
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 06 December 2022
Sec. Pediatric Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1045628
This article is part of the Research TopicEndocrine and Cardiometabolic Alterations in Pediatric Patients with Chronic DiseasesView all 7 articles
 Lilian Nkinda1*
Lilian Nkinda1* Eliud Buberwa1
Eliud Buberwa1 Peter Memiah2Alieth Ntagalinda1Martin George1
Peter Memiah2Alieth Ntagalinda1Martin George1 Frank Msafiri1
Frank Msafiri1 Agricola Joachim1
Agricola Joachim1 Mtebe Majigo1Kaushik Ramaiya3
Mtebe Majigo1Kaushik Ramaiya3 Bruno Sunguya4
Bruno Sunguya4Objective: This study assessed impaired fasting glucose and associated factors among perinatally HIV-infected adolescents and youths in Dar es salaam Tanzania.
Background: Impaired fasting glucose is a marker of heightened risk for developing type 2 diabetes among perinatally HIV-infected individuals. Therefore, identifying individuals at this stage is crucial to enable early intervention. Therefore, we assessed impaired fasting glucose (IFG) and associated factors among perinatally HIV-infected population in Dar es salaam Tanzania.
Methods: A cross-sectional study was conducted among 152 adolescents and youth attending HIV clinic at Muhimbili National Hospital and Infectious Disease Centre from July to August 2020. Fasting blood glucose (>8 hours) was measured using one-touch selects LifeScan, CA, USA. We also examined C-Reactive Protein and interleukin-6 inflammatory biomarkers in relation to impaired fasting glucose (IFG). Associations between categorical variables were explored using Chi-square, and poison regression with robust variance was used to calculate the prevalence ratios.
Results: Of the 152 participants, the majority were male (n=83[54.6%]), and the median age was 15(14-18) years. Overweight or obesity was prevalent in 16.4%, while more than one in ten (13.2%) had high blood pressure (≥149/90mmHg). All participants were on antiretroviral therapy (ART); 46% had used medication for over ten years, and about one in three had poor medication adherence. Among the recruited participants, 29% had impaired fasting glucose. The odds of IFG were two times higher in males compared to females (PR, 2.07, 95% CI 1.19 -3.59 p=0.001). Moreover, we found with every increase of Interleukin 6 biomarker there was a 1.01 probability increase of impaired fasting glucose (PR, 1.01, 95% CI 1.00 – 1.02 p=0.003).
Conclusion: About one in three perinatally HIV-infected youths had impaired fasting glucose in Dar es Salaam, Tanzania, with males bearing the biggest brunt. Moreover, with every increase of 1.101 of the probability of having IFG increased. This calls for urgent measures to interrupt the progression to diabetes disease and prevent the dual burden of disease for this uniquely challenged population.
Impaired fasting glucose (IFG) is a type of pre-diabetes where an individual’s blood sugar levels during fasting are consistently above the normal range but below the diagnostic cut-off for type 2 diabetes mellitus (1). The burden of diabetes mellitus type 2 is higher in lower- and middle-income countries, and it is estimated that about a 90% increment of new cases will be from sub-Saharan Africa alone by the year 2030 (2). This increment will cripple economic progress and burden the country’s already overstretched health system. In addition, IFG has a higher predictive value for type 2 diabetes (3). Therefore, targeting those at the highest risk is the most cost-effective strategy for limited resources countries (4).
HIV-infected adults have a five-fold risk of developing diabetes mellitus compared to their HIV negative counter (5). It is also known that perinatally infected youth (acquired infection during pregnancy, birth or breastfeeding) have an excess risk of non-AIDS defining illnesses compared to adults or otherwise behaviorally HIV-infected youth and adolescents (6). Reports on the prevalence of insulin resistance, among HIV infected adolescents a condition preceding pre-diabetes and full-blown diabetes disease ranges from 6.5-34% (7–9). In contrast studies on perinatally infected adolescents and young adults evidences a higher rate (18-43% (10–12). The HIV infection on the immature immune system, long-term antiretroviral therapy (ART) exposure, and high HIV-related inflammation following poor adherence to ART are associated with this increased risk (13). As they transition to adulthood, the incidence of diabetes for this population is likely to surpass that of the current behaviorally infected adults.
Interventions and disease interrupters during the pre-diabetes stage can prevent or delay the occurrence of Type 2 diabetes (14). Disease interrupters such as rigorous screening, use of anti-inflammatory agents, and lifestyle changes have been implemented among the adult HIV population (15, 16). However, the burden of non-AIDS events is sparsely characterized among HIV-infected adolescents and youth, limiting the application of these interventions for this population. Furthermore, most diabetes risk behaviors, including poor diets and sedentary lifestyles, begin during adolescence (17). Therefore, reinforcing healthier choices and protective measures during this critical period can significantly change the health trajectory into adulthood and reduce the burden of comorbidity among the HIV population (17). However, evidence is unavailable on the burden and characteristics of IFG among perinatally HIV-infected youths in a high HIV prevalence context like Tanzania. This study was therefore conducted to address this gap.
This cross-sectional study was conducted among HIV-positive adolescents and young adults attending HIV care and treatment centers at Infectious Disease Center (IDC) and Muhimbili National Hospital (MNH), both located in Ilala district, Dar es salaam Tanzania. These facilities jointly serve 234 active adolescents and youth who attend from all the four districts of the region.
