
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 16 December 2022
Sec. Clinical Diabetes
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1066521
This article is part of the Research Topic Application of Telehealth to Diabetes Care Delivery and Medical Training: Challenges and Opportunities View all 8 articles
 Ananta Addala1*
Ananta Addala1* Stephanie L. Filipp2Lauren E. Figg1Claudia Anez-Zabala2Rayhan A. Lal1,3Matthew J. Gurka2
Stephanie L. Filipp2Lauren E. Figg1Claudia Anez-Zabala2Rayhan A. Lal1,3Matthew J. Gurka2 Michael J. Haller2David M. Maahs1,4Ashby F. Walker5 and for the Project ECHO Diabetes Research Team
Michael J. Haller2David M. Maahs1,4Ashby F. Walker5 and for the Project ECHO Diabetes Research TeamIntroduction: In the US, many individuals with diabetes do not have consistent access to endocrinologists and therefore rely on primary care providers (PCPs) for their diabetes management. Project ECHO (Extension for Community Healthcare Outcomes) Diabetes, a tele-education model, was developed to empower PCPs to independently manage diabetes, including education on diabetes technology initiation and use, to bridge disparities in diabetes.
Methods: PCPs (n=116) who participated in Project ECHO Diabetes and completed pre- and post-intervention surveys were included in this analysis. The survey was administered in California and Florida to participating PCPs via REDCap and paper surveys. This survey aimed to evaluate practice demographics, protocols with adult and pediatric T1D management, challenges, resources, and provider knowledge and confidence in diabetes management. Differences and statistical significance in pre- and post-intervention responses were evaluated via McNemar’s tests.
Results: PCPs reported improvement in all domains of diabetes education and management. From baseline, PCPs reported improvement in their confidence to serve as the T1D provider for their community (pre vs post: 43.8% vs 68.8%, p=0.005), manage insulin therapy (pre vs post: 62.8% vs 84.3%, p=0.002), and identify symptoms of diabetes distress (pre vs post: 62.8% vs 84.3%, p=0.002) post-intervention. Compared to pre-intervention, providers reported significant improvement in their confidence in all aspects of diabetes technology including prescribing technology (41.2% vs 68.6%, p=0.001), managing insulin pumps (41.2% vs 68.6%, p=0.001) and hybrid closed loop (10.2% vs 26.5%, p=0.033), and interpreting sensor data (41.2% vs 68.6%, p=0.001) post-intervention.
Discussion: PCPs who participated in Project ECHO Diabetes reported increased confidence in diabetes management, with notable improvement in their ability to prescribe, manage, and troubleshoot diabetes technology. These data support the use of tele-education of PCPs to increase confidence in diabetes technology management as a feasible strategy to advance equity in diabetes management and outcomes.
Disparities in diabetes management and outcomes are increasingly recognized as important to address (1–3). The drivers of disparities are multi-layered with contributions from social determinants of health, structural inequities, insurance policies, and health care providers (1, 4). Many individuals with diabetes do not consistently receive subspecialty care from an endocrinologist or diabetologist and rely on primary care providers (PCPs) for their diabetes management (5, 6). However, PCPs are not trained on the specifics of diabetes management, including the nuances of insulin dosing and diabetes technology management. Although PCPs report regularly filling insulin prescriptions for individuals with diabetes, they report low confidence in providing diabetes care, including diabetes technology management (6). Lack of provider confidence in diabetes technology management and provider bias are barriers to technology access and utilization for individuals with diabetes (7–9). Disparities in diabetes management are pronounced in underrepresented groups including individuals who do not receive care from an endocrinologists/diabetologist, those from racial/ethnic minority groups, with public insurance, from low socioeconomic groups, and/or live in rural communities (5, 10–12).
During the COVID-19 pandemic, increase in telehealth utilization, where the endocrinology subspecialty provider engages in direct patient care and management, has become a more commonplace and well-accepted (13–15). While this model has been considered useful in increasing the access to subspecialty care, barriers to telehealth utilization have included limitations due to English proficiency, health literacy, technology access, and broadband/connectivity issues (16–18). Additionally, there’s a well-established shortage of endocrinology subspecialty providers that make it challenging for individuals living with diabetes to reliably and consistently seek medical care from an endocrinologist (6, 19–21). In addition to the shortage of pediatric and adult endocrinology providers, the incidence and prevalence of pediatric and adult diabetes is increasing which further exacerbates the access gap, particularly for underrepresented populations (22–24). The COVID-19 pandemic accelerated telehealth implementation for nearly all diagnoses such that telemedicine is now considered a standard modality for health care delivery (13, 14, 25, 26). That said, telehealth alone is not sufficient to ensure access to standard of care for many individuals living with diabetes. This is especially true when it comes to the democratization of adjuvant pharmacotherapy and access to diabetes technologies.
PCP education is a reliable method to increase comfort with medical management and has been utilized to expand access and reliably deliver standard of care (25–32). Additionally, self-reported improvements in provider confidence are associated with changes in clinical practice and behavior in the medical field at large (33–35). To increase PCP comfort with diabetes management, Project ECHO (Extension for Community Healthcare Outcomes) Diabetes was developed as a tele-education model to democratize diabetes knowledge to PCPs (5, 6, 36–38).The education provided in Project ECHO Diabetes aimed to address general diabetes knowledge, insulin and diabetes pharmacotherapy, diabetes technology management, and psychosocial considerations. In this analysis, we aim to evaluate the impact of Project ECHO Diabetes on PCP confidence in management of diabetes. We hypothesized that with systematic education, PCPs will have an increased confidence in all domains of diabetes management.
University of Florida and Stanford University (research “Hubs”) expanded the existing Project ECHO® model (25–28) in collaboration with the University of New Mexico to develop Project ECHO Diabetes, a tele-education program that aimed to train health care providers in underserved areas of California and Florida with a specific focus on recruiting PCPs from federally qualifying health centers and community health centers. The Project ECHO Diabetes program provided participating health centers (“spokes”; Appendix B lists all participating research spokes) and their providers tele-education with continuing medical education credits for participation that details diabetes management. The Project ECHO Diabetes program implemented a stepped-wedge study design with staggered control and intervention periods for new participating spokes. Provider outcomes were collected at baseline, six and 12 months, marking the study end.
