
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Endocrinol., 28 June 2022
Sec. Pediatric Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.884107
 Diego Yeste1,2
Diego Yeste1,2 Cristina Aguilar-Riera1
Cristina Aguilar-Riera1 Gennaro Canestrino3
Gennaro Canestrino3 Paula Fernández-Alvarez4
Paula Fernández-Alvarez4 María Clemente1,2
María Clemente1,2 Núria Camats-Tarruella2,5*
Núria Camats-Tarruella2,5*MAMLD1 (X chromosome) is one of the recognized genes related to different sex development. It is expressed in testis and ovaries and seems to be involved in fetal sex development and in adult reproductive function, including testosterone biosynthesis. However, its exact role remains unclear. Over 40 genetic variants have been described, mainly in male individuals and mostly associated with hypospadias. Although MAMLD1 has been shown to regulate the expression of the steroidogenic pathway, patients with MAMLD1 variants mostly show normal gonadal function and normal testosterone levels. Here we describe a patient (46,XY) with hypospadias and microphallus, with low testosterone and dihydrotestosterone (DHT) levels, and with inappropriately low values of luteinizing hormone (LH) during minipuberty. This hormonal pattern was suggestive of partial hypogonadotropic hypogonadism. A stimulation test with hCG (4 months) showed no significant increase in both testosterone and dihydrotestosterone concentrations. At 5 months of age, he was treated with intramuscular testosterone, and the penis length increased to 3.5 cm. The treatment was stopped at 6 months of age. Our gonadal function massive-sequencing panel detected a previously unreported nonsense variant in the MAMLD1 gene (c.1738C>T:p.Gln580Ter), which was classified as pathogenic. This MAMLD1 variant, predicting a truncated protein, could explain his genital phenotype. His hormonal profile (low testosterone, dihydrotestosterone, and LH concentrations) together with no significant increase of testosterone and DHT plasma concentrations (hCG test) highlight the potential role of this gene in the biosynthesis of testosterone during the fetal stage and minipuberty of the infant. Besides this, the LH values may suggest an involvement of MAMLD1 in the LH axis or a possible oligogenesis. It is the first time that a decrease in DHT has been described in a patient with an abnormal MAMLD1.
MAMLD1 (Xq28, OMIM 300120) is one of the genes related to different sex development (DSD) (1, 2). It is expressed in human fetal and adult testes and in human ovaries (1, 3, 4), and it seems to be involved in sex development in fetal life and in adult reproductive function. It contributes to the development and formation of the male external genitalia in the late stages of fetal organogenesis (weeks 8–12) (3), and it has been related to testosterone biosynthesis in mice (5–7). Follow-up studies in patients with variants in MAMLD1 diagnosed in infancy have shown an impaired testicular function with aging (8), but patients can be fertile (4). Interestingly, MAMLD1’s exact role is still not clear (4, 9, 10). Recently, it has also been related to early-onset obesity (11).
The variants in MAMLD1 are inherited in an X-linked recessive fashion. Over 40 MAMLD1 sequence variations have been described (12) not only mainly in males and mostly associated with hypospadias (1, 4, 12–18) but also together with microphallus (4, 12, 14, 15, 19) and/or cryptorchidism (1, 4, 12, 13, 15). More severe DSD cases such as 46,XY individuals with female external genitalia (1, 4) and 46,XY with complete gonadal dysgenesis (20) have been described. Furthermore, in 46,XX females, one homozygous MAMLD1 variant was also reported in a patient with gonadal dysgenesis, primary amenorrhea, bilateral streak gonads, and clitoromegaly (21) and in one heterozygous female patient who presented primary ovarian insufficiency (9).
Although MAMLD1 has been shown to regulate the expression of the steroidogenic pathway, patients with MAMLD1 variants mostly show normal gonadal function and normal testosterone levels (12). Here we describe a patient with hypospadias and microphallus, with low testosterone and dihydrotestosterone (DHT) levels, and with inappropriately low values of luteinizing hormone (LH) due to a variant in the MAMLD1 gene.
The patient is a 40-week gestation newborn with a microphallus of 1.5 cm in length (normal values: 3.5 cm ± 0.4) and a terminal hypospadias with 3-ml testes located in the scrotal bag. He presented normal anthropometry. At 6 days of life, a hormonal study was carried out (Table 1), which showed total plasma testosterone values of 69 ng/dl. At 1 month of age, two 25-mg doses of intramuscular testosterone—separated by 2 weeks—were administered.

