Abstract
Background:
There is accumulating evidence support human epidermal growth factor receptor 2 (HER2)-low as a biologically distinct subtype of breast cancer. The present study was conducted to explore whether HER2-low expression will affect the clinical efficacy of cyclin-dependent kinase (CDK) 4/6 inhibitor for patients with hormone receptor (HR)-positive, HER-2 negative metastatic breast cancer.
Methods:
Patients with HR+/HER2- metastatic breast cancer who were treated with palbociclib from January 2019 to June 2021 were retrospectively analyzed based on real-world clinical practice. HER2-zero was defined as immunohistochemistry (IHC) 0, and HER2-low was defined as IHC 1+ or IHC 2+/fluorescence in situ hybridization (FISH) negative. The primary end point was progression free survival (PFS), and the secondary end points were objective response rate (ORR), disease control rate (DCR), overall survival(OS) and safety.
Results:
45 patients received palbociclib plus aromatase inhibitor (AI) or fulvestrant therapy, including 24 HER-2-zero and 21 HER-2-low patients. There were no statistically significant differences in clinicopathological characteristics between the two groups. No significant differences were observed in ORR (41.7% vs. 28.6%, P=0.360) and DCR (79.2% vs. 76.2%, P=0.811) between HER-2-zero and HER-2-low patients. And simultaneously, HER2-zero and HER2-low patients obtained similar median PFS (16.2m vs. 14.1m, P=0.263). The median OS was not reached. Neutropenia and leukopenia were the most common adverse events. Grade 3-4 adverse events(AEs) occurred in 58.3% and 57.1% of patients, respectively.
Conclusions:
HER2-low expression does not affect the clinical efficacy of palbociclib and our present study did not support incorporating HER2-low into systemic therapy decisions for patients with HR+/HER2- metastatic breast cancer treated with CDK4/6 inhibitor.
Introduction
Global cancer registration data in 2020 demonstrated that breast cancer has become the most common malignant tumor in the world, accounting for 11.7% of all cancers (1). Although the overall treatment level of breast cancer has improved significantly in recent years, metastatic breast cancer is still a bottleneck affecting the prognosis of patients. With the success of the PALOMA (2–4), MONARCH (5–7) and MONALEESA (8–10) series of trials, cyclin-dependent kinase (CDK) 4/6 inhibitor plus traditional endocrine therapy has become the standard treatment strategy for hormone receptor (HR)-positive and human epidermal growth factor receptor 2 (HER2) negative metastatic breast cancer, which prompting HR+/HER2- metastatic breast cancer to enter a new era of targeted therapy combined endocrine therapy.
Many clinical studies have demonstrated that antibody drug conjugate(ADC) drugs are not only effective in HER2-positive breast cancer, but also show good anti-tumor activity in patients with low HER2 expression (11, 12). And there is accumulating evidence support HER2-low as a distinct subtype of breast cancer (13). Most clinical trials use immunohistochemistry (IHC) 1+, or IHC 2+ and FISH negative as the definition of HER2-low breast cancer and the proportion of people with HER2 low expression is as high as 45%-55% with this diagnostic criteria (14, 15). However, there has been little focus on this patient population with low expression of HER2 due to lack of understanding of its biological behavior and absence of tailored treatment manner.
Our previous research confirmed that HER2-low breast cancer exhibit specific clinicopathological features and different response to neoadjuvant chemotherapy (NAC). However, there have been no reports on whether the low expression of HER2 is related to the treatment response of endocrine therapy for metastatic breast cancer. The present study was conducted to explore whether HER2-low expression will affect the clinical efficacy of endocrine therapy for patients with HR+/HER2- metastatic breast cancer who received CDK4/6 inhibitor.
Methods
Patient population
From January 2019 to June 2021, patients with HR+/HER2- metastatic breast cancer who have received palbociclib plus aromatase inhibitor (AI) or fulvestrant therapy at Henan Provincial People’s Hospital were retrospectively collected in this study. The main selection criteria included: 1) histopathological confirmed metastatic breast cancer; 2) HR+/HER2 negative, which determined by immunohistochemistry (IHC) or fluorescence in situ hybridization (FISH); 3) have received palbociclib plus AI or fulvestrant therapy; 4) based on RECIST v1.1, presence of at least one measurable lesion. The exclusion criteria included: 1) received less than two cycles of palbociclib plus AI or fulvestrant treatment and could not evaluate the efficacy; 2) follow-up data are not available.
Treatment and follow-up
Estrogen receptor (ER) and progesterone receptor (PR) were detected by IHC, and the cut-off value was set to ≥1%. HR (hormone-receptor) positive was defined as ER or PR positive. The detection of HER2 refers to the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines for HER2 testing. HER2 negative breast cancer was divided into two groups: HER2-zero and HER2-low. HER2-zero was defined as IHC 0, and HER2-low was defined as IHC 1+ or IHC 2+/FISH negative.