The Project ECHO Diabetes Curriculum was curated and developed by the multi-disciplinary Hub teams at University of Florida and Stanford University, comprised of pediatric and adult endocrinologists, registered nurses, Certified Diabetes Care and Education Specialists, pharmacists, diabetes psychologists, exercise physiologists, and social workers, to name a few. Education first begins during an orientation session which included providing continuous glucose monitoring (CGM) to providers to experience wearing a CGM and an overview of key diabetes management areas. After the onboarding process, weekly tele-education sessions included a 20 to 30 minute didactic session by experts from the Hub team or affiliated experts to deliver content on diabetes management consistent with the American Diabetes Association Standards of Care (39–44). Table 1 outlines 24 weekly sessions carried out over the 6-month curriculum. Didactic sessions are followed by a case presentation from the spokes, where the presenting provider details a clinical conundrum in the management of diabetes. Feedback is initially solicited from the spokes, followed by input from the Hub. These tele-education clinic sessions are accredited by both universities for Continuing Medical Education credits, which are provided at no cost to attendees.
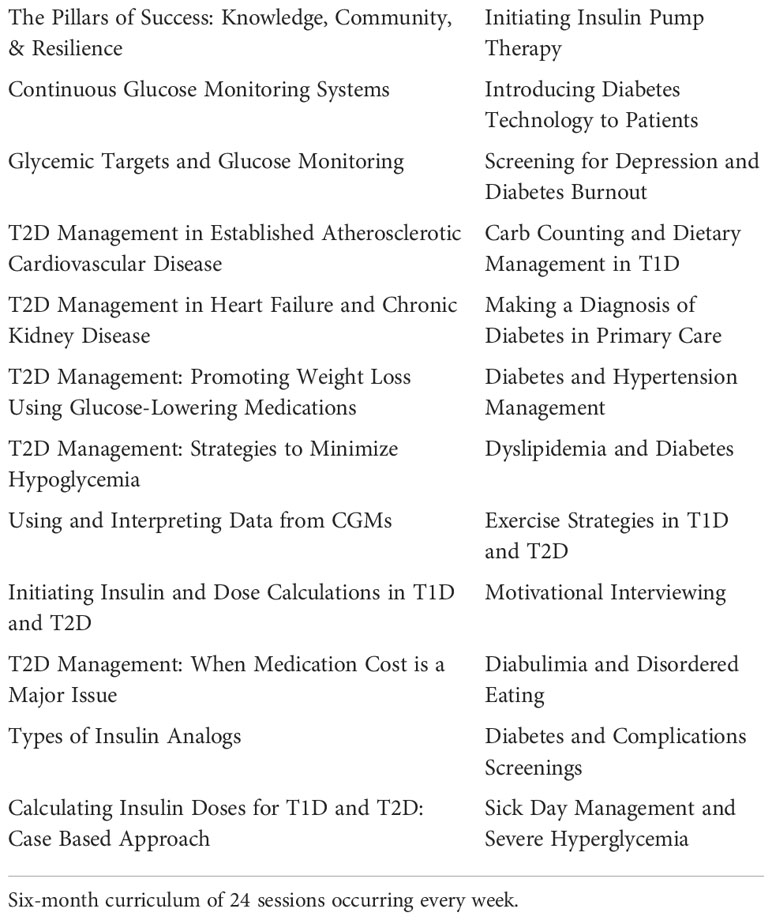
Table 1 Project ECHO Diabetes Curriculum.
Participating providers were invited to take pre- and post-intervention surveys administered via REDCap© (Research Electronic Data Capture) prior to and after the 6-month intervention. REDCap is a secure online-enabled platform which allowed surveys to be sent directly via email and taken electronically using any web browser.
The survey content was designed to assess knowledge (using 18 multiple-choice test questions) and confidence (using 28 questions with a 4-point Likert scale response set ranging from ‘not at all confident’ to ‘extremely confident’) in diabetes care. Domains of confidence included: general diabetes management, insulin management, diabetes technology, and psychosocial management. Providers were offered surveys at all three data collection windows. Due to variable kick-off dates for the implementation of Project ECHO Diabetes for cohorts 1 and 2, providers were offered either two pre-surveys and one post survey or one pre-survey followed by two post surveys at 6-month intervals.
The a priori primary outcome of this analysis was changes in provider confidence and the secondary outcome was improvement in provider knowledge. To account for variable survey administration, data were extracted on an individual-basis from the earliest pre-test and the latest post-test. Only those providers with at least one pre- and one post-survey were included in the statistical analysis to evaluate change in provider confidence, and acquisition of knowledge with the Project ECHO Diabetes curriculum.
All data management and analyses were conducted using SAS 9.4® (Cary, NC). Descriptive statistics are reported for provider and practice characteristics. Paired pre and post-intervention comparisons were made among new spoke participants to evaluate for change in confidence and knowledge using McNemar’s test; a predetermined alpha of 0.05 was used to evaluate statistical significance. Aggregate data are presented descriptively to elucidate the scope of adult referrals to endocrinology and CGM/insulin pump prescriptions pre- and post-intervention among all responding providers.
Project ECHO Diabetes received institutional review board (IRB) approval by University of Florida and Stanford University.
In total, 274 providers (123 from California, 145 from Florida) were referred to Project ECHO Diabetes for participation by their Spoke site’s ECHO Champion and 116 providers completed at least one survey (Table 2). Providers were predominately PCPs (63.7% physicians and 29.1% advanced practice providers). Responding providers have been in practice for a median of 7.5 years (IQR 2.5,16.5). Across the three data collection time windows, 110 providers completed a pre-intervention survey, 58 providers completed a post-intervention survey, and among those, 52 providers completed both a pre- and post-intervention survey.
