
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol. , 01 December 2022
Sec. Neuroendocrine Science
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1024794
This article is part of the Research Topic Association of Metabolic Diseases with Cognition Impairment and Dementia View all 9 articles
 Andreea Ciudin1,2,3*
Andreea Ciudin1,2,3* Rafael Simó1,3,4*
Rafael Simó1,3,4*The presence of type 2 diabetes acts as an accelerator of cognitive impairment (mild cognitive impairment and later dementia), with a significant impact on the management of the disease and its complications. Therefore, it is recommended to perform an annual evaluation of cognitive function in patients with diabetes older than 65 years. Current guidelines still recommend the use of the Minimental State Evaluation Test (MMSE) as screening test, but it has a modest sensitivity and specificity for identifying mild cognitive impairment. This represents an important gap because patients with mild cognitive impairment are at risk of progressing to dementia. The neurocognitive diagnosis is based on complex neuropsychological tests, which require specifically trained personnel and are time consuming, making its routine incorporation into daily clinical practice unfeasible. Therefore, at present there are no reliable biomarkers to identify patients with type 2 diabetes at increased risk of developing cognitive impairment. Since the brain and the retina have a common embryological origin, our Research Group, has worked over the last 10 years evaluating the usefulness of the retina as a “window” to the brain. We provided evidence that retinal microperimetry is a simple, feasible and useful tool for screening and monitoring cognitive function in patients with type 2 diabetes. We propose a review of actual tests recommended for screening of cognitive impairment as well as an update of new emerging methods, such as retinal microperimetry.
Current epidemiological data show that type 2 diabetes (T2D) increases 2-3 times the risk of developing dementia, in comparison with non-diabetic population matched by age and other risk factors (1).
T2D and dementia, in particular Alzheimer´s disease (AD), share several common pathophysiological mechanisms. Both, in T2D and Alzheimer´s disease insulin resistance, low-grade inflammation, oxidative stress, high levels of angiotensin-II and advanced end-glycation products (AGE) are found and contribute to the progression of the disease. Furthermore, a common genetic background was described- Additionally, patients with T2D have smaller brain volumes and white matter disruption as a result of this pathophysiological mechanisms- as reflected by Figure 1 (2–5).
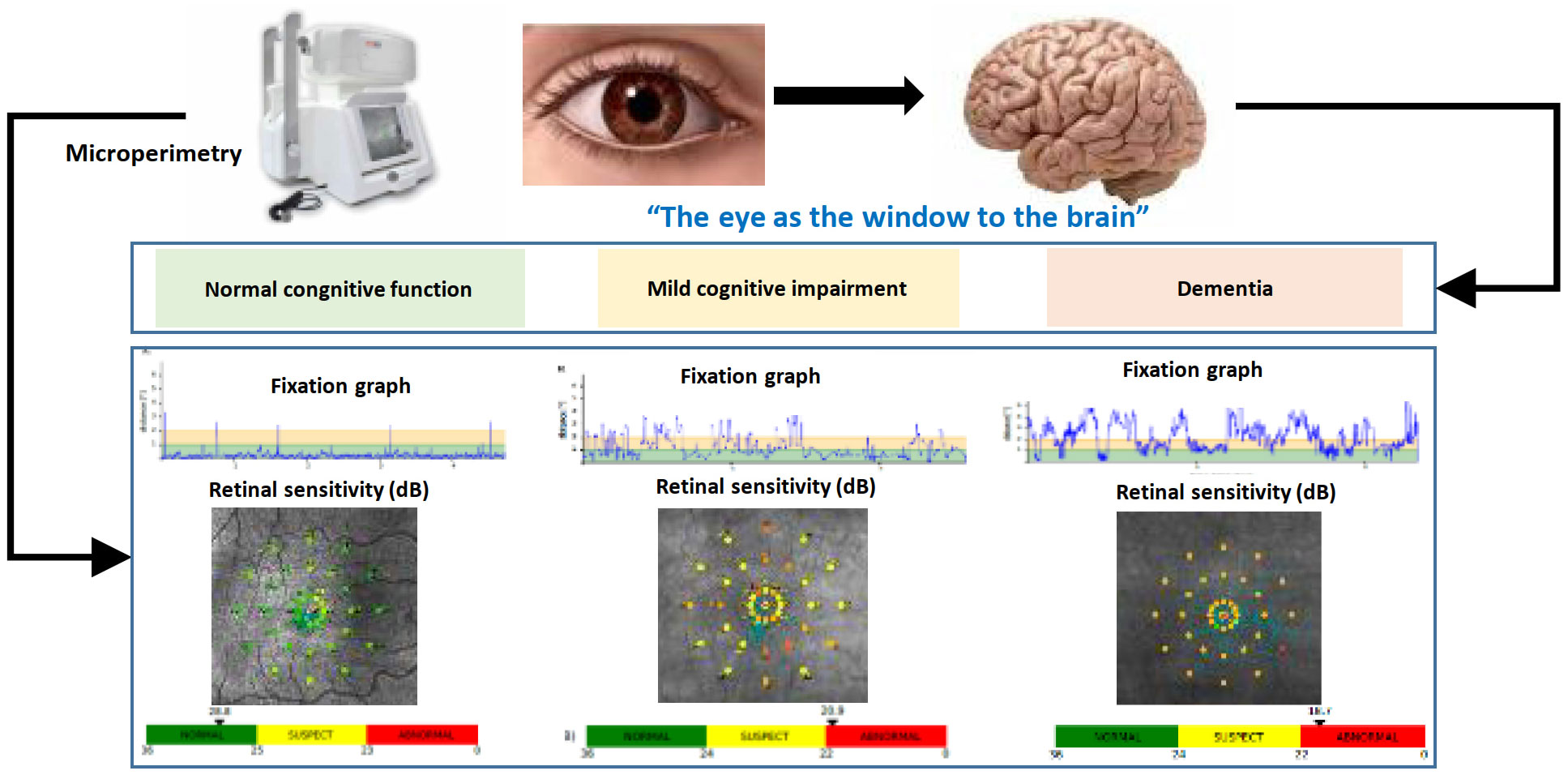
Figure 1 Common mechanisms shared by Type 2 diabetes and Cognitive impairment.
On these bases we hypothesized that T2D could act as an accelerator of cognitive decline in two ways: by inducing a slow cognitive decline, also called “dementia related to Diabetes”, or by precipitating a rapid cognitive decline to AD, in the presence of predisposing genetic factors, like APOEϵ4 allele (3). Additionally, the presence of complications related to diabetes (micro and macrovascular), as well as metabolic control and the episodes of hypoglycemia will accelerate the progression of cognitive impairment (6–10).
