 Anna Wawrzyniak1Marzena Skrzypczak-Zielińska2
Anna Wawrzyniak1Marzena Skrzypczak-Zielińska2 Michał Michalak3Marta Kaczmarek-Ryś2
Michał Michalak3Marta Kaczmarek-Ryś2 Alicja Ewa Ratajczak4,5*
Alicja Ewa Ratajczak4,5* Anna Maria Rychter4,5
Anna Maria Rychter4,5 Kinga Skoracka4,5
Kinga Skoracka4,5 Michalina Marcinkowska1
Michalina Marcinkowska1 Ryszard Słomski2Agnieszka Dobrowolska4
Ryszard Słomski2Agnieszka Dobrowolska4 Iwona Krela-Kaźmierczak4
Iwona Krela-Kaźmierczak4- 1Department of Family Medicine, Poznan University of Medical Sciences, Poznań, Poland
- 2Institute of Human Genetics, Polish Academy of Sciences, Poznań, Poland
- 3Department of Computer Science and Statistics, Poznan University of Medical Sciences, Poznań, Poland
- 4Department of Gastroenterology, Dietetics and Internal Diseases, Poznan University of Medical Sciences, Poznań, Poland
- 5Doctoral School, Poznan University of Medical Sciences, Poznań, Poland
Introduction: One of the challenges of personalized medicine is a departure from traditional pharmacology toward individualized, genotype-based therapies. Postmenopausal osteoporosis is a prevalent condition requiring intensive treatment, whose effects are measurable only after a long time, and the goal is bone fracture prevention. This study aimed to determine the influence of VDR gene variation on anti-osteoporotic one-year treatment with denosumab in 63 Polish women with postmenopausal osteoporosis.
Materials and methods: The correlation between bone mineral density (BMD) of the lumbar vertebral column (L1–L4) and femoral neck, and genotype distributions for the ApaI, BsmI, FokI, and TaqI variants of the VDR gene was analyzed. Bone fractures during denosumab therapy were also investigated.
Results: In the case of the Bsml polymorphism, female patients with BB and Bb genotypes had statistically significantly higher values of BMD and T-score/Z-score indicators, which persisted after a year of denosumab treatment. Our results indicated that the Bsml polymorphism contributes to better bone status, and, consequently, to more efficient biological therapy. The study did not reveal significant differences between changes (delta) in BMD and genotypes for the analyzed VDR gene loci. In the entire study group, one bone fracture was observed in one patient throughout the yearlong period of denosumab therapy.
Conclusions: BB and Bb genotypes of the Bsml polymorphism of the VDR gene determine higher DXA parameter values both before and after one-year denosumab therapy in postmenopausal women with osteoporosis.
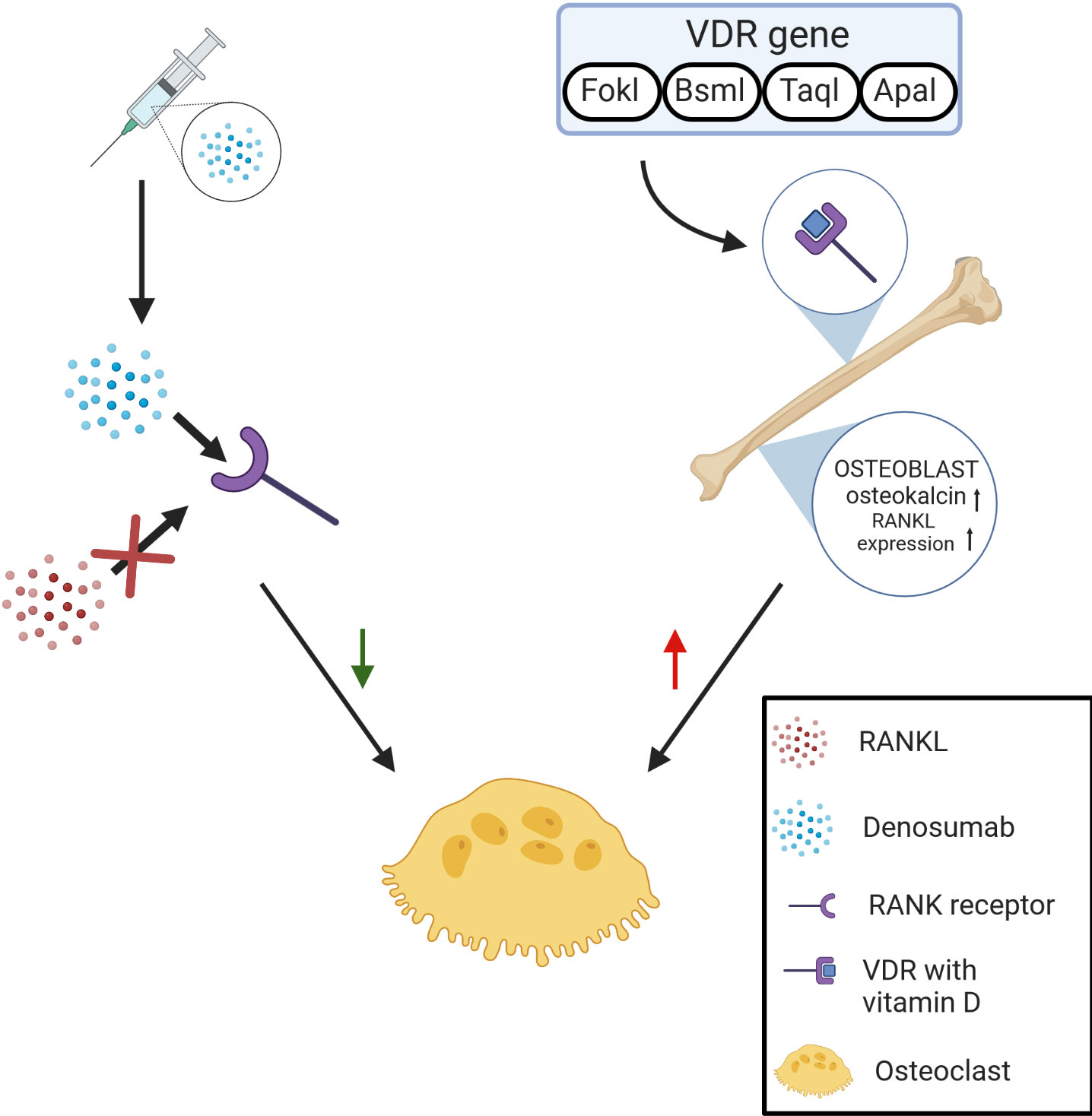
Graphical Abstract
1. Introduction
The individualization of treatment is a strategy used in many areas of medicine. In osteoporosis pharmacotherapy, this is extremely important due to hard-to-define therapy objectives and the extensive time it takes to assess treatment. The therapy of osteoporosis - bone disorder, which is a consequence of the imbalance between bone resorption and bone formation - should prevent the first and subsequent osteoporotic fractures. The DXA method indirectly assesses its effects in regular bone mass. Changes in bone mineral density (BMD) reflect the path of transformation, and an increase in density is a substitute indicator of therapy efficacy. The therapy is difficult to manage because DXA assessment makes sense only after one year, at which point a lack of response may also be observed. The fact is that even the most effective drugs do not produce the anticipated results in all patients, and the efficacy of available treatment is evaluated at 70% in terms of vertebral fracture reduction. Therefore, the ability to identify patients - before treatment - who will respond to a drug from those who will not is crucial.
