seventy-three prepubertal children with obesity were included, from an outpatient long-term intervention program over a period of 2 years. Inclusion criteria were the presence of obesity as defined by body mass index (BMI) > 2 standard deviation (SD) scores for age and sex upon Spanish normative charts (26), aged between 6 and 10 years and prepubertal according to Tanner staging (27, 28). Controls were forty-seven prepubertal healthy children attending for preoperative blood tests before minor surgery. They were matched by age and gender. Exclusion criteria were the presence of endocrinopathies, obesity-associated syndrome, and any infectious or inflammatory disease in the past 10 days, or taking medication that affected weight, lipid metabolism, or arterial blood pressure (BP). Written informed consent was obtained from all patients’ parents, and all investigations followed the Helsinki Declaration. The study was approved by the Ethics Committee of our Institution (reference code 2004104).
Detailed medical, personal, and family history of obesity and cardiometabolic risk was obtained from all subjects, including birth weight and length for gestational age. A complete physical examination was performed. Height was measured by a Harpenden stadiometer to the nearest 0.1 cm and body weight by balance scale to the nearest 0.1 kg. Waist circumference was measured with a tape at the middle point between the last rib and the superior iliac crest, adjusted to the nearest 0.1 cm, and compared with an age and sex-reference population (29). All measurements were performed for duplication by the same investigator, with the patient in light clothes and without shoes. The mean of the two determinations was used for calculations. Adiposity was evaluated by BMI (calculated as weight in kilograms divided by the square of height in meters). Pubertal development was assessed by direct physical examination according to Tanner staging. Blood pressure was measured by triplicate with the Critikon Dinamap 8100 automatic system (Johnson-Johnson Company, Tampa, FL, USA), with an appropriate sized cuff and after at least ten minutes resting in supine position. The lowest BP value was recorded and evaluated using the percentiles of the International Task Force for Blood Pressure (30).
Obesity degree was fixed with z-BMI using the LMS method (31). We also applied the obesity criteria by Cole (International Obesity Task Force) (32) to our BMI data.
Blood samples were obtained after a 12-hours overnight fast. Concentrations of soluble TWEAK, soluble CD163, alanine aminotransferase (ALT), uric acid, glucose, insulin, cholesterol and triglycerides were determined. Likewise, a standard 2-hours oral glucose tolerance test was performed in subjects with obesity.
Samples were stored at -80°C until their analysis. Plasma glucose was measured by the glucose hexokinase method, insulin by an electrochemiluminescent method, cholesterol and its fractions by cholesterol esterase/oxidase, and triglycerides by lipase/glycerol kinase (Roche Diagnostics, Mannheim, Germany). Intra- and inter-assay coefficient of variation (CV) values were 1.9–2.1% for glucose and 2.6–2.8% for insulin, respectively.
Plasma soluble TWEAK was measured by an enzyme-linked immunoassay (ELISA) technique with a sensitivity of 0.02 pg/mL (intra-assay CV <10%, inter-assay CV <9%). Plasma soluble CD163 was measured by ELISA with a sensitivity of 0.1 ng/mL (intra-assay CV <6%, inter-assay CV <7%). Impaired glucose metabolism was defined according to the American Diabetes Association criteria (33). Insulin resistance was evaluated using the Homeostatic Model Assessment for Insulin Resistance (34).
After the baseline evaluation, 73 prepubertal children with obesity started a lifestyle intervention program that included a balanced norm caloric diet adjusted by age and a personally adapted exercise program. The diet contained 30% of energy intake from fat, 15% from protein, and 55% from carbohydrate (5% as sugar). A plan of 30–45 minutes of moderate exercise three times a week was negotiated. Television and video games were limited to a maximum of 2 hours a day. Follow-up visits were scheduled every 4 months.
After 2 years, a clinical and metabolic evaluation was performed with the same parameters as in the baseline evaluation. We considered a significant weight loss if the z-score of BMI had decreased at least 0.5 SD (35).
