 Tian-han Zhou1
Tian-han Zhou1 Bei Lin1
Bei Lin1 Fan Wu1Kai-ning Lu2Lin-lin Mao2
Fan Wu1Kai-ning Lu2Lin-lin Mao2 Ling-qian Zhao1Ke-cheng Jiang1Yu Zhang2Wei-Jun Zheng3Ding-cun Luo2*
Ling-qian Zhao1Ke-cheng Jiang1Yu Zhang2Wei-Jun Zheng3Ding-cun Luo2*- 1The Fourth Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, China
- 2Department of Surgical Oncology, Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine, Hangzhou, China
- 3The School of Public Health, Zhejiang Chinese Medical University, Hangzhou, China
Purpose: To investigate the prognostic significance of extranodal extension (ENE) in papillary thyroid cancer (PTC).
Methods: Seven hundred forty-three PTC patients were enrolled in the study from January 2014 to December 2017. The patients were dichotomized according to the presence of ENE. Logistic analysis was used to compare differences between the two groups. Kaplan–Meier (K-M) curve and propensity score matching (PSM) analyses were used for recurrence-free survival (RFS) comparisons. Cox regression was performed to analyze the effects of ENE on RFS in PTC.
Results: Thirty-four patients (4.58%) had ENE. Univariate analysis showed that age, tumor size, extrathyroidal extension, and nodal stage were associated with ENE. Further logistic regression analysis showed that age, extrathyroidal extension, and nodal stage remained statistically significant. Evaluation of K-M curves showed a statistically significant difference between the two groups before and after PSM. Cox regression showed that tumor size and ENE were independent risk factors for RFS.
Conclusions: Age ≥55 years, extrathyroidal extension, and lateral cervical lymph node metastasis were identified as independent risk factors for ENE. ENE is an independent prognostic factor in PTC.
Introduction
With the rapid development of medical technology, the demand for evidence-based clinical practice and decision-making has progressively increased. Recent studies using real-world data (RWD) are increasingly high profile and have received increasing attention in the medical field (1). Within the context of a rapidly rising incidence of thyroid tumors, a wealth of clinical data about papillary thyroid carcinoma (PTC) has been accumulated (2).
In previous studies on PTC, approximately 20%–80% of patients have cervical lymph node metastasis when diagnosed (3, 4). However, PTC has an indolent clinical course despite the high incidence of lymph node metastasis. The prognosis of lymph node metastasis in PTC patients remains controversial (5). When PTC develops lymph node metastasis, some metastatic cancers may break through the node capsule into neighboring tissue and metastasize to regional organs, which is called extranodal extension (ENE) (6). On the one hand, it has been reported that 14.5% of PTC patients with ENE may relapse, and ENE is considered to be an independent risk factor for recurrence and survival (7). On the other hand, some scholars have pointed out that invasive ENE does not affect the survival of PTC patients (8).
However, the above studies were all retrospective studies conducted under natural conditions, and confounding factors on the prognostic significance of ENE were not eliminated. Therefore, the purpose of this study was to evaluate the prognostic significance of ENE in PTC using the propensity score matching (PSM) method, which will provide more updated, comprehensive evidence for clinical decision-making.
Materials and Methods
Patients and Clinicopathological Data
We retrospectively reviewed the electronic medical records of 2,094 PTC patients in the Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine, from January 2014 to December 2017. Then, patients were selected according to the following inclusion criteria: 1) PTC and cervical lymph node metastasis were confirmed by pathologic examination and 2) the clinical and pathological data were complete. The exclusion criteria were as follows: 1) the patient had other malignant tumors and 2) the patient had a history of cervical radiotherapy or trauma. All the patients who underwent surgery signed informed consent forms, and all the study contents were approved. The process of patient enrollment to the study cohort is shown in Figure 1. The present study was approved by the ethics committee of our institution.
