
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol. , 19 December 2022
Sec. Cardiovascular Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1064969
This article is part of the Research Topic Advances in Research of the Cardiovascular Disease Continuum: Endocrine Aspects of Disease Pathophysiology, Risk Predictors, Therapeutics, and Management of Diabetes and Hypertension Volume II View all 9 articles
 Tadesse Asmamaw Dejenie1*
Tadesse Asmamaw Dejenie1* Markeshaw Tiruneh G/Medhin1
Markeshaw Tiruneh G/Medhin1 Fitalew Tadele Admasu2
Fitalew Tadele Admasu2 Getachew Asmare Adella3
Getachew Asmare Adella3 Engidaw Fentahun Enyew4
Engidaw Fentahun Enyew4 Zemene Demelash Kifle5
Zemene Demelash Kifle5 Mohammed Abdu Seid6
Mohammed Abdu Seid6 Misganaw Asmamaw Mengstie2
Misganaw Asmamaw Mengstie2 Endeshaw Chekol Abebe2
Endeshaw Chekol Abebe2Cardiometabolic disease is a spectrum of diseases including, cardiovascular diseases, and metabolic syndrome. It is the leading cause of morbidity and mortality worldwide, with premature deaths being preventable. Currently, sleep has emerged as a potential target for cardiometabolic disease prevention. Several epidemiological studies have provided ample evidence that objectively measured short sleep duration increases the risk of cardiometabolic disease. However, the findings are inconsistent, and few studies measure sleep duration on cardiometabolic profiles objectively. Therefore, in this review, we focused on the recently published literature that explored the association between objectively measured sleep duration and cardiometabolic profiles (cardiovascular diseases, type 2 diabetes mellitus, and metabolic syndrome), seeking more insights regarding the applicability and, in turn, the impact of objectively measured sleep duration on cardiometabolic health, which is relatively understudied. We retrieved the information manually from PubMed, Google Scholar, HINARI, and the Cochrane Library from 2015 to 2022 using appropriate search terms, we included 49 articles. In this review, we found a strong relationship between objectively measured sleep duration and the risk of cardiometabolic disease, indicating that objectively measured short sleep durations increase cardiometabolic risks. In general, the association between objectively measured sleep duration and increased cardiometabolic risks (CMR) has been well-documented in higher-income countries. Several studies found that longer sleep duration was associated with a more favorable cardiometabolic profile in early adolescence, independent of other risk factors. On the other hand, objectively measured short sleep duration is associated with adverse cardiometabolic health outcomes such as coronary heart disease, hypertension, type 2 diabetes mellitus, and metabolic syndrome.
Cardiometabolic disease is a spectrum of diseases including, cardiovascular diseases, and metabolic syndrome (1). Currently, it is the main contributor to morbidity and mortality globally with premature deaths being preventable. Factors contributing to cardiometabolic diseases are varied and influenced by environmental, social, political, and commercial determinants of health (2). The American College of Cardiology defines cardio-metabolic risks (CMR) as a collection of interconnected factors including hypertension, elevated fasting blood sugar, dyslipidemia, abdominal obesity, and elevated triglycerides (3). Based on the American Heart Association (AHA), in collaboration with the National Institutes of Health in 2019, the global prevalence of cardio-metabolic risks such as obesity (39.6%), hypertension (45.6%), diabetes mellitus (9.8%) and metabolic syndrome was found to be 21% (4). The aforementioned factors were thought to be major contributors to cardiovascular disease (CVD), which is responsible for 15% of global disability-adjusted life years (DALYs) and 30% of all deaths (5). The pooled prevalence of metabolic syndrome in Ethiopia is found to be 34.89%, with the weighted pooled prevalence of metabolic syndrome being higher in females (36.74%) compared to males (22.22%) (6). Subgroups at increased risk are type 2 diabetes patients, hypertensive patients, psychiatric patients, and HIV patients on HAART (7).
Sleep is an essential biological and behavioral process that plays a substantial role in maintaining good health and quality of life. It is controlled by diurnal, homeostatic, and neurohormonal mechanisms (8). Researchers have identified sleep as an essential modulator of cardiovascular function, blood glucose regulation, and hormonal secretion. Furthermore, sleep duration has an impact on metabolic hormones, body weight, the autonomic nervous system, the coagulation system, endothelial function, and metabolic regulation (9). Healthy sleep is characterized by many dimensions, including adequate duration, high quality, appropriate timing, and the absence of sleep disorders. Not getting enough sleep at night is generally associated with daytime sleepiness, daytime fatigue, depression, poor daytime functioning, and other health and safety problems (10).
In general, individuals’ sleep quality and quantity varies depending on age, sex, genetic factors, occupation, educational level, socioeconomic status, race, family relationships, and pathological conditions (11). Several studies also report that, in comparison with whites, African Americans are more likely to have sleep delays and short sleep durations. A delayed sleep phase was more likely to be observed among African American individuals with a morning or intermediate chronotype than among white individuals with the same chronotype (12, 13). Cespedes et al. report that objective sleep timing, including weekday time in bed, weekday time asleep, weekend time in bed, weekend time asleep, weekday mid-sleep time, weekday sleep duration, weekday in bed duration, weekend sleep duration, and weekend in bed duration, all differ significantly between African American and white participants (Table 1) (15). Based on the US National Sleep Foundation, adequate sleep recommendations also vary across lifespans and are inversely related to age, with 7–9 hrs recommended for adults (26, 27). However, in recent decades, the average sleep duration has decreased across the globe, and this has negatively impacted cardiometabolic health (11).