There is a gradual progression from the so-called subjective memory complaints (SMC) to mild cognitive impairment (MCI), which is the prelude to dementia. MCI represents a deterioration in cognition superior to that observed with normal cognitive decline associated with age, but not severe enough to cause significantly impaired daily function (11)
Data in the literature showed that about 33% of women and 20% of men over 65 years of age with MCI could develop dementia throughout during their lifespan (12). Recent data showed that T2D is an independent risk factor, besides the presence of the APOEε4 allele for conversion to dementia in patients with MCI (1). The presence of MCI can lead to mismanagement of the specific treatment for T2D. This can favor episodes of severe hypoglycemia, thus worsening the patients’ cognitive status, all of which translates into an increase in direct and indirect healthcare costs (13, 14). Additionally, hypoglycemia can alter the cognitive function and accelerates the progression to dementia (15–17). For this reason, it is important to diagnose cognitive impairment in early stages in patients with T2D.
Since 2018, the ADA clinical guidelines started to recommend screening for early detection of cognitive impairment for adults≥ 65 years of age with T2D at the initial visit and annually as appropriate (18, 19). The current guideline (19), recommend for this purpose screening tools such as the Mini Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA), especially in those patients in whom dementia is suspected. Additionally, annual monitoring is indicated for adults >65years with T2D for early detection of mild cognitive impairment or dementia.
The MMSE, 10-15 minutes test (20)is a test largely used to screen for cognitive impairment. A standard MMSE cut score of 24 (≤23) yielded a sensitivity of 0.58 and a specificity of 0.98 in detecting probable and possible Alzheimer’s disease. A cut score of 27 of a maximum 30 (≤26) resulted in an improved balance of sensitivity and specificity (0.79 and 0.90, respectively). In MCI group the standard cut-off score of 24 yielded a sensitivity of 0.38 and a specificity of 1.00 while raising the cut score to 27 resulted in an improved balance of 0.59 and 0.96 of sensitivity and specificity, respectively (20) (21). Nevertheless, it should be noted that these data are supported on limited number of patients. A recent meta-analysis (22), evaluated the usefulness of MMSE for the detection of dementia in people with MCI. The conclusion, based on 11 studies that meet the accuracy criteria, was that there no reliable evidence to support a substantial role of MMSE in identifying those patients with MCI at risk of developing dementia. The data from the clinical studies that were evaluated is heterogeneous regarding the optimal cut-off, the influence of educational background or the effect of literacy in the accuracy of MMSE.
