 Yu-Shun Qiao1Yin-He Chai1Hong-Jian Gong1Zhiyessova Zhuldyz1Coen D. A. Stehouwer2
Yu-Shun Qiao1Yin-He Chai1Hong-Jian Gong1Zhiyessova Zhuldyz1Coen D. A. Stehouwer2 Jian-Bo Zhou3*
Jian-Bo Zhou3* Rafael Simó4,5,6
Rafael Simó4,5,6- 1Beijing Tongren Hospital, Capital Medical University, Beijing, China
- 2Department of Internal Medicine and Cardiovascular Research Institute Maastricht (CARIM) School for Cardiovascular Diseases, Maastricht University Medical Center, Maastricht, Netherlands
- 3Department of Endocrinology, Beijing Tongren Hospital, Capital Medical University, Beijing, China
- 4Endocrinology and Nutrition Derpartment, Vall d’Hebron University Hospital, Autonomous University, Barcelona, Spain
- 5Diabetes and Metabolism Research Unit, Vall d’Hebron Research Institute (VHIR), Barcelona, Spain
- 6Centro de Investigación Biomédica en Red de Diabetes y Enfermedades Metabólicas Asociadas (CIBERDEM), Instituto de Salud Carlos III (ICSIII), Madrid, Spain
Aim: We performed a meta-analysis of observational studies to evaluate the association between the presence of sarcopenia and HbA1c, prediabetes, diabetes and diabetic complications.
Method: The PubMed, Embase, Cochrane and Web of Science databases were searched from inception to May 2021. We included full-text English language articles that reported the prevalence of sarcopenia in patients with and without diabetes. Quality assessment was performed according to the Newcastle- Ottawa scale for observational studies.
Results: Sixteen studies were included in the meta-analysis. Three studies showed that high HbA1c levels lead to loss of muscle mass, and one study involving prediabetes showed that people with prediabetes had lower muscle mass, strength, and performance than non-diabetic population. Seven studies showed that people with diabetes had a higher risk of sarcopenia than those without diabetes (combined OR: 2.09, 95% CI:1.62-2.70). The remaining five studies suggested that diabetic complications increased the risk of sarcopenia (combined OR: 2.09,95% CI:1.62-2.70).
Conclusion: High HbA1c levels, prediabetes, diabetes and diabetes complications were associated with an increased risk of sarcopenia. Therapeutic strategies addressed to avoid the conversion of IGT to diabetes and to optimize glycemic control are warranted to prevent or arrest sarcopenia in the diabetic population
Introduction
The term sarcopenia refers to the loss of muscle mass, muscle strength or physical function that occurs with aging. Sarcopenia is an emerging health concern that mainly affects the quality of life of older people and is an underlying factor for falls, fractures, deaths and a series of adverse events (1–3). Therefore, early identification is crucial for implementing appropriate preventive actions and studying its pathogenesis and influencing factors, such as aging (4), obesity (5), cancer (6) and other diseases (7, 8). Diabetes has been reported as an influencing factor for sarcopenia (9). When insulin resistance occurs in skeletal muscles, glucose utilization and protein synthesis are reduced, which, in turn, aggravates insulin resistance and muscle loss, thus evolving into a vicious circle (10, 11). According to statistics from a systematic literature review, up to 70% of adults with diabetes have difficulty performing routine physical tasks, with lower extremity mobility limitations particularly evident (12).
Further, literature shows that many previous studies (13) have suggested that patients with diabetes have a significantly increased risk of sarcopenia. However, it is unknown whether this relationship is also present in subjects with prediabetes. In addition, the role of glycemic control and diabetic complications remains to be elucidated. Therefore, we conducted a meta-analysis of the literature to study the relationship between sarcopenia and diabetes, prediabetes, glycemic control and diabetic complications.
Method
Search Strategy
This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. We systematically searched for relevant literature in the PubMed, Embase, Cochrane and Web of Science databases for studies published from inception to May 2021. The following items (single or combined) were included in the search strategy: sarcopenia, skeletal muscle, muscle mass, muscle strength, physical performance, gait speed, hyposthenia, grip strength, diabetes, diabetes mellitus, hemoglobin a1c, impaired fasting glucose, impaired glucose tolerance and prediabetes. The studies were based on patients with type 2 diabetes mellitus (T2DM), rather than type 1 diabetes mellitus (T1DM) or other special types of diabetes. Each study was required to consider essential variables, such as age (years), sex (% male), duration of diabetes (years) and body mass index (kg/m²). The reference lists of all retrieved articles were manually reviewed. Two independent authors (YHC and independently) analyzed each article and performed data extraction. A third investigator consulted (xx) in cases of disagreement. Discrepancies were resolved by consensus.
Diagnostic Criteria
This study only discussed the association between sarcopenia and T2DM rather than other types diabetes mellitus. T2DM was diagnosed as having fasting blood glucose measurement (FPG≥7.0 mmol/L) with or without 2-hour postprandial blood glucose ≥11.1 mmol/L during an oral glucose tolerance test (OGTT), according to World Health Organization (WHO) 1999 criteria. Prediabetes was defined as having 6.1 and 7.0mmol/L with or without a 2-hour OGTT between and 11.1mmol/L. The diagnostic criteria for sarcopenia and involved muscle mass measured by dual X-ray absorptiometry (DXA) or bioelectrical impedance analysis (BIA), in accordance with Asian Working Group for Sarcopenia (AWGS), European Working Group on Sarcopenia in Older People (EWGSOP), or Foundation for the NIH (FNIH) diagnostic criteria.
Study Selection
The inclusion criteria for the selected articles were as follows: (1) the included study subjects were older than 60 years; (2) the prevalence of sarcopenia in the diabetic, prediabetic, and non-diabetic groups was calculated; (3) type of diabetes mellitus was T2DM; (4) low muscle mass was considered for the indispensable diagnosis of sarcopenia; (5) research design belonged to observational (cross-sectional or case–control or cohort) studies (6) extractable data was available on sarcopenia in adults with diabetes or prediabetes and euglycemic subjects.
The exclusion criteria for selected articles were as follows: (1) control group (euglycemic subjects) was not set up; (2) reviews, letters or conference abstracts; (3) repeat publications; (4) studies that were not written in English; (5) individuals with severe diabetes and complications who are unable to walk or lack activity capability; (6) participants with acute disease, history of stroke, myocardial infarction or cancer; (7) individuals aged >85 years, severe heart failure (New York Heart Association Class II-IV), or had severe liver impairment (liver enzyme ALT≥3-fold the upper limit of normal range), severe renal dysfunction (estimated glomerular filtration rate [eGFR]<30 mL/min/1.73m2), or a history of thyroid or adrenal diseases, were also excluded.
