 Li Rong
Li Rong Junyan Zou
Junyan Zou Wei Ran3
Wei Ran3 Yaokai Chen
Yaokai Chen Hongjuan Cui
Hongjuan Cui Jinjun Guo
Jinjun Guo
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol. , 16 January 2023
Sec. Gut Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1087260
This article is part of the Research Topic The NAFLD-MAFLD Conundrum View all 8 articles
Non-alcoholic fatty liver disease (NAFLD) is a series of diseases, involving excessive lipid deposition in the liver and is often accompanied by obesity, diabetes, dyslipidemia, abnormal blood pressure, and other metabolic disorders. In order to more accurately reflect its pathogenesis, an international consensus renamed NAFLD in 2020 as metabolic (dysfunction) associated with fatty liver disease (MAFLD). The changes in diet and lifestyle are recognized the non-drug treatment strategies; however, due to the complex pathogenesis of NAFLD, the current drug therapies are mainly focused on its pathogenic factors, key links of pathogenesis, and related metabolic disorders as targets. There is still a lack of specific drugs. In clinical studies, the common NAFLD treatments include the regulation of glucose and lipid metabolism to protect the liver and anti-inflammation. The NAFLD treatments based on the enterohepatic axis, targeting gut microbiota, are gradually emerging, and various new metabolism-regulating drugs are also under clinical development. Therefore, this review article has comprehensively discussed the research advancements in NAFLD treatment in recent years.
With the deepening of the research on the mechanism of Non-alcoholic fatty liver disease(NAFLD), the two-hit theory cannot fully explain interactions between genetics and environment as well as those between different organ systems; therefore, the multi-hit theory has gradually been accepted (1). Currently, NAFLD is considered a complex metabolic disease, resulting from the complex interactions among genetic susceptibility, host metabolic disorders, and environmental factors. Numerous factors affect its clinical manifestations and disease progression, including race, genetic susceptibility, dietary habits, metabolism, immunity, gut microbiota, and other factors. Insulin resistance is one of the recognized mechanisms of NAFLD. However, the interaction between lipid metabolism disorder and its triggered inflammatory response can jointly promote the occurrence and development of NAFLD. In recent years, numerous genome-wide studies on NAFLD identified multiple polymorphic changes in the genes associated with the susceptibility to NAFLD, suggesting that both the genetic and epigenetic changes might play an important role in the pathogenesis of NAFLD. The abnormal immune microenvironment of the liver and its mediated inflammatory response might also play an important role in the pathogenesis of NAFLD. More studies showed that the changes in the composition and structure of gut microbiota might also have an important impact on the occurrence and development of NAFLD. The incidence of NAFLD is continuously increasing rapidly worldwide and has become the primary cause of chronic liver diseases in the world. Therefore, the studies and development of targeted drugs based on the above-mentioned important links in the pathogenesis of NAFLD are also in full swing. Therefore, it is necessary to have a systematic understanding of the current treatment methods and drugs for NAFLD in order to provide a certain reference and help effectively improve the clinical prognosis of NAFLD patients.
Although the exact pathogenesis of NAFLD remains to be elucidated, the associated risk factors are clear and include unhealthy lifestyle, insulin resistance (IR), type 2 diabetes mellitus (T2DM), increased liver lipogenesis, and dysregulation of gut microbiota. There is currently no standard treatment for NAFLD; however, the clinical practice guidelines of the European Association for the Study of Liver (EASL) -European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO) (2) and the American Association for the Study of Liver Diseases(AASLD) Practice Guidelines (3) clearly state that the lifestyle changes can lead to 5-10% weight loss in the overweight/obese NAFLD patients. Furthermore, the National Institute for Health and Care Excellence (NICE) guidelines (4) also recommend changes in lifestyle as the first choice of treatment for NAFLD patients. Therefore, optimizing the lifestyle through a rational diet and exercise intervention is undoubtedly the basis and important link of NAFLD treatment. The combination of drugs, which can effectively regulate glucose and lipid metabolism and reduce liver inflammation and fibrosis, might be more beneficial for the treatment of NAFLD.
Severely restricting total calories, inducing ketosis, or reducing free sugar intake and limiting carbohydrate consumption can enhance liver protection, thereby making the dietary interventions a promising strategy for the treatment of NAFLD (5). Caloric restriction (CR) is the most common dietary intervention treatment strategy for NAFLD.
A meta-analysis found that western dietary patterns could increase the risk of NAFLD by 56%, indicating that dietary pattern was associated with the risk of NAFLD, whereas a Mediterranean diet (MD) could reduce this risk by 23% (6). MD is defined as a plant-based diet characterized by a high proportion of monounsaturated fatty acids (MUFA) and saturated fatty acids (SFA), in which, the total fat accounts for 30-40% of the daily energy consumption (7), and is based on fruits and vegetables, fish, whole grains, legumes, and olive oil (8). The EASL-EASD-EASO Clinical Practice Guidelines recommend MD as an optional diet for the treatment of NAFLD because MD can improve metabolism by reducing IR and lipid concentrations and induce the regression of steatosis as well as significantly reduce the cardiovascular events (1, 2, 7, 9, 10). Therefore, this might be an effective and safe approach for the treatment of patients with MS and NAFLD (11). MD could improve overweight and visceral obesity, reduce hepatic steatosis, and reduce liver cirrhosis in NAFLD patients (12–14). It could also improve IR, which in turn improved the disease condition of NAFLD patients (7, 15). A meta-analysis by Japanese scholar Takumi Kawaguchi also confirmed this view that MD could improve hepatic steatosis and IR in patients with NAFLD (16). Recently, clinical trials have provided evidence of MD feasibility in adolescents and children with NAFLD. In children aged 9-17 years with NAFLD, the 12-week administration of MD could improve IR (17). Similarly, this diet plan could reduce the body mass index (BMI), fat mass, and hepatic steatosis, improve IR, and reduce the levels of transaminases, inflammatory markers, and oxidative stress markers in children aged 11-18 years with NAFLD (18).
In addition to MD, the ketogenic diet (KD) has also been used as a dietary intervention for the treatment of NAFLD in recent years. KD has a high proportion of fats and a low proportion of carbohydrates, proteins, and other nutrients, and due to its extremely low proportion of carbohydrates, it also plays a positive role in the treatment of NAFLD (19). It can significantly alter the mitochondrial flux and redox status of the liver to promote ketogenesis without affecting the synthesis of intrahepatic triglycerides (IHTG), thereby significantly improving the visceral fat contents and IR (20). Although the above studies suggest that KD has certain therapeutic effects on NAFLD patients, several animal and clinical trials have indicated its risk. An animal study showed that the high-fat diet (HFD)-induced obese or NAFLD male C57Bl/6NJ mice were likely to develop hepatic mitochondrial dysfunction after the long-term intervention of KD (21). A case study has also reported the risks of acutely-worsened hyperlipidemia and elevated liver enzymes associated with a KD (22). Therefore, based on the current clinical research results, the safety of KD for the treatment of NALFD requires further investigations.
In addition, several new dietary interventions have been used for the gradual treatment of NAFLD patients. For example, a low-calorie and low-fat diet could significantly reduce the liver fat contents (LFCs) in NAFLD patients in the short term (23). A high-protein (animal or plant) diet could also significantly reduce the LFC, IR, and levels of inflammatory markers (24). An eight-week free sugar restriction diet could reduce liver fat (25) and improve liver steatosis in adolescent boys with NAFLD (26). However, due to the limited number of clinical trials based on these dietary interventions, they have not yet drawn sufficient conclusions. Similarly, there is limited clinical data and unclear results for the interventions of very low-calorie KD (VLCKD), intermittent feeding (IF), and time-restricted feeding (TRF); Therefore, their safety and effectiveness cannot be verified currently.
In addition to dietary intervention, exercise can also improve glucose and lipid metabolism disorders (27) and reduce LFC (28) and is an effective method for the treatment of metabolic-related diseases. Regular exercise can effectively treat NAFLD in both non-obese and obese patients (29), and the combination of resistance exercise and aerobic exercise has been proved to be more reasonable and effective in clinical practice. For instance, resistance exercise is relatively safe and could effectively improve the metabolic status of NAFLD patients (30). A 12-week resistance exercise, consisting of push-ups and squats, could help in the prevention of NAFLD progression (31). Aerobic exercise also showed similar effects. A 12-week aerobic exercise intervention could improve liver fibrosis (32). Furthermore, the high-intensity interval (HII) exercise for 12 weeks could reduce the blood glucose contents and waist circumference in NAFLD patients (33). The individually designed eight-week exercise program could reduce liver steatosis, the level of inflammatory markers including hypersensitivity C-reactive protein (hs-CRP), and ferritin, and reduce fibrosis (34). However, studies have shown that there was no significant difference in the effects of the different amounts or intensities of aerobic exercise on the LFC; the 8 weeks of low-medium-intensity high-volume aerobic exercise, moderate-to-low-intensity low-volume aerobic exercise, and high-intensity low-volume aerobic exercise could reduce LFC and visceral adipose tissue (VAT) with insignificant differences between them (35). Both the HII and moderate-intensity continuous (MIC) aerobic exercise for 8 weeks could reduce IHTG and visceral fats in obese NAFLD patients with T2DM (36).
The sample size of these clinical studies on exercise intervention was relatively small, and most of the researchers only focused on observing the effects of an exercise intervention on certain body indices, such as BMI, blood sugar, LFC, etc., in patients with NAFLD (37). At the same time, most relevant studies did not focus on the benefits of an exercise intervention on liver fibrosis in NAFLD patients. Therefore, there is currently insufficient evidence that these interventions might bring definite benefits to patients with NAFLD.
The methods of combining exercise with caloric restriction might affect NAFLD by increasing energy expenditure, reducing lipid overload, and improving metabolic homeostasis (15). This dual intervention approach might have better effects both in animal and clinical studies. Exercise and changing the diet from an HFD to a regular diet could alleviate HFD-induced hepatic steatosis in Sprague Dawley (SD) rats (38).
In a randomized controlled trial, the combination of exercise with a green-MD (a diet with a limited amount of red/processed meat and an increased proportion of green plants and polyphenols in MD) could further reduce intrahepatic fat contents and NAFLD prevalence as compared to normal diet and MD (39). Similarly, a randomized controlled trial (40) reported that exercise and dietary interventions could improve LFC and glucose metabolism in NAFLD patients. These studies suggested that the combination of exercise with dietary intervention might have a better effect on NAFLD patients (41). Therefore, for obese patients with NAFLD, who have time and energy, a combination of exercise and diet interventions should be prioritized.
Bariatric surgery is an option for obese patients with NAFLD, who are non-responsive to dietary changes and exercise or unable to lose weight through lifestyle changes. Bariatric surgery is another common method for the treatment of obesity in the United States and European countries, but it is relatively rare in China. The American Society for Metabolic and Bariatric Surgery Pediatric Committee (ASMBS) recommends metabolic and bariatric surgery (MBS) as an effective treatment for severe obesity in adolescents and should be considered the standard of care (42). Similarly, the AALSD practice guidelines also recommend that foregut bariatric surgery might be considered in obese patients with NAFLD or NASH (43). Bariatric surgery can improve liver histology, including fibrosis, which is secondary to NASH. In addition, bariatric surgery has other benefits, including improvement or remission of T2DM, dyslipidemia, and hypertension, and reduction of cardiovascular disease (CVD)’s morbidity or mortality (44). Bariatric surgery could also significantly improve the BMI and liver fibrosis scores (45) as well as all the histological features of NAFLD, including fibrosis (2, 3, 46).
As any surgical treatment has risks, bariatric surgery is also not completely safe and effective. The condition of a NAFLD patient deteriorated after bariatric surgery. Although the patient lost 35% of his body weight rapidly, he developed acute liver failure as a serious complication (47). There are high risks of postoperative complications in patients with cirrhosis reportedly, while in well-compensated cirrhotic patients, it might be used as an aid to improve the long-term outcome (48). Overall, the clinical efficacy and safety of bariatric surgery require further investigations to make it suitable for NAFLD patients.
Although the exact pathogenesis of NAFLD is still unclear, IR plays a key role in the development of NAFLD. The prevalence of NAFLD is high in T2DM patients; it is closely associated with obesity, hyper-glycated hemoglobin, hyperlipidemia, and hyper-alanine aminotransferase (hyper-ALT) (49). Therefore, antidiabetic drugs are often used for the clinical treatment of T2DM patients with NAFLD.
GLP-1, an intestinal hormone released from the foregut in response to food consumption, can stimulate insulin secretion and inhibit glucagon secretion. GLP-1RAs, such as liraglutide, semaglutide, dulaglutide, exenatide, etc., are new antidiabetics. Studies showed that these drugs could reduce body weight and improve IR as well as improve liver enzyme levels and reduce LFC in T2DM patients; this might be beneficial for the treatment of NAFLD/NASH patients (50). Therefore, these drugs have often been used in clinical studies of NAFLD in recent years.
Liraglutide has been the most widely studied GLP-1RA drug in NAFLD (51), which can improve IR (52) and reduce LFC in T2DM patients (53). A Phase II clinical trial showed that the subcutaneous injection of liraglutide at a dose of 1.8 mg/d in NASH patients could improve the histopathology of the liver, which was manifested as regression of NASH, patient’s well-tolerance, and no progression of liver fibrosis (54). In a study by Feng et al., the treatment effects of liraglutide on T2DM patients with NAFLD were better than that of metformin and gliclazide (55), mainly in reducing the body weight, waist circumference, and intrahepatic fat contents. However, in terms of safety, as shown in clinical trials, the use of liraglutide is often associated with some mild gastrointestinal adverse reactions, including diarrhea, constipation, loss of appetite, etc. (54).
A study by Philip Newsome’s team found that obesity and T2DM were the drivers of NAFLD, and semaglutide could significantly reduce plasma ALT and hs-CRP levels in obese patients with T2DM; this demonstrated the potential of semaglutide for alleviating NAFLD (56). Then, they launched a randomized, placebo-controlled phase II clinical trial to investigate the clinical efficacy of semaglutide by subcutaneously injecting its different doses into patients with NASH. After 72 weeks of treatment, NSAH in the experimental group was relieved, which was mainly reflected in the reduction of liver inflammatory cells and liver cell degeneration; moreover, the proportion of patients with no further liver fibrosis was significantly higher than that in the control group. The optimal injection concentration obtained from the clinical trial was 0.4 mg/d, which showed the best effects. However, semaglutide could not significantly improve the degree of liver fibrosis in the patients (57). Currently, they are planning a phase III clinical trial to further validate the clinical efficacy of semaglutide in improving metabolic disorders (58). A study by Anne Flint’s team also showed that as compared to placebo, the subcutaneous injection of semaglutide at a dose of 0.4 mg/d could reduce LFC and improve liver enzyme levels; however, the effects on remission of liver cirrhosis were not obvious (59). Similar to liraglutide, semaglutide has some gastrointestinal side effects, among which, nausea is the most common (57, 60).