In this study, the patients received palbociclib plus AI or fulvestrant therapy until disease progression, death or unacceptable toxicity. Palbociclib was given at a dose of 125mg orally as the initial dose once a day on d1 to d21 every four weeks. Anastrozole or fulvestrant was administered concurrently. Fulvestrant was administered intramuscularly at a dose of 500 mg on d1 and d15 of cycle 1 and then every four weeks from cycle 2. Anastrozole 1mg was administered orally on a continuous daily dosing schedule. For premenopausal patients, gonadotropin-releasing hormone (GnRH) agonist was administered before endocrine therapy. 3.6 mg of goserelin was injected subcutaneously once every 28 days. After treatment, imaging examinations were performed after every two cycles of in all patients to evaluate the clinical efficacy.
Statistical analysis
All the statistical analyses were performed with SPSS 22.0 software (SPSS Inc., IL, US) software. P<0.05 was considered significant. Pearson’s chi squared test or Fisher’s exact test were used to compare the difference between groups. Survival curves of patients were estimated by the Kaplan-Meier method. The follow-up deadline is June 1, 2021. Progression free survival (PFS) was defined as from the date of palbociclib treatment to disease progression or death. Overall survival (OS) was defined as from the date of palbociclib treatment to patient death or last follow-up.
Results
Patient and treatment
A total of 45 patients were enrolled in the present study. Table 1 shows patient and treatment characteristics. In the entire cohort, 73.3% patients were ECOG PS 0-1 and 26.7% patients were ECOG PS 2. The proportion of premenopausal patients is 64.4%, and 35.6% patients were postmenopausal. The disease status in 4(8.9%) patients was initial diagnosis stage IV, and in 41(91.1%) patients was recurrence and metastasis. Therefore, most patients in this study had received prior surgery (41,91.1%), neo-adjuvant/adjuvant chemotherapy (32,71.1%) and adjuvant endocrine therapy (39,86.7%).
Table 1
| Characteristic | Total (n = 45) n (%) | HER2-zero (n = 24) n (%) | HER2-low (n = 21) n (%) | P |
|---|---|---|---|---|
| Age (years, median) | 50 (27-84) | 43 (27-84) | 54 (36-73) | |
| ECOG | 0.280 | |||
| 0-1 | 33 (73.3) | 16 (66.7) | 17 (81.0) | |
| 2 | 12 (26.7) | 8 (33.3) | 4 (19.0) | |
| Menopausal status | 0.739 | |||
| Premenopausal | 29 (64.4) | 16 (66.7) | 13 (61.9) | |
| Postmenopausal | 16 (35.6) | 8 (33.3) | 8 (38.1) | |
| Prior chemotherapy before metastasis | 0.965 | |||
| Neo-adjuvant/Adjuvant | 32 (71.1) | 17 (70.8) | 15 (71.4) | |
| None | 13 (28.9) | 7 (29.2) | 6 (28.6) | |
| Prior adjuvant endocrine therapy | 0.691 | |||
| Tamoxifen | 21 (46.7) | 10 (41.7) | 11 (52.4) | |
| AI | 18 (40.0) | 10 (41.7) | 8 (38.1) | |
| None | 6 (13.3) | 4 (16.7) | 2 (9.5) | |
| Prior surgery before metastasis | 0.889 | |||
| Yes | 41 (91.1) | 22 (91.7) | 19 (90.5) | |
| No | 4 (8.9) | 2 (8.3) | 2 (9.5) | |
| Disease status | 0.889 | |||
| Initial diagnosis stage IV | 4 (8.9) | 2 (8.3) | 2 (9.5) | |
| Recurrence and metastasis | 41 (91.1) | 22 (91.7) | 19 (90.5) | |
| HR status at metastasis stage | 0.718 | |||
| ER+ and PR+ | 32 (71.1) | 17 (70.8) | 15 (71.4) | |
| ER+ and PR- | 10 (22.2) | 6 (25.0) | 4 (19.0) | |
| ER- and PR+ | 3 (6.7) | 1 (4.2) | 2 (9.5) | |
| Metastatic site | 0.432 | |||
| Lymph node | 17 (37.8) | 9 (37.5) | 8 (38.1) | |
| Chest wall | 8 (17.8) | 2 (8.3) | 6 (28.6) | |
| Liver | 11 (24.4) | 7 (29.2) | 4 (19.0) | |
| Lung | 20 (44.4) | 8 (33.3) | 12 (57.1) | |
| Bone | 29 (64.4) | 17 (70.8) | 12 (57.1) | |
| Brain | 3 (6.7) | 1 (4.2) | 2 (9.5) | |
| Number of metastatic sites | 0.565 | |||
| 1-2 | 28 (62.2) | 14 (58.3) | 14 (66.7) | |
| ≥ 3 | 17 (37.8) | 10 (41.7) | 7 (33.3) | |
| Metastatic sites type | 0.322 | |||
| Visceral | 31 (68.9) | 15 (62.5) | 16 (76.2) | |
| Non-Visceral | 14 (31.1) | 9 (37.5) | 5 (23.8) | |
| Prior chemotherapy after metastasis | 0.511 | |||
| Yes | 17 (37.8) | 8 (33.3) | 9 (42.9) | |
| No | 28 (62.2) | 16 (66.7) | 12 (57.1) | |
| Prior endocrine therapy after metastasis | 0.580 | |||
| AI | 23 (51.1) | 14 (58.3) | 9 (42.9) | |
| Fulvestrant | 4 (8.9) | 2 (8.3) | 2 (9.5) | |
| None | 22 (48.9) | 10 (41.7) | 12 (57.1) | |
| Treatment manner | 0.632 | |||
| CDK4/6 + AI | 24 (53.3) | 12 (50.0) | 12 (57.1) | |
| CDK4/6 + Fulvestrant | 21 (46.7) | 12 (50.0) | 9 (42.9) | |
| Treatment line | 0.951 | |||
| 1 | 14 (31.1) | 7 (29.2) | 7 (33.3) | |
| 2 | 18 (40.0) | 10 (41.7) | 8 (38.1) | |
| ≥ 3 | 13 (28.9) | 7 (29.2) | 6 (28.6) |
Patient and treatment characteristics.