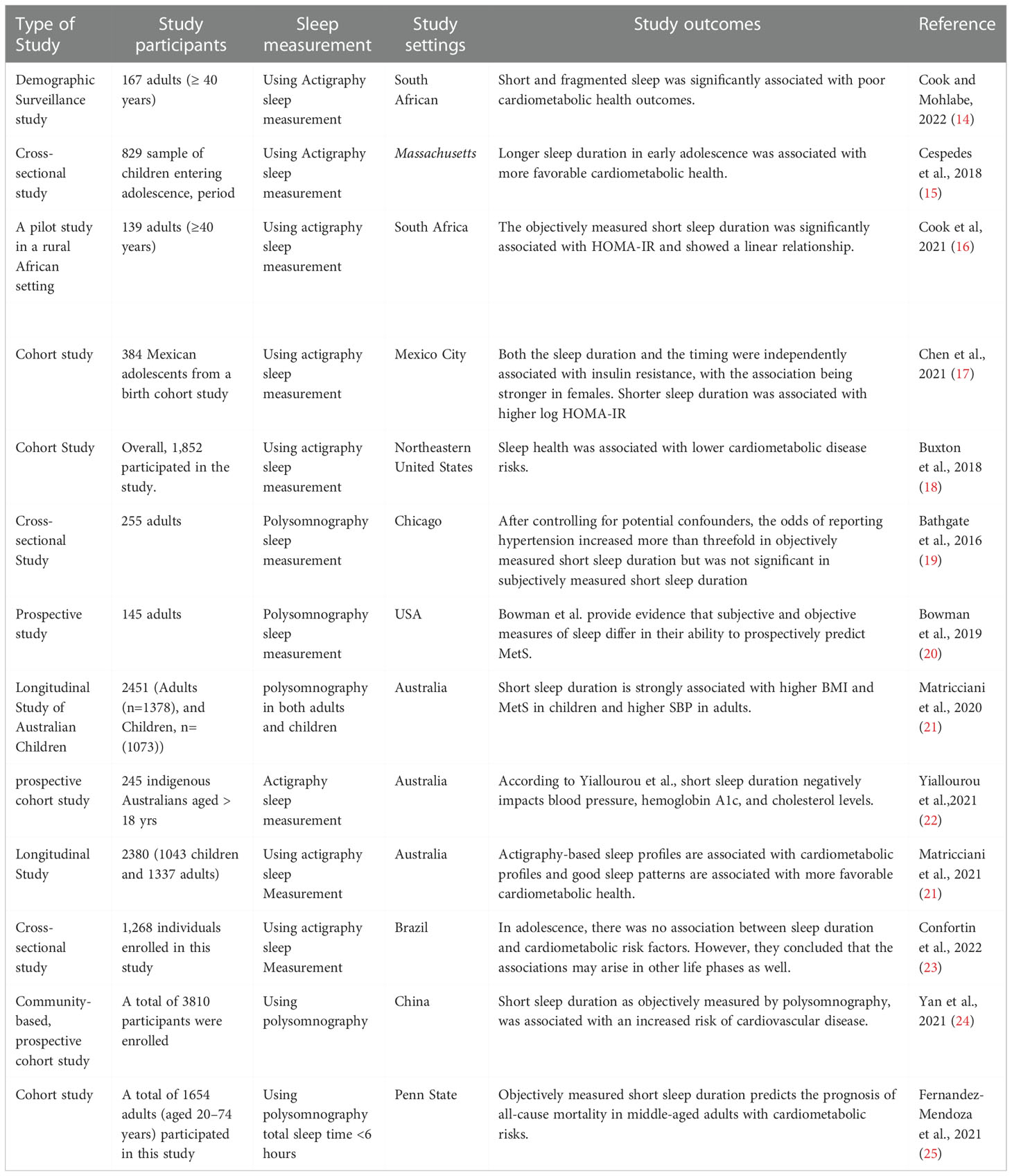
Table 1 summary of studies on objective sleep duration and cardiometabolic health adverse outcomes.
To assess sleep, a variety of tools are used. There are valid questionnaires and surveys that provide information on subjective sleep parameters (28), including quantity, latency to sleep onset, duration, and level of daytime sleepiness, such as the Pittsburgh Sleep Quality Index (29) and Epworth Sleepiness Scales (30). Even though self-reported sleep parameters are relatively easy to administer and inexpensive, methodological concerns and finding inconsistencies arise (31). Currently, objective sleep measuring tools are widely used mainly in developed countries. Among the objective sleep measuring tools, polysomnography (PSG) is a sleep laboratory test that provides detailed information on nocturnal physiology, including a recording of objective sleep architecture as well as measures of cardiopulmonary function (32). Actigraphy, which is another objective sleep measurement, evaluates sleep versus wake time with a small wrist-worn monitor and can more conveniently capture information (33). Importantly, there may be major differences in outcomes when comparing subjective versus objectively recorded sleep quantity and quality (27). Currently, several studies have reported that individuals with sleep disorders and objectively measured short sleep duration were found to have a higher risk of adverse cardiometabolic profiles in objectively recorded sleep, although no significant association was observed using subjectively assessed sleep (25, 34).
In this review, we focused on the recently published literature that explored the association between objectively measured sleep duration and cardiometabolic diseases (cardiovascular diseases, type 2 diabetes mellitus, and metabolic syndrome), seeking more insights regarding the applicability and, in turn, the impact of objectively measured sleep duration on cardiometabolic health, which is relatively understudied.