Data were expressed as mean ± SD for quantitative variables and as percentages for categorical variables. Logarithmic transformation before the analysis was used when variables did not follow a normal distribution. Student’s t-test or Mann-Whitney U test were used for comparing differences between groups. Paired t-test or Wilcoxon test was used to compare variables before and after the intervention program. Bivariate correlations were evaluated with Pearson’s and Spearman’s coefficients as appropriate. Furthermore, some multivariate linear regression models were used. TWEAK, CD163 or CD163/TWEAK ratio as dependent variables and age, sex, weight status (BMI), HOMA-IR and lipid profile, as independent variables. A p value < 0.05 was considered significant. Analyses were performed with SAS v9.4, SAS Institute Inc., Cary, NC, USA.
73 children with obesity and 47 controls were included in the study. Characteristics of subjects are shown in Table 1. Comparing cases and controls, CD163 levels were higher in children with obesity. No statistically significant differences were found in TWEAK and CD163/TWEAK ratio.
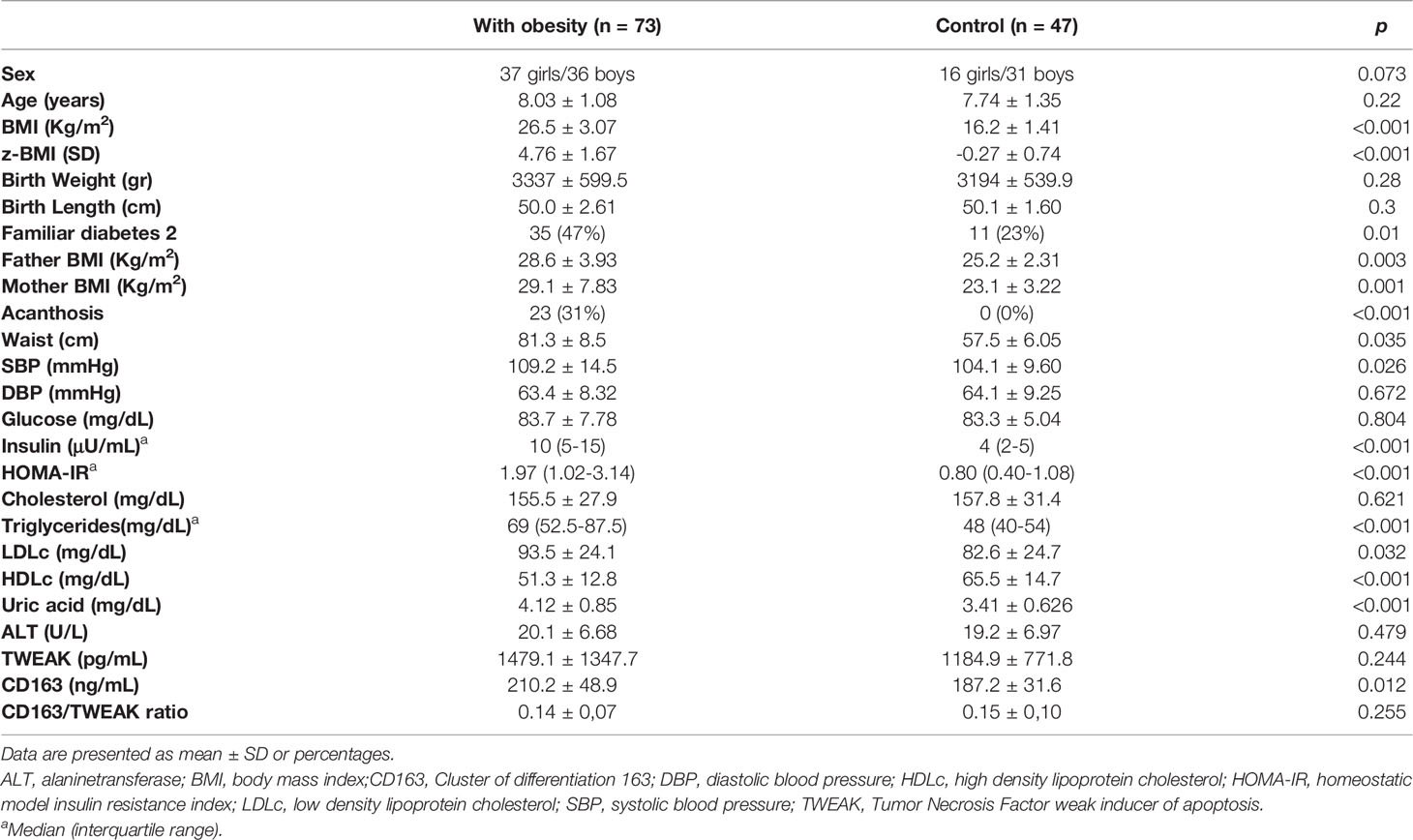
Table 1 Baseline Subjects Characteristics.