Regarding the annual monitoring, the same meta-analysis showed a specificity of 88% and sensitivity of 40% in detecting progression of MCI (22).
The MoCA test (23), a 10-15 minutes is the other neurocognitive test recommended for screening of cognitive function in patients with T2D>65years. The cut-off of >26 out of maximum 30 identified patients with MCI with a sensitivity of 91% and specificity of 90%. This test needs previous training and periodical certification of the personnel. Furthermore, the result is influenced by the educational level and the mood of the subject.
A recent study (24) showed that MoCA is superior to MMSE in detecting patients at higher risk of dementia. Nonetheless, it should be noted that this conclusion is based on small sample size (<100 subjects in total) and different cut-offs were used (19-20 for MoCA and 23-24 for MMSE).
Additionally, studies that evaluated the usefulness of both MMSE or MoCA excluded patients with depressive symptoms, evaluated by specific questionnaires, such as geriatric depression scale (GDS) or medical history (22, 24). This represents an important limitation because the associated anxiety-depression and impaired quality or life (QoL) occur in a significant proportion of ageing T2D patients. This is important because, apart from influencing the result of neuropsychological tests, the psychological abnormalities related to a decrease in QoL in T2D patients could play a role in aggravating their cognitive decline. In fact, depression was associated with cognitive decline in the ACCORD-MIND study (25). Additionally, the prevalence of depression is two-fold higher in T2D compared with the general population worldwide (26) and it has recently been reported of 27,5% among T2D patients in the Mediterranean population (27) This prevalence rate could even be higher in the older adults with diabetes because depressive symptoms may be overlooked (27).
On these bases, we should raise serious questions about the accuracy and the applicability of these recommended screening tests at large scale in the population with T2D >65 years, especially if we intent to detect cognitive impairment in early stages.
● Low sensitivity and specificity for detecting early stages of cognitive impairment
● Results based on studies with small sample size, heterogeneous cut-offs, patients with depressive symptoms were excluded.
● Depend on the educational level and the mood of the patient.
The current guidelines recommend screening of cognitive impairment especially in those patients in whom dementia is suspected (28). Nonetheless, the early recognition of cognitive impairment is crucial for a personalized medicine and is an essential issue in diabetes care. The early detection of mild cognitive impairment or even subjects with SMC at risk of progression is important because T2D patients with cognitive impairment are more prone to present an impaired self-management of diabetes, poor glycemic control and an increased incidence of diabetes-related complications. In this regard, the actually recommended tools have serious limitations and at present there is gap due to the lack of rapid, reliable tools for early detection of cognitive impairment in patients with T2D >65years, regardless of the mood or educational level.
In recent years new methods have emerged for the screening and monitoring of the congnitive function in patients with T2D>65years: the Diabetes Specific Dementia Risk Score (DSDRS) (29) and retinal microperimetry (30).
DSRDS was proposed in 2013 by Exalto et al. (29) as a risk score for the prediction of 10-year dementia risk in patients with T2D. This score consists of several clinical and demographic variables (age, gender, education, history of diabetic foot, acute metabolic events, depression, microvascular disease, cardiovascular disease and cerebrovascular disease) and ranges from a 5% 10-year dementia risk for those with the lowest score up to a 73% risk for the highest score.
The DSDRS was not initially designed as a screening tool. Recently, as part of a European project (31),MOPEAD study (32), our research group evaluated the usefulness of the DSDRS as a screening tool for MCI, alone or combined with MMSE. The cognitive status of the patients was confirmed by neuropsycholgical tests battery performed by trained neuropsychologists at the memory clinic. The results showed that a cut-off of DSDRS≥7 had a predictive value of AUC 0.739 (CI95%, [0.557-0.921]) and of 0.902 (CI 95% [0.840-0.992]) when combined with MMSE (33), suggesting that DSRDS could be a reliable screening tool for cognitive decline in patients with T2D>65 years with a sensitivity 88.37% CI95% (78.9-97.9) and specificity 55.26% CI 95% (48.9-60.5). Additionally, a recent study from another group studied the utility of the DSDRS for lower cognitive performance and found similar results, with a sensitivity of 83.3% and specificity of 54.3% (31).