The subcutaneous injection of dulaglutide at a dose of 1.5 mg/week could reduce plasma ALT, aspartate aminotransferase (AST), and γ-glutamyl transpeptidase (GGT) levels in the patients with T2DM (61). Therefore, this drug could be applied for alleviating NAFLD. As compared to liraglutide, dulaglutide had the advantage of less frequent injections, usually once a week. A study by Kuchay et al. showed that the subcutaneous injection of dulaglutide at a dose of 1.5 mg/week could significantly reduce LFC and GGT in patients with T2DM and NAFLD without serious adverse reactions. Consequently, they suggested that dulaglutide could be used for the early treatment of T2DM patients with NAFLD (62). Similarly, a study conducted in Japan also showed that the subcutaneous injection of dulaglutide at a dose of 0.75 mg/week for 12 weeks could reduce body weight and improve liver enzyme levels in T2DM patients with NAFLD (63).
An early study reported that exenatide could improve blood glucose, body weight, and liver enzyme levels in T2DM patients with NAFLD (64). Due to the good liver protecting effects of exenatide, it was more suitable for NAFLD patients with obesity, elevated liver enzymes, and T2DM (65). A recent study by Liu et al. showed that the subcutaneous injection of exenatide at a dose of 10 μg twice a day could also reduce LFC in T2DM patients with NAFLD (66). A study conducted in Turkey also confirmed that the same dose of exenatide treatment could reduce blood sugar, reduce body weight, and improve liver fibrosis scores in T2DM patients with NAFLD (67). Gastaldelli et al. showed that the combination of exenatide and dapagliflozin was more effective as compared to their single drug treatment in the T2DM patients with NAFLD; this provided a novel treatment idea for the use of clinical drugs; however, more prospective trials are needed to verify these results (68).
Overall, most of the clinical studies conducted on using GLP-1RA drugs for the treatment of T2DM complicated with NAFLD or NASH showed that these drugs were safe and effective (Table 1), and the most common side effects included some gastrointestinal adverse reactions, such as diarrhea, nausea, vomiting, constipation, loss of appetite, etc. However, numerous prospective studies are needed to explore the reasonable dose and duration of these drugs.
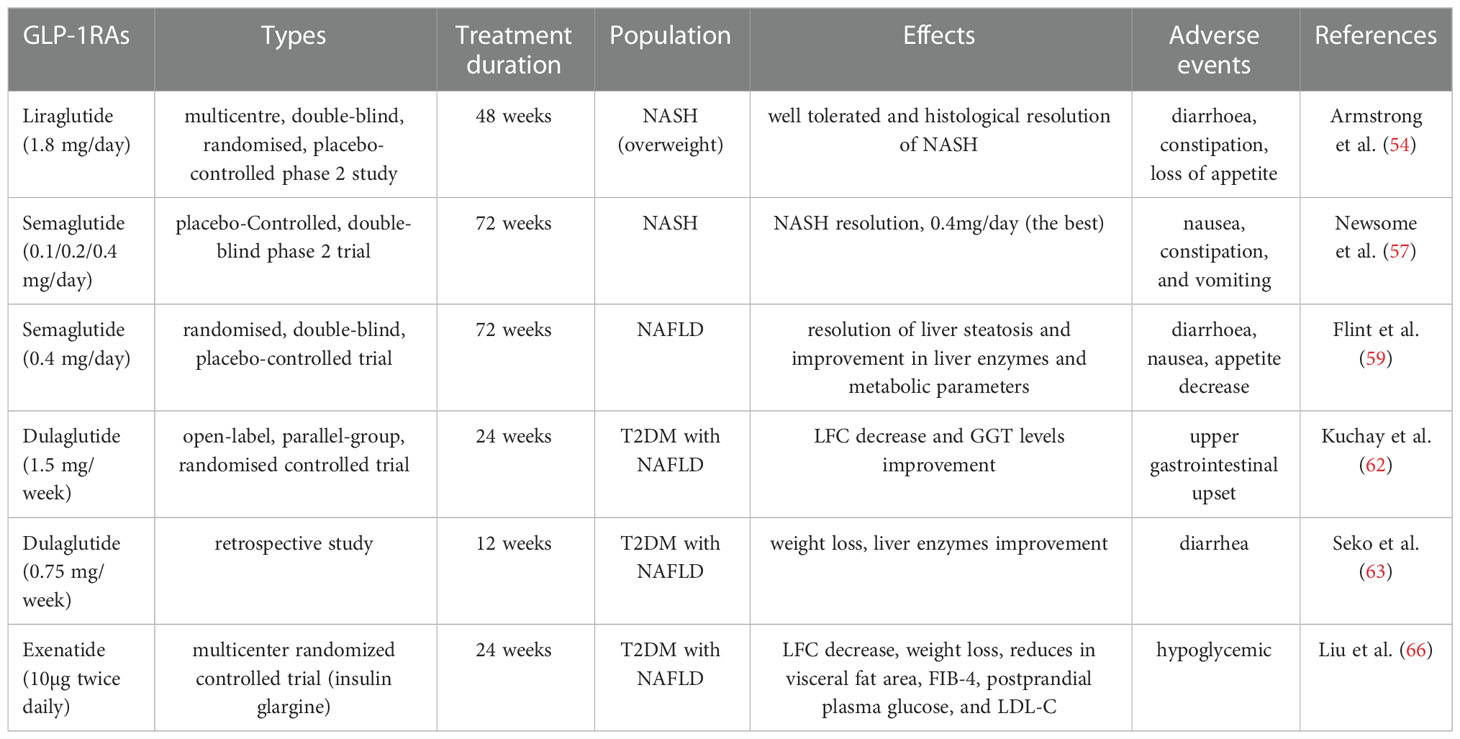
Table 1 Effect of GLP-1RAs in patients of NAFLD/NASH: Data from clinical studies.
SGLT2i is a new type of oral antidiabetic drug, which can inhibit the reabsorption of glucose by the kidneys, thereby reducing blood glucose levels. A retrospective analysis found that SGLT2i could improve steatosis and fibrosis in patients with T2DM, therefore, they might be beneficial for the NAFLD patients (69). Japanese researchers conducted a five-year follow-up study on six T2DM patients with NAFLD and showed that three patients had improved liver histology after SGLT2i treatment (70). An 18-month randomized study by Korean researchers suggested that adding SGLT2i to common anti-sugar therapy in T2DM patients could better reduce fat contents and improve liver enzyme levels (71). A meta-analysis, summarizing 10 clinical trials, indicated that drug therapy with SGLT2i could improve LFC, liver enzyme levels, BMI, inflammatory markers, etc. in Asian T2DM patients with NAFLD (72). Likewise, another systematic review also confirmed the ameliorating effects of SGLT2i on LFC and liver enzyme levels (73).
Clinical trials have also proved the above point of view. Gaborit et al. suggested that the oral administration of empaglifozin (EMPA) at a dose of 30 mg/kg/day for 12 weeks in the C57BL/6 mice could reduce LFC, while the oral administration of EMPA at a dose of 10 mg/day for 12 weeks in T2DM patients could also reduce LFC effectively (74). Coincidentally, a randomized double-blind placebo-controlled phase IV clinical trial showed that the oral administration of EMPA at a dose of 25 mg/day for 24 weeks could effectively control blood sugar and reduce LFC in patients with T2DM (75). Recently, another trial in T2DM patients with CVD showed that either 10 or 25 mg/d EMPA treatment could reduce steatosis, but not liver fibrosis risk (76). Furthermore, in NAFLD patients without T2DM, the oral administration of 10 mg/d EMPA for 24 weeks could also improve hepatic steatosis and fibrosis (77).
Similarly, the oral administration of ipragliflozin at a dose of 50 mg/day for 24 weeks could improve liver enzyme levels and fasting blood glucose levels in T2DM patients with NAFLD (78). Japanese researchers reported similar findings (79). In another multicenter, open-label randomized controlled trial, a treatment regimen of 72 weeks with ipragliflozin could improve liver fibrosis, blood sugar levels, and obesity in NAFLD patients, and none of the patients developed NASH compared as compared to controls; therefore, ipragliflozin might play a role in the prevention and treatment of NASH (80).
In a double-blind, controlled, randomized trial, the oral administration of dapagliflozin at a dose of 10 mg/day for 8 weeks reduced serum aminotransferase levels and LFC in the patients with T2DM, which was beneficial to the liver (81). When applied to the T2DM patients with NAFLD, and the treatment regimen was extended to 12 weeks, dapagliflozin reduced the levels of hepatocyte injury biomarkers, including ALT, AST, GGT, etc., in patients, indicating an improving effect of dapagliflozin on NAFLD (82). A prospective study by Japanese researchers showed that in addition to the local standard of care for T2DM, the oral administration of dapagliflozin at a dose of 5 mg/day for 24 weeks could improve hepatic steatosis in T2DM patients with NAFLD and attenuate hepatic fibrosis in patients with significant hepatic fibrosis (83). As for the efficacy of dapagliflozin in NAFLD patients without T2DM, another prospective study by Japanese researchers, including 12 patients, showed that the oral administration of dapagliflozin at a dose of 5 mg/d for 12 weeks could reduce weight and improve liver enzymes (84).
There are relatively few studies on the administration of canagliflozin. The oral administration of canagliflozin at a dose of 100 mg/day for 24 weeks could improve liver function and reduce visceral fat, thereby exhibiting therapeutic potential for T2DM patients with NAFLD (85). However, this study included only five patients. Another retrospective study had the same limitation. A study of 7 patients suggested that the long-term treatment with canagliflozin at a dose of 100 mg/d could improve liver histology in six patients and worsen it in one patient (86). Therefore, further studies are needed to discover the efficacy of canagliflozin.
To sum up, in clinical studies, most of the SGLT2i drugs are applied to T2DM patients with NAFLD (Table 2). Although there are fewer clinical studies on the applications of these drugs to NAFLD patients without T2DM, they have good application prospects. The safety of drugs should also be investigated. SGLT2i has several adverse reactions, such as hypoglycemia, ketoacidosis, and urinary tract and genital infections, when used for the treatment of T2DM patients (87). As a result, their clinical use in patients with NAFLD requires more exploration.
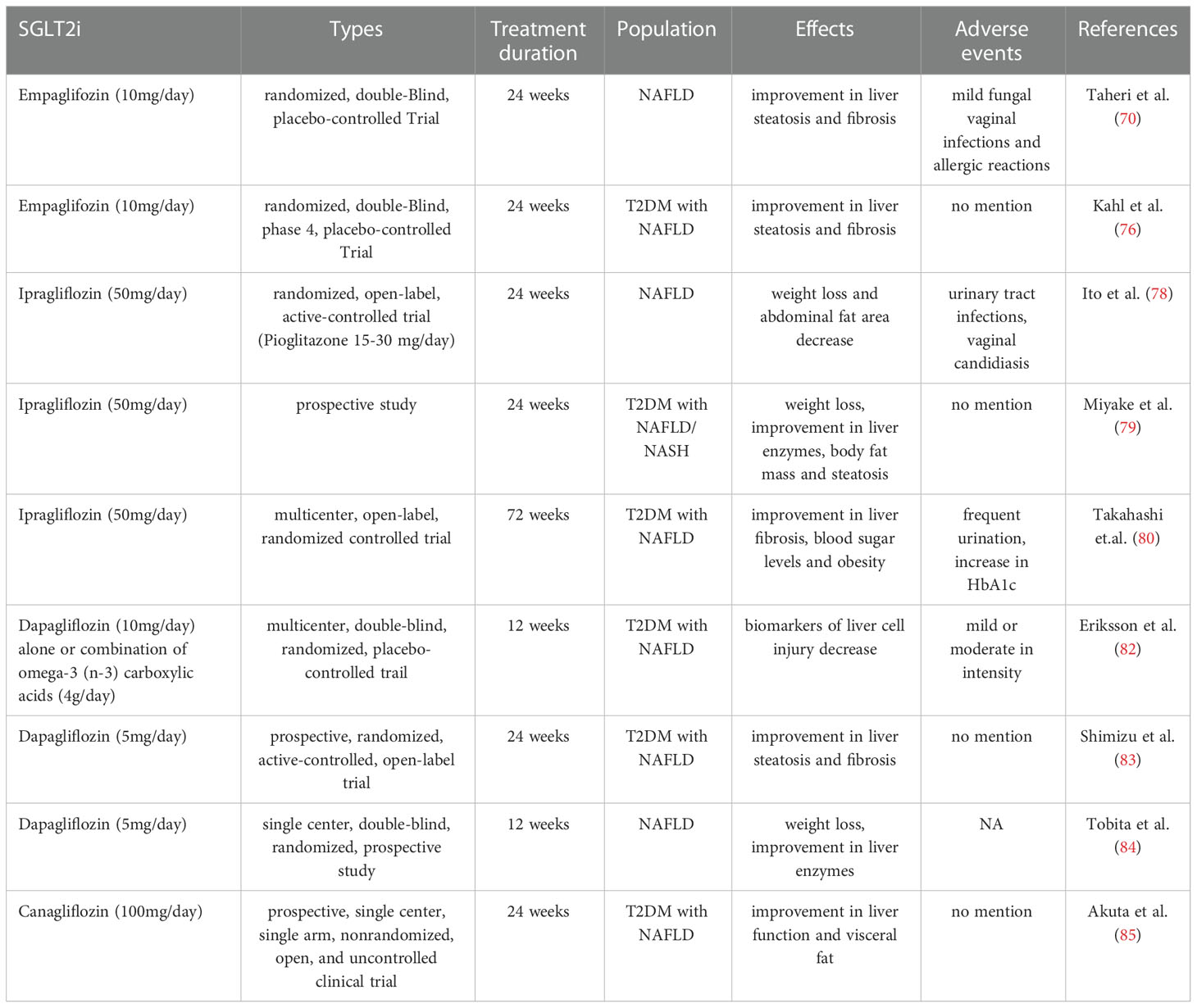
Table 2 Effect of SGLT2i in patients of NAFLD/NASH: Data from clinical studies.