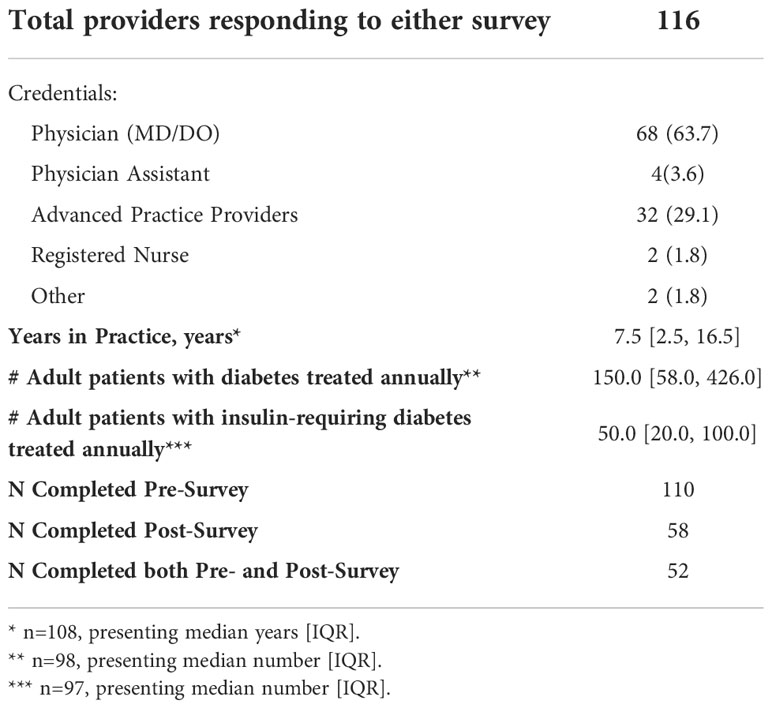
Table 2 Provider characteristics.
When evaluating data for those providers who had a pre- and post-intervention survey available (n=52), providers demonstrated an improvement in confidence to manage diabetes in all the surveyed questions with 64.3% of improvements reaching statistical significance (Table 3). Despite functioning as a primary diabetes provider, 43.8% of surveyed providers felt confidence in being a diabetes resource for the community as well as for other providers and clinics. However, after Project ECHO Diabetes, this confidence increased to 68.8% (p=0.005). Provider confidence increased in general diabetes management including collecting diabetes-focused health history (pre vs post: 78.4% vs. 94.1%, p=0.01) and incorporating diabetes guidelines into clinical care (pre vs post: 72.6% vs. 86.3%, p=0.02).
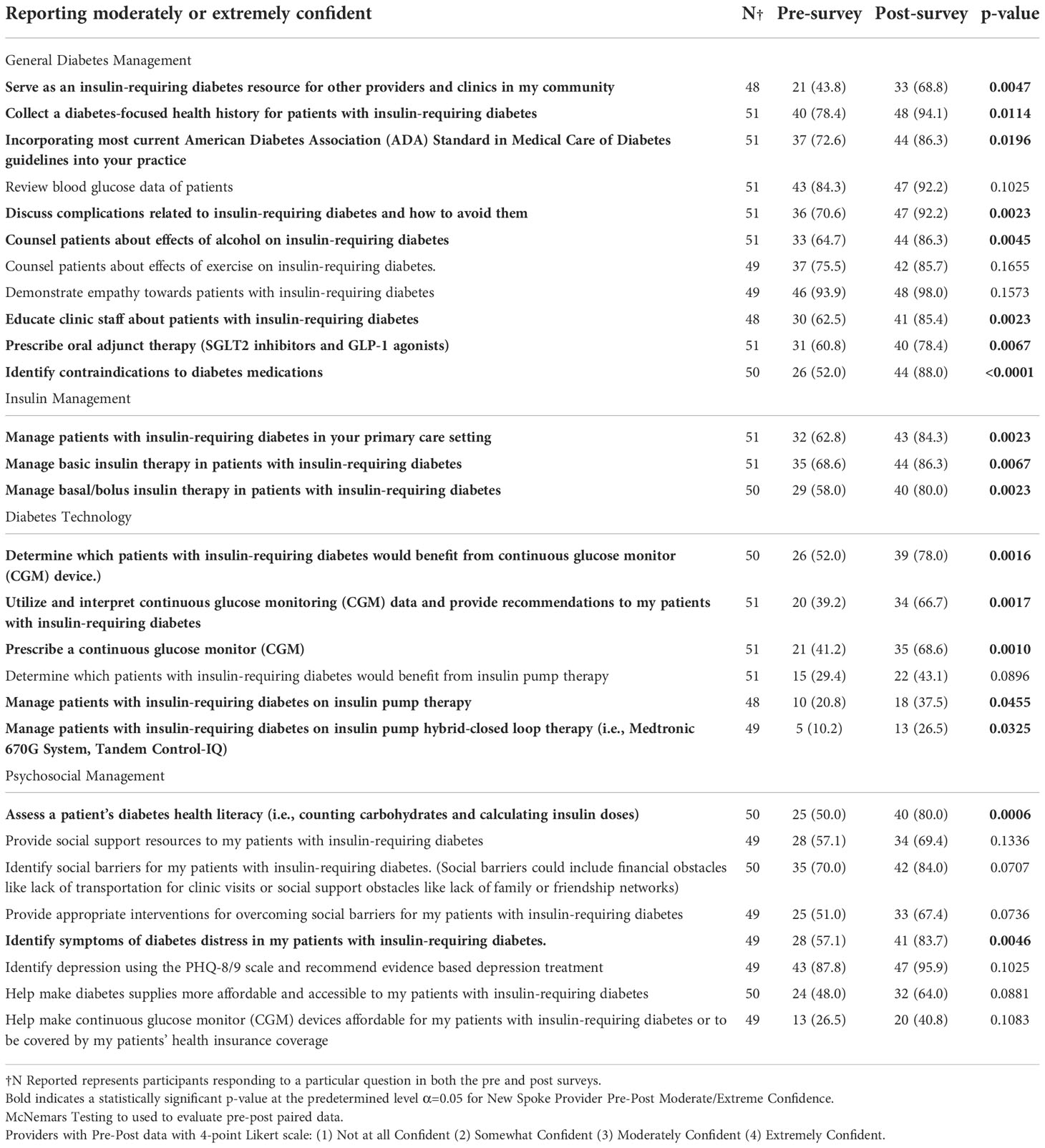
Table 3 Providers report confidence on a variety of diabetes-related items.