ECOG, Eastern Cooperative Oncology Group; HR, hormone receptor; AI, aromatase inhibitor; CDK4/6, cyclin-dependent kinase 4 and 6.
The proportions of ER+/PR+, ER+/PR- and ER-/PR+ at metastasis stage were 71.1%, 22.2% and 6.7%, respectively. The common metastatic sites included bone (64.4%), lung (44.4%), lymph node (37.8%), liver (24.4%), chest wall (17.8%) and brain (6.7%). Number of metastatic sites in 28 (62.2%) patients were 1 or 2, and the other 17 (37.8%) patients were 3 or more. Thirty-one patients (68.9%) had visceral metastasis, and the other 14 patients (31.1%) had non-visceral metastasis. In metastatic disease stage, 37.8% patients had received chemotherapy and 51.1% patients had received endocrine therapy, including AI and fulvestrant. Palbociclib was administered as first line in 14 (31.1%) patients, as second line in 18 (40.0%) patients and as third or above line in 13 (28.9%) patients. 24 (53.3%) patients received palbociclib plus anastrozole and the other 21 (46.7%) patients received palbociclib plus fulvestrant.
In the the entire cohort, 24 (53.3%) patients were HER2-zero, and 21 (46.7%) patients were HER2-low. There were no statistically significant differences between HER2-zero and HER2-low breast cancer with respect to baseline clinicopathological characteristics.
Efficacy
In the the entire cohort, complete response (CR) was not obtained, 16 patients had partial response (PR), 19 patients were evaluated as stable disease (SD) and 10 patients were evaluated as progressive disease (PD). The overall ORR and DCR were 35.6% (16/45) and 77.8% (35/45), respectively (Table 2). In HER2-zero breast cancer patients, CR was not obtained, 10 patients had PR, 9 patients were evaluated as SD and 5 patients were evaluated as PD. The overall ORR and DCR were 41.7% (10/24) and 79.2% (19/24), respectively. In HER2-low breast cancer patients, CR was not obtained, 6 patients had PR, 10 patients were evaluated as SD and 5 patients were evaluated as PD. The overall ORR and DCR were 28.6% (6/21) and 76.2% (16/21), respectively. There were no significant differences in ORR and DCR between HER2-zero and HER2-low breast cancer patients. Although there is no statistical difference, the ORR and DCR in patients who received palbociclib as third or above line therapy were inferior to patients who received palbociclib as first and second line therapy. There were also no statistically significant differences in ORR and DCR with respect to treatment manner (CDK4/6 + AI vs. CDK4/6 + Fulvestrant) and metastatic sites type (non-Visceral vs. visceral).
Table 2
| Parameter | Best response | ORR | P | DCR | P | Median PFS (95%CI) | P | |||
|---|---|---|---|---|---|---|---|---|---|---|
| CR | PR | SD | PD | |||||||
| Total | 0 | 16 | 19 | 10 | 35.6% | 77.8% | 16.2(12.0-20.4) | |||
| HER2 status | 0.360 | 0.811 | 0.263 | |||||||
| HER2-zero | 0 | 10 | 9 | 5 | 41.7% | 79.2% | 16.2(10.9-21.5) | |||
| HER2-low | 0 | 6 | 10 | 5 | 28.6% | 76.2% | 14.1(9.0-19.2) | |||
| Treatment line | 0.196 | 0.589 | 0.019 | |||||||
| First-line | 0 | 6 | 6 | 2 | 42.9% | 85.7% | 22.6(19.3-25.9) | |||
| Second-line | 0 | 8 | 6 | 4 | 44.4% | 77.8% | 16.5(10.1-22.9) | |||
| Third-line or above | 0 | 2 | 7 | 4 | 15.4% | 69.2% | 10.8(9.3-12.3) | |||
| Treatment manner | 0.771 | 0.231 | 0.115 | |||||||
| CDK4/6 + AI | 0 | 9 | 8 | 7 | 37.5% | 70.8% | 10.8(2.9-18.7) | |||
| CDK4/6 + Fulvestrant | 0 | 7 | 11 | 3 | 33.3% | 85.7% | 16.9(10.1-23.7) | |||
| Metastatic sites type | 0.511 | 0.102 | 0.158 | |||||||
| Non-Visceral | 0 | 4 | 9 | 1 | 28.6% | 92.9% | 21.5(12.9-30.1) | |||
| Visceral | 0 | 12 | 10 | 9 | 38.7% | 71.0% | 12.9(6.3-19.5) | |||
Efficacy of CDK4/6 inhibitor treatment in metastatic breast cancer.
CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; ORR, overall response rate; DCR, disease control rate; PFS, progression free survival; OS, overall survival. Bold values: P–0.05.
In the the entire cohort, the median PFS was 16.2 (95% CI= 12.0-20.4) months (Figure 1) and the median OS was not reached. The median PFS were 16.2 (95%CI=10.9-21.5) and 14.1 (95%CI=9.0-19.2) months in the HER2-zero and HER2-low breast cancer patients, respectively (P=0.263; Figure 2A). The median PFS in patients who received palbociclib as third or above line therapy was 10.8 (95%CI=9.3-12.3) months, which was worse than patients who received palbociclib as first [22.6 (95%CI=19.3-25.9) months] and second [16.5 (95%CI=10.1-22.9) months] line therapy (P=0.019; Figure 2B). There were also no statistically significant differences in median PFS with respect to treatment manner (CDK4/6 + AI vs. CDK4/6 + Fulvestrant) and metastatic sites type (non-Visceral vs. visceral) (Figures 2C, D).
Figure 1

Kaplan-Meier curve of PFS in the entire cohort.
Figure 2
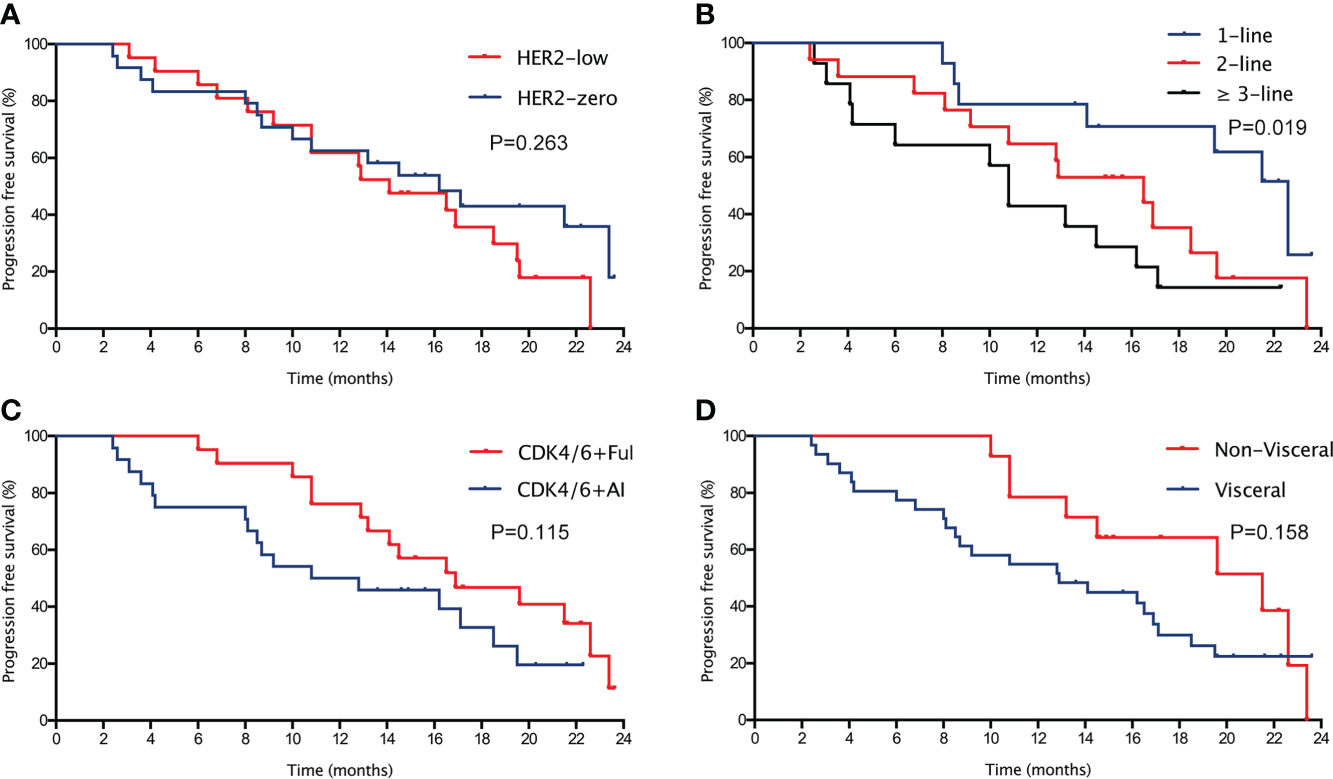
Kaplan-Meier curve of PFS (A) in the entire cohort with different HER2 status (HER2-zero vs. HER2-low). Kaplan-Meier curve of PFS (B) in patients with different treatment line (first-line, second-line vs. third-line or above). Kaplan-Meier curve of PFS (C) in patients with different treatment manner (CDK4/6 + AI vs. CDK4/6 + fulvestrant). Kaplan-Meier curve of PFS (D) in patients with different metastatic sites type (non-visceral vs. visceral).
