 Ziyan Xie
Ziyan Xie Xinhua Xiao
Xinhua Xiao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol., 25 November 2022
Sec. Clinical Diabetes
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1065856
This article is part of the Research TopicOcular Complications Associated with Diabetes MellitusView all 22 articles
The global burden due to microvascular complications in patients with diabetes mellitus persists and even increases alarmingly, the intervention and management are now encountering many difficulties and challenges. This paper reviews the recent advancement and progress in novel biomarkers, artificial intelligence technology, therapeutic agents and approaches of diabetic retinopathy and nephropathy, providing more insights into the management of microvascular complications.
Diabetes mellitus (DM) is a chronic metabolic disorder affecting more than 400 million people worldwide and is still on the rise. The long-standing hyperglycemia and genetic predisposition contribute to higher risks for macrovascular and microvascular complications among individuals with diabetes, which substantially places large financial and societal burden. Diabetic microvascular complications are associated with long term impairment and dysfunctions of various organs and systems including retina and kidney, which potentially result in blindness and end-stage kidney disorder, contributing significantly to the morbidity and mortality. These complications often already present in newly diagnosed diabetes and most patients may lost the opportunity to be diagnosed in the early stages to achieve clinically significant improvement. Therefore, early detection and novel treatment strategies are mandatory for alleviating progression and improving outcomes of microvascular complications. Nowadays, with the widely application of omics-technique, multiple novel biomarkers emerge as predictive and therapeutic targets for diabetic complications and increasing potential agents are in clinical trials or undergoing preclinical investigations. Furthermore, artificial intelligence (AI) is also developed and has been applicated in precision medicine, which facilitates the improvement of diagnosis and prognosis of microvascular complications. In this review, we highlighted the recent advances and new frontiers in the diagnosis and management of microvascular complications, especially focused on diabetic retinopathy (DR) and nephropathy (DN), providing perspectives on the clinical applications and implementation of novel biomarkers, diagnostic techniques and therapeutic agents.
DR remains the leading cause of visual impairment and blindness in working-age populations globally. Known risk factors including the duration of diabetes and poor glycemic control, however, cannot fully explain and predict the occurrence and progression of DR. And the present DR screening approaches all have different limitations such as poor accuracy, difficulty of obtaining high-quality images, invasive operation and high cost, which largely influence the early detection rate (1). Increasing evidence shows that pathological changes like inflammation and neuronal dysfunction may have occurred before retinal vasculature changes. Therefore, the development of a cost-effective biomarker that facilitates early risk assessment and accurate diagnosis is therefore urgently needed. The potential biomarkers of DR studied in recent years are listed in Table 1.

Table 1 Biomarkers for DR and DN.
Due to the indispensable role of inflammation in the pathogenesis of DR, close attention has been paid to inflammatory biomarkers for DR. A variety of clinical studies have provided evidence for the inflammatory biomarkers of DR. Multiple proinflammatory cytokines and adhesion molecules have been found increased in serum and ocular samples from both vitreous and aqueous humor of patients with DR, including interleukin family (IL-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-17), monocyte chemotactic protein-1 (MCP-1), tumor necrosis factor-α (TNF-α), interferon-γ (IFN-γ) and intercellular adhesion molecule-1 (ICAM-1), etc (2–5). And the level of IL-2, IL-5, IL-4, IL-6, IL-8, TNF-α, MCP-1 and macrophage inflammatory protein (MIP)-1α were significantly higher in early-onset proliferative diabetic retinopathy (PDR) patients compared to non-PDR (NPDR) and late-onset PDR, which facilitate evaluating the severity and predicting prognosis of DR in clinical practice (2, 6, 7). Besides, long pentraxin 3 (PTX3) has also been considered as a novel biomarker in DR. PTX3 is produced by endothelial cells in response to inflammation. Studies have shown elevated levels of PTX3 in the serum or aqueous humor of patients with DR compared with non-retinopathy or non-diabetic controls (9). Recently, King et al. recognized retinol-binding protein 3 (RBP3) as a potential biomarker for DR severity and progression. The level of RBP3 in aqueous humor was found to be reduced from mild NPDR, moderate and severe NPDR to PDR patients gradually (10). Elevated RBP3 level in the vitreous was correlated with lower levels of TNF-α, TNF-β and VEGF were associated with a lower risk of PDR (11).
Recent preclinical experiments also have gained progress in identification of potential biomarkers further used in DR detection and diagnosis. The main characteristics of inflammatory response in DR includes infiltration of immune cells such as macrophages, neutrophils, B and T cells, activation of microglia and enrichment of cytokines and chemokines (50, 51). Under normal condition, there is generally no immune cells within the vitreous body (52). However, in DR, which the blood-retinal barrier is disrupted, multiple immune cells (leukocytes and T, B cells) will enter the vitreous and trigger inflammatory reactions (53). Therefore, some immune cells and their related genes have been reported to be associated with DR, which may act as inflammatory biomarkers. Bioinformatics analysis identified 8 CD8+T lymphocytes-related genes linked to the occurrence and progress of diabetic macular edema (DME) in human macular samples and verified the expressions in DR mouse model (54). Similarly, hub genes of T-helper 17 (Th17) cells gained good diagnostic values in distinguishing PDR patients from normal subjects with the predictive role of the DR progression (NPDR and DME) (55). Furthermore, evidence have shown that inflammatory mediators initially rise in the retina and then enter the vitreous (12), implying the early predictive role of biomarkers in retina. Several monocyte/macrophage markers (e.g.,F4/80mRNA, CCL2) and glial cells markers (e.g.,NF-κB, IL-17) in retina are found correlated with the progression of DR in rat models (8), which need further confirmation in clinical practice.
Angiogenesis is an critical pathological factor in the occurrence and progression of DR. Vascular endothelial growth factor (VEGF) is the main angiogenic regulator which serves as a promising predictive biomarker and target for the treatment of DR. Accumulating evidence has suggested the circulating or even tear’s level of VEGF, significantly increased in PDR compared with NPDR, which predict DR severity (13). Clinical studies indicate that serum VEGF-A, VEGF-C, VEGF-D and placental growth factor (PlGF), and vitreous and aqueous VEGF-A and PlGF are positively correlated with the severity of DR and are strong predictors for DR occurrence in diabetic individuals (12, 14). And anti-VEGF injection in PDR patients significantly reduced the levels of VEGF-A in aqueous, which suggests the potential role of aqueous VEGF in evaluating the efficacy of PDR therapies (12). Besides, circulating angiopoietin-like 3 (ANGPTL3) is also considered as a promising biomarker which independently and strongly associated with DR onset and development (15). Moreover, recent studies revealed more candidate angiogenic factors like ITGA7, FGF23, THBS1, COL1A1, MAPK13, and AIF1 in early stage of DR (56), which may be novel intervention targets. Exploring the mechanisms of angiogenesis also could facilitate early recognition of DR.
In recent years, extracellular vesicles (EVs) have gained increasingly attention as potential sources of new biomarkers for multiple diseases. According to their size and biogenesis, EVs can be classified as exosomes, microvesicles, or apoptotic bodies. It was found that hyperglycemia leads to the increase of EVs from donor cell. The molecular profiles and origins of EVs are distinct between DR and normal, presenting proinflammatory and proangiogenic properties. 90 proteins in the proteomic profiles of plasma EVs significantly changed between DR and non-DR subjects, among them, tumor necrosis factor-α-induced protein 8 (TNFAIP8) was increased in DR patients (16). In vitro experiment confirmed the angiogenic role of TNFAIP8 in retinal microvascular endothelial cell, indicating that TNFAIP8 in plasma EVs may act as a new biomarker for DR (16). Aleksandra et al. have described that the plasma level of microvesicles containing RANTES and CCR5 receptors, which both act as inflammatory and proangiogenic factors, were significantly higher in NPDR than diabetic patients without DR, and were positively associated with the progression of DR (17). Furthermore, Ogata et al. have reported gradually elevated levels of platelet- and monocyte-derived EVs in the early and advanced stage of DR (18, 19). These platelet-derived EVs induce oxidative stress and monocyte-derived EVs exaggerate inflammatory responses, leading to retinal vascular damages during the development of DR. Therefore, circulating EVs as carriers of proteins and RNAs, are not only the messengers for cell-cell communications, but serve as important biomarkers for prediction of disease occurrence and progression.
Plasma lipid parameters not only predict cardiovascular outcomes but also act as markers for microvascular complications. Serum total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) are found significantly elevated in DR patients, acting as risk factors for the presence of DR. Besides, the atherogenic plasma index calculated as (LDL-C/HDL-C) and atherogenic index calculated as (TC-(HDL-C))/HDL-C also possess great values in predicting the onset and severity of DR compared with the traditional lipid indexes (14). Apolipoprotein (apo) profiles in non-DR, NPDR and PDR subjects revealed a panel of apos as independent risk factors for the occurrence and severity of DR and two apos as protective factors, which could be further used as biomarkers for predicting DR (20). Additionally, some lipid parameter has also been suggested to guide treatment of DR. For example, small dense low-density lipoprotein cholesterol (sdLDL-C) was identified as a sensitive biomarker for evaluating the need of laser treatment for DR patients (21).