Biguanides are very effective in the treatment of T2DM. Metformin, a common antidiabetic drug, is an example of biguanides. It can reduce endogenous glucose production, activate AMPK, and inhibit mitochondrial glycerophosphate dehydrogenase (88); however, its safety and efficacy in NAFLD patients are still controversial (89). In an animal experiment, the administration of 300 mg/kg/d metformin in diet could reduce the occurrence of NAFLD in C57Bl/6J mice as compared to the high-sugar and high-fat diets alone (90). However, unlike animal experiments, metformin did not show the same effects in clinical studies. Metformin showed modest improvement in body weight, waist circumference, and liver enzyme levels after 24 weeks of long-term treatment in T2DM patients with NAFLD (55). Similarly, a systematic review and meta-analysis demonstrated that metformin treatment could not improve liver histopathology in NASH patients (91). In recent years, its effectiveness has been controversial. Japanese researchers showed that increasing the dose of metformin to 1500 mg 2-3 times/d for 52 weeks could reduce hepatic steatosis in T2DM patients with NAFLD (92). A study by Mitrovic et al. demonstrated that metformin could also reduce the levels of hs-CRP, ferritin, and other inflammatory factors in non-obese T2DM patients with NAFLD (93). In addition, some clinical trials investigated the concomitant effects of metformin with GLP-1RA or SGLT2i in T2DM patients with NAFLD; however, their effects were not satisfactory. For example, a 24-week prospective randomized placebo-controlled trial by Harreiter et al. showed that metformin combined with exenatide or dapagliflozin did not show additive effects on hepatocyte lipid reduction (94). Overall, there is insufficient evidence that Metformin has a definite effect in the treatment of NAFLD; however, some studies suggest that Metformin might play a role in the prevention of hepatocellular carcinoma and tumors (95), which requires further studies.
Thiazolidinediones act as peroxisome proliferator-activating receptor PPAR-γ agonists that improve IR in obese and concomitant type 2 diabetes mellitus. Pioglitazone is the only diabetic agent incorporated into the treatment guidelines for NASH (2, 3, 96). A randomized controlled trial showed that the oral administration of metformin at a dose of 2g/d combined with a low dose (mean 26 mg/d) of pioglitazone for one year could improve liver steatosis, inflammation, and IR in the T2DM patients with NAFLD (97). The effectiveness of pioglitazone alone was investigated in a placebo-controlled study. The oral administration of pioglitazone at a dose of 30 mg/d for 96 weeks could improve liver histology, liver enzyme levels, and IR in non-diabetic NASH patients (98). Similarly, in a study by Aithal et al., a treatment regimen with the same dose for 12 months could improve liver metabolic and histological parameters, most notably in the level of liver injury and fibrosis in NASH patients (99). The restricted dietary interventions combined with pioglitazone therapy might also improve liver metabolism in NASH patients. In a study by Renata Belfort et al., a low-calorie diet (500-kcal/d deficit from weight-maintaining caloric intake) combined with 45 mg/d pioglitazone for 6 months could improve metabolism and liver histology in the NASH patients (100). Similar results were also demonstrated by Kenneth Cusi et al. A treatment regimen with the same intervention conditions described above for 18 months was safe and effective in the patients with prediabetes or T2DM and NASH as well as improved their liver histology without worsening fibrosis (71). However, pioglitazone is not suitable for all patients. It might aggravate lower extremity edema; therefore, caution should be taken in patients with severe obesity, diastolic dysfunction, congestive heart failure, concomitant use of amlodipine or high-dose insulin, etc (96).
In general, the antidiabetic drugs used to alleviate NAFLD have certain clinical effects and research potential. Relevant guidelines have also recommended some antidiabetic drugs for the clinical treatment of NAFLD.
Statins, common clinical lipid-lowering drugs, can inhibit cholesterol synthesis by blocking 3-hydroxy-3-methyl glutaryl coenzyme A (HMG-CoA) reductase (101). Dyslipidemia in NAFLD patients is typically characterized by elevated triglyceride (TG) and low-density lipoprotein cholesterol (LDL-C) levels and reduced high-density lipoprotein cholesterol (HDL-C) levels, and the deposition of hepatic cholesterol also contributes to the progression of NAFLD (102, 103). A meta-analysis by Kim et al. showed that statins could reduce the risk of cirrhotic decompensation and mortality in patients with cirrhosis, while in the non-cirrhotic patients, statins were not significantly associated with the risk of developing cirrhosis or fibrosis progression (104). However, Athyros et al. suggested a different view. They suggested that statin therapy might play a role in reducing steatosis and improving steatohepatitis and fibrosis (105). A large population-based nested case-control study backed up their point. Statin could reduce NAFLD risk and liver fibrosis risk in NAFLD patients (106). Another four-year study reported that the administration of atorvastatin at a dose of 20 mg in combination with vitamins could effectively reduce the odds of developing hepatic steatosis by 71% in NAFLD patients (107). Similarly, the oral administration of rosuvastatin at a dose of 5 mg/d for 24 weeks could also reduce LFC in patients (108).
However, it has long been generally accepted that statin is potentially hepatotoxic; therefore, its use for the treatment of NAFLD patients has been low in the past. A recent analysis of trends in statin use among adults with NAFLD in the United States suggested that the onset of NAFLD was associated with inadequate early statin use in the disease (109). With the in-depth study of statin, this trend is gradually changing. Studies also showed that statin was associated with a significant reduction in cancer-related mortality in NAFLD patients (110). NAFLD/NASH patients often have a high CVD risk. Studies showed that the application of statins could significantly reduce the CVD risk of NAFLD/NASH patients (111). In a randomized controlled trial, evaluating the effects of pioglitazone in the treatment of NASH, a post hoc analysis of the statin safety showed that statin could reduce plasma total cholesterol levels and LDL-C levels. The three-year follow-up reported no adverse effect of statin on liver enzyme levels; therefore, they suggested that it could be used in T2DM patients with NAFLD (112). On the other hand, the analysis of statin use and risk of new-onset diabetes indicated that statins were associated with a risk of hyperglycemia and their use should be limited in patients with prediabetes or at risk for diabetes (113).
Ezetimibe, a cholesterol absorption inhibitor, could significantly improve fatty liver in rats by increasing cholesterol efflux transporter (114) and could also prevent and improve liver steatosis in the HFD mice (115). Ezetimibe at a dose of 10 mg/d for 6 months could significantly reduce serum total cholesterol levels and improve liver fibrosis scores in NAFLD patients (116). In a study by Park et al., a similar treatment regimen for 24 months could improve metabolism and liver histology in NAFLD patients, showing promising results (117). In another study, a treatment regimen, containing 10 mg/d of ezetimibe and 5 mg/d of rosuvastatin for 24 weeks, could significantly reduce LFC in patients (108). However, a meta-analysis by Lee et al. showed that ezetimibe could not improve liver steatosis (118). Another study also claimed that in combination with lifestyle intervention, ezetimibe could not improve liver histology in NASH patients (119). Therefore, further studies are needed to demonstrate its efficacy.
An increase in intrahepatic vascular resistance has been observed in both the early-stage NAFLD patients and animal models of NAFLD (120, 121), leading to tissue hypoxia and triggering disease progression. The liver vessels are highly responsive to vasoconstrictors. Clinically, NAFLD is associated with tew-onset hypertension in patients, and elevated blood pressure is associated with the progression of fatty liver disease and fibrosis in patients. Therefore, vasoconstrictor antagonists might be used for the treatment of NAFLD (122, 123).
In the Wistar rat model of diet-induced steatosis, endothelin-1 (ET-1), angiotensin II (AT-II), thromboxane A2 (TxA2) could increase the transhepatic pressure gradients (THPG), which could be reduced by bosentan (ET-1 antagonist), valsartan (AT-II-receptor blocker) and celecoxib (COX-2 inhibitor). In the Zucker rat model of NASH, comparing the therapeutic effects of bosentan and placebo showed that bosentan could reduce steatosis and structural liver damage; therefore, the vasoconstrictor antagonists might improve intrahepatic vascular function, demonstrating their potential therapeutic effects in early NAFLD (122). In the diet-induced rat model of NASH, the combination of atorvastatin and ambrisentan could significantly improve liver histology, thereby suggesting the potential application of combination therapy in NASH patients (124). In the NAFLD mouse models, Losartan could prevent hepatic steatosis and macrophage polarization in the ob/ob mice by inhibiting the hypoxia-inducible factor-1α (HIF-1α). The Losartan-treated mice showed a significant increase in the levels of TG and free fatty acid (FFA), thereby preventing NAFLD (125). Telmisartan, also a potential therapeutic drug for NAFLD, could inhibit liver fibrosis by blocking the AT-II receptors (126). Studies also showed that it was a partial agonist of PPAR-γ, thereby improving IR, lipid metabolism and disease condition of liver steatosis and fibrosis and reducing the expression of pro-inflammatory cytokines as well as the levels of fatty acids and TGs (127). In general, based on animal experiments, antihypertensive drugs like sartans have shown efficacy in the treatment of NAFLD; however, their similar effects in NAFLD patients require clinical verification.
UDCA is an endogenous synthetic bile acid in the human body and has antioxidant and anti-inflammatory effects, preventing mitochondrial dysfunction in the progression of obesity-related diseases. In some early clinical trials, UDCA did not show much efficacy in the NAFLD/NASH patients (128–130). However, its liver protective effects had been demonstrated; therefore, both animal and clinical studies on UDCA did not stop. In ob/ob mice, UDCA could regulate liver energy homeostasis and macrophage polarization in the white adipose tissues (131). A randomized controlled trial by Ratziu et al. suggested that the high-dose (28-35 mg/kg/d) UDCA treatment for 12 months could reduce hepatic aminotransferase levels in NASH patients and improve glycemic control and IR. In addition, UDCA has a good safety profile with no deterioration of liver function, and the main adverse reactions are abdominal discomfort and diarrhea (132). A study by Nadinskaia et al. supplemented UDCA at 15 mg/kg/d based on changes in diet and exercise. In the first three months, NAFLD patients showed normalization of the liver enzyme levels and improvement in lipid profile and fatty liver degeneration, and the six-month treatment was beneficial to reduce CVD risk (133).
Farnesol X receptors (FXR), a member of the nuclear receptor superfamily, regulate bile acid synthesis, glycolipid metabolism, liver inflammation, and fibrosis processes. The FXR agonists enhance insulin sensitivity, inhibit bile acid synthesis, and promote mitochondrial fatty acid oxidation. Obeticholic acid (OCA) is a representative FXR drug (134). In a phase II trial by Sunder Mudaliar et al., a continuous treatment with 25 or 50 mg/d OCA for 6 weeks could improve IR and reduce the levels of liver inflammatory and fibrosis markers in the T2DM patients with NAFLD and was well-tolerated (135). In a double-blind placebo-controlled trial by Neuschwander-Tetri et al., the 25 mg/d OCA treatment for 72 weeks could improve the histological features of NASH; however, the long-term OCA administration resulted in pruritus in about 23% of patients (136). Based on previous studies, Younossi et al. designed a phase III clinical trial to evaluate the effects of OCA on fibrosis in NASH patients (137). They conducted an interim analysis after 18 months of treatment and showed that 10 or 25 mg/d OCA treatment could significantly improve fibrosis in NASH patients; however, long-term OCA treatment could cause skin and subcutaneous tissue diseases, gastrointestinal disorders, and cholesterol (138). These adverse reactions might limit the use of OCA in NAFLD/NASH patients.
Targeting intestinal microbes has been a hot topic in NAFLD therapy in recent years. Gut microbiota might play a role in the pathogenesis of NASH by releasing lipopolysaccharide (LPS), increasing ethanol production, and activating inflammatory cytokines in the luminal epithelial cells and hepatic macrophages (139). In addition, the gut microbiota can also influence the development of NAFLD by increasing the metabolisms of choline and bile acids and the production of SCFAs (acetate, propionate, and butyrate) during bacterial fermentation (140). Moreover, gut dysbiosis, such as the abnormal release of LPS and SCFAs and ceramides fibrosis, induces liver inflammation and hepatic inflammation by increasing the release of damage-associated molecular patterns (DAMPs) and pathogen-associated molecular patterns (PAMPs) (141, 142). In the mice’s gut, the reduced butyrate levels and increased bacterial LPS translocation could contribute to NAFLD and IR. However, its effectiveness in clinical applications has not been explored yet. Generally, intestinal microecological disorders are prevalent in chronic liver diseases and play an important role in the occurrence and development of liver cirrhosis caused by various etiologies (143). Probiotics, prebiotics, synbiotics, fecal microbiota transplantation (FMT), etc. are increasingly appearing in clinical trials as common intestinal microecological regulatory methods (144).
In a placebo-controlled trial by Aller et al., the oral combination of Lactobacillus bulgaricus and Streptococcus thermophilus at 500 million CFU/d for 3 months could improve liver aminotransferase levels in patients with NAFLD (145). A randomized controlled trial showed that as compared to milk, the probiotic-fortified yogurt was more beneficial in improving IR and LFC in obese women with NAFLD and MS. A daily intake of 220 g of yogurt for 24 weeks could reduce inflammation and oxidative stress, modulate lipid metabolism, and alter the composition of gut microbiota (146). Based on diet and exercise intervention, the supplementation of Saccharomyces boulardii powder (Beda Pharma, France) for 12 weeks could significantly decrease the levels of total bilirubin (TBil), AST, ALT, GGT, serum total cholesterol, LDL-C, and fasting insulin in NAFLD patients (147). Another placebo-controlled trial suggested that the oral administration of probiotic capsules Lactocare (Zist-takhmir, Tehran, Iran, containing 7 kinds of probiotics) at a dose of 2 capsules/d for 8 consecutive weeks could improve IR in NAFLD patients and decrease the levels of inflammatory factors, including tumor necrosis factor α (TNF-α) and interleukin- 6 (IL-6) (148). Similarly, the probiotic Symbiter (Prolisok, Ukrainian, a mixture of 14 probiotics) could reduce the levels of LFC, TNF-α, and IL-6 and transaminase activity in patients with NAFLD (149). In another study, the oral supplementation of Symbiter once per day with omega-3 fatty acids (250 mg each of edible flax and wheat germ oil, the omega-3 fatty acid content of 3%-5%) for 8 weeks could reduce LFC in NAFLD patients, improve blood lipid content, metabolic level, and reduce systemic chronic inflammation (150). However, some studies have reported different results. Recently, in a randomized, double-blind, placebo-controlled trial, the oral administration of a multi-strain probiotic, containing six different Lactobacillus and Bifidobacterium species (MCP BCMC strains), at 30 billion CFU/d for 6 months showed no significant effects on hepatic steatosis and fibrosis. However, this study indicated that probiotics could stabilize the immune function of the intestinal mucosa and improve mucosal permeability (151).
A placebo-controlled trial of 14 NASH patients reported that the oral administration of fructo-oligosaccharides (Fos) (8 g/d for 12 weeks, then 16 g/d for 24 weeks) could reduce histological steatosis in NASH patients (152). Besides, based on the changes in diet and exercise, the oral administration of Bifidobacterium longum and Fos for 24 weeks could significantly reduce serum TNF-α, CRP, and AST levels in NASH patients, and improve liver steatosis and fibrosis score (153). Similarly, another placebo-controlled trial also suggested that synbiotics could improve TNF-α and CRP levels in NAFLD patients (154). A double-blind placebo-controlled phase II trial, including 104 NAFLD patients, showed that the oral administration of synbiotics (Bifidobacterium animalis and Fos) for one year could alter the composition of gut microbiota, containing high proportions of Bifidobacterium and low proportion of Oscillibacter and Alistipe species, but did not alter LFC or fibrosis. In another placebo-controlled study, the supplementation of probiotic formulations Familact (Zisttakhmir, containing seven probiotics) and Fos for 8 weeks could improve liver steatosis in NAFLD patients; however, it had no significant effects on liver enzyme levels (155).