Table 1 Hormonal values, testosterone treatment, and penis length of our patient.
The patient was first seen at our hospital at 2 months of age. The length of the penis was 2 cm. To further characterize the patient, we calculated the external genital score (EGS). The EGS according to van der Straaten et al. (25) was 9.5 (undervirilization) and according to Ahmed and Rodie (26) was 8 (undervirilization). A new hormonal test that was performed (Table 1) showed low testosterone and DHT levels with inappropriately low values of LH for the levels of serum testosterone, normal thyroid and adrenal hormone profile, and normal prolactin and normal IGF-1 and IGFBP3 values. His karyotype was 46,XY. The hypothalamic–pituitary magnetic resonance was normal, and the ultrasound showed testes with homogeneous structure and of normal size. At the age of 4 months, a stimulation test with hCG at 1,000 IU/dose was performed (3 times/week for 2 weeks), which showed no significant increase in penis length or in the concentrations of testosterone (111.1 ng/dl) and DHT (0.05 ng/ml) (Table 1). Normal follicle-stimulating hormone (FSH), anti-Müllerian hormone, and inhibin B levels and 3-ml testicular volume ruled out gonadal dysgenesis.
To study both DSD and hypogonadotropic hypogonadism (HH), we performed two massive-sequencing gene panels: one including genes related to gonadal function (GeneRead DNA Library l Core Kit, Qiagen) and another including genes related to HH (Cell3 Target Custom Panel tier 2, NONACUS). The gonadal function gene panel included the genes AR, CYP11A1, CYP17A1, HSD17B3, LHCGR, MAMLD1, NR0B1, NR5A1, SRD5A2, SRY, STAR, and WT1. The HH panel included the genes ANOS1, CDH7, FGF8, FGFR1, FSHB, GLI2, GNRH1, GNRHR, IL17RD, KISS1, KISS1R, KLB, LHB, MKRN3, NSMF, OTX2, PAX6, PROP1, SOX3, SOX10, TAC3, TACR3, and WDR11. We identified a hemizygous nonsense variant in the MAMLD1 gene (c.1738C>T:p.Gln580Ter) located in exon 3 (Figure 1). This variant was classified as pathogenic (ACMG fulfilled criteria PVS1, PM2, and PP3; ACMG classification; https://varsome.com) (27), and it has not been previously reported based on literature review and database [Human Genome Mutation Database (HGMD), Qiagen] search. No other genetic variants were detected.
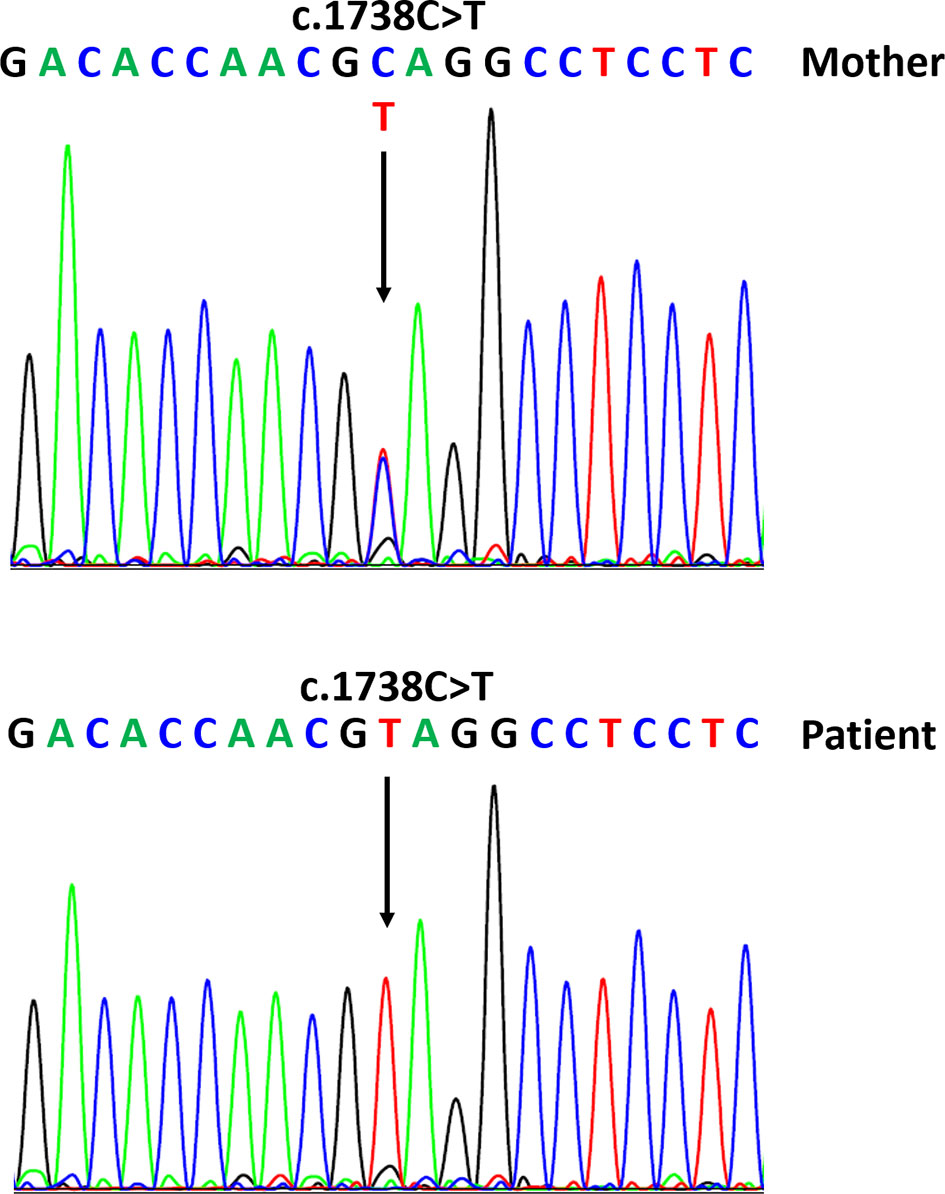
Figure 1 Sequences of the MAMLD1 gene with the detected variant corresponding to our patient (hemizygous) and his mother (heterozygous).
At 5 months of age, treatment with intramuscular testosterone was started (50 mg in two doses every three weeks), showing a favorable response to treatment with an increase in penis length to 3.5 cm. The treatment was stopped when he was 6 months old.
We report a patient with hypospadias and microphallus with low testosterone, DHT, and LH levels due to a novel nonsense variant in the MAMLD1 gene. The occurrence of hypospadias and microphallus is one of the manifestations of patients with MAMLD1 variants (4, 14, 15, 19). Importantly, our patient showed a favorable response to treatment (intramuscular testosterone), with an increase in penis length of up to 3.5 cm.