The information was manually retrieved from PubMed, Google Scholar, HINARI, and the Cochrane Library from 2015 to 2022 (Figure 1), to assess studies that examined the relationship between objectively measured sleep duration and cardiometabolic disease (metabolic syndrome, cardiovascular disease, and type 2 diabetes mellitus). We used appropriate search terms from 2015 scoping searches, target references, and browsing of database thesauruses (objective sleep duration and cardiometabolic diseases) A basic search strategy was developed for PubMed and modified accordingly for other research engines using the following search criteria; objective sleep duration OR cardiometabolic adverse outcomes OR cardiovascular disease OR metabolic syndrome OR type 2 diabetes mellitus; OR objective sleep duration AND cardiometabolic adverse outcomes AND cardiovascular disease AND metabolic syndrome AND type 2 diabetes mellitus. Those articles written in English and which were based on objectively measured sleep duration and were recently published from 2015 to 2022 were included for this review. On the other hand, articles written in languages other than English, based on self or parental sleep assessments, and published prior to 2015, with the exception of the definition of terms and proposed mechanisms that show the link between objectively short sleep duration and cardiometabolic health adverse outcomes, which can be the same for both objectively and subjectively measured sleep duration, were excluded from the review.

Figure 1 Flowchart of the literature search.
A strong relationship between sleep duration and the risk of cardiometabolic disease has been found in several studies, indicating that objectively measured short sleep durations increase cardiometabolic risks (35, 36). In the general, the association between objectively measured sleep insufficiency and increased cardiometabolic risks (CMR) has been well-documented in higher-income countries (37). However, it is relatively limited in low-income countries such as Sub-Saharan Africa (9, 38). Thus, little is known about the prevalence and consequences of objectively measured sleep disorders in most African populations, and their association with CMR has not yet been well documented (37). In fact, more research has been conducted on the relationship between sleep and cardiometabolic health in developed nations. For instance, in a cross-sectional study of 829 adolescents using wrist actigraphy recording, Feliciano et al. found that Independent of other risk factors, optimum sleep duration and better sleep quality were linked to a more favorable cardiometabolic profile in early adolescence (15). However, some studies also showed that very long sleep duration was associated with poor cardiometabolic health outcomes, stating that there were increased odds of diabetes among long sleepers (>8 hr) and that it was also associated with a higher risk of CVD mortality (24). Evidence studies suggest a U-shaped association between sleep duration and T2DM and show that long sleepers have almost 60% higher odds of developing T2DM compared to normal sleepers (39). On the other hand, objectively measured short sleep duration is associated with adverse cardiometabolic health outcomes such as coronary heart disease, hypertension, type 2 diabetes mellitus, and metabolic syndrome (40). In the following sections, the authors have discussed each component of cardiometabolic disease and its association with objectively measured sleep duration.
The leading cause of death in the world today is cardiovascular disease (CVD), including coronary heart disease (CHD), stroke, peripheral arterial disease, deep vein thrombosis, and pulmonary embolism (41, 42). By addressing modifiable risk factors, such as reducing excessive dietary salt, improving a poor diet, lowering obesity, avoiding excessive alcohol consumption, increasing physical activity, and improving socioeconomic conditions, premature deaths from cardiovascular disease can be prevented (43). This is the most cost-effective intervention for reducing cardiovascular disease-related morbidity and mortality and improving cardiovascular health.
According to the Coronary Artery Risk Development in Young Adults (CARDIA) cohort study conducted in Chicago, there is evidence of an association between objectively measured sleep duration and cardiometabolic disease (43). From this report, 18- to 30-year-old individuals were participated and were followed up for five years. The sleep metrics were measured using wrist actigraphy, and to measure the calcifications of their coronary arteries, a CT scan was used. After excluding the possible confounding factors, participants with a sleep habit of 5 hours or less had a sharp increase in their risk of developing coronary calcifications, which is in turn a risk factor for myocardial infarction. Women are more affected than men, although the possible justification of gender differences is not well stated. Similar to what was reported, individuals who regularly slept less than 5 or 6 hours were more likely to experience episodes of coronary heart disease and develop stroke in the long run than people who typically slept for about 6 to 8 hours each night (44). If the short sleep is accompanied by poor sleep quality, the risk is greater. In general, few studies have investigated the associations of objectively measured sleep duration with incident cardiovascular diseases (CVDs). A prospective cohort study of 12,770 people in the United Kingdom discovered that getting enough sleep is associated with a lower risk of cardiovascular disease in people with diabetes (45). A cross-sectional study involving a sample of 893 adults found that shorter sleep duration, as determined by wrist actigraphy, is associated with higher SBP and possibly cardiovascular risk. Objectively measured short sleep duration may therefore be a modifiable behavioral target for reducing cardiovascular risk (46). Yadav et al. also showed that objectively measured short sleep duration was consistently associated with the occurrence of hypertension in middle-aged participants (47). The findings were in line with previous studies carried out by Bertisch et al. which also reported that short sleep duration was associated with hypertension compared to individuals who had normal sleep duration (48). Another prospective study of 1715 Korean adults aged 40 to 70 years found that objectively short sleep duration is independently associated with the development of hypertension among middle-aged and elderly Korean adults (47). Thus, the study encourages clinicians and researchers to promote sound sleep practices in society by giving evidence that explains the association between objective short sleep duration and hypertension as a risk predictor of the incidence of cardiovascular disease.
Hypertension is a known risk factor for cardiovascular disease and leads to disability and death. It is often described as a “silent killer” because it rarely causes symptoms (49). Currently, studies prove a significant association between short sleep (less than 5 hours per night) and an increased risk of hypertension (19, 50). In the Penn State Cohort study, Bertisch et al. showed that objectively measured short sleep duration is a clinically significant risk factor for the development of hypertension independent of other risk factors such as age, race, obesity, diabetes mellitus, smoking, caffeine, or alcohol consumption (48). Using a cross-sectional, observational study design of 255 adult volunteers, Bathgate et al. reported that objectively measured short sleep duration of < 6 hr was associated with an increased risk of hypertension development as compared to individuals with a sleep duration of >6 hrs (51). However, no significant risk was observed using subjectively measured sleep duration groups in this study. Finally, this study concluded that objectively short sleep duration increased the likelihood of hypertension more than three times, taking into account possible confounding variables, and, in turn, increased the risk of cardiovascular disease (51).