After a 2-year follow-up of the cases, 62 completed the study and 11 dropped out (15%). 31 patients achieved a significant weight loss. Comparing patients with and without weight loss after the intervention program, TWEAK decreased in both groups after the intervention program. However, we observed that this parameter was higher in patients who achieved weight loss, before and after the intervention program. Serum levels of CD163 decreased after 2 years in both groups, and the decrease was more pronounced in patients with weight loss (Figure 1). CD163/TWEAK ratio was higher in children without weight loss, and it increased after 2 years in this group (Figure 2). Data are shown in Table 2.

Figure 1 CD163 decreased after 2 years in both groups, and the decrease was more pronounced in patients with weight loss.
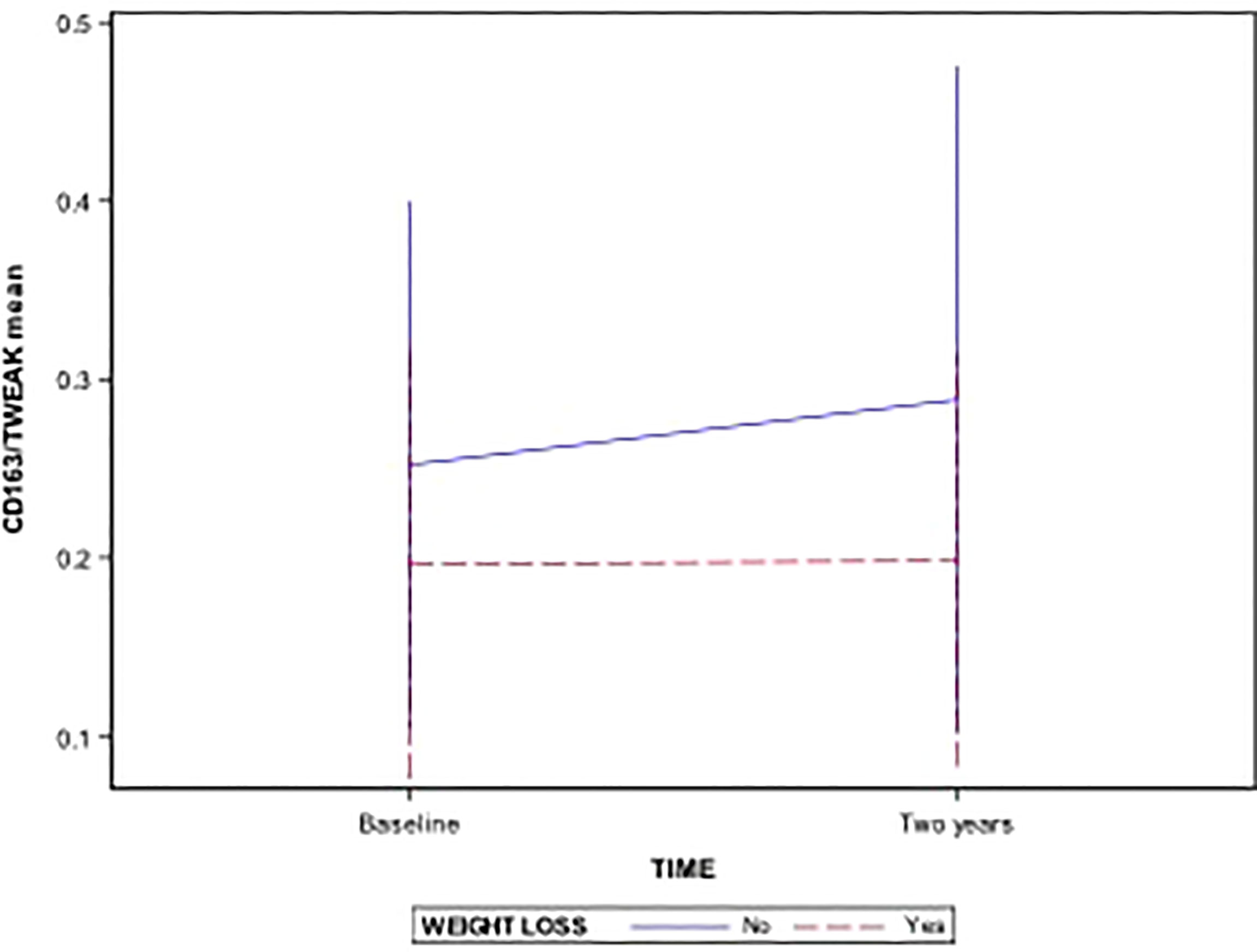
Figure 2 CD163/TWEAK ratio was higher in children without weight loss, and it increased after 2 years in this group.
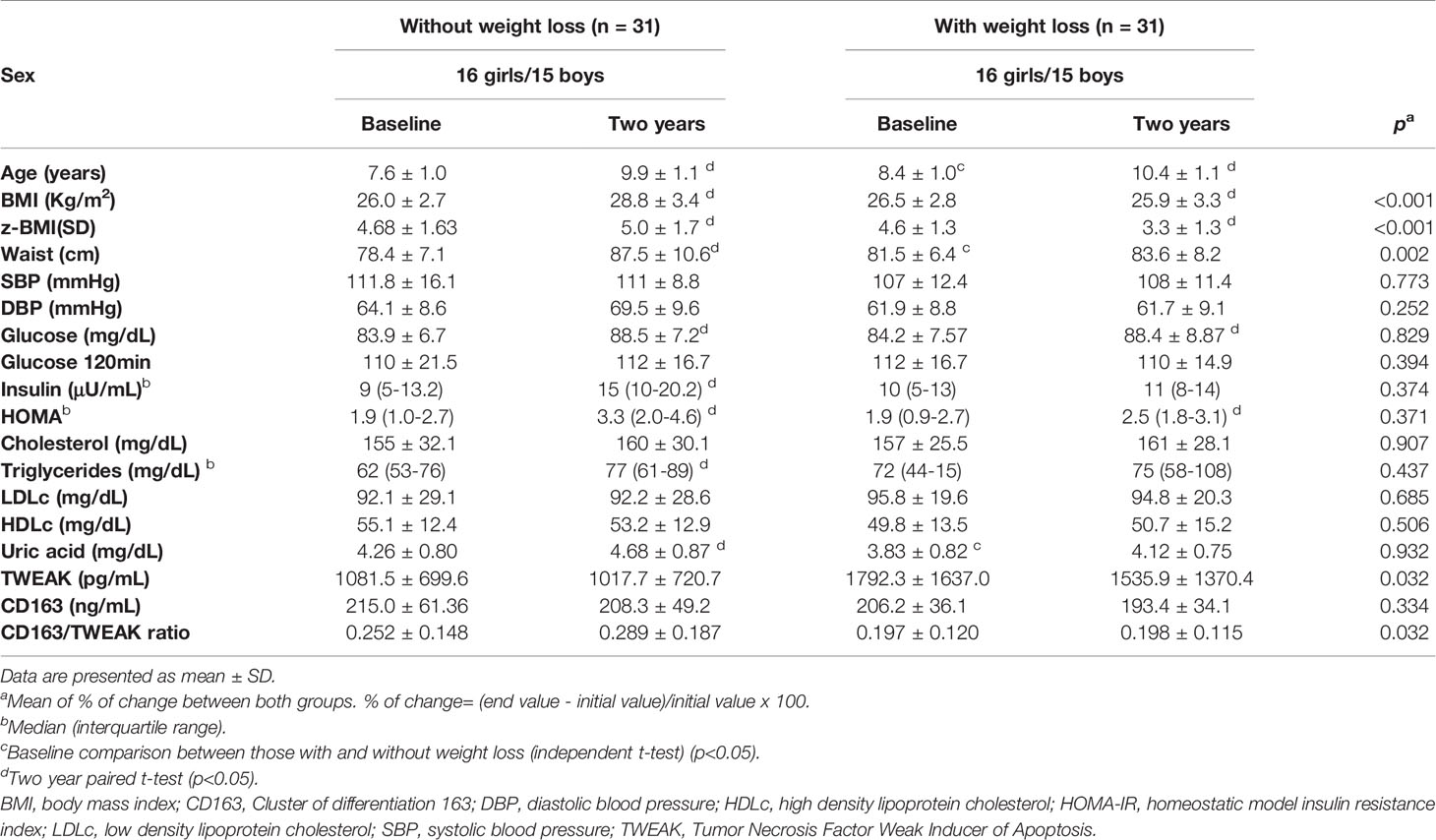
Table 2 Baseline and after 2-years follow up characteristics according to weight loss in children with obesity.