Development of high-throughput sequencing techniques allows the detection and quantification of the overall and dynamic changes in genome, transcriptome, proteome and metabolome, which produce a large amount of date in a short time and provide insight in identification of novel biomarkers (57). A recent metabolomics study observed a serum metabolites panel associated with DR occurrence and development. Serum 12-hydroxyeicosatetraenoic acid and 2-piperidone exhibited better diagnostic value than hemoglobin A1c (HbA1c) in differentiating DR from non-DR diabetes, which can be used for detection of early-stage DR (22). Besides, proteomics analysis from tears of DR patients uncovered multiple proteins changed correlating with the occurrence and severity of DR, providing evidence and targets for tear-based protein biomarkers for early diagnosis of DR (23). Furthermore, non-coding RNAs, especially microRNAs, are also the most well-studied biomarkers of DR (8). MicroRNAs have been shown to regulate multiple pathological processes during DR, including cell proliferation, apoptosis, inflammation and microcirculation impairments and exerted differential expressions in blood and vitreous samples from DR patients (24, 58). Therefore, microRNAs may act as promising biomarkers for early diagnosis and progression of DR.
Diagnosis and monitoring the progression of DR heavily reliance on imaging, artificial intelligence (AI) has been a pioneer in the early detection and screening of DR. Based on the rich data generated by imaging techniques, using machine learning and deep learning, AI is now being applied in facilitating the early recognition, prognosis and treatment selection. Pivotal studies have demonstrated the clinical benefits of AI system for detection and screening of DR. A prospective multicenter study evaluated the efficacy of the AI DR detection system (EyeArt) in detecting more-than-mild DR and vision-threatening DR (59). The findings found high sensitivity and specificity of the AI system in detecting more-than-mild DR (95.5% and 85%, respectively) and even vision-threatening DR (95.1% and 89%), without physician assistance. Dai et al. (60) developed DeepDR system based on deep learning method, which can automatically detect the whole course of DR from mild to PDR, providing real-time feedback to the quality of fundus images as well as the recognition and segmentation of fundus diseases. Furthermore, AI techniques have also been used in DR prognosis and treatment efficacy judgement. A prospective study evaluated the potential of AI using optical coherence tomography data including segmentation of intraretinal cystoid fluid (IRC), retinal layer segmentation and subretinal fluid, to predict the prognosis of patients with DME. The findings showed that IRC possessed the greatest predictive value for best-corrected visual acuity (BCVA) at baseline, while IRC and total retinal thickness had greater prognostic value for BCVA after 4 and 12 weeks. The application of AI transforms descriptive data into information and factors that can be used for prediction. The establishment of predictive models for the prognosis will encourage patients to pursue aggressive treatment and make optimal treatment options (61). Early detection is critical for DR management and reducing the blindness rate of DR. However, current DR screening faces the dilemma of insufficient ophthalmologists for standardized image reading and lack of awareness for DR screening. AI with the characteristics of high accuracy, easy to copy and promote, is promising to make up for staff shortages and facilitate early screening, intelligent fundus reading and intelligent diagnosis of DR in clinical practice. Until now, both the EyeArt and DeepDR systems have been approved for clinical practice. Similarly, other AI systems like IDx-DR (62), RetmarkerDR (63), Singapore SERI-NUS (64) and so on, also obtain good results in DR screening in different populations.
Treatment for DR generally includes systemic control, laser photocoagulation, and pharmacotherapies targeting mediators involved in pathogenesis of DR. The recent progress of therapeutic research in DR continues the previous academic concerns including anti-VEGF therapy, anti-inflammatory treatment, traditional Chinese medicine, and precision drug delivery, etc.
Approved in 2013 by US FDA, Anti-VEGF drugs are currently the first line therapy of DME with vision loss. Several studies, such as RESTORE (65), VISTA and VIVID (66) study have shown that the emergence of anti-VEGF therapy led to significant clinical improvements compared to laser therapy alone. Besides, a recent randomized clinical trial observed that combination of intravitreal bevacizumab injections and laser photocoagulation was more effective in preventing neovascularization and ameliorating visual field than pan-retinal photocoagulation (PRP) or bevacizumab alone in PDR patients (67). The combined protocol reduced the adverse effects of full PRP and need fewer injections and visits, suggesting that for some high-risk patients, anti-VEGF combined with PRP therapy may be more helpful in delaying the progression and improving the adherence of injections in DR. Furthermore, PANORAMA study found that anti-VEGF therapy also improve NPDR without DME (68). Compared with sham, intravitreal aflibercept significantly improved retinopathy severity scale and reduced vision-threatening adverse effects in moderately severe to severe NPDR. Though anti-VEGF therapy have gained benefit in clinical trials, frequent injections, close monitoring and heterogeneous response of patients are current barriers to achieve optimal outcomes in real world. Recently, long-acting and slow-release anti-VEGF agents have shown benefits in clinical trials. KESTREL and KITE study demonstrated that brolucizumab, a new agent targeting VEGF-A and facilitating high and sustained molar concentration, improved BCVA and reduced central subfield thickness (CSFT), subretinal and/or intraretinal fluid in DME patients during 52 weeks therapy (69). Additionally, Abicipar pegol, a VEGF-A inhibitor with longer half-life and higher affinity than ranibizumab, has also shown functional and anatomical improvements with fewer injections compared with ranibizumab administered every 4 weeks over a period of 28 weeks in DME patients (70). Alternatively, the port delivery system for anti-VEGF drugs also allows long-term, continuous delivery of ranibizumab into the vitreous, which maintains optimal vision and anatomic outcomes with reduced number of injections and gains high treatment satisfaction from patients (71, 72). This technology is now applied in patients with neovascular age-related macular degeneration in clinical trial stage and is expected to be further used in the treatment of DME. New agents beyond the VEGF pathway are also developed to optimize the efficacy and compliance of DR treatment. Faricimab is a novel antibody inhibiting angiopoietin2 (ANGPT2) and VEGF-A with high affinity and specificity. Two phase III trials indicated that faricimab administration achieved vision gains and improved anatomical outcomes with fewer visits and increased dosing compared with aflibercept in DME treatment (73). Furthermore, gene therapy is of great interest in the treatment of DR. RGX-314 uses the NAV AAV8 vector to deliver anti-VEGF monoclonal antibody fragment and is promising to maintain continuous expression of anti-VEGF-A protein in retina with a single administration (74). And an ongoing phase II clinical trial (ALTITUDE) is now conducted to evaluate the safety, tolerance and efficacy of RGX-314 in patients with moderate to severe NPDR and mild PDR. Further research is still needed to determine the safety, efficacy, durability and targeted population of gene therapy prior to implementing into clinical practice. Anti-VEGF agents targeting DR are summarized in Table 2.