The retina is ontogenically a brain-derived tissue and it has been suggested that it may provide an easily accessible and non-invasive way of examining the pathology of the brain: “the eye as a window of the brain”. Retinal microperimetry, is a simple, rapid and non-invasive test that measures retinal sensitivity in terms of the minimum light intensity that patients can perceive when spots of light stimulate specific areas of the retina, and also evaluate gaze fixation stability (30, 34).
We showed for the first time that the retinal sensitivity significantly correlated with brain imaging (MRI and PET) and identified patients with MCI and dementia, as confirmed by complete neuropsychological battery- Figure 2.
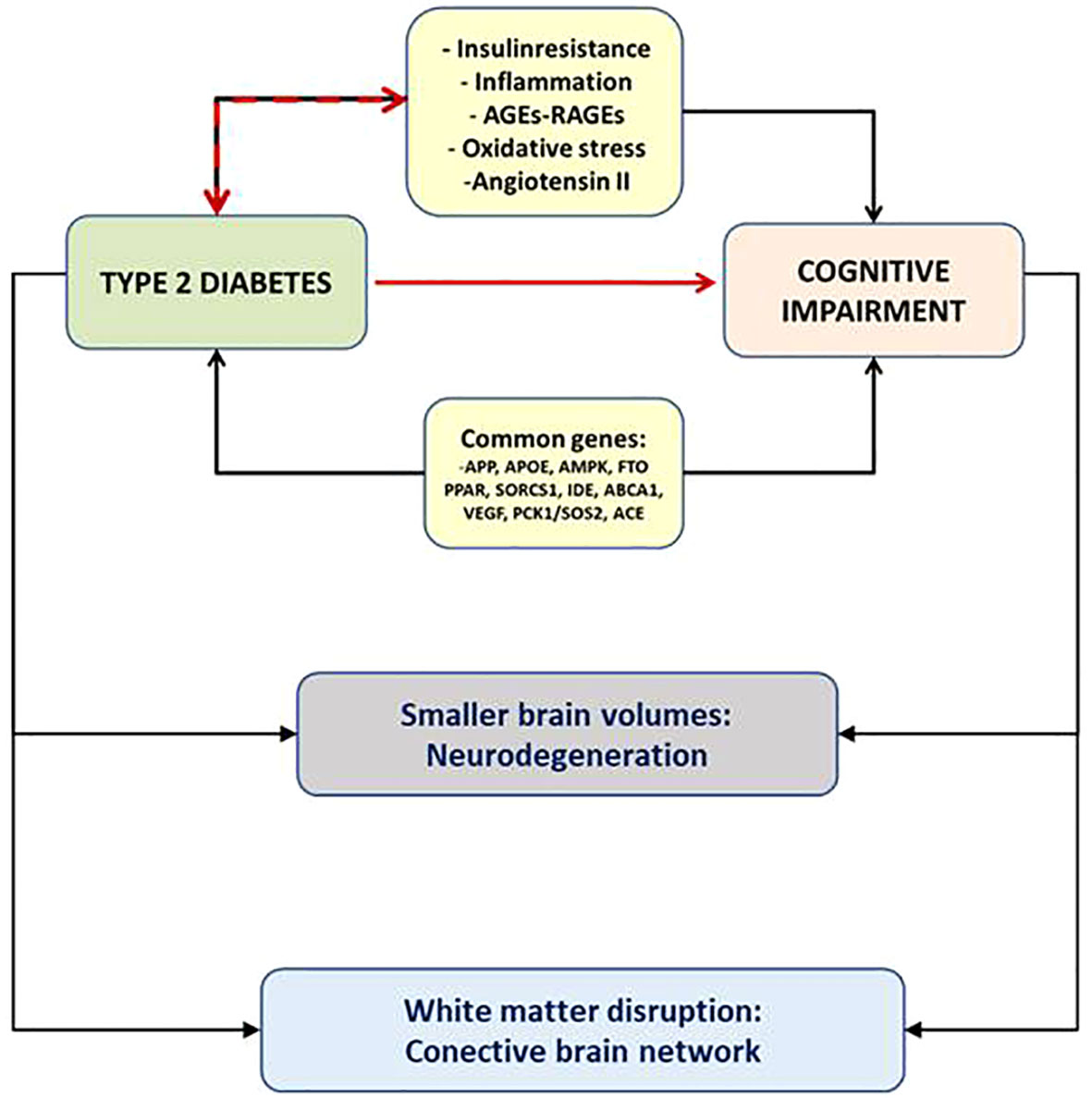
Figure 2 The eye as the window to the brain.