An FMT trial by Craven et al. enrolled 21 patients with a 6-month follow-up. The results suggested that allogeneic or autologous FMT could not significantly improve IR in NAFLD patients, but could potentially improve small intestinal permeability (156). Recently, Chinese researchers conducted an FMT and oral probiotics-based randomized controlled clinical trial. The FMT group patients were orally administered with 200 mL of fresh bacterial solution for three consecutive days, and the probiotic group patients were orally administered with Bifidobacterium preparations and Lactobacillus acidophilus capsules. Both the groups had a daily healthy diet and performed over 40 minutes of exercise. The results of a one-month follow-up showed that FMT could reduce fat accumulation in the liver by improving the dysbiosis of gut microbiota, thereby reducing fatty liver disease and showing more effectiveness in non-obese NAFLD patients (157).
In general, most of these trials suggested that targeting the gut microbiota might have a certain therapeutic effect on NAFLD. However, related studies have come to different conclusions. There is no uniform standard for the time of intervention, a method used, number of samples, indicators of the study, and endpoint of the study. Therefore, further optimization of the study is needed to evaluate the real benefits of probiotics in the treatment of NAFLD.
PPAR agonists can help in improving blood sugar and lipid levels (fat and cholesterol). In addition to the T2DM drug pioglitazone mentioned above, numerous PPAR agonists are currently being developed. Saroglitazar, a dual PPRA-α/γ agonist, can regulate glucose and lipid metabolism and is currently approved in India as an NAFLD therapeutic drug (158). A study by Indian scholars showed that Saroglitazar could significantly improve hepatic steatosis in high-fat diet-induced NASH male Wistar rats (159). A randomized, double-blind, controlled phase II clinical trial conducted by Gawrieh et al. found that the 4-mg/d dose of Saroglitazar in NAFLD/NASH patients for 16 weeks could improve dyslipidemia and significantly reduce fat contents and triglyceride levels in the liver while improving IR (160). A randomized, double-blind, placebo, controlled phase IIb clinical trial in NASH patients revealed that the 1200-mg/d dose of Lanifibranor, a pan-PPAR agonist, for 24 weeks could significantly reduce the patient’s liver fibrosis score (SAF-A score), decrease liver lipid content, and improve liver enzyme levels, and Francque’s team will conduct a phase III trial of the drug for further validation (161). A clinical study by Gastaldelli’s and colleagues also showed that the PPAR-γ agonist pioglitazone could induce changes in visceral fat and adiponectin levels, thereby alleviating steatohepatitis in NASH patients (162). Ratziu et al. showed that the 120-mg/d dose of Elafibranor, a PPAR-α/δ agonist, for one year significantly improved the fat content in the liver as well as the liver enzyme levels without worsening fibrosis (163). A clinical trial conducted by Japanese scholars found that although Pemafibrate, a novel selective PPAR-α modulator, could not significantly reduce fat contents, it significantly reduced liver stiffness and was recommended to treat NASH in combination with other drugs (164). In conclusion, the overall safety and tolerability of these drugs are good; however, the minor adverse effects, which are currently faced by patients, also require further investigations (Table 3).
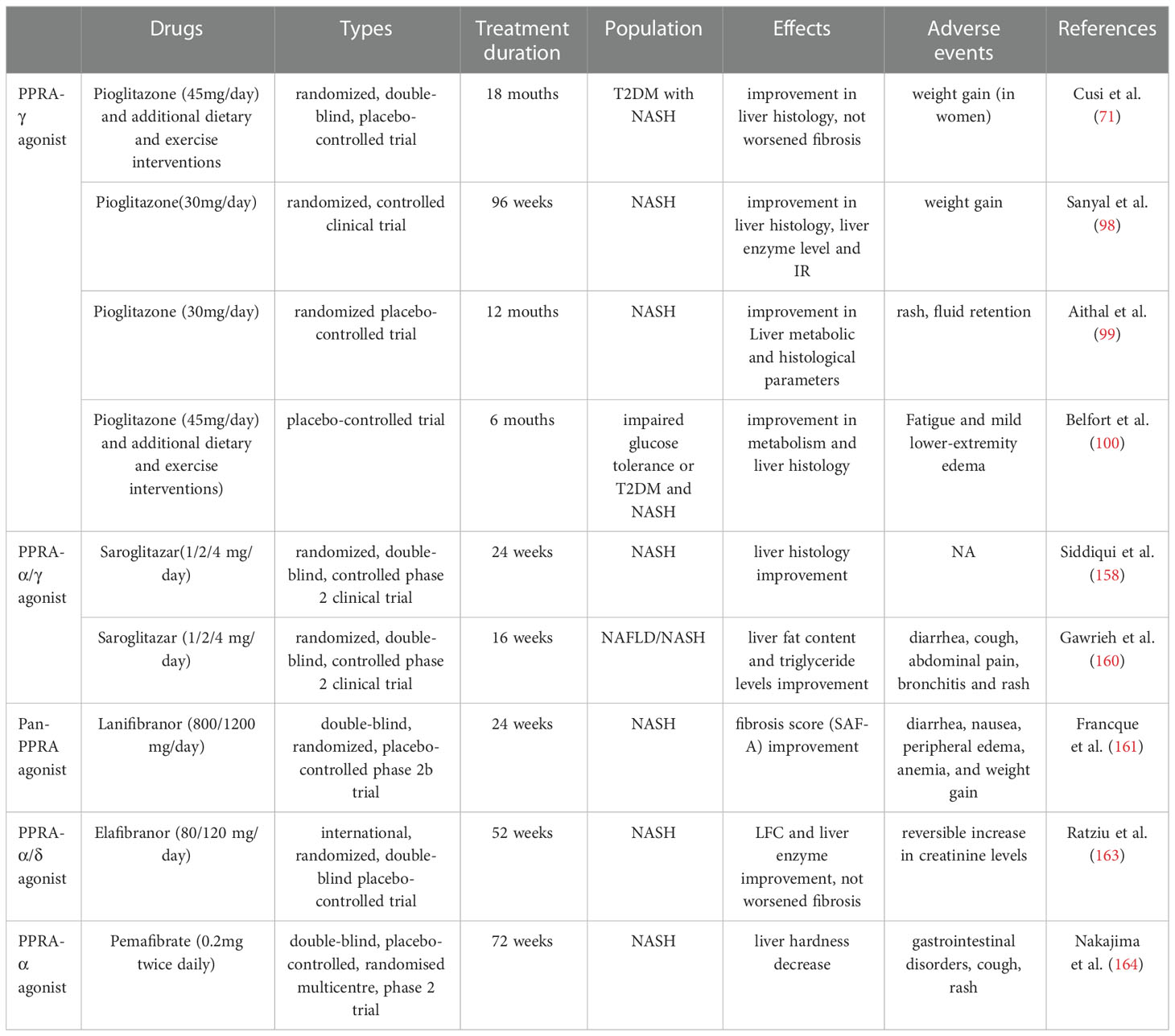
Table 3 Effect of PPRA agonist in patients of NAFLD/NASH: Data from clinical studies.
THR-β is involved in various metabolic pathways, such as glycolipid and cholesterol metabolisms in the liver, and has also been used as a therapeutic target for the research and development of novel therapeutic drugs for NAFLD/NASH. Resmetirom (MGL-3196), a novel THR-β agonist, targets the liver. The treatment of high-fat and high-sugar diet-induced obese NASH mice with MGL-3196 treatment at a 3-mg/kg/day dose could significantly reduce liver weight, hepatic steatosis, plasma ALT activity, liver and plasma cholesterol, and blood glucose (165). A 36-week randomized, double-blind, placebo-controlled, multicenter phase II clinical trial conducted by Harrison’s team showed significant reductions in the liver fat contents in NASH patients after 12 and 36 weeks of oral treatment with 80 mg/day of MGL-3196 (166). In an expansion study of this phase II study, the oral treatment with 80 or 100 mg/d of MGL-3196 was well-tolerated and safe for patients, and the drug is currently in phase III clinical study (167). TG68 is another novel THR-β agonist used to treat NAFLD. In animal studies, TG68 has shown significant effects on the liver fat contents and hepatic steatosis in high-fat diet-induced NASH C57BL/6 mice, and its efficacy is comparable to that of MGL-3196 (168); however, further clinical studies are needed to verify these results.
FGF19 and FGF21 are novel endocrine messengers, which regulate multiple aspects of energy homeostasis, such as lipid and carbohydrate metabolisms. Their analogs were initially developed to improve hyperglycemia in T2DM patients; however, their robust, consistent, and durable effects on lipid metabolism in human trials gradually transformed their clinical emphasis toward their use for NASH treatments. Therefore, they are now considered credible and promising novel NAFLD/NASH therapeutic drugs (169). In a randomized, double-blind, placebo-controlled Phase II clinical study, the treatment of NASH patients with 3 or 6 mg/day of Aldafermin (NGM282), an engineered analog of the gut hormone FGF19, reduced liver fat content with a good safety profile (170). A multicenter, randomized, double-blind, placebo-controlled study conducted by Harrison’s team revealed that the treatment of NASH patients with 1 or 3 mg/d of NGM282 improved the histological features and fibrosis score of NASH over 12 weeks while also improving the levels of liver enzymes, such as AST and ALT (171). Subsequently, they conducted a 24-week phase II clinical study, which also showed that the NGM282 treatment reduced liver fat and tended to improve fibrosis (172). Recently, their team conducted a randomized, double-blind, placebo-controlled, phase IIb clinical study, in which, they set up different doses of the drug groups, including 0.3 mg/d and 1 mg/d. The results showed that the treatment was generally well-tolerated; however, there was no significant difference between the different doses in improving fibrosis (173). Studies also showed that NGM282 could reduce liver fat, liver damage, and inflammation in NASH patients, but elevated cholesterol levels. In a multicenter, open-label phase II clinical study, in combination with statins, NGM282 was more effective in controlling cholesterol levels (174). Overall, NGM282 is well-tolerated and safe, and the common adverse reactions include nausea, vomiting, and mild or moderate diarrhea.
FGF21, a member of the FGF19 signaling subfamily, is considered a potential target for the treatment of NAFLD. Targeting the FGF21/FGFR/β-Klotho signaling pathway might block or reverse hepatic fat infiltration, inflammation, and fibrosis (175). Pegbelfermin (BMS-986036) is a PEGylated FGF21analogue. The phase II clinical studies in obese and T2DM patients suggested that BMS-986036 could improve metabolic parameters and fibrotic markers (176). A multicenter, randomized, double-blind, placebo-controlled phase IIa study showed that the subcutaneous injection of NASH patients with 10 mg/day or 20 mg/week of BMS-986036 for 16 weeks reduced the liver fat scores and was well-tolerated by the patients (177). There are currently fewer clinical studies on these drugs, and more clinical trials are needed to confirm their long-term benefits on the outcomes, such as liver histology, development of cirrhosis, or survival (178).
TVB2640 is a novel lipase synthesis inhibitor, which can reduce liver fat synthesis in men (179). A phase IIa clinical trial suggested that the treatment of patients with TVB2640 at the doses of 25/50 mg/day for 12 weeks significantly reduced liver fat contents and improved the biomarkers of liver biochemistry, inflammation, and fibrosis in a dose-dependent manner (180). Namodenoson, an A3 adenosine receptor (A3AR) agonist, also showed promising results in a recent phase II clinical trial by improving the liver function/pathology in NASH (181). Currently, other novel drugs are being investigated in clinical studies, such as HM15211, a novel long-acting GLP-1/GIP/Glucagon triple agonist; AZD2693, a Patatin-like phospholipase domain containing 3 (PNPLA3) antisense oligonucleotide drug; and BMS-986263, a lipid nanoparticle drug containing siRNA that inhibits heat shock protein 47 (HSP47). Some new drugs for NAFLD/NASH patients, which are in clinical trials, are summarized in Table 4.
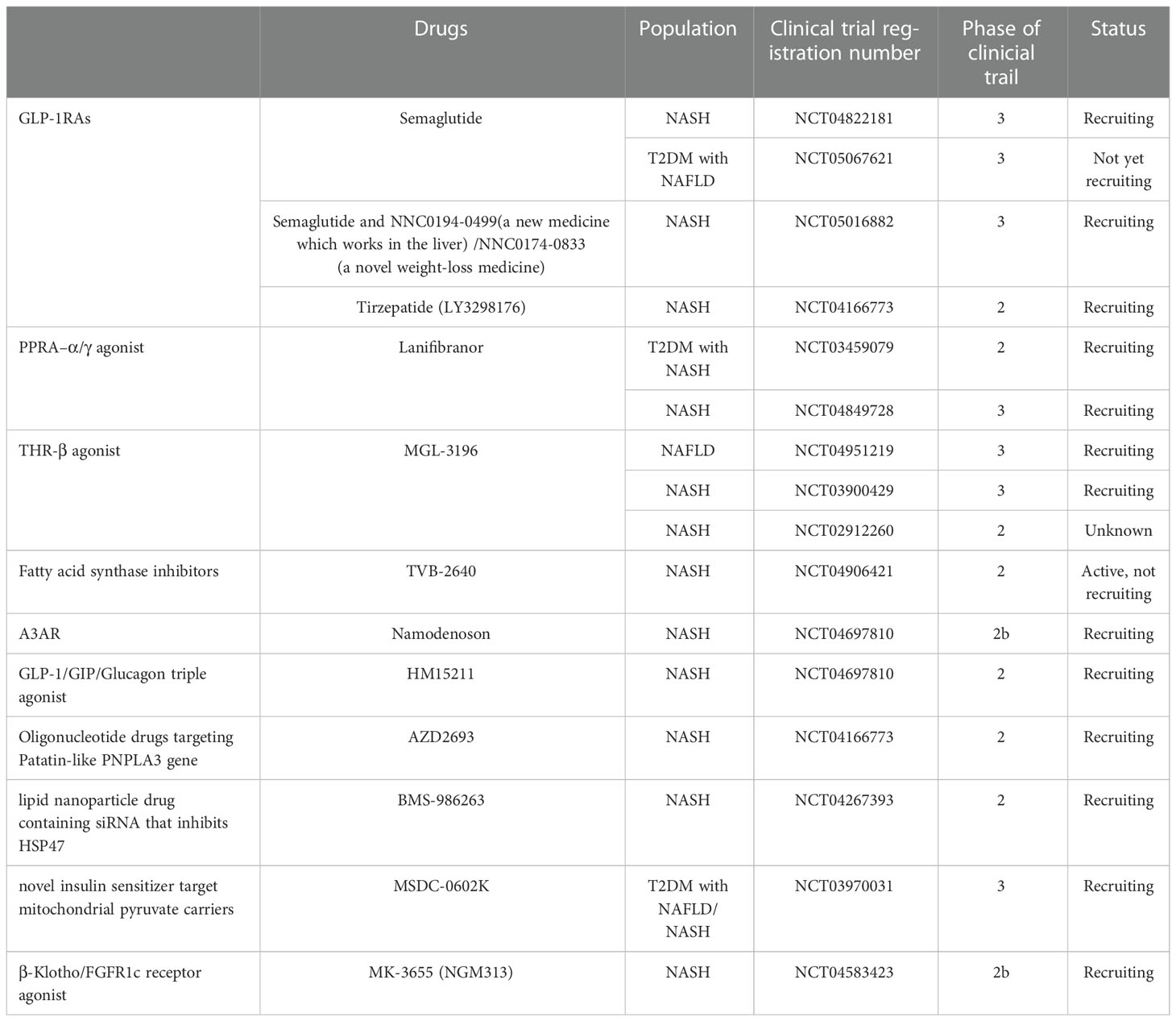
Table 4 Partial drug clinical trials in progress or in preparation (data from ClinicalTrials.gov).