There were a few exceptions that should be explained here: (1) the study of Sambashivaish was on the association between prediabetes and sarcopenia. Hence, we did not limit our age to over 60 years. (2) while the mean age of participants was lesser (44.3 ± 9.4 years) in Anbalagan’s study, there was a age and sex match between the test group and control group. Therefore, the literature is involved in this study.
Data Extraction and Quality Assessment
The following data were extracted: (1) first author (2) publication year (3) country (4) study design (5) the basic information of participants (total number, mean age and proportion of female) (6) the number of participants with diabetes, diabetes complications or prediabetes and control group subjects (7) the prevalence rate of sarcopenia. Quality assessment was conducted by using The Newcastle-Ottawa scale (NOS), including three aspects of assessment: selection of subjects, comparability and assessment of outcomes. NOS allows four stars for subject selection, two stars for comparability, and three stars for outcomes assessment, therefore, a study can get up to nine stars. The quality of each study was graded as low (0–3), moderate (4–6), or high (7–9). Two independent researchers respectively did quality assessments, and a third researcher rescored the different results. Differences were resolved by consensus.
Statistical Analyses
We analyzed and pooled Odd Ratios and 95% Confidence Intervals of the association between sarcopenia and diabetes or diabetes complications from the raw prevalence data, respectively. The ORs of the relationship between sarcopenia and diabetes complications were calculated by adjusting for confounding factors and other diabetes complications, such as age, sex, and hypertension, to reduce the interaction between various diabetes complications. The ORs and 95%CIs were converted into the natural logarithm (ln OR) and standard error values. Heterogeneity testing was evaluated using the I² statistic, and a fixed effects model was applied when heterogeneity was small (I² ≤50%); otherwise, a random effects model was used. Funnel plots were used to assess the potential for publication bias. However, to avoid the possible impact of visual perception, Egger’s test was conducted to assess publication bias more accurately (P-values <0.1 indicated that there was no publication bias). To explore the source of heterogeneity, subgroup analyses were used to evaluate age (<60 and ≥60 years), types of diabetes vascular disease (microvascular and macrovascular), and types of diabetes complications (diabetic nephropathy, diabetic foot, diabetic retinopathy and diabetic neuropathy). A sensitivity analysis was used to evaluate the robustness of the meta-analysis results. All analyses were performed using Stata 12.0 software (StataCorp LP, TX). Statistical significance was set at P <0.05.
Results
Literature Search Outcomes and Validity Assessment
The search strategy identified 2,331 potentially relevant records, from multiple scientific studies and 713 were excluded as duplicates. The remaining manuscripts were searched for screening the title and abstract, and 1,559 publications were excluded because they were reviews, letters, or conference abstracts. Thus, 59 articles were eligible for full-text review and data assessment. Finally, 16 studies (14–29) were included in the current meta-analysis and systemic review. Among those publications, three (14–16) mentioned the relationship between HbA1c and sarcopenia, one (17) mentioned prediabetes, seven (18–24) mentioned diabetes, and five (25–29) mentioned diabetes-related complications, (Figure 1). The characteristics of studies included were shown in Table 1. The total sample size in 16 studies was 15,326, and all participants were >18 years old. All studies included control groups.
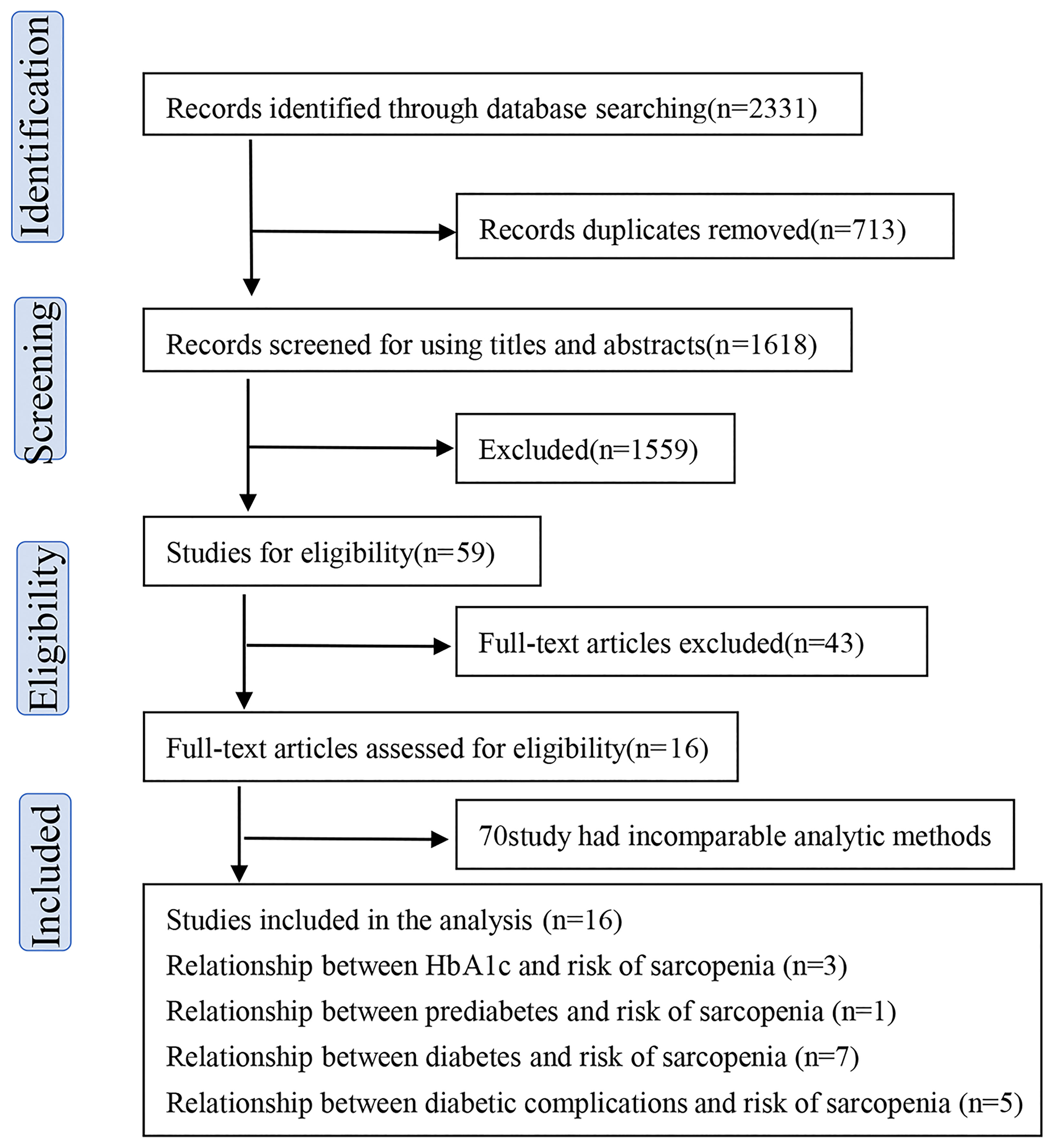
Figure 1 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) study.