By adding the gaze fixation parameters to the retinal sensitivity the probability to identify cognitive impairment significantly increased in an independent manner, suggesting that retinal sensitivity and gaze fixation explore different neuronal circuits and are complementary (35), converting the retinal microperimetry into a potential useful tool for the screening of MCI in patients with T2D >65 years (with a sensitivity of 72.7% and sensibility of 87.9%).
Furthermore, we have recently evaluated the usefulness of retinal microperimetry as a monitoring tool for the cognitive function in patients >65 years with T2D (36). We found that the worsening in cognitive function went in parallel with worsening of gaze fixation, suggesting this parameter can be a reliable and more subtle tool for the monitoring of the cognitive function in patients with type 2 diabetes. These results suggest that since retinal sensitivity is a reliable screening tool for diagnosis, the evaluation of gaze fixation could represent a better biomarker for annual follow-up. As previously explained (35), this finding could be attributed to the fact that the brain areas involved in gaze fixation are not the same as in retinal sensitivity. Retinal sensibility relies on the retina and the neural pathway of vision, which includes the geniculate body and correlated with grey matter volumes in brain MRI in T2D patients with MCI and AD but not white matter (30), suggesting that could be a marker of neurodegeneration. On the other hand, gaze fixation depends on the complex white matter network (37).
It should be noted that fixation eye movements are affected by attention and working memory (38). In this regard, micro-saccade rates transiently decrease during an attentional task (39).The omnipause neurons (located in the nucleus raphe interpositus of the paramedian pontine reticular formation) or the superior colliculus (SC) are two of the main brain areas involved in fixation. It is possible that these areas are affected early in the neurodegenerative process (40). While performing the retinal microperimetry, the subjects are asked to maintain their gaze fixated on a central target, while stimuli with different intensities are presented at 37 points in 3 concentric circles of 2, 6, and 10 degrees of diameter (41). It could be hypothesized that subjects with cognitive impairment are unable to inhibit the saccades triggered by the most eccentric stimuli and maintain their gaze fixated on a central target. Furthermore, certain areas of the cerebral cortex, such as the parietal and frontal cortex (frontal eye fields and the dorsomedial prefrontal cortex), show elevated firing rates during fixation. These areas could contribute to the control of fixation through descending projections to the SC and the omnipause region (40).
Retinal microperimetry, used in the daily clinical practice, as part of the ophthalmological evaluation, is a simple, objective and rapid test that can be largely used for the monitoring of the cognitive performance, regardless of the educational level. Nevertheless, at present retinal microperimetry as a tool for the screening and monitoring of cognitive function has some limitations. First, the presence of advanced DR might be a limiting factor. However, we propose it as tool for early detection of cognitive impairment and at this stage a large percentage of patients with T2D present only mild or moderate DR. Secondly, the device might not be widely available in many primary or even tertiary care settings. Third, although it seems that the test is not influenced by psychological or mood status, at present there are no studies specifically aimed at evaluating this issue. For all these reasons we have to still consider retinal microperimetry as an emerging and promising tool that needs further validation and cost-effectiveness analysis.
These preliminary data, both on DSDRS and microperimetry have the potential of changing the current guidelines of clinical practice in patients with T2D if the results are confirmed in larger clinical trials. In this regard, a European project is ongoing (RECOGNISED study, NCT04281186), aimed at validating the usefulness of retinal microperimetry and DSRDS as reliable screening and monitoring tools for cognitive impairment in patients with T2D >65 years. These two tests can be easily implemented and applied at large scale in the daily clinic. If our results are confirmed, the DSDRS could be a screening tool that might easily be implemented and automatically calculated by the electronic medical records of the patients, as part of the daily clinical practice. Additionally, for the annual microperimetry performance in the ophthalmology clinic, an automatic software could provide reliable data on the patients with T2D>65 years that present significant changes in gaze fixation and retinal sensitivity annually, as possible patients at higher risk of progression of their cognitive impairment, on which diabetes care providers should focus and make an accurate diagnosis and management.
