
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 05 October 2021
Sec. Obesity
Volume 12 - 2021 | https://doi.org/10.3389/fendo.2021.743962
This article is part of the Research Topic Association of Novel Anthropometric Indexes with Metabolic Syndrome View all 15 articles
 Yu’e Xi1
Yu’e Xi1 Wenjing Gao1*Ke Zheng1Jun Lv1Canqing Yu1
Wenjing Gao1*Ke Zheng1Jun Lv1Canqing Yu1 Shengfeng Wang1Tao Huang1
Shengfeng Wang1Tao Huang1 Dianjianyi Sun1Chunxiao Liao1Yuanjie Pang1
Dianjianyi Sun1Chunxiao Liao1Yuanjie Pang1 Zengchang Pang2Min Yu3Hua Wang4Xianping Wu5Zhong Dong6Fan Wu7Guohong Jiang8Xiaojie Wang9Yu Liu10Jian Deng11Lin Lu12Weihua Cao1*Liming Li1
Zengchang Pang2Min Yu3Hua Wang4Xianping Wu5Zhong Dong6Fan Wu7Guohong Jiang8Xiaojie Wang9Yu Liu10Jian Deng11Lin Lu12Weihua Cao1*Liming Li1Aims/Hypothesis: We aimed to explore whether and to what extent overweight or obesity could increase the risk of hypertension, and further to estimate the roles of genetic and early-life familial environmental factors in their association.
Methods: This prospective twin study was based on the Chinese National Twin Registry (CNTR), which collected information from self-report questionnaires. We conducted unmatched case-control analysis to examine the association between overweight or obesity and hypertension. And further to explore whether genetics and familiar environments shared within a twin pair, accounted for their association via co-twin matched case-control design. Generalized estimating equation (GEE) models and conditional logistic regressions were used in the unmatched and matched analyses, respectively. Then, we used logistic regressions to test the difference in odds ratios (ORs) between the unmatched and matched analyses. Finally, through bivariate twin model, the roles of genetic and environmental factors in the body mass index (BMI)- hypertension association were estimated.
Results: Overall, we included a total of 30,617 twin individuals, of which 7533 (24.6%) twin participants were overweight or obesity and 757 (2.5%) developed hypertension during a median follow-up time of 4.4 years. In the GEE model, overweight or obesity was associated with a 94% increased risk of hypertension (OR=1.94, 95% confidence interval (CI): 1.64~2.30). In the conditional logistic regression, the multi-adjusted OR was 1.80 (95% CI: 1.18~2.74). The difference in OR between unmatched and matched analyses was significant (P=0.016). Specifically, overweight or obesity was not associated with hypertension risk in the co-twin design when we full controlled genetic and familiar environmental factors (OR=0.89, 95 CI: 0.46~1.72). After controlling for age and sex, we found the positive BMI-hypertension association was mainly explained by a genetic correlation between them (rA= 0.59, 95% CI: 0.44~1.00).
Conclusions/Interpretation: Genetics and early-life environments shared by participants within a twin pair appear to account for the association between overweight or obesity and hypertension risk.
Raised blood pressure remains the leading cause of death globally, high systolic blood pressure accounted for 10·8 million deaths in 2019 (1). Unfortunately, hypertension has high prevalence but low rate of control. It is estimated that 1 in 4 men and 1 in 5 women (1.13 billion people), living with hypertension in 2015, but less than 1/5 have their blood pressure under control (2).
In the worldwide, a large number of people suffer from higher body mass index (BMI), including overweight and obesity. In 2016, a total of 39% adults are overweight, with a BMI ≥ 25 kg/m2, and 13% are obese (BMI ≥ 30 kg/m2) (3). Higher BMI is a major risk factor of hypertension. In the original Framingham cohort, Wilson et al. (4) found overweight and obese status were associated with increased risk of hypertension: the multi-adjusted risk ratios (RRs) among the overweight was 1.48 in men and 1.70 in women, while among the obese was 2.23 in men and 2.63 in women. In another Framingham study, weight loss led to a 21%~29% reduction in long-term hypertension risk (5). Mendelian randomization (MR) analysis, using genetic variants as the instrumental variable, has also demonstrated the causality between obesity and hypertension (6).