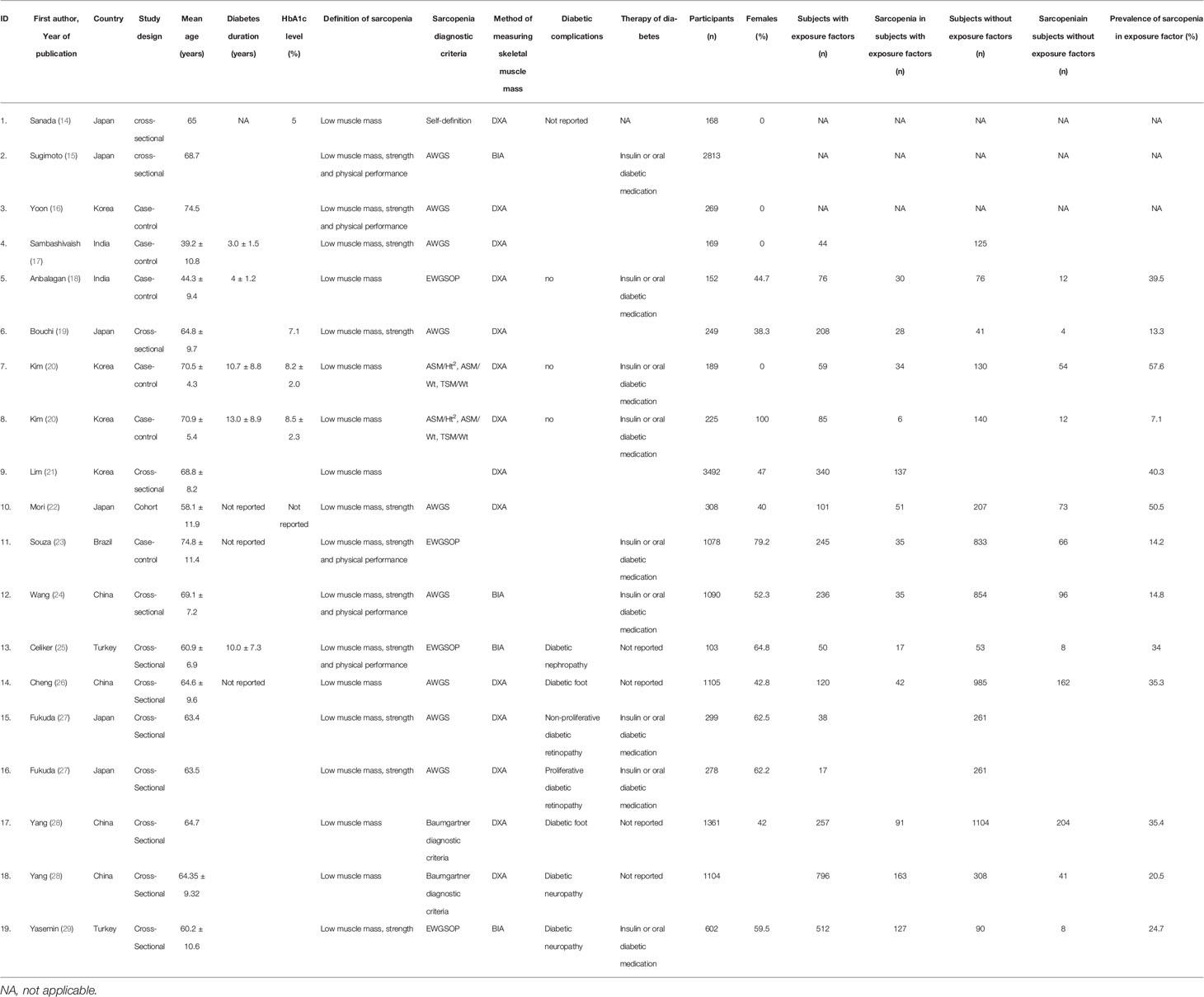
Table 1 Characteristics of the included studies.
Meta-Analysis of the Association Between Diabetes and the Risk of Sarcopenia
Seven studies (18–24) (n=6,783 participants, female: 52.7%) were included. The random effect model was used according to the I2. The combined OR was 1.95 (95% CI: 1.24–3.06, I²=69.3%, P=0.002), showing that patients with diabetes have a significantly higher risk of sarcopenia than patients without diabetes (Figure 2A).
The results of the subgroup analysis (Figure 2B) showed that the relationship between diabetes and the risk of sarcopenia was subject to age. Surprisingly, the risk of sarcopenia was higher in the patients aged <60 years (OR=3.21, 95% CI: 1.77—5.85, I²=0%) than in those aged ≥60 years (OR 1.69, 95% CI: 1.03—2.78, I²=70.6%). After removing studies one by one, the sensitivity analysis conclusively showed that patients with diabetes had a significantly higher risk of sarcopenia than patients without diabetes.