Providers also felt more comfortable with insulin management in the primary care setting (pre vs post: 62.8% vs. 84.3%, p=0.002) as well as in basic insulin management (pre vs post: 68.6% vs. 86.3%, p=0.007) and management of basal/bolus therapy (pre vs post: 58.0% vs. 80.0%, p=0.002). Providers had significant improvement in their comfort with oral adjuvant therapy in the treatment of insulin-requiring diabetes including the use of GLP1 agonists and SGLT2 inhibitors (pre vs post: 60.8% vs. 78.4%, p=0.007) and endorsed an ability to identify contraindications in diabetes medications (pre vs post: 52.0% vs. 88.0%, p<0.0001).
When compared to pre-intervention, provider confidence increased in nearly all aspects of CGM management post-intervention, including determining which patients would benefit from CGM (52.0% vs. 78.0%, p=0.002), prescribing CGM (41.2% vs. 68.6%, p=0.001), and interpreting CGM (39.2% vs. 66.7%, p=0.002). Similarly, providers endorsed increased confidence with managing insulin pumps (28.8% vs. 37.5, p=0.046) including hybrid closed loop systems (10.2% vs. 26.5%, p=0.03).
In addition to improvements in confidence, providers demonstrated an improvement in knowledge pertaining to diabetes management (Supplemental Table 1). In particular, provider knowledge increased with respect to calculating insulin doses (pre vs post: 19.2% vs. 48.1%, p=0.002), understanding the impact of metformin in insulin-requiring diabetes (pre vs post: 57.7% vs. 75.0%, p=0.04), pharmacotherapy for weight management in type 2 diabetes (pre vs post: 88.5% vs. 96.2%, p=0.046), and identifying function of various CGM reports (pre vs post: 17.3% vs. 46.2%, p=0.046).
In addition to evaluation of pre-post data among those responding, we descriptively assessed prescribing and referral practices for all providers who responded to any survey, including those who didn’t complete both pre and post. Supplemental Table 2 presents provider confidence for all available pre- and post-intervention surveys (110 and 58 surveys, respectively). Descriptive improvements were observed in all four domains of provider confidence with the greatest improvement gains in CGM prescription (pre: 39.5% and post: 66.7%) and utilization (pre: 38.5% and post: 66.7%). Among providers who completed pre-intervention surveys, 39.3% (n=107 responding) of providers were moderately or extremely comfortable serving as the diabetes resource and post-intervention, 60.7% (n=56 responding) of providers were moderately or extremely comfortable.
We descriptively evaluated prescribing and referral practices for all providers who responded to any survey, including those who didn’t complete both pre and post (Supplemental Table 3). Before Project ECHO Diabetes, 15.4% (n=65 responding) PCPs indicated they always (vs. sometimes or never) referred diabetes care to an endocrinologist but after the intervention, only 5.0% (n=20 responding) would always refer care. Pre-intervention, among all responding providers, only 31.3% reported always prescribing CGM, and 7.3% reported always prescribing insulin pumps. Post-intervention, prescription rose to 51.0% for providers always prescribing CGM and 12.8% for always prescribing insulin pumps.
We report success in increasing PCP confidence and knowledge in the management of diabetes in the primary care setting with a tele-education model as a means to improve access to diabetes standard of care. Project ECHO Diabetes was designed with the pillars of modern medical educational framework to include didactics, case presentations, and supervision from experienced diabetes clinicians (25–28). The systematic delivery of tele-education curriculum to PCPs to execute subspecialized medical care delivery has been successful with the Project ECHO® model (25–32), however this model is under-studied with respect to diabetes field with only two active Project ECHO protocols to address diabetes care (5, 30).
By arming PCPs to effectively manage diabetes, the potential exists to bridge disparities in diabetes management and outcomes. PCPs had a significant increase in their confidence to manage insulin for individuals with diabetes, which was a commonly stated barrier before Project ECHO Diabetes was initiated in the clinics. They also better understood the role that metformin plays on insulin dosing and management. This increased confidence in the management of insulin, including comfort with a basal/bolus regimen, is foundational to the intensive insulin therapy which is associated with improvements in short- and long-term diabetes health outcomes. Providers also had an increase in comfort with new and effective adjuvant therapy for type 2 diabetes including SGLT2 inhibitors and GLP-1 agonist which are associated with a decrease in micro- and macro-vascular complications. PCPs increased comfort with the utilization of adjuvant therapy for type 2 diabetes management is likely to improve utilization of these effective pharmacotherapy. An important next step for this research will be to better understand the impact of this increase in provider confidence on improvements in provider knowledge and changes in prescribing practices. Further studies are needed to better understand how PCP knowledge is impacted with increased confidence as well as if and how this translates to improvements in diabetes technology access for their patients.