Genetic and early-life environmental factors, including shared fetal environment, childhood socioeconomic situation and adolescent environment, might have long-term effects on the subsequent risk of obesity (7–9) and hypertension (10–12). However, due to the limitations of general population-based study, their roles in the obesity-hypertension association are uncertain. Co-twin case-control analysis could address part of this difficulty, by controlling for genetic background and key shared familial environmental factors associated with obesity and hypertension. Twins are generally raised together, so they share their early-life environmental factors. They also share the same genetic predisposition and intrauterine environments. Therefore, as naturally matched pairs, co-twin case-control analyses provide an opportunity to explore the role of genetic and early-life environmental factors in the association between overweight or obesity and hypertension (13, 14).
The purpose of this study was to examine the association between overweight or obesity and hypertension, and to explore whether the association could be explained by genetic and common environmental factors shared within a twin pair, based on information from the Chinese National Twin Registry (CNTR).
This prospective study enrolled twin participants from the CNTR (15), a twin population-based cohort study. Briefly, a total of 61,566 twin pairs, including 31,705 monozygotic (MZ) twins and 15,060 same-sex dizygotic (DZ) twins, from 11 provinces and cities in China were included at the baseline since 2001. Totally, the current study included 32,197 twins whose age was more than 18 years and participated in the resurvey.
We excluded 14 participants whose sex was missing. We also excluded 619 twins whose BMI was missing or with extreme outliers (under 3 or over 3-Z score of the BMI). In addition, we excluded those who were diagnosed with hypertension at baseline (892), and those who had no disease information at baseline or at the time of resurveys (55). Finally, a total of 30,617 twins were included for further association analysis (Figure 1).
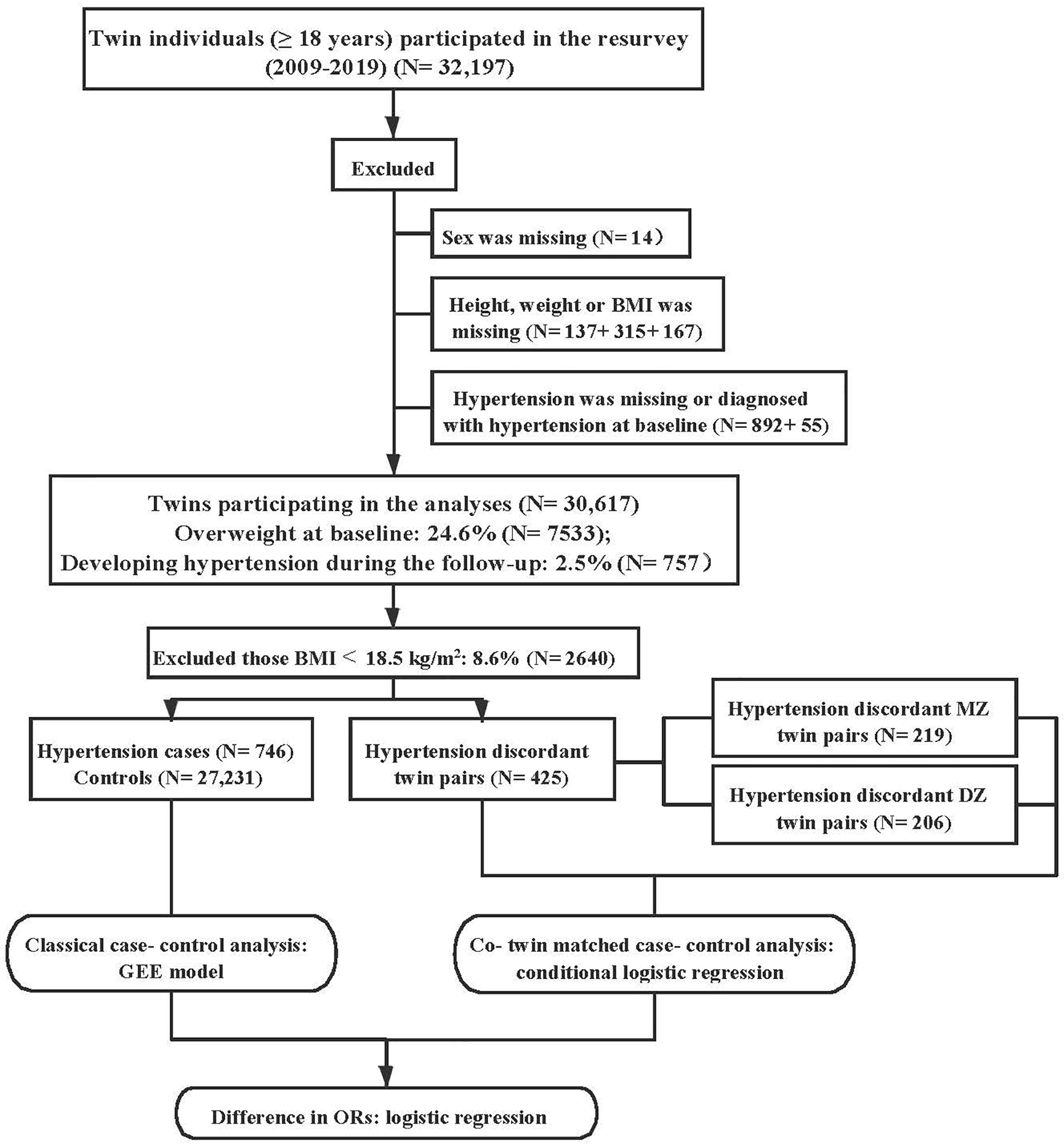
Figure 1 Flow chart of the study population and data analysis. BMI, body mass index; MZ, monozygotic; DZ, dizygotic; GEE, generalized estimating equation; OR, odds ratio.