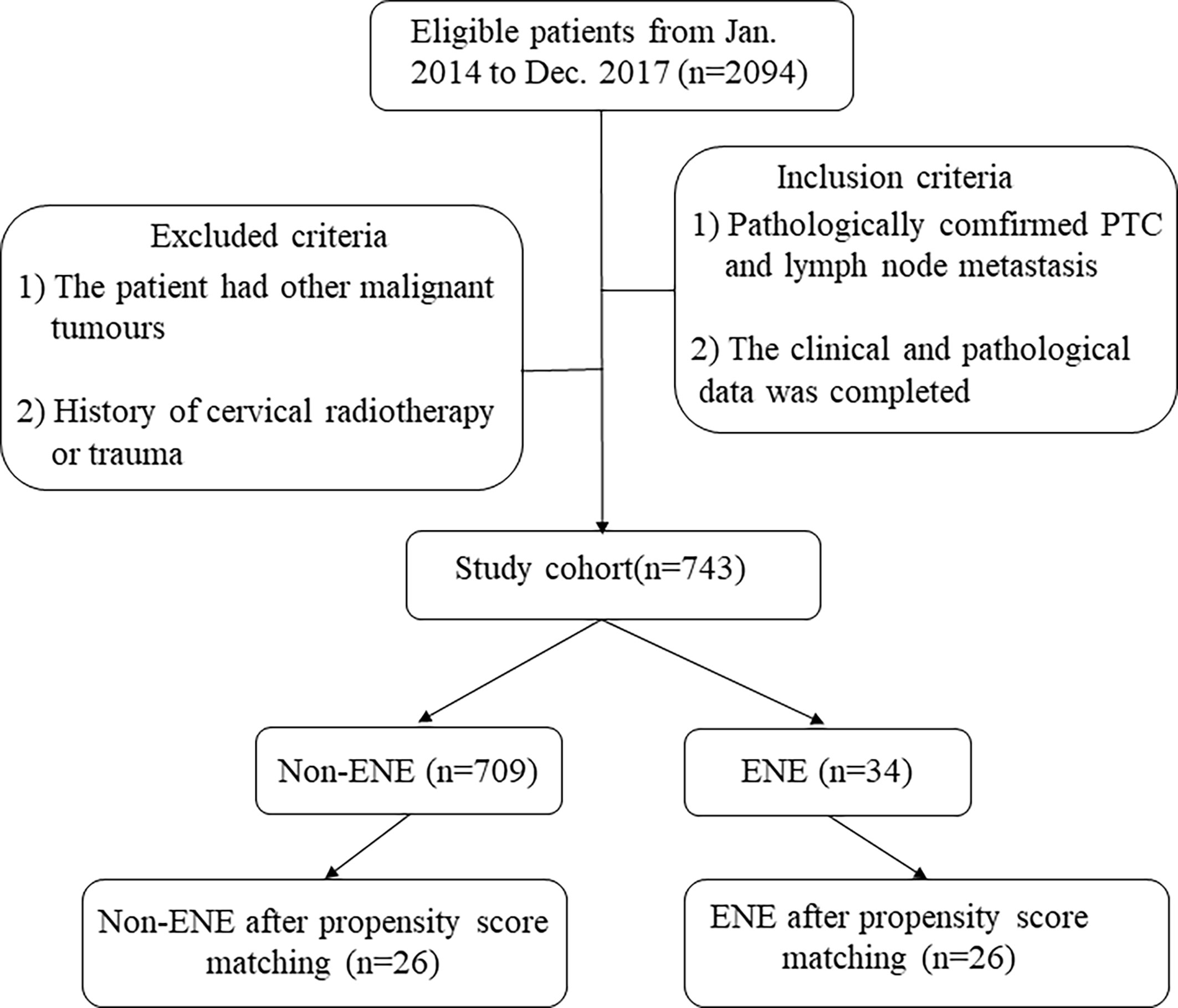
Figure 1 Process of patient enrollment into the study cohort and included patients. ENE, extranodal extension; PTC, papillary thyroid carcinoma.
Evaluation of Extranodal Extension and Extrathyroidal Extension
All clinical data were available through the electronic medical records, and patients with macroscopic ENE and macroscopic extrathyroidal extension were included in this study. ENE was defined as follows: intraoperative findings indicating that the organ had gross invasion by lymph node metastasis. As showed in Figure 2 Extrathyroidal extension was defined as invasion of the larynx, trachea, esophagus, recurrent laryngeal nerve, mediastinal vessels, or carotid artery from the thyroid primary tumor site but not invasion of the sternothyroid or sternohyoid muscle (8, 9).
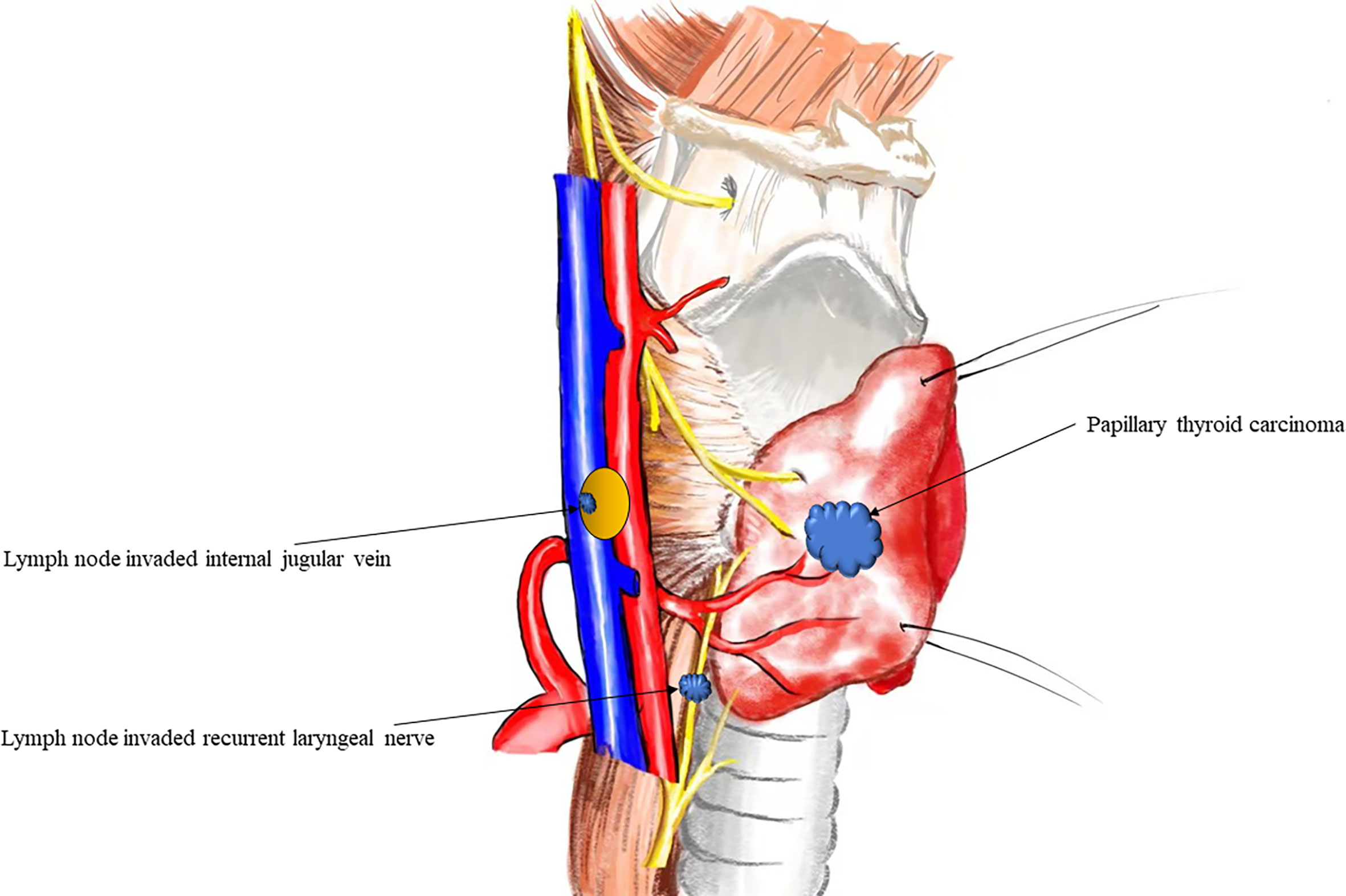
Figure 2 Anatomical diagram of extranodal extension in papillary thyroid cancer.