To further understand the relationship between TWEAK and CD163 and the rest of the variables, we carried out some bivariate correlation analysis with each of them. Age, sex, HOMA, and lipid profile were included as independent variables. No significant correlation among all these variables was found.
Forty-nine percent of the patients began puberty (assessed by Tanner stage) during the follow-up phase. After adjusting the regression model by Tanner, results were not modified.
TWEAK and CD163 have been linked to obesity and associated cardiovascular diseases in adults (15). However, there are still few data about these cytokines in children.
Our investigation did not find statistically significant differences in TWEAK or CD163/TWEAK ratio of children with obesity compared to controls. A possible explanation for this might be that this cytokine is involved in processes such as cell proliferation and differentiation (36), present in childhood growth. The protective role of TWEAK in obesity is not demonstrated in prepubertal children, although some studies observed an anti-inflammatory role of this cytokine in obese adults (25, 37).
Regarding CD163, this cytokine is higher in adults with obesity, and known as a biomarker of insulin resistance (23). Carolan et al. observed elevated CD163 in children with obesity, suggesting that it could be a biomarker to prioritize lifestyle intervention in childhood (38). In our study, CD163 serum levels were also higher in children with obesity compared to lean.
The present study is the first to observe a favorable effect of a 2-year lifestyle intervention program in prepubertal children who achieved a significant weight loss compared with those who did not. We observed expected higher levels of TWEAK, lower CD163/TWEAK ratio, and a more pronounced decrease of CD163 in the group of patients who achieved weight loss.
This study is the first one to observe the evolution of these parameters in prepubertal children, supporting the hypotheses that these cytokines may play a role in childhood obesity. One study found similar results in adults with severe obesity after weight loss achieved by bariatric surgery (25). Kazankov et al. observed a decrease in CD163 after 10 weeks of a lifestyle intervention in children with a mean age of 12 years (39).
This research has some limitations. It has a weak external validity because all subjects were only from one center. However, inclusion criteria for subjects are enough to guarantee a strong internal validity in our results. Unfortunately we don’t have estradiol, testosterone levels or TWEAK evolution of control group after two years of follow-up.