We used the method of ‘Peas in the Pod Questionnaire (PPQ)’ to determine zygosity, asking about the degree of similarity shared by twins when they were at school age. Two former studies, based on the data from the CNTR, have verified its accuracy from 85% to 89% (16, 17).
All participants provided informed consent, and the study protocol was approved by the Ethics Committee at Peking University Health Science Center (IRB00001052-11029/14021).
We collected information, including demographics (age, sex, marital status and educational attainment), lifestyles (smoking status, drinking status and physical activity), anthropometric measures (weight and height), twin zygosity and history of diseases (including diabetes and hypertension), from face-to-face questionnaire interview by trained interviewers.
Self-reported questionnaire was used to attain the information of height (in centimeter) and weight (in kilograms) at baseline. BMI was calculated by weight in kilograms divided by squared height in meters (kg/m2). According to the Chinese criteria of obesity (18), we categorized BMI into four groups: underweight (<18.5 kg/m2), normal weight (18.5 to 23.9 kg/m2), overweight (24.0 to 27.9 kg/m2) and obesity (≥ 28.0 kg/m2). In the current study, overweight or obesity was defined as BMI ≥24 kg/m2, that is, obesity was merged into overweight.
We collected the information on hypertension during the follow-up, asking “Have you ever been diagnosed with hypertension by a county/district level or above hospital”. Whether the participants are with hypertension or not depends on the doctor’s definite diagnosis, not just on their self-reported symptoms.
Marital status was defined as married (or cohabitating) vs single (or divorced). Education attainment was categorized as primary, secondary and tertiary. Smoking status was grouped into never, former and current smoking. Drinking status was similarly divided into never, past and current drinking. Adequate physical activity was defined as exercising at least 30-minute moderate to high-intensity physical activity a day, and engaging in at least 5 days per week (19). Prevalence of diabetes was dichotomized into diabetes and diabetes-free.