Follow-Up Strategy for Papillary Thyroid Carcinoma Patients
During follow-up, the endpoint was recurrence-free survival (RFS) (without regional recurrence after surgery). All patients were regularly followed up by clinical evaluation, serum thyroglobulin level measurement, and ultrasound examinations 6 months after surgery. Recurrence was defined as structural recurrence and pathologically confirmed by fine-needle aspiration biopsy (FNAB) or distant recurrence. If the patient was lost to follow-up, their data were censored.
Treatment Strategy for Papillary Thyroid Carcinoma Patients
All patients underwent open surgery. Thyroidectomy and cervical lymph node dissection were performed concurrently. Central lymph nodes were routinely dissected. Lateral cervical dissection was performed in patients with evidence of lateral cervical lymph node metastases through FNAB or preoperative imaging evidence. Important structures, such as the internal jugular arteriovenous, sternocleidomastoid muscle, and spinal accessory nerve, were spared. The therapeutic strategy for PTC with ENE was no residual resection or iodine 131 treatment. All PTC patients continued thyroid-stimulating hormone (TSH) suppression therapy after surgical treatment.
Statistical Analysis
Statistical analysis was performed with R Studio (Version 1.3.1093). Normally distributed data are expressed as the mean ± standard deviation (SD), and skewed data are expressed as the interquartile range. Univariate and multivariable logistic regression analyses were used to compare two groups. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. The log-rank test and Kaplan–Meier (K-M) curves were used for prognosis comparisons. Cox regression was performed to calculate the hazard ratios (HRs) and 95% CIs to determine the effects of ENE on RFS in PTC. P < 0.05 was considered statistically significant.
PSM analysis was conducted to minimize the effects of potential confounders on selection bias. PSM was performed with 1:1 matching and a caliper value of 0.02.
Results
During the study period, 743 PTC patients were included. Among them, 220 were male and 523 were female. The age range of the patients was 18–76 years, with a mean of 42.84 years and an SD of 12.75 years. The baseline features of the PTC patients are presented in Table 1.
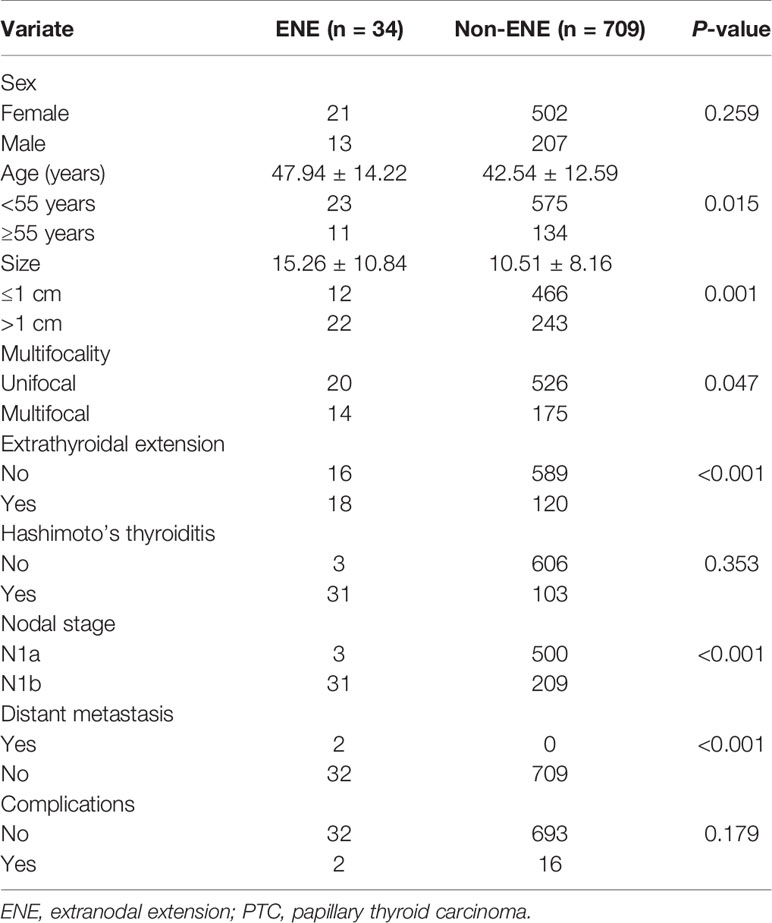
Table 1 Baseline characteristics of the PTC patients.