Safety
The spectrum of treatment-related toxicity was consistent with previous clinical studies. Treatment-related death and unexpected side effects were not occurred (Table 3). Treatment was temporarily interrupted in 28 (62.2%) patients as a result of adverse events (AEs), and 8 (17.8%) patients underwent dose reductions due to grade 3-4 AEs. The most common treatment-related AEs was hematological toxicity, including neutropenia (38, 84.4%), leukopenia (22, 48.9%), decreased platelet (11, 24.4%) and anemia (9, 20.0%). The common non-hematological toxicity were fatigue (19, 42.2%), asthenia (16, 35.6%), rash (8, 17.8%), constipation (8, 17.8%), anorexia (7, 15.6%), alopecia (7, 15.6%), nausea or vomiting (6, 13.4%) and diarrhea (5, 11.1%). The incidence of grade 3-4 AEs was 57.8%, including neutropenia, leukopenia, increased alanine aminotransferase (ALT)/aspartate aminotransferase (AST) and diarrhea.
Table 3
| Adverse Event | All | HER2-zero | HER2-low | |||||
|---|---|---|---|---|---|---|---|---|
| All Grade | ≥ Grade3 | All Grade | ≥ Grade3 | All Grade | ≥ Grade3 | |||
| Non-hematologic | ||||||||
| Alopecia | 7 (15.6) | 0 | 3 (12.5) | 0 | 4 (19.0) | 0 | ||
| Fatigue | 19 (42.2) | 0 | 10 (41.7) | 0 | 9 (42.9) | 0 | ||
| Nausea or Vomiting | 6 (13.3) | 0 | 3 (12.5) | 0 | 3 (14.3) | 0 | ||
| Anorexia | 7 (15.6) | 0 | 4 (16.7) | 0 | 3 (14.3) | 0 | ||
| Diarrhea | 5 (11.1) | 1 (2.2) | 3 (12.5) | 1 (4.2) | 2 (9.5) | 0 | ||
| Muscle pain/joint pain | 4 (8.9) | 0 | 2 (8.3) | 0 | 2 (9.5) | 0 | ||
| Constipation | 8 (17.8) | 0 | 4 (16.7) | 0 | 4 (19.0) | 0 | ||
| Pyrexia | 4 (8.9) | 0 | 3 (12.5) | 0 | 1 (4.8) | 0 | ||
| Rash | 8 (17.8) | 0 | 4 (16.7) | 0 | 4 (19.0) | 0 | ||
| Oral mucositis | 3 (6.7) | 0 | 2 (8.3) | 0 | 1 (4.8) | 0 | ||
| Asthenia | 16 (35.6) | 0 | 8 (33.3) | 0 | 8 (38.1) | 0 | ||
| Hematologic | ||||||||
| Leukopenia | 22 (48.9) | 9 (20.0) | 11 (45.8) | 5 (20.8) | 11(52.4) | 4(19.0) | ||
| Neutropenia | 38 (84.4) | 25 (55.6) | 20 (83.3) | 13 (54.2) | 18 (85.7) | 12 (57.1) | ||
| Anemia | 9 (20.0) | 0 | 4 (16.7) | 0 | 5 (23.8) | 0 | ||
| Decreased platelet | 11 (24.4) | 0 | 5 (20.8) | 0 | 6 (28.6) | 0 | ||
| Increased ALT/AST | 5 (11.1) | 1 (2.2) | 3 (12.5) | 0 | 2 (9.5) | 1 (4.8) | ||
Treatment-related toxicity.
The number of patients with interruptions and dose reduction as a result of AEs in HER2-zero breast cancer were 15(62.5%) and 4(16.7%), while in HER2-low breast cancer were 13(61.9%) and 4(19.0%), respectively. The incidence of grade 3-4 AEs in these two groups were 58.3% and 57.1%, respectively. These were no statistically significant differences in treatment-related toxicity among breast cancer patients with HER2-zero and HER2-low.