The study population included HIV-infected individuals aged between 10 to 21 years who had fasted for more than 8 hours. Pregnant participants were excluded because of the possibility of pregnancy affecting glucose levels and participants on anti-inflammatory drugs in the last three months were excluded from this study, because it would interfere with the results inflammatory biomarkers levels.
The minimum sample size was 152 participants, calculated using Fisher’s formula. This study enrolled all adolescents who met the inclusion criteria and where willing to assented to participate in the study, but also had written informed consent from their parents. Informed consent for participants was obtained for participants 18 years old and above.
The outcome variable was Impaired fasting glucose, this was defined as fasting glucose levels above 6.1 but less than 7mmol/L (18). Body mass index (BMI) was weight divided by height square (kg/m²) and classified as underweight, overweight, and obese. Under-weight (BMI < 18 kg/m2), normal (BMI ≥ 18 kg/m2 and ≤ 25 kg/m2), overweight (BMI > 25 kg/m2and < 30 kg/m2, and obese (BMI ≥ 30 kg/m2). In addition, blood pressure was considered high if BP ≥140/90mm/Hg (19). The adherence level at the last visit was extracted from the HIV ART card and recorded on a study tool as assessed by the attending Health care provider whether “GOOD”, MODERATE” or “POOR”. Good adherence referred to ≥95% adherence if less than three pills are missed, fair refers to 80–95% if 3–12 missed while poor adherence is less than 80% if 12 pills missed, all within one month of period (30days) (20). Smoking and alcohol consumption were determined if they had been used in the last 30 days from the day of interview. Occupation was asked to determine if the participants were still only students, or they were involved in income generating activities of moderate intensity (office work) or vigorous intensity causing excessive sweating (hard work). Physical activity was determined if one walked/cycled for at least 10 minutes daily (19).
The study used structured data collection tools (annex 1) to gather demographic characteristics such as age, sex, family history of diabetes (first degree relative), and behavioral risk factors like alcohol consumption and smoking. In addition, HIV-related factors included duration of ART use, ART adherence, and HIV viral load. Also, we conducted physical measurements for blood pressure, weight, and height. Blood pressure was measured twice on the left arm of the seated and relaxed participant using a sphygmomanometer. The body weight and height were measured in light clothes without footwear.
Four mls of EDTA blood was collected from every eligible adolescent. First, fasting glucose was measured using One-touch select © LifeScan, Inc AW 06716201A, whose 100% of glucose results of <100 mg/dL were within a bias of ±15 mg/dL, and 99.5% of results ≥100 mg/dL had a bias within the ±15% limit (21). Afterward, plasma was aliquoted and stored under −20°c awaiting inflammatory markers; Interleukin 6 and C-reactive Protein.
C-Reactive Protein and Interleukin 6 biomarkers were analyzed in the lab as described on this publication. CRP concentration above 3.1ng/liter will be considered high. The concentration of IL-6 beyond five pg/ml will be considered high (19).
Descriptive statistics were performed, proportions were reported for categorical variables while median and interquartile range (IQR) for skewed data. To explore association for Impaired fasting glucose a chi-square test was used. The dependent variables considered for the analysis was in binary variables. For variables with the expected numbers of observations per cell less than 5, the fisher’s exact test was used in estimating the p-value. Variables with a p-value less than 0.2 were subjected to poison regression with robust variance to analyze the prevalence ratios. A p-value less than 0.05 was considered statistically significant.
The characteristics of 152 study participants are summarized in Table 1. The median age was 15 years, with most of the participants being male (n=83[54.6%]) and 118 (77.6%) being students. Eighty-seven (57.2%) participants had completed their primary education. A total of 67(42.1%) had a family history of diabetes, 67(44.1%) were regularly performing physical activities, 7(4.6%) were smokers, and 16 (10.5%) were alcohol consumers. Twenty participants (13.2%) had high blood pressure, and 25(16.4%) were overweight/obese. About 45(29.6%) participants had poor ART adherence, 39(25.7%) had a high viral load above 5000 copies/ml, and 70(46.1%) participants had used antiretroviral drugs for above ten years.