The term “metabolic syndrome” refers to a group of metabolic risk factors including glucose intolerance, dyslipidemia, hypertension, and central obesity that are associated with an increased risk of type 2 diabetes mellitus (T2DM) and cardiovascular disease (CVD), including glucose intolerance, dyslipidemia, hypertension, and central obesity (52). According to the Joint Interim Statement (JIS) harmonized, the following three components are required for the definition of Metabolic Syndrome (MetS), of which waist circumference is not a prerequisite: High resting blood pressure (≥ 130/85 mmHg) or on hypertension treatment; ≥ 5.6 mmol/l fasting blood sugar or on diabetes treatment: Elevated waist circumference (WC): Females ≥92 cm, males ≥86 cm; elevated triglycerides (TG): ≥1.7 mmol/l and reduced high-density lipoprotein cholesterol (HDL-C): men < 1.0 mmol/l, women < 1.3 mmol/l (53). Most previous studies exploring the relationship between sleep duration and MetS-related morbidity and mortality were inconsistent and underwhelming (54–56). For instance in In a cross-sectional study of Chinese children and adolescents, Duan et al. reported that objective short sleep duration is associated with higher odds of metabolic syndrome and abdominal obesity. However, the relationship between short sleep duration and MetS in children and adolescents has been inconsistent (56). In a population-based study, Fernandez-Mendoza et al. demonstrated the PSG and reported that objectively measured short sleep duration modifies the elevated risk of CVD mortality associated with MetS. Importantly, this is primarily caused by the high blood pressure and glucose dysregulation components of MetS, which suggests that objectively short sleep duration in those with MetS may be related to the degree of central autonomic and metabolic dysfunction (57). On the other hand, Cook et al. found a significant non-linear (U-shaped) association between short sleep duration and JIS-MetS risk (p = 0.0308) (Table 1) (16). The findings of this study are consistent with the study conducted by Rae et al. (9). According to the authors, this was the first actigraphy-measured sleep and cardiometabolic health study from a rural South African setting. Future clinical trials should investigate whether long-duration sleep improves the prognosis of people with MetS.
The global prevalence of obesity has increased dramatically over the past few decades, and the World Health Organization has declared it a global epidemic (58). The rise in obesity is paralleled with a decrease in sleep duration. Most of the previous studies were predominantly cross-sectional; that is, they measured both sleep duration and the presence of obesity at the same time. Therefore, a possible relationship cannot support a causal association. More recently, however, objective measures of sleep using actigraphy and more specific measures of adiposity (fat mass versus lean body mass) appear to support the link between sleep deprivation and obesity (59). Experimental studies provide a good explanation of the plausible mechanism of how short sleep leads to obesity. Chronic short-term sleep results in increased energy intake and decreased energy expenditure by activating hormonal responses that regulate appetite and energy balance (60). During sleep deprivation, there are reciprocal changes in leptin, a hormone that regulates energy storage and satiety, and ghrelin, a hormone that increases appetite (Figure 1) (61). These two hormones regulate the hunger and satiety of individuals.
Several epidemiologic and longitudinal studies have reported that short sleep duration is a risk factor for the incidence of obesity. For example, in sex-and age-stratified analyses, Sluggett et al. indicated that short sleep duration increased the likelihood of being overweight or obese in children and adolescents compared to longer sleepers (62). In contrast to this study, a cohort sleep laboratory study using polysomnography (PSG) showed that objectively measured short sleep duration is not significantly associated with obesity (63).
Type-2 diabetes is the most common type of diabetes in the world, and it is characterized by the body’s inability to use glucose from circulation, resulting in hyperglycemia. This is caused by peripheral tissue resistance to the action of insulin to take up glucose into the cell (insulin resistance) or inadequate pancreatic insulin production in response to a glucose load (64).
Currently, several studies have revealed that sleep duration is associated with poor glycemic control (17, 65, 66). In a sample of 384 Mexican adolescents from a birth cohort study, Chen et al. reported that objectively shorter sleep duration and later sleep midpoint was associated with higher insulin resistance (HOMA-IR). In linear regression analysis, they found that shorter sleep duration was associated with higher log HOMA-IR after adjusting for age, sex, and sleep midpoint. In the sex-stratified models, the associations between insulin resistance and short sleep duration were more evident among girls (17). Another prospective cohort study of nulliparous women recruited between 16 and 21 weeks gestation found that shorter sleep duration and a later sleep midpoint using the actigraphy sleep measuring tool were associated with an increased risk of gestational diabetes. This study concluded that short sleep duration is the sole contributing factor to gestational diabetes in nulliparous women (67). This research was consistent with a cross-sectional study done in the UK with 2848 adult participants, which showed a link between short sleep duration and the incidence of diabetes mellitus (64). According to a population-based study conducted in 2021 on a Taiwanese population, short sleep duration increased the risk of T2DM. This study found that women who sleep for shorter periods have a higher risk of developing type 2 diabetes, which has an impact on the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) index (68). In this review, the authors observed that the association between sleep durations and increased CMR has been well-documented in higher-income countries (37). However, objective sleep measures are relatively limited in low-income countries such as Sub-Saharan Africa. The majority of sleep studies conducted in this region most frequently used self-reported sleep. Thus, little is known about the prevalence and consequences of sleep disorders in African populations, and their association with type 2 diabetes mellitus has not yet been well investigated, based on objective sleep measures, in most parts of African countries (37).
