 Ge Chen1,2
Ge Chen1,2 Mingchu Li
Mingchu Li Wenlong Xu
Wenlong Xu Ming Feng
Ming Feng Renzhi Wang
Renzhi Wang Xiaohai Liu
Xiaohai Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 06 April 2022
Sec. Pituitary Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.800923
This article is part of the Research Topic The Progress of Rare Lesions of the Sellar Region View all 23 articles
Objective: Clival chordoma is a locally aggressive tumor with low metastatic potential. In the past decade, endoscopic endonasal approach (EEA) for clival chordoma has had a higher resection rate and a lower morbidity rate than transcranial approaches. Here, we present our initial single-center experience after EEA of clival chordomas.
Patients and methods: This study retrospectively analyzed 17 consecutive patients with clival chordoma who received EEA in our department between March 2015 and September 2021. The operation was performed by a single surgeon with EEA. The clinical and pathological characteristics were analyzed along with the surgical outcomes and complications.
Results: A total of 17 consecutive patients with clival chordoma received EEA with a median follow-up of 29.2 months (range 1-79). Gross total resection (GTR) was performed in 7 cases (41%), subtotal resection (STR) in 7 case (41%) and partially resection (PR) in 3 cases (18%). Cerebrospinal fluid leakage occurred in 2 cases (12%) and meningitis developed in 3 patients (18%) which were all successfully treated with intravenous antibiotics without any complications. There were no perioperative deaths or new focal neurological deficits postoperatively. Four in 7 patients with STR have had radiotherapy while the other three chose to be monitored. Till the last follow-up, three patients in STR group who received radiotherapy (3 in 4) had no tumor regrowth, while one in STR group with radiotherapy (1 in 4) showed tumor progression. Two patients in STR group without radiotherapy (2 in 3) showed stable tumor while the left one (1 in 3) showed tumor progression. One patient in the PR group died of tumor progression 2 years postoperation and the other one showed tumor progression and died of lung cancer 1 year postoperation. In addition, 1 in 7 patients with GTR had tumor recurrence in situ after 10 months and developed surgical pathway seeding in the spinal canal in C1 after 16 months. No recurrence occurred in the other 6 cases with GTR during the follow-up.
Conclusion: Although more cases are needed, our case series showed EEA is a safe and reliable method for clival chordoma with high resection rates and low morbidity rates. GTR without tumor residuum would improve the outcome.
Chordomas are rare and locally invasive bone tumors originating from remnants of the embryologic notochord with an incidence of approximately 0.1/100,000/year (1). The most common site of chordoma is the sacrococcygeal region (50%), followed by the skull base (35%), especially the clival region and vertebra (15%) (2). Although clival chordomas account for only 0.2% of all central nervous system tumors, they are characterized by local destruction, dural invasion, bone erosion, and cranial nerve palsy, and even metastasis, resulting in challenges for the surgical removal of this lesion. Moreover, local recurrence rates of clival chordoma are very high even after radical resection and adjuvant radiotherapy (3, 4), while chemotherapeutic agents are rare and are largely ineffective (5).
Most recently, endoscopic endonasal approach (EEA) was recommended as a first-line option with a higher resection rate and a lower surgical complication rate compared to the transcranial surgery for the treatment of clival chordomas, which is not yet widely accepted yet (6, 7). In this study, we aimed to report our single-center experience and surgical outcomes after EEA for the resection of clival chordomas, and showed that EEA provided a safe and reliable method for the resection of clival chordoma.
A total of 17 consecutive patients with clival chordoma who underwent EEA in Beijing Xuanwu Hospital between January 2015 and December 2021 were retrospectively analyzed. All the patients included had complete clinical, radiological, and biochemical data, over 18 years old, were treated with EEA and had at least half a year of follow-up. Histopathological and immunohistochemical examinations confirmed clival chordoma in all patients. The surgical procedures were performed by a single neurosurgeon (Ge Chen) with the surgical goal of total tumor resection. MRI was performed in all patients pre- and 1 week, 3 months, 6 months and every year post-operatively. The tumor size was measured as the maximum tumor diameter on MRI. The study was approved by the Research Ethics Committee of our hospital and written informed consent was obtained from all patients.