Clinical Characteristics of Extranodal Extension Patients
Thirty-four patients (34/743, 4.58%) with ENE were enrolled. The invaded organs were classified according to their location in the central neck compartment or lateral neck compartment. Thirty patients showed ENE of the central lymph nodes, and the median tumor size was 17.76 ± 13.66 mm. Lymph nodes mainly invaded the recurrent laryngeal nerve, followed by the surrounding adipose tissue and parathyroid gland. Twenty-two patients showed ENE of the lateral lymph nodes, and the median tumor size was 15.27 ± 10.87 mm. The internal jugular vein was the most frequently invaded of the cervical artery, followed by the adipose tissue, accessory nerve, and common carotid artery (Table 2).

Table 2 Extranodal extension in the central and lateral neck compartments.
Risk Factors of Papillary Thyroid Carcinoma Patients With Extranodal Extension
Univariate analysis showed that age, tumor size, extrathyroidal extension, and nodal stage were associated with ENE, whereas sex, multifocality, and Hashimoto’s thyroiditis were not. We conducted multivariate analysis to further verify whether risk factors affected PTC patients with ENE. Our results showed that age, extrathyroidal extension, and nodal stage remained significantly different, but tumor size did not (Table 3).
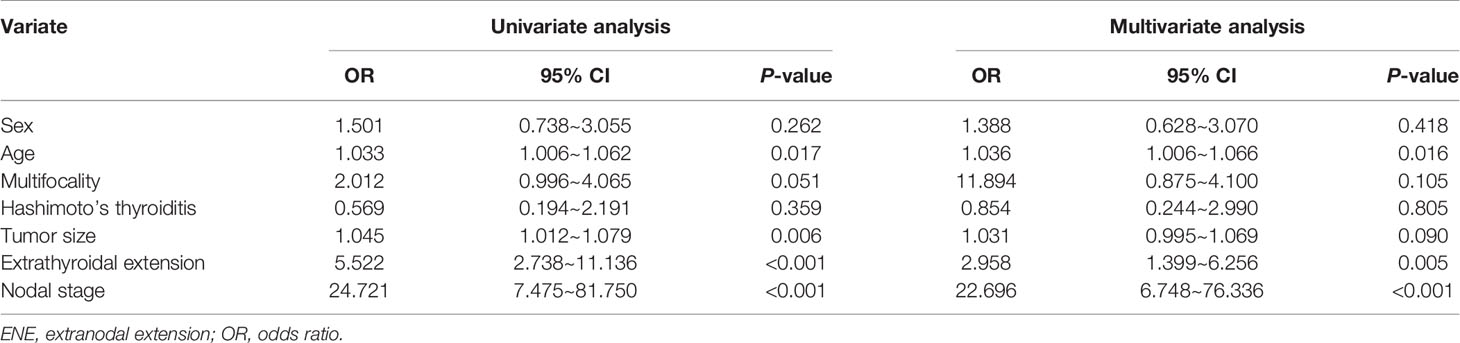
Table 3 Logistic regression analysis of ENE-related risk factors.
Comparison of the Effect of Extranodal Extension on Patient Recurrence-Free Survival
Twenty-three patients were lost to follow-up during the study period. The median follow-up time was 40.46 ± 15.51 months, and 15 of 720 PTC patients in this study experienced relapse. A comparison of the prognosis of the patients in the two groups indicated that the RFS of patients with ENE was lower than that of patients without ENE, and there was a significant difference between the two groups (P < 0.001; Figure 3).