However, pharmacogenetics seems to meet those requirements. Polymorphisms of a number of genes including receptors, e.g. VDR, ESR1, PTHR1, LRP5, and TNFRSF11B (known as OPG) have been described as associated with an increased incidence of fractures and a reduced BMD (1). Therefore, there can be as many candidates for pharmacogenes of osteoporosis as in the case of the polygenic basis of the disease itself. Nevertheless, the VDR gene (OMIM 601769), which codes the protein receptor of vitamin D, is one of the best-studied in terms of its association with osteoporosis and bone fractures. Isolated works concern its potential influence on the effect of osteoporosis therapy. Denosumab is a human monoclonal antibody (IgG2) that counteracts the receptor activator of nuclear factor kappa beta ligand (RANKL), which blocks its binding with RANK, resulting in an inhibition of osteoclast development and activity. Furthermore, a decrease in bone resorption and an increase in BMD leads to a reduction in the number of vertebral body fractures and non-vertebral fractures (2–5). In osteoblasts 1,25(OH)2-D3, it increases the synthesis of osteocalcin and osteopontin, as well as ligand expression for osteoprotegerin/RANK (RANKL, RANK ligand), which, by binding with its RANK receptor (receptor activator of NF-κ B) on prosteoclasts, stimulates their maturation into osteoclasts. The common end metabolic pathway within bones, where the activity of osteotropic hormones coincides with many other local factors (including inflammation mediators and immunological responses), is the configuration of osteoprotegerin/RANK-RANKL, which is responsible for osteoclastogenesis and coupling between bone resorption by osteoclasts, and bone formation by osteoblasts (6). Denosumab is used to prevent skeletal-related events, treat Giant cell tumors of the bone, treat hypercalcemia of malignancy, treat osteoporosis, glucocorticoid-induced osteoporosis, and bone loss (7). Denosumab should be considered in contraindication or no effects of standard treatment (8). There is no unified approach to genetic testing in osteoporosis. The only firm conclusion in many meta-analyses is that different populations can differ significantly in this respect (9). Our previous research showed that the ApaI, BsmI, and TaqI polymorphisms of the VDR gene could be predictors of low-energy fractures. However, it was not observed that these changes are associated with bone mass (10). The VDR gene is located on the long arm of chromosome 12 at position 13.11, has a length of 63,492 base pairs, and consists of 11 exons. VDR protein belongs to the nuclear receptor family and functions as a transcription factor. It was found that the polymorphisms of four loci - ApaI (rs7975232), BsmI (rs1544410), FokI (rs10735810), and TaqI (rs731236) - within the VDR gene are related to changes BMD (11–13). The literature contains no studies indicating a correlation between denosumab therapy efficacy and VDR gene polymorphism. However, it was proven that the optimal (at least 50 nmol/L) concentration of 25 (OH) vitamin D in serum, as a ligand of the VDR receptor, improves denosumab therapy efficacy. This observation is still being explained (14). Pharmacogenetic studies raise the question of whether polymorphism of the VDR gene influences denosumab treatment efficacy in women with postmenopausal osteoporosis. The objective of this study was to answer this question by assessing BMD changes in the lumbar spine (L1–L4) and femoral neck over one year, as well as the incidence of new fractures during therapy in female patients with single ApaI, BsmI, FokI and TaqI polymorphic variations of the VDR gene.
This study aimed to determine the influence of VDR gene variants on anti-osteoporotic one-year treatment with denosumab in 63 Polish women with postmenopausal osteoporosis.
2. Materials and methods
The sample group consisted of 63 women, aged between 57 and 86 (mean 75.0 ± 7.3 years) being treated for postmenopausal osteoporosis from Greater Poland in the Endocrinology and Osteoporosis Outpatient Clinic [Poznan University of Medical Sciences, Heliodor Swiecicki Hospital]. In the group of women enrolled in the study before denosumab therapy began, 55 (87.3%) had been diagnosed with bone fractures, including 40 (63.49%) with vertebral fractures, 6 (9.52%) with femoral neck fractures, and 36 (57.14%) with non-vertebral fractures. The patients were subject to one year of observation while undergoing denosumab therapy in the form of single, 60 mg subcutaneous injections of denosumab once every six months, in accordance with the product profile (2, 15, 16). All patients used 800–1,200 mg/day of standard calcium supplementation and up to 1,000 IU/day of vitamin D. All patients gave their written consent to participate in the study and genetic testing. The study was approved by the Bioethical Committee of the Poznan University of Medical Sciences (Poland; approval no. 508/13).
The inclusion criteria were diagnosis of postmenopausal osteoporosis according to the WHO criteria and lack of contraindications to denosumab treatment in accordance with the product profile. Based on medical history, clinical examination, and laboratory tests, women with secondary variants of the disease (i.e. hyperthyroidism, hyperparathyroidism, Cushing’s disease, kidney disease, rheumatoid arthritis, malabsorption syndromes) were excluded from the group. To investigate the associations of single ApaI, BsmI, FokI, and TaqI polymorphic variants of the VDR gene with changes in BMD over one year, molecular and densitometry tests using the dual-photon X-ray absorptiometry (DXA) method were conducted twice – once before and once after the one-year denosumab therapy period using the DPX-Plus device (Lunar). The incidence of bone fractures during and after the one-year denosumab treatment period was also assessed.
2.1. Genotyping
DNA was isolated from peripheral blood leukocytes by the guanidinium isothiocyanate method (17). The polymerase chain reaction (PCR) was carried out in 20 μl with 200 ng genomic DNA, 50 mM KCl, 10 mM Tris–HCl (pH 8.3), 1.5 mM MgCl2, 0.25 mM dNTP, 7.5 pmol of each primer, and 0.5 units of Taq polymerase (Sigma). The reaction was conducted as follows: initial denaturation at 94°C for 4 min; followed by 35 cycles of denaturation at 94°C or 40 s; primer annealing for 40 s; elongation at 72°C for 100 s; final incubation at 72°C for 180 s. For BsmI polymorphism, 837 bp fragment was amplified at an annealing temperature of 55°C using primers forward 5’-GGCAACCAAGACTACAAGTACC-3’ and reverse 5’-TCTTCCACCTCTAACCAGCG-3’. For FokI, 267 fragment was amplified at an annealing temperature of 60°C using primers forward 5’- AGCTGGCCCTGGCACTGACTCTGCTCT -3’ and reverse 5’- ATGGAAACACCTTGCTTCTTCTCCCTC-3’ (18, 19). For ApaI and TaqI polymorphisms of the VDR gene, 745 bp fragment was amplified at an annealing temperature of 64°C using primers forward 5’-CAG AGCATGGACAGGGAGCAA-3’ and reverse 5’-GCACTCCTCATGGCTGAGGTCTC-3’ (19). The PCR product was then subjected to restriction fragment length polymorphism (RFLP) analysis using the following restriction enzymes: TaqI (Fermentas); ApaI, Bsp120I (Fermentas); BsmI, and Mva1269I (Fermentas). PCR and RFLP analysis was performed using Applied Biosystems 2720 Thermal Cycler (Applied Biosystems, Foster City, CA). All analyses were carried out according to the manufacturer’s recommendations, and the products of hydrolysis were separated on 1.5% agarose gel and visualized with ethidium bromide.
The numbers of single alleles were calculated as a sum of a double number of homozygotes (dominant or recessive) and a single number of heterozygotes of each studied allele.
2.2. Statistical analysis
Before starting this study, we preliminarily assumed that during the follow-up (one year), we might expect an increase of BMD by 5% and changes in T-score and Z-score by 20%. Taking this assumption and the significance level at α = 0.05 and the power of the test as 80%, we have calculated a minimal sample size of n = 21 for BMD and n = 43 for T- and Z-scores. Finally, we took the sample size n = 63 since that number of patients consented to the study.
All data are expressed as the mean ± SD, unless otherwise stated. The analyzed data were expressed on an interval and nominal scale. To compare the two groups, Student’s t test for dependent data was performed, or, in the absence of the required assumptions (normality and homogeneity of variance), the Wilcoxon test was used. The calculation regarding normal distribution was checked by Shapiro-Wilks test. The Chi-square test or Fisher exact test was used to analyze nominal data. When comparing more than two groups simultaneously, a univariate analysis of variance with Tukey post hoc test was used. Additionally, we checked the Hardy-Weinberg equation for analyzed polymorphisms to measure whether the observed genotype frequencies in a studied population differ from the frequencies predicted by the equation. All tests were analyzed at the significance level of α = 0.05. Statistical analysis was done using Statistica 13.0 software (Stat Soft Inc, Tulsa, USA) and STATA 15.1 (StataCorp LLC).