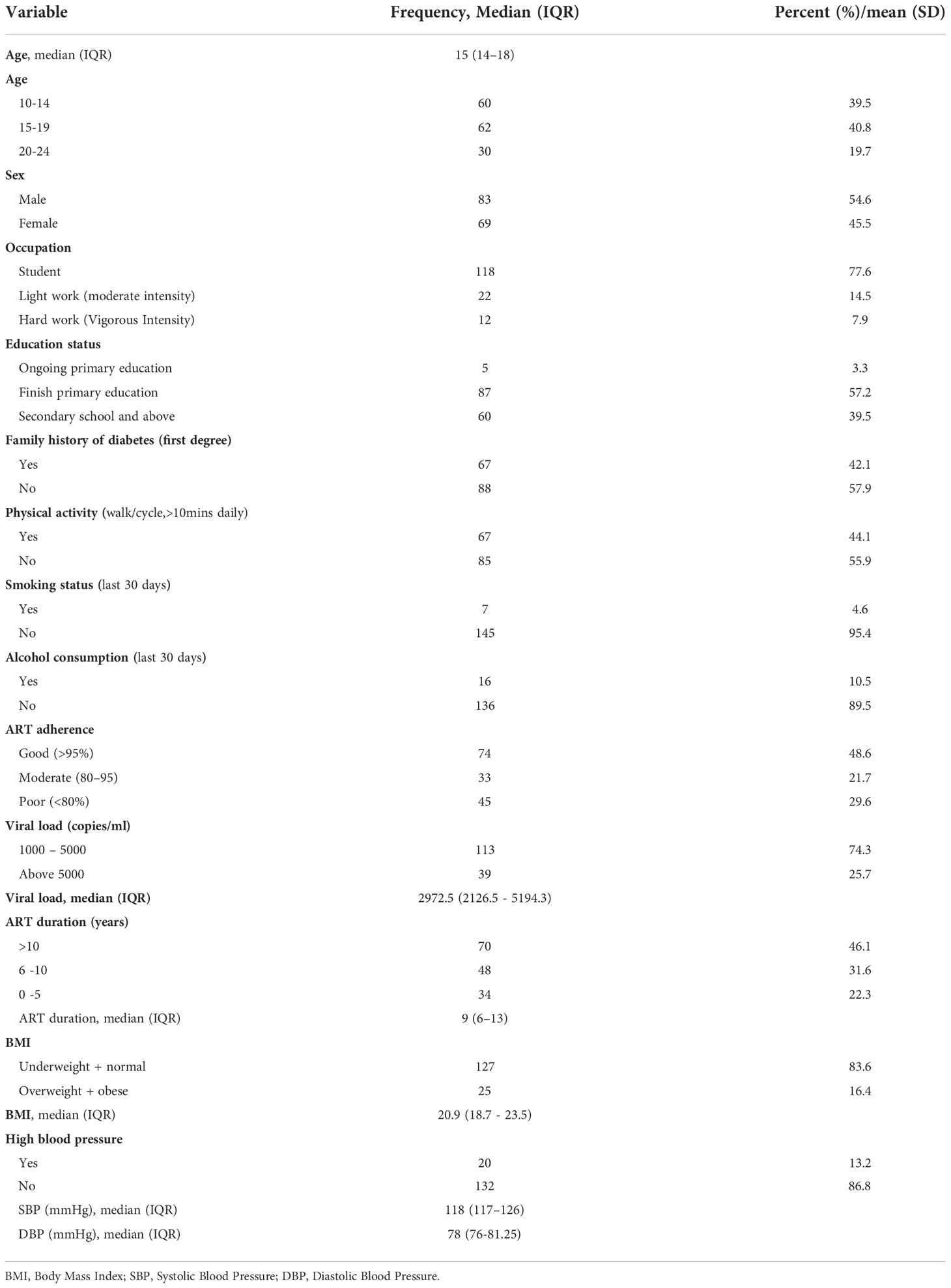
Table 1 Characteristics of study participants .
The proportion of participants with impaired fasting glucose was 28.9% (n=45). High IL6 and High CRP were observed in 34 (22.4%) and 78 (51.30%) participants, respectively. Thirteen (8.6%) participants had impaired fasting glucose and high IL6 levels. Likewise, impaired fasting glucose and high levels of CRP were observed in 26(17.1%) (Table 2).
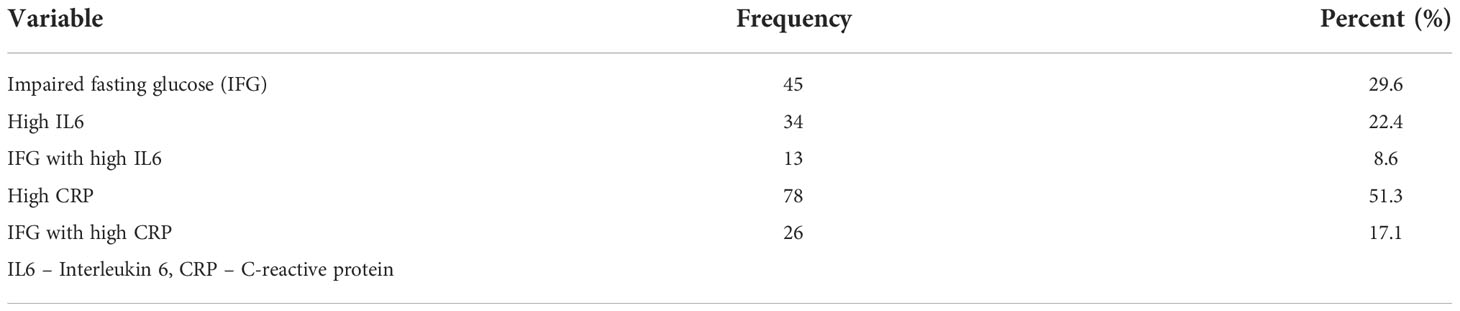
Table 2 Proportion of impaired fasting glucose, high IL6, and high CRP (n = 152).
Among the analyzed factors, only gender was significantly associated with IFG (p=0.008). Therefore, all variables with a p-value ≤0.2, which were family history of diabetes, physical activity, alcohol consumption and IL6 inflammatory biomarker, were subjected to poison regression analysis with robust variance. BMI and viral load had high multicollinearity (R=0.88) hence only one of the variables (BMI) was subjected to the model with other factors. The odds of having IFG were two times higher in males compared to female (PR, 2.07, 95%CI, 1.19 – 3.59 p=0.001) Moreover, with every increase of 1.101 of IL6 the probability of having IFG increased (PR, 1.01, 95 CI (1.00 – 1.02 p=0.003) (Table 3).