In general, the association between objectively measured sleep duration using actigraphy or/and Polysomnography and increased cardiometabolic risks (CMR) has been well-documented in higher-income countries. However, studies in developing nation mainly parent- or self-reported sleep assessment tools, and very few studies have examined the association between objectively measured sleep duration and cardiometabolic health outcomes. For example, in a demographic surveillance study done in South Africa using actigraphy sleep measures, it was found that insufficient and fragmented sleep were significantly associated with poor cardiometabolic health outcomes (14) (Table 1). Another pilot study in a rural setting in South Africa using the same sleep measurements found that objectively measured short sleep duration was significantly associated with HOMA-IR and showed a linear relationship with type-2 diabetes mellitus (16).
A vast majority of studies conducted in developed nations used objective sleep assessment tools. For instance, a cross-sectional study using actigraphy sleep measurement in Massachusetts reported that longer sleep duration in early adolescence was associated with more favorable cardiometabolic health outcomes (15). Studies also showed that very long sleep duration was associated with poor cardiometabolic health outcomes (24), showing that there is a U-shaped association between sleep duration and cardiometabolic health outcomes (39). A cohort study conducted on Mexican adolescents found that both the objectively measured sleep duration and timing were independently associated with cardiometabolic risks, with the association being stronger in females (17) (Table 1). In line with this, a study conducted in the Northeastern United States found that healthy sleep was associated with lower cardiometabolic disease risks (18), which agreed with a study conducted in Chicago that indicated the odds of reporting hypertension increased more than threefold in objectively measured short sleep duration but were not significant in subjectively measured short sleep duration (19). Another prospective study in the United States using the same sleep measurement tool provided evidence that subjective and objective measures of sleep differ in their ability to prospectively predict cardiometabolic risk (20). On the other hand, a longitudinal study in Australia reported that objectively measured short sleep duration is strongly associated with higher BMI and MetS in children and higher SBP in adults (21). In the same study setting, another study on indigenous Australians aged > 18 years found that short sleep duration negatively impacts blood pressure, hemoglobin A1C, and cholesterol levels (22). On the one hand, a cross-sectional study that was conducted in Brazil concluded that there was no association between sleep duration and cardiometabolic risk factors and justified the notion that the associations may arise in other life phases as well (21). Besides, a study conducted at Penn State reported that objectively measured short sleep duration predicts the prognosis of all-cause mortality in middle-aged adults with cardiometabolic risks (25).
In this review, we noted that the impact of short sleep duration on cardiometabolic health is widely acknowledged and has been thoroughly examined in the literature over the past decades. There is a strong and consistent association between the duration of sleep, especially short sleep duration, and cardiometabolic health outcomes. A U-shaped relationship between sleep duration and the risk of cardiometabolic disease has been found in several studies, indicating that objectively measured very long and short sleep durations increase cardiometabolic risks.
We suggest that future studies should investigate population-based longitudinal associations between sleep and cardiometabolic health with the use of objective sleep measurements conducted for several days and at multiple time points over time. Meanwhile, based on the available evidence, we recommend that children and adolescents should get adequate amounts of good sleep in a regular pattern.
Furthermore, we suggest conducting more studies examining the associations between gender-stratified sleep patterns and cardiometabolic health as well as more studies to be performed in developing countries because most sleep research is conducted in developed nations, but cardiometabolic risk factors are more prevalent in developing countries. Besides the authors observed that many of the sleep studies on cardiometabolic health were conducted in older adults, but sleep-disorder-related factors, including duration, quality, and timing, may be emerging as early as childhood. As a result, further research should be performed on the role of childhood sleep insufficiency across the life course as a determinant factor for developing the adult cardiometabolic disease.
All authors made a significant contribution to the work reported, whether in drafting or critical revision for important intellectual content; the conception, study design, execution, acquisition, and interpretation; or in all these areas; they took part in critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Type-2 diabetes mellitus (T2DM), United States (US), Polysomnography (PSG), Coronary Heart Disease (CHD), Coronary Artery Risk Development in Young Adults (CARDIA), Computerized Tomography (CT), Joint Interim Statement (JIS), Metabolic Syndrome (MetS), Waist circumference (WC), United Kingdom (UK), Homeostatic Model Assessment for Insulin Resistance (HOMA-IR), Cardiometabolic Risks (CMR), Cardiovascular diseases (CVDs) and Systolic Blood Pressure (SBP).