3. Results
The mean BMI value in the sample group was 23.9 ± 2.9 kg/m2 (mean body weight: 58.3 ± 7.4 kg, mean height: 154.3 ± 6.7 cm). The time since menopause occurs, on average, is 25.8 ± 8.5 years. The mean baseline level of 25-hydroxyvitamin D in the study group was 25.2 ± 7.1 ng/ml. The average values of DXA measurements of the lumbar vertebral column (L1–L4) and femoral neck prior to biological treatment and one year after denosumab therapy are presented in Figure 1 and Supplementary Table S1, 2.
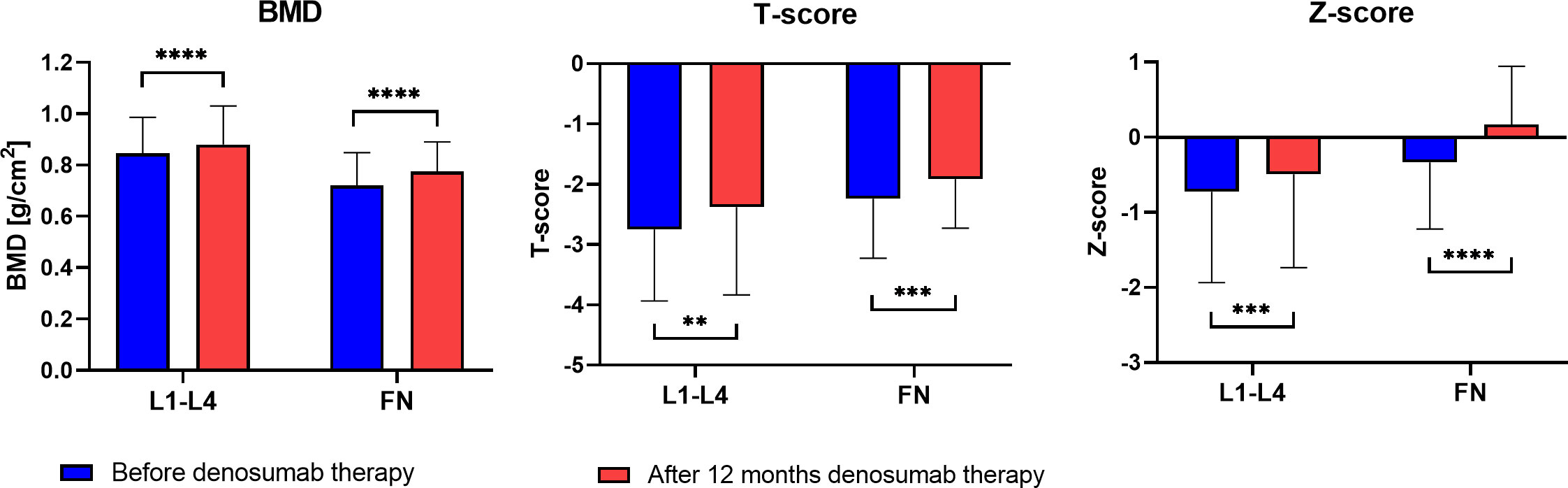
Figure 1 DXA parameters of the lumbar spine and femoral neck (FN)) before and after one year of denosumab therapy in the sample group (**P < 0.01, ***P < 0.001, ****P < 0.001).
The incidence of bone fractures was also observed in the sample group. During the entire denosumab treatment period (12 months), one event of vertebral fractures was observed in one female patient. Due to low variability, this was not subject to statistical analysis.
In the case of all 4 loci, both types of homozygotes (AA, aa, BB, bb, FF, ff, TT and tt) and heterozygotes (Aa, Bb, Ff and Tt) were observed. The TaqI polymorphism (T allele 66.94% and t allele 33.06%) showed the lowest variability. For the remaining changes, the rate of alleles was closer to 50% (Table 1). In contrast to ApaI and TaqI polymorphisms, Bsml and Fokl polymorphisms were not in accordance with the Hardy–Weinberg principle (P > 0.05), Table 1.
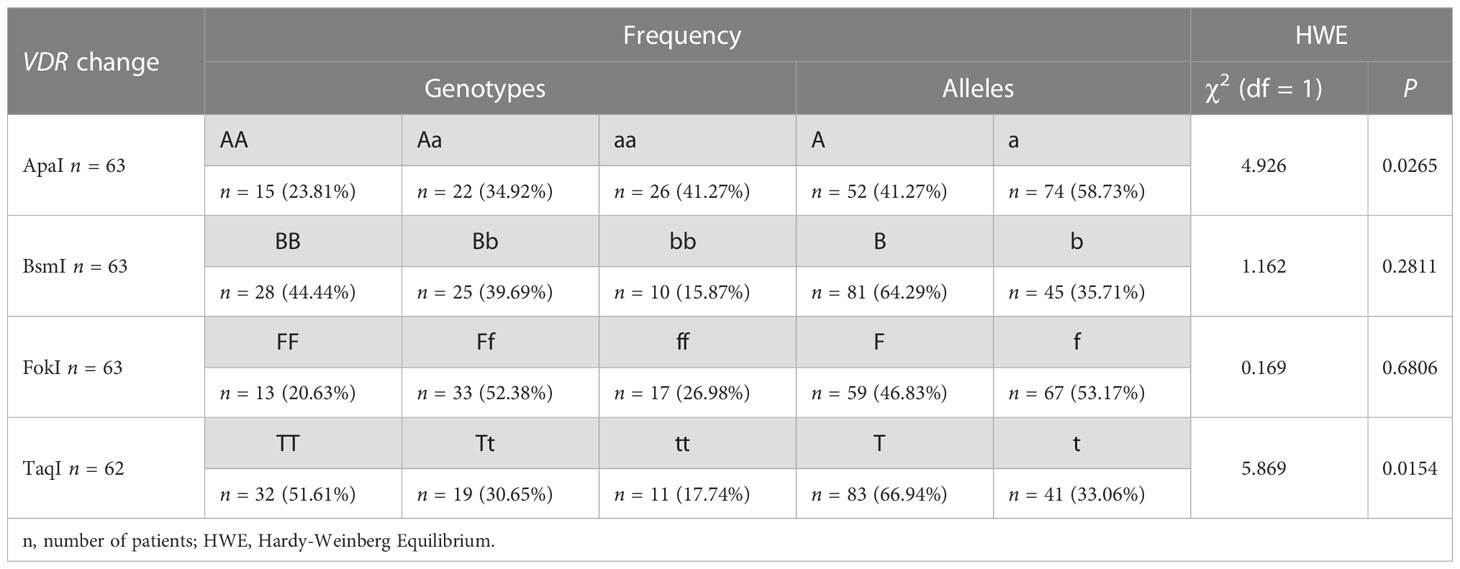
Table 1 Allele and genotype distribution for the ApaI, BsmI, FokI and TaqI polymorphisms of the VDR gene in the sample group.
The results of BMD, T-score and Z-score before and after one year of denosumab therapy in the area of the femoral neck and L1–L4 for genotypes the ApaI, BsmI, FokI, and TaqI of the VDR gene are illustrated in Figures 2–4. Moreover, the calculated differences between delta changes in densitometry parameters are presented in Supplementary Tables S3-S9 and in Table 2 (due to statistically significant results).