Utilization of diabetes technology in the management of diabetes is also associated with improvements in glycemic and quality of life outcomes (45). Providers have been identified as a key barrier to diabetes technology uptake and lack of provider knowledge and confidence in prescribing and managing diabetes technology may be a driver (6, 36). The challenges in obtaining and sustaining technology coverage are barriers for providers due to changing coverage policies, cumbersome paperwork, and the time required to complete the paperwork to secure diabetes technology (46, 47). Additional challenges include sustaining technology coverage as well as interpreting 288 daily glucose points and trends. For primary care clinics that do not have specialized staff to support paperwork and prior authorizations, prescribing diabetes technology devices can be time consuming and compound the limited time PCPs have for care delivery. To address provider acceptance of diabetes technology, we facilitated the use of CGM during the Project ECHO Diabetes orientation for all interested providers and discussed the role of provider implicit bias and payer policies in technology utilization. In the Project ECHO Diabetes curriculum, multiple didactic sessions formally covered management of diabetes technology. During the case presentations, diabetes technology was included in recommendations when clinically indicated. In addition to interpreting CGM data and discussing associated insulin dose changes, we also discussed the burden of alarms, skin irritation, and the psychosocial considerations of starting and maintaining diabetes technology use (36, 48, 49). The orientation and curriculum intentionally focused on strategies to optimize coverage of diabetes technology including requirements to secure technology coverage for individuals with public insurance, navigating prior authorizations, modifying EMR templates to include authorization information, and other strategies suggested by spokes to increase the likelihood of payers covering technology. These solutions likely played a role in increasing PCP comfort with diabetes technology.
Provider confidence in the domain of psychosocial management did not change as dramatically as the other domains. The two areas of increased confidence for providers were in their ability to apply the diabetes distress scale and address health literacy in the management of diabetes. The remaining questions in this domain included concepts more commonly covered in primary care such as identifying and addressing social barriers and utilization of evidence-based depression screening as they are part of well adult care (50). In the remaining domains, other questions where there was not a statistical improvement in confidence were areas where providers had started Project ECHO Diabetes with high confidence (for example, demonstrating empathy towards patients living with insulin requiring diabetes). Providers had low confidence in identifying which patients with insulin-requiring diabetes would benefit from insulin pump therapy, and this did not improve with Project ECHO Diabetes. Many providers care predominantly for individuals with type 2 diabetes and there are currently no standard of care or guidelines detailing when an individual with type 2 diabetes may benefit from insulin pump therapy.
These data should be interpreted in the setting of several limitations including selection bias given the response rates and the likelihood that a provider willing to participate in additional education to learn about diabetes care and management may not be representative of all primary care providers. Providers in the study were also confined to practicing in the state of California and Florida, the location of the Hubs, and therefore these data may not be generalizable to other provider practice areas. The assessment of provider confidence and provider knowledge are reported subjectively and not via previously validated scales. Additionally, provider knowledge assessment did not extensively evaluate all aspects of diabetes management including insulin pump management. While the scales used in this study were iteratively developed and refined from the Project ECHO Diabetes pilot study, PCP self-efficacy scores may not necessarily correlate with other objective measures of PCP competency and may not reflect changes in diabetes technology prescribing habits. A possible confounding factor is that providers may have received information about diabetes in a setting outside of Project ECHO Diabetes that resulted in improved confidence and knowledge in diabetes care. Despite these limitations, these data offer a promising strategy to increase PCPs confidence to deliver diabetes standard of care.
Training PCPs to deliver subspecialty diabetes care including management of insulin, diabetes technology, and oral adjuvant therapy via a tele-education model is effective in improving provider confidence. We demonstrate that this increase in provider confidence translates to an increase in provider knowledge and changes to prescribing practices. Given the increasing burden of diabetes both nationally and globally, partnering with PCPs, who are already caring for individuals with diabetes, to deliver the standard of care in diabetes is a viable path to addressing disparities in access to diabetes care and management.
The raw data support the conclusions of this article will be made available by the authors, without undue reservation upon reasonable request.
Project ECHO Diabetes received institutional review board (IRB) approval by University of Florida and Stanford University. The patients/participants provided their written informed consent to participate in this study.
University of Florida Diabetes Institute:
Michael Haller, MD – Principal Investigator, Pediatric Endocrinologist
Ashby Walker, PhD – Co-Principal Investigator and Project Director, Medical Sociologist
Eleni Sheehan APRN, FNP, CDCES – Clinic Manager
Angelina Bernier, MD – Pediatric Endocrinologist
Sarah Westen, PhD – Clinical Health Psychologist
Hannah Stahmer, RD, CDCES – Registered Dietician
William Troy Donahoo, MD, FTOS – Adult Endocrinologist
Xanadu Roque, BA – Research Coordinator
Gabby Malden, BA – Administrative Assistant
Melanie Hechavarria, MPH – Clinical Research Coordinator
Stanford University:
David Maahs, MD, PhD – Principal Investigator, Pediatric Endocrinologist
Rayhan Lal, MD – Pediatric/Adult Endocrinologist, Clinic Co-Director
Ananta Addala, DO, MPH – Pediatric Endocrinologist, Clinic Co-Director
Lauren Figg, MSW – Program Administrator
Katarina Yabut, BS – Research Assistant
Noor Alramahi, BA – Assistant Clinical Research Coordinator
Ana Cortes, BS – Clinical Research Coordinator, ECHO Clinic Coordinator
Dessi Zaharieva, PhD – Exercise Physiologist
Marina Basina, MD – Adult Endocrinologist
Katie Judge, ACNS-BS, CDCES – Diabetes Educator
Lety Wilke, RN, MSN, ACNS-BC, BC-ADM, CDCES – Diabetes Educator
Korey Hood, PhD – Diabetes Psychologist
Jessie Wong, PhD – Diabetes Psychologist
Jason Wang, MD, PhD – General Pediatrics, Policy Outcomes & Prevention
Suruchi Bhatia, MD – Pediatric Endocrinologist
Eugene Lewit, PhD – Health Economist
University of Florida – Florida Sites
Community Health of South Florida
Miami Beach Community Health Centers
Jessie Trice Community Health System
Evara – Adult Practice
Banyan Health Systems
Orange Blossom Family Health Center
Premier Community HealthCare
Tampa Family Health Centers East
Tampa Family Health Centers West
Borinquen Medical Center
Treasure Coast Community Health
Evara – Pediatric Practice
UF Family Medicine Old Town
UF Family MedicineEastside
Health Care Network SWFLWFL
Stanford University – California Sites
Humboldt Independent Practice Association
CommuniCare – Salud Clinic
Solano County Family Health Services
Open Door Community Health Centers
Mendocino Coast Clinics
Shasta Community Health Center
Shasta Cascade Health Centers
Santa Rosa Community Health
Hill Country Community Clinic
CommuniCare – Davis Community Clinic
CommuniCare – Hansen Family Health Center
Valley Diabetes and Obesity
St Agnes Medical Center
United Indian Health Services – Potawot Health Village
Harmony Health Medical Clinic
DAP Health
Health Service Alliance
La Clinica
Tahoe Forest Multispecialty Clinics
AA, DMM, MJH, and AFW contributed to the concept and design of the study. AA, AFW SLF and MJG structured and SLF and MJG completed the analyses. AA wrote the manuscript with critical contributions from DMM, MJH, RAL, LEF, and AFW. All authors contributed to the article and approved the submitted version.