The characteristics were compared between hypertension and non-hypertension groups. χ2 tests were used for categorical variables, independent sample t tests for continuous variables with normal distribution, and Mann Whitney U tests for continuous variables with non-normal distribution.
Generalized estimating equation (GEE) models were applied to assess the overweight-hypertension association, which are conceptually equivalent to logistic regressions for the classic case-control analysis, but controlling for the clustering of twins within a pair. In the co-twin matched case-control design, in which co-twin (both MZ and DZ twins) without hypertension was treated as a control for hypertension twin, we used conditional logistic regressions to explore the associations. Because cases and controls are matched for genetics and familial environments, discordant twin pairs were more informative than unrelated samples (20). Due to MZ twins share 100% genetic predisposition, while DZ twins share only 50%, we stratified the co-twin matched case-control analysis in MZ and DZ twins, respectively. Finally, logistic regressions were fitted to examine whether the ORs from the GEE model and conditional logistic regression are different, by comparing the distribution of overweight or obesity in the unmatched controls and co-twin controls (21). If a significant association between overweight or obesity and hypertension is only found in the GEE analysis, or OR in the co-twin analysis becomes significantly strengthened or attenuated, genetic and/or early-life environmental factors might play roles in their association (22, 23). In contrast, if difference in ORs between the GEE model and conditional logistic regression is not significant, then the genetic and shared familiar factors might not account for the observed association (14, 21, 24).
Age, sex, marital status, education attainment, smoking status, drinking status, physical activity and diabetes were considered as potential confounders. The basic-adjusted models were controlled for age and sex (twins within a pair have the same age, thus only sex was adjusted in the co-twin analysis). The multi-adjusted models were further adjusted for marital status, education, smoking, drinking, physical activity and diabetes.
The classical twin method decomposes the phenotype variation, based on the phenotypic correlations between twin pairs: MZ twins share 100% genetic materials, whereas DZ twins average share 50% of their segregating genes; all twins are correlated for environmental influences to the same extent. In this study, the liability threshold model, an extension of the classical twin modelling was used, assuming individual differences in a trait come from additive genetic (A), nonadditive genetic (D), shared environmental (C) and nonshared environmental (E) influences. The bivariate genetic model estimates the influence of A, C, D and E on each trait (BMI and hypertension), and also explores how much of the association (phenotypic correlation, rph) between them can be partitioned into addictive genetic (rA), nonaddictive genetic (rD), shared environmental (rC), and unique environmental (rE) correlation. Because of the effects of C and D are confounded in the classical twin model, including twin pairs reared together, they cannot be calculated simultaneously (25). For both BMI and hypertension, the ADE model was only fitted when the intraclass correlation coefficient (ICC) of MZ was more than double that of DZ twins. To investigate how much of the BMI-hypertension association is attributed to genetic or environmental correlations, we compared the difference of cross-trait, cross-twin correlations (CTCTs) between MZ and DZ twin pairs. A higher CTCT in MZ than in DZ twin pairs indicates that BMI and hypertension are associated because of correlated genetic influences. Based on the full ACE models, several nested models, including AE, CE and E, were fitted by dropping C, A and both components for the selection of best fitting model.
The likelihood ratio test was used to assess the fit of nested models, which approximately follows a χ2 distribution in that the degree of freedom is equal to the difference of the parameters number between the two models. Each nested model was compared with the full model to choose the best fitting model. The Akaike’s information criterion (AIC) was applied for the model selection, in which lower values suggesting a better balance between explanatory power and parsimony (26).
Data cleaning and statistical analyses were performed using Stata/MP 14.0. Structural equation models were fitted in R 3.5.1 with the use of an open source software package named OpenMx (version 2.14.11) (27).