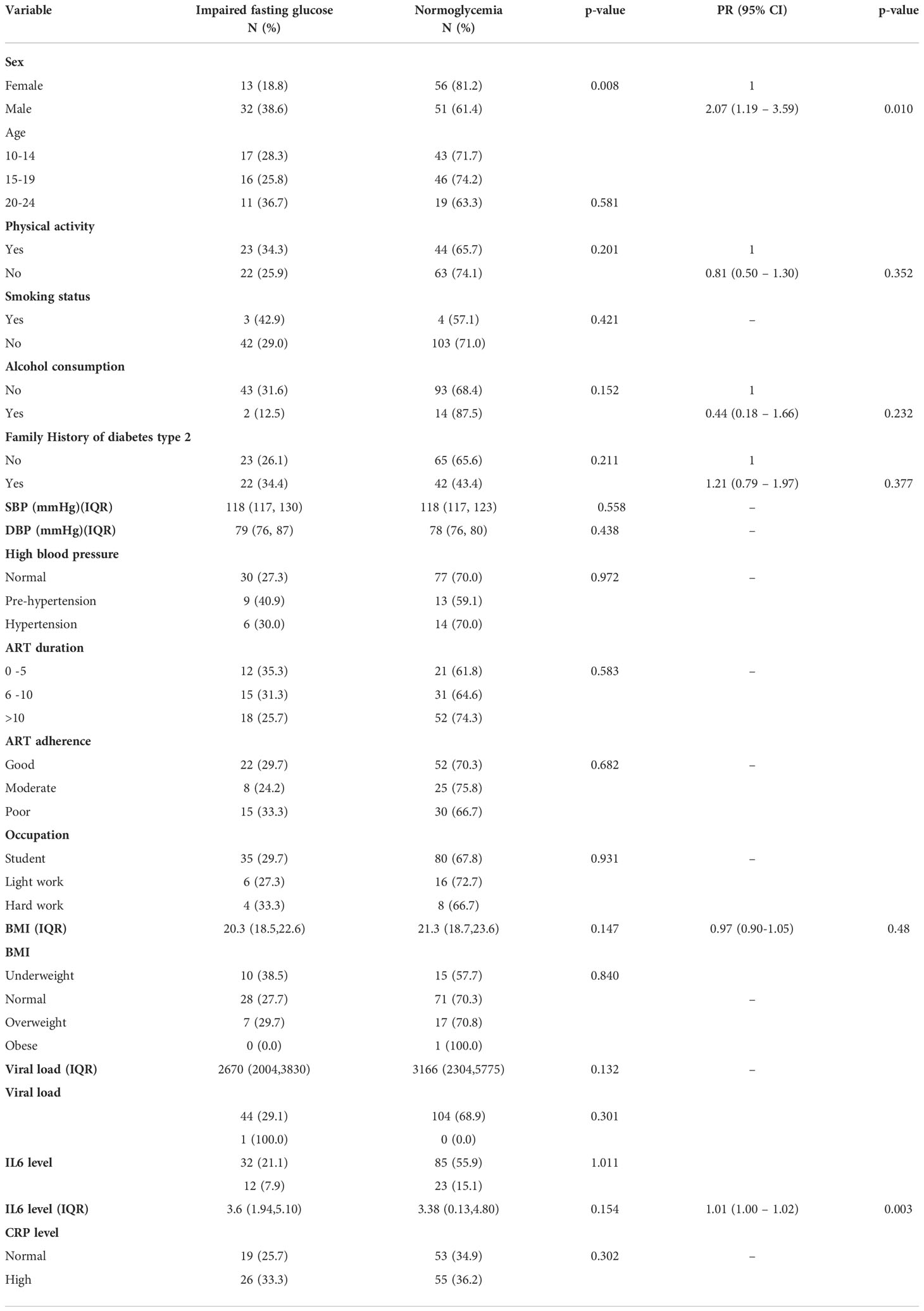
Table 3 Bivariate and Multivariate analysis of factors associated with impaired fasting glucose.
The current study revealed a relatively high burden of impaired blood glucose among perinatally HIV-infected youth in Dar es Salaam, Tanzania. In addition, our study observed that around 13% of participants have high blood pressure (≥149/90mmHg), and nearly one-third have poor adherence to antiretroviral therapy. Both conditions are important risk factors for the early onset of non-communicable diseases, a growing burden in the country. Moreover, with every increase of 1.101 of IL6 the probability of having IFG increased and the males were twice more likely to have IFG compared to females.
HIV perinatally infected youth are currently living for many years since the introduction of antiretroviral therapy (18). However, several studies have observed glucose impairment ranging from insulin resistance (8–10) to pre-diabetes (11, 12), and even full-blown diabetes disease (9). The current study observed that close to one in three youths (29%) had impaired fasting glucose, but the affected youths were unaware of their status, which further increase the risk of poor disease progression. Data from sub–Saharan Africa(SSA) have shown IFG to range from 2-6% (8, 22, 23). These results are comparatively lower than the current study. Although the difference could be attributed by the lower mean age of 9-12 years or mean duration of ARV use of 4-6 years compared to the current study where the mean age is 16 years and 10years respectively. Data from a Hispanic population with similar mean age (15 years) and ART duration (11years) reported IFG of 4.6% (24). Given that the occurrence of glucose alterations is multifactorial, these varying results across different geographical regions could reflect the varying dietary habits, genetic attributes and ethnicity (24, 25). Moreover, from the Findings from Latin America and Europe have shown the prevalence of IFG to range from 0.4-7% (26–29), while reports from Asian communities range from 2.6-43% (9, 11, 12). This necessitates for population specific data, to make informed decisions.