Our findings show that TWEAK and CD163 may be involved in the pathogenesis of obesity in prepubertal children. Childhood is a necessary stage for the prevention of consequences derived from obesity. This study opens an interesting line of research aimed at this objective.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by CEIC from FUNDACIÓ INSTITUT D’INVESTIGACIÓ I INNOVACIÓ PARC TAULÍ (I3PT). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
AC, RC, and JG-C conceived the study. RC obtained informed consent and clinical variables. JV analyzed samples. MF and RE performed literature search. All authors were involved in writing the paper and had final approval of the submitted and published versions.
This project was supported by a grant from Fundació Parc Taulí 2004104.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank John Giba for his assistance in language editing.
1. Bendor CD, Bardugo A, Pinhas-Hamiel O, Afek A, Twig G. Cardiovascular Morbidity, Diabetes and Cancer Risk Among Children and Adolescents With Severe Obesity. Cardiovasc Diabetol (2020) 19(1):79. doi: 10.1186/s12933-020-01052-1
2. Pasquali R, Casanueva F, Haluzik M, van Hulsteijn L, Ledoux S, Monteiro MP, et al. European Society of Endocrinology Clinical Practice Guideline: Endocrine Work-Up in Obesity. Eur J Endocrinol (2020) 182(1):G1–G32. doi: 10.1530/EJE-19-0893
3. Thota P, Perez-Lopez FR, Benites-Zapata VA, Pasupuleti V, Hernandez AV. Obesity-Related Insulin Resistance in Adolescents: A Systematic Review and Meta-Analysis of Observational Studies. Gynecol Endocrinol (2017) 33(3):179–84. doi: 10.1080/09513590.2016.1273897
4. Weiss R, Dziura J, Burgert T, Tamborlane W, Taksali S, Yeckel C, et al. Obesity and the Metabolic Syndrome in Children and Adolescents. N Engl J Med (2004) 350(23):2362–74. doi: 10.1056/NEJMoa031049
5. Sinha R, Fisch G, Teague B, Tamborlane W, Banyas B, Allen K, et al. Prevalence of Impaired Glucose Tolerance Among Children and Adolescents With Marked Obesity. N Engl J Med (2002) 346(11):802–10. doi: 10.1056/NEJMoa012578
6. Wiegand S, Maikowski U, Blankenstein O, Biebermann H, Tarnow P, Grüters A. Type 2 Diabetes and Impaired Glucose Tolerance in European Children and Adolescents With Obesity – A Problem That Is No Longer Restricted to Minority Groups. Eur J Endocrinol (2004) 151(2):199–206. doi: 10.1530/eje.0.1510199
7. Lobstein T, Jackson-Leach R. Estimated Burden of Paediatric Obesity and Co-Morbidities in Europe. Part 2. Numbers of Children With Indicators of Obesity-Related Disease. Int J Pediatr Obes (2006) 1(1):33–41. doi: 10.1080/17477160600586689
8. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of Potentially Modifiable Risk Factors Associated With Myocardial Infarction in 52 Countries (The INTERHEART Study): Case-Control Study. Lancet (2004) 364(9438):937–52. doi: 10.1016/S0140-6736(04)17018-9
9. Karczewski J, Śledzińska E, Baturo A, Jończyk I, Maleszko A, Samborski P, et al. Obesity and Inflammation. Eur Cytokine Netw (2018) 29(3):83–94. doi: 10.1684/ecn.2018.0415
10. Rohm TV, Meier DT, Olefsky JM, Donath MY. Inflammation in Obesity, Diabetes, and Related Disorders. Immunity (2022) 55(1):31–55. doi: 10.1016/j.immuni.2021.12.013
11. Khafagy R, Dash S. Obesity and Cardiovascular Disease: The Emerging Role of Inflammation. Front Cardiovasc Med (2021) 8. doi: 10.3389/fcvm.2021.768119