Interestingly, our patient showed low testosterone and DHT levels and inappropriately normal LH levels in relation to testosterone at 2 months of age (Table 1), which, at first, let us to consider a case of partial hypogonadotropic hypogonadism with normal function of the FSH axis. At 2 months of age, after the first testosterone treatment, we expected a sensitization of the central axis and therefore an increase in LH. However, at 3 months of age, testosterone was already normal, whereas LH remained low. At 4 months, an hCG stimulation test was conducted: the basal testosterone values were normal before testing and decreased after, but LH remained low even post-hCG test. Furthermore, whereas it showed a decrease in testosterone levels, the DHT levels remained low through both minipuberty and hCG treatment. Our interpretation regarding these results is that the biosynthesis and LH axis were clearly affected in his first months after birth. Testosterone biosynthesis affectation would concur with a pathogenic variant in MAMLD1, whereas we suggest a possible implication of this gene in the LH axis. An alternative explanation for LH suppression may be that intramuscular testosterone (administered at 1 month of age) caused a decrease in LH. Regarding the decrease in testosterone levels after hCG stimulation, we believe that, although testosterone first increased, the decrease observed in the subsequent weeks may have been due to the child’s increasing age and physiological stage.
Although MAMLD1 has been shown to be involved in androgen biosynthesis (7), patients with MAMLD1 variants mostly show normal gonadal function and normal testosterone levels (1, 4, 8, 12, 16, 18, 28). However, some patients do show low testosterone levels regardless of LH concentrations. Kalfa et al. have previously reported a MAMLD1 patient with hypospadias with a significant reduction in plasma testosterone concentrations at 3 months of age (12, 15). This same patient also showed low concentrations of LH. Fukami et al. reported a patient with testosterone in the lower normal range and LH with normal values (low range) (1). Furthermore, Fujisawa reported a follow-up of this and other 2 patients (7–13 years of age) of the Fukami study (1) presenting with hypospadias and microphallus, which showed normal pre-hCG test testosterone levels but non-increased post-hCG. LH was normal at pre-test and elevated at post-test (8). Recently, Li and collaborators also reported some MAMLD1 patients with low plasma testosterone levels, but in these cases, the LH concentrations ranged from low to normal (29). As far as we know, MAMLD1 has not been related to LH axis regulation, yet other patients and ours present low LH levels. Regarding DHT, a few patients were reported, all with normal DHT levels at different ages in infancy (1, 13). However, this is the first report of low levels of DHT.