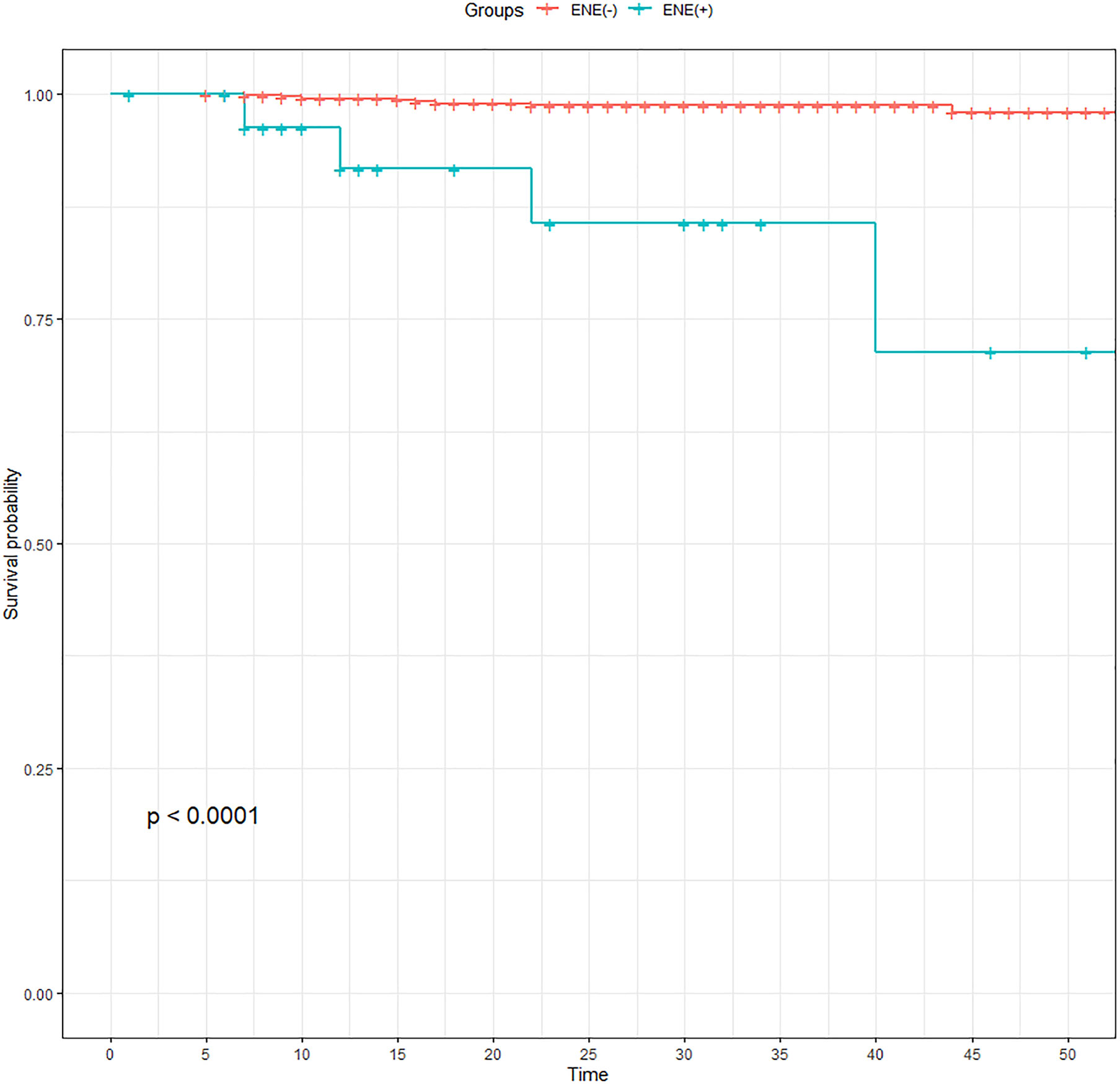
Figure 3 Comparison of recurrence-free survival of PTC patients before propensity score matching. ENE, extranodal extension; PTC, papillary thyroid carcinoma.
Then, we conducted PSM analysis to minimize the effects of potential confounders on selection bias. The model was adjusted for the following variables: sex, age, multifocality, tumor size, extrathyroidal extension, Hashimoto’s thyroiditis, and nodal stage. Finally, a total of 52 patients (26 one-to-one matched patients from each cohort) were compared, and RFS was subsequently compared (Table 4). The K-M curve indicated a statistically significant difference between the two groups after PSM (P = 0.049; Figure 4).
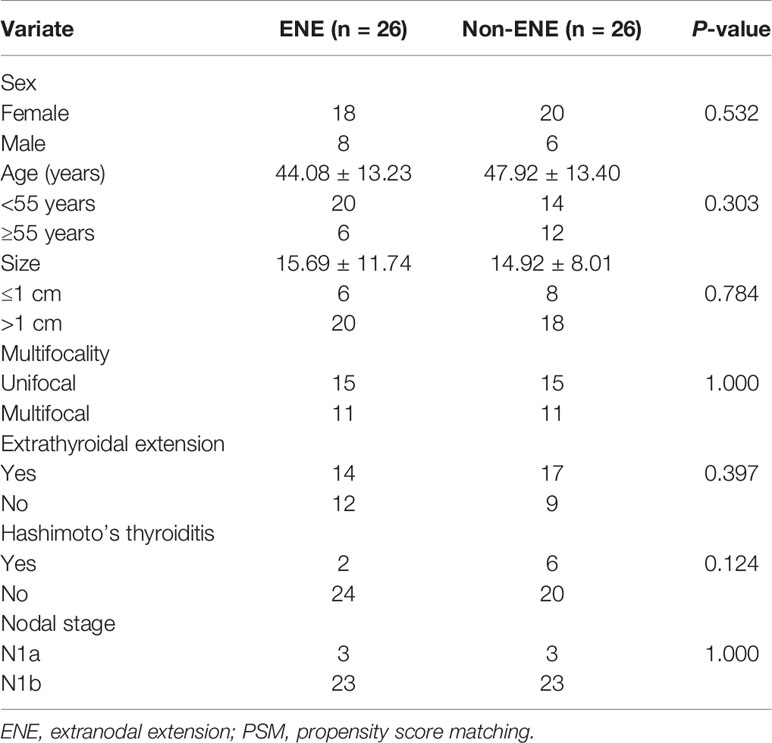
Table 4 Baseline clinical characteristics and procedure characteristics after PSM.