12. Escoté X, Gómez-Zorita S, López-Yoldi M, Milton-Laskibar I, Fernández-Quintela A, Martínez JA, et al. Role of Omentin, Vaspin, Cardiotrophin-1, TWEAK and NOV/CCN3 in Obesity and Diabetes Development. Int J Mol Sci (2017) 18(8):1770. doi: 10.3390/ijms18081770
13. Blaszczak AM, Jalilvand A, Hsueh WA. Adipocytes, Innate Immunity and Obesity: A Mini-Review. Front Immunol (2021) 12. doi: 10.3389/fimmu.2021.650768
14. Barakat B, Almeida MEF. Biochemical and Immunological Changes in Obesity. Arch Biochem Biophys (2021) 708:108951. doi: 10.1016/j.abb.2021.108951
15. Vendrell J, Chacón MR. TWEAK: A New Player in Obesity and Diabetes. Front Immunol (2013) 4. doi: 10.3389/fimmu.2013.00488
16. Corripio R, Gónzalez-Clemente JM, Pérez-Sánchez J, Näf S, Gallart L, Nosàs R, et al. Weight Loss in Prepubertal Obese Children is Associated With a Decrease in Adipocyte Fatty-Acid-Binding Protein Without Changes in Lipocalin-2: A 2-Year Longitudinal Study. Eur J Endocrinol (2010) 163(6):887–93. doi: 10.1530/EJE-10-0408
17. Yepes M, Winkles JA. Inhibition of TWEAK Activity as a New Treatment for Inflammatory and Degenerative Diseases. Drug News Perspect (2006) 19(10):589–95. doi: 10.1358/dnp.2006.19.10.1068005
18. Tiller G, Fischer-Posovszky P, Laumen H, Finck A, Skurk T, Keuper M, et al. Effects of TWEAK (TNF Superfamily Member 12) on Differentiation, Metabolism, and Secretory Function of Human Primary Preadipocytes and Adipocytes. Endocrinology (2009) 150(12):5373–83. doi: 10.1210/en.2009-0488
19. Chacón MR, Richart C, Gómez JM, Megía A, Vilarrasa N, Fernández-Real JM, et al. Expression of TWEAK and its Receptor Fn14 in Human Subcutaneous Adipose Tissue. Relationship With Other Inflammatory Cytokines in Obesity. Cytokine (2006) 33(3):129–37. doi: 10.1016/j.cyto.2005.12.005
20. Díaz-López A, Chacón MR, Bulló M, Maymó-Masip E, Martínez-González MA, Estruch R, et al. Serum sTWEAK Concentrations and Risk of Developing Type 2 Diabetes in a High Cardiovascular Risk Population: A Nested Case-Control Study. J Clin Endocrinol Metab (2013) 98(8):3482–90. doi: 10.1210/jc.2013-1848
21. Maymó-Masip E, Fernández-Veledo S, Garcia España A, Vázquez-Carballo A, Tinahones FJ, García-Fuentes E, et al. The Rise of Soluble TWEAK Levels in Severely Obese Subjects After Bariatric Surgery may Affect Adipocyte-Cytokine Production Induced by Tnfα. J Clin Endocrinol Metab (2013) 98(8):E1323–33. doi: 10.1210/jc.2012-4177
22. Etzerodt A, Moestrup SK. CD163 and Inflammation: Biological, Diagnostic, and Therapeutic Aspects. Antioxid Redox Signal (2013) 18(17):2352–63. doi: 10.1089/ars.2012.4834
23. Bover LC, Cardó-Vila M, Kuniyasu A, Sun J, Rangel R, Takeya M, et al. A Previously Unrecognized Protein-Protein Interaction Between TWEAK and CD163: Potential Biological Implications. J Immunol (2007) 178(12):8183–94. doi: 10.4049/jimmunol.178.12.8183
24. Fjeldborg K, Christiansen T, Bennetzen M, J Møller H, Pedersen SB, Richelsen B. The Macrophage-Specific Serum Marker, Soluble CD163, is Increased in Obesity and Reduced After Dietary-Induced Weight Loss. Obes (Silver Spring) (2013) 21(12):2437–43. doi: 10.1002/oby.20376
25. Maymó Masip E. Estudio De La Citocina Tweak Y De Su Receptor Fn14 En El Contexto De La Obesidad. [Thesis]. [Tarragona]: Universitat Rovira i Virgili (2015).