NAFLD, a multi-system metabolic disease, is usually accompanied by T2DM and MS, which jointly promote disease progression. The incidence of NAFLD is increasing annually, and it has a worldwide prevalence, while its pathogenesis has not been fully understood yet. Therefore, NAFLD has become a new challenge and a major public health concern in the field of liver diseases and metabolisms worldwide. Lifestyle intervention is an important basic treatment. Regulating glucolipid metabolism has still been focused on in the NAFLD treatment. The studies on targeting gut microbiota for the treatment of NAFLD are also deepening. Moreover, various novel metabolic drugs represented by PPAR agonists, FXR agonists, and THR-β agonists are also being developed and are in the clinical trial stages. However, developing new drugs for NAFLD has still a long way to go. The results of clinical trials of most therapeutic drugs are not ideal, and the liver histological endpoint has not been reached yet, which might be due to the complex heterogeneity of NAFLD, limitations of therapeutic targets, drug safety, and other factors. An in-depth understanding of the pathogenesis of NAFLD might help in. finding drugs, which can not only improve metabolic disorders but also reduce liver inflammation and fibrosis in the near future. Of course, considering the medical, economic, and social burden caused by the global epidemic of NAFLD, the global vulnerable population, medical personnel, and medical institutions should improve their awareness of this disease in order to make early interventions and achieve better prevention and control effects.
LR and JZ jointly conceived and drafted the review. WR and XQ suggested some important changes to the content of the review. YC and HC refined the language, and JG directed and proofread the review throughout. All authors contributed to the article and approved the submitted version.
Chongqing Medical Scientific Research Project (Joint Projectof Chongqing Health Commission and Science and Technology Bureau) (2022GDRC019) and Chongqing Natural Science Foundation (CSTB2022NSCQ-MSX1257, cstc2019jcyj-msxmX0752, cstc2018jcyj-AX0006).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (Nafld). Metabolism (2016) 65(8):1038–48. doi: 10.1016/j.metabol.2015.12.012
2. European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO). Easl-Easd-Easo clinical practice guidelines for the management of non-alcoholic fatty liver disease. J Hepatol (2016) 64(6):1388–402. doi: 10.1016/j.jhep.2015.11.004
3. Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American association for the study of liver diseases. Hepatology (2018) 67(1):328–57. doi: 10.1002/hep.29367
4. Glen J, Floros L, Day C, Pryke R. Non-alcoholic fatty liver disease (Nafld): Summary of nice guidance. BMJ (Clinical Res ed (2016) 354:i4428. doi: 10.1136/bmj.i4428
5. Risi R, Tozzi R, Watanabe M. Beyond weight loss in nonalcoholic fatty liver disease: The role of carbohydrate restriction. Curr Opin Clin Nutr Metab Care (2021) 24(4):349–53. doi: 10.1097/mco.0000000000000762
6. Hassani Zadeh S, Mansoori A, Hosseinzadeh M. Relationship between dietary patterns and non-alcoholic fatty liver disease: A systematic review and meta-analysis. J Gastroenterol Hepatol (2021) 36(6):1470–8. doi: 10.1111/jgh.15363
7. Plaz Torres MC, Aghemo A, Lleo A, Bodini G, Furnari M, Marabotto E, et al. Mediterranean Diet and nafld: What we know and questions that still need to be answered. Nutrients (2019) 11(12):2971. doi: 10.3390/nu11122971
8. Shi JP, Xu JL. Non-drug therapy of non-alcoholic fatty liver disease. Chin J Dig (2020) 40(9):587–90. doi: 10.3760/cma.j.cn311367-20200424-00262
9. Esposito K, Kastorini CM, Panagiotakos DB, Giugliano D. Mediterranean Diet and metabolic syndrome: An updated systematic review. Rev Endocrine Metab Disord (2013) 14(3):255–63. doi: 10.1007/s11154-013-9253-9
10. Esposito K, Giugliano D. Mediterranean Diet for primary prevention of cardiovascular disease. New Engl J Med (2013) 369(7):674–5. doi: 10.1056/NEJMc1306659
11. Pérez-Guisado J, Muñoz-Serrano A. The effect of the Spanish ketogenic Mediterranean diet on nonalcoholic fatty liver disease: A pilot study. J Med Food (2011) 14(7-8):677–80. doi: 10.1089/jmf.2011.0075
12. Katsagoni CN, Papatheodoridis GV, Ioannidou P, Deutsch M, Alexopoulou A, Papadopoulos N, et al. Improvements in clinical characteristics of patients with non-alcoholic fatty liver disease, after an intervention based on the Mediterranean lifestyle: A randomised controlled clinical trial. Br J Nutr (2018) 120(2):164–75. doi: 10.1017/s000711451800137x
13. Properzi C, O'Sullivan TA, Sherriff JL, Ching HL, Jeffrey GP, Buckley RF, et al. Ad libitum Mediterranean and low-fat diets both significantly reduce hepatic steatosis: A randomized controlled trial. Hepatology (2018) 68(5):1741–54. doi: 10.1002/hep.30076
14. Biolato M, Manca F, Marrone G, Cefalo C, Racco S, Miggiano GA, et al. Intestinal permeability after Mediterranean diet and low-fat diet in non-alcoholic fatty liver disease. World J Gastroenterol (2019) 25(4):509–20. doi: 10.3748/wjg.v25.i4.509
15. Romero-Gómez M, Zelber-Sagi S, Trenell M. Treatment of nafld with diet, physical activity and exercise. J Hepatol (2017) 67(4):829–46. doi: 10.1016/j.jhep.2017.05.016
16. Kawaguchi T, Charlton M, Kawaguchi A, Yamamura S, Nakano D, Tsutsumi T, et al. Effects of Mediterranean diet in patients with nonalcoholic fatty liver disease: A systematic review, meta-analysis, and meta-regression analysis of randomized controlled trials. Semin liver Dis (2021) 41(3):225–34. doi: 10.1055/s-0041-1723751
17. Akbulut UE, Isik IA, Atalay A, Eraslan A, Durmus E, Turkmen S, et al. The effect of a Mediterranean diet vs. a low-fat diet on non-alcoholic fatty liver disease in children: A randomized trial. Int J Food Sci Nutr (2022) 73(3):357–66. doi: 10.1080/09637486.2021.1979478
18. Yurtdaş G, Akbulut G, Baran M, Yılmaz C. The effects of Mediterranean diet on hepatic steatosis, oxidative stress, and inflammation in adolescents with non-alcoholic fatty liver disease: A randomized controlled trial. Pediatr Obes (2022) 17(4):e12872. doi: 10.1111/ijpo.12872
19. Watanabe M, Tozzi R, Risi R, Tuccinardi D, Mariani S, Basciani S, et al. Beneficial effects of the ketogenic diet on nonalcoholic fatty liver disease: A comprehensive review of the literature. Obes Rev an Off J Int Assoc Study Obes (2020) 21(8):e13024. doi: 10.1111/obr.13024
20. Luukkonen PK, Dufour S, Lyu K, Zhang XM, Hakkarainen A, Lehtimäki TE, et al. Effect of a ketogenic diet on hepatic steatosis and hepatic mitochondrial metabolism in nonalcoholic fatty liver disease. Proc Natl Acad Sci United States America (2020) 117(13):7347–54. doi: 10.1073/pnas.1922344117
21. Muyyarikkandy MS, McLeod M, Maguire M, Mahar R, Kattapuram N, Zhang C, et al. Branched chain amino acids and carbohydrate restriction exacerbate ketogenesis and hepatic mitochondrial oxidative dysfunction during nafld. FASEB J Off Publ Fed Am Societies Exp Biol (2020) 34(11):14832–49. doi: 10.1096/fj.202001495R
22. Anekwe CV, Chandrasekaran P, Stanford FC. Ketogenic diet-induced elevated cholesterol, elevated liver enzymes and potential non-alcoholic fatty liver disease. Cureus (2020) 12(1):e6605. doi: 10.7759/cureus.6605
23. Crabtree CD, Kackley ML, Buga A, Fell B, LaFountain RA, Hyde PN, et al. Comparison of ketogenic diets with and without ketone salts versus a low-fat diet: Liver fat responses in overweight adults. Nutrients (2021) 13(3):966. doi: 10.3390/nu13030966
24. Markova M, Pivovarova O, Hornemann S, Sucher S, Frahnow T, Wegner K, et al. Isocaloric diets high in animal or plant protein reduce liver fat and inflammation in individuals with type 2 diabetes. Gastroenterology (2017) 152(3):571–85.e8. doi: 10.1053/j.gastro.2016.10.007
25. Cohen CC, Li KW, Alazraki AL, Beysen C, Carrier CA, Cleeton RL, et al. Dietary sugar restriction reduces hepatic De novo lipogenesis in adolescent boys with fatty liver disease. J Clin Invest (2021) 131(24):e150996. doi: 10.1172/jci150996
26. Schwimmer JB, Ugalde-Nicalo P, Welsh JA, Angeles JE, Cordero M, Harlow KE, et al. Effect of a low free sugar diet vs usual diet on nonalcoholic fatty liver disease in adolescent boys: A randomized clinical trial. Jama (2019) 321(3):256–65. doi: 10.1001/jama.2018.20579
27. So B, Kim HJ, Kim J, Song W. Exercise-induced myokines in health and metabolic diseases. Integr Med Res (2014) 3(4):172–9. doi: 10.1016/j.imr.2014.09.007
28. Brouwers B, Schrauwen-Hinderling VB, Jelenik T, Gemmink A, Sparks LM, Havekes B, et al. Exercise training reduces intrahepatic lipid content in people with and people without nonalcoholic fatty liver. Am J Physiol Endocrinol Metab (2018) 314(2):E165–e73. doi: 10.1152/ajpendo.00266.2017
29. Wong VW, Wong GL, Chan RS, Shu SS, Cheung BH, Li LS, et al. Beneficial effects of lifestyle intervention in non-obese patients with non-alcoholic fatty liver disease. J Hepatol (2018) 69(6):1349–56. doi: 10.1016/j.jhep.2018.08.011
30. Jia GY, Han T, Gao L, Wang L, Wang SC, Yang L, et al. [Effect of aerobic exercise and resistance exercise in improving non-alcoholic fatty liver disease: A randomized controlled trial]. Zhonghua gan zang bing za zhi = Zhonghua ganzangbing zazhi = Chin J Hepatol (2018) 26(1):34–41. doi: 10.3760/cma.j.issn.1007-3418.2018.01.009
31. Takahashi A, Abe K, Fujita M, Hayashi M, Okai K, Ohira H. Simple resistance exercise decreases cytokeratin 18 and fibroblast growth factor 21 levels in patients with nonalcoholic fatty liver disease: A retrospective clinical study. Medicine (2020) 99(22):e20399. doi: 10.1097/md.0000000000020399
32. O'Gorman P, Naimimohasses S, Monaghan A, Kennedy M, Melo AM, NF D, et al. Improvement in histological endpoints of mafld following a 12-week aerobic exercise intervention. Aliment Pharmacol Ther (2020) 52(8):1387–98. doi: 10.1111/apt.15989
33. Babu AF, Csader S, Männistö V, Tauriainen MM, Pentikäinen H, Savonen K, et al. Effects of exercise on nafld using non-targeted metabolomics in adipose tissue, plasma, urine, and stool. Sci Rep (2022) 12(1):6485. doi: 10.1038/s41598-022-10481-9
34. Huber Y, Pfirrmann D, Gebhardt I, Labenz C, Gehrke N, Straub BK, et al. Improvement of non-invasive markers of nafld from an individualised, web-based exercise program. Aliment Pharmacol Ther (2019) 50(8):930–9. doi: 10.1111/apt.15427
35. Keating SE, Hackett DA, Parker HM, O'Connor HT, Gerofi JA, Sainsbury A, et al. Effect of aerobic exercise training dose on liver fat and visceral adiposity. J Hepatol (2015) 63(1):174–82. doi: 10.1016/j.jhep.2015.02.022
36. Abdelbasset WK, Tantawy SA, Kamel DM, Alqahtani BA, Elnegamy TE, Soliman GS, et al. Effects of high-intensity interval and moderate-intensity continuous aerobic exercise on diabetic obese patients with nonalcoholic fatty liver disease: A comparative randomized controlled trial. Medicine (2020) 99(10):e19471. doi: 10.1097/md.0000000000019471
37. Keating SE, Hackett DA, George J, Johnson NA. Exercise and non-alcoholic fatty liver disease: A systematic review and meta-analysis. J Hepatol (2012) 57(1):157–66. doi: 10.1016/j.jhep.2012.02.023
38. Gao Y, Zhang W, Zeng LQ, Bai H, Li J, Zhou J, et al. Exercise and dietary intervention ameliorate high-fat diet-induced nafld and liver aging by inducing lipophagy. Redox Biol (2020) 36:101635. doi: 10.1016/j.redox.2020.101635
39. Yaskolka Meir A, Rinott E, Tsaban G, Zelicha H, Kaplan A, Rosen P, et al. Effect of green-Mediterranean diet on intrahepatic fat: The direct plus randomised controlled trial. Gut (2021) 70(11):2085–95. doi: 10.1136/gutjnl-2020-323106
40. Cheng R, Wang L, Le S, Yang Y, Zhao C, Zhang X, et al. A randomized controlled trial for response of microbiome network to exercise and diet intervention in patients with nonalcoholic fatty liver disease. Nat Commun (2022) 13(1):2555. doi: 10.1038/s41467-022-29968-0
41. Franco I, Bianco A, Mirizzi A, Campanella A, Bonfiglio C, Sorino P, et al. Physical activity and low glycemic index Mediterranean diet: Main and modification effects on nafld score. Results from a randomized clinical trial. Nutrients (2020) 13(1):66. doi: 10.3390/nu13010066
42. Pratt JSA, Browne A, Browne NT, Bruzoni M, Cohen M, Desai A, et al. Asmbs pediatric metabolic and bariatric surgery guidelines, 2018. Surg Obes related Dis Off J Am Soc Bariatric Surg (2018) 14(7):882–901. doi: 10.1016/j.soard.2018.03.019
43. Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology (2018) 67(1):328–57. doi: 10.1002/hep.29367
44. Chauhan M, Singh K, Thuluvath PJ. Bariatric surgery in nafld. Dig Dis Sci (2022) 67(2):408–22. doi: 10.1007/s10620-021-07317-3
45. Nickel F, Tapking C, Benner L, Sollors J, Billeter AT, Kenngott HG, et al. Bariatric surgery as an efficient treatment for non-alcoholic fatty liver disease in a prospective study with 1-year follow-up : Bariscan study. Obes Surg (2018) 28(5):1342–50. doi: 10.1007/s11695-017-3012-z