There are few reports on LH levels in patients with normal testosterone (at different ages), which are as follows: low-normal range LH (1), normal (low range) LH but increased LH after hCG stimulation (1, 8), and normal LH (high range) (15). Furthermore, a comparative study of testosterone and LH levels between MAMLD1-hypospadias patients and control individuals of the same age gave statistically significant differences only in the 4- to 8-year-old group and not at lower ages (28).
In our study, the testosterone, DHT, and gonadotropin concentrations during minipuberty (0 to 4 months of age) were measured. Both androgens and LH showed low serum levels and low pre- and post-hCG test levels (Table 1), with the exception of testosterone previous to the hCG test. We consider that the low testosterone and LH concentrations during this infant’s minipuberty stage and the non-significant increase in plasma concentrations of LH, testosterone, and DHT in the hCG test highlight the potential role of this gene in the biosynthesis of testosterone during the fetal stage and, specifically, in the minipuberty of the infant. Additionally, the LH values may suggest an implication of MAMLD1 in the LH axis. Other groups have also reported values during minipuberty, and the results range from normal to low testosterone levels (1, 4, 12, 15, 29). Our group also reported a patient with hypospadias and microphallus with normal baseline testosterone (3 months) (4). These and our results expand the biochemical spectrum of patients with MAMLD1 variants.
Up to now, there are over 40 MAMLD1 reported variants (29–31) (HGMD database, Qiagen). The HGMD database reported to date 30 MAMLD1 variants (including 2 long insertions) (HGMD Nov2021, Qiagen). This contrasts with the 41 single-nucleotide variants and small duplications/insertions in this gene reported in the latest and recent review (12). Forty were reported in 46,XY individuals and two in 46,XX female patients: one in homozygosity (12, 21) and one in heterozygosity (9). The homozygous variant (c.1514T>C:p.Val432Ala) in 46,XX has been confirmed to provide gain-of-function and has also been reported in other 46,XY male patients (4, 13, 14, 32). Moreover, some of the variants were reported in more than one family and report (12). It is worth noting that 13 variants reviewed by Miyado et al. were not included in HGMD (12) (HGMD database, Qiagen).
Regarding variants predicting a shorter protein product, nine MAMLD1 nonsense variants have been reported (12). Our novel nonsense variant (c.1738C>T:p.Gln580Ter) in silico predicts a truncated protein and has not been detected in any control population database. It has been classified as pathogenic according to the ACMG criteria (https://varsome.com, November 2021) (27). Furthermore, there is strong evidence that nonsense MAMLD1 variants are deleterious because all MAMLD1 nonsense tested variants do show compromised transactivating activities (4, 6). All these evidences would concur with the production of a truncated protein or the absence of protein, maybe through nonsense-mediated decay mechanisms. Therefore, we consider that it could justify his genital and biochemical phenotype. Unfortunately, the MAMLD1 domains have only been described as amino acid-rich regions (6), and the Uniprot website describes the different domains as “disordered” (https://www.uniprot.org/uniprot/Q13495). To our knowledge, MAMLD1’s exact function and interaction properties still remain unclear. In particular, amino acid position 580 (p.Gln580Ter) is in the last part of the peptide sequence, after the domains described in Fukami’s work (6).
The in vitro and in vivo studies give evidence of the involvement of MAMLD1 in sex development, reproduction, and androgen production. Interestingly, Mamld1-knockdown in vitro assays in mouse Leydig tumor cells have shown a significant reduction of expression of different genes related to androgen biosynthesis, together with Insl3, related to testicular descent. This has led to low androgen levels in these cells (7). In contrast, normal testosterone concentrations have also been described in Mamld1-knockout fetal male mice (5), whereas these individuals have shown low mRNA levels of genes only expressed in the testes (i.e., Star, Cyp11a1, Cyp17a1, Hsd3b1, and Insl3) (5). Adult knockout mice present small testes with reduced seminiferous tubule size and proliferating germ cells but exhibit normal external genitalia and reproduce similarly to wild-type mice (5, 33). Moreover, MAMLD1 is regulated by NR5A1/SF-1, which is involved in many processes of sex development and function (6), yet it has not been directly related to the regulation of the LH axis. There also seems to be a difference in its role between humans and mice and even in other species (12).