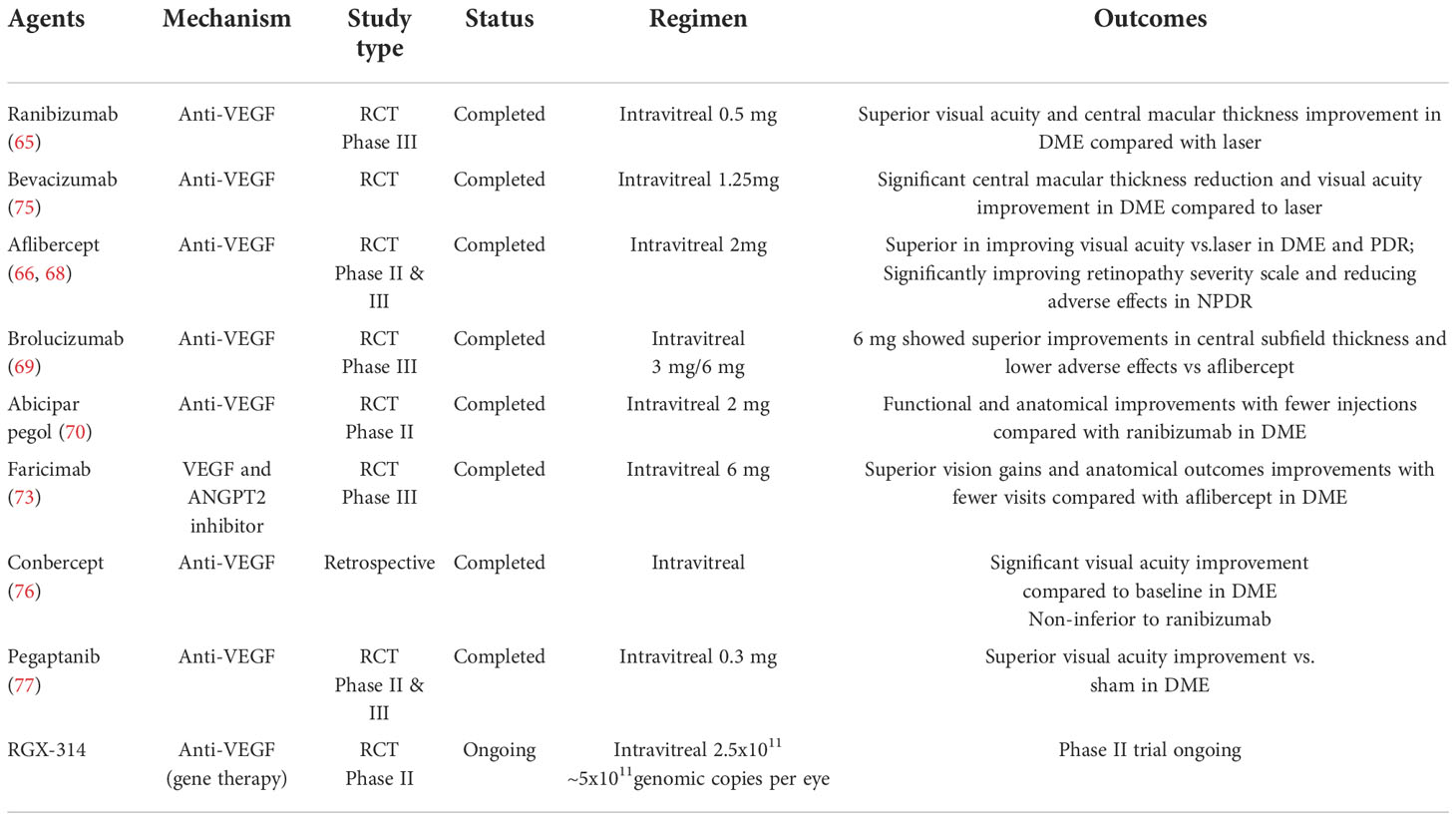
Table 2 Anti-VEGF agents for treatment of DR.
Inflammation plays a critical role in the pathogenesis of DR, and anti-inflammatory agents have shown functional and anatomical improvement in DR and DME. Clinical studies demonstrated that the visual outcomes of intravitreal dexamethasone injection were comparable with the anti-VEGF group after 1 year (78). DR patients who did not respond to anti-VEGF drugs, switching to dexamethasone sustained-release therapy may still reduce macular edema and improve vision (79). In vitro experiments implied that dexamethasone reduced the level of cytokines, including IL-1β, IL-6, and TNF-α in retinal ganglion cell and Müller cells, which alleviated hyperglycemia induced inflammation and improved cell survival rate (80). In addition to glucocorticoids, key inflammatory factors can be used as new targets for DR treatment. CD40 is a critical driver of DR which induces proinflammatory cytokines release in myeloid cells, and treatment blocking CD40 signaling decreased the level of inflammatory molecules in retina of diabetic mice, providing evidence for the potential of CD40 in DR treatment (81). Moreover, nuclear factor of activated T cells (NFAT) and RBP3 are also important biomarkers involved in retinal inflammation. Inhibition of NFAT prevented retinal vascular leakage and inflammation in DR mice model; while intravitreal injection of recombinant human RBP3 reversed high glucose induced retinal vascular dysfunction and inflammatory cytokine elevations in STZ rats. The role of these inflammatory biomarkers in the progression of DR needs further research, and they are expected to become novel targets in pharmacotherapeutics.
RAAS activation potentially has a role in the development of end-organ damage, and has been considered as a risk factor for DR. Activation of the angiotensin receptor 1 (AT1-R) induces the progression of DR by stimulating multiple pathways involved in the pathogenesis including advanced glycosylation end-products (AGE) accumulation, inflammation, oxidative stress, and several crucial mediators of angiogenesis such as VEGF (82). Clinical and animal experiments showed that the RAAS is activated in diabetic retinopathy and its inhibitors may exert protective role against retinal damage (83, 84). Several clinical trials indicated that ACE inhibitors and/or ARBs treatments reduced the incidence of DR in hypertensive diabetic people (85–87). However, there also exists studies that showed no benefit in DR incidence or DR progression from the ACE inhibitor and ARB therapy (85, 88), which indicates that mechanism other than RAAS also responsible for the progression of DR, and further research working on the efficacy of RAAS inhibitor to prevent the progression of DR in diabetic people are still needed.
Recently, nanotechnology has been widely applied in the medical field, broaden the horizon of new drug discovery, drug delivery and precision treatment. The diameter of nanomolecules ranges from 1 to 100 nanometers, enabling the drugs pass through the blood-retinal barrier. Nanoparticle-based delivery of triamcinolone acetonide are safe and long-lasting and significantly improved anatomic outcome and functional activity of retina in DR rat model (89). In addition, multiple micro RNAs (miRNA) and DNAs can also be delivered by nanomaterials, which are expected to delay DR progress and promote retinal regeneration.
Early recognition of DN is key to preventing renal function reduction, however, biomarkers currently used in clinical practice such as albumin, creatinine and eGFR do not sufficiently predict and assess the progression of DN (90). Therefore, novel biomarkers to predict the risk of functional decline have been urgently sought. In recent years, multiple efforts have been made to identify new reliable and sensitive biomarkers for the early diagnosis and monitoring of DN (Table 1).
Several biomarkers indicating kidney injury are being developed (34). Neutrophil gelatinase-associated lipocalin (NGAL) is a well-studied tubular damage marker. DN patients with normo-albuminuria have present increased levels of urinary NGAL, which implies that tubular damage may occur in very early stages (30–32). Besides, kidney injury molecule 1 (KIM-1) and β-2-Microglobulin (B2M) have also been extensively studied in DN. Longitudinal studies indicated that high level of KIM-1 had a strong correlation with higher risk of eGFR decline and increased risk of DKD (43, 91). Evidence also showed that diabetic individuals with elevated B2M levels had a higher risk for DN, which may serve as promising predictors of DN progression in diabetic patients (35). ANGPT are vascular growth factors that promote angiogenesis and vascular repair and play a crucial role in the glomerular capillaries (36). Elevated level of urinary ANGPT2 was found in T2D patients with renal damage and was associated with albuminuria (36). Inversely, ANGPT1 has exerted a protective effect against renal function decline and reduced level of ANGPT1 was detected in early diabetic kidney disease (37). Other growth factors such as VEGF and fibroblast growth factor (FGF) have also been previously evaluated as important biomarkers and targets in DN diagnosis and progression (38, 39). Furthermore, recent studies illustrated that serum cystatin C, another marker of tubular damage, shows better predicting value of eGFR decline in diabetes patients than creatinine (33).
Markers involved in inflammation are also highly reported (34). Chemokines such as CCL19,CCL5 and CCL15 have been identified as critical genes of DN. Bioinformatics analysis and in vitro experiments revealed that CCL19 was significantly upregulated in tubular samples of DN patients (40). Besides, urinary level of CCL5 was correlated with renal function reducing and the extent of renal interstitial fibrosis (41). While serum CCL15 is found negatively correlated with eGFR and independently associated with high DN risk in T2D patients (42). In addition, prospective studies reported that diabetic patients with higher plasma levels of TNFR1, TNFR2 and MCP1 had increased risk of progression of DN (43). On the other hand, some anti-inflammatory markers have also been studied in DN. Klotho protein mainly expressed in the kidney and can suppress the inflammatory response. A recent meta-analysis found that the soluble Klotho was significantly lower in DN than that in control, and this decrease can be detected in the early stages of DN (44). Lutein is an oxygenated carotenoid with antioxidation and anti-inflammatory effects. Serum lutein level is negatively associated with the risk of DN and possesses a good diagnostic value of DN with an AUC of 0.779 (45).
The urinary proteomic CKD273 score was used to quantify the risk for the new onset of albuminuria. CKD-273 was validated in T2D cohorts and shown to predict the progression of albuminuria in DN (46, 47). Besides, metabolomics of urine samples from 2670 T1D individuals revealed five urinary metabolites closely associated with kidney disease progressing, and the level of 2-hydroxyisobutyrate reflected the progression of DN in individuals with normo-albuminuria (48). Urinary or serum miRNAs also emerge as new biomarkers for DN depending on the microarray and RNA-sequencing techniques (49).
The current therapy for DN including glycemic control, blood pressure and cholesterol management, focus on the systematic control of DR. As the emergence of abundant targets involved in DN, the direction of DN treatment investigation has been progressed to focus on molecular mechanism and target the critical molecules or signaling pathways in the progression of DN.