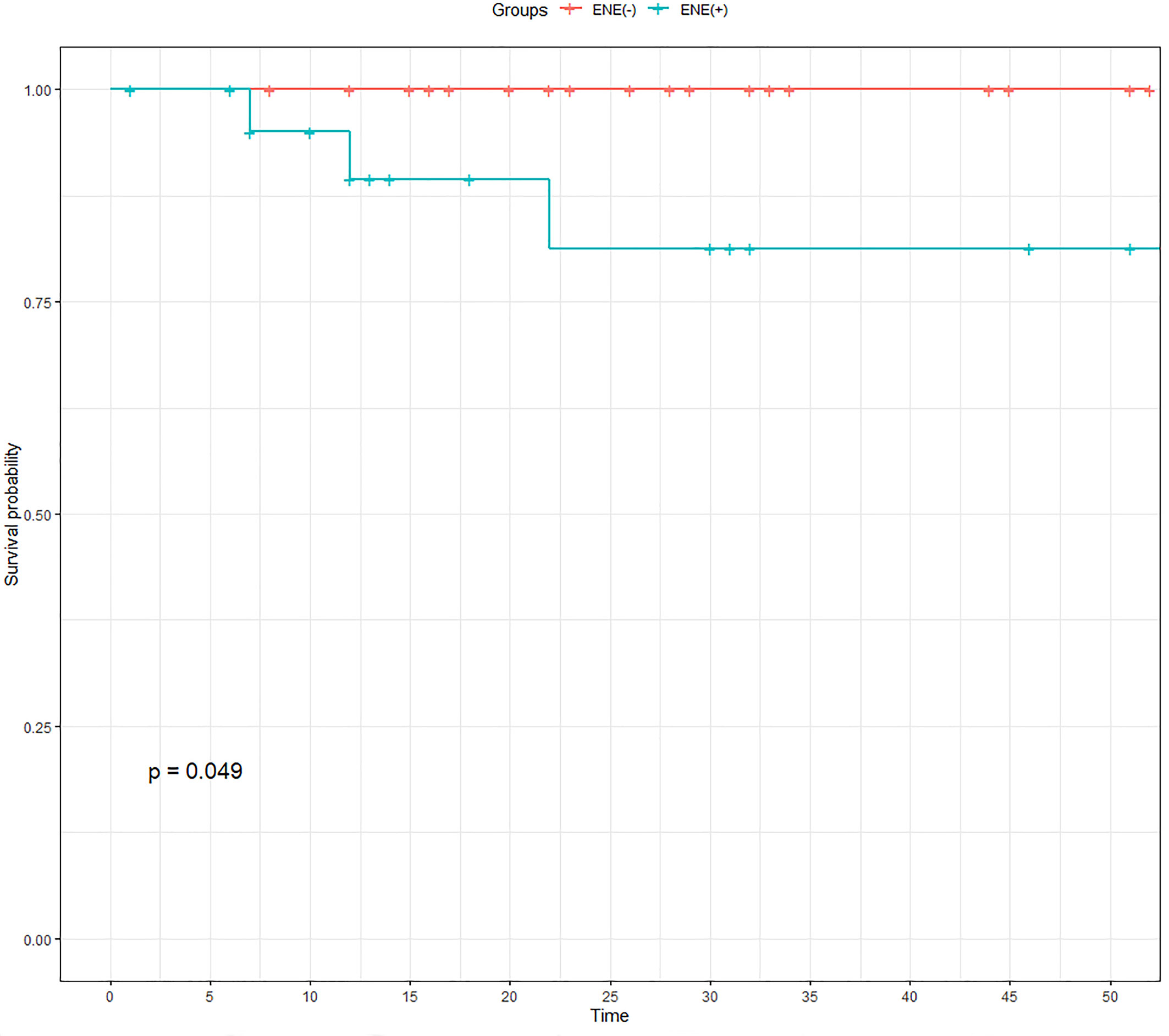
Figure 4 Comparison of recurrence-free survival of PTC patients after propensity score matching. ENE, extranodal extension; PTC, papillary thyroid carcinoma.
We further conducted Cox regression analysis to determine the effects of ENE on RFS in PTC. Our results showed that age, tumor size, and ENE were independent risk factors for RFS before PSM. Then, we balanced the confounding factors, and tumor size and ENE still showed statistical significance after PSM (Table 5).

Table 5 Cox regression analysis of patients before and after PSM.
Discussion
In recent years, thyroid carcinoma has exhibited the most rapid increase in incidence among solid tumors, and PTC is the most common malignant thyroid cancer (10). Previous studies have shown that lymph node metastasis is very common, with an occurrence rate of 20%~80% in PTC. In our study, the lymph node metastasis rate was 35.48% (743/2094), which is consistent with that in the literature (3, 4). The American Thyroid Association risk stratification system includes the size and number of positive lymph nodes but not ENE (9). The presence of ENE is an important prognostic indicator in breast cancer and oral cancer. It has been previously suggested that a new risk stratification system incorporating ENE for predicting structural recurrent disease should be developed, but Shen et al. questioned this (11, 12). The prognostic role of ENE in PTC has long been controversial.
Previous studies, including a meta-analysis, suggest that the presence of ENE is a significant poor prognostic factor in PTC (13). Wu et al. (7) found that age ≥45 years and ENE are significant adverse independent prognostic factors for patients with PTC. Suh et al. (13) showed that PTC patients with ENE had a 2.01-fold higher risk of recurrence and a 3.37-fold higher risk of death than patients without ENE. At the same time, our results show that ENE is an independent risk factor for RFS. After PSM, we further confirmed the relationship between ENE and prognosis. Therefore, ENE has been suggested as a potential prognostic factor in previous studies.