1. Guo F, Moellering DR, Garvey WT. The progression of the cardiometabolic disease: validation of a new cardiometabolic disease staging system applicable to obesity. Obesity (2014) 22(1):110–8. doi: 10.1002/oby.20585
2. Miranda JJ, Barrientos-Gutiérrez T, Corvalan C, Hyder AA, Lazo-Porras M, Oni T, et al. Understanding the rise of cardiometabolic diseases in low-and middle-income countries. Nat Med (2019) 25(11):1667–79. doi: 10.1038/s41591-019-0644-7
3. Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, et al. AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American college of Cardiology/American heart association joint committee on clinical practice guidelines. Circulation (2021) 144(22):e368–454. doi: 10.1161/CIR.0000000000001029
4. Dorans KS, Mills KT, Liu Y, He J. Trends in prevalence and control of hypertension according to the 2017 American college of Cardiology/American heart association (ACC/AHA) guideline. J Am Heart Assoc (2018) 7(11):e008888. doi: 10.1161/JAHA.118.008888
5. Münzel T, Hahad O, Sørensen M, Lelieveld J, Duerr GD, Nieuwenhuijsen M, et al. Environmental risk factors and cardiovascular diseases: a comprehensive expert review. Cardiovasc Res (2022) 118(14):2880–902. doi: 10.1093/cvr/cvab316
6. Jemere T, Kefale B. Metabolic syndrome and its associated factors in Ethiopia: A systematic review and meta-analysis. J Diabetes Metab Disord (2021) 20(1):1021–31. doi: 10.1007/s40200-021-00815-1
7. Maggi P, Santoro CR, Nofri M, Ricci E, De Gennaro N, Bellacosa C, et al. Clusterization of co-morbidities and multi-morbidities among persons living with HIV: a cross-sectional study. BMC Infect diseases (2019) 19(1):1–9. doi: 10.1186/s12879-019-4184-z
8. Mosavat M, Mirsanjari M, Arabia D, Smyth A, Whitehead L. The role of sleep curtailment on leptin levels in obesity and diabetes mellitus. Obes Facts (2021) 14(2):214–21. doi: 10.1159/000514095
9. Tobaldini E, Fiorelli EM, Solbiati M, Costantino G, Nobili L, Montano N. Short sleep duration and cardiometabolic risk: from pathophysiology to clinical evidence. Nat Rev Cardiol (2019) 16(4):213–24. doi: 10.1038/s41569-018-0109-6
10. Chaput J-P, Dutil C, Sampasa-Kanyinga H. Sleeping hours: what is the ideal number, and how does age impact this? Nat Sci sleep (2018) 10:421. doi: 10.2147/NSS.S163071
11. Miguez MJ, Bueno D, Perez C. Disparities in sleep health among adolescents: The role of sex, age, and migration. Sleep Disord (2020) 2020:5316364. doi: 10.1155/2020/5316364
12. Bailey O, Combs D, Sans-Fuentes M, Havens CM, Grandner MA, Poongkunran C, et al. Delayed sleep time in African americans and depression in a community-based population. J Clin Sleep Med (2019) 15(6):857–64. doi: 10.5664/jcsm.7836
13. Malone SK, Patterson F, Lu Y, Lozano A, Hanlon A. Ethnic differences in sleep duration and morning–evening type in a population sample. Chronobiol Int (2016) 33(1):10–21. doi: 10.3109/07420528.2015.1107729
14. Cook I, Mohlabe M. Objectively-measured sleep patterns and cardiometabolic health in a rural south African setting: a cross-sectional analysis. Sleep Sci Practice. (2022) 6(1):1–10. doi: 10.1186/s41606-022-00070-0
15. Cespedes Feliciano EM, Quante M, Rifas-Shiman SL, Redline S, Oken E, Taveras EM. Objective sleep characteristics and cardiometabolic health in young adolescents. Pediatrics (2018) 142(1). doi: 10.1542/peds.2017-4085
16. Cook I, Mohlabe M, Makgopa HM. Association between cardiometabolic health and objectively measured, free-living sleep parameters: a pilot study in a rural African setting. Sleep Sci Practice. (2021) 5(1):1–10. doi: 10.1186/s41606-020-00054-y
17. Chen P, Baylin A, Lee J, Dunietz GL, Cantoral A, Rojo MMT, et al. The association between sleep duration and sleep timing and insulin resistance among adolescents in Mexico city. J Adolesc Health (2021) 69(1):57–63. doi: 10.1016/j.jadohealth.2020.10.012
18. Buxton OM, Lee S, Marino M, Beverly C, Almeida DM, Berkman L. Sleep health and predicted cardiometabolic risk scores in employed adults from two industries. J Clin Sleep Med (2018) 14(3):371–83. doi: 10.5664/jcsm.6980
19. Bock JM, Vungarala S, Covassin N, Somers VK. Sleep duration and hypertension: Epidemiological evidence and underlying mechanisms. Am J hypertension (2022) 35(1):3–11. doi: 10.1093/ajh/hpab146
20. Bowman MA, Duggan KA, Brindle RC, Kline CE, Krafty RT, Thayer JF, et al. Prospective associations among objectively and subjectively assessed sleep and the metabolic syndrome. Sleep Med (2019) 58:1–6. doi: 10.1016/j.sleep.2019.02.005
21. Matricciani L, Dumuid D, Paquet C, Fraysse F, Wang Y, Baur LA, et al. Sleep and cardiometabolic health in children and adults: examining sleep as a component of the 24-h day. Sleep Med (2021) 78:63–74. doi: 10.1016/j.sleep.2020.12.001
22. Yiallourou SR, Maguire GP, Carrington MJ. Sleep quantity and quality and cardiometabolic risk factors in indigenous australians. J Sleep Res (2021) 30(2):e13067. doi: 10.1111/jsr.13067
23. Confortin SC, Aristizábal LYG, da Silva Magalhães EI, Barbosa AR, Ribeiro CCC, Batista RFL, et al. Association between sleep duration and cardiometabolic factors in adolescents. BMC Public Health (2022) 22(1):1–10. doi: 10.1186/s12889-022-13119-7