Discussion
The present study compared the clinical efficacy of CDK4/6 inhibitor for HR positive patients with HER2-zero or HER2-low metastatic breast cancer, no significant differences were observed in treatment response and median PFS between the two groups. To our knowledge, until now this is the first study of evaluating whether HER2-low expression will affect the clinical efficacy of CDK4/6 inhibitor for patients with HR+/HER2- metastatic breast cancer based on real-world clinical practice. Our present study demonstrated that HER2-low expression does not affect the clinical efficacy of palbociclib, which did not support incorporating HER2-low into systemic therapy decisions for patients with HR+/HER2- metastatic breast cancer treated with CDK4/6 inhibitor.
In breast cancer, about 15%-20% of patients have abnormal amplification or overexpression of HER2 gene (16). HER2 status has become an important indicator for molecular typing of breast cancer, and simultaneously, HER2 is also an important target for breast cancer (17). The clinical application of anti HER2 targeted drugs represented by trastuzumab in neoadjuvant therapy, adjuvant therapy and advanced rescue therapy has changed the diagnosis and treatment mode of breast cancer, and also greatly improved the prognosis of HER2 positive breast cancer patients (18–20). However, the expression level of HER2 was a continuous process in pathology, rather than the concept of absolute distinction between positive and negative (21, 22). Therefore, the concept of HER2 low expression emerged (23). Most clinical trials use IHC 1+, or IHC 2+ and FISH negative as the definition of HER2-low breast cancer. The proportion of breast cancer with HER2 low expression is as high as 45%-55% according to this criteria. So far, little is currently known about the biological behavior of tumors with HER2 low expression.
There is still controversy over HER2-low as a distinct biological subtype of breast cancer. Several previous studies suggested that the proportion of HER2-low in HR positive breast cancer was higher than in triple negative breast cancer (TNBC) (24). Data from our institution demonstrated that in HR positive breast cancer, HER2-low patients showed less lymph node metastatic burden and earlier stage. In contrast, HER2-low breast cancer had later clinical stage than HER2-zero patients in TNBC. Another study suggested that histological grade 2 was more common in patients with HER2-low breast cancer, and the expression level of Ki67 was significantly lower than that in patients with HER2-zero (25). PAM50 gene analysis showed that in HR+ breast cancer, HER2-low breast cancer had more expressed ERBB2 and luminal-related genes than HER2-zero breast cancer, but not in TNBC (26). The genomic data from 523 breast cancer patients suggested that HER2-low and HER2-zero breast cancer exhibit distinct gene mutation signatures (27). HER2-zero tumors had more gene mutations in p53 signaling and cell cycle pathway, and HER2-low breast cancer exhibit more gene mutations which involved in PI3K-Akt signaling pathway. However, in metastatic breast cancer, whether HER2-low and HER2-zero breast cancer differ in clinical and gene expression features has not been reported. In our present study, no significant differences were found between HER2-zero and HER2-low metastatic breast cancer in clinical and pathological characteristics.
Low expression of HER2 may be related to treatment efficacy of breast cancer. In neoadjuvant chemotherapy (NAC) setting, a previous pooled analysis of four neoadjuvant chemotherapy clinical trials (GeparSepto, GeparOcto, GeparX, and Gain-2 neoadjuvant) confirmed that HER2-low breast cancer had a significantly lower pathological complete response(pCR) rate than HER2-zero patients (24). Our recent study analyzed 314 HER2 negative breast cancer patients who received NAC and found that with the pCR defined as ypT0ypN0, the pCR rate in HER2-low breast cancer was significantly lower than HER2-zero breast cancer in entire cohort(24.3% vs. 36.4%, P=0.032) and HR-positive subgroup(18.7% vs. 32.1%, P=0.035). In targeted anti-HER2 therapy for metastatic breast cancer setting, DS8201-A-J101, DESTINY-Breast04 and DESTINY-Breast06 studies showed that trastuzumab deruxtecan (T-DXd, DS-8201a) provide a novel treatment strategy for patients with low HER2 expression (11, 12). In endocrine therapy for metastatic breast cancer setting, our present study compared the clinical efficacy of CDK4/6 inhibitor for patients with HR positive HER2-zero and HER2-low metastatic breast cancer, no significant differences were observed in treatment response and patient prognosis. In this study, we show for the first time that HER2-low expression does not affect the clinical outcomes of metastatic breast cancer treated with CDK4/6 inhibitor.
Treatment-related toxicity of palbociclib was consistent with previous relevant clinical trials, hematological toxicity was the most common AEs (28–30). No statistically significant differences in treatment-related toxicity between HER2-zero and HER2-low breast cancer patients were found, including the incidence of grade 3-4 AEs, interruptions and dose reduction.
Our present study has several limitations, because it is a single center and observational study, and the number of patients included is not many. Therefore, the results of this study need future validation clinical trials to confirm whether HER2-low expression will affect the treatment decision of metastatic breast cancer.
Conclusion
In conclusion, these data confirm that HER2-low expression does not affect the clinical efficacy of palbociclib and our present study did not support incorporating HER2-low into systemic therapy decisions for patients with HR+/HER2- metastatic breast cancer treated with CDK4/6 inhibitor.
Funding
This work was supported by Beijing Medical Award Foundation Project (No.YXJL-2020-0941-0748) and Medical Science and Technique Foundation of Henan Province (No. LHGJ20210055).