46. Nguyen NT, Varela JE. Bariatric surgery for obesity and metabolic disorders: State of the art. Nat Rev Gastroenterol Hepatol (2017) 14(3):160–9. doi: 10.1038/nrgastro.2016.170
47. Sagredo S, Brahm J, Uribe M, Codoceo V, Smok G. [Acute liver failure after bariatric surgery. a case report and literature review]. Gastroenterol y hepatol (2013) 36(2):76–80. doi: 10.1016/j.gastrohep.2012.06.004
48. Younus H, Sharma A, Miquel R, Quaglia A, Kanchustambam SR, Carswell KA, et al. Bariatric surgery in cirrhotic patients: Is it safe? Obes Surg (2020) 30(4):1241–8. doi: 10.1007/s11695-019-04214-7
49. Ali A, Amin MJ, Ahmed MU, Taj A, Aasim M, Tabrez E. Frequency of non-alcoholic fatty liver disease (Nafld) and its associated risk factors among type-2 diabetics. Pak J Med Sci (2022) 38(1):28–33. doi: 10.12669/pjms.38.1.4968
50. Petit JM, Vergès B. Glp-1 receptor agonists in nafld. Diabetes Metab (2017) 43 Suppl 1:2s28–33. doi: 10.1016/s1262-3636(17)30070-8
51. Cusi K. Incretin-based therapies for the management of nonalcoholic fatty liver disease in patients with type 2 diabetes. Hepatology (2019) 69(6):2318–22. doi: 10.1002/hep.30670
52. Jinnouchi H, Sugiyama S, Yoshida A, Hieshima K, Kurinami N, Suzuki T, et al. Liraglutide, a glucagon-like peptide-1 analog, increased insulin sensitivity assessed by hyperinsulinemic-euglycemic clamp examination in patients with uncontrolled type 2 diabetes mellitus. J Diabetes Res (2015) 2015:706416. doi: 10.1155/2015/706416
53. Petit JM, Cercueil JP, Loffroy R, Denimal D, Bouillet B, Fourmont C, et al. Effect of liraglutide therapy on liver fat content in patients with inadequately controlled type 2 diabetes: The lira-nafld study. J Clin Endocrinol Metab (2017) 102(2):407–15. doi: 10.1210/jc.2016-2775
54. Armstrong MJ, Gaunt P, Aithal GP, Barton D, Hull D, Parker R, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (Lean): A multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet (London England) (2016) 387(10019):679–90. doi: 10.1016/s0140-6736(15)00803-x
55. Feng W, Gao C, Bi Y, Wu M, Li P, Shen S, et al. Randomized trial comparing the effects of gliclazide, liraglutide, and metformin on diabetes with non-alcoholic fatty liver disease. J Diabetes (2017) 9(8):800–9. doi: 10.1111/1753-0407.12555
56. Newsome P, Francque S, Harrison S, Ratziu V, Van Gaal L, Calanna S, et al. Effect of semaglutide on liver enzymes and markers of inflammation in subjects with type 2 diabetes and/or obesity. Aliment Pharmacol Ther (2019) 50(2):193–203. doi: 10.1111/apt.15316
57. Newsome PN, Buchholtz K, Cusi K, Linder M, Okanoue T, Ratziu V, et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. New Engl J Med (2021) 384(12):1113–24. doi: 10.1056/NEJMoa2028395
58. Dickson I. Semaglutide is safe and efficacious for Nash resolution. Nat Rev Gastroenterol Hepatol (2021) 18(1):6. doi: 10.1038/s41575-020-00396-z
59. Flint A, Andersen G, Hockings P, Johansson L, Morsing A, Sundby Palle M, et al. Randomised clinical trial: Semaglutide versus placebo reduced liver steatosis but not liver stiffness in subjects with non-alcoholic fatty liver disease assessed by magnetic resonance imaging. Aliment Pharmacol Ther (2021) 54(9):1150–61. doi: 10.1111/apt.16608
60. Dichtel LE. The glucagon-like peptide-1 receptor agonist, semaglutide, for the treatment of nonalcoholic steatohepatitis. Hepatology (2021) 74(4):2290–2. doi: 10.1002/hep.31886
61. Cusi K, Sattar N, García-Pérez LE, Pavo I, Yu M, Robertson KE, et al. Dulaglutide decreases plasma aminotransferases in people with type 2 diabetes in a pattern consistent with liver fat reduction: A Post hoc analysis of the award programme. Diabetic Med J Br Diabetic Assoc (2018) 35(10):1434–9. doi: 10.1111/dme.13697
62. Kuchay MS, Krishan S, Mishra SK, Choudhary NS, Singh MK, Wasir JS, et al. Effect of dulaglutide on liver fat in patients with type 2 diabetes and nafld: Randomised controlled trial (D-lift trial). Diabetologia (2020) 63(11):2434–45. doi: 10.1007/s00125-020-05265-7
63. Seko Y, Sumida Y, Tanaka S, Mori K, Taketani H, Ishiba H, et al. Effect of 12-week dulaglutide therapy in Japanese patients with biopsy-proven non-alcoholic fatty liver disease and type 2 diabetes mellitus. Hepatol Res Off J Japan Soc Hepatol (2017) 47(11):1206–11. doi: 10.1111/hepr.12837
64. Fan H, Pan Q, Xu Y, Yang X. Exenatide improves type 2 diabetes concomitant with non-alcoholic fatty liver disease. Arquivos brasileiros endocrinol e metabol (2013) 57(9):702–8. doi: 10.1590/s0004-27302013000900005
65. Shao N, Kuang HY, Hao M, Gao XY, Lin WJ, Zou W. Benefits of exenatide on obesity and non-alcoholic fatty liver disease with elevated liver enzymes in patients with type 2 diabetes. Diabetes/metab Res Rev (2014) 30(6):521–9. doi: 10.1002/dmrr.2561
66. Liu L, Yan H, Xia M, Zhao L, Lv M, Zhao N, et al. Efficacy of exenatide and insulin glargine on nonalcoholic fatty liver disease in patients with type 2 diabetes. Diabetes/metab Res Rev (2020) 36(5):e3292. doi: 10.1002/dmrr.3292
67. Unsal İO, Calapkulu M, Sencar ME, Cakal B, Ozbek M. Evaluation of nafld fibrosis, fib-4 and apri score in diabetic patients receiving exenatide treatment for non-alcoholic fatty liver disease. Sci Rep (2022) 12(1):283. doi: 10.1038/s41598-021-04361-x
68. Gastaldelli A, Repetto E, Guja C, Hardy E, Han J, Jabbour SA, et al. Exenatide and dapagliflozin combination improves markers of liver steatosis and fibrosis in patients with type 2 diabetes. Diabetes Obes Metab (2020) 22(3):393–403. doi: 10.1111/dom.13907
69. Colosimo S, Ravaioli F, Petroni ML, Brodosi L, Marchignoli F, Barbanti FA, et al. Effects of antidiabetic agents on steatosis and fibrosis biomarkers in type 2 diabetes: A real-world data analysis. Liver Int (2021) 41(4):731–42. doi: 10.1111/liv.14799
70. Akuta N, Kawamura Y, Fujiyama S, Saito S, Muraishi N, Sezaki H, et al. Favorable impact of long-term Sglt2 inhibitor for nafld complicated by diabetes mellitus: A 5-year follow-up study. Hepatol Commun (2022) 6(9):2286–97. doi: 10.1002/hep4.2005
71. Cusi K, Orsak B, Bril F, Lomonaco R, Hecht J, Ortiz-Lopez C, et al. Long-term pioglitazone treatment for patients with nonalcoholic steatohepatitis and prediabetes or type 2 diabetes mellitus: A randomized trial. Ann Internal Med (2016) 165(5):305–15. doi: 10.7326/m15-1774
72. Wong C, Yaow CYL, Ng CH, Chin YH, Low YF, Lim AYL, et al. Sodium-glucose Co-transporter 2 inhibitors for non-alcoholic fatty liver disease in Asian patients with type 2 diabetes: A meta-analysis. Front Endocrinol (2020) 11:609135. doi: 10.3389/fendo.2020.609135
73. Dwinata M, Putera DD, Hasan I, Raharjo M. Sglt2 inhibitors for improving hepatic fibrosis and steatosis in non-alcoholic fatty liver disease complicated with type 2 diabetes mellitus: A systematic review. Clin Exp Hepatol (2020) 6(4):339–46. doi: 10.5114/ceh.2020.102173
74. Gaborit B, Ancel P, Abdullah AE, Maurice F, Abdesselam I, Calen A, et al. Effect of empagliflozin on ectopic fat stores and myocardial energetics in type 2 diabetes: The empacef study. Cardiovasc Diabetol (2021) 20(1):57. doi: 10.1186/s12933-021-01237-2
75. Kahl S, Gancheva S, Straßburger K, Herder C, Machann J, Katsuyama H, et al. Empagliflozin effectively lowers liver fat content in well-controlled type 2 diabetes: A randomized, double-blind, phase 4, placebo-controlled trial. Diabetes Care (2020) 43(2):298–305. doi: 10.2337/dc19-0641
76. Kahl S, Ofstad AP, Zinman B, Wanner C, Schüler E, Sattar N, et al. Effects of empagliflozin on markers of liver steatosis and fibrosis and their relationship to cardiorenal outcomes. Diabetes Obes Metab (2022) 24(6):1061–71. doi: 10.1111/dom.14670
77. Taheri H, Malek M, Ismail-Beigi F, Zamani F, Sohrabi M, Reza Babaei M, et al. Effect of empagliflozin on liver steatosis and fibrosis in patients with non-alcoholic fatty liver disease without diabetes: A randomized, double-blind, placebo-controlled trial. Adv Ther (2020) 37(11):4697–708. doi: 10.1007/s12325-020-01498-5
78. Ito D, Shimizu S, Inoue K, Saito D, Yanagisawa M, Inukai K, et al. Comparison of ipragliflozin and pioglitazone effects on nonalcoholic fatty liver disease in patients with type 2 diabetes: A randomized, 24-week, open-label, active-controlled trial. Diabetes Care (2017) 40(10):1364–72. doi: 10.2337/dc17-0518
79. Miyake T, Yoshida S, Furukawa S, Sakai T, Tada F, Senba H, et al. Ipragliflozin ameliorates liver damage in non-alcoholic fatty liver disease. Open Med (Warsaw Poland) (2018) 13:402–9. doi: 10.1515/med-2018-0059
80. Takahashi H, Kessoku T, Kawanaka M, Nonaka M, Hyogo H, Fujii H, et al. Ipragliflozin improves the hepatic outcomes of patients with diabetes with nafld. Hepatol Commun (2022) 6(1):120–32. doi: 10.1002/hep4.1696
81. Latva-Rasku A, Honka MJ, Kullberg J, Mononen N, Lehtimäki T, Saltevo J, et al. The Sglt2 inhibitor dapagliflozin reduces liver fat but does not affect tissue insulin sensitivity: A randomized, double-blind, placebo-controlled study with 8-week treatment in type 2 diabetes patients. Diabetes Care (2019) 42(5):931–7. doi: 10.2337/dc18-1569
82. Eriksson JW, Lundkvist P, Jansson PA, Johansson L, Kvarnström M, Moris L, et al. Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: A double-blind randomised placebo-controlled study. Diabetologia (2018) 61(9):1923–34. doi: 10.1007/s00125-018-4675-2
83. Shimizu M, Suzuki K, Kato K, Jojima T, Iijima T, Murohisa T, et al. Evaluation of the effects of dapagliflozin, a sodium-glucose Co-Transporter-2 inhibitor, on hepatic steatosis and fibrosis using transient elastography in patients with type 2 diabetes and non-alcoholic fatty liver disease. Diabetes Obes Metab (2019) 21(2):285–92. doi: 10.1111/dom.13520
84. Tobita H, Yazaki T, Kataoka M, Kotani S, Oka A, Mishiro T, et al. Comparison of dapagliflozin and teneligliptin in nonalcoholic fatty liver disease patients without type 2 diabetes mellitus: A prospective randomized study. J Clin Biochem Nutr (2021) 68(2):173–80. doi: 10.3164/jcbn.20-129
85. Akuta N, Watanabe C, Kawamura Y, Arase Y, Saitoh S, Fujiyama S, et al. Effects of a sodium-glucose cotransporter 2 inhibitor in nonalcoholic fatty liver disease complicated by diabetes mellitus: Preliminary prospective study based on serial liver biopsies. Hepatol Commun (2017) 1(1):46–52. doi: 10.1002/hep4.1019
86. Akuta N, Kawamura Y, Fujiyama S, Sezaki H, Hosaka T, Kobayashi M, et al. Sglt2 inhibitor treatment outcome in nonalcoholic fatty liver disease complicated with diabetes mellitus: The long-term effects on clinical features and liver histopathology. Internal Med (Tokyo Japan) (2020) 59(16):1931–7. doi: 10.2169/internalmedicine.4398-19
87. Scheen AJ. An update on the safety of Sglt2 inhibitors. Expert Opin Drug Saf (2019) 18(4):295–311. doi: 10.1080/14740338.2019.1602116
88. Madiraju AK, Erion DM, Rahimi Y, Zhang XM, Braddock DT, Albright RA, et al. Metformin suppresses gluconeogenesis by inhibiting mitochondrial glycerophosphate dehydrogenase. Nature (2014) 510(7506):542–6. doi: 10.1038/nature13270
89. Buse JB, Wexler DJ, Tsapas A, Rossing P, Mingrone G, Mathieu C, et al. 2019 Update to: Management of hyperglycemia in type 2 diabetes, 2018. a consensus report by the American diabetes association (Ada) and the European association for the study of diabetes (Easd). Diabetes Care (2020) 43(2):487–93. doi: 10.2337/dci19-0066
90. Brandt A, Hernández-Arriaga A, Kehm R, Sánchez V, Jin CJ, Nier A, et al. Metformin attenuates the onset of non-alcoholic fatty liver disease and affects intestinal microbiota and barrier in small intestine. Sci Rep (2019) 9(1):6668. doi: 10.1038/s41598-019-43228-0
91. Li Y, Liu L, Wang B, Wang J, Chen D. Metformin in non-alcoholic fatty liver disease: A systematic review and meta-analysis. Biomed Rep (2013) 1(1):57–64. doi: 10.3892/br.2012.18
92. Komorizono Y, Hosoyamada K, Imamura N, Kajiya S, Hashiguchi Y, Ueyama N, et al. Metformin dose increase versus added linagliptin in non-alcoholic fatty liver disease and type 2 diabetes: An analysis of the J-link study. Diabetes Obes Metab (2021) 23(3):832–7. doi: 10.1111/dom.14263
93. Mitrovic B, Gluvic Z, Macut D, Obradovic M, Sudar-Milovanovic E, Soskic S, et al. Effects of metformin-single therapy on the level of inflammatory markers in serum of non-obese T2dm patients with nafld. Endocr Metab Immune Disord Drug Targets (2022) 22(1):117–24. doi: 10.2174/1871530321666210225110140
94. Harreiter J, Just I, Leutner M, Bastian M, Brath H, Schelkshorn C, et al. Combined exenatide and dapagliflozin has no additive effects on reduction of hepatocellular lipids despite better glycaemic control in patients with type 2 diabetes mellitus treated with metformin: Exenda, a 24-week, prospective, randomized, placebo-controlled pilot trial. Diabetes Obes Metab (2021) 23(5):1129–39. doi: 10.1111/dom.14319