It is expected to observe a higher burden of diabetes and pre-diabetes in adults than in adolescents and youth (23); however, the prevalence in the current study is comparable to the prevalence of Pre-diabetes reported among adult PLWH in sub-Saharan Africa, which ranges from 15-27% (3, 5, 19). Despite the growing concerns about the increasing burden of impaired glucose metabolism among the HIV population (5, 19), no specific preventive measure has been incorporated into HIV care and treatment in Tanzania. The perinatally HIV-infected individuals will have a lifetime exposure to ART and HIV-related inflammation, hence have a greater risk of succumbing to the dual burden of disease at a younger age (16, 30) if no measures are taken. To the best of our knowledge this is among the pioneer study reporting IFG among perinatal infected adolescent and youth in Tanzania.
Moreover, we found with every increase of Interleukin 6 biomarker there is a 1.01 probability increase of IFG. Even with effective ART, chronic inflammation persists and has been linked the incidence of insulin insensitivity and eventually diabetes mellitus type 2 (3, 19). Several findings have shown incidence of diabetes following high levels of IL6 among other markers such as CRP (31, 32). Whether IL6 can predict the incidence of diabetes for the HIV population is still not clear, as the findings are highly heterogenous (19, 31). According to Farmer et al. the predictability of a marker is also influenced by the genetic variability and ethnicity, therefore more studies on a similar population are warranted to establish a reliable marker for the adolescent and youth population (33). The current study also measured CRP levels among the participants, but the findings were not significantly correlated.
Being male increased the risk of IFG by two-fold in this study. Similar findings have been reported elsewhere for the general population and PLHIV infection (5, 34). Contrasting findings argue that glucose impairment fluctuates depending on the life stage; where females are reported to have higher rates of glucose disturbances during youth, while males have higher odds at mid-life (35). A comparably smaller sample size could in-part explain the variation of these findings since a large study (n=4.4m) involving 146 countries reported men to have a higher prevalence of glucose-impaired metabolism independent of age (36). The other explanation could be the modality of glucose screening, where findings from a large European Diabetes Epidemiology study confirmed male predominance when fasting blood is used for diagnosis but not when a 2hour plasma glucose is tested after oral glucose load (37). Therefore, these findings could be an underestimation of the actual burden.
This study reports hypertension being prevalent among adolescents and youth (13%) who were perinatally infected with HIV. This is lower than another study conducted among adult perinatally infected subjects (30%) with a median age of 26 years (38). The age gap could have influenced this difference, as evidenced in the Baltimore study that reported a prevalence of hypertension of 26% among young adults, and the incidence significantly increased as the population reached adulthood (<18 years) (39). Factors at play for the perinatally HIV-infected individuals are not characterized, most probably because of the multifactorial pathophysiology (40). However, structural changes in the cardiac vasculature are observed as early as the first ten years of life for vertically HIV-infected subjects (41). Poorly controlled hypertension may eventually lead to cardiovascular diseases, kidney diseases, and mortality (42); hence early identification of high-risk individuals through screening is critical to prevent the development of these outcomes.
Having Poor ART drug adherence was not significantly associated with having IFG, although 29% were reported to have poor adherence to medication. This is regarded as a health risk behavior as it endangers the life and livelihood of the concerned and increases the risk of HIV transmission (43). Similar to the current study, sub-optimal ART adherence is reported in several studies among perinatally HIV-infected individuals (44, 45), where several factors have been correlated to contribute, such as the child’s age, developmental stage, and psychosocial state, among others (46). The dual burden of HIV and non-AIDS chronic disease could further complicate HIV care and treatment outcomes, including adherence to care; hence, youth-friendly adherence counseling is necessary to reduce adherence barriers for this uniquely challenged population (12, 46).
About 16% of our study participants were overweight or obese, but this was not significantly associated with impaired fasting glucose in our study. Although, it is a well-documented risk factor influencing glucose metabolism impairment and cardiovascular disease among the HIV population (3, 34). Similar findings have been reported in other studies, where a significant correlation was not attained (5, 19). The lower proportion of this variable may have limited the our ability to detect such associations.
Of note, we observed a trend of a non-significant low proportion of IFG in those with physical activity. According to Kemps et al, physical training can improve insulin sensitivity and overall sugar levels (47). Not being physically active could be influenced by being an urban resident, this is also reported in several studies that compared urban and HIV rural populations (48). Interestingly being physically active is reported to improve ART adherence (49). This could be because of its potential to improve one’s mood and alienate depressive symptoms (49), although further studies are required on this phenomenon to justify incorporating physical exercise in HIV care and treatment for perinatally infected individuals.
This study is not without limitation: this includes the use of a point of care device to measure glucose levels as this may overestimate the burden glucose impairment (21). None the less these are the devices used for screening and diagnosis of diabetes in SSA (50). Furthermore, the puberty stage has been associated with insulin insensitivity, however we did not study the role of puberty in relation to impaired fasting glucose because of the challenges in assessing this variable using tanner staging scale in the midst of provision of HIV care and treatment routine services.
The prevalence of IFG was high among HIV perinatally infected youths, found more in males than females. Furthermore increase of 1.101 of IL6 increased the probability of having IFG. Therefore, this study recommends incorporating scheduled glucose screening to identify these individuals early before developing full-blown diabetes. Furthermore, this study calls for urgent measures to interrupt the progression to diabetes to prevent the dual burden of disease for this uniquely challenged population.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Senate of Research and Publication Committee and the Institutional Review Board of Muhimbili University of Health and Allied Sciences (MUHAS). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from a parent/legal guardian as well as the Nurse Matron for those below the age of 18. In addition, permission to be involved in the study was obtained from the child himself/herself. For children above the age of 18 years written informed consent was obtained from all subjects before the study began.