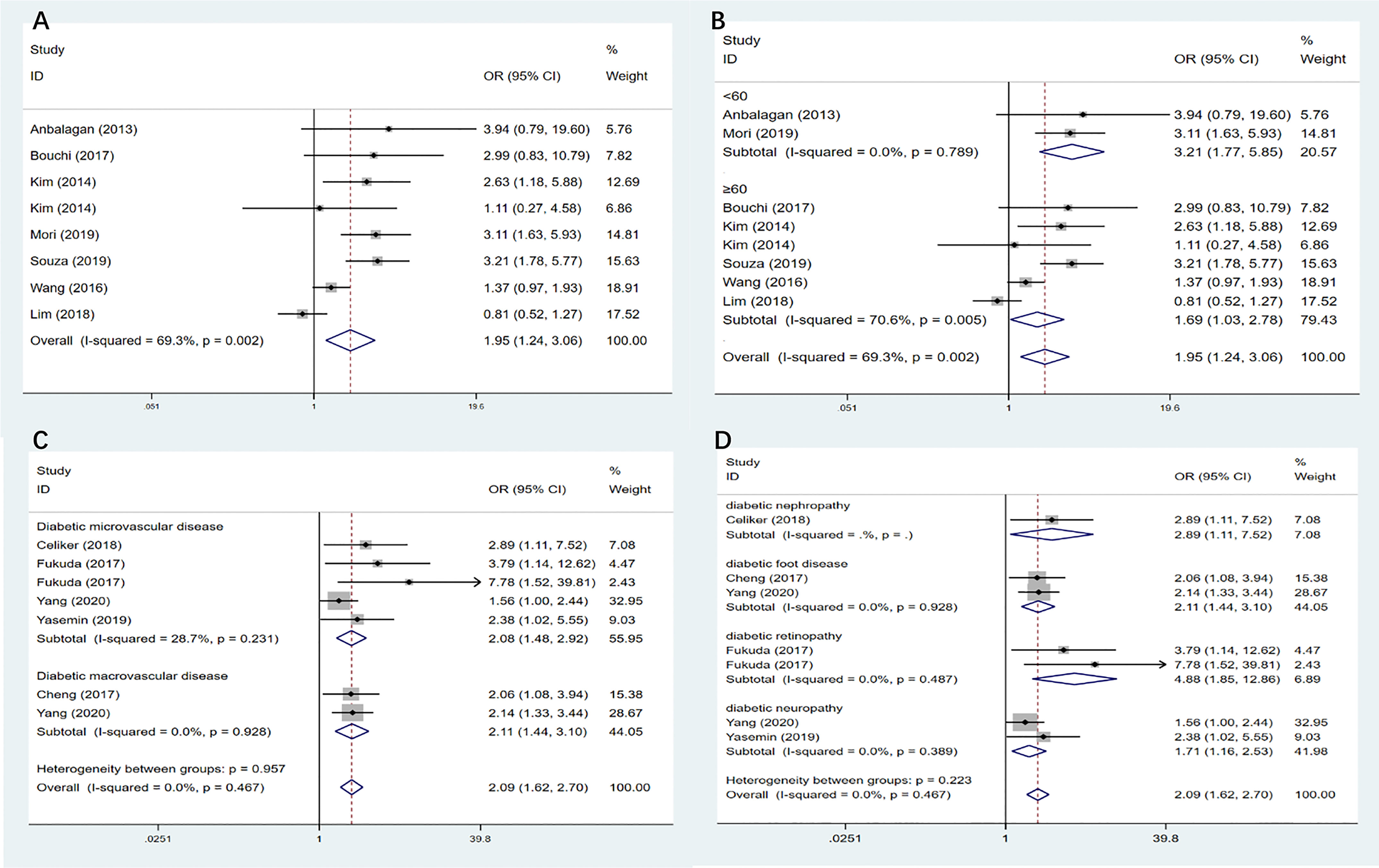
Figure 2 (A) Meta-analysis of the association between diabetes and the risk of sarcopenia. (B) Subgroup analysis of the association between diabetes and the risk of sarcopenia according to age. (C) Subgroup analysis of the association between diabetes complications and the risk of sarcopenia according to diabetic vascular disease. (D) Subgroup analysis of the association between diabetes complications and the risk of sarcopenia according to different diabetic complications. OR, odds ratio; CI, confidence interval. Where I2 is the variation in effect estimates attributable to heterogeneity, overall is the pooled random/fixed effect estimate of all studies. subtotal is the pooled random effects estimate of sub-group analysis studies. Weights are from random-effects analysis. %Weight is the weight assigned to each study, based on the inverse of the within- and between-study variance. The size of the grey boxes around the point estimates reflects the weight assigned to each study.
Systemic Review of the Association Between HbA1c and the Risk of Sarcopenia
Three studies (14–16) mentioned the relationship between different HbA1c levels and the risk of sarcopenia. Unfortunately, we could not combine their data because of the different grouping standards. The first study (14) showed that men with class 1 sarcopenia (6.87< appendicular muscle mass (AMM)/height²<7.77 kg/m2) had higher levels of HbA1c than patients with normoglycemia. However, this association was not significant among women. In the second study (15), regardless sex, sarcopenia was positively correlated with HbA1c levels in subjects with T2DM. In addition, the authors reported that HbA1c levels were associated with low muscle mass rather than low muscle strength and performance. The third study (16) reported a negative relationship between HbA1c levels, muscle mass, and performance in patients with T2D, which was more evident when the HbA1c level was ≥8.5%. Overall, these studies confirmed the association between high HbA1c levels and sarcopenia.
Systemic Review of the Association Between Prediabetes and the Risk of Sarcopenia
Only one study (17) focused on the association between prediabetes and the risk of sarcopenia. The participants in the study were all male, with ages ranging from 20 to 50 years. The study showed that subjects with prediabetes presented lower muscle mass, strength, and performance than non-diabetic subjects, suggesting that prediabetes is closely associated with the risk of sarcopenia.
Meta-Analysis of the Association Between Diabetes Complications and the Risk of Sarcopenia
A total of five studies (25–29) (n=3286 participants, females: 46.4%) were included. The combined OR of the relationship between diabetes complications and the risk of sarcopenia was 2.09 (95% CI:1.62–2.70, I²=0%, P=0.467). This increased risk was maintained when microangiopathic and macroangiopathic complications were analyzed separately (Figure 2C, Table 2). The subgroup of diabetic complications (Figure 2D) showed that individuals with diabetic retinopathy had a higher significant risk than patients with diabetes without diabetic retinopathy, and the OR of diabetic retinopathy was 4.88 (95% CI:1.85—12.86). More importantly, proliferative diabetic retinopathy increased the risk of sarcopenia than non-proliferative diabetic retinopathy; the ORs were 7.78 (95% CI: 1.52—39.81) and 3.79 (95% CI: 1.14—12.62), respectively. Patients with diabetic nephropathy (OR=2.89, 95% CI: 1.11—7.52) or neuropathy (OR=1.71, 95% CI: 1.16—2.53) also had a higher prevalence of sarcopenia. After removing studies one by one, the sensitivity analysis suggests that patients with diabetic complications have a significantly higher risk of sarcopenia than patients with diabetes without complications.