95. Pinyopornpanish K, Leerapun A, Pinyopornpanish K, Chattipakorn N. Effects of metformin on hepatic steatosis in adults with nonalcoholic fatty liver disease and diabetes: Insights from the cellular to patient levels. Gut liver (2021) 15(6):827–40. doi: 10.5009/gnl20367
96. Cusi K. A diabetologist's perspective of non-alcoholic steatohepatitis (Nash): Knowledge gaps and future directions. Liver Int (2020) 40 Suppl 1:82–8. doi: 10.1111/liv.14350
97. Della Pepa G, Russo M, Vitale M, Carli F, Vetrani C, Masulli M, et al. Pioglitazone even at low dosage improves nafld in type 2 diabetes: Clinical and pathophysiological insights from a subgroup of the Tosca.It randomised trial. Diabetes Res Clin Pract (2021) 178:108984. doi: 10.1016/j.diabres.2021.108984
98. Sanyal AJ, Chalasani N, Kowdley KV, McCullough A, Diehl AM, Bass NM, et al. Pioglitazone, vitamin e, or placebo for nonalcoholic steatohepatitis. New Engl J Med (2010) 362(18):1675–85. doi: 10.1056/NEJMoa0907929
99. Aithal GP, Thomas JA, Kaye PV, Lawson A, Ryder SD, Spendlove I, et al. Randomized, placebo-controlled trial of pioglitazone in nondiabetic subjects with nonalcoholic steatohepatitis. Gastroenterology (2008) 135(4):1176–84. doi: 10.1053/j.gastro.2008.06.047
100. Belfort R, Harrison SA, Brown K, Darland C, Finch J, Hardies J, et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. New Engl J Med (2006) 355(22):2297–307. doi: 10.1056/NEJMoa060326
101. Sirtori CR. The pharmacology of statins. Pharmacol Res (2014) 88:3–11. doi: 10.1016/j.phrs.2014.03.002
102. Zhang QQ, Lu LG. Nonalcoholic fatty liver disease: Dyslipidemia, risk for cardiovascular complications, and treatment strategy. J Clin Trans Hepatol (2015) 3(1):78–84. doi: 10.14218/jcth.2014.00037
103. Katsiki N, Mikhailidis DP, Mantzoros CS. Non-alcoholic fatty liver disease and dyslipidemia: An update. Metabolism (2016) 65(8):1109–23. doi: 10.1016/j.metabol.2016.05.003
104. Kim RG, Loomba R, Prokop LJ, Singh S. Statin use and risk of cirrhosis and related complications in patients with chronic liver diseases: A systematic review and meta-analysis. Clin Gastroenterol Hepatol (2017) 15(10):1521–30.e8. doi: 10.1016/j.cgh.2017.04.039
105. Athyros VG, Boutari C, Stavropoulos K, Anagnostis P, Imprialos KP, Doumas M, et al. Statins: An under-appreciated asset for the prevention and the treatment of nafld or Nash and the related cardiovascular risk. Curr Vasc Pharmacol (2018) 16(3):246–53. doi: 10.2174/1570161115666170621082910
106. Lee JI, Lee HW, Lee KS, Lee HS, Park JY. Effects of statin use on the development and progression of nonalcoholic fatty liver disease: A nationwide nested case-control study. Am J Gastroenterol (2021) 116(1):116–24. doi: 10.14309/ajg.0000000000000845
107. Foster T, Budoff MJ, Saab S, Ahmadi N, Gordon C, Guerci AD. Atorvastatin and antioxidants for the treatment of nonalcoholic fatty liver disease: The St Francis heart study randomized clinical trial. Am J Gastroenterol (2011) 106(1):71–7. doi: 10.1038/ajg.2010.299
108. Cho Y, Rhee H, Kim YE, Lee M, Lee BW, Kang ES, et al. Ezetimibe combination therapy with statin for non-alcoholic fatty liver disease: An open-label randomized controlled trial (Essential study). BMC Med (2022) 20(1):93. doi: 10.1186/s12916-022-02288-2
109. Henson JB, Patel YA, Muir AJ. Trends in statin utilisation in us adults with non-alcoholic fatty liver disease. Aliment Pharmacol Ther (2021) 54(11-12):1481–9. doi: 10.1111/apt.16646
110. Hajifathalian K, Tafesh Z, Rosenblatt R, Kumar S, Homan EA, Sharaiha RZ, et al. Effect of statin use on cancer-related mortality in nonalcoholic fatty liver disease: A prospective united states cohort study. J Clin Gastroenterol (2022) 56(2):173–80. doi: 10.1097/mcg.0000000000001503
111. Doumas M, Imprialos K, Dimakopoulou A, Stavropoulos K, Binas A, Athyros VG. The role of statins in the management of nonalcoholic fatty liver disease. Curr Pharm design (2018) 24(38):4587–92. doi: 10.2174/1381612825666190117114305
112. Bril F, Portillo Sanchez P, Lomonaco R, Orsak B, Hecht J, Tio F, et al. Liver safety of statins in prediabetes or T2dm and nonalcoholic steatohepatitis: Post hoc analysis of a randomized trial. J Clin Endocrinol Metab (2017) 102(8):2950–61. doi: 10.1210/jc.2017-00867
113. Casula M, Mozzanica F, Scotti L, Tragni E, Pirillo A, Corrao G, et al. Statin use and risk of new-onset diabetes: A meta-analysis of observational studies. Nutrition Metab Cardiovasc Dis NMCD (2017) 27(5):396–406. doi: 10.1016/j.numecd.2017.03.001
114. Tanaka Y, Ikeda T, Ogawa H, Kamisako T. Ezetimibe markedly reduces hepatic triglycerides and cholesterol in rats fed on fish oil by increasing the expression of cholesterol efflux transporters. J Pharmacol Exp Ther (2020) 374(1):175–83. doi: 10.1124/jpet.120.265660
115. Toyoda Y, Takada T, Umezawa M, Tomura F, Yamanashi Y, Takeda K, et al. Identification of hepatic Npc1l1 as an nafld risk factor evidenced by ezetimibe-mediated steatosis prevention and recovery. FASEB bioAdvances (2019) 1(5):283–95. doi: 10.1096/fba.2018-00044
116. Takeshita Y, Takamura T, Honda M, Kita Y, Zen Y, Kato K, et al. The effects of ezetimibe on non-alcoholic fatty liver disease and glucose metabolism: A randomised controlled trial. Diabetologia (2014) 57(5):878–90. doi: 10.1007/s00125-013-3149-9
117. Park H, Shima T, Yamaguchi K, Mitsuyoshi H, Minami M, Yasui K, et al. Efficacy of long-term ezetimibe therapy in patients with nonalcoholic fatty liver disease. J Gastroenterol (2011) 46(1):101–7. doi: 10.1007/s00535-010-0291-8
118. Lee HY, Jun DW, Kim HJ, Oh H, Saeed WK, Ahn H, et al. Ezetimibe decreased nonalcoholic fatty liver disease activity score but not hepatic steatosis. Korean J Internal Med (2019) 34(2):296–304. doi: 10.3904/kjim.2017.194
119. Noto D, Petta S, Giammanco A, Spina R, Cabibbi D, Porcasi R, et al. Lifestyle versus ezetimibe plus lifestyle in patients with biopsy-proven non-alcoholic steatohepatitis (Listen): A double-blind randomised placebo-controlled trial. Nutrition Metab Cardiovasc Dis NMCD (2022) 32(5):1288–91. doi: 10.1016/j.numecd.2022.01.024
120. Van der Graaff D, Kwanten WJ, Couturier FJ, Govaerts JS, Verlinden W, Brosius I, et al. Severe steatosis induces portal hypertension by systemic arterial hyporeactivity and hepatic vasoconstrictor hyperreactivity in rats. Lab investigat J Tech Methods Pathol (2018) 98(10):1263–75. doi: 10.1038/s41374-017-0018-z
121. Francque S, Laleman W, Verbeke L, Van Steenkiste C, Casteleyn C, Kwanten W, et al. Increased intrahepatic resistance in severe steatosis: Endothelial dysfunction, vasoconstrictor overproduction and altered microvascular architecture. Lab investigat J Tech Methods Pathol (2012) 92(10):1428–39. doi: 10.1038/labinvest.2012.103
122. van der Graaff D, Chotkoe S, De Winter B, De Man J, Casteleyn C, Timmermans JP, et al. Vasoconstrictor antagonism improves functional and structural vascular alterations and liver damage in rats with early nafld. JHEP Rep (2022) 4(2):100412. doi: 10.1016/j.jhepr.2021.100412
123. Oikonomou D, Georgiopoulos G, Katsi V, Kourek C, Tsioufis C, Alexopoulou A, et al. Non-alcoholic fatty liver disease and hypertension: Coprevalent or correlated? Eur J Gastroenterol Hepatol (2018) 30(9):979–85. doi: 10.1097/meg.0000000000001191
124. Bravo M, Raurell I, Barberá A, Hide D, Gil M, Estrella F, et al. Synergic effect of atorvastatin and ambrisentan on sinusoidal and hemodynamic alterations in a rat model of Nash. Dis Models Mech (2021) 14(5):dmm048884. doi: 10.1242/dmm.048884
125. Wang CH, Liu HM, Chang ZY, Huang TH, Lee TY. Losartan prevents hepatic steatosis and macrophage polarization by inhibiting hif-1α in a murine model of nafld. Int J Mol Sci (2021) 22(15):7841. doi: 10.3390/ijms22157841
126. Park JG, Mok JS, Han YI, Park TS, Kang KW, Choi CS, et al. Connectivity mapping of angiotensin-ppar interactions involved in the amelioration of non-alcoholic steatohepatitis by telmisartan. Sci Rep (2019) 9(1):4003. doi: 10.1038/s41598-019-40322-1
127. Borém LMA, Neto JFR, Brandi IV, Lelis DF, Santos SHS. The role of the angiotensin ii type I receptor blocker telmisartan in the treatment of non-alcoholic fatty liver disease: A brief review. Hypertension Res Off J Japanese Soc Hypertension (2018) 41(6):394–405. doi: 10.1038/s41440-018-0040-6
128. Dufour JF, Oneta CM, Gonvers JJ, Bihl F, Cerny A, Cereda JM, et al. Randomized placebo-controlled trial of ursodeoxycholic acid with vitamin e in nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol (2006) 4(12):1537–43. doi: 10.1016/j.cgh.2006.09.025
129. Haedrich M, Dufour JF. Udca for Nash: End of the story? J Hepatol (2011) 54(5):856–8. doi: 10.1016/j.jhep.2010.10.009
130. Lindor KD, Kowdley KV, Heathcote EJ, Harrison ME, Jorgensen R, Angulo P, et al. Ursodeoxycholic acid for treatment of nonalcoholic steatohepatitis: Results of a randomized trial. Hepatology (2004) 39(3):770–8. doi: 10.1002/hep.20092
131. Chen YS, Liu HM, Lee TY. Ursodeoxycholic acid regulates hepatic energy homeostasis and white adipose tissue macrophages polarization in leptin-deficiency obese mice. Cells (2019) 8(3):253. doi: 10.3390/cells8030253
132. Ratziu V, de Ledinghen V, Oberti F, Mathurin P, Wartelle-Bladou C, Renou C, et al. A randomized controlled trial of high-dose ursodesoxycholic acid for nonalcoholic steatohepatitis. J Hepatol (2011) 54(5):1011–9. doi: 10.1016/j.jhep.2010.08.030
133. Nadinskaia M, Maevskaya M, Ivashkin V, Kodzoeva K, Pirogova I, Chesnokov E, et al. Ursodeoxycholic acid as a means of preventing atherosclerosis, steatosis and liver fibrosis in patients with nonalcoholic fatty liver disease. World J Gastroenterol (2021) 27(10):959–75. doi: 10.3748/wjg.v27.i10.959
134. Kunne C, Acco A, Duijst S, de Waart DR, Paulusma CC, Gaemers I, et al. Fxr-dependent reduction of hepatic steatosis in a bile salt deficient mouse model. Biochim Biophys Acta (2014) 1842(5):739–46. doi: 10.1016/j.bbadis.2014.02.004
135. Mudaliar S, Henry RR, Sanyal AJ, Morrow L, Marschall HU, Kipnes M, et al. Efficacy and safety of the farnesoid X receptor agonist obeticholic acid in patients with type 2 diabetes and nonalcoholic fatty liver disease. Gastroenterology (2013) 145(3):574–82.e1. doi: 10.1053/j.gastro.2013.05.042
136. Neuschwander-Tetri BA, Loomba R, Sanyal AJ, Lavine JE, Van Natta ML, Abdelmalek MF, et al. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (Flint): A multicentre, randomised, placebo-controlled trial. Lancet (London England) (2015) 385(9972):956–65. doi: 10.1016/s0140-6736(14)61933-4
137. Ratziu V, Sanyal AJ, Loomba R, Rinella M, Harrison S, Anstee QM, et al. Regenerate: Design of a pivotal, randomised, phase 3 study evaluating the safety and efficacy of obeticholic acid in patients with fibrosis due to nonalcoholic steatohepatitis. Contemp Clin trials (2019) 84:105803. doi: 10.1016/j.cct.2019.06.017
138. Younossi ZM, Ratziu V, Loomba R, Rinella M, Anstee QM, Goodman Z, et al. Obeticholic acid for the treatment of non-alcoholic steatohepatitis: Interim analysis from a multicentre, randomised, placebo-controlled phase 3 trial. Lancet (London England) (2019) 394(10215):2184–96. doi: 10.1016/s0140-6736(19)33041-7
139. Iacono A, Raso GM, Canani RB, Calignano A, Meli R. Probiotics as an emerging therapeutic strategy to treat nafld: Focus on molecular and biochemical mechanisms. J Nutr Biochem (2011) 22(8):699–711. doi: 10.1016/j.jnutbio.2010.10.002
140. Aron-Wisnewsky J, Vigliotti C, Witjes J, Le P, Holleboom AG, Verheij J, et al. Gut microbiota and human nafld: Disentangling microbial signatures from metabolic disorders. Nat Rev Gastroenterol Hepatol (2020) 17(5):279–97. doi: 10.1038/s41575-020-0269-9
141. Park JS, Seo JH, Youn HS. Gut microbiota and clinical disease: Obesity and nonalcoholic fatty liver disease. Pediatr gastroenterol Hepatol Nutr (2013) 16(1):22–7. doi: 10.5223/pghn.2013.16.1.22
142. Shao L, Song Y, Shi JP. Role of gut-liver-immune axis in the pathogenesis of nonalcoholic steatohepatitis. Chin J Hep (2021) 29(6):505–9. doi: 10.3760/cma.j.cn501113-20210430-00215
143. Stefan N, Häring HU, Cusi K. Non-alcoholic fatty liver disease: Causes, diagnosis, cardiometabolic consequences, and treatment strategies. Lancet Diabetes Endocrinol (2019) 7(4):313–24. doi: 10.1016/s2213-8587(18)30154-2
144. Hao ZY, Zeng X, Lin Y. Role of the gut microbiota in the diagnosis and treatment of hepatobiliary diseases. Chin J Dig (2020) 40(1):69–70. doi: 10.3760/cma.j.issn.0254-1432.2020.01.017
145. Aller R, De Luis DA, Izaola O, Conde R, Gonzalez Sagrado M, Primo D, et al. Effect of a probiotic on liver aminotransferases in nonalcoholic fatty liver disease patients: A double blind randomized clinical trial. Eur Rev Med Pharmacol Sci (2011) 15(9):1090–5.