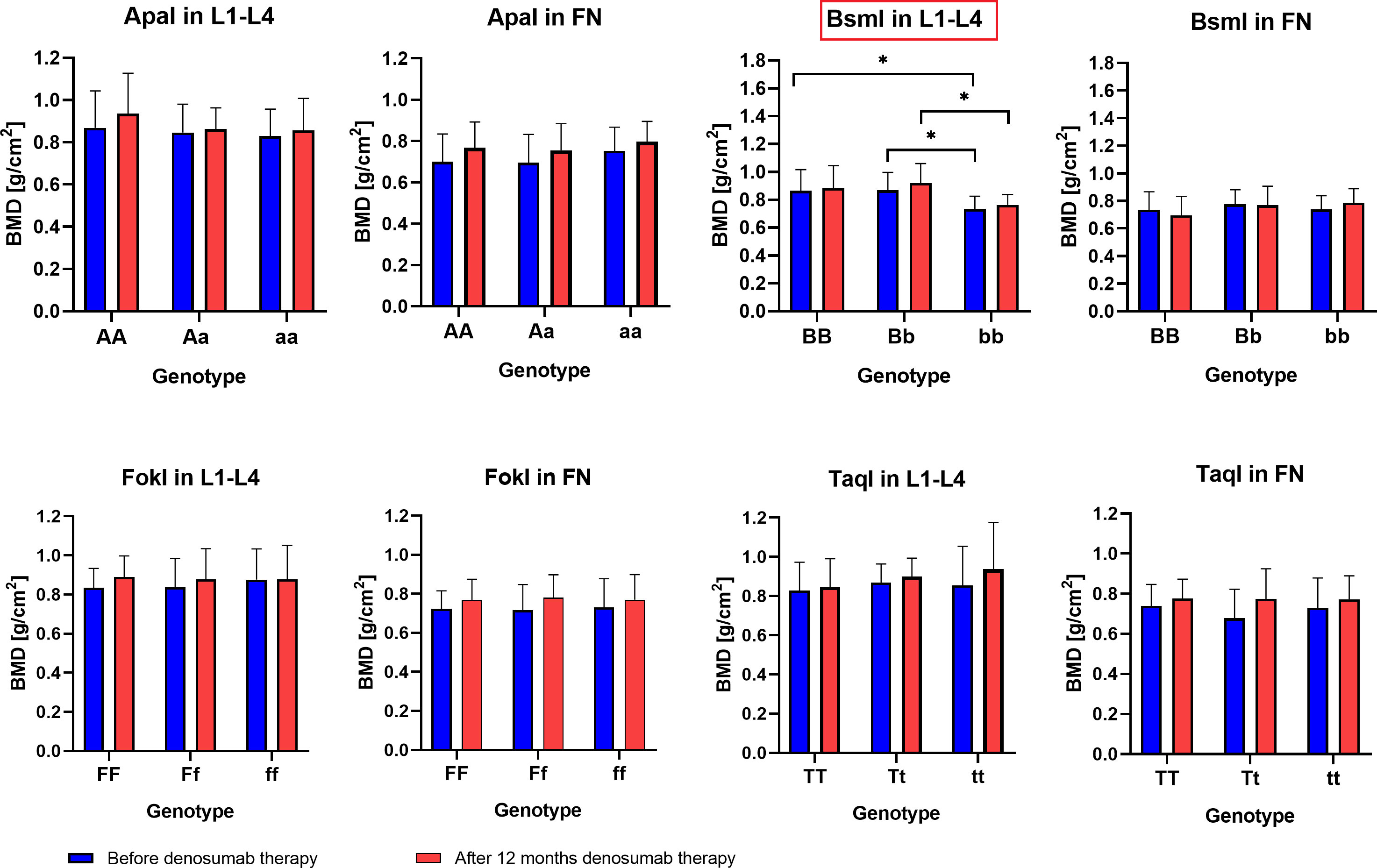
Figure 2 BMD results in the femoral neck (FN) and L1–L4 area for ApaI, BsmI, FokI, and TaqI genotypes of the VDR gene in a studied group before and after one year of denosumab therapy (*P < 0.05).
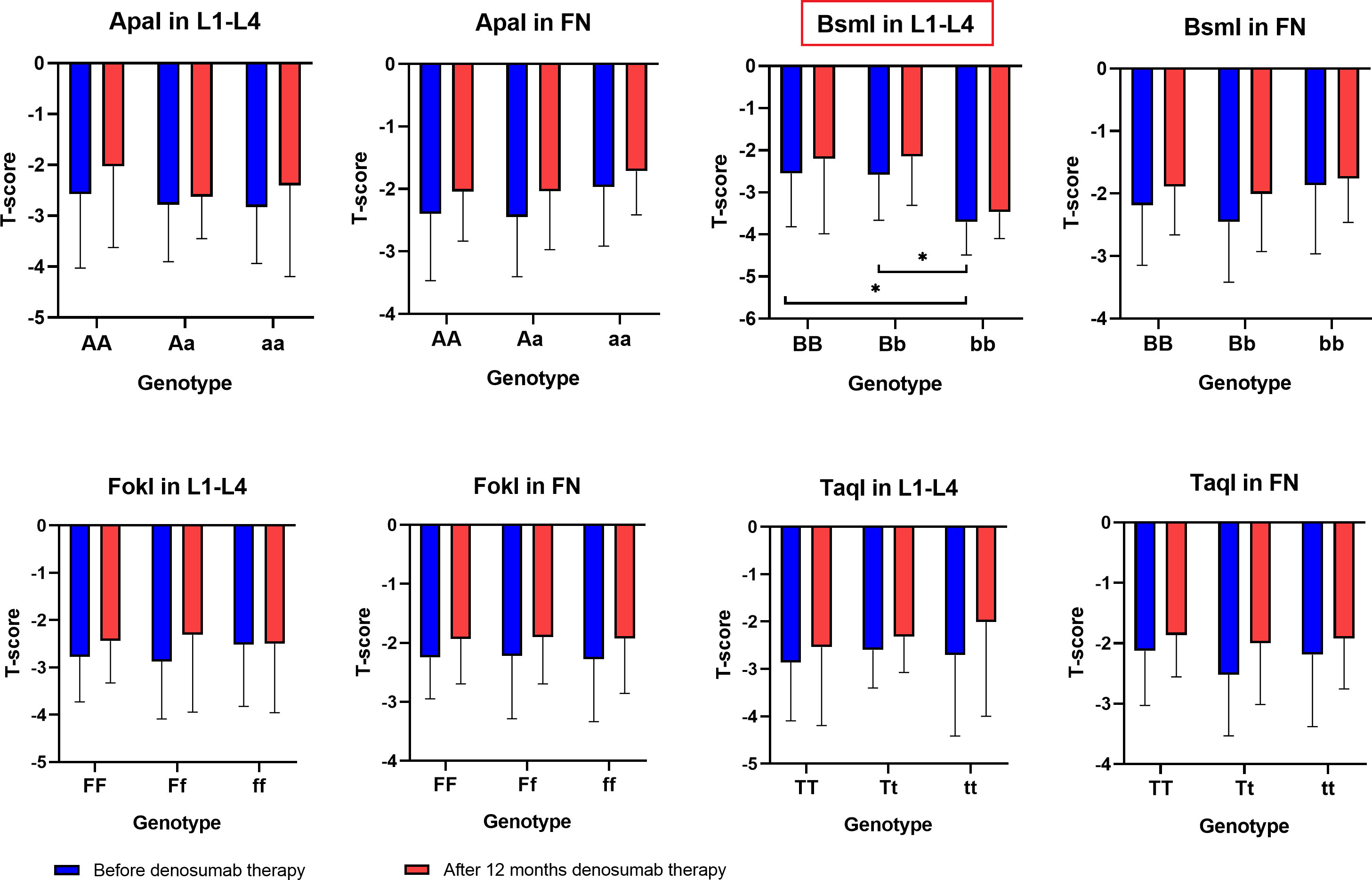
Figure 3 T-score results in the femoral neck (FN) and L1–L4 area for ApaI, BsmI, FokI, and TaqI genotypes of the VDR gene in a studied group before and after one year of denosumab therapy (*P < 0.05).