This work was supported by the Helmsley Charitable Trusts [Grant 147320]. AA is supported by the Maternal Child Health Research Institute and by NIDDK K23 (K23DK131342).
DM has received research support from the National Institutes of Health, JDRF, NSF, and the Helmsley Charitable Trust; and his institution has received research support from Medtronic, Dexcom, Insulet, Bigfoot Biomedical, Tandem, and Roche. He has consulted for Abbott, the Helmsley Charitable Trust, Sanofi, Novo Nordisk, Eli Lilly, and Insulet, and is supported by grant number P30DK116074.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.1066521/full#supplementary-material
Supplementary Table 1 | Provider Knowledge: Number of providers with the correct answers as captured by pre- and post- intervention surveys. Corrected answer highlighted in green. †N Reported represents participants responding to a particular question in both the pre and post surveys. Bold indicates a statistically significant p-value at the predetermined level α=0.05 for New Spoke Provider Pre-Post Moderate/Extreme Confidence. McNemars Testing to used to evaluate pre-post paired data.
Supplementary Table 2 | Providers Report Confidence on a Variety of Diabetes-Related Items Providers with Pre- or Post-intervention data with 4-point Likert scale: (1) Not at all Confident (2) Somewhat Confident (3) Moderately Confident (4) Extremely Confident. †N Reported represents participants responding to a particular question for either the Pre-Survey or Post-Survey.
Supplementary Table 3 | Aggregate pre- & post-intervention survey for providers who completed surveys. * N denotes number of respondents for each question. Response rates for each question varied by which questions providers chose to complete.
1. Hill-Briggs F, Adler NE, Berkowitz SA, Chin MH, Gary-Webb TL, Navas-Acien A, et al. Social determinants of health and diabetes: A scientific review. Dia Care (2021) 44(1):258–79. doi: 10.2337/dci20-0053
2. Lipman TH, Hawkes CP. Racial and socioeconomic disparities in pediatric type 1 diabetes: Time for a paradigm shift in approach. Diabetes Care (2021) 44(1):14–6. doi: 10.2337/dci20-0048
3. CDC. Advancing Health Equity. Centers for disease control and prevention. Available at: https://www.cdc.gov/diabetes/health-equity/index.html.
4. Ogunwole SM, Golden SH. Social determinants of health and structural inequities–root causes of diabetes disparities. Diabetes Care (2020) 44(1):11–3. doi: 10.2337/dci20-0060
5. Walker AF, Cuttriss N, Haller MJ, Hood KK, Gurka MJ, Filipp SL, et al. Democratizing type 1 diabetes specialty care in the primary care setting to reduce health disparities: project extension for community healthcare outcomes (ECHO) T1D. BMJ Open Diabetes Res Care (2021) 9(1):e002262. doi: 10.1136/bmjdrc-2021-002262
6. Lal RA, Cuttriss N, Haller MJ, Yabut K, Anez-Zabala C, Hood KK, et al. Primary care providers in California and Florida report low confidence in providing type 1 diabetes care. Clin Diabetes (2020) 38(2):159–65. doi: 10.2337/cd19-0060
7. Tanenbaum ML, Adams RN, Lanning MS, Hanes SJ, Agustin BI, Naranjo D, et al. Using cluster analysis to understand clinician readiness to promote continuous glucose monitoring adoption. J Diabetes Sci Technol (2018) 12(6):1108–15. doi: 10.1177/1932296818786486
8. Addala A, Hanes S, Naranjo D, Maahs DM, Hood KK. Provider implicit bias impacts pediatric type 1 diabetes technology recommendations in the united states: Findings from the gatekeeper study. J Diabetes Sci Technol (2021) 15:19322968211006476. doi: 10.1177/19322968211006476
9. Odugbesan O, Addala A, Nelson G, Hopkins R, Cossen K, Schmitt J, et al. Implicit racial-ethnic and insurance mediated bias to recommending diabetes technology: Insights from T1D exchange multi-center pediatric and adult diabetes provider cohort. Diabetes Technol Ther (2022) 24(9):619–27. doi: 10.1089/dia.2022.0042
10. Addala A, Auzanneau M, Miller K, Maier W, Foster N, Kapellen T, et al. Decade of disparities in diabetes technology use and HbA1c in pediatric type 1 diabetes: A transatlantic comparison. Diabetes Care (2020) 44(1):133–40. doi: 10.2337/dc20-0257
11. Agarwal S, Kanapka LG, Raymond JK, Walker A, Gerard-Gonzalez A, Kruger D, et al. Racial-ethnic inequity in young adults with type 1 diabetes. J Clin Endocrinol Metab (2020) 105(8):e2960–9. doi: 10.1210/clinem/dgaa236
12. Majidi S, Ebekozien O, Noor N, Lyons SK, McDonough R, Gandhi K, et al. Inequities in health outcomes in children and adults with type 1 diabetes: Data from the T1D exchange quality improvement collaborative. Clin Diabetes (2021) 39(3):278–83. doi: 10.2337/cd21-0028
13. Cahan EM, Maturi J, Bailey P, Fernandes S, Addala A, Kibrom S, et al. The impact of telehealth adoption during COVID-19 pandemic on patterns of pediatric subspecialty care utilization. Acad Pediatr (2022) 22(8):1375–83. doi: 10.1016/j.acap.2022.03.010
14. Prahalad P, Leverenz B, Freeman A, Grover M, Shah S, Conrad B, et al. Closing disparities in pediatric diabetes telehealth care: Lessons from telehealth necessity during the COVID-19 pandemic. Clin Diabetes (2022) 40(2):153–7. doi: 10.2337/cd20-0123