Cognitive impairment is an emerging condition in T2D but often remains undiagnosed due to lack of simple tools for screening at large scale. This is important because T2D patients with cognitive impairment are more prone to present an impaired self-management of diabetes, poor glycemic control and an increased incidence of diabetes-related complications. Unfortunately, current guidelines still recommend the use of tests that depend on the mood of the patient and the educational level, with modest sensitivity and specificity for identifying mild cognitive impairment. This represents an important gap because patients with mild cognitive impairment are at risk of progressing to dementia and the early and reliable identification at large scale will allow the implementation of a patient-centered treatment based on simplifying the regimes and prioritizing antidiabetic treatments with low capacity to provoke hypoglycemia. Recently, new methods have emerged as reliable tools for the cognitive evaluation in patients with T2D>65 years, such as DSRDS and more importantly, retinal microperimetry, that have the potential to change the current guidelines if preliminary results are confirmed in a large ongoing European trial (RECOGNISED).
AC: Conceptualization, first draft writing, revision. RS: Supervision, draft revision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ciudin A, Espinosa A, Simó-Servat O, Ruiz A, Alegret M, Hernández C, et al. Type 2 diabetes is an independent risk factor for dementia conversion in patients with mild cognitive impairment. J Diabetes Complications (2017) 31(8):1272–4. doi: 10.1016/j.jdiacomp.2017.04.018
2. Spauwen PJJ, Köhler S, Verhey FRJ, Stehouwer CDA, van Boxtel MPJ. Effects of type 2 diabetes on 12-year cognitive change: results from the maastricht aging study. Diabetes Care (2013) 36(6):1554–61. doi: 10.2337/dc12-0746
3. Simó R, Ciudin A, Simó-Servat O, Hernández C. Cognitive impairment and dementia: a new emerging complication of type 2 diabetes–the diabetologist’s perspective. Acta Diabetol (2017) 54(5):417–24. doi: 10.1007/s00592-017-0970-5
4. Espeland MA, Bryan RN, Goveas JS, Robinson JG, Siddiqui MS, Liu S, et al. Influence of type 2 diabetes on brain volumes and changes in brain volumes: Results from the women’s health initiative magnetic resonance imaging studies. Diabetes Care (2013) 36(1):90–7. doi: 10.2337/dc12-0555
5. Reijmer YD, Brundel M, de Bresser J, Kappelle LJ, Leemans A, Biessels GJ. Microstructural white matter abnormalities and cognitive functioning in type 2 diabetes: A diffusion tensor imaging study. Diabetes Care (2013) 36(1):137–44. doi: 10.2337/dc12-0493
6. Feinkohl I, Keller M, Robertson CM, Morling JR, Williamson RM, Nee LD, et al. Clinical and subclinical macrovascular disease as predictors of cognitive decline in older patients with type 2 diabetes: The Edinburgh type 2 diabetes study. Diabetes Care (2013) 36(9):2779–86.10.2337/dc12-2241
7. Hugenschmidt CE, Lovato JF, Ambrosius WT, Bryan RN, Gerstein HC, Horowitz KR, et al. The cross-sectional and longitudinal associations of diabetic retinopathy with cognitive function and brain MRI findings: The action to control cardiovascular risk in diabetes (ACCORD) trial. Diabetes Care (2014) 37(12):3244–52. doi: 10.2337/dc14-0502
8. Ding J, Strachan MWJ, Reynolds RM, Frier BM, Deary IJ, Fowkes FGR, et al. Diabetic retinopathy and cognitive decline in older people with type 2 diabetes: The Edinburgh type 2 diabetes studyDiabetes(2010)59(11):2883–9. doi: 10.2337/db10-0752
9. Exalto LG, Biessels GJ, Karter AJ, Huang ES, Quesenberry CP, Whitmer RA. Severe diabetic retinal disease and dementia risk in type 2 diabetes. J Alzheimer’s Disease (2014) 40(03):S109–17. doi: 10.3233/JAD-132570