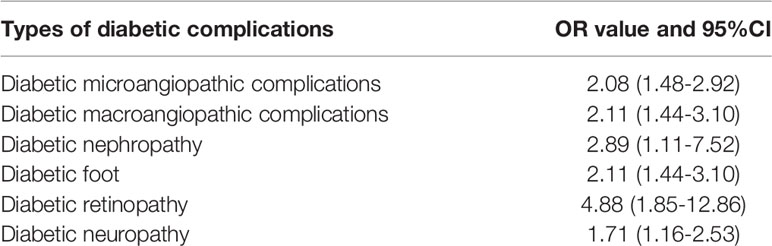
Table 2 The OR values and 95%CI of diabetic complications.
Quality Assessment
Quality assessment of the studies revealed scores of 6–9 on the NOS (30). Two studies scored 6, five were scored 7, seven were scored 8, and two were scored 9. Thus, high-quality studies were included in this meta-analysis (Supplementary Table 1).
Publication Bias
According to the Cochrane Handbook (31), as a rule of thumb, tests for funnel plot asymmetry should be used only when there are enough studies, included in the meta-analysis because when there are fewer studies, the power of the tests is too low to distinguish real asymmetry from coincidence. In this study, the P-value of the Egger test was >0.05 (P = 0.227) for the relationship between diabetes and the risk of sarcopenia, indicating no significant bias. The funnel figure of these studies showed a symmetrical inverted distribution, which is consistent with the results of the Egger test (Supplementary Figure 1).
Discussion
In this systematic review and meta-analysis, we included 16 studies to analyze the relationship between diabetes and sarcopenia. The results showed that the presence of diabetes, poor glycemic control, and related chronic complications significantly increased the risk of sarcopenia. In addition, a relationship between prediabetes and sarcopenia was observed.
Previous studies reported a harmful influence of diabetes on sarcopenia, which was based on studies showing that muscle mass, strength, and performance were significantly lower in patients with diabetes than in non-diabetic controls (32–35). However, few studies have examined whether there is a difference in the risk of sarcopenia among patients with diabetes, taking into account crucial variables such as the degree of glycemic control and the presence of long-term diabetic complications. Therefore, a novel contribution of this systematic review is its demonstration that poor glycemic control, assessed by HbA1c level, is an additional risk factor for the development or progression of sarcopenia among patients with diabetes. Although HbA1c reflects glycemic control in the previous 2–3 months (11), daily glycemic control is also very important. According to reports, large daily glycemic fluctuations also increased the risk of muscle loss (OR=1.045) (36), which suggests that both short-and long-term blood glycemic control should be emphasized.
Whether poor glycemic control is related to both muscle loss, muscle strength, and performance remains an open question. Three studies (14–16) using either body mass index, skeletal mass index (SMI), or appendicular skeletal muscle mass as measurements of muscle mass, showed that poor glycemic control was closely associated with the loss of muscle mass rather than the loss of muscle strength and performance. In contrast, in the Baltimore Longitudinal Study of Aging, knee extensor strength was lower across increasing quartiles of HbA1c (37). The differences in race, sample size, and assessment methods can explain the divergent results. Therefore, larger studies using uniform methods to evaluate muscle morphology and function are needed.
Muscle mass and prediabetes are likely to have bidirectional relationships. In a cross-sectional analysis of the National Health and Nutrition Examination Survey from the United States, after adjusting for multiple confounding factors, each 10% increase in SMI was associated with a 12% relative reduction in prediabetes prevalence (95% CI, 1%—21%) (38). These results suggest that muscle mass is inversely proportional to the risk of prediabetes. Since glucose levels are only slightly impaired in the prediabetic stage, it could be postulated that the pathways activated by insulin resistance, rather than those activated by chronic hyperglycemia, are meaningful in the development of sarcopenia.
A clear influence of diabetic complications was found on the risk of sarcopenia. In this regard, we would like to emphasize that diabetic retinopathy and diabetic nephropathy tend to coexist and can synergistically increase the risk of sarcopenia. In addition, although previous studies (39–41) have mostly analyzed the association between one or two complications of diabetes and sarcopenia, compared with patients without diabetic complications, each type of complication will significantly increase the risk of sarcopenia which is consistent with our findings.
In the age-based subgroup analysis (< 60 years group and ≥60 years group), the results indicated that the risk of sarcopenia in patients with diabetes aged < 60 years (OR: 3.21, 95% CI: 1.77—5.85) was higher than that in patients with diabetes that are aged ≥60 years (OR: 1.69, 95% CI: 1.03—2.78). However, this does not mean that as age increases, patients with diabetes have a lower risk of sarcopenia. First, age is a common risk factor for diabetes and sarcopenia. With age, insulin resistance becomes more common (9) and the ability of insulin to stimulate protein synthesis gradually weakens (42). Ageing is accompanied by major changes in body composition, including a gradual decrease in muscle mass, strength, and performance, which can markedly affect the daily activities of older adults (43, 44). Second, older age tends to be accompanied by a longer duration of diabetes, although this is not absolute. In a study from Japan on participants with diabetes aged ≥ 60 years (108 males and 105 females), the prevalence of sarcopenia was 19.2% and the risk of sarcopenia increased with longer duration of diabetes in women (OR = 1.43) (45). Finally, few studies on patients with diabetes aged <60 years were included, which may have induced bias.
The mechanisms involved in the association between diabetes and the risk of sarcopenia need to be fully elucidated, but some pathophysiological explanations have been provided. First, insulin resistance, through inhibition of the mTOR pathway (46), activation of autophagy (46), activation of the ubiquitin-proteasome proteolytic pathway (47), and accelerated muscle protein degradation may cause sarcopenia. Second, poor blood glucose control causes many metabolic abnormalities (10), such as the activation of apoptosis triggered by TNF-α (48) and impaired muscle mitochondrial oxidative capacity (49), thereby contributing to muscle cell damage (10). Third, repeated episodes of ischemia-reperfusion caused by vascular complications are a common pathway for muscle loss (50). Finally, in diabetic neuropathy, loss of motor neurons (51) or imbalance between denervation and reinnervation (51) can induce loss of muscle mass and strength.
In this study, some clinical issues were worthy of attention. In the prediabetes stage, it is crucial to reduce the risk of impaired glucose tolerance (IGT) progressing towards overt diabetes; therefore, lifestyle interventions are strongly recommended. In this regard, a clinical trial conducted in the U.S. (2.8 years of follow-up) showed that lifestyle intervention reduced the incidence of diabetes by 58% (95% CI: 48%—66%) in comparison with placebo (52). In addition, treatment with metformin and acarbose has a positive effect on reducing the risk of conversion from IGT to diabetes (52, 53). In patients with diabetes and sarcopenia, tight control of blood glucose levels is recommended, and for this reason, monitoring HbA1c levels and blood glucose monitoring should be strengthened.