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by The ethics committee of the Henan Provincial People’s Hospital. The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors contributed to the article and approved the submitted version. YS and HL designed the research, analyzed the data and drafted the paper. YS, ZL, YY, and QC were mainly responsible for data collection and analysis. YH, CL, BN and FZ were primarily responsible for statistical analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1
Siegel RL Miller KD Jemal A . Cancer statistics, 2020. CA Cancer J Clin (2020) 70(1):7–30. doi: 10.3322/caac.21590
2
Cristofanilli M Turner NC Bondarenko I Ro J Im SA Masuda N et al . Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol (2016) 17(4):425–39. doi: 10.1016/S1470-2045(15)00613-0
3
Finn RS Crown JP Lang I Boer K Bondarenko IM Kulyk SO et al . The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol (2015) 16(1):25–35. doi: 10.1016/S1470-2045(14)71159-3
4
Rugo HS Finn RS Gelmon K Joy AA Harbeck N Castrellon A et al . Progression-free survival outcome is independent of objective response in patients with estrogen receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer treated with palbociclib plus letrozole compared with letrozole: Analysis from PALOMA-2. Clin Breast Cancer (2020) 20(2):e173–80. doi: 10.1016/j.clbc.2019.08.009
5
Sledge GW Jr. Toi M Neven P Sohn J Inoue K Pivot X et al . The effect of abemaciclib plus fulvestrant on overall survival in hormone receptor-positive, ERBB2-negative breast cancer that progressed on endocrine therapy-MONARCH 2: A randomized clinical trial. JAMA Oncol (2020) 6(1):116–24. doi: 10.1001/jamaoncol.2019.4782
6
Goetz MP Toi M Campone M Sohn J Paluch-Shimon S Huober J et al . MONARCH 3: Abemaciclib as initial therapy for advanced breast cancer. J Clin Oncol (2017) 35(32):3638–46. doi: 10.1200/JCO.2017.75.6155
7
Dickler MN Tolaney SM Rugo HS Cortes J Dieras V Patt D et al . MONARCH 1, a phase II study of abemaciclib, a CDK4 and CDK6 inhibitor, as a single agent, in patients with refractory HR(+)/HER2(-) metastatic breast cancer. Clin Cancer Res (2017) 23(17):5218–24. doi: 10.1158/1078-0432.CCR-17-0754
8
Lu YS Im SA Colleoni M Franke F Bardia A Cardoso F et al . Updated overall survival of ribociclib plus endocrine therapy versus endocrine therapy alone in pre- and perimenopausal patients with HR+/HER2- advanced breast cancer in MONALEESA-7: A phase III randomized clinical trial. Clin Cancer Res (2022) 28(5):851–9. doi: 10.1158/1078-0432.CCR-21-3032
9
Slamon DJ Neven P Chia S Jerusalem G De Laurentiis M Im S et al . Ribociclib plus fulvestrant for postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the phase III randomized MONALEESA-3 trial: updated overall survival. Ann Oncol (2021) 32(8):1015–24. doi: 10.1016/j.annonc.2021.05.353
10
Hortobagyi GN Stemmer SM Burris HA Yap YS Sonke GS Paluch-Shimon S et al . Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol (2018) 29(7):1541–7. doi: 10.1093/annonc/mdy155
11
Modi S Park H Murthy RK Iwata H Tamura K Tsurutani J et al . Antitumor activity and safety of trastuzumab deruxtecan in patients with HER2-Low-Expressing advanced breast cancer: Results from a phase ib study. J Clin Oncol (2020) 38(17):1887–96. doi: 10.1200/JCO.19.02318
12
Modi S Jacot W Yamashita T Sohn J Vidal M Tokunaga E et al . Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med (2022) 387(1):9–20. doi: 10.1056/NEJMoa2203690
13
Tarantino P Hamilton E Tolaney SM Cortes J Morganti S Ferraro E et al . HER2-low breast cancer: Pathological and clinical landscape. J Clin Oncol (2020) 38(17):1951–62. doi: 10.1200/JCO.19.02488
14
Agostinetto E Rediti M Fimereli D Debien V Piccart M Aftimos P et al . HER2-low breast cancer: Molecular characteristics and prognosis. Cancers (Basel) (2021) 13(11):2824. doi: 10.3390/cancers13112824
15
de Moura Leite L Cesca MG Tavares MC Santana DM Saldanha EF Guimaraes PT et al . HER2-low status and response to neoadjuvant chemotherapy in HER2 negative early breast cancer. Breast Cancer Res Treat (2021) 190(1):155–63. doi: 10.1007/s10549-021-06365-7
16
Slamon DJ Clark GM Wong SG Levin WJ Ullrich A McGuire WL . Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. (1987) 235(4785):177–82. doi: 10.1126/science.3798106
17
Seshadri R Firgaira FA Horsfall DJ McCaul K Setlur V Kitchen P . Clinical significance of HER-2/neu oncogene amplification in primary breast cancer. the south Australian breast cancer study group. J Clin Oncol (1993) 11(10):1936–42. doi: 10.1200/JCO.1993.11.10.1936
18
Slamon D Eiermann W Robert N Pienkowski T Martin M Press M et al . Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med (2011) 365(14):1273–83. doi: 10.1056/NEJMoa0910383
19
Gianni L Pienkowski T Im YH Tseng LM Liu MC Lluch A et al . 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): a multicentre, open-label, phase 2 randomised trial. Lancet Oncol (2016) 17(6):791–800. doi: 10.1016/S1470-2045(16)00163-7
20
Swain SM Baselga J Kim SB Ro J Semiglazov V Campone M et al . Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med (2015) 372(8):724–34. doi: 10.1056/NEJMoa1413513
21
Marchio C Annaratone L Marques A Casorzo L Berrino E Sapino A . Evolving concepts in HER2 evaluation in breast cancer: Heterogeneity, HER2-low carcinomas and beyond. Semin Cancer Biol (2021) 72:123–35. doi: 10.1016/j.semcancer.2020.02.016
22
Pernas S Tolaney SM . Targeting HER2 heterogeneity in early-stage breast cancer. Curr Opin Oncol (2020) 32(6):545–54. doi: 10.1097/CCO.0000000000000685
23
Mutai R Barkan T Moore A Sarfaty M Shochat T Yerushalmi R et al . Prognostic impact of HER2-low expression in hormone receptor positive early breast cancer. Breast. (2021) 60:62–9. doi: 10.1016/j.breast.2021.08.016
24
Denkert C Seither F Schneeweiss A Link T Blohmer JU Just M et al . Clinical and molecular characteristics of HER2-low-positive breast cancer: pooled analysis of individual patient data from four prospective, neoadjuvant clinical trials. Lancet Oncol (2021) 22(8):1151–61. doi: 10.1016/S1470-2045(21)00301-6
25
Won HS Ahn J Kim Y Kim JS Song JY Kim HK et al . Clinical significance of HER2-low expression in early breast cancer: a nationwide study from the Korean breast cancer society. Breast Cancer Res (2022) 24(1):22. doi: 10.1186/s13058-022-01519-x
26
Schettini F Chic N Braso-Maristany F Pare L Pascual T Conte B et al . Clinical, pathological, and PAM50 gene expression features of HER2-low breast cancer. NPJ Breast Cancer (2021) 7(1):1. doi: 10.1038/s41523-020-00208-2
27
Zhang G Ren C Li C Wang Y Chen B Wen L et al . Distinct clinical and somatic mutational features of breast tumors with high-, low-, or non-expressing human epidermal growth factor receptor 2 status. BMC Med (2022) 20(1):142. doi: 10.1186/s12916-022-02346-9
28
Iwata H Im SA Masuda N Im YH Inoue K Rai Y et al . PALOMA-3: Phase III trial of fulvestrant with or without palbociclib in premenopausal and postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer that progressed on prior endocrine therapy-safety and efficacy in Asian patients. J Glob Oncol (2017) 3(4):289–303. doi: 10.1200/JGO.2016.008318
29
Cristofanilli M Rugo HS Im SA Slamon DJ Harbeck N Bondarenko I et al . Overall survival with palbociclib and fulvestrant in women with HR+/HER2- ABC: Updated exploratory analyses of PALOMA-3, a double-blind, phase 3 randomized study. Clin Cancer Res (2022). doi: 10.1158/1078-0432.CCR-22-0305
30
Xu B Li H Zhang Q Sun W Yu Y Li W et al . Pharmacokinetics, safety, activity, and biomarker analysis of palbociclib plus letrozole as first-line treatment for ER+/HER2- advanced breast cancer in Chinese women. Cancer Chemother Pharmacol (2021) 88(1):131–41. doi: 10.1007/s00280-021-04263-9
Summary
Keywords
breast cancer, CDK4/6 inhibitor, HER2-low, endocrine therapy, palbociclib
Citation
Shao Y, Luo Z, Yu Y, Chen Q, He Y, Liu C, Nie B, Zhu F and Liu H (2022) HER2-low expression does not affect the clinical outcomes of metastatic breast cancer treated with CDK4/6 inhibitor: A real-world study. Front. Endocrinol. 13:1000704. doi: 10.3389/fendo.2022.1000704
Received
22 July 2022
Accepted
02 August 2022
Published
18 August 2022
Volume
13 - 2022
Edited by
Erika Di Zazzo, University of Molise, Italy
Reviewed by
Pasquale Pisapia, University of Naples Federico II, Italy; Mariarosaria Conte, University of Campania Luigi Vanvitelli, Italy
Updates
Copyright
© 2022 Shao, Luo, Yu, Chen, He, Liu, Nie, Zhu and Liu.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hui Liu, rxliuhui@zzu.edu.cn
This article was submitted to Cancer Endocrinology, a section of the journal Frontiers in Endocrinology
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.