The relationship between ENE and prognosis was further analyzed using PSM. PSM is an effective statistical method that can process nonrandomized study data (such as RWD) and effectively reduce the confounding factors to fully equalize differences between the study groups (14). For PSM, we adjusted for confounding factors that may have an impact on prognosis. Indeed, the independent prognostic predictive capability of ENE was retained even after adjustment for confounding factors.
This study also showed a significant association between ENE and the clinicopathological features of PTC, such as age, tumor size, extrathyroidal extension, and nodal stage. Roh et al. (15) found that age, tumor size, and nodal stage were significant factors for predicting ENE, which is similar to our research results. However, our study showed that tumor size was the only meaningful factor in the univariate analysis, and its predictive advantage was not seen in the multivariate analysis; it will be the subject of further study. Jointly, the two studies suggest that ENE is more likely to occur in older PTC patients with lymph node metastases in the lateral neck compartment. At the same time, various studies have confirmed the significant correlation between extrathyroidal extension and ENE. Kim et al. (16) reported that extrathyroidal extension was an independent predictor of ENE in a retrospective analysis of 1,693 PTC patients. In a study of 193 PTC patients with cervical lymph node metastasis, Clain et al. (17) found that the incidence of ENE increased 13-fold when patients with cervical lymph node metastasis also had extrathyroidal extension, which is consistent with our research results. Therefore, patients with these two clinical factors should be aware of the increased potential for ENE and the possible prognostic implications.
In the central neck compartment, the recurrent laryngeal nerve was most frequently infiltrated by lymph nodes with ENE. Moritani (8) found that there was a lower probability of neural palsy with ENE than with tumors directly invading the recurrent laryngeal nerve, so PTC patients often have no obvious clinical manifestations, such as hoarseness, before surgery. Ultrasound has certain significance for swollen lymph nodes with fusion signs, microcalcifications, cystic degeneration, and a ratio of length to short diameter of <2 to demonstrate ENE (18), but Alpert et al. (19) pointed out that ENE is not positively correlated with lymph node size, with lymph nodes less than 1 cm in diameter also being prone to ENE. The sensitivity of detecting lymph nodes invading nerves through ultrasound or neck enhanced computed tomography (CT) and other imaging data is low, so it is difficult to identify ENE with nerve involvement before surgery.
There are still some shortcomings in this study. 1) The follow-up time of this study is brief, and we will continue to follow-up this group of patients to further compare the difference in the long-term survival of patients. 2) This study focused on the prognostic significance of patients with macroscopic ENE. Further comprehensive studies on the prognostic significance of microscopic ENE are expected.
In summary, ENE is relatively uncommon in thyroid carcinoma, accounting for only 4.58% of all cases of lymph node metastasis in this study. Age ≥55 years, extrathyroidal extension, and lateral cervical lymph node metastasis have been identified as independent risk factors for ENE. ENE is an independent prognostic factor in PTC.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Hangzhou First People’s Hospital. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
D-CL and T-HZ: drafted the work, designed the work, collected and analyzed data, revised the article for important content, final approval of the article to be published, agreement to be accountable for the work. FW: drafted the work, designed the work, collected and analyzed data, wrote the article, revised the article for important content, final approval of the article to be published, agreement to be accountable for the work. K-NL: designed the work, collected and analyzed data, revised the article for important content, final approval of the article to be published, and agreement to be accountable for the work. L-LM: collected and analyzed data, revised the article for important content, final approval of the article to be published, and agreement to be accountable for the work. L-QZ: collected and analyzed data, final approval of the article to be published, and agreement to be accountable for the work. K-CJ: collected and analyzed data, final approval of the article to be published, and agreement to be accountable for the work. YZ: drafted the work, designed the work, revised the article for important content, final approval of the article to be published, and agreement to be accountable for the work. BL and W-JZ: Statistical analysis and data processing, final approval of the article to be published, and agreement to be accountable for the work. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (Grant numbers 0020190490 and 0020190151), the Medical and Health Technology Project of Hangzhou (Grant number A20200432), and the Zhejiang Provincial Medical and Health Technology Project (Grant number 2019RC240).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors thank Mr Zhuan Yang for drawing the schematic in Figure 2.