26. Hernández M, Castellet J, Narvaiza JL, Rincón JM, Ruiz I, Sánchez E, et al. Curvas Y Tablas De Crecimiento. 1988 Ed. Desarrollo I, editor. Madrid: Fundación F Orbegozo (1988). p. 33.
27. Marshall WA, Tanner JM. Variations in Pattern of Pubertal Changes in Girls. Arch Dis Child. (1969) 44(235):291–303. doi: 10.1136/adc.44.235.291
28. Marshall WA, Tanner JM. Variations in the Pattern of Pubertal Changes in Boys. Arch Dis Child. (1970) 45(239):13–23. doi: 10.1136/adc.45.239.13
29. Serra Majem L, Ribas Barba L, Aranceta Bartrina J, Pérez Rodrigo C, Saavedra Santana P, Peña Quintana L. [Childhood and Adolescent Obesity in Spain. Result EnKid Study (1998-2000)] Med Clin (Barc) (2003) 121(19):725–32. doi: 10.1016/s0025-7753(03)74077-9
30. Adolescents NHBPEPWGoHBPiCa. The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Pediatrics (2004) 114(2 Suppl 4th Report)::555–76.
31. Cole TJ. The LMS Method for Constructing Normalized Growth Standards. Eur J Clin Nutr (1990) 44(1):45–60.
32. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a Standard Definition for Child Overweight and Obesity Worldwide: International Survey. BMJ (2000) 320(7244):1240–3. doi: 10.1136/bmj.320.7244.1240
33. Association AD. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care (2004) 27 Suppl 1:S5–S10.
34. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function From Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia (1985) 28(7):412–9. doi: 10.1007/BF00280883
35. Reinehr T, Andler W. Changes in the Atherogenic Risk Factor Profile According to Degree of Weight Loss. Arch Dis Child. (2004) 89(5):419–22. doi: 10.1136/adc.2003.028803
36. Vendrell J, Maymó-Masip E, Tinahones F, García-España A, Megia A, Caubet E, et al. Tumor Necrosis-Like Weak Inducer of Apoptosis as a Proinflammatory Cytokine in Human Adipocyte Cells: Up-Regulation in Severe Obesity is Mediated by Inflammation But Not Hypoxia. J Clin Endocrinol Metab (2010) 95(6):2983–92. doi: 10.1210/jc.2009-2481
37. Vázquez Carballo A. Papel Protector Del TWEAK Sobre La Resistencia a La Insulina Asociada a La Obesidad: Efecto Sobre La Migración Celular. [Thesis]. Madrid: Universidad Complutense de Madrid (2014).
38. Carolan E, Hogan AE, Corrigan M, Gaotswe G, O'Connell J, Foley N, et al. The Impact of Childhood Obesity on Inflammation, Innate Immune Cell Frequency, and Metabolic microRNA Expression. J Clin Endocrinol Metab (2014) 99(3):E474–8. doi: 10.1210/jc.2013-3529
Keywords: TWEAK, CD163, childhood, obesity, prepubertal
Citation: Escartín R, Font M, González-Clemente JM, Vendrell J, Caixàs A and Corripio R (2022) New Insights in Cytokines in Childhood Obesity: Changes in TWEAK and CD163 After a 2-Year Intervention Program in Prepubertal Children With Obesity. Front. Endocrinol. 13:909201. doi: 10.3389/fendo.2022.909201
Received: 31 March 2022; Accepted: 07 June 2022;
Published: 08 July 2022.
Edited by:
Iwona Ben-Skowronek, Medical University of Lublin, PolandReviewed by:
Malgorzata Wojcik, Jagiellonian University Medical College, PolandCopyright © 2022 Escartín, Font, González-Clemente, Vendrell, Caixàs and Corripio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Corripio, cmFxdWVsY29ycmlwaW9AZ21haWwuY29t; cmNvcnJpcGlvQHRhdWxpLmNhdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.