15. Wosik J, Fudim M, Cameron B, Gellad ZF, Cho A, Phinney D, et al. Telehealth transformation: COVID-19 and the rise of virtual care. J Am Med Inform Assoc (2020) 27(6):957–62. doi: 10.1093/jamia/ocaa067
16. Govier DJ, Cohen-Cline H, Marsi K, Roth SE. Differences in access to virtual and in-person primary care by race/ethnicity and community social vulnerability among adults diagnosed with COVID-19 in a large, multi-state health system. BMC Health Serv Res (2022) 22(1):511. doi: 10.1186/s12913-022-07858-x
17. Adepoju OE, Chae M, Ojinnaka CO, Shetty S, Angelocci T. Utilization gaps during the COVID-19 pandemic: Racial and ethnic disparities in telemedicine uptake in federally qualified health center clinics. J Gen Intern Med (2022) 37(5):1191–7. doi: 10.1007/s11606-021-07304-4
18. Roth SE, Govier DJ, Marsi K, Cohen-Cline H. Differences in outpatient health care utilization 12 months after COVID-19 infection by Race/Ethnicity and community social vulnerability. Int J Environ Res Public Health (2022) 19(6):3481. doi: 10.3390/ijerph19063481
19. Rizza RA, Vigersky RA, Rodbard HW, Ladenson PW, Young WF Jr, Surks MI, et al. A model to determine workforce needs for endocrinologists in the united states until 2020*. Diabetes Care (2003) 26(5):1545–52. doi: 10.2337/diacare.26.5.1545
20. Vigersky RA, Fish L, Hogan P, Stewart A, Kutler S, Ladenson PW, et al. The clinical endocrinology workforce: Current status and future projections of supply and demand. J Clin Endocrinol Metab (2014) 99(9):3112–21. doi: 10.1210/jc.2014-2257
21. Garvey KC, Finkelstein JA, Zhang F, LeCates R, Laffel L, Wharam JF. Health care utilization trends across the transition period in a national cohort of adolescents and young adults with type 1 diabetes. Diabetes Care (2022) 22(8):1375–83. doi: 10.2337/dc22-0152
22. Wang H, Li N, Chivese T, Werfalli M, Sun H, Yuen L, et al. IDF diabetes atlas: Estimation of global and regional gestational diabetes mellitus prevalence for 2021 by international association of diabetes in pregnancy study group’s criteria. Diabetes Res Clin Pract (2022) 183:109050. doi: 10.1016/j.diabres.2021.109050
23. Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan L, et al. Incidence trends of type 1 and type 2 diabetes among youths, 2002–2012. N Engl J Med (2017) 376(15):1419–29. doi: 10.1056/NEJMoa1610187
24. Rogers MAM, Rogers BS, Basu T. Prevalence of type 1 diabetes among people aged 19 and younger in the united states. Prev Chronic Dis (2018) 15:180323. doi: 10.5888/pcd15.180323
25. Arora S, Geppert CMA, Kalishman S, Dion D, Pullara F, Bjeletich B, et al. Academic health center management of chronic diseases through knowledge networks: Project ECHO. Acad Med (2007) 82(2):10. doi: 10.1097/ACM.0b013e31802d8f68
26. Arora S, Kalishman S, Thornton K, Komaromy M, Katzman J, Struminger B, et al. (Project extension for community healthcare outcomes): A national and global model for continuing professional development. J Continuing Educ Health Professions. (2016) 36:S48. doi: 10.1097/CEH.0000000000000097
27. McBain RK, Sousa JL, Rose AJ, Baxi SM, Faherty LJ, Taplin C, et al. Impact of project ECHO models of medical tele-education: A systematic review. J Gen Intern Med (2019) 34(12):2842–57. doi: 10.1007/s11606-019-05291-1
28. Zhou C, Crawford A, Serhal E, Kurdyak P, Sockalingam S. The impact of project ECHO on participant and patient outcomes: A systematic review. Acad Med (2016) 91(10):1439–61. doi: 10.1097/ACM.0000000000001328
29. Zittleman L, Curcija K, Nease DE, Fisher M, Miriam Dickinson L, Thomas JF, et al. Increasing capacity for treatment of opioid use disorder in rural primary care practices. Ann Fam Med (2022) 20(1):18–23. doi: 10.1370/afm.2757
30. Bouchonville MF, Paul MM, Billings J, Kirk JB, Arora S. Taking telemedicine to the next level in diabetes population management: a review of the endo ECHO model. Curr Diabetes Rep (2016) 16(10):96. doi: 10.1007/s11892-016-0784-9
31. Bouchonville MF, Hager BW, Kirk JB, Qualls CR, Arora S. ENDO ECHO IMPROVES PRIMARY CARE PROVIDER AND COMMUNITY HEALTH WORKER SELF-EFFICACY IN COMPLEX DIABETES MANAGEMENT IN MEDICALLY UNDERSERVED COMMUNITIES. Endocr Pract (2018) 24(1):40–6. doi: 10.4158/EP-2017-0079
32. Blecker S, Lemieux E, Paul MM, Berry CA, Bouchonville MF, Arora S, et al. Impact of a primary care provider tele-mentoring and community health worker intervention on utilization in Medicaid patients with diabetes. Endocr Pract (2020) 26(10):1070–6. doi: 10.4158/EP-2019-0535
33. Salbach NM, Guilcher SJT, Jaglal SB, Davis DA. Factors influencing information seeking by physical therapists providing stroke management. Phys Ther (2009) 89(10):1039–50. doi: 10.2522/ptj.20090081
34. Olson KR, Caldwell A, Sihombing M, Guarino AJ, Nelson BD, Petersen R. Assessing self-efficacy of frontline providers to perform newborn resuscitation in a low-resource setting. Resuscitation (2015) 89:58–63. doi: 10.1016/j.resuscitation.2015.01.008
35. Hyman DJ, Maibach EW, Flora JA, Fortmann SP. Cholesterol treatment practices of primary care physicians. Public Health Rep (1992) 107(4):441–8.