However, its specific function remains unclear and, lately, its role in sex development has become controversial. There are several reasons for this, including the fact that some MAMLD1 variants have been detected in non-DSD individuals (control populations) (1, 14, 34, 35) and in patients with different DSD phenotypes (4). Furthermore, in some families, only part of the DSD individuals present a MAMLD1 variant (1), and in vitro studies showed that several variants functioned similar to the wild type (4). Finally, Mamld1-knockout male mice have normal genitalia and reproduction (5, 33). These evidence have also led us to propose that MAMLD1 may be linked to an oligogenic origin of the DSD of these MAMLD1 patients (4, 9, 12, 31). The idea of various gene defects adding up to cause a specific disease/disorder has also been proposed in several endocrine/reproductive disorders such as hypogonadotropic hypogonadism (36), congenital hypothyroidism (37), and even in DSD related to NR5A1 (38), thanks to high-throughput sequencing (39). Remarkably, our patient was suspected of partial hypogonadotropic hypogonadism due to his low LH levels, until we detected this MAMLD1 variant. His biochemical characteristics also concur with some of the reported MAMLD1 patients.
In line with the hypothesis of oligogenicity, we had previously performed a study searching for other variants in MAMLD1 patients to explain the variability in DSD phenotypes (9). We detected additional variants in WDR11 (40) and in the pituitary transcription factor PROP1 (41) in one of the patients (hypospadias, microphallus, and small testes) and showed that PROP1 is part of the MAMLD1 network, connected to MAMLD1 through NOTCH1/2 (9). Alternatively, the MAMLD1 defects may be directly linked to a partial affectation of the LH axis. There are reported evidences of MAMLD1 connections to pituitary hormone deficiency (9), signaling pathways (9), or gonadotropic cell proliferation and migration (specifically in gonadotroph pituitary adenomas) (42) that should be further explored. Taken together, our data may either reveal a new MAMLD1 function related to LH axis regulation or strengthen the possibility of oligogenicity in our and similar MAMLD1 patients.
Our patient presents a pathogenic variant in MAMDL1 not previously described and that in silico predicts a truncated protein that could justify his genital phenotype. The existence of low testosterone, DHT, and LH concentrations during the infant’s minipuberty stage and the absence of a significant increase in plasma concentrations of testosterone and DHT in the hCG test highlight the potential role of this gene in the biosynthesis of testosterone during the fetal stage and minipuberty of the infant. Furthermore, LH values may suggest an implication of MAMLD1 in the LH axis or a possible oligogenicity. It is the first time that a decrease in DHT has been described in a patient with an abnormal MAMLD1. We have also demonstrated that intramuscular testosterone treatment is effective in these patients.
The datasets for this article are not publicly available due to concerns regarding participant/patient anonymity. Requests to access the datasets should be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Comité Ético de Investigación Clínica y Comisión de Proyectos de Investigación del Hospital Universitari Vall d’Hebron (CEIC Hospital Universitari Vall d’Hebron). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
DY, MC, CAR, and GC clinically and biochemically evaluated the patient. PFA performed the molecular analysis. DY and NCT contributed to the molecular evaluation and concept of the article. NCT drafted the article. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the patient and his family. We also thank Prof. S. Faisal Ahmed and Dr. Supitcha Pajmontri for their interest in and kind discussion of this case.