Pentoxifylline (PTF) is a methylxanthine derivate and plays an anti-inflammatory role in kidney disorder progression. An early meta-analysis summarized that PTF may reduce proteinuria in patients with DN (92). The PREDIAN Trial and a recent randomized clinical trial both confirmed that the addition of PTF to renin-angiotensin system antagonists resulted in a more significant reduction of urine albumin excretion and slowed the progression of renal function decline (93, 94). Besides, some chemokine antagonists also exert beneficial effects in clinical studies. CCX140-B, a selective MCP-1 inhibitor, significantly reduced albuminuria by 18% in DN patients (95). A phase II study in T2D patients with albuminuria demonstrated that emapticap pegol (NOX-E36), another antagonist of MCP-1, was safe and well tolerated during administration, and significantly improved urinary albumin/creatinine ratio (ACR) compared to the placebo group (96). Klotho could inhibit the expression of MCP-1 and ICAM-1, resulting in lower accumulation of macrophages, thus exerting anti-inflammatory function and reduced tubulointerstitial injury (97).
Some agents have been found to target renal cell function for anti-fibrotic effect in DN. Oxymatrine prevented renal extracellular matrix deposition by inhibiting the epithelial-to-mesenchymal transition (EMT) process and ultimately attenuated tubulointerstitial fibrosis (98). The extract of P. fallax has been demonstrated to downregulate the expression of ECM proteins, such as FN, Col IV, MMP-9, and MMP-2, therefore protecting glomerular mesangial cell from high glucose induced fibrosis (99).
The RAAS plays an important role in renal disease. In DN, the RAAS has been linked with changes in intraglomerular hemodynamics as well as structural alterations in both the glomerulus and tubulointerstitium (100). Growing evidence has revealed that RAAS inhibitors blocked the development of kidney diseases, manifesting as improved proteinuria and well-maintained renal function (101). It has been shown that ACEI or ARB which block the RAAS delayed the development of DN and reduced the incidence of end-stage renal disease in DN patients with large albuminuria (102).
Recently, the emergence of novel anti-diabetic drugs not only improve the management of hyperglycemia, but also obtain heart and kidney benefits. SGLT2 inhibitors are oral hypoglycemic drugs and exhibit renoprotective effects. Studies demonstrated that SGLT2 inhibitors therapy decreased albuminuria, prevented GFR decline, and reduced need for renal replacement therapy or death from kidney causes in diabetes patients (103, 104). Besides, data suggested DPP-4 inhibitors and GLP-1 agonists also have renoprotective effect in diabetic patients through antioxidant, anti-inflammatory and antifibrotic mechanisms, which prevent DN occurrence and development (105, 106).
Endothelin (ET) is a kind of vasoconstrictor which has vasoactive, inflammatory, and profibrogenic characters and is significantly correlated with kidney disorders. Animal experiments suggested that ET receptor antagonists reduced proteinuria and exerted nephroprotective effect in experimental models of DN (107). Phase III clinical trials also showed that ET receptor antagonists decreased albuminuria in patients with DN (108). However, the safety and side effects (congestive heart failure) of ET receptor blockers require further investigation.
Some clinical trials and observational studies have supported the benefits of vitamin D supplementation in DN treatment. A randomized control study revealed that paricalcitol decreased urinary albumin excretion rate by 18% in T1D patients compared to placebo (109). Similarly, an observational study also showed that oral cholecalciferol therapy for 4 months significantly reduced the albuminuria in T2D patients (110). A meta-analysis including 20 randomized clinical trials with total 1464 DN patients suggested that vitamin D supplement (calcitriol, alfacalcidol and vitamin D3) improved 24-hour urine protein and urine albumin excretion rate, as well as inflammatory indexes, such as hs-CRP, TNF-α and IL-6 (111). But there was no significant difference in serum creatine, eGFR or HbA1c. Therefore, more trials are needed to confirm the therapeutic value of vitamin D supplementation in DN for reaching a consensus and recommendation.
Recent research assembled synthetic high-density lipoprotein (sHDL) with a liver X receptor (LXR) agonist, which aim to deliver LXR agonists to kidney and promote the removal of excessive lipids from mesangial cells, thus attenuating inflammation and recovering renal function, and the efficacy of sHDL nanoparticle has been confirmed in DN animal experiments (112).
DR and DN are both major microvascular complications of diabetes. DR is the leading cause of blindness in adults aged 20-74 years, with almost all type 1 diabetes and 60% of type 2 diabetes occurring after 20 years. DN is one of the major causes of end stage renal disease (ESRD), contributing to significant morbidity and cardiovascular mortality (113). The connection between DR and DN can be addressed in many aspects. Firstly, these two complications share common pathogenetic mechanisms (114). The main biological mechanisms of microvascular complications include advanced glycation end products (AGEs) accumulation, polyol pathway activation, oxidative stress, inflammatory responses (e.g., activation of NF-kB, adipokines, chemokines, adhesion molecules and proinflammatory cytokines), hemodynamic alterations (e.g., RAAS activation) and growth factors overexpression (e.g., VEGF is one of the most important factors in the progression of DR and DN). Secondly, the similar underlying pathogenetic mechanisms contribute to the overlap of biomarkers for predicting the progress of DR and DN. As we discussed previously, DR and DN share many common biomarkers, such as inflammatory biomarkers, angiogenetic biomarkers, and lipid profiles. Therefore, combination of these biomarkers could facilitate detecting early disease affecting both systems, and therapeutic strategies targeting their common markers may also gain retinal and renal benefits. Moreover, DR and DN have a predictive effect on each other. Accumulating evidence suggested that the presence of DR increased the incidence of DN in diabetic patients and DR has been considered as the predictor of DN, especially PDR as a more sensitive predictor (115, 116). Yang et al. (117) found that haptoglobin, a urine proteome specific for PDR could serve as an indicator complementing to urine albumin to predict renal dysfunction in patients with T2D. Likewise, DN can also predict DR to some extent. A prospective ten-year follow-up study demonstrated that eGFR and ratio of urine albumin to creatinine (ACR) served as sensitive biomarkers to predict the incidence of DR (118). And serum creatinine and decreased eGFR has been shown to be associated with the progression and severity of DR in diabetic patients (119, 120). Although the onset of retinopathy symptoms is very hidden, with the development of fundus examination and AI, accurate and early recognition of DR gains clinical feasibility. However, the early stage of DN lacks specific clinical symptoms and requires kidney biopsy to confirm the diagnosis, which is the greatest challenge for clinical promotion. Microalbuminuria, the most used indicator, however, its accuracy remains controversial. Therefore, considering the close link between DR and DN, it is promising to replace invasive and unpredictable detection of other microvascular complications with noninvasive, simple, and low-cost ophthalmoscopy. And vice versa, it also useful to screen patients with kidney disorders for associated retinal diseases. Comprehensive clinical evaluation in patients with CKD or ESRD should include external ophthalmoscopy and direct ophthalmoscopy. These recommendations may facilitate early recognition of both retinal and renal damages in diabetic patients and provide evidence for multi-factorial approach and potential multi-target therapeutic strategies.
In conclusion, sensitive and cost-effective biomarkers facilitating early identification guarantees optimal treatment of DM related microvascular complications. Multi-omics techniques provide huge data for candidate biomarker discovery, however, most of them remains further confirmation in clinical practice. The application of AI technology may also be expected to achieve effective diagnosis, efficacy determination, and prognosis of microvascular complications. Furthermore, in view of the close association between DR and DN, biomarkers and therapeutic strategies targeting their common pathophysiology mechanism such as VEGF and inflammation are key research directions in the future. Novel agents targeting multifactor which will complement current therapies in effects, such as SGLT-2 inhibitor and DPP-4 inhibitor, etc., are expected to benefit more patients. Finally, nanotechnology have shown incomparable benefits in non-invasive and precise drugs delivery. The application of nanomaterial-based drug delivery systems in microvascular complications therapy is of great potential and interests.
Manuscript drafted by ZX, edited and revised by XX. All authors contributed to the article and approved the submitted version.