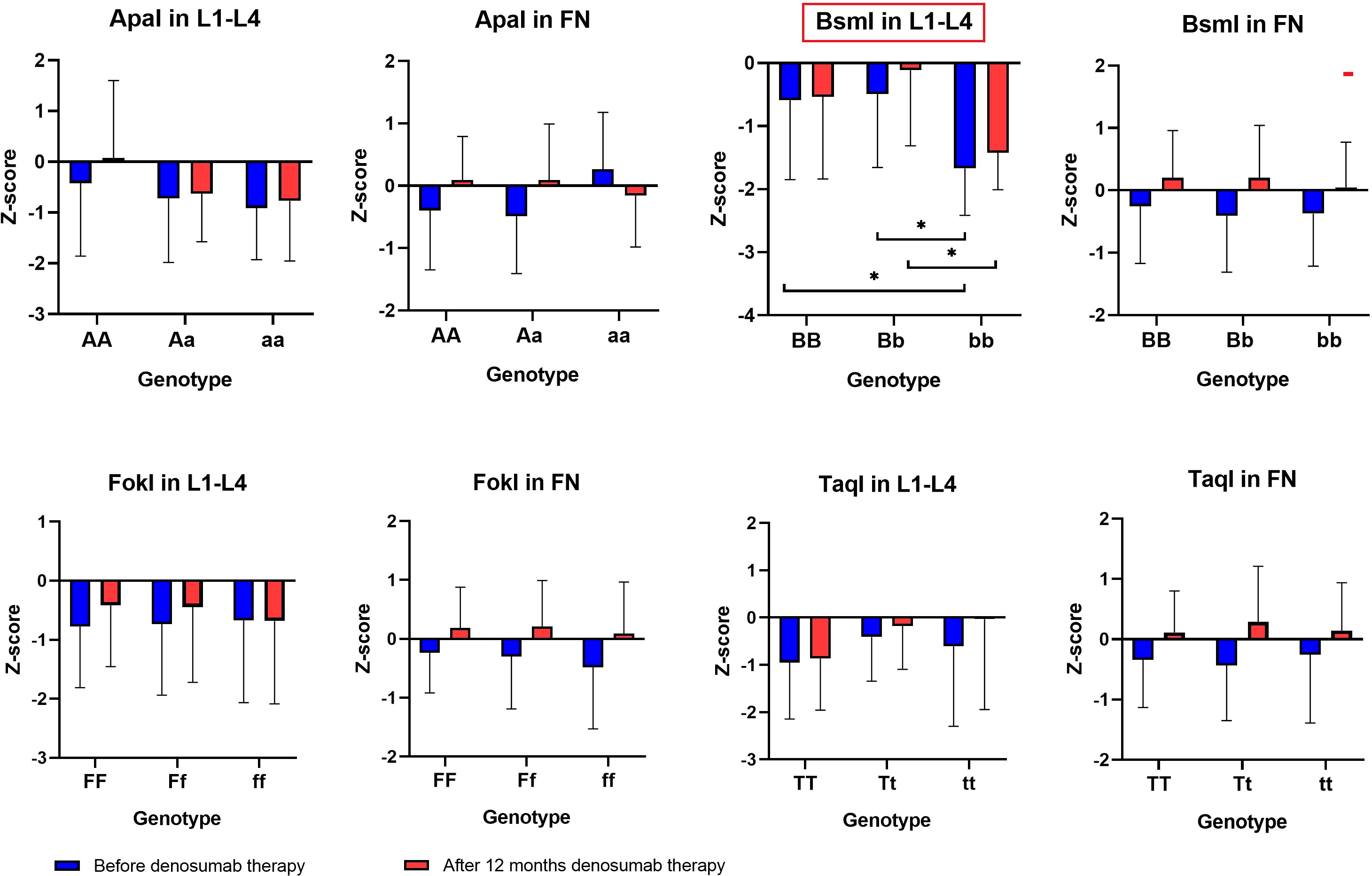
Figure 4 Z-score results in the femoral neck and L1–L4 area for ApaI, BsmI, FokI, and TaqI genotypes of the VDR gene in a studied group before and after one year of denosumab therapy (*P < 0.05).
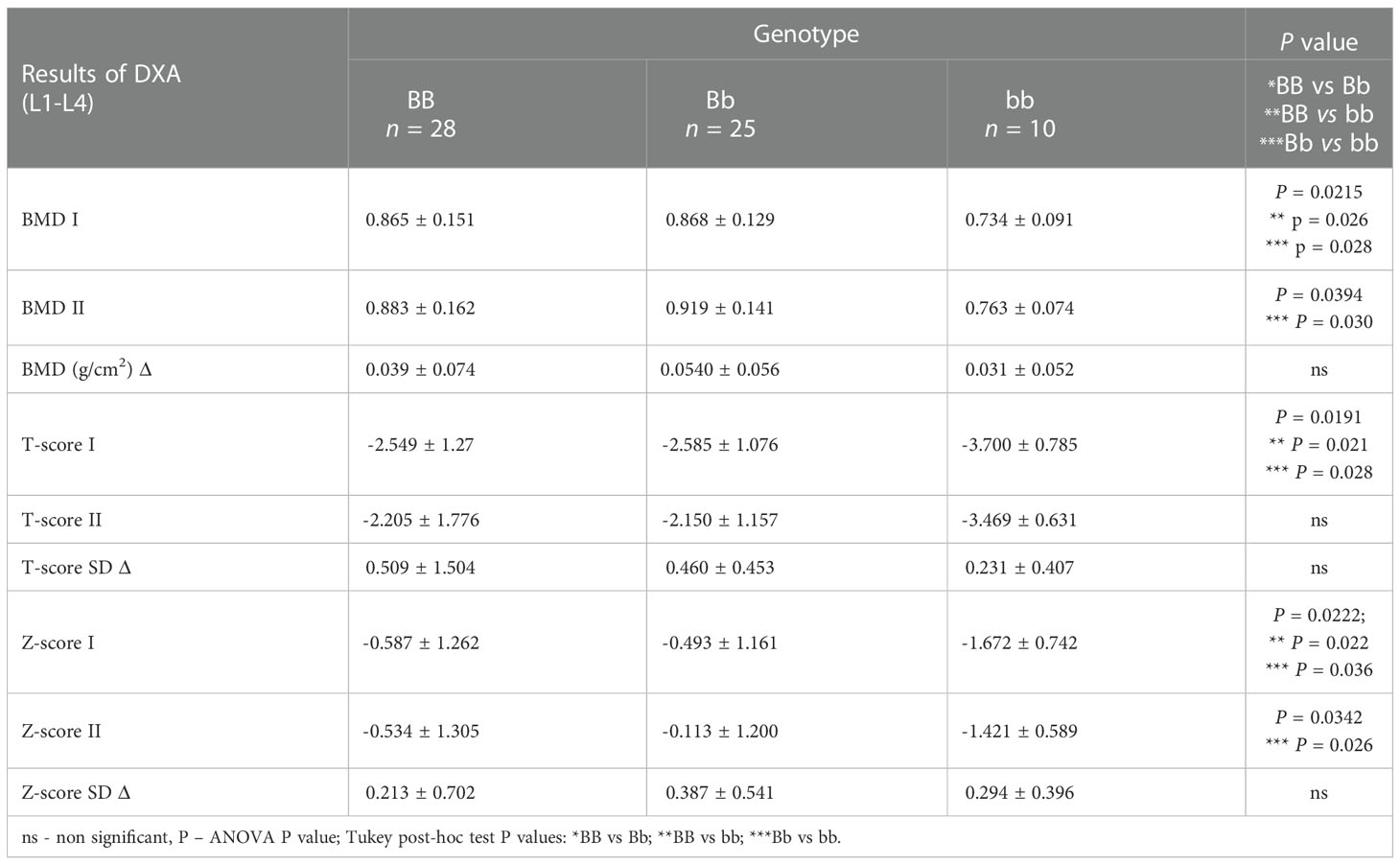
Table 2 Delta changes in DXA parameters for the VDR BsmI polymorphism in L1-L4.