36. Walker AF, Hood KK, Gurka MJ, Filipp SL, Anez-Zabala C, Cuttriss N, et al. Barriers to technology use and endocrinology care for underserved communities with type 1 diabetes. Diabetes Care (2021) 44(7):1480–90. doi: 10.2337/dc20-2753
37. Walker AF, Hu H, Cuttriss N, Anez-Zabala C, Yabut K, Haller MJ, et al. The neighborhood deprivation index and provider geocoding identify critical catchment areas for diabetes outreach. J Clin Endocrinol Metab (2020) 105(9):3069–75. doi: 10.1210/clinem/dgaa462
38. Walker AF, Addala A, Sheehan E, Lal R, Haller M, Cuttriss N, et al. Using peer power to reduce health disparities: Implementation of a diabetes support coach program in federally qualified health centers. Diabetes Spectr. (2022) 35(3):295–303. doi: 10.2337/dsi22-0004
39. American Diabetes Association Professional Practice Committee, American Diabetes Association Professional Practice Committee, Draznin B, Aroda VR, Bakris G, Benson G, et al. 14. children and adolescents: Standards of medical care in diabetes-2022. Diabetes Care (2022) 45(Suppl 1):S208–31. doi: 10.2337/dc22-S014
40. American Diabetes Association Professional Practice Committee, American Diabetes Association Professional Practice Committee, Draznin B, Aroda VR, Bakris G, Benson G, et al. Diabetes technology: Standards of medical care in diabetes-2022. Diabetes Care (2022) 45(Suppl 1):S97–112. doi: 10.2337/dc22-S007
41. American Diabetes Association Professional Practice Committee. Comprehensive medical evaluation and assessment of comorbidities: Standards of medical care in diabetes–2022. Diabetes Care (2021) 45(Supplement_1):S46–59. doi: 10.2337/dc22-S004
42. American Diabetes Association Professional Practice Committee. Facilitating behavior change and well-being to improve health outcomes: Standards of medical care in diabetes–2022. Diabetes Care (2021) 45(Supplement_1):S60–82. doi: 10.2337/dc22-S005
43. American Diabetes Association Professional Practice Committee. Glycemic targets: Standards of medical care in diabetes–2022. Diabetes Care (2021) 45(Supplement_1):S83–96. doi: 10.2337/dc22-S006
44. American Diabetes Association Professional Practice Committee. Pharmacologic approaches to glycemic treatment: Standards of medical care in diabetes–2022. Diabetes Care (2021) 45(Supplement_1):S125–43. doi: 10.2337/dc22-S009
45. Foster NC, Beck RW, Miller KM, Clements MA, Rickels MR, DiMeglio LA, et al. State of type 1 diabetes management and outcomes from the T1D exchange in 2016–2018. Diabetes Technol Ther (2019) 21(2):66–72. doi: 10.1089/dia.2018.0384
46. Addala A, Maahs DM, Scheinker D, Chertow S, Leverenz B, Prahalad P. Uninterrupted continuous glucose monitoring access is associated with a decrease in HbA1c in youth with type 1 diabetes and public insurance. Pediatr Diabetes. (2020) 21(7):1301–9. doi: 10.1111/pedi.13082
47. Anderson JE, Gavin JR, Kruger DF. Current eligibility requirements for CGM coverage are harmful, costly, and unjustified. Diabetes Technol Ther (2020) 22(3):169–73. doi: 10.1089/dia.2019.0303
48. Gajewska KA, Biesma R, Bennett K, Sreenan S. Barriers and facilitators to accessing insulin pump therapy by adults with type 1 diabetes mellitus: a qualitative study. Acta Diabetol (2021) 58(1):93–105. doi: 10.1007/s00592-020-01595-5
49. Naranjo D, Tanenbaum ML, Iturralde E, Hood KK. Diabetes technology: Uptake, outcomes, barriers, and the intersection with distress. J Diabetes Sci Technol (2016) 10(4):852–8. doi: 10.1177/1932296816650900
50. AAFP Health Maintenance and Counseling. Available at: https://www.aafp.org/pubs/afp/topics/by-topic.html.
Keywords: equity, primary care provider education, disparities, health, type 1 diabetes, tele-education
Citation: Addala A, Filipp SL, Figg LE, Anez-Zabala C, Lal RA, Gurka MJ, Haller MJ, Maahs DM, Walker AF and for the Project ECHO Diabetes Research Team (2022) Tele-education model for primary care providers to advance diabetes equity: Findings from Project ECHO Diabetes. Front. Endocrinol. 13:1066521. doi: 10.3389/fendo.2022.1066521
Received: 10 October 2022; Accepted: 29 November 2022;
Published: 16 December 2022.
Edited by:
Matt Bouchonville, University of New Mexico School of Medicine, United StatesReviewed by:
Anshu Gupta, Virginia Commonwealth University, United StatesCopyright © 2022 Addala, Filipp, Figg, Anez-Zabala, Lal, Gurka, Haller, Maahs, Walker and for the Project ECHO Diabetes Research Team. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ananta Addala, YWFkZGFsYUBzdGFuZm9yZC5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.