Overall, a total of 30,617 twin individuals, including 17,571 (57.4%) men and 13,570 (44.8%) DZ twins were included in the current study. The average age at baseline was 32.6 ± 11.4 years, the median follow-up time was 4.4 years. 7533 participants (24.6%) were overweight, and 757 (2.5%) participants were diagnosed with hypertension in the resurvey. And among the overweight or obesity individuals at baseline, 371 (4.9%) twins developed hypertension during the follow-up. Participants who had hypertension were more likely to be older, male, overweight, current smokers, current drinkers, to have adequate physical activity, higher education, and to be diagnosed with diabetes, compared with those who were hypertension-free (Table 1).
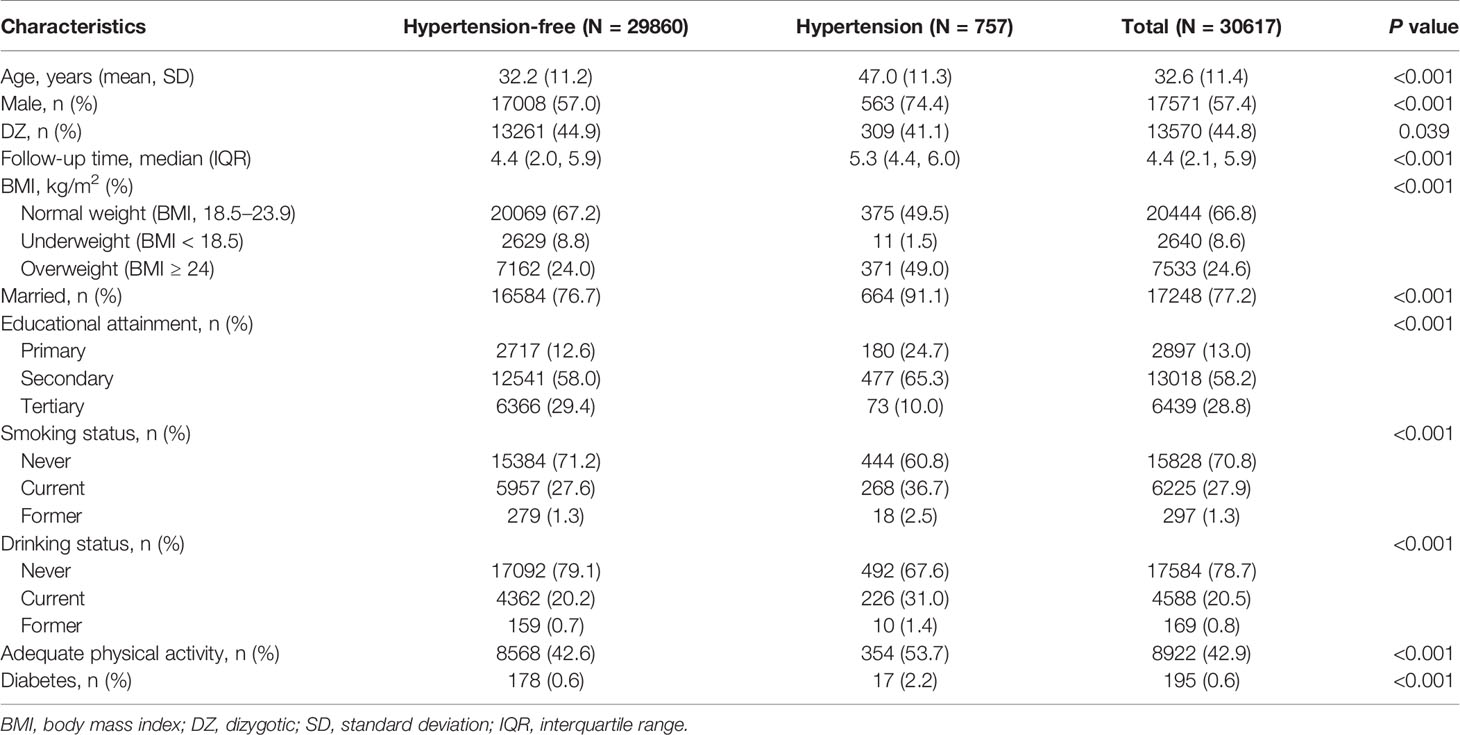
Table 1 Characteristics of the study participants by hypertension diagnosis (N = 30617).