24. Yan B, Yang J, Zhao B, Fan Y, Wang W, Ma X. Objective sleep efficiency predicts cardiovascular disease in a community population: the sleep heart health study. J Am Heart Assoc (2021) 10(7):e016201. doi: 10.1161/JAHA.120.016201
25. Fernandez-Mendoza J, He F, Puzino K, Amatrudo G, Calhoun S, Liao D, et al. Insomnia with objective short sleep duration is associated with cognitive impairment: a first look at cardiometabolic contributors to brain health. Sleep (2021) 44(1):zsaa150. doi: 10.1093/sleep/zsaa150
26. Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, et al. National sleep foundation’s sleep time duration recommendations: methodology and results in summary. Sleep Health (2015) 1(1):40–3. doi: 10.1016/j.sleh.2014.12.010
27. Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, et al. National sleep foundation’s updated sleep duration recommendations: final report. Sleep Health (2015) 1(4):233–43. doi: 10.1016/j.sleh.2015.10.004
28. Girschik J, Fritschi L, Heyworth J, Waters F. Validation of self-reported sleep against actigraphy. J Epidemiol (2012) 22(5):462–8. doi: 10.2188/jea.JE20120012
29. Setyowati A, Chung MH. Validity and reliability of the Indonesian version of the Pittsburgh sleep quality index in adolescents. Int J Nurs Practice. (2021) 27(5):e12856. doi: 10.1111/ijn.12856
30. Omobomi O, Quan SF. A requiem for the clinical use of the epworth sleepiness scale. J Clin Sleep Med (2018) 14(5):711–2. doi: 10.5664/jcsm.7086
31. Rahimi-Eichi H, Coombs IIIG, Bustamante CMV, Onnela J-P, Baker JT, Buckner RL. Open-source longitudinal sleep analysis from accelerometer data (DPSleep): Algorithm development and validation. JMIR mHealth uHealth. (2021) 9(10):e29849. doi: 10.2196/29849
32. Kukwa W, Migacz E, Lis T, Ishman SL. The effect of in-lab polysomnography and home sleep polygraphy on sleep position. Sleep Breathing. (2021) 25(1):251–5. doi: 10.1007/s11325-020-02099-w
33. Borger JN, Huber R, Ghosh A. Capturing sleep-wake cycles by using day-to-day smartphone touchscreen interactions. NPJ digital Med (2019) 2(1):1–8. doi: 10.1038/s41746-019-0147-4
34. Aluzaite K, Wu H, Hyslop B, Young J, Schultz M, Brockway B. Perceived versus objective sleep quality in long-stay hospitalized older adults–mixed methods study. Age Ageing (2021) 50(3):955–62. doi: 10.1093/ageing/afaa292
35. Smiley A. Association of sleep and metabolic Syndrome/Metabolic syndrome components among participants in Jackson heart study (JHS) and the reasons for geographic and racial differences in stroke (REGARDS). Indiana University (2019).
36. Song Q, Liu X, Zhou W, Wang X, Wu S. Changes in sleep duration and risk of metabolic syndrome: the kailuan prospective study. Sci Rep (2016) 6(1):1–7. doi: 10.1038/srep36861
37. Roche J, Rae DE, Redman KN, Knutson KL, Von Schantz M, Gómez-Olivé FX, et al. Impact of obstructive sleep apnea on cardiometabolic health in a random sample of older adults in rural south Africa: building the case for the treatment of sleep disorders in underresourced settings. J Clin sleep Med (2021) 17(7):1423–34. doi: 10.5664/jcsm.9214
38. Akanbi MO, Agaba PA, Ozoh OB, Ocheke AN, Gimba ZM, Ukoli CO, et al. Obesity and obstructive sleep apnea risk among nigerians. J Med tropics (2017) 19(2):110. doi: 10.4103/jomt.jomt_17_17
39. Jackson CL, Ward JB, Johnson DA, Sims M, Wilson J, Redline S. Concordance between self-reported and actigraphy-assessed sleep duration among African-American adults: findings from the Jackson heart sleep study. Sleep (2020) 43(3):zsz246. doi: 10.1093/sleep/zsz246
40. Killick R, Stranks L, Hoyos CM. Sleep deficiency and cardiometabolic disease. Clinics Chest Med (2022) 43(2):319–36. doi: 10.1016/j.ccm.2022.02.011
41. Sharif N, Opu RR, Ahmed SN, Sarkar MK, Jaheen R, Daullah MU, et al. Prevalence and impact of comorbidities on disease prognosis among patients with COVID-19 in Bangladesh: a nationwide study amid the second wave. Diabetes Metab Syndrome: Clin Res Rev (2021) 15(4):102148. doi: 10.1016/j.dsx.2021.05.021
42. Maloberti A, Qualliu E, Occhi L, Sun J, Grasso E, Tognola C, et al. Hyperuricemia prevalence in healthy subjects and its relationship with cardiovascular target organ damage. Nutrition Metab Cardiovasc Diseases (2021) 31(1):178–85. doi: 10.1016/j.numecd.2020.08.015
43. Chandola T, Ferrie JE, Perski A, Akbaraly T, Marmot MG. The effect of short sleep duration on coronary heart disease risk is greatest among those with sleep disturbance: a prospective study from the Whitehall II cohort. Sleep (2010) 33(6):739–44. doi: 10.1093/sleep/33.6.739
44. Leng Y, Cappuccio FP, Wainwright NW, Surtees PG, Luben R, Brayne C, et al. Sleep duration and risk of fatal and nonfatal stroke: a prospective study and meta-analysis. Neurology (2015) 84(11):1072–9. doi: 10.1212/WNL.0000000000001371
45. Tao F, Cao Z, Jiang Y, Fan N, Xu F, Yang H, et al. Associations of sleep duration and quality with incident cardiovascular disease, cancer, and mortality: a prospective cohort study of 407,500 UK biobank participants. Sleep Med (2021) 81:401–9. doi: 10.1016/j.sleep.2021.03.015
46. Sun J, Wang M, Yang L, Zhao M, Bovet P, Xi B. Sleep duration and cardiovascular risk factors in children and adolescents: a systematic review. Sleep Med Rev (2020) 53:101338. doi: 10.1016/j.smrv.2020.101338