It was observed that the BMD of the lumbar vertebral column bones (L1–L4) both before (P = 0.0215) and after denosumab treatment (P = 0.0394), as well as T-score values (before treatment P = 0.0191) and Z-score values (before treatment P = 0.0222 and after treatment P = 0.0342), are statistically significantly dependent on the Bsml polymorphism (Table 2). The bb genotype contributes to lower BMD and T-score/Z-score indicators values, whereas BB and Bb genotypes are characteristic for female patients with better bone DXA parameters. However, the differences (BMD Δ, T score Δ, Z score Δ) calculated from the recorded DXA parameters for lumbar vertebral column bones (L1–L4) and femoral neck bones do not show any significant correlation with genotypes for the ApaI, BsmI, FokI, and TaqI polymorphic variants of the VDR gene. Therefore, comparing DXA results before and after the sample group’s denosumab treatment indicates an upward trend for single genotypes. This trend is not statistically significant, but the vital differences between single genotypes are preserved.
4. Discussion
The molecular diagnostics of osteoporosis aim to identify polymorphisms that determine predispositions to developing this disease. Assessment of its genetic foundations is difficult in the case of a multi-gene conditioned phenotype, which is subject to additional modifications due to the strong influence of many environmental factors. Single polymorphisms of genes involved in bone tissue metabolism insignificantly influence phenotype, and only the combined effect of adverse changes in many genes is visible. Moreover, the phenotype is further affected by the interference of environmental factors such as diet, lifestyle, and hormones. Therefore, a genotype predisposed to osteoporosis is not an indicator of its occurrence. Anticipating responses to the pharmacological treatment given certain genetic conditions is becoming increasingly important. A meta-analysis of 25 studies in which 4,075 postmenopausal women in China were assessed showed a statistically significant relationship between Apal and Bsml polymorphisms of the VDR and BMD genes was observed. BMD was significantly higher in heterozygotes of the polymorphisms studied (20).
This study focuses on the analysis of 4 polymorphisms of one gene, the protein product of which is significantly involved in bone tissue metabolism. The vitamin D receptor (VDR) was one of the first genes studied for its influence on osteoporosis development. Moslai et al. observed that vitamin D concentration influences the response to denosumab treatment (14). Building on their assumptions regarding the correlation between bisphosphonate activity and vitamin D concentration, it might also be the case that vitamin D with auto/paracrine properties can be synergically active with denosumab, improving bone mineralization by stimulating osteoblast maturation and mineralization-related gene expression (14, 21). The protein of vitamin D receptors could play an essential role in this process. Given these considerations, we decided to assess four main polymorphisms (ApaI, BsmI, FokI, TaqI) of the vitamin D receptor gene for their responses to denosumab treatment. For many years, VDR gene polymorphisms have been the subject of global research that has yielded a wide range of results in different populations (9, 10). Seremak-Mrozikiewicz A. et al. showed that the T allele of the TaqI polymorphism could determine a higher risk of osteoporosis in postmenopausal women. Consequently, the t allele could have a protective effect. The presence of the A allele (ApaI polymorphism) seems to be loosely connected with susceptibility to osteoporosis (22).
Although genetic tests concerning the relation between VDR genotypes and bone quality yield contrary results, pharmacogenetic tests on individual responses to osteoporosis treatment yield more consistent and important data. Hormonal replacement therapy (HRT), used in monotherapy or in conjunction with alendronate, results in a significant increase of BMD in postmenopausal women (23, 24). Essentially, the majority of pharmacogenetic studies concentrate on response variability to HRT (25–27). Research on Italian women with postmenopausal osteoporosis addressed the influence of two polymorphisms of the VDR gene - BsmI and FokI - on BMD in response to bisphosphonate treatment or strontium ranelate treatment demonstrated that FokI, but not BsmI, can influence the response to postmenopausal osteoporosis therapy. This conclusion supports the idea that treatment should be individualized (28).
Denosumab is a fully human monoclonal antibody that counteracts the receptor activator of nuclear factor kappa beta ligand (RANKL). It diminishes the generation, function, and survival of osteoclasts and is used to treat postmenopausal women with osteoporosis with increased or high fracture risk. During the 3-year FREEDOM study, 60 mg of denosumab administered subcutaneously every six months significantly decreased the number of vertebral column fractures (68%), hip fractures (40%), and non-vertebral fractures (20%). It also increased BMD and decreased the activity of bone turnover markers to a greater extent than placebos in postmenopausal women with osteoporosis (29). This research was continued through a comparison of the effects of denosumab in postmenopausal women with osteoporosis over a 5-year period to a placebo group treated for only three years. Five years of therapy decreased the activity of bone turnover markers (BTM) and increased BMD, which was associated with a low number of fractures and a favorable risk-benefit ratio (30).
As in many other investigations, our study revealed that in all women with postmenopausal osteoporosis, one year of denosumab therapy was beneficial and resulted in increased BMD. During the treatment, one new bone fracture was reported in one woman. In randomized studies, 60 mg of denosumab significantly reduced the fracture risk compared to placebo and bisphosphonate treatment, and decreased the bone turnover marker value, while simultaneously increasing the BMD (2, 31–39). Nevertheless, recent observations have shown that discontinuation of denosumab treatment is associated with decreased BMD and bone fracture risk. Popp AW et al. proved that termination of denosumab treatment after long-term exposure resulted in a significant BMD decrease at all measured sites, which suggests that treatment duration can predict the speed and volume of bone loss (40). Moreover, another study observed vertebral fractures after discontinuation of denosumab (41). Therefore, the search for a genetically conditioned response to denosumab treatment therefore appears justified concerning long-term post-treatment.
Our results did not reveal statistically significant differences between delta changes (after one year of denosumab treatment) in densitometric parameters in the area of the femoral neck and L1–L4 for the following single genotypes of the VDR gene: AA, Aa and aa Apa; BB, Bb and bb BsmI; FF, Ff and ff FokI; and TT, Tt and tt TaqI. However, in the case of the Bsml polymorphism, it was interestingly observed that female patients with BB and Bb genotypes have statistically significantly higher values of BMD and T-score/Z-score indicators, which persist after a year of denosumab treatment. We can claim that the Bsml polymorphism determines better bone status in female patients, which continues over one year of treatment with denosumab. Though this observation was not the primary objective, it can help guide the denosumab treatment process. Further studies should verify this conclusion by prolonging the observation period and increasing the sample group size. Focusing on studies from recent years regarding the impact of the BsmI variant of the VDR gene in women with postmenopausal osteoporosis, regardless of the treatment, the results are discrepant. On the one hand, favorable relationships between the bb variants and bone density were observed, which partly confirms the results of our research. Namely, other Polish researchers showed that women with the bb genotype presented lower BMD values of the hip compared to patients with the BB or Bb genotypes (42). In our results, the dependencies concerned the lumbar vertebral column (L1–L4) but indicated a positive impact of ‘BB’ or ‘Bb’ genotypes on DXA parameters. Pederera-Canal et al., after five years of observation of patients with postmenopausal osteoporosis, found a significant modification of BMD at the femoral neck based on the rs1544410 genotype (BB vs. Bb) i. e. the BB group gained more BMD than the Bb group (43). On the other hand, many recent studies have not shown a relationship between the BsmI polymorphism and bone density in Spanish postmenopausal women (44) or that this variant was related to an increased risk of osteoporosis (45–47).
Moreover, polymorphism studies of genes other than VDR genes involved in bone metabolism - especially the metabolic pathway RANKL-RANK-OPG, influenced by the studied drug, denosumab – may prove more accurate for individualized antiosteoporotic treatment. Increasing the sample group size and extending the observation period would be a valuable addition to the study. Furthermore, it is worth considering studies of other genes, especially from the RANKL-RANK-OPG metabolic pathway.