References
1. Booth CM, Karim S, Mackillop WJ. Real-World Data: Towards Achieving the Achievable in Cancer Care. Nat Rev Clin Oncol (2019) 16:312–25. doi: 10.1038/s41571-019-0167-7
2. Lyu YS, Pyo JS, Cho WJ, Kim SY, Kim JH. Clinicopathological Significance of Papillary Thyroid Carcinoma Located in the Isthmus: A Meta-Analysis. World J Surg (2021) 45:2759–68. doi: 10.1007/s00268-021-06178-1
3. Sun W, Lan X, Zhang H, Dong W, Wang Z, He L, et al. Risk Factors for Central Lymph Node Metastasis in CN0 Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. PloS One (2015) 10:e0139021. doi: 10.1371/journal.pone.0139021
4. Luo DC, Xu XC, Ding JW, Zhang Y, Peng Y, Pan G, et al. Clinical Value and Indication for the Dissection of Lymph Nodes Posterior to the Right Recurrent Laryngeal Nerve in Papillary Thyroid Carcinoma. Oncotarget (2017) 8:79897–905. doi: 10.18632/oncotarget.20275
5. Lu S, Zhao R, Ni Y, Ding J, Qiu F, Peng Y, et al. Development and Validation of a Nomogram for Preoperative Prediction of Cervical Lymph Node Involvement in Thyroid Microcarcinoma. Aging (Albany NY) (2020) 12:4896–906. doi: 10.18632/aging.102915
6. Rowe ME, Ozbek U, Machado RA, Yue LE, Hernandez-Prera JC, Valentino A, et al. The Prevalence of Extranodal Extension in Papillary Thyroid Cancer Based on the Size of the Metastatic Node: Adverse Histologic Features Are Not Limited to Larger Lymph Nodes. Endocr Pathol (2018) 29:80–5. doi: 10.1007/s12022-018-9518-7
7. Wu MH, Shen WT, Gosnell J, Duh QY. Prognostic Significance of Extranodal Extension of Regional Lymph Node Metastasis in Papillary Thyroid Cancer. Head Neck (2015) 37:1336–43. doi: 10.1002/hed.23747
8. Moritani S. Impact of Invasive Extranodal Extension on the Prognosis of Patients With Papillary Thyroid Carcinoma. Thyroid (2014) 24:1779–83. doi: 10.1089/thy.2014.0167
9. American Thyroid Association Surgery Working Group, American Association of Endocrine Surgeons, American Academy of Otolaryngology-Head and Neck Surgery, American Head and Neck Society, Carty SE, Cooper DS, et al. Consensus Statement on the Terminology and Classification of Central Neck Dissection for Thyroid Cancer. Thyroid (2009) 19:1153–8. doi: 10.1089/thy.2009.0159
10. Morris LG, Sikora AG, Tosteson TD, Davies L. The Increasing Incidence of Thyroid Cancer: The Influence of Access to Care. Thyroid (2013) 23:885–91. doi: 10.1089/thy.2013.0045
11. Kim HI, Hyeon J, Park SY, Ahn HS, Kim K, Han JM, et al. Impact of Extranodal Extension on Risk Stratification in Papillary Thyroid Carcinoma. Thyroid (2019) 29:963–70. doi: 10.1089/thy.2018.0541
12. Shen M WC, Li Z. Re: “Impact of Extranodal Extension on Risk Stratification in Papillary Thyroid Carcinoma” by Kim Et al. Thyroid (2020) 30:466. doi: 10.1089/Thy.2018.0541
13. Suh S, Pak K, Seok JW, Kim IJ. Prognostic Value of Extranodal Extension in Thyroid Cancer: A Meta-Analysis. Yonsei Med J (2016) 57:1324–8. doi: 10.3349/ymj.2016.57.6.1324
14. Mangiafico S, Pigo F, Bertani H, Caruso A, Grande G, Sgamato C, et al. Over-The-Scope Clip vs Epinephrine With Clip for First-Line Hemostasis in Non-Variceal Upper Gastrointestinal Bleeding: A Propensity Score Match Analysis. Endosc Int Open (2020) 8:E50–8. doi: 10.1055/a-1005-6401
15. Roh JL PJ, Jeong J, Gong G, Cho KJ, Choi SH, Nam SY, et al. Extranodal Extension of Lymph Node Metastasis as a Prognostic Indicator of Recurrence and Survival in Papillary Thyroid Carcinoma. J Surg Oncol (2017) 116:450–8. doi: 10.1002/jso.24713
16. Kim JW RJ, Gong G, Cho KJ, Choi SH, Nam SY, Kim SY. Extent of Extrathyroidal Extension as a Significant Predictor of Nodal Metastasis and Extranodal Extension in Patients With Papillary Thyroid Carcinoma. Ann Surg Oncol (2017) 24:460–8. doi: 10.1245/s10434-016-5594-4
17. Clain JB SS, Dos Reis L, Turk A, Wenig BM, Mehra S, Karle WE, et al. Extrathyroidal Extension Predicts Extranodal Extension in Patients With Positive Lymph Nodes: An Important Association That May Affect Clinical Management. Thyroid (2014) 24:951–7. doi: 10.1089/thy.2013.0557
18. Mu JL, Li FX, Wei X, Xin XJ, Zhang S. Clinicopathological and Ultrasound Characteristics of Extranodal Extension in Metastatic Papillary Thyroid Carcinoma Patients. Zhonghua Zhong Liu Za Zhi (2018) 40:264–7. doi: 10.3760cma.j.issn.0253-3766.2018.04.005
Keywords: extranodal extension, papillary thyroid carcinoma, prognosis, propensity score matching, lymph node metastasis, the real world
Citation: Zhou T-h, Lin B, Wu F, Lu K-n, Mao L-l, Zhao L-q, Jiang K-c, Zhang Y, Zheng W-J and Luo D-c (2021) Extranodal Extension Is an Independent Prognostic Factor in Papillary Thyroid Cancer: A Propensity Score Matching Analysis. Front. Endocrinol. 12:759049. doi: 10.3389/fendo.2021.759049
Received: 15 August 2021; Accepted: 05 October 2021;
Published: 03 November 2021.
Edited by:
Akira Sugawara, Tohoku University, JapanReviewed by:
Junichi Tani, Tohoku Medical and Pharmaceutical University, JapanKhawla S. Al-Kuraya, King Faisal Specialist Hospital & Research Centre, Saudi Arabia
Copyright © 2021 Zhou, Lin, Wu, Lu, Mao, Zhao, Jiang, Zhang, Zheng and Luo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ding-cun Luo, bGRjNjVAMTYzLmNvbQ==