This work was supported by the grants from the National Natural Science Foundation of China (No. 82170854, 81870579, 81870545, 81570715, 81170736) and National High Level Hospital Clinical Research Funding (2022-PUMCH-C-019).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Jampol LM, Glassman AR, Sun J. Evaluation and care of patients with diabetic retinopathy. N Engl J Med (2020) 382(17):1629–37. doi: 10.1056/NEJMra1909637
2. Wu H, Hwang D-K, Song X, Tao Y. Association between aqueous cytokines and diabetic retinopathy stage. J Ophthalmol (2017) 2017:9402198. doi: 10.1155/2017/9402198
3. Yan A, Zhang Y, Wang X, Cui Y, Tan W. Interleukin 35 regulates interleukin 17 expression and T helper 17 in patients with proliferative diabetic retinopathy. Bioengineered. (2022) 13(5):13293–9. doi: 10.1080/21655979.2022.2080367
4. Wu G, Liu B, Wu Q, Tang C, Du Z, Fang Y, et al. Correlations between different angiogenic and inflammatory factors in vitreous fluid of eyes with proliferative diabetic retinopathy. Front In Med (2021) 8:727407. doi: 10.3389/fmed.2021.727407
5. Mason RH, Minaker SA, Lahaie Luna G, Bapat P, Farahvash A, Garg A, et al. Changes in aqueous and vitreous inflammatory cytokine levels in proliferative diabetic retinopathy: a systematic review and meta-analysis. Eye (London England) (2022). doi: 10.1038/s41433-022-02127-x
6. Ke D, Hong Y, Jiang X, Sun X. Clinical features and vitreous biomarkers of early-onset type 2 diabetes mellitus complicated with proliferative diabetic retinopathy. Diabetes Metab Syndr Obes (2022) 15:1293–303. doi: 10.2147/DMSO.S362074
7. Amil-Bangsa NH, Mohd-Ali B, Ishak B, Abdul-Aziz CNN, Ngah NF, Hashim H, et al. Total protein concentration and tumor necrosis factor α in tears of nonproliferative diabetic retinopathy. Optom Vis Sci (2019) 96(12):934–9. doi: 10.1097/OPX.0000000000001456
8. Ren J, Zhang S, Pan Y, Jin M, Li J, Luo Y, et al. Diabetic retinopathy: Involved cells, biomarkers, and treatments. Front In Pharmacol (2022) 13:953691. doi: 10.3389/fphar.2022.953691
9. Stravalaci M, Ferrara M, Pathak V, Davi F, Bottazzi B, Mantovani A, et al. The long pentraxin PTX3 as a new biomarker and pharmacological target in age-related macular degeneration and diabetic retinopathy. Front In Pharmacol (2021) 12:811344. doi: 10.3389/fphar.2021.811344
10. Yokomizo H, Maeda Y, Park K, Clermont AC, Hernandez SL, Fickweiler W, et al. Retinol binding protein 3 is increased in the retina of patients with diabetes resistant to diabetic retinopathy. Sci Transl Med (2019) 11(499):eaau6627. doi: 10.1126/scitranslmed.aau6627
11. Fickweiler W, Park H, Park K, Mitzner MG, Chokshi T, Boumenna T, et al. Elevated retinol binding protein 3 concentrations are associated with decreased vitreous inflammatory cytokines, VEGF, and progression of diabetic retinopathy. Diabetes Care (2022) 45(9):2159–62. doi: 10.2337/dc22-0165
12. Wu F, Phone A, Lamy R, Ma D, Laotaweerungsawat S, Chen Y, et al. Correlation of aqueous, vitreous, and plasma cytokine levels in patients with proliferative diabetic retinopathy. Invest Ophthalmol Visual Sci (2020) 61(2):26. doi: 10.1167/iovs.61.2.26
13. Ang WJ, Zunaina E, Norfadzillah AJ, Raja-Norliza RO, Julieana M, Ab-Hamid SA, et al. Evaluation of vascular endothelial growth factor levels in tears and serum among diabetic patients. PloS One (2019) 14(8):e0221481. doi: 10.1371/journal.pone.0221481
14. Zhang X, Qiu B, Wang Q, Sivaprasad S, Wang Y, Zhao L, et al. Dysregulated serum lipid metabolism promotes the occurrence and development of diabetic retinopathy associated with upregulated circulating levels of VEGF-a, VEGF-d, and PlGF. Front Med (Lausanne) (2021) 8:779413. doi: 10.3389/fmed.2021.779413
15. Yu C-G, Yuan S-S, Yang L-Y, Ke J, Zhang L-J, Lang J-N, et al. Angiopoietin-like 3 is a potential biomarker for retinopathy in type 2 diabetic patients. Am J Ophthalmol (2018) 191:34–41. doi: 10.1016/j.ajo.2018.03.040
16. Xiao J, Zhang H, Yang F, Xiao M, Zhou L, Yu R, et al. Proteomic analysis of plasma sEVs reveals that TNFAIP8 is a new biomarker of cell proliferation in diabetic retinopathy. J Proteome Res (2021) 20(3):1770–82. doi: 10.1021/acs.jproteome.0c01048
17. Tokarz A, Konkolewska M, Kuśnierz-Cabala B, Maziarz B, Hanarz PŻurakowski A, Szuścik I, Stępień EŁ. Retinopathy severity correlates with RANTES concentrations and CCR 5-positive microvesicles in diabetes. Folia Med Cracov (2019) 59(3):95–112. doi: 10.24425/fmc.2019.131139
18. Ogata N, Imaizumi M, Nomura S, Shozu A, Arichi M, Matsuoka M, et al. Increased levels of platelet-derived microparticles in patients with diabetic retinopathy. Diabetes Res Clin Practice (2005) 68(3):193–201. doi: 10.1016/j.diabres.2004.10.010
19. Ogata N, Nomura S, Shouzu A, Imaizumi M, Arichi M, Matsumura M. Elevation of monocyte-derived microparticles in patients with diabetic retinopathy. Diabetes Res Clin Practice (2006) 73(3):241–8. doi: 10.1016/j.diabres.2006.01.014
20. Zhang X, Nie Y, Gong Z, Zhu M, Qiu B, Wang Q. Plasma apolipoproteins predicting the occurrence and severity of diabetic retinopathy in patients with type 2 diabetes mellitus. Front Endocrinol (Lausanne) (2022) 13:915575. doi: 10.3389/fendo.2022.915575
21. Nakayama A, Morita H, Sato T, Kawahara T, Takeda N, Kato S, et al. Small dense low-density lipoprotein cholesterol is a potential marker for predicting laser treatment for retinopathy in diabetic patients. J Atheroscler Thromb (2022) 29(5):678–91. doi: 10.5551/jat.62889
22. Xuan Q, Ouyang Y, Wang Y, Wu L, Li H, Luo Y, et al. Multiplatform metabolomics reveals novel serum metabolite biomarkers in diabetic retinopathy subjects. Adv Sci (Weinh) (2020) 7(22):2001714. doi: 10.1002/advs.202001714
23. Nandi SK, Singh D, Upadhay J, Gupta N, Dhiman N, Mittal SK, et al. Identification of tear-based protein and non-protein biomarkers: Its application in diagnosis of human diseases using biosensors. Int J Biol Macromol (2021) 193(Pt A):838–46. doi: 10.1016/j.ijbiomac.2021.10.198
24. Grieco GE, Sebastiani G, Eandi CM, Neri G, Nigi L, Brusco N, et al. MicroRNA expression in the aqueous humor of patients with diabetic macular edema. Int J Mol Sci (2020) 21(19):7328. doi: 10.3390/ijms21197328
25. Liu Y, Yang Q, Fu H, Wang J, Yuan S, Li X, et al. Müller glia-derived exosomal miR-9-3p promotes angiogenesis by restricting sphingosine-1-phosphate receptor S1P in diabetic retinopathy. Mol Ther Nucleic Acids (2022) 27:491–504. doi: 10.1016/j.omtn.2021.12.019
26. Yu B, Xiao M, Yang F, Xiao J, Zhang H, Su L, et al. MicroRNA-431-5p encapsulated in serum extracellular vesicles as a biomarker for proliferative diabetic retinopathy. Int J Biochem Cell Biol (2021) 135:105975. doi: 10.1016/j.biocel.2021.105975
27. Barutta F, Corbetta B, Bellini S, Guarrera S, Matullo G, Scandella M, et al. MicroRNA 146a is associated with diabetic complications in type 1 diabetic patients from the EURODIAB PCS. J Trans Med (2021) 19(1):475. doi: 10.1186/s12967-021-03142-4
28. Helal HG, Rashed MH, Abdullah OA, Salem TI, Daifalla A. MicroRNAs (-146a, -21 and -34a) are diagnostic and prognostic biomarkers for diabetic retinopathy. BioMed J (2021) 44(6 Suppl 2):S242–S51. doi: 10.1016/j.bj.2020.11.003
29. Solis-Vivanco A, Santamaría-Olmedo M, Rodríguez-Juárez D, Valdés-Flores M, González-Castor C, Velázquez-Cruz R, et al. miR-145, miR-92a and miR-375 show differential expression in serum from patients with diabetic retinopathies. Diagnostics (Basel) (2022) 12(10):2275. doi: 10.3390/diagnostics12102275