5. Conclusions
In the group of 63 Polish women with postmenopausal osteoporosis, BB and Bb genotypes of the Bsml polymorphism determine higher DXA parameter values both before and after biological treatment. No statistically significant differences between the ApaI, BsmI, FokI, and TaqI polymorphisms of the VDR gene in response to one-year denosumab therapy were observed.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Bioethical Committee of the Poznan University of Medical Sciences. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Conceptualization, AW, MM, and IK-K; methodology, AW, MS-Z, MMi, MK-R, MM, and IK-K; investigation, AW and IK-K; writing—original draft preparation, AW, MS-Z, AER, AMR, and KS; writing—review and editing, RS, AD, and IK-K; visualization, MS-Z; supervision, IK-K; project administration, AD. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
In memory of: the late Professor Wanda Horst-Sikorska, who supported us with her ideas, knowledge and kindness. The authors give thanks to Berlineo - The Translation Company for professional translation and preparation of the English version of the article. Ms Anna Maria Rychter, Ms Kinga Skoracka and Ms Alicja Ewa Ratajczak are participants of STER Internationalisation of Doctoral Schools Programme from NAWA Polish National Agency for Academic Exchange No. PPI/STE/2020/1/00014/DEC/02.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.1063762/full#supplementary-material
References
1. Fernandez C, Tennyson J, Priscilla AS. Osteoporosis and its association with vitamin d receptor, oestrogen α receptor, parathyroid receptor and collagen type I alpha receptor gene polymorphisms with bone mineral density: A pilot study from south Indian postmenopausal women of Tamil nadu. Biochem Genet (2022) 60(6):2015–36. doi: 10.1007/s10528-022-10197-5
2. Cummings SR, San Martin J, McClung MR, Siris ES, Eastell R, Reid IR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med (2009) 361(8):756–65. doi: 10.1056/NEJMoa0809493
3. Tang CH. Osteoporosis: From molecular mechanisms to therapies 2.0. Int J Mol Sci (2020) 21(21). doi: 10.3390/ijms21218005
4. Pang KL, Low NY, Chin KY. A review on the role of denosumab in fracture prevention. Drug Des Devel Ther (2020) 14:4029–51. doi: 10.2147/DDDT.S270829
5. Wu F, Zhou D, Shen G, Cui Y, Lv Q, Wei F. Association of VDR and OPG gene polymorphism with osteoporosis risk in Chinese postmenopausal women. Climacteric (2019) 22(2):208–12. doi: 10.1080/13697137.2018.1554643
7. Hildebrand GK, Kasi A. Denosumab. W. In: StatPearls. Treasure Island (FL: StatPearls Publishing (2020). Available at: http://www.ncbi.nlm.nih.gov/books/NBK535388/.
8. Polyzos SA, Makras P, Tournis S, Anastasilakis AD. Off-label uses of denosumab in metabolic bone diseases. Bone (2019) 129:115048. doi: 10.1016/j.bone.2019.115048
9. Uitterlinden AG, Ralston SH, Brandi ML, Carey AH, Grinberg D, Langdahl BL, et al. The association between common vitamin d receptor gene variations and osteoporosis: A participant-level meta-analysis. Ann Intern Med (2006) 145(4):255–64. doi: 10.7326/0003-4819-145-4-200608150-00005
10. Horst-Sikorska W, Dytfeld J, Wawrzyniak A, Marcinkowska M, Michalak M, Franek E, et al. Vitamin d receptor gene polymorphisms, bone mineral density and fractures in postmenopausal women with osteoporosis. Mol Biol Rep (2013) 40(1):383–90. doi: 10.1007/s11033-012-2072-3
11. Peacock M, Turner CH, Econs MJ, Foroud T. Genetics of osteoporosis. Endocr Rev (2002) 23(3):303–26. doi: 10.1210/edrv.23.3.0464
12. Ralston SH, Uitterlinden AG. Genetics of osteoporosis. Endocr Rev (2010) 31(5):629–62. doi: 10.1210/er.2009-0044
13. Valdivielso JM, Fernandez E. Vitamin d receptor polymorphisms and diseases. Clin Chim Acta (2006) 371(1–2):1–12. doi: 10.1016/j.cca.2006.02.016
14. Mosali P, Bernard L, Wajed J, Mohamed Z, Ewang M, Moore A, et al. Vitamin d status and parathyroid hormone concentrations influence the skeletal response to zoledronate and denosumab. Calcif Tissue Int (2014) 94(5):553–9. doi: 10.1007/s00223-014-9840-0
15. Herrero S, Pico Y. Treatments for post-menopausal osteoporotic women, what’s new? How can we manage long-term treatment? Eur J Pharmacol (2016) 779:8–21. doi: 10.1016/j.ejphar.2016.02.053
16. Cairoli E, Eller-Vainicher C, Chiodini I. Update on denosumab in the management of postmenopausal osteoporosis: Patient preference and adherence. Int J Womens Health (2015) 7:833–9. doi: 10.2147/IJWH.S75681
17. Słomski R, Szalata M, Wolko Ł, Wielgus K. DNA Isolation. In: Słomski R, editor. Analysis of DNA- theory and practice. Poznań: Life Sciences Publishing House (2011). p. 44–53.
18. Horst-Sikorska W, Kalak R, Wawrzyniak A, Marcinkowska M, Celczynska-Bajew L, Slomski R. Association analysis of the polymorphisms of the VDR gene with bone mineral density and the occurrence of fractures. J Bone Miner Metab (2007) 25(5):310–9. doi: 10.1007/s00774-007-0769-5
19. Francis RM, Harrington F, Turner E, Papiha SS, Datta HK. Vitamin d receptor gene polymorphism in men and its effect on bone density and calcium absorption. Clin Endocrinol (Oxf). (1997) 46(1):83–6. doi: 10.1046/j.1365-2265.1997.d01-1735.x
20. Li Y, Xi B, Li K, Wang C. Association between vitamin d receptor gene polymorphisms and bone mineral density in Chinese women. Mol Biol Rep 1 maj (2012) 39(5):5709–17. doi: 10.1007/s11033-011-1380-3
21. van Driel M, Koedam M, Buurman CJ, Hewison M, Chiba H, Uitterlinden AG, et al. Evidence for auto/paracrine actions of vitamin d in bone: 1alpha-hydroxylase expression and activity in human bone cells. FASEB J (2006) 20(13):2417–9. doi: 10.1096/fj.06-6374fje
22. Seremak-Mrozikiewicz A, Drews K, Pm M, Bartkowiak-Wieczorek J, Marcinkowska M, Wawrzyniak A, et al. Correlation of vitamin d receptor gene (VDR) polymorphism with osteoporotic changes in polish postmenopausal women. Neuro Endocrinol Lett (2009) 30(4):540–6.