After adjustment of age, sex, marital status, education, smoking, drinking, physical activity and diabetes, overweight or obesity increased a 94% risk of hypertension in the GEE model (OR=1.94, 95% CI: 1.64~2.30) (Table 2). In the multi-adjusted conditional logistic regression, overweight or obesity was associated with an 80% higher hypertension risk (OR=1.80, 95% CI: 1.18~2.74). In the matched analysis of DZ twins, controlling 50% genetic factors, overweight or obesity increased the risk of hypertension under the control of confounders (OR=2.86, 95% CI: 1.57~5.21). However, in the co-twin case-control analysis of MZ twins, the association between overweight or obesity and hypertension was not significant, the multi-adjusted OR was 0.89 (95% CI: 0.46~1.72) (Table 3). When we adjusted for the potential confounding variables, the difference in ORs between unmatched and matched case-control analyses was significant in all twin pairs (P=0.016), suggesting genetic, early-life familial environmental factors or both of them may partially contribute to the overweight-hypertension association (Table 4).
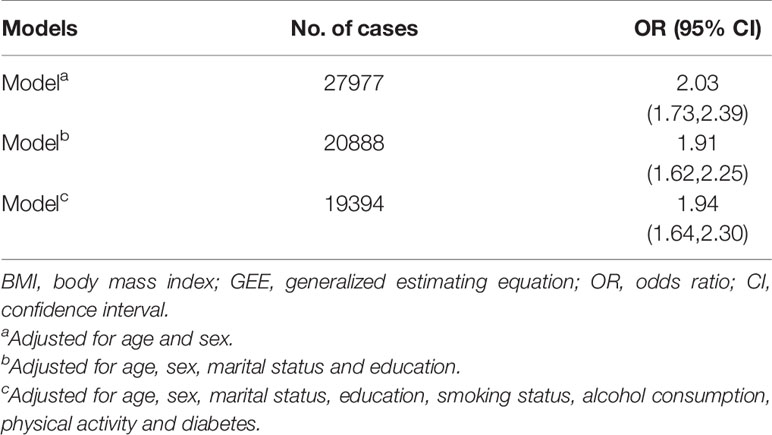
Table 2 ORs (95% CIs) of overweight or obesity-hypertension association (normal BMI as the reference) from the GEE models.
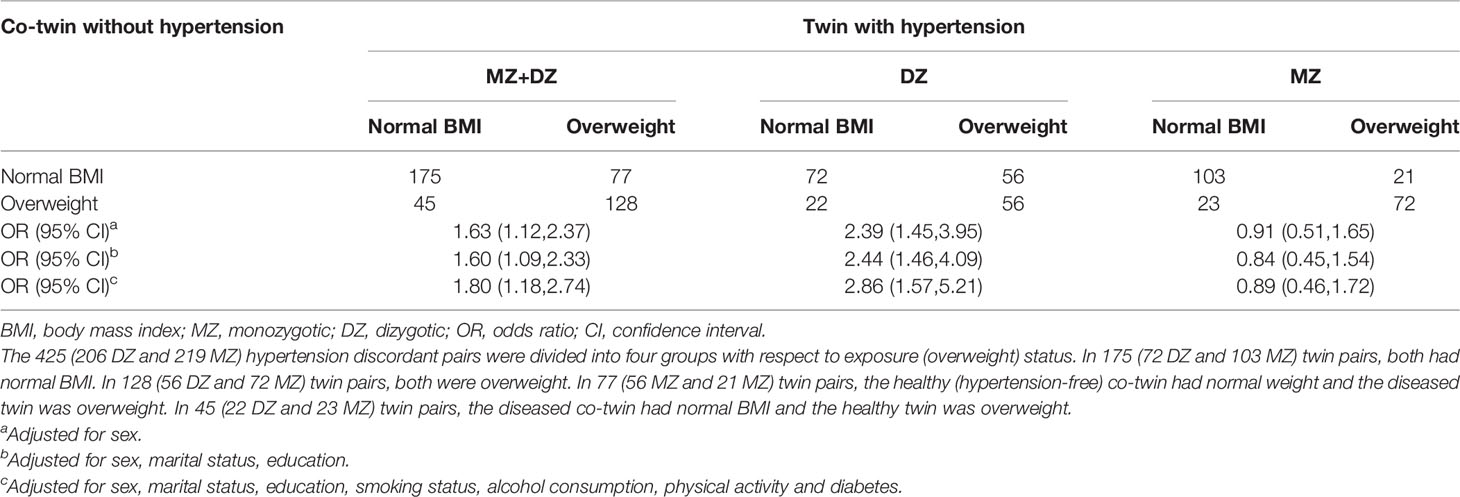