1. Fukami M, Wada Y, Miyabayashi K, Nishino I, Hasegawa T, Nordenskjold A, et al. CXorf6 is a Causative Gene for Hypospadias. Nat Genet (2006) 38(12):1369–71. doi: 10.1038/ng1900
2. Baxter RM, Arboleda VA, Lee H, Barseghyan H, Adam MP, Fechner PY, et al. Exome Sequencing for the Diagnosis of 46,XY Disorders of Sex Development. J Clin Endocrinol Metab (2015) 100(2):E333–44. doi: 10.1210/jc.2014-2605
3. O’Shaughnessy PJ, Baker PJ, Monteiro A, Cassie S, Bhattacharya S, Fowler PA. Developmental Changes in Human Fetal Testicular Cell Numbers and Messenger Ribonucleic Acid Levels During the Second Trimester. J Clin Endocrinol Metab (2007) 92(12):4792–801. doi: 10.1210/jc.2007-1690
4. Camats N, Fernández-Cancio M, Audí L, Mullis PE, Moreno F, González Casado I, et al. Human MAMLD1 Gene Variations Seem Not Sufficient to Explain a 46,XY DSD Phenotype. PLoS One (2015) 10(11):e0142831. doi: 10.1371/journal.pone.0142831
5. Miyado M, Nakamura M, Miyado K, Morohashi K, Sano S, Nagata E, et al. Mamld1 Deficiency Significantly Reduces mRNA Expression Levels of Multiple Genes Expressed in Mouse Fetal Leydig Cells But Permits Normal Genital and Reproductive Development. Endocrinology (2012) 153(12):6033–40. doi: 10.1210/en.2012-1324
6. Fukami M, Wada Y, Okada M, Kato F, Katsumata N, Baba T, et al. Mastermind-Like Domain-Containing 1 (MAMLD1 or CXorf6) Transactivates the Hes3 Promoter, Augments Testosterone Production, and Contains the SF1 Target Sequence. J Biol Chem (2008) 283(9):5525–32. doi: 10.1074/jbc.M703289200
7. Nakamura M, Fukami M, Sugawa F, Miyado M, Nonomura K, Ogata T. Mamld1 Knockdown Reduces Testosterone Production and Cyp17a1 Expression in Mouse Leydig Tumor Cells. PLoS One (2011) 6(4):e19123. doi: 10.1371/journal.pone.0019123
8. Fujisawa Y, Fukami M, Hasegawa T, Uematsu A, Muroya K, Ogata T. Long-Term Clinical Course in Three Patients With MAMLD1 Mutations. Endocr J (2016) 63(9) 835–39. doi: 10.1507/endocrj.EJ16-0143
9. Flück CE, Audí L, Fernández-Cancio M, Sauter K-S, Martinez de LaPiscina I, Castaño L, et al. Broad Phenotypes of Disorders/Differences of Sex Development in MAMLD1 Patients Through Oligogenic Disease. Front Genet (2019) 10. doi: 10.3389/fgene.2019.00746
10. McElreavey K, Bashamboo A. Monogenic Forms of DSD: An Update. Horm Res Paediatr (2021). doi: 10.1159/000521381
11. Pettersson M, Viljakainen H, Loid P, Mustila T, Pekkinen M, Armenio M, et al. Copy Number Variants are Enriched in Individuals With Early-Onset Obesity and Highlight Novel Pathogenic Pathways. J Clin Endocrinol Metab (2017) 102(8):3029–39. doi: 10.1210/jc.2017-00565
12. Miyado M, Fukami M, Ogata T. MAMLD1 and Differences/Disorders of Sex Development: An Update. Sex Dev (2021), 1–12. doi: 10.1159/000519298
13. Kalfa N, Liu B, Klein O, Audran F, Wang MH, Mei C, et al. Mutations of CXorf6 are Associated With a Range of Severities of Hypospadias. Eur J Endocrinol (2008) 159(4):453–8. doi: 10.1530/EJE-08-0085
14. Chen Y, Thai HT, Lundin J, Lagerstedt-Robinson K, Zhao S, Markljung E, et al. Mutational Study of the MAMLD1-Gene in Hypospadias. Eur J Med Genet (2010) 53(3):122–6. doi: 10.1016/j.ejmg.2010.03.005
15. Kalfa N, Fukami M, Philibert P, Audran F, Pienkowski C, Weill J, et al. Screening of MAMLD1 Mutations in 70 Children With 46,XY DSD: Identification and Functional Analysis of Two New Mutations. PLoS One (2012) 7(3):e32505. doi: 10.1371/journal.pone.0032505
16. Metwalley KA, Farghaly HS. X-Linked Congenital Adrenal Hypoplasia Associated With Hypospadias in an Egyptian Baby: A Case Report. J Med Case Rep (2012) 6:428. doi: 10.1186/1752-1947-6-428