10. Barzilay JI, Lovato JF, Murray AM, Williamson J, Ismail-Beigi F, Karl D, et al. Albuminuria and cognitive decline in people with diabetes and normal renal function. Clin J Am Soc Nephrol (2013) 8(11):1907–14. doi: 10.2215/CJN.11321112
11. Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. The diagnosis of mild cognitive impairment due to alzheimer’s disease: Recommendations from the national institute on aging-alzheimer’s association workgroups on diagnostic guidelines for alzheimer’s disease. Alzheimer’s Dementia (2011) 7(3):270–9. doi: 10.1016/j.jalz.2011.03.008
12. Cahill S. WHO’s global action plan on the public health response to dementia: some challenges and opportunities. Aging Ment Health (2020) 24:197–9. doi: 10.1080/13607863.2018.1544213
13. Abbatecola AM, Bo M, Barbagallo M, Incalzi RA, Pilotto A, Bellelli G, et al. Severe hypoglycemia is associated with antidiabetic oral treatment compared with insulin analogs in nursing home patients with type 2 diabetes and dementia: results from the DIMORA study. J Am Med Dir Assoc (2015) 16(4):349.e7–349.e12. doi: 10.1016/j.jamda.2014.12.014
14. Matsuhisa M, Kuroda A. New risk factors of severe hypoglycemia. J Diabetes Investig (2019) 10(2):219–20. doi: 10.1111/jdi.12925
15. Frier BM. Hypoglycaemia in diabetes mellitus: epidemiology and clinical implications. Nat Rev Endocrinol (2014) 10(12):711–22. doi: 10.1038/nrendo.2014.170
16. Sircar M, Bhatia A, Munshi M. Review of hypoglycemia in the older adult: Clinical implications and management. Can J Diabetes (2016) 40(1):66–72. doi: 10.1016/j.jcjd.2015.10.004
17. Meneilly GS, Tessier DM. Diabetes, dementia and hypoglycemia. Can J Diabetes (2016) 40(1):73–6. doi: 10.1016/j.jcjd.2015.09.006
18. American Diabetes Association. 2. Class1. American diabetes association. 2. classification and diagnosis of diabetes: Standards of medical care in diabetes-2018. Diabetes Care (2018) 41(Suppl 1):S13–27. doi: 10.2337/dc18-S002
19. Classification and diagnosis of diabetes: Standards of medical care in diabetes–2022. Diabetes Care (2022) 45. doi: 10.2337/dc22-S002
20. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res (1975) 12(3):189–98. doi: 10.1016/0022-3956(75)90026-6
21. Spering CC, Hobson V, Lucas JA, Menon CV, Hall JR, O’Bryant SE. Diagnostic accuracy of the MMSE in detecting probable and possible alzheimer’s disease in ethnically diverse highly educated individuals: an analysis of the NACC database. J Gerontol A Biol Sci Med Sci (2012) 67(8):890–6. doi: 10.1093/gerona/gls006
22. Arevalo-Rodriguez I, Smailagic N, Roqué-Figuls M, Ciapponi A, Sanchez-Perez E, Giannakou A, et al. Mini-mental state examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Systemat Rev (2021) 2021. doi: 10.1002/14651858.CD010783.pub3
23. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. J Am Geriatr Soc (2005) 53(4):695–9. doi: 10.1111/j.1532-5415.2005.53221.x
24. Dong YH, Lee WY, Basri NA, Collinson SL, Merchant RA, Venketasubramanian N, et al. The Montreal cognitive assessment is superior to the MiniMental state examination in detecting patients at higher risk of dementia. Int Psychogeriatr (2012) 24(11):1749–55. doi: 10.1017/S1041610212001068
25. Sullivan MD, Katon WJ, Lovato LC, Miller ME, Murray AM, Horowitz KR, et al. Association of depression with accelerated cognitive decline among patients with type 2 diabetes in the ACCORD-MIND trial. JAMA Psychiatry (2013) 70(10):1041–7.10.1001/jamapsychiatry.2013.1965
26. Roy T, Lloyd CE. Epidemiology of depression and diabetes: A systematic review. J Affect Disord (2012) 142(Suppl):S8–S21. doi: 10.1016/S0165-0327(12)70004-6
27. Nicolau J, Simó R, Sanchís P, Ayala L, Fortuny R, Rivera R, et al. Prevalence and clinical correlators of undiagnosed significant depressive symptoms among individuals with type 2 diabetes in a Mediterranean population. Exp Clin Endocrinol Diabetes (2016) 124(10):630–6.10.1055/s-0042-109606