47. Yadav D, Hyun DS, Ahn SV, Koh SB, Kim JY. A prospective study of the association between total sleep duration and incident hypertension. J Clin Hypertension (2017) 19(5):550–7. doi: 10.1111/jch.12960
48. Bertisch SM, Pollock BD, Mittleman MA, Buysse DJ, Bazzano LA, Gottlieb DJ, et al. Insomnia with objective short sleep duration and risk of incident cardiovascular disease and all-cause mortality: Sleep heart health study. Sleep (2018) 41(6):zsy047. doi: 10.1093/sleep/zsy047
49. Zhou B, Bentham J, Di Cesare M, Bixby H, Danaei G, Cowan MJ, et al. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet (2017) 389(10064):37–55. doi: 10.1016/S0140-6736(16)31919-5
50. Chang X, Chen X, Ji JS, Luo G, Sun Q, Zhang N, et al. Association between sleep duration and hypertension in southwest China: a population-based cross-sectional study. BMJ Open (2022) 12(6):e052193. doi: 10.1136/bmjopen-2021-052193
51. Bathgate CJ, Edinger JD, Wyatt JK, Krystal AD. Objective but not subjective short sleep duration associated with increased risk for hypertension in individuals with insomnia. Sleep (2016) 39(5):1037–45. doi: 10.5665/sleep.5748
52. Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med (2011) 9(1):1–13. doi: 10.1186/1741-7015-9-48
53. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation (2009) 120(16):1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
54. Shan Z, Ma H, Xie M, Yan P, Guo Y, Bao W, et al. Sleep duration and risk of type 2 diabetes: a meta-analysis of prospective studies. Diabetes Care (2015) 38(3):529–37. doi: 10.2337/dc14-2073
55. Wang Y, Huang W, O’Neil A, Lan Y, Aune D, Wang W, et al. Association between sleep duration and mortality risk among adults with type 2 diabetes: a prospective cohort study. Diabetologia (2020) 63(11):2292–304. doi: 10.1007/s00125-020-05214-4
56. Duan Y, Sun J, Wang M, Zhao M, Magnussen CG, Xi B. Association between short sleep duration and metabolic syndrome in Chinese children and adolescents. Sleep Med (2020) 74:343–8. doi: 10.1016/j.sleep.2020.08.018
57. Fernandez-Mendoza J, He F, LaGrotte C, Vgontzas AN, Liao D, Bixler EO. The impact of the metabolic syndrome on mortality is modified by objective short sleep duration. J Am Heart Assoc (2017) 6(5):e005479. doi: 10.1161/JAHA.117.005479
58. Foundation NS Sleep in America poll: Sleep in the modern family. Washington (DC: The Foundation (2014).
59. Saidi O, Rochette E, Del Sordo G, Doré É, Merlin É, Walrand S, et al. Eucaloric balanced diet improved objective sleep in adolescents with obesity. Nutrients (2021) 13(10):3550. doi: 10.3390/nu13103550
60. Hysing M, Pallesen S, Stormark KM, Jakobsen R, Lundervold AJ, Sivertsen B. Sleep and use of electronic devices in adolescence: results from a large population-based study. BMJ Open (2015) 5(1):e006748. doi: 10.1136/bmjopen-2014-006748
61. Smiley A, Wolter S, Nissan D. Mechanisms of association of sleep and metabolic syndrome. J Med Clin Res Rev (2019) 3(3):1–9. doi: 10.33425/2639-944X.1089
62. Sluggett L, Wagner SL, Hardy C, Harris RL. Associations between sleep duration and indicators of cardiometabolic disease in Canadian children and adolescents: Analyses of the 2007–2009 Canadian health measures survey. Childhood Obes (2016) 12(5):325–33. doi: 10.1089/chi.2015.0214
63. Larsen SC, Horgan G, Mikkelsen ML, Palmeira AL, Scott S, Duarte C, et al. Association between objectively measured sleep duration, adiposity and weight loss history. Int J Obes (2020) 44(7):1577–85. doi: 10.1038/s41366-020-0537-3
64. Tinajero MG, Malik VS. An update on the epidemiology of type 2 diabetes: A global perspective. Endocrinol Metab Clinics North America. (2021) 50(3):337–55. doi: 10.1016/j.ecl.2021.05.013
65. Bawadi H, Al Sada A, Al Mansoori N, Al Mannai S, Hamdan A, Shi Z, et al. Sleeping duration, napping and snoring in association with diabetes control among patients with diabetes in Qatar. Int J Environ Res Public Health (2021) 18(8):4017. doi: 10.3390/ijerph18084017
66. Brady EM, Bodicoat DH, Hall AP, Khunti K, Yates T, Edwardson C, et al. Sleep duration, obesity and insulin resistance in a multi-ethnic UK population at high risk of diabetes. Diabetes Res Clin practice. (2018) 139:195–202. doi: 10.1016/j.diabres.2018.03.010
67. Facco FL, Grobman WA, Reid KJ, Parker CB, Hunter SM, Silver RM, et al. Objectively measured short sleep duration and later sleep midpoint in pregnancy are associated with a higher risk of gestational diabetes. Am J obstetrics gynecol (2017) 217(4):447.e1–.e13. doi: 10.1016/j.ajog.2017.05.066
Keywords: cardiometabolic health, type 2 diabetes, cardiovascular disease, objective, sleep duration
Citation: Dejenie TA, G/Medhin MT, Admasu FT, Adella GA, Enyew EF, Kifle ZD, Seid MA, Mengstie MA and Abebe EC (2022) Impact of objectively-measured sleep duration on cardiometabolic health: A systematic review of recent evidence. Front. Endocrinol. 13:1064969. doi: 10.3389/fendo.2022.1064969
Received: 09 October 2022; Accepted: 05 December 2022;
Published: 19 December 2022.
Edited by:
Gerald J. Maarman, Stellenbosch University, South AfricaReviewed by:
Regina Felső, University of Pécs, HungaryCopyright © 2022 Dejenie, G/Medhin, Admasu, Adella, Enyew, Kifle, Seid, Mengstie and Abebe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tadesse Asmamaw Dejenie, YXMyNHRhZGVzc2VAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.