146. Chen Y, Feng R, Yang X, Dai J, Huang M, Ji X, et al. Yogurt improves insulin resistance and liver fat in obese women with nonalcoholic fatty liver disease and metabolic syndrome: A randomized controlled trial. Am J Clin Nutr (2019) 109(6):1611–9. doi: 10.1093/ajcn/nqy358
147. Gao ML, Zhao BS, Zhou LH. Effects of intestinal flora regulation therapy on liver function and blood lipid metabolism in patients with non-alcoholic fatty liver. J North Sichuan Med Coll (2021) 36(12):1597–1599,1608. doi: 10.3969/j.issn.1005-3697.2021.12.014
148. Sepideh A, Karim P, Hossein A, Leila R, Hamdollah M, Mohammad EG, et al. Effects of multistrain probiotic supplementation on glycemic and inflammatory indices in patients with nonalcoholic fatty liver disease: A double-blind randomized clinical trial. J Am Coll Nutr (2016) 35(6):500–5. doi: 10.1080/07315724.2015.1031355
149. Kobyliak N, Abenavoli L, Mykhalchyshyn G, Kononenko L, Boccuto L, Kyriienko D, et al. A multi-strain probiotic reduces the fatty liver index, cytokines and aminotransferase levels in nafld patients: Evidence from a randomized clinical trial. J gastrointestinal liver Dis JGLD (2018) 27(1):41–9. doi: 10.15403/jgld.2014.1121.271.kby
150. Kobyliak N, Abenavoli L, Falalyeyeva T, Mykhalchyshyn G, Boccuto L, Kononenko L, et al. Beneficial effects of probiotic combination with omega-3 fatty acids in nafld: A randomized clinical study. Minerva Med (2018) 109(6):418–28. doi: 10.23736/s0026-4806.18.05845-7
151. Mohamad Nor MH, Ayob N, Mokhtar NM, Raja Ali RA, Tan GC, Wong Z, et al. The effect of probiotics (Mcp(®) bcmc(®) strains) on hepatic steatosis, small intestinal mucosal immune function, and intestinal barrier in patients with non-alcoholic fatty liver disease. Nutrients (2021) 13(9):3192. doi: 10.3390/nu13093192
152. Bomhof MR, Parnell JA, Ramay HR, Crotty P, Rioux KP, Probert CS, et al. Histological improvement of non-alcoholic steatohepatitis with a prebiotic: A pilot clinical trial. Eur J Nutr (2019) 58(4):1735–45. doi: 10.1007/s00394-018-1721-2
153. Malaguarnera M, Vacante M, Antic T, Giordano M, Chisari G, Acquaviva R, et al. Bifidobacterium longum with fructo-oligosaccharides in patients with non alcoholic steatohepatitis. Dig Dis Sci (2012) 57(2):545–53. doi: 10.1007/s10620-011-1887-4
154. Eslamparast T, Poustchi H, Zamani F, Sharafkhah M, Malekzadeh R, Hekmatdoost A. Synbiotic supplementation in nonalcoholic fatty liver disease: A randomized, double-blind, placebo-controlled pilot study. Am J Clin Nutr (2014) 99(3):535–42. doi: 10.3945/ajcn.113.068890
155. Asgharian A, Askari G, Esmailzade A, Feizi A, Mohammadi V. The effect of symbiotic supplementation on liver enzymes, c-reactive protein and ultrasound findings in patients with non-alcoholic fatty liver disease: A clinical trial. Int J Prev Med (2016) 7:59. doi: 10.4103/2008-7802.178533
156. Craven L, Rahman A, Nair Parvathy S, Beaton M, Silverman J, Qumosani K, et al. Allogenic fecal microbiota transplantation in patients with nonalcoholic fatty liver disease improves abnormal small intestinal permeability: A randomized control trial. Am J Gastroenterol (2020) 115(7):1055–65. doi: 10.14309/ajg.0000000000000661
157. Xue L, Deng Z, Luo W, He X, Chen Y. Effect of fecal microbiota transplantation on non-alcoholic fatty liver disease: A randomized clinical trial. Front Cell infection Microbiol (2022) 12:759306. doi: 10.3389/fcimb.2022.759306
158. Siddiqui MS, Idowu MO, Parmar D, Borg BB, Denham D, Loo NM, et al. A phase 2 double blinded, randomized controlled trial of saroglitazar in patients with nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol (2021) 19(12):2670–2. doi: 10.1016/j.cgh.2020.10.051
159. Akbari R, Behdarvand T, Afarin R, Yaghooti H, Jalali MT, Mohammadtaghvaei N. Saroglitazar improved hepatic steatosis and fibrosis by modulating inflammatory cytokines and adiponectin in an animal model of non-alcoholic steatohepatitis. BMC Pharmacol Toxicol (2021) 22(1):53. doi: 10.1186/s40360-021-00524-8
160. Gawrieh S, Noureddin M, Loo N, Mohseni R, Awasty V, Cusi K, et al. Saroglitazar, a ppar-A/Γ agonist, for treatment of nafld: A randomized controlled double-blind phase 2 trial. Hepatology (2021) 74(4):1809–24. doi: 10.1002/hep.31843
161. Francque SM, Bedossa P, Ratziu V, Anstee QM, Bugianesi E, Sanyal AJ, et al. A randomized, controlled trial of the pan-ppar agonist lanifibranor in Nash. New Engl J Med (2021) 385(17):1547–58. doi: 10.1056/NEJMoa2036205
162. Gastaldelli A, Sabatini S, Carli F, Gaggini M, Bril F, Belfort-DeAguiar R, et al. Ppar-Γ-Induced changes in visceral fat and adiponectin levels are associated with improvement of steatohepatitis in patients with Nash. Liver Int (2021) 41(11):2659–70. doi: 10.1111/liv.15005
163. Ratziu V, Harrison SA, Francque S, Bedossa P, Lehert P, Serfaty L, et al. Elafibranor, an agonist of the peroxisome proliferator-activated receptor-A and -Δ, induces resolution of nonalcoholic steatohepatitis without fibrosis worsening. Gastroenterology (2016) 150(5):1147–59.e5. doi: 10.1053/j.gastro.2016.01.038
164. Nakajima A, Eguchi Y, Yoneda M, Imajo K, Tamaki N, Suganami H, et al. Randomised clinical trial: Pemafibrate, a novel selective peroxisome proliferator-activated receptor A modulator (Spparmα), versus placebo in patients with non-alcoholic fatty liver disease. Aliment Pharmacol Ther (2021) 54(10):1263–77. doi: 10.1111/apt.16596
165. Kannt A, Wohlfart P, Madsen AN, Veidal SS, Feigh M, Schmoll D. Activation of thyroid hormone receptor-B improved disease activity and metabolism independent of body weight in a mouse model of non-alcoholic steatohepatitis and fibrosis. Br J Pharmacol (2021) 178(12):2412–23. doi: 10.1111/bph.15427
166. Harrison SA, Bashir MR, Guy CD, Zhou R, Moylan CA, Frias JP, et al. Resmetirom (Mgl-3196) for the treatment of non-alcoholic steatohepatitis: A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet (London England) (2019) 394(10213):2012–24. doi: 10.1016/s0140-6736(19)32517-6
167. Harrison SA, Bashir M, Moussa SE, McCarty K, Pablo Frias J, Taub R, et al. Effects of resmetirom on noninvasive endpoints in a 36-week phase 2 active treatment extension study in patients with Nash. Hepatol Commun (2021) 5(4):573–88. doi: 10.1002/hep4.1657
168. Caddeo A, Kowalik MA, Serra M, Runfola M, Bacci A, Rapposelli S, et al. Tg68, a novel thyroid hormone receptor-B agonist for the treatment of nafld. Int J Mol Sci (2021) 22(23):13105. doi: 10.3390/ijms222313105
169. Talukdar S, Kharitonenkov A. Fgf19 and Fgf21: In Nash we trust. Mol Metab (2021) 46:101152. doi: 10.1016/j.molmet.2020.101152
170. Harrison SA, Rinella ME, Abdelmalek MF, Trotter JF, Paredes AH, Arnold HL, et al. Ngm282 for treatment of non-alcoholic steatohepatitis: A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet (London England) (2018) 391(10126):1174–85. doi: 10.1016/s0140-6736(18)30474-4
171. Harrison SA, Rossi SJ, Paredes AH, Trotter JF, Bashir MR, Guy CD, et al. Ngm282 improves liver fibrosis and histology in 12 weeks in patients with nonalcoholic steatohepatitis. Hepatology (2020) 71(4):1198–212. doi: 10.1002/hep.30590
172. Harrison SA, Neff G, Guy CD, Bashir MR, Paredes AH, Frias JP, et al. Efficacy and safety of aldafermin, an engineered Fgf19 analog, in a randomized, double-blind, placebo-controlled trial of patients with nonalcoholic steatohepatitis. Gastroenterology (2021) 160(1):219–31.e1. doi: 10.1053/j.gastro.2020.08.004
173. Harrison SA, Abdelmalek MF, Neff G, Gunn N, Guy CD, Alkhouri N, et al. Aldafermin in patients with non-alcoholic steatohepatitis (Alpine 2/3): A randomised, double-blind, placebo-controlled, phase 2b trial. Lancet Gastroenterol Hepatol (2022) 7(7):603–16. doi: 10.1016/s2468-1253(22)00017-6
174. Rinella ME, Trotter JF, Abdelmalek MF, Paredes AH, Connelly MA, Jaros MJ, et al. Rosuvastatin improves the Fgf19 analogue Ngm282-associated lipid changes in patients with non-alcoholic steatohepatitis. J Hepatol (2019) 70(4):735–44. doi: 10.1016/j.jhep.2018.11.032
175. Ritchie M, Hanouneh IA, Noureddin M, Rolph T, Alkhouri N. Fibroblast growth factor (Fgf)-21 based therapies: A magic bullet for nonalcoholic fatty liver disease (Nafld)? Expert Opin investigat Drugs (2020) 29(2):197–204. doi: 10.1080/13543784.2020.1718104
176. Charles ED, Neuschwander-Tetri BA, Pablo Frias J, Kundu S, Luo Y, Tirucherai GS, et al. Pegbelfermin (Bms-986036), pegylated Fgf21, in patients with obesity and type 2 diabetes: Results from a randomized phase 2 study. Obes (Silver Spring Md) (2019) 27(1):41–9. doi: 10.1002/oby.22344
177. Sanyal A, Charles ED, Neuschwander-Tetri BA, Loomba R, Harrison SA, Abdelmalek MF, et al. Pegbelfermin (Bms-986036), a pegylated fibroblast growth factor 21 analogue, in patients with non-alcoholic steatohepatitis: A randomised, double-blind, placebo-controlled, phase 2a trial. Lancet (London England) (2019) 392(10165):2705–17. doi: 10.1016/s0140-6736(18)31785-9
178. Verzijl CRC, Van De Peppel IP, Struik D, Jonker JW. Pegbelfermin (Bms-986036): An investigational pegylated fibroblast growth factor 21 analogue for the treatment of nonalcoholic steatohepatitis. Expert Opin investigat Drugs (2020) 29(2):125–33. doi: 10.1080/13543784.2020.1708898
179. Syed-Abdul MM, Parks EJ, Gaballah AH, Bingham K, Hammoud GM, Kemble G, et al. Fatty acid synthase inhibitor tvb-2640 reduces hepatic De novo lipogenesis in males with metabolic abnormalities. Hepatology (2020) 72(1):103–18. doi: 10.1002/hep.31000
180. Loomba R, Mohseni R, Lucas KJ, Gutierrez JA, Perry RG, Trotter JF, et al. Tvb-2640 (Fasn inhibitor) for the treatment of nonalcoholic steatohepatitis: Fascinate-1, a randomized, placebo-controlled phase 2a trial. Gastroenterology (2021) 161(5):1475–86. doi: 10.1053/j.gastro.2021.07.025
Keywords: nonalcoholic fatty liver disease, non-alcoholic steatohepatitis, diet, exercise, medical treatment
Citation: Rong L, Zou J, Ran W, Qi X, Chen Y, Cui H and Guo J (2023) Advancements in the treatment of non-alcoholic fatty liver disease (NAFLD). Front. Endocrinol. 13:1087260. doi: 10.3389/fendo.2022.1087260
Received: 02 November 2022; Accepted: 28 December 2022;
Published: 16 January 2023.
Edited by:
Andrea Dalbeni, Verona University Hospital, ItalyCopyright © 2023 Rong, Zou, Ran, Qi, Chen, Cui and Guo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinjun Guo, Z3VvamluanVuMTk3MkAxNjMuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.