30. Yürük Yıldırım Z, Nayır A, Yılmaz A, Gedikbaşı A, Bundak R. Neutrophil gelatinase-associated lipocalin as an early sign of diabetic kidney injury in children. J Clin Res Pediatr Endocrinol (2015) 7(4):274–9. doi: 10.4274/jcrpe.2002
31. de Carvalho JAM, Tatsch E, Hausen BS, Bollick YS, Moretto MB, Duarte T, et al. Urinary kidney injury molecule-1 and neutrophil gelatinase-associated lipocalin as indicators of tubular damage in normoalbuminuric patients with type 2 diabetes. Clin Biochem (2016) 49(3):232–6. doi: 10.1016/j.clinbiochem.2015.10.016
32. Anderson AH, Xie D, Wang X, Baudier RL, Orlandi P, Appel LJ, et al. Novel risk factors for progression of diabetic and nondiabetic CKD: Findings from the chronic renal insufficiency cohort (CRIC) study. Am J Kidney Dis (2021) 77(1):56–73.e1. doi: 10.1053/j.ajkd.2020.07.011
33. Wang N, Lu Z, Zhang W, Bai Y, Pei D, Li L. Serum cystatin c trajectory is a marker associated with diabetic kidney disease. Front Endocrinol (Lausanne) (2022) 13:824279. doi: 10.3389/fendo.2022.824279
34. Jung CY, Yoo TH. Pathophysiologic mechanisms and potential biomarkers in diabetic kidney disease. Diabetes Metab J (2022) 46(2):181–97. doi: 10.4093/dmj.2021.0329
35. Gholaminejad A, Moein S, Roointan A, Mortazavi M, Nouri R, Mansourian M, et al. Circulating β2 and α1 microglobulins predict progression of nephropathy in diabetic patients: a meta-analysis of prospective cohort studies. Acta Diabetol (2022) 59(11):1417–27. doi: 10.1007/s00592-022-01940-w
36. Gnudi L. Angiopoietins and diabetic nephropathy. Diabetologia. (2016) 59(8):1616–20. doi: 10.1007/s00125-016-3995-3
37. Butler AE, Al-Qaissi A, Sathyapalan T, Atkin SL. Angiopoietin-1: an early biomarker of diabetic nephropathy? J Transl Med (2021) 19(1):427. doi: 10.1186/s12967-021-03105-9
38. Wong TY, Cheung CMG, Larsen M, Sharma S, Simó R. Diabetic retinopathy. Nat Rev Dis Primers (2016) 2:16012. doi: 10.1038/nrdp.2016.12
39. Chang LH, Chu CH, Huang CC, Lin LY. Fibroblast growth factor 21 levels exhibit the association with renal outcomes in subjects with type 2 diabetes mellitus. Front Endocrinol (Lausanne) (2022) 13:846018. doi: 10.3389/fendo.2022.846018
40. Chen H, Zhang Z, Zhou L, Cai T, Liu B, Wang L, et al. Identification of CCL19 as a novel immune-related biomarker in diabetic nephropathy. Front Genet (2022) 13:830437. doi: 10.3389/fgene.2022.830437
41. Feng ST, Yang Y, Yang JF, Gao YM, Cao JY, Li ZL, et al. Urinary sediment CCL5 messenger RNA as a potential prognostic biomarker of diabetic nephropathy. Clin Kidney J (2022) 15(3):534–44. doi: 10.1093/ckj/sfab186
42. Zhao B, Zhang M, Xie J, Jiang T, Li J, Yang Z. Implications of increased circulating macrophage inhibitory protein-5 in patients with type 2 diabetes mellitus. Int Immunopharmacol (2022) 109:108916. doi: 10.1016/j.intimp.2022.108916
43. Coca SG, Nadkarni GN, Huang Y, Moledina DG, Rao V, Zhang J, et al. Plasma biomarkers and kidney function decline in early and established diabetic kidney disease. J Am Soc Nephrol JASN (2017) 28(9):2786–93. doi: 10.1681/ASN.2016101101
44. Xin C, Sun X, Li Z, Gao T. Relationship of soluble klotho and early stage of diabetic nephropathy: A systematic review and meta-analysis. Front Endocrinol (Lausanne) (2022) 13:902765. doi: 10.3389/fendo.2022.902765
45. Pan F, Cui W, Gao L, Shi X, Yang H, Hu Y, et al. Serum lutein is a promising biomarker for type 2 diabetes mellitus and diabetic kidney disease in the elderly. J Clin Lab Anal (2022) 36(4):e24350. doi: 10.1002/jcla.24350
46. Lindhardt M, Persson F, Zürbig P, Stalmach A, Mischak H, de Zeeuw D, et al. Urinary proteomics predict onset of microalbuminuria in normoalbuminuric type 2 diabetic patients, a sub-study of the DIRECT-protect 2 study. Nephrology Dialysis Transplant Off Publ Eur Dialysis Transplant Assoc - Eur Renal Assoc (2017) 32(11):1866–73. doi: 10.1093/ndt/gfw292
47. Tofte N, Lindhardt M, Adamova K, Bakker SJL, Beige J, Beulens JWJ, et al. Early detection of diabetic kidney disease by urinary proteomics and subsequent intervention with spironolactone to delay progression (PRIORITY): a prospective observational study and embedded randomised placebo-controlled trial. Lancet Diabetes Endocrinol (2020) 8(4):301–12. doi: 10.1016/S2213-8587(20)30026-7
48. Mutter S, Valo E, Aittomaki V, Nybo K, Raivonen L, Thorn LM, et al. Urinary metabolite profiling and risk of progression of diabetic nephropathy in 2670 individuals with type 1 diabetes. Diabetologia. (2022) 65(1):140–9. doi: 10.1007/s00125-021-05584-3
49. Sankrityayan H, Kulkarni YA, Gaikwad AB. Diabetic nephropathy: The regulatory interplay between epigenetics and microRNAs. Pharmacol Res (2019) 141:574–85. doi: 10.1016/j.phrs.2019.01.043
50. Kinuthia UM, Wolf A, Langmann T. Microglia and inflammatory responses in diabetic retinopathy. Front In Immunol (2020) 11:564077. doi: 10.3389/fimmu.2020.564077
51. Sabanayagam C, Banu R, Chee ML, Lee R, Wang YX, Tan G, et al. Incidence and progression of diabetic retinopathy: a systematic review. Lancet Diabetes Endocrinol (2019) 7(2):140–9. doi: 10.1016/S2213-8587(18)30128-1
52. Taylor AW. Ocular immune privilege. Eye (London England) (2009) 23(10):1885–9. doi: 10.1038/eye.2008.382
53. Rudraraju M, Narayanan SP, Somanath PR. Regulation of blood-retinal barrier cell-junctions in diabetic retinopathy. Pharmacol Res (2020) 161:105115. doi: 10.1016/j.phrs.2020.105115
54. Huang J, Zhou Q. CD8+T cell-related gene biomarkers in macular edema of diabetic retinopathy. Front Endocrinol (Lausanne) (2022) 13:907396. doi: 10.3389/fendo.2022.907396
55. Huang J, Zhou Q. Gene biomarkers related to Th17 cells in macular edema of diabetic retinopathy: Cutting-edge comprehensive bioinformatics analysis and In vivo validation. Front Immunol (2022) 13:858972. doi: 10.3389/fimmu.2022.858972
56. Gu C, Lhamo T, Zou C, Zhou C, Su T, Draga D, et al. Comprehensive analysis of angiogenesis-related genes and pathways in early diabetic retinopathy. BMC Med Genomics (2020) 13(1):142. doi: 10.1186/s12920-020-00799-6
57. Olivier M, Asmis R, Hawkins GA, Howard TD, Cox LA. The need for multi-omics biomarker signatures in precision medicine. Int J Mol Sci (2019) 20(19):4781. doi: 10.3390/ijms20194781
58. Niu S-R, Hu J-M, Lin S, Hong Y. Research progress on exosomes/microRNAs in the treatment of diabetic retinopathy. Front In Endocrinology (2022) 13:935244. doi: 10.3389/fendo.2022.935244
59. Ipp E, Liljenquist D, Bode B, Shah VN, Silverstein S, Regillo CD, et al. Pivotal evaluation of an artificial intelligence system for autonomous detection of referrable and vision-threatening diabetic retinopathy. JAMA Netw Open (2021) 4(11):e2134254. doi: 10.1001/jamanetworkopen.2021.34254
60. Dai L, Wu L, Li H, Cai C, Wu Q, Kong H, et al. A deep learning system for detecting diabetic retinopathy across the disease spectrum. Nat Commun (2021) 12(1):3242. doi: 10.1038/s41467-021-23458-5
61. Gerendas BS, Bogunovic H, Sadeghipour A, Schlegl T, Langs G, Waldstein SM, et al. Computational image analysis for prognosis determination in DME. Vision Res (2017) 139:204–10. doi: 10.1016/j.visres.2017.03.008
62. Abràmoff MD, Lavin PT, Birch M, Shah N, Folk JC. Pivotal trial of an autonomous AI-based diagnostic system for detection of diabetic retinopathy in primary care offices. NPJ Digital Med (2018) 1:39. doi: 10.1038/s41746-018-0040-6