LN conceptualized the study. Methodology and data collection were done by EB, AN, MG. FM and MM performed data analysis. LN developed the initial manuscript draft. AJ, PM, BS and KR critically reviewed the manuscript. All authors have read and approved this manuscript. This manuscript has been submitted solely to this journal and is not published or submitted elsewhere.
We are grateful to IDC and MNH nurses and phlebotomists for their invaluable support during data collection. We also thank the youth who participated in this study, which enabled this manuscript’s write-up.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.1045628/full#supplementary-material
1. Duncan GE. Prevalence of diabetes and impaired fasting glucose levels among USA adolescents. Arch Pediatr Adolesc Med (2006) 160:1999–2002. doi: 10.1001/archpedi.160.5.523
2. Mwanri AW, Kinabo J, Ramaiya K, Feskens EJM. Prevalence of gestational diabetes mellitus in urban and rural Tanzania. Diabetes Res Clin Pract [Internet] (2016) 103(1):71–8. doi: 10.1016/j.diabres.2013.11.021
3. Njuguna B, Kiplagat J, Bloomfield GS, Pastakia SD, Vedanthan R, Koethe JR. Prevalence, risk factors, and pathophysiology of dysglycemia among people living with HIV in Sub-Saharan Africa. J Diabetes Res (2018) 2018(6916497):12. doi: 10.1155/2018/6916497
4. Slim J, Saling CF. A review of management of inflammation in the HIV population. BioMed Res Int (2016) 2016(3420638):12. doi: 10.1155/2016/3420638
5. Maganga E, Smart LR, Kalluvya S, Kataraihya JB, Saleh AM, Obeid L, et al. Glucose metabolism disorders, HIV and antiretroviral therapy among Tanzanian adults. PLoS One (2015) 10(8):e0134410. doi: 10.1371/journal.pone.0134410
6. Innes S, Patel K. Noncommunicable diseases in adolescents with perinatally acquired HIV-1 infection in high-income and low-income settings. Curr Opin HIV AIDS (2018) 13(3):187–95. doi: 10.1097/COH.0000000000000458
7. Lee B, Aurpibul L, Sirisanthana V, Mangklabruks A, Sirisanthana T, Puthanakit T. Low prevalence of insulin resistance among HIV-infected children receiving nonnucleoside reverse transcriptase inhibitor-based highly active antiretroviral therapy in Thailand. HIV Med (2009) 10(2):72–8. doi: 10.1111/j
8. Francisco K, Pole B, Tchiva S, Ngwiri T, Nduati R, Mungai L. Insulin resistance and glucose intolerance in HIV infected children on antiretroviral therapy at lubango pediatric hospital-Angola. Int J Virol AIDS 7 (2020) 071:10–23937. doi: 10.3389/fphar.2021.635089
9. Seang K, Javanbakht M, Lee SJ, Brookmeyer R, Pheng P, Chea P, et al. Differences in prevalence and risk factors of non-communicable diseases between young people living with HIV (YLWH) and young general population in Cambodia. PLoS One (2022) 17(6):e0269989. doi: 10.1371/journal.pone.0269989
10. Frigati LJ, Jao J, Mahtab S, Agyei N-AA, Cotton MF, Myer L, et al. Insulin resistance in south African youth living with perinatally acquired HIV receiving antiretroviral therapy. AIDS Res Hum Retroviruses (2019) 35(1):56–62. doi: 10.1089/aid.2018.0092
11. Santiprabhob J, Tanchaweng S, Maturapat S, Maleesatharn A, Lermankul W, Sricharoenchai S, et al. Metabolic disorders in HIV-infected adolescents receiving protease inhibitors. BioMed Res Int (2017) 2017(7481597):14. doi: 10.1155/2017/7481597
12. Aurpibul L, Namwongprom S, Sudjaritruk T, Ounjaijean S. Metabolic syndrome, biochemical markers, and body composition in youth living with perinatal HIV infection on antiretroviral treatment. PLoS One (2020) 15(3):e0230707. doi: 10.1371/journal.pone.0230707
13. Lowenthal ED, Bakeera-Kitaka S, Marukutira T, Chapman J, Goldrath K, Ferrand RA. Perinatally acquired HIV infection in adolescents from sub-Saharan Africa: a review of emerging challenges. Lancet Infect Dis [Internet] (2014) 14(7):627–39. doi: 10.1016/S1473-3099(13)70363-3
14. Routy J-P, Isnard S, Mehraj V, Ostrowski M, Chomont N, Ancuta P, et al. Effect of metformin on the size of the HIV reservoir in non-diabetic ART-treated individuals: single-arm non-randomised lilac pilot study protocol. BMJ Open [Internet] (2019) 9(4):e028444. doi: 10.1136/bmjopen-2018-028444
15. Nimitphong H, Jiriyasin S, Kasemasawachanon P, Sungkanuparph S. Metformin for preventing progression from prediabetes to diabetes mellitus in people living with human immunodeficiency virus. Cureus (2022) 14(4):e24540. doi: 10.7759/cureus.24540
16. Kamkuemah M, Gausi B, Oni T. Missed opportunities for NCD multimorbidity prevention in adolescents and youth living with HIV in urban south Africa. BMC Public Health (2020) 20(1):821. doi: 10.1186/s12889-020-08921-0
17. Azzopardi P. The art of medicine: Adolescent health comes of age. Lancet (2012) 379(9826):1583–4. doi: 10.1016/S0140-6736(12)60666-7
18. World Health Organization. Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia:Report of a WHO/IDF consultation. Production (2006) 1–52. Available at: https://apps.who.int/iris/handle/10665/43588.