23. Mohammadi Z, Fayyazbakhsh F, Ebrahimi M, Amoli MM, Khashayar P, Dini M, et al. Association between vitamin d receptor gene polymorphisms (Fok1 and Bsm1) and osteoporosis: A systematic review. J Diabetes Metab Disord (2014) 13(1):98. doi: 10.1186/s40200-014-0098-x
24. Giguère Y, Dodin S, Blanchet C, Morgan K, Rousseau F. The association between heel ultrasound and hormone replacement therapy is modulated by a two-locus vitamin d and estrogen receptor genotype. J Bone Miner Res (2000) 15(6):1076–84. doi: 10.1359/jbmr.2000.15.6.1076
25. Morrison NA, Qi JC, Tokita A, Kelly PJ, Crofts L, Nguyen TV, et al. Prediction of bone density from vitamin d receptor alleles. Nature (1994) 367(6460):284–7. doi: 10.1038/367284a0
26. Lindsay R, Cosman F, Lobo RA, Walsh BW, Harris ST, Reagan JE, et al. Addition of alendronate to ongoing hormone replacement therapy in the treatment of osteoporosis: A randomized, controlled clinical trial. J Clin Endocrinol Metab (1999) 84(9):3076–81. doi: 10.1210/jcem.84.9.5989
27. Tiraş MB, Noyan V, Yildiz A, Yildirim M, Daya S. Effects of alendronate and hormone replacement therapy, alone or in combination, on bone mass in postmenopausal women with osteoporosis: A prospective, randomized study. Hum Reprod (2000) 15(10):2087–92. doi: 10.1093/humrep/15.10.2087
28. Palomba S, Orio F, Colao A, di Carlo C, Sena T, Lombardi G, et al. Effect of estrogen replacement plus low-dose alendronate treatment on bone density in surgically postmenopausal women with osteoporosis. J Clin Endocrinol Metab (2002) 87(4):1502–8. doi: 10.1210/jcem.87.4.8323
29. Watts NB, Brown JP, Papapoulos S, Lewiecki EM, Kendler DL, Dakin P, et al. Safety observations with 3 years of denosumab exposure: Comparison between subjects who received denosumab during the randomized FREEDOM trial and subjects who crossed over to denosumab during the FREEDOM extension. J Bone Mineral Res (2017) 32(7):1481–5. doi: 10.1002/jbmr.3119
30. Papapoulos S, Chapurlat R, Libanati C, Brandi ML, Brown JP, Czerwiński E, et al. Five years of denosumab exposure in women with postmenopausal osteoporosis: Results from the first two years of the FREEDOM extension. J Bone Miner Res (2012) 27(3):694–701. doi: 10.1002/jbmr.1479
31. Kurabayashi T, Tomita M, Matsushita H, Yahata T, Honda A, Takakuwa K, et al. Association of vitamin d and estrogen receptor gene polymorphism with the effect of hormone replacement therapy on bone mineral density in Japanese women. Am J Obstet Gynecol. (1999) 180(5):1115–20. doi: 10.1016/S0002-9378(99)70603-4
32. Simsek M, Cetin Z, Bilgen T, Taskin O, Luleci G, Keser I. Effects of hormone replacement therapy on bone mineral density in Turkish patients with or without COL1A1 Sp1 binding site polymorphism. J Obstet Gynaecol Res (2008) 34(1):73–7. doi: 10.1111/j.1447-0756.2007.00680.x
33. Conti V, Russomanno G, Corbi G, Toro G, Simeon V, Filippelli W, et al. A polymorphism at the translation start site of the vitamin d receptor gene is associated with the response to anti-osteoporotic therapy in postmenopausal women from southern Italy. Int J Mol Sci (2015) 16(3):5452–66. doi: 10.3390/ijms16035452
34. Brown JP, Prince RL, Deal C, Recker RR, Kiel DP, de Gregorio LH, et al. Comparison of the effect of denosumab and alendronate on BMD and biochemical markers of bone turnover in postmenopausal women with low bone mass: A randomized, blinded, phase 3 trial. J Bone Miner Res (2009) 24(1):153–61. doi: 10.1359/jbmr.0809010
35. Kendler DL, Roux C, Benhamou CL, Brown JP, Lillestol M, Siddhanti S, et al. Effects of denosumab on bone mineral density and bone turnover in postmenopausal women transitioning from alendronate therapy. J Bone Miner Res (2010) 25(1):72–81. doi: 10.1359/jbmr.090716
36. Roux C, Hofbauer LC, Ho PR, Wark JD, Zillikens MC, Fahrleitner-Pammer A, et al. Denosumab compared with risedronate in postmenopausal women suboptimally adherent to alendronate therapy: Efficacy and safety results from a randomized open-label study. Bone (2014) 58:48–54. doi: 10.1016/j.bone.2013.10.006
37. Recknor C, Czerwinski E, Bone HG, Bonnick SL, Binkley N, Palacios S, et al. Denosumab compared with ibandronate in postmenopausal women previously treated with bisphosphonate therapy: A randomized open-label trial. Obstet Gynecol. (2013) 121(6):1291–9. doi: 10.1097/AOG.0b013e318291718c
38. Miller PD, Pannacciulli N, Brown JP, Czerwinski E, Nedergaard BS, Bolognese MA, et al. Denosumab or zoledronic acid in postmenopausal women with osteoporosis previously treated with oral bisphosphonates. J Clin Endocrinol Metab (2016) 101(8):3163–70. doi: 10.1210/jc.2016-1801
39. Fahrleitner-Pammer A, Papaioannou N, Gielen E, Feudjo Tepie M, Toffis C, Frieling I, et al. Factors associated with high 24-month persistence with denosumab: Results of a real-world, non-interventional study of women with postmenopausal osteoporosis in Germany, Austria, Greece, and Belgium. Arch Osteoporos (2017) 12(1):58. doi: 10.1007/s11657-017-0351-2
40. Popp AW, Varathan N, Buffat H, Senn C, Perrelet R, Lippuner K. Bone mineral density changes after 1 year of denosumab discontinuation in postmenopausal women with long-term denosumab treatment for osteoporosis. Calcif Tissue Int (2018) 103(1):50–4. doi: 10.1007/s00223-018-0394-4
41. Anastasilakis AD, Tournis S, Yavropoulou MP, Polyzos SA, Makras P. Multiple vertebral fractures following denosumab discontinuation: Are we exaggerating? Calcif Tissue Int (2018) 103(1):107–8. doi: 10.1007/s00223-018-0409-1
42. Ae S, I M, A W, I R, E S, E Ż. VDR polymorphisms effect on bone mineral density in polish postmenopausal women. In: Homo : Internationale zeitschrift fur die vergleichende forschung am menschen, vol. 72. (2021). Available at: https://pubmed.ncbi.nlm.nih.gov/34296242/.
43. Pedrera-Canal M, Moran JM, Vera V, Roncero-Martin R, Lavado-Garcia JM, Aliaga I, et al. Lack of influence of vitamin d receptor BsmI (rs1544410) polymorphism on the rate of bone loss in a cohort of postmenopausal Spanish women affected by osteoporosis and followed for five years. PloS One (2015) 10(9):e0138606. doi: 10.1371/journal.pone.0138606
44. Moran JM, Pedrera-Canal M, Rodriguez-Velasco FJ, Vera V, Lavado-Garcia JM, Fernandez P, et al. Lack of association of vitamin d receptor BsmI gene polymorphism with bone mineral density in Spanish postmenopausal women. PeerJ (2015) 3:e953. doi: 10.7717/peerj.953
45. Marozik PM, Tamulaitiene M, Rudenka E, Alekna V, Mosse I, Rudenka A, et al. Association of vitamin d receptor gene variation with osteoporosis risk in belarusian and Lithuanian postmenopausal women. Front Endocrinol (Lausanne). (2018) 9:305. doi: 10.3389/fendo.2018.00305
46. Marozik P, Rudenka A, Kobets K, Rudenka E. Vitamin d status, bone mineral density, and VDR gene polymorphism in a cohort of belarusian postmenopausal women. Nutrients (2021) 13(3):837. doi: 10.3390/nu13030837
Keywords: VDR gene polymorphism, denosumab therapy, postmenopausal osteoporosis, bone fracture, osteoporosis
Citation: Wawrzyniak A, Skrzypczak-Zielińska M, Michalak M, Kaczmarek-Ryś M, Ratajczak AE, Rychter AM, Skoracka K, Marcinkowska M, Słomski R, Dobrowolska A and Krela-Kaźmierczak I (2023) Does the VDR gene polymorphism influence the efficacy of denosumab therapy in postmenopausal osteoporosis? Front. Endocrinol. 13:1063762. doi: 10.3389/fendo.2022.1063762
Received: 07 October 2022; Accepted: 21 December 2022;
Published: 13 January 2023.
Edited by:
Giovanni Lombardi, Galeazzi Orthopedic Institute (IRCCS), ItalyReviewed by:
Shaden Haddad, Damascus University, SyriaDina Keumala Sari, Universitas Sumatera Utara, Indonesia
Copyright © 2023 Wawrzyniak, Skrzypczak-Zielińska, Michalak, Kaczmarek-Ryś, Ratajczak, Rychter, Skoracka, Marcinkowska, Słomski, Dobrowolska and Krela-Kaźmierczak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alicja Ewa Ratajczak, YWxpY2phZXdhcmF0YWpjemFrQGdtYWlsLmNvbQ==