63. Tufail A, Kapetanakis VV, Salas-Vega S, Egan C, Rudisill C, Owen CG, et al. An observational study to assess if automated diabetic retinopathy image assessment software can replace one or more steps of manual imaging grading and to determine their cost-effectiveness. Health Technol Assess (2016) 20(92):1–72. doi: 10.3310/hta20920
64. Ting DSW, Cheung CY-L, Lim G, Tan GSW, Quang ND, Gan A, et al. Development and validation of a deep learning system for diabetic retinopathy and related eye diseases using retinal images from multiethnic populations with diabetes. JAMA. (2017) 318(22):2211–23. doi: 10.1001/jama.2017.18152
65. Mitchell P, Bandello F, Schmidt-Erfurth U, Lang GE, Massin P, Schlingemann RO, et al. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. (2011) 118(4):615–25. doi: 10.1016/j.ophtha.2011.01.031
66. Brown DM, Schmidt-Erfurth U, Do DV, Holz FG, Boyer DS, Midena E, et al. Intravitreal aflibercept for diabetic macular edema: 100-week results from the VISTA and VIVID studies. Ophthalmology. (2015) 122(10):2044–52. doi: 10.1016/j.ophtha.2015.06.017
67. Shahraki T AA, Nourinia R, Beheshtizadeh NF, Entezari M, Nikkhah H, Karimi S, et al. PANRETINAL PHOTOCOAGULATION VERSUS INTRAVITREAL BEVACIZUMAB VERSUS a PROPOSED MODIFIED COMBINATION THERAPY FOR TREATMENT OF PROLIFERATIVE DIABETIC RETINOPATHY_ a randomized three-arm clinical trial (CTPDR study). Retina. (2022) 42(6):1065–76. doi: 10.1097/IAE.0000000000003450
68. Brown DM, Wykoff CC, Boyer D, Heier JS, Clark WL, Emanuelli A, et al. Evaluation of intravitreal aflibercept for the treatment of severe nonproliferative diabetic retinopathy: Results from the PANORAMA randomized clinical trial. JAMA Ophthalmol (2021) 139(9):946–55. doi: 10.1001/jamaophthalmol.2021.2809
69. Brown DM, Emanuelli A, Bandello F, Barranco JJE, Figueira J, Souied E, et al. KESTREL and KITE: 52-week results from two phase III pivotal trials of brolucizumab for diabetic macular edema. Am J Ophthalmol (2022) 238:157–72. doi: 10.1016/j.ajo.2022.01.004
70. Arrigo A, Bandello F. Molecular features of classic retinal drugs, retinal therapeutic targets and emerging treatments. Pharmaceutics. (2021) 13(7):1102. doi: 10.3390/pharmaceutics13071102
71. Campochiaro PA, Marcus DM, Awh CC, Regillo C, Adamis AP, Bantseev V, et al. The port delivery system with ranibizumab for neovascular age-related macular degeneration: Results from the randomized phase 2 ladder clinical trial. Ophthalmology. (2019) 126(8):1141–54. doi: 10.1016/j.ophtha.2019.03.036
72. Chang MA, Kapre A, Kaufman D, Kardatzke DR, Rabena M, Patel S, et al. Patient preference and treatment satisfaction with a port delivery system for ranibizumab vs intravitreal injections in patients with neovascular age-related macular degeneration: A randomized clinical trial. JAMA Ophthalmol (2022) 140(8):771–8. doi: 10.1001/jamaophthalmol.2022.1091
73. Wykoff CC, Abreu F, Adamis AP, Basu K, Eichenbaum DA, Haskova Z, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. Lancet (2022) 399(10326):741–55. doi: 10.1016/S0140-6736(22)00018-6
74. Al-Khersan H, Hussain RM, Ciulla TA, Dugel PU. Innovative therapies for neovascular age-related macular degeneration. Expert Opin Pharmacother (2019) 20(15):1879–91. doi: 10.1080/14656566.2019.1636031
75. Wells JA, Glassman AR, Ayala AR, Jampol LM, Bressler NM, Bressler SB, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema: Two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology. (2016) 123(6):1351–9. doi: 10.1016/j.ophtha.2016.02.022
76. Zhou Q, Guo C, You A, Wang D, Wang W, Zhang X. One-year outcomes of novel VEGF decoy receptor therapy with intravitreal conbercept in diabetic retinopathy-induced macular edema. Mol Vis (2019) 25:636–44.
77. Sultan MB, Zhou D, Loftus J, Dombi T, Ice KS. A phase 2/3, multicenter, randomized, double-masked, 2-year trial of pegaptanib sodium for the treatment of diabetic macular edema. Ophthalmology. (2011) 118(6):1107–18. doi: 10.1016/j.ophtha.2011.02.045
78. Callanan DG, Loewenstein A, Patel SS, Massin P, Corcóstegui B, Li X-Y, et al. A multicenter, 12-month randomized study comparing dexamethasone intravitreal implant with ranibizumab in patients with diabetic macular edema. Graefes Arch Clin Exp Ophthalmol (2017) 255(3):463–73. doi: 10.1007/s00417-016-3472-1
79. Busch C, Fraser-Bell S, Iglicki M, Lupidi M, Couturier A, Chaikitmongkol V, et al. Real-world outcomes of non-responding diabetic macular edema treated with continued anti-VEGF therapy versus early switch to dexamethasone implant: 2-year results. Acta Diabetol (2019) 56(12):1341–50. doi: 10.1007/s00592-019-01416-4
80. Pereiro X, Ruzafa N, Acera A, Fonollosa A, Rodriguez FD, Vecino E. Dexamethasone protects retinal ganglion cells but not müller glia against hyperglycemia in vitro. PloS One (2018) 13(11):e0207913. doi: 10.1371/journal.pone.0207913
81. Portillo JC, Yu JS, Vos S, Bapputty R, Lopez Corcino Y, Hubal A, et al. Disruption of retinal inflammation and the development of diabetic retinopathy in mice by a CD40-derived peptide or mutation of CD40 in Muller cells. Diabetologia (2022) 65(12):2157–71. doi: 10.1007/s00125-022-05775-6
82. Simo R, Hernandez C. Novel approaches for treating diabetic retinopathy based on recent pathogenic evidence. Prog Retin Eye Res (2015) 48:160–80. doi: 10.1016/j.preteyeres
83. Kanda A, Noda K, Saito W, Ishida S. (Pro)renin receptor is associated with angiogenic activity in proliferative diabetic retinopathy. Diabetologia. (2012) 55(11):3104–13. doi: 10.1007/s00125-012-2702-2
84. Chaturvedi N, Sjolie AK, Stephenson JM, Abrahamian H, Keipes M, Castellarin A, et al. Effect of lisinopril on progression of retinopathy in normotensive people with type 1 diabetes. the EUCLID study group. EURODIAB controlled trial of lisinopril in insulin-dependent diabetes mellitus. Lancet (1998) 351(9095):28–31. doi: 10.1016/s0140-6736(97)06209-0
85. Chaturvedi N, Porta M, Klein R, Orchard T, Fuller J, Parving HH, et al. Effect of candesartan on prevention (DIRECT-prevent 1) and progression (DIRECT-protect 1) of retinopathy in type 1 diabetes: randomised, placebo-controlled trials. Lancet. (2008) 372(9647):1394–402. doi: 10.1016/S0140-6736(08)61412-9
86. Sjølie AK, Klein R, Porta M, Orchard T, Fuller J, Parving HH, et al. Effect of candesartan on progression and regression of retinopathy in type 2 diabetes (DIRECT-protect 2): a randomised placebo-controlled trial. Lancet. (2008) 372(9647):1385–93. doi: 10.1016/S0140-6736(08)61411-7
87. Harindhanavudhi T, Mauer M, Klein R, Zinman B, Sinaiko A, Caramori ML. Benefits of renin-angiotensin blockade on retinopathy in type 1 diabetes vary with glycemic control. Diabetes Care (2011) 34(8):1838–42. doi: 10.2337/dc11-0476
88. Patel A, MacMahon S, Chalmers J, Neal B, Woodward M, Billot L, et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. (2007) 370(9590):829–40. doi: 10.1016/S0140-6736(07)61303-8
89. Mahaling B, Srinivasarao DA, Raghu G, Kasam RK, Bhanuprakash Reddy G, Katti DS. A non-invasive nanoparticle mediated delivery of triamcinolone acetonide ameliorates diabetic retinopathy in rats. Nanoscale. (2018) 10(35):16485–98. doi: 10.1039/c8nr00058a
90. Tanaka K, Hara S, Hattori M, Sakai K, Onishi Y, Yoshida Y, et al. Role of elevated serum uric acid levels at the onset of overt nephropathy in the risk for renal function decline in patients with type 2 diabetes. J Diabetes Investig (2015) 6(1):98–104. doi: 10.1111/jdi.12243