19. Nkinda L, Patel K, Njuguna B, Ngangali JP, Memiah P, Bwire GM, et al. C-reactive protein and interleukin-6 levels among human immunodeficiency virus-infected patients with dysglycemia in Tanzania. BMC Endocrine Disord (2019) 19(1):1–8. doi: 10.1186/s12902-019-0407-y
20. Desta AA, Kidane KM, Woldegebriel AG, Ajemu KF, Berhe AA, Zgita DN, et al. Level of adherence and associated factors among HIV-infected patients on antiretroviral therapy in northern Ethiopia: retrospective analysis. Patient preference adherence (2020) 14:1585. doi: 10.2147/PPA.S268395
21. Katz LB, Stewart L, Guthrie B, Cameron H. Patient satisfaction with a new, high accuracy blood glucose meter that provides personalized guidance, insight, and encouragement. J Diabetes Sci Technology (2020) 14(2):318–23. doi: 10.1177/1932296819867396
22. Oyenusi EE, Micondo KH, Dainguy ME, Abodo RJ, Folquet MA, Oduwolé AO. Fasting blood glucose profile of children living with HIV taking first-line antiretroviral treatment in Abidjan, cote D’Ivoire: A cross-sectional study. Romanian J Diabetes Nutr Metab Diseases (2020) 27(2):90–8. Available at: https://www.rjdnmd.org/index.php/RJDNMD/article/view/706.
23. Ohuche IO, Chikani UN, Oyenusi EE, Onu JU, Oduwole A. Correlates of fasting blood glucose among children living with hiv in a Nigerian tertiary hospital: a cross-sectional study. BMC pediatrics (2020) 20(1):1–7. doi: 10.1186/s12887-020-02335-y
24. Blázquez D, Ramos-Amador JT, Saínz T, Mellado MJ, García-Ascaso M, De José MI, et al. Lipid and glucose alterations in perinatally-acquired HIV-infected adolescents and young adults. BMC Infect diseases (2015) 15(1):1–7. doi: 10.1186/s12879-015-0853-8
25. Pham TM, Carpenter JR, Morris TP, Sharma M, Petersen I. Ethnic differences in the prevalence of type 2 diabetes diagnoses in the UK: Cross-sectional analysis of the health improvement network primary care database. Clin Epidemiol (2019) 11:1081–8. doi: 10.2147/CLEP.S227621
26. Geffner ME, Patel K, Jacobson DL, Julia WU, Miller TL, Hazra R, et al. Changes in insulin sensitivity over time and associated factors in HIV-infected adolescents. AIDS (london England) (2018) 32(5):613. doi: 10.1097/QAD.0000000000001731
27. Espiau M, Yeste D, Noguera-Julian A, González-Tomé MI, Falcón-Neyra L, Gavilán C, et al. Metabolic syndrome in children and adolescents living with HIV. Pediatr Infect Dis J (2016) 35(6):e171–176. doi: 10.1097/INF.0000000000001118
28. Hazra R, Hance LF, Monteiro JP, Ruz NP, Machado DM, Saavedra M, et al. Insulin resistance and glucose and lipid concentrations in a cohort of perinatally HIV-infected Latin American children. Pediatr Infect Dis J (2013) 32(7):757. doi: 10.1097/INF.0b013e318286c774
29. Paganella MP, Cohen RA, Harris DR, de Souza Kuchenbecker R, Sperhacke RD, Kato SK, et al. NISDI PLACES protocol. association of dyslipidemia and glucose abnormalities with antiretroviral treatment in a cohort of HIV-infected Latin American children. J Acquir Immune Defic Syndr (2017) 74(1):e1–8. doi: 10.1097/QAI.0000000000001163
30. Kamkuemah M, Gausi B, Oni T. High prevalence of multimorbidity and non-communicable disease risk factors in south African adolescents and youth living with HIV: Implications for integrated prevention. S Afr Med J (2022) 112(4):259–67. doi: 10.7196/SAMJ.2022.v112i4.15967
31. Borges ÁH, O'Connor JL, Phillips AN, Neaton JD, Grund B, Neuhaus J, et al. Interleukin 6 is a stronger predictor of clinical events than high-sensitivity c-reactive protein or d-dimer during HIV infection. J Infect Dis (2016) 214(3):408–16. doi: 10.1093/infdis/jiw173
32. Dooko CB, De Wit S, Neuhaus J, Palfreeman A, Pepe R, Pankow JS, et al. Interleukin-6, high sensitivity c-reactive protein, and the development of type 2 diabetes among HIV positive patients taking antiretroviral therapy. J acquired Immune deficiency syndromes (1999) (2014) 67(5):538. doi: 10.1097/QAI.0000000000000354
33. Farmer HR, Slavish DC, Ruiz J, Dietch JR, Ruggero CJ, Messman BA, et al. Racial/ethnic variations in inflammatory markers: exploring the role of sleep duration and sleep efficiency. J Behav Med (2022) 27:1–3. doi: 10.1007/s10865-022-00357-8
34. Tramunt B, Smati S, Grandgeorge N, Lenfant F, Arnal JF, Montagner A, et al. Sex differences in metabolic regulation and diabetes susceptibility. Diabetologia (2020) 63(3):453–61. doi: 10.1007/s00125-019-05040-3