Table 3 ORs (95% CIs) for the association between overweight or obesity and hypertension in co-twin control analyses using hypertension discordant twin pairs from the conditional logistic regressions.
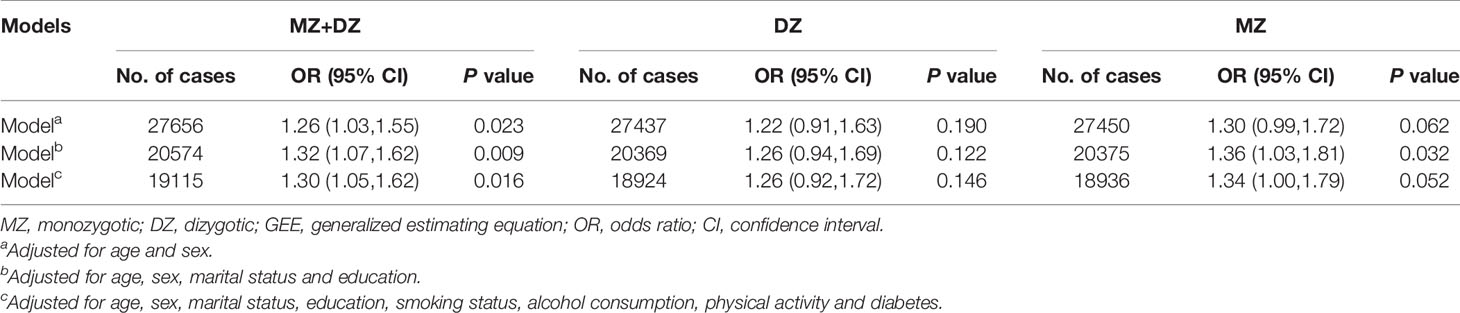
Table 4 Differences in ORs (95% CIs) for the unmatched GEE models and matched co-twin control analyses (the difference in overweight or obesity between unmatched and co-twin matched controls).
For both BMI and hypertension, the ICCs of MZ twins were larger than DZ twins, which implied genetic influences on both traits. Compared with DZ twins (r=0.10, 95% CI: 0.04~0.16), the CTCT was higher for MZ twins (r=0.18, 95% CI: 0.13~0.23), suggesting a genetic correlation between BMI and hypertension (Table 5). The analysis revealed that the full ACE model was the best-fitting one, which was therefore used for estimation of genetic and environmental influences (Supplementary Table 3). The additive genetic factors explained 45% (95% CI: 41%~49%) and 32% (95% CI: 8%~59%) variance of BMI and hypertension, respectively. The genetic correlation, which pointed to what degree genetic variance of BMI predicted the genetic influences on hypertension, was 0.59 (95% CI: 0.44~1.00). The shared and non-shared environmental correlations were not significant (Table 6).

Table 5 Correlations (95% CIs) for BMI, hypertension, and BMI-hypertension by zygosity.