28. Cardiovascular disease and risk management: Standards of medical care in diabetes–2022. Diabetes Care (2022) 45:S144–74. doi: 10.2337/dc22-S010
29. Exalto LG, Biessels GJ, Karter AJ, Huang ES, Katon WJ, Minkoff JR, et al. Risk score for prediction of 10 year dementia risk in individuals with type 2 diabetes: a cohort study. Lancet Diabetes Endocrinol (2013) 1(3):183–90.10.1016/S2213-8587(13)70048-2
30. Ciudin A, Simó-Servat O, Hernández C, Arcos G, Diego S, Sanabria Á, et al. Retinal microperimetry: A new tool for identifying patients with type 2 diabetes at risk for developing Alzheimer disease. Diabetes (2017) 66(12):3098–04. doi: 10.2337/db17-0382
31. Bello-Chavolla OY, Aguilar-Salinas CA, Avila-Funes JA. The type 2 diabetes-specific dementia risk score (DSDRS) is associated with frailty, cognitive and functional status amongst Mexican community-dwelling older adults. BMC Geriatr (2020) 20(1):1–10. doi: 10.1186/s12877-020-01776-5
32. Rodríguez-Gómez O, Rodrigo A, Iradier F, Santos-Santos MA, Hundemer H, Ciudin A, et al. The MOPEAD project: Advancing patient engagement for the detection of “hidden” undiagnosed cases of alzheimer’s disease in the community. Alzheimer’s Dementia (2019) 15:828–39. doi: 10.1016/j.jalz.2019.02.003
33. Zuñiga AMO, Simó R, Rodriguez-Gómez O, Hernández C, Rodrigo A, Jamilis L, et al. Clinical applicability of the specific risk score of dementia in type 2 diabetes in the identification of patients with early cognitive impairment: Results of the mopead study in Spain. J Clin Med (2020) 9(9):2726. doi: 10.3390/jcm9092726.
34. Wu Z, Ayton LN, Guymer RH, Luu CD. Comparison between multifocal electroretinography and microperimetry in age-related macular degeneration. Invest Ophthalmol Vis Sci (2014) 55(10):6431–9. doi: 10.1167/iovs.14-14407
35. Simó-Servat O, Ciudin A, Ortiz-Zúñiga ÁM, Hernández C, Simó R. Usefulness of eye fixation assessment for identifying type 2 diabetic subjects at risk of dementia. . J Clin Med (2019) 8(1):59–64.
36. Ortiz-Zúñiga ÁM, Simó-Servat O, Rojano-Toimil A, Vázquez-de Sebastian J, Castellano-Tejedor C, Hernández C, et al. The gaze fixation assessed by microperimetry: A useful tool for the monitoring of the cognitive function in patients with type 2 diabetes. J Pers Med (2021) 11(8):698.
37. Ciudin A, Ortiz-Zuñiga AM, Fidilio E, Romero D, Sánchez M, Comas M, et al. Retinal microperimetry: A useful tool for detecting insulin resistance-related cognitive impairment in morbid obesity. J Clin Med (2019) 8(12):2181.
38. Molitor RJ, Ko PC, Ally BA. Eye movements in alzheimer’s disease. J Alzheimers Dis (2015) 44(1):1–12.
39. Martinez-Conde S. Fixational eye movements in normal and pathological vision. Prog Brain Res (2006) 154(SUPPL. A):151–76.
40. Krauzlis RJ, Goffart L, Hafed ZM. Neuronal control of fixation and fixational eye movements. Philos Trans R Soc Lond B Biol Sci (2017) 372(1718).
Keywords: type 2 diabetes, mild cognitive impairment, dementia, retinal microperimetry, neuropsychological tests
Citation: Ciudin A and Simó R (2022) New methods for the diagnosis and monitoring of cognitive function in patients with type 2 diabetes. Front. Endocrinol. 13:1024794. doi: 10.3389/fendo.2022.1024794
Received: 22 August 2022; Accepted: 04 November 2022;
Published: 01 December 2022.
Edited by:
Victor Alan Gault, Ulster University, United KingdomReviewed by:
Weigang Gong, Qilu Hospital, Shandong University, ChinaCopyright © 2022 Ciudin and Simó. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andreea Ciudin, YW5kcmVlYS5jaXVkaW5AdmFsbGhlYnJvbi5jYXQ=; Rafael Simó, cmFmYWVsLnNpbW9Admhpci5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.