35. Huebschmann AG, Huxley RR, Kohrt WM, Zeitler P, Regensteiner JG, Reusch JE. Sex differences in the burden of type 2 diabetes and cardiovascular risk across the life course. Diabetologia (2019) 62(10):1761–72. doi: 10.1007/s00125-019-4939-5
36. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet (2016) 387(10027):1513–30. doi: 10.1016/S0140-6736(16)00618-8
37. DECODA Study Group. Age-and sex-specific prevalence of diabetes and impaired glucose regulation in 11 Asian cohorts. Diabetes Care (2003) 26(6):1770–80. doi: 10.2337/diacare.26.1.61
38. O’Neil PJ, Stafford KA, Ryscavage PA. Assessing risk factors for hypertension in young adults with perinatally acquired HIV infection: A case–control study. HIV Med (2022) 23(5):457–64. doi: 10.1111/hiv.13199
39. Ryscavage P, Macharia T, Trinidad LR, Lovelace S, Tepper V, Redfield R. Patterns of systemic hypertension among adults with perinatally acquired HIV. J Int Assoc Provid AIDS Care [Internet] (2016) 16(1):3–7. doi: 10.1177/2325957416668034
40. Deeks SG, Phillips AN. HIV Infection, antiretroviral treatment, ageing, and non-AIDS related morbidity. BMJ [Internet] (2009) 338:a3172. doi: 10.1136/bmj.a3172
41. Sainz T, Álvarez-Fuente M, Navarro ML, Díaz L, Rojo P, Blázquez D, et al. Subclinical atherosclerosis and markers of immune activation in HIV-infected children and adolescents: The CaroVIH study. JAIDS J Acquir Immune Defic Syndr (2014) 65(1):42–9. doi: 10.1097/QAI.0b013e3182a9466a
42. Olaiya O, Weiser J, Zhou W, Patel P, Bradley H. Hypertension among persons living with HIV in medical care in the united states-medical monitoring project, 2013-2014. Open Forum Infect Dis [Internet] (2018) 5(3):ofy028–8. doi: 10.1093/ofid/ofy028
43. Foster C, Ayers S, Fidler S. Antiretroviral adherence for adolescents growing up with HIV: understanding real life, drug delivery and forgiveness. Ther Adv Infect Disease (2020) 7:2049936120920177. doi: 10.1177/2049936120920177
44. Xu L, Munir K. Factors influencing antiretroviral treatment suboptimal adherence among perinatally HIV-infected adolescents in Thailand. PLoS One [Internet] (2017) 12(2):e0172392–e0172392. doi: 10.1371/journal.pone.0172392
45. Fields EL, Bogart LM, Thurston IB, Hu CH, Skeer MR, Safren SA, et al. Qualitative comparison of barriers to antiretroviral medication adherence among perinatally and behaviorally HIV-infected youth. Qual Health Res (2017) 27(8):1177–89. doi: 10.1177/1049732317697674
46. Panel on Antiretroviral Therapy and Medical Management of Children Living with HIV. Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection (2020). Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/pediatricguidelines.pdf. [Accessed 22 Nov 2022].
47. Kemps H, Kränkel N, Dörr M, Moholdt T, Wilhelm M, Paneni F, et al. Exercise training for patients with type 2 diabetes and cardiovascular disease: What to pursue and how to do it. a position paper of the European association of preventive cardiology (EAPC). Eur J Prev Cardiol (2019) 26(7):709–27. doi: 10.1177/2047487318820420
48. Tegene Y, Mengesha S, van der Starre C, Lako S, Toma A, Spigt M. Physical activity level and associated factors among adult HIV patients in Ethiopia. BMC Infect Dis (2022) 22(1):123. doi: 10.1186/s12879-022-07120-z
49. Dang AK, Nguyen LH, Nguyen AQ, Tran BX, Tran TT, Latkin CA, et al. Physical activity among HIV-positive patients receiving antiretroviral therapy in Hanoi and nam dinh, Vietnam: a cross-sectional study. BMJ Open (2018) 8(5):e020688–e020688. doi: 10.1136/bmjopen-2017-020688
Keywords: pre-diabetes, impaired fasting glucose, HIV, perinatal infection, adolescents, youth
Citation: Nkinda L, Buberwa E, Memiah P, Ntagalinda A, George M, Msafiri F, Joachim A, Majigo M, Ramaiya K and Sunguya B (2022) Impaired fasting glucose levels among perinatally HIV-infected adolescents and youths in Dar es Salaam, Tanzania. Front. Endocrinol. 13:1045628. doi: 10.3389/fendo.2022.1045628
Received: 15 September 2022; Accepted: 14 November 2022;
Published: 06 December 2022.
Edited by:
Jessie Zurita-Cruz, Hospital Infantil de México Federico Gómez, MexicoReviewed by:
Meera Ladwa, Barts Health NHS Trust, United KingdomCopyright © 2022 Nkinda, Buberwa, Memiah, Ntagalinda, George, Msafiri, Joachim, Majigo, Ramaiya and Sunguya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lilian Nkinda, bGlseW5raW5kYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.