The strength of this meta-analysis is that many factors associated with the risk of sarcopenia were considered, thus providing a more comprehensive analysis of the factors affecting sarcopenia. However, this study has certain limitations. First, due to the statistical difference in age and duration of diabetes between groups in some included studies, we cannot adequately consider these two variables, as they may cause bias in the results of this study. Second, data in some studies did not consider the influence of confounding factors, such as the severity of diabetes complications and the ranges of HbA1c and interactions among diabetes complications, which may have led to an overestimation of the study results. Third, although it had been meta-analyzed using multiple sarcopenia diagnostic criteria (AWGS, EWGSOP, FNIH criteria), the diagnostic criteria for sarcopenia also included observational studies measured by BIA. Fourth, the number of studies included in the subgroup analysis was relatively small, which may have caused false-negative results. Finally, the participants in many studies were not from the community but from the hospital, which may have resulted in lack of representativeness. In the future, more studies should be conducted to address these shortcomings.
In conclusion, high HbA1c levels, prediabetes, diabetes, and diabetes complications were significantly associated with an increased risk of sarcopenia. Whether these associations are further affected by age, sex and duration of diabetes complications needs to be tested in more prospective cohort studies. Meanwhile, therapeutic strategies aimed at avoiding the conversion of IGT to diabetes and optimizing glycemic control seem to be the best way to prevent or arrest sarcopenia in the diabetic population.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Statement
This article does not contain any studies with human participants or animals performed by any of the authors.
Author Contributions
YQ contributed the interpretation of data, and drafting the report. ZZ contributed to statistical analysis, interpretation of data. YC and HG contributed the re-analysis, interpretation of data. J-BZ and RS contributed to study design and review. CS revised the manuscript. J-BZ is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82070851, 81870556), Beijing Municipal Administration of Hospitals’ Youth Program (QML20170204), Excellent Talents in Dongcheng District of Beijing.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2021.782391/full#supplementary-material
References
1. Woo J, Leung J, Morley JE. Defining Sarcopenia in Terms of Incident Adverse Outcomes. J Am Med Directors Assoc (2015) 16(3):247–52. doi: 10.1016/j.jamda.2014.11.013
2. Beaudart C, Zaaria M, Pasleau F, Reginster JY, Bruyère O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLloS One (2017) 12(1):e0169548. doi: 10.1371/journal.pone.0169548
3. Bijlsma AY, Pasma JH, Lambers D, Stijntjes M, Blauw GJ, Meskers CG, et al. Muscle Strength Rather Than Muscle Mass Is Associated With Standing Balance in Elderly Outpatients. J Am Med Directors Assoc (2013) 14(7):493–8. doi: 10.1016/j.jamda.2013.02.001
4. Short KR, Vittone JL, Bigelow ML, Proctor DN, Nair KS. Age and Aerobic Exercise Training Effects on Whole Body and Muscle Protein Metabolism. Am J Physiol Endocrinol Metab (2004) 286(1):E92–101. doi: 10.1152/ajpendo.00366.2003
5. Waters DL, Baumgartner RN. Sarcopenia and Obesity. Clinics Geriatric Med (2011) 27(3):401–21. doi: 10.1016/j.cger.2011.03.007
6. Dodson S, Baracos VE, Jatoi A, Evans WJ, Cella D, Dalton JT, et al. Muscle Wasting in Cancer Cachexia: Clinical Implications, Diagnosis, and Emerging Treatment Strategies. Annu Rev Med (2011) 62:265–79. doi: 10.1146/annurev-med-061509-131248
7. Tessari P. Protein Metabolism in Liver Cirrhosis: From Albumin to Muscle Myofibrils. Curr Opin Clin Nutr Metab Care (2003) 6(1):79–85. doi: 10.1097/00075197-200301000-00012
8. McDermott MM, Guralnik JM, Albay M, Bandinelli S, Miniati B, Ferrucci L. Impairments of Muscles and Nerves Associated With Peripheral Arterial Disease and Their Relationship With Lower Extremity Functioning: The InCHIANTI Study. J Am Geriatrics Soc (2004) 52(3):405–10. doi: 10.1111/j.1532-5415.2004.52113.x
9. Kalyani RR, Corriere M, Ferrucci L. Age-Related and Disease-Related Muscle Loss: The Effect of Diabetes, Obesity, and Other Diseases. Lancet Diabetes Endocrinol (2014) 2(10):819–29. doi: 10.1016/S2213-8587(14)70034-8
10. Landi F, Onder G, Bernabei R. Sarcopenia and Diabetes: Two Sides of the Same Coin. J Am Med Directors Assoc (2013) 14(8):540–1. doi: 10.1016/j.jamda.2013.05.004
11. Sherwani SI, Khan HA, Ekhzaimy A, Masood A, Sakharkar MK. Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients. Biomark Insights (2016) 11:95–104. doi: 10.4137/BMI.S38440
12. Kalyani RR, Saudek CD, Brancati FL, Selvin E. Association of Diabetes, Comorbidities, and A1C With Functional Disability in Older Adults: Results From the National Health and Nutrition Examination Survey (NHANES), 1999-2006. Diabetes Care (2010) 33(5):1055–60. doi: 10.2337/dc09-1597