17. Eggers S, Sadedin S, van den Bergen JA, Robevska G, Ohnesorg T, Hewitt J, et al. Disorders of Sex Development: Insights From Targeted Gene Sequencing of a Large International Patient Cohort. Genome Biol (2016) 17(1):243. doi: 10.1186/s13059-016-1105-y
18. Igarashi M, Wada Y, Kojima Y, Miyado M, Nakamura M, Muroya K, et al. Novel Splice Site Mutation in MAMLD1 in a Patient With Hypospadias. Sex Dev (2015) 9(3):130–5. doi: 10.1159/000380842
19. Liu Y, Zhuang L, Ye W, Wu M, Huang Y. Association of MAMLD1 Single-Nucleotide Polymorphisms With Hypospadias in Chinese Han Population. Front Biosci (2017) 22:1173–6. doi: 10.2741/4540
20. Ruiz-Arana IL, Hubner A, Cetingdag C, Krude H, Gruters A, Fukami M, et al. A Novel Hemizygous Mutation of MAMLD1 in a Patient With 46,XY Complete Gonadal Dysgenesis. Sex Dev (2015) 9:80–5. doi: 10.1159/000371603
21. Brandao MP, Costa EM, Fukami M, Gerdulo M, Pereira NP, Domenice S, et al. MAMLD1 (Mastermind-Like Domain Containing 1) Homozygous Gain-of-Function Missense Mutation Causing 46,XX Disorder of Sex Development in a Virilized Female. Adv Exp Med Biol (2011) 707:129–31. doi: 10.1007/978-1-4419-8002-1_28
22. Lahlou N, Fennoy I, Carel JC, Roger M. Inhibin B and Anti-Müllerian Hormone, But Not Testosterone Levels, are Normal in Infants With Nonmosaic Klinefelter Syndrome. J Clin Endocrinol Metab (2004) 89(4):1864–8. doi: 10.1210/jc.2003-031624
23. Bergadá I, Milani C, Bedecarrás P, Andreone L, Ropelato MG, Gottlieb S, et al. Time Course of the Serum Gonadotropin Surge, Inhibins, and Anti-Müllerian Hormone in Normal Newborn Males During the First Month of Life. J Clin Endocrinol Metab (2006) 91(10):4092–8. doi: 10.1210/jc.2006-1079
24. Guerrero-Fernández J, Azcona C, Barreiro J, de la Vega JAB, Carcavilla A, Castaño L, et al. Guía De Actuación En Las Anomalías De La Diferenciación Sexual (ADS) / Desarrollo Sexual Diferente (DSD). Pediatr (2018) 89(5):315.e1–15.e19. doi: 10.1016/j.anpedi.2018.06.009
25. Van Der Straaten S, Springer A, Zecic A, Hebenstreit D, Tonnhofer U, Gawlik A, et al. The External Genitalia Score (EGS): A European Multicenter Validation Study. J Clin Endocrinol Metab (2020) 105(3):dgz142. doi: 10.1210/clinem/dgz142
26. Ahmed SF, Rodie M. Investigation and Initial Management of Ambiguous Genitalia. Best Pract Res: Clin Endocrinol Metab (2010) 24(2):197–218.. doi: 10.1016/j.beem.2009.12.001
27. Kopanos C, Tsiolkas V, Kouris A, Chapple CE, Aguilera MA, Meyer R, et al. VarSome: The Human Genomic Variant Search Engine | Bioinformatics | Oxford Academic. Bioinformatics (2019). doi: 10.1101/367359
28. Ratan SK, Sharma A, Kapoor S, Polipalli SK, Dubey D, Mishra TK, et al. Polymorphism of 3′ UTR of MAMLD1 Gene is Also Associated With Increased Risk of Isolated Hypospadias in Indian Children: A Preliminary Report. Pediatr Surg Int (2016) 32(5):515–24. doi: 10.1007/s00383-016-3856-7
29. Li L, Su C, Fan L, Gao F, Liang X, Gong C. Clinical and Molecular Spectrum of 46,XY Disorders of Sex Development That Harbour MAMLD1 Variations: Case Series and Review of Literature. Orphanet J Rare Dis (2020) 15(1):188. doi: 10.1186/s13023-020-01459-9
30. Fernández N, Pabon J, Ayala P, Pérez J, Ortiz AM, Zarante I. Description of a Novel Variant in the MAMLD1 Gene in Isolated Hypospadias. Urol Colomb (2018) 27(01):105–09 . doi: 10.1016/j.uroco.2016.09.001
31. Li L, Gao F, Fan L, Su C, Liang X, Gong CX. Disorders of Sex Development in Individuals Harbouring MAMLD1 Variants: WES and Interactome Evidence of Oligogenic Inheritance. Front Endocrinol (Lausanne) (2020) 11. doi: 10.3389/fendo.2020.582516
32. Ogata T, Sano S, Nagata E, Kato F, Fukami M. MAMLD1 and 46,XY Disorders of Sex Development. Semin Reprod Med (2012) 30(5):410–6. doi: 10.1055/s-0032-1324725
33. Miyado M, Yoshida K, Miyado K, Katsumi M, Saito K, Nakamura S, et al. Knockout of Murine Mamld1 Impairs Testicular Growth and Daily Sperm Production But Permits Normal Postnatal Androgen Production and Fertility. Int J Mol Sci (2017) 18(6). doi: 10.3390/ijms18061300
34. Gaspari L, Paris F, Philibert P, Audran F, Orsini M, Servant N, et al. “Idiopathic” Partial Androgen Insensitivity Syndrome in 28 Newborn and Infant Males: Impact of Prenatal Exposure to Environmental Endocrine Disruptor Chemicals? Eur J Endocrinol. European Journal of Endocrinology (2011) 165(4):579–87. doi: 10.1530/EJE-11-0580
35. Kalfa N, Cassorla F, Audran F, Oulad Abdennabi I, Philibert P, Beroud C, et al. Polymorphisms of MAMLD1 Gene in Hypospadias. J Pediatr Urol (2011) 7(6):585–91. doi: 10.1016/j.jpurol.2011.09.005
36. Sykiotis GP, Plummer L, Hughes VA, Au M, Durrani S, Nayak-Young S, et al. Oligogenic Basis of Isolated Gonadotropin-Releasing Hormone Deficiency. Proc Natl Acad Sci USA (2010) 107:15140–4. doi: 10.1073/pnas.1009622107
37. Satoh M, Aso K, Ogikubo S, Yoshizawa-Ogasawara A, Saji T. Hypothyroidism Caused by the Combination of Two Heterozygous Mutations: One in the TSH Receptor Gene the Other in the DUOX2 Gene. J Pediatr Endocrinol Metab (2015) 28(5–6):657–61. doi: 10.1515/jpem-2014-0078
38. Camats N, Fernández-Cancio M, Audí L, Schaller A, Flück CE. Broad Phenotypes in Heterozygous NR5A1 46,XY Patients With a Disorder of Sex Development: An Oligogenic Origin? Eur J Hum Genet (2018) 26:749–57. doi: 10.1038/s41431-018-0202-7
39. Boehm U, Bouloux PM, Dattani MT, de Roux N, Dode C, Dunkel L, et al. Expert Consensus Document: European Consensus Statement on Congenital Hypogonadotropic Hypogonadism–Pathogenesis, Diagnosis and Treatment. Nat Rev Endocrinol (2015) 11(9):547–64. doi: 10.1038/nrendo.2015.112
40. Kim HG, Ahn JW, Kurth I, Ullmann R, Kim HT, Kulharya A, et al. WDR11, a WD Protein That Interacts With Transcription Factor EMX1, is Mutated in Idiopathic Hypogonadotropic Hypogonadism and Kallmann Syndrome. Am J Hum Genet (2010) 87(4):465–79. doi: 10.1016/j.ajhg.2010.08.018
41. Reynaud R, Barlier A, Vallette-Kasic S, Saveanu A, Guillet MP, Simonin G, et al. An Uncommon Phenotype With Familial Central Hypogonadism Caused by a Novel PROP1 Gene Mutant Truncated in the Transactivation Domain. J Clin Endocrinol Metab (2005) 90(8):4880–7. doi: 10.1210/jc.2005-0119
Keywords: MAMLD1 gene, hypospadias, minipuberty, hypogonadotropic hypogonadism, microphallus, different sex development (DSD)
Citation: Yeste D, Aguilar-Riera C, Canestrino G, Fernández-Alvarez P, Clemente M and Camats-Tarruella N (2022) A New MAMLD1 Variant in an Infant With Microphallus and Hypospadias With Hormonal Pattern Suggesting Partial Hypogonadotropic Hypogonadism—Case Report. Front. Endocrinol. 13:884107. doi: 10.3389/fendo.2022.884107
Received: 25 February 2022; Accepted: 17 May 2022;
Published: 28 June 2022.
Edited by:
Tsutomu Ogata, Hamamatsu University School of Medicine, JapanReviewed by:
Rodolfo A Rey, Hospital de Niños Ricardo Gutiérrez, ArgentinaCopyright © 2022 Yeste, Aguilar-Riera, Canestrino, Fernández-Alvarez, Clemente and Camats-Tarruella. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Núria Camats-Tarruella, bnVyaWEuY2FtYXRzQHZoaXIub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.