91. Schrauben SJ, Shou H, Zhang X, Anderson AH, Bonventre JV, Chen J, et al. Association of multiple plasma biomarker concentrations with progression of prevalent diabetic kidney disease: Findings from the chronic renal insufficiency cohort (CRIC) study. J Am Soc Nephrol JASN (2021) 32(1):115–26. doi: 10.1681/ASN.2020040487
92. McCormick BB, Sydor A, Akbari A, Fergusson D, Doucette S, Knoll G. The effect of pentoxifylline on proteinuria in diabetic kidney disease: a meta-analysis. Am J Kidney Dis (2008) 52(3):454–63. doi: 10.1053/j.ajkd.2008.01.025
93. Navarro-Gonzalez JF, Mora-Fernandez C, Muros de Fuentes M, Chahin J, Mendez ML, Gallego E, et al. Effect of pentoxifylline on renal function and urinary albumin excretion in patients with diabetic kidney disease: the PREDIAN trial. J Am Soc Nephrol (2015) 26(1):220–9. doi: 10.1681/ASN.2014010012
94. Moosaie F, Rabizadeh S, Fallahzadeh A, Sheikhy A, Meysamie A, Dehghani Firouzabadi F, et al. Effects of pentoxifylline on serum markers of diabetic nephropathy in type 2 diabetes. Diabetes Ther (2022) 13(5):1023–36. doi: 10.1007/s13300-022-01250-y
95. de Zeeuw D, Bekker P, Henkel E, Hasslacher C, Gouni-Berthold I, Mehling H, et al. The effect of CCR2 inhibitor CCX140-b on residual albuminuria in patients with type 2 diabetes and nephropathy: a randomised trial. Lancet Diabetes Endocrinol (2015) 3(9):687–96. doi: 10.1016/S2213-8587(15)00261-2
96. Menne J, Eulberg D, Beyer D, Baumann M, Saudek F, Valkusz Z, et al. C-c motif-ligand 2 inhibition with emapticap pegol (NOX-E36) in type 2 diabetic patients with albuminuria. Nephrol Dial Transplant (2017) 32(2):307–15. doi: 10.1093/ndt/gfv459
97. Tesch GH. Diabetic nephropathy - is this an immune disorder? Clin Sci (Lond) (2017) 131(16):2183–99. doi: 10.1042/CS20160636
98. Xiao Y, Liang D, Li Z, Feng Z, Yuan Z, Zhang F, et al. BMP-7 upregulates Id2 through the MAPK signaling pathway to improve diabetic tubulointerstitial fibrosis and the intervention of oxymatrine. Front Pharmacol (2022) 13:900346. doi: 10.3389/fphar.2022.900346
99. Wang M, Liu X, Wang Z, Xu Q. The extract of polygala fallax hemsl. slows the progression of diabetic nephropathy by targeting TLR4 anti-inflammation and MMP-2/9-mediated anti-fibrosis in vitro. Phytomedicine. (2022) 104:154251. doi: 10.1016/j.phymed.2022.154251
100. Wennmann DO, Hsu H-H, Pavenstädt H. The renin-angiotensin-aldosterone system in podocytes. Semin Nephrol (2012) 32(4):377–84. doi: 10.1016/j.semnephrol
101. Umanath K, Lewis JB. Update on diabetic nephropathy: Core curriculum 2018. Am J Kidney Dis (2018) 71(6):884–95. doi: 10.1053/j.ajkd.2017.10.026
102. Deng X, Li D, Tang Q, Chen Y. ACEI and ARB lower the incidence of end-stage renal disease among patients with diabetic nephropathy: A meta-analysis. Comput Math Methods Med (2022) 2022:6962654. doi: 10.1155/2022/6962654
103. Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. New Engl J Med (2016) 375(4):323–34. doi: 10.1056/NEJMoa1515920
104. Roett MA, Liegl S, Jabbarpour Y. Diabetic nephropathy–the family physician's role. Am Fam Physician (2012) 85(9):883–9.
105. Panchapakesan U, Pollock C. The role of dipeptidyl peptidase - 4 inhibitors in diabetic kidney disease. Front In Immunol (2015) 6:443. doi: 10.3389/fimmu.2015.00443
106. Kristensen SL, Rørth R, Jhund PS, Docherty KF, Sattar N, Preiss D, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol (2019) 7(10):776–85. doi: 10.1016/S2213-8587(19)30249-9
107. Georgianos PI, Agarwal R. Endothelin a receptor antagonists in diabetic kidney disease. Curr Opin Nephrol Hypertens (2017) 26(5):338–44. doi: 10.1097/MNH.0000000000000342
108. Mann JFE, Green D, Jamerson K, Ruilope LM, Kuranoff SJ, Littke T, et al. Avosentan for overt diabetic nephropathy. J Am Soc Nephrol JASN (2010) 21(3):527–35. doi: 10.1681/ASN.2009060593
109. Joergensen C, Tarnow L, Goetze JP, Rossing P. Vitamin d analogue therapy, cardiovascular risk and kidney function in people with type 1 diabetes mellitus and diabetic nephropathy: a randomized trial. Diabetes Med (2015) 32(3):374–81. doi: 10.1111/dme.12606
110. Kim MJ, Frankel AH, Donaldson M, Darch SJ, Pusey CD, Hill PD, et al. Oral cholecalciferol decreases albuminuria and urinary TGF-β1 in patients with type 2 diabetic nephropathy on established renin-angiotensin-aldosterone system inhibition. Kidney Int (2011) 80(8):851–60. doi: 10.1038/ki.2011.224
111. Wang Y, Yang S, Zhou Q, Zhang H, Yi B. Effects of vitamin d supplementation on renal function, inflammation and glycemic control in patients with diabetic nephropathy: a systematic review and meta-analysis. Kidney Blood Press Res (2019) 44(1):72–87. doi: 10.1159/000498838
112. He H, Halseth TA, Mei L, Shen C, Liu L, Schwendeman A. Nanodisc delivery of liver X receptor agonist for the treatment of diabetic nephropathy. J Control Release (2022) 348:1016–27. doi: 10.1016/j.jconrel.2022.06.029
113. de Mello VD, Selander T, Lindstrom J, Tuomilehto J, Uusitupa M, Kaarniranta K. Serum levels of plasmalogens and fatty acid metabolites associate with retinal microangiopathy in participants from the Finnish diabetes prevention study. Nutrients. (2021) 13(12):4452. doi: 10.3390/nu13124452
114. Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes. (2005) 54(6):1615–25. doi: 10.2337/diabetes.54.6.1615
115. Pearce I, Simó R, Lövestam-Adrian M, Wong DT, Evans M. Association between diabetic eye disease and other complications of diabetes: Implications for care. a systematic review. Diabetes Obes Metab (2019) 21(3):467–78. doi: 10.1111/dom.13550
116. Grunwald JE, Pistilli M, Ying G-S, Maguire MG, Daniel E, Whittock-Martin R, et al. Progression of retinopathy and incidence of cardiovascular disease: findings from the chronic renal insufficiency cohort study. Br J Ophthalmol (2021) 105(2):246–52. doi: 10.1136/bjophthalmol-2019-315333
117. Yang J-K, Wang Y-Y, Liu C, Shi T-T, Lu J, Cao X, et al. Urine proteome specific for eye damage can predict kidney damage in patients with type 2 diabetes: A case-control and a 5.3-year prospective cohort study. Diabetes Care (2017) 40(2):253–60. doi: 10.2337/dc16-1529
118. Romero-Aroca P, Baget-Bernaldiz M, Navarro-Gil R, Moreno-Ribas A, Valls-Mateu A, Sagarra-Alamo R, et al. Glomerular filtration rate and/or ratio of urine albumin to creatinine as markers for diabetic retinopathy: A ten-year follow-up study. J Diabetes Res (2018) 2018:5637130. doi: 10.1155/2018/5637130
119. Zhang X, Kumari N, Low S, Ang K, Yeo D, Yeoh LY, et al. The association of serum creatinine and estimated glomerular filtration rate variability with diabetic retinopathy in asians with type 2 diabetes: A nested case-control study. Diabetes Vasc Dis Res (2018) 15(6):548–58. doi: 10.1177/1479164118786969
Keywords: microvascular complications, diabetic retinopathy, diabetic nephropathy, biomarkers, therapy, artificial intelligence
Citation: Xie Z and Xiao X (2022) Novel biomarkers and therapeutic approaches for diabetic retinopathy and nephropathy: Recent progress and future perspectives. Front. Endocrinol. 13:1065856. doi: 10.3389/fendo.2022.1065856
Received: 10 October 2022; Accepted: 09 November 2022;
Published: 25 November 2022.
Edited by:
Xinyuan Zhang, Beijing Tongren Hospital, Capital Medical University, ChinaReviewed by:
Min Zhao, INSERM U1138 Centre de Recherche des Cordeliers (CRC), FranceCopyright © 2022 Xie and Xiao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xinhua Xiao, eGlhb3hoMjAxNEB2aXAuMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.