13. Anagnostis P, Gkekas NK, Achilla C, Pananastasiou G, Taouxidou P, Mitsiou M, et al. Type 2 Diabetes Mellitus Is Associated With Increased Risk of Sarcopenia: A Systematic Review and Meta-Analysis. Calcif Tissue Int (2020) 107(5):453–63. doi: 10.1007/s00223-020-00742-y
14. Sanada K, Miyachi M, Tanimoto M, Yamamoto K, Murakami H, Okumura S, et al. A Cross-Sectional Study of Sarcopenia in Japanese Men and Women: Reference Values and Association With Cardiovascular Risk Factors. Eur J Appl Physiol (2010) 110(1):57–65. doi: 10.1007/s00421-010-1473-z
15. Sugimoto K, Tabara Y, Ikegami H, Takata Y, Kamide K, Ikezoe T, et al. Hyperglycemia in Non-Obese Patients With Type 2 Diabetes Is Associated With Low Muscle Mass: The Multicenter Study for Clarifying Evidence for Sarcopenia in Patients With Diabetes Mellitus. J Diabetes Investig (2019) 10(6):1471–9. doi: 10.1111/jdi.13070
16. Yoon JW, Ha YC, Kim KM, Moon JH, Choi SH, Lim S, et al. Hyperglycemia Is Associated With Impaired Muscle Quality in Older Men With Diabetes: The Korean Longitudinal Study on Health and Aging. Diabetes Metab J (2016) 40(2):140–6. doi: 10.4093/dmj.2016.40.2.140
17. Sambashivaiah S, Harridge SDR, Sharma N, Selvam S, Rohatgi P, Kurpad AV. Asian Indians With Prediabetes Have Similar Skeletal Muscle Mass and Function to Those With Type 2 Diabetes. Front Nutr (2019) 6:179. doi: 10.3389/fnut.2019.00179
18. Anbalagan VP, Venkataraman V, Pradeepa R, Deepa M, Anjana RM, Mohan V. The Prevalence of Presarcopenia in Asian Indian Individuals With and Without Type 2 Diabetes. Diabetes Technol Ther (2013) 15(9):768–75. doi: 10.1089/dia.2013.0068
19. Bouchi R, Fukuda T, Takeuchi T, Nakano Y, Murakami M, Minami I, et al. Association of Sarcopenia With Both Latent Autoimmune Diabetes in Adults and Type 2 Diabetes: A Cross-Sectional Study. J Diabetes Complications (2017) 31(6):992–6. doi: 10.1016/j.jdiacomp.2017.02.021
20. Kim KS, Park KS, Kim MJ, Kim SK, Cho YW, Park SW. Type 2 Diabetes is Associated With Low Muscle Mass in Older Adults. Geriatr Gerontol Int (2014) 14 Suppl 1:115–21. doi: 10.1111/ggi.12189
21. Lim HS, Park YH, Suh K, Yoo MH, Park HK, Kim HJ, et al. Association Between Sarcopenia, Sarcopenic Obesity, and Chronic Disease in Korean Elderly. J Bone Metab (2018) 25(3):187–93. doi: 10.11005/jbm.2018.25.3.187
22. Mori K, Nishide K, Okuno S, Shoji T, Emoto M, Tsuda A, et al. Impact of Diabetes on Sarcopenia and Mortality in Patients Undergoing Hemodialysis. BMC Nephrol (2019) 20(1):105. doi: 10.1186/s12882-019-1271-8
23. Souza ABF, Nascimento DAC, Rodrigues IJM, Charone CCO, Lopes GL, Lima RS, et al. Association Between Sarcopenia and Diabetes in Community Dwelling Elderly in the Amazon Region - Viver Mais Project. Arch Gerontol Geriatr (2019) 83:121–5. doi: 10.1016/j.archger.2019.03.020
24. Wang T, Feng X, Zhou J, Gong H, Xia S, Wei Q, et al. Type 2 Diabetes Mellitus is Associated With Increased Risks of Sarcopenia and Pre-Sarcopenia in Chinese Elderly. Sci Rep (2016) 6:38937. doi: 10.1038/srep38937
25. Celiker M, Selcuk MY, Olt S. Sarcopenia in Diabetic Nephropathy: A Cross-Sectional Study. Rom J Intern Med (2018) 56(2):102–8. doi: 10.2478/rjim-2018-0003
26. Cheng Q, Hu J, Yang P, Cao X, Deng X, Yang Q, et al. Sarcopenia Is Independently Associated With Diabetic Foot Disease. Sci Rep (2017) 7(1):8372. doi: 10.1038/s41598-017-08972-1
27. Fukuda T, Bouchi R, Takeuchi T, Nakano Y, Murakami M, Minami I, et al. Association of Diabetic Retinopathy With Both Sarcopenia and Muscle Quality in Patients With Type 2 Diabetes: A Cross-Sectional Study. BMJ Open Diabetes Res Care (2017) 5(1):e000404. doi: 10.1136/bmjdrc-2017-000404
28. Yang Q, Zhang Y, Zeng Q, Yang C, Shi J, Zhang C, et al. Correlation Between Diabetic Peripheral Neuropathy and Sarcopenia in Patients With Type 2 Diabetes Mellitus and Diabetic Foot Disease: A Cross-Sectional Study. Diabetes Metab Syndr Obes (2020) 13:377–86. doi: 10.2147/DMSO.S237362
29. Yasemin O, Seydahmet A, Ozcan K. Relationship Between Diabetic Neuropathy and Sarcopenia. Prim Care Diabetes (2019) 13(6):521–8. doi: 10.1016/j.pcd.2019.04.007
30. Formiga F, Ferrer A, Padros G, Contra A, Corbella X, Pujol R, et al. Thyroid Status and Functional and Cognitive Status at Baseline and Survival After 3 Years of Follow-Up: The OCTABAIX Study. Eur J Endocrinol (2014) 170(1):69–75. doi: 10.1530/EJE-13-0722
31. Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's Tool for Assessing Risk of Bias in Randomised Trials. BMJ (Clin Res Ed) (2011) 343:d5928. doi: 10.1136/bmj.d5928
32. Park SW, Goodpaster BH, Strotmeyer ES, de Rekeneire N, Harris TB, Schwartz AV, et al. Decreased Muscle Strength and Quality in Older Adults With Type 2 Diabetes: The Health, Aging, and Body Composition Study. Diabetes (2006) 55(6):1813–8. doi: 10.2337/db05-1183
33. Volpato S, Bianchi L, Lauretani F, Lauretani F, Bandinelli S, Guralnik JM, et al. Role of Muscle Mass and Muscle Quality in the Association Between Diabetes and Gait Speed. Diabetes Care (2012) 35(8):1672–9. doi: 10.2337/dc11-2202
34. Kalyani RR, Tra Y, Yeh HC, Egan JM, Ferrucci L, Brancati FL. Quadriceps Strength, Quadriceps Power, and Gait Speed in Older U.S. Adults With Diabetes Mellitus: Results From the National Health and Nutrition Examination Survey, 1999-2002. J Am Geriatrics Soc (2013) 61(5):769–75. doi: 10.1111/jgs.12204