All EEAs were performed endoscopically using a Karl Storz endoscope through bi-nostrils, following the protocols described by the Pittsburg group (8). Hadad-Bassagasteguy (H-B) vascularized septal flaps with blood supply were performed in all cases (9). Septostomy and large sphenoidotomy were performed to provide access to the sellar area and clivus. Further surgical approaches depend on the location of the tumor and its upper and lateral extent. During the operation, we tried to detect the pseudocapsule of the tumor before the tumor resection. The adjacent dura mater was resected in all cases to achieve maximum surgical resection. All patients underwent multilayer closure with dura implantation, fat transplantation (when necessary), and a vascularized H-B flap. The internal carotid artery and basal artery were confirmed using Doppler in the patients with vascular invasion. Cerebrospinal fluid lumbar drainage was given postoperatively in all cases and was removed within 7 days after surgery. The MRI scans were evaluated by a neuroradiologist and another endoscopic surgeon to determine the extent of the tumor removal.
Statistical analysis was performed with SPSS 18.0 software (SPSS, Inc., Chicago, IL, USA). Descriptive statistics were performed to report data related to patients’ demographics and clinicopathological characteristics.
A total of 17 EEAs were performed in 17 patients. Three patients received one or two craniotomies while no one received radiotherapy before EEA and 2 cases with preoperative occipitocervical fusion surgery. The median age at diagnosis was 45 years and ranged from 10 to 67 years. The male to female ratio is 7:10. Nine patients out of 17 (53%) had headache, and eight patients were diagnosed with visual impairment or field defect (47%). Diplopia was the third most common symptom, which occurred in 6 patients (35%). Two patients exhibited dysphagia and dysphonia (12%) and hypophysis were seen in five patients at the time of diagnosis (29%). The average time from symptoms onset to diagnosis were 10.6 months (range 0.5–24 months). The maximum diameter and location of tumors are shown in Table 1. The maximum diameter of the 17 tumors arranged from 24.4 to 83.4 mm, with the mean diameter 45.9 mm. The mean tumor volume was 49.7 cm3 (range 3.1–220.5 cm3). Fourteen tumors (82%) were solid while only three were cystic. The tumor involved the clivus in 15 cases (88%), the sphenoid sinus in 6 cases (35%), the sella in 11 cases (65%), suprasella in 3 cases (18%) and in cavernous sinus 6 cases (35%). In one case, the tumor was located extended to the craniocervical junction. The pre- and post- MRIs of all the patients were shown in Figure 1.
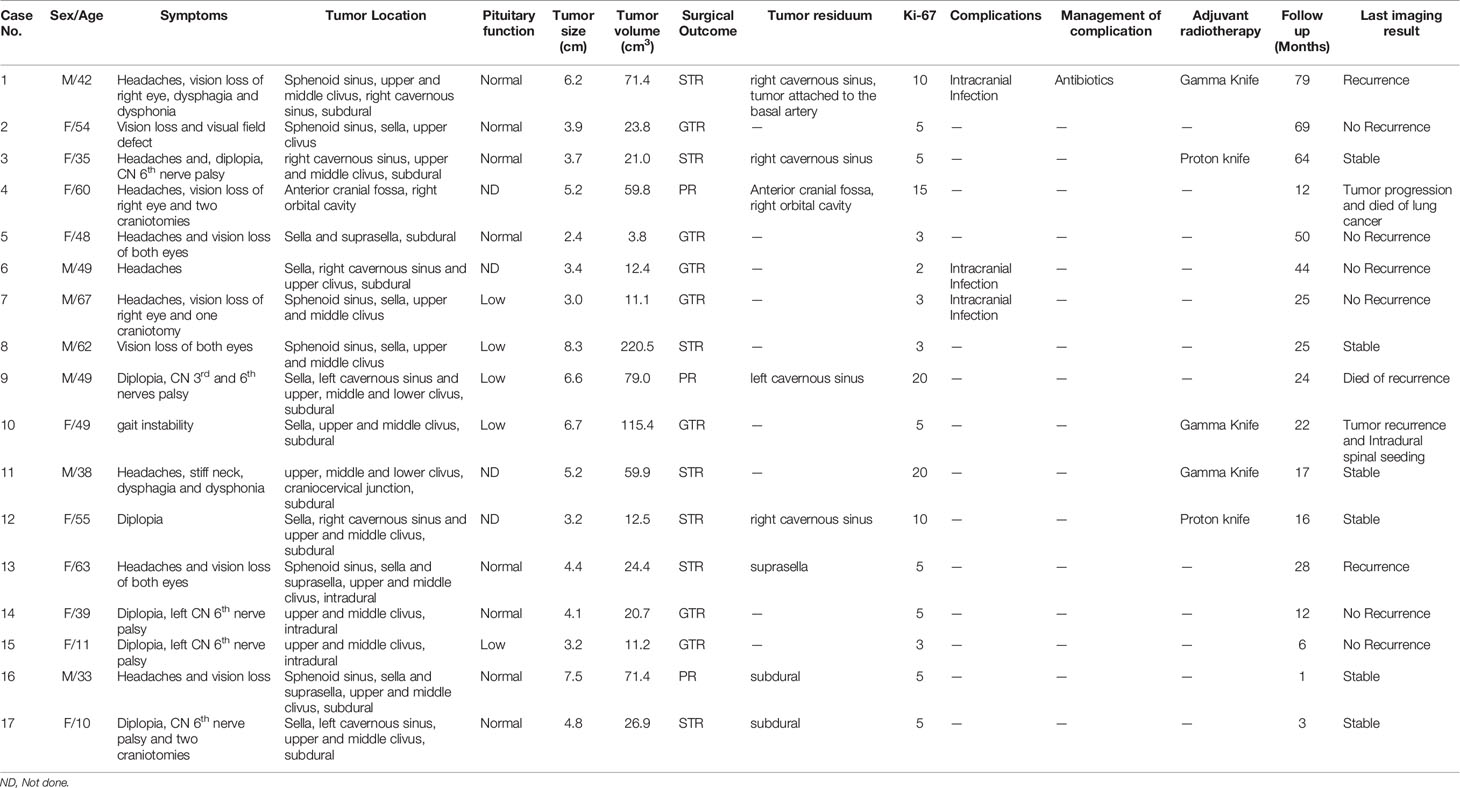
Table 1 Clinical characteristics and surgical outcomes of the 17 patients with clival chordoma.
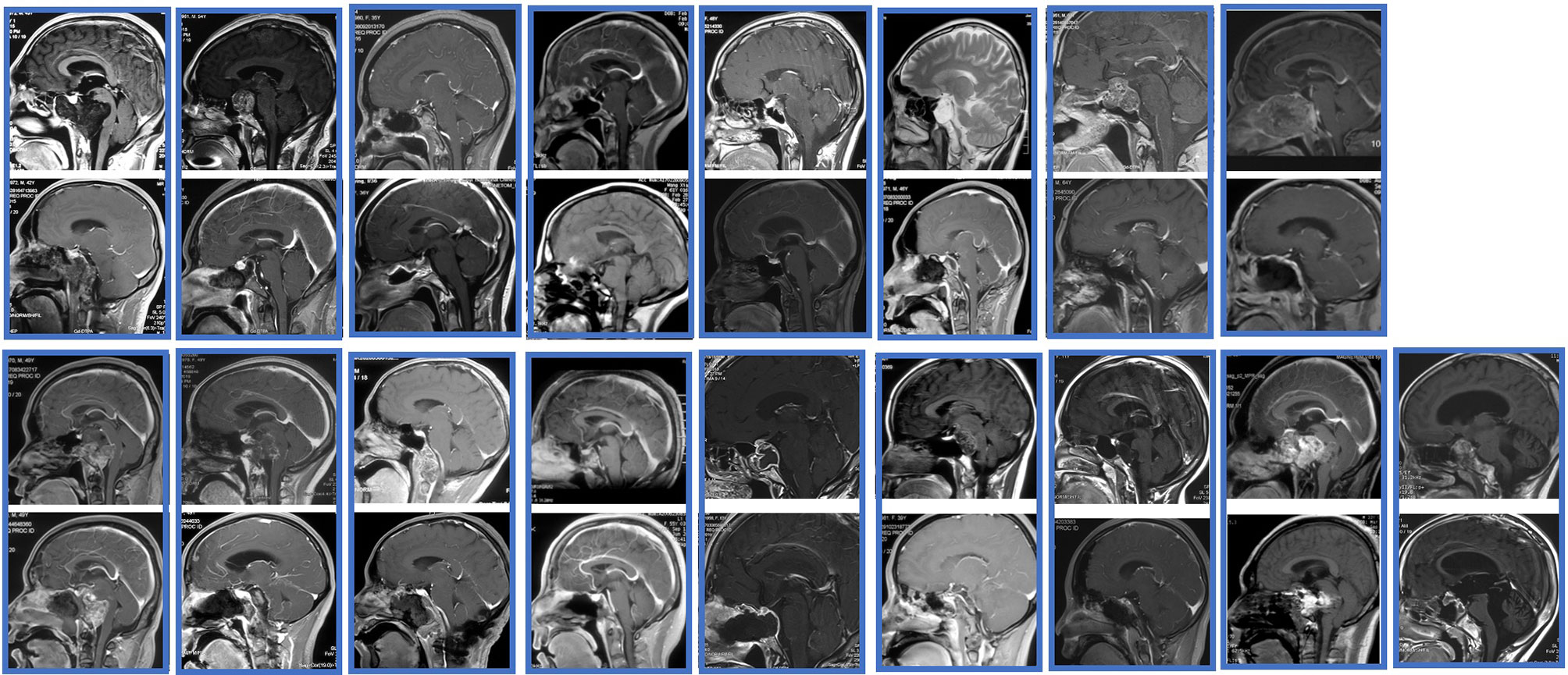
Figure 1 The pre- and post- MRIs of all the patients.
Gross total resection was performed in 7 cases (41%), STR in 7 case (41%) and PR in 3 case (18%) (Figure 1). The mean maximum diameters of the GTR, STR, and PR groups were 38.1, 51.1, and 64.3 mm, respectively. The value in the GTR group was significantly smaller than in the other 2 groups by multiple comparisons (P < 0.001, P < 0.001, respectively). The residual tumor was either in the cavernous sinus or in the subdural space, which could be adhered tightly to the dura and to the important vessels, such as the basal artery. Another reason for the tumor residual was due to the texture of the tumor. Headache and visual impairment or field defect were improved in most of the patients while five patients with the symptom of diplopia (5 in 6) resolved within 6 months after surgery. All the two patients with dysphagia and dysphonia were recovered within one year postoperation. The Ki-67 index ranged from 3-20%, with a mean value of 7.6%, showing its active proliferation capacity. Interestingly, the residual tumor in one of the three patients in the PR group showed rapid tumor growth in the follow up and died 12 months after surgery with a Ki-67 index of 20%.
As the tumor invaded the dura in 13 patients, the repair using the fascia of thigh muscle and H-B flap were performed in these patients. A second lumbar drainage after operation was used to manage the cerebrospinal fluid leakage. One patient developed cerebrospinal fluid leakage 2 weeks after the operation and required a secondary endoscopic repair. Postoperative bacterial meningitis was found in 3 patients who had no significant cerebrospinal fluid leakage. All three patients were successfully treated with intravenous antibiotics without any complications. One patient who received GTR developed deterioration of pituitary function after the EEA and received adrenocorticoid and thyroid hormone replacement therapy, while one in four patient who had pituitary function failure had normal function in the last follow-up. Two patients with GTR developed temporary diabetes after the EEA and were successfully treated with desmopressin. None of these patients developed persistent diabetes or new-onset neurological dysfunction. All the 7 patients with STR were considered for adjuvant radiotherapy, while only 4 of them have had radiotherapy and the other three chose to be monitored, including one female patient aged 10 years who were not suitable for radiotherapy. Till the last follow-up, three patients in STR group who received radiotherapy (3 in 4) had no tumor regrowth, while one in STR group with radiotherapy (1 in 4) showed tumor progression. Two patients in STR group without radiotherapy (2 in 3) showed stable tumor while the left one (1 in 3) showed tumor progression. One patient in the PR group died of tumor progression 2 years postoperation and the other one showed tumor progression and died of lung cancer 1 year postoperation. In addition, 1 in 7 patients with GTR had tumor recurrence in situ after 10 months and developed surgical pathway seeding in the spinal canal in C1 after 16 months. No recurrence occurred in the other 6 cases with GTR during the follow-up.
Chordomas were first described by Virchow in 1857 (10), while the term chordoma was first proposed by Ribbert in the 1890s, representing the microscopic characteristics of the tumor derived from undifferentiated notochordal remnants (11). According to the Surveillance, Epidemiology and End Results (SEER) database, the incidence of chordomas is 0.08 per 100,000, which occurs mainly in males, and occurs between 50 and 60 years of age, with a median survival of 6.29 years (12). Although chordomas represent only 0.2% of all central nervous system tumors, the most common site of origin is the clivus for intracranial chordomas. Because they are characterized by local destruction, dural invasion, bone erosion, and cranial nerve palsy, and even metastasis, clival chordomas are difficult to manage and easily recur, resulting in poor prognosis (13).
Chordomas may be located on the upper clivus, along the caudal edge of the clivus, the sellar area, sphenoid sinus, nasopharynx, maxilla, or even the intradural area (14). The clinical manifestations are varied and are associated with the location and involvement of adjacent structures of the clival chordoma. Patients usually present with headache, diplopia and vision loss. In rare oropharyngeal manifestations, dysphagia and speaking difficulties are present, which is common in clival chordoma with parapharyngeal and retropharyngeal extension (15). Although a definitive diagnosis of clival chordoma requires histopathological results with the characteristic material-like appearance of cells, typical clinical signs should be evaluated for the early diagnosis and treatment (16).
Although the lateral transcranial approach provides better vascular control and a better view of the brainstem-tumor interface (17), some have argued that EEA may not only provide direct surgical access but also provide a better visualization of surrounding structures, which is safer and minimally invasive (18). In the past decade, the use of EEA has been recommended more with increasing indications and better results (12). Here, we present our initial single-center experience and short-term outcomes after endoscopic endonasal approach resection of clival chordomas.
As surgery is the first-line treatment for clival chordoma, there are many surgical approaches for chordoma resection. Traditional transcranial approaches often lead to more brain tissue retraction with increased cerebral edema, hematoma and more damage to surrounding structures such as the basilar artery and optic nerve (19). As clival chordoma is located in the middle line of the skull base, EEA for clival chordoma resection can easily provide the surgical pathway and excellent exposure of the tumor and adjacent structures (especially the anterior dura and basilar arteries) (20, 21). The use of angled endoscopy has an advantage in showing hidden areas that cannot be seen with the transcranial approach. Zhang et al. proposed a surgical strategy for EEA according to the tumor growth directions, contributing to increasing the GTR rate (22). Therefore, EEA for clival chordoma resection has less morbidity compared to the transcranial approach (23). In our study, EEA resulted in a high GTR rate and a low surgical complication rate. Although intraoperative cerebrospinal fluid is very common, it is still inevitable during endoscopic surgery as cerebrospinal fluid repair could be performed after tumor resection with improved reconstructive techniques.
When the neurovascular structures of the surrounding area are locally invaded by the clival chordoma, the surgical principle is to minimize neurological dysfunction, even at the expense of having a postoperative residual tumor (12). After aggressive resection, radiotherapy could be used, with which residual tumors, especially small ones, can be effectively treated by radiotherapy. In 19 patients who underwent surgery and postoperative stereotactic radiotherapy, high-dose radiotherapy effectively controlled the small residual tumor volume (24). In a previous report, eleven patients underwent chordoma resection, of which 7 had subtotal or partial resections (24). Transient neurological deterioration (cranial nerve defects) occurred in seven patients, all of whom returned to neurological baseline. Following these considerations, 2 patients developed diplopia postoperatively but both returned to normal within 6 months in our case series, providing the evidence that the surgical strategies should not be overly aggressive, but should consider the option of radiotherapy and residual tumor observation.
Local recurrence is the main form of treatment failure (25). Radiotherapy can be used to treat recurrent clival chordoma patients who are not suitable for surgery (26). En bloc excision plus high dose radiation (27) or en bloc resection with proton beam radiation (28) were both the best evidences for improving survival in these patients. In our case series, one patient showed a recurrence in situ after EEA and gamma knife treatment was performed. After a follow-up of 16 months, a new lesion was seen in the spinal canal at C1 to C2, where an intradural spinal seeding chordoma was highly suspected. After a craniotomy, the lesion in the spinal canal was totally removed and the pathology confirmed a chordoma with increasing proliferative potential. And the patient was still in intensive follow-up.
Although the pathogenesis of chordoma is still unclear, loss of heterozygosity (LOH) of 1p36 is very common among sporadic chordomas and is related to tumorigenesis (29). As the molecular pathogenesis of clival chordoma is still unknown, no chemotherapy or targeted therapy has been developed until now. There is no specific genetic biomarker involved in predicting the recurrence and metastatic potential of chordomas. Although long-term prospective studies should be carried out to evaluate the role of endoscopic endonasal surgery in clival chordoma, endoscopic endonasal resection of clival chordoma is minimally invasive and reliable, which is correlated with a high GRT rate and a low morbidity.
Although more cases are needed, our case series showed EEA is a safe and reliable method for clival chordoma with high resection rates and low morbidity rates. GTR without tumor residuum would improve the outcome.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of Xuanwu Hospital Capital Medical University, Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article
Design, provision of patients, collection and assembly of data, data analysis and interpretation, manuscript writing. All authors contributed to the article and approved the submitted version.
The financial support for this study was provided by Beijing Hospitals Authority Youth Program (Code: QMS20210802 to XL).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
EEA, endoscopic endonasal approach; GTR, Gross total resection; PR, partially resection; STR, subtotal resection.
1. Castellanos LE, Gutierrez C, Smith T, Laws ER, Iorgulescu JB. Epidemiology of Common and Uncommon Adult Pituitary Tumors in the U.S. According to the 2017 World Health Organization Classification. Pituitary (2021) 27(1):201–9. doi: 10.1007/s11102-021-01189-6
2. Erdem E, Angtuaco EC, Van Hemert R, Park JS, Al-Mefty O. Comprehensive Review of Intracranial Chordoma. Radiographics (2003) 23(4):995–1009. doi: 10.1148/rg.234025176
3. Hug EB, Slater JD. Proton Radiation Therapy for Chordomas and Chondrosarcomas of the Skull Base. Neurosurg Clin N Am (2000) 11(4):627–38. doi: 10.1016/S1042-3680(18)30088-3
4. Noël G, Habrand JL, Jauffret E, de Crevoisier R, Dederke S, Mammar H, et al. Radiation Therapy for Chordoma and Chondrosarcoma of the Skull Base and the Cervical Spine. Prognostic Factors and Patterns of Failure. Strahlenther Onkol (2003) 179(4):241–8. doi: 10.1007/s00066-003-1065-5
5. Chugh R, Dunn R, Zalupski MM, Biermann JS, Sondak VK, Mace JR, et al. Phase II Study of 9-Nitro-Camptothecin in Patients With Advanced Chordoma or Soft Tissue Sarcoma. J Clin Oncol (2005) 23(15):3597–604. doi: 10.1200/JCO.2005.02.170
6. Zoli M, Milanese L, Bonfatti R, Faustini-Fustini M, Marucci G, Tallini G, et al. Clival Chordomas: Considerations After 16 Years of Endoscopic Endonasal Surgery. J Neurosurg (2018) 128(2):329–38. doi: 10.3171/2016.11.JNS162082
7. Yousaf J, Afshari FT, Ahmed SK, Chavda SV, Sanghera P, Paluzzi A. Endoscopic Endonasal Surgery for Clival Chordomas - A Single Institution Experience and Short Term Outcomes. Br J Neurosurg (2019) 33(4):388–93. doi: 10.1080/02688697.2019.1567683
8. Stippler M, Gardner PA, Snyderman CH, Carrau RL, Prevedello DM, Kassam AB. Endoscopic Endonasal Approach for Clival Chordomas. Neurosurgery (2009) 64(2):268–77. discussion 277-8. doi: 10.1227/01.NEU.0000338071.01241.E2
9. Hadad G, Bassagasteguy L, Carrau RL, Mataza JC, Kassam A, Snyderman CH, et al. A Novel Reconstructive Technique After Endoscopic Expanded Endonasal Approaches: Vascular Pedicle Nasoseptal Flap. Laryngoscope (2006) 116(10):1882–6. doi: 10.1097/01.mlg.0000234933.37779.e4
11. Horten BC, Montague SR. In Vitro Characteristics of a Sacrococcygeal Chordoma Maintained in Tissue and Organ Culture Systems. Acta Neuropathol (1976) 35(1):13–25. doi: 10.1007/BF00688940
12. McMaster ML, Goldstein AM, Bromley CM, Ishibe N, Parry DM. Chordoma: Incidence and Survival Patterns in the United States, 1973–1995. Cancer Causes Control (2001) 12:1–11. doi: 10.1023/A:1008947301735
13. Walcott BP, Nahed BV, Mohyeldin A, Coumans JV, Kahle KT, Ferreira MJ. Chordoma: Current Concepts, Management, and Future Directions. Lancet Oncol (2012) 13(2):e69–76. doi: 10.1016/S1470-2045(11)70337-0
14. Burge AJ. A Case of Oropharyngeal Chordoma. J Laryngol Otol (1975) 89(1):115–9. doi: 10.1017/S0022215100080142
15. Mindell ER. Chordoma. J Bone Joint Surg Am (1981) 63(3):501–5. doi: 10.2106/00004623-198163030-00035
16. Castro JR, Linstadt DE, Bahary JP, Petti PL, Daftari I, Collier JM, et al. Experience in Charged Particle Irradiation of Tumors of the Skull Base: 1977-1992. Int J Radiat Oncol Biol Phys (1994) 29(4):647–55. doi: 10.1016/0360-3016(94)90550-9
17. Tzortzidis F, Elahi F, Wright D, Natarajan SK, Sekhar LN. Patient Outcome at Long-Term Follow-Up After Aggressive Microsurgical Resection of Cranial Base Chordomas. Neurosurgery (2006) 59(2):230–37. doi: 10.1227/01.NEU.0000223441.51012.9D
18. Dehdashti AR, Karabatsou K, Ganna A, Witterick I, Gentili F. Expanded Endoscopic Endonasal Approach for Treatment of Clival Chordomas: Early Results in 12 Patients. Neurosurgery (2008) 63(2):299–307. doi: 10.1227/01.NEU.0000316414.20247.32
19. Hong Jiang W, Ping Zhao S, Hai Xie Z, Zhang H, Zhang J, Yun Xiao J. Endoscopic Resection of Chordomas in Different Clival Regions. Acta Otolaryngol (2009) 129(1):71–83. doi: 10.1080/00016480801995404
20. Koutourousiou M, Gardner PA, Tormenti MJ, Henry SL, Stefko ST, Kassam AB, et al. Endoscopic Endonasal Approach for Resection of Cranial Base Chordomas: Outcomes and Learning Curve. Neurosurgery (2012) 71(3):614–25. doi: 10.1227/NEU.0b013e31825ea3e0
21. Kassam AB, Prevedello DM, Carrau RL, Snyderman CH, Thomas A, Gardner P, et al. Endoscopic Endonasal Skull Base Surgery: Analysis of Complications in the Authors’ Initial 800 Patients. J Neurosurg (2011) 114(6):1544–68. doi: 10.3171/2010.10.JNS09406
22. Bai J, Li M, Xiong Y, Shen Y, Liu C, Zhao P, et al. Endoscopic Endonasal Surgical Strategy for Skull Base Chordomas Based on Tumor Growth Directions: Surgical Outcomes of 167 Patients During 3 Years. Front Oncol (2021) 22(11):724972. doi: 10.3389/fonc.2021.724972
23. Bongers MER, Dea N, Ames CP, Schwab JH. Surgical Strategies for Chordoma. Neurosurg Clin N Am (2020) 31(2):251–61. doi: 10.1016/j.nec.2019.11.007
24. Potluri S, Jefferies SJ, Jena R, Harris F, Burton KE, Prevost AT, et al. Residual Postoperative Tumor Volume Predicts Outcome After High-Dose Radiotherapy for Chordoma and Chondrosarcoma of the Skull Base and Spine. Clin Oncol (R Coll Radiol) (2011) 23(3):199–208. doi: 10.1016/j.clon.2010.09.011
25. Gheorghiu ML, Gheorghisan-Galateanu AA. Clivus Chordoma. Acta Endocrinol (Buchar) (2019) 15(3):406. doi: 10.4183/aeb.2019.406
26. Hafez RFA, Fahmy OM, Hassan HT. Gamma Knife Surgery Efficacy in Controlling Postoperative Residual Clival Chordoma Growth. Clin Neurol Neurosurg (2019) 178:51–5. doi: 10.1016/j.clineuro.2019.01.017
27. Boriani S, Chevalley F, Weinstein JN, Biagini R, Campanacci L, De Iure F, et al. Chordoma of the Spine Above the Sacrum. Treatment and Outcome in 21 Cases. Spine (Phila Pa 1976) (1996) 21(13):1569–77. doi: 10.1097/00007632-199607010-00017
28. Hug EB, Loredo LN, Slater JD, DeVries A, Grove RI, Schaefer RA, et al. Proton Radiation Therapy for Chordomas and Chondrosarcomas of the Skull Base. J Neurosurg (1999) 91(3):432–9. doi: 10.3171/jns.1999.91.3.0432
Keywords: clival chordoma, endoscopic transnasal approach, surgical outcome, surgical complications, single center experience
Citation: Chen G, Li M, Xu W, Wang X, Feng M, Wang R and Liu X (2022) Surgical Outcomes of Clival Chordoma Through Endoscopic Endonasal Approach: A Single-Center Experience. Front. Endocrinol. 13:800923. doi: 10.3389/fendo.2022.800923
Received: 24 October 2021; Accepted: 14 March 2022;
Published: 06 April 2022.
Edited by:
Run Yu, University of California, Los Angeles, United StatesReviewed by:
Xiaorong Yan, First Affiliated Hospital of Fujian Medical University, ChinaCopyright © 2022 Chen, Li, Xu, Wang, Feng, Wang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaohai Liu, bGl1eGlhb2hhaTA5QDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.