35. Kim TN, Park MS, Yang SJ, Yoo HJ, Kang HJ, Song W, et al. Prevalence and Determinant Factors of Sarcopenia in Patients With Type 2 Diabetes: The Korean Sarcopenic Obesity Study (KSOS). Diabetes Care (2010) 33(7):1497–9. doi: 10.2337/dc09-2310
36. Ogama N, Sakurai T, Kawashima S, Tanikawa T, Tokuda H, Satake S, et al. Association of Glucose Fluctuations With Sarcopenia in Older Adults With Type 2 Diabetes Mellitus. J Clin Med (2019) 8(3):319. doi: 10.3390/jcm8030319
37. Kalyani RR, Metter EJ, Egan J, Golden SH, Ferrucci L. Hyperglycemia Predicts Persistently Lower Muscle Strength With Aging. Diabetes Care (2015) 38(1):82–90. doi: 10.2337/dc14-1166
38. Srikanthan P, Karlamangla AS. Relative Muscle Mass is Inversely Associated With Insulin Resistance and Prediabetes. Findings From the Third National Health and Nutrition Examination Survey. J Clin Endocrinol Metab (2011) 96(9):2898–903. doi: 10.1210/jc.2011-0435
39. Zhang Y, Shen X, He L, Zhao F, Yan S. Association of Sarcopenia and Muscle Mass With Both Peripheral Neuropathy and Nerve Function in Patients With Type 2 Diabetes. Diabetes Res Clin Pract (2020) 162:108096. doi: 10.1016/j.diabres.2020.108096
40. Oh TJ, Kang S, Lee JE, Moon JH, Choi SH, Lim S, et al. Association Between Deterioration in Muscle Strength and Peripheral Neuropathy in People With Diabetes. J Diabetes Its Complications (2019) 33(8):598–601. doi: 10.1016/j.jdiacomp.2019.04.007
41. Takahashi F, Hashimoto Y, Kaji A, Sakai R, Okamura T, Hamaguchi M, et al. Sarcopenic Obesity Is Associated With Macroalbuminuria in Patients With Type 2 Diabetes: A Cross-Sectional Study. Endocr J (2021) 68(7):781–9. doi: 10.1507/endocrj.EJ20-0655
42. Fujita S, Glynn EL, Timmerman KL, Rasmussen BB, Volpi E. Supraphysiological Hyperinsulinaemia is Necessary to Stimulate Skeletal Muscle Protein Anabolism in Older Adults: Evidence of a True Age-Related Insulin Resistance of Muscle Protein Metabolism. Diabetologia (2009) 52(9):1889–98. doi: 10.1007/s00125-009-1430-8
43. Candow DG, Chilibeck PD. Differences in Size, Strength, and Power of Upper and Lower Body Muscle Groups in Young and Older Men. J Gerontol A Biol Sci Med Sci (2005) 60(2):148–56. doi: 10.1093/gerona/60.2.148
44. Lauretani F, Russo CR, Bandinelli S, Bartali B, Cavazzini C, Di Iorio A, et al. Age-Associated Changes in Skeletal Muscles and Their Effect on Mobility: An Operational Diagnosis of Sarcopenia. J Appl Physiol (Bethesda Md 1985) (2003) 95(5):1851–60. doi: 10.1152/japplphysiol.00246.2003
45. Nishimura A, Harashima SI, Hosoda K, Arai H, Inagaki N. Sex-Related Differences in Frailty Factors in Older Persons With Type 2 Diabetes: A Cross-Sectional Study. Ther Adv Endocrinol Metab (2019) 10:2042018819833304. doi: 10.1177/2042018819833304
46. Kaushik S, Singh R, Cuervo AM. Autophagic Pathways and Metabolic Stress. Diabetes Obes Metab (2010) 12(Suppl 2):4–14. doi: 10.1111/j.1463-1326.2010.01263.x
47. Wang X, Hu Z, Hu J, Du J, Mitch WE. Insulin Resistance Accelerates Muscle Protein Degradation: Activation of the Ubiquitin-Proteasome Pathway by Defects in Muscle Cell Signaling. Endocrinology (2006) 147(9):4160–8. doi: 10.1210/en.2006-0251
48. Marzetti E, Lees HA, Manini TM, Buford TW, Aranda JM Jr, Calvani R, et al. Skeletal Muscle Apoptotic Signaling Predicts Thigh Muscle Volume and Gait Speed in Community-Dwelling Older Persons: An Exploratory Study. PLloS One (2012) 7(2):e32829. doi: 10.1371/journal.pone.0032829
49. DeFronzo RA, Tripathy D. Skeletal Muscle Insulin Resistance Is the Primary Defect in Type 2 Diabetes. Diabetes Care (2009) 32(Suppl 2):S157–63. doi: 10.2337/dc09-S302
50. Buford TW, Anton SD, Judge AR, Marzetti E, Wohlgemuth SE, Carter CS, et al. Models of Accelerated Sarcopenia: Critical Pieces for Solving the Puzzle of Age-Related Muscle Atrophy. Ageing Res Rev (2010) 9(4):369–83. doi: 10.1016/j.arr.2010.04.004
51. Campbell MJ, McComas AJ, Petito F. Physiological Changes in Ageing Muscles. J Neurol Neurosurg Psychiatry (1973) 36(2):174–82. doi: 10.1136/jnnp.36.2.174
52. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the Incidence of Type 2 Diabetes With Lifestyle Intervention or Metformin. N Engl J Med (2002) 346(6):393–403. doi: 10.1056/NEJMoa012512
53. Holman RR, Coleman RL, Chan JCN, Chiasson JL, Feng H, Ge J, et al. Effects of Acarbose on Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE): A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Diabetes Endocrinol (2017) 5(11):877–86. doi: 10.1016/S2213-8587(17)30309-1
Keywords: sarcopenia, HbA1c, prediabetes, diabetic complications, diabetes mellitus, observational study
Citation: Qiao Y-S, Chai Y-H, Gong H-J, Zhuldyz Z, Stehouwer CDA, Zhou J-B and Simó R (2021) The Association Between Diabetes Mellitus and Risk of Sarcopenia: Accumulated Evidences From Observational Studies. Front. Endocrinol. 12:782391. doi: 10.3389/fendo.2021.782391
Received: 01 October 2021; Accepted: 17 November 2021;
Published: 23 December 2021.
Edited by:
Paulo Matafome, University of Coimbra, PortugalReviewed by:
Hiroyasu Mori, Tokushima University, JapanKei Nakajima, Kanagawa University of Human Services, Japan
Copyright © 2021 Qiao, Chai, Gong, Zhuldyz, Stehouwer, Zhou and Simó. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jian-Bo Zhou, amlhbmJvLnpob3VAZm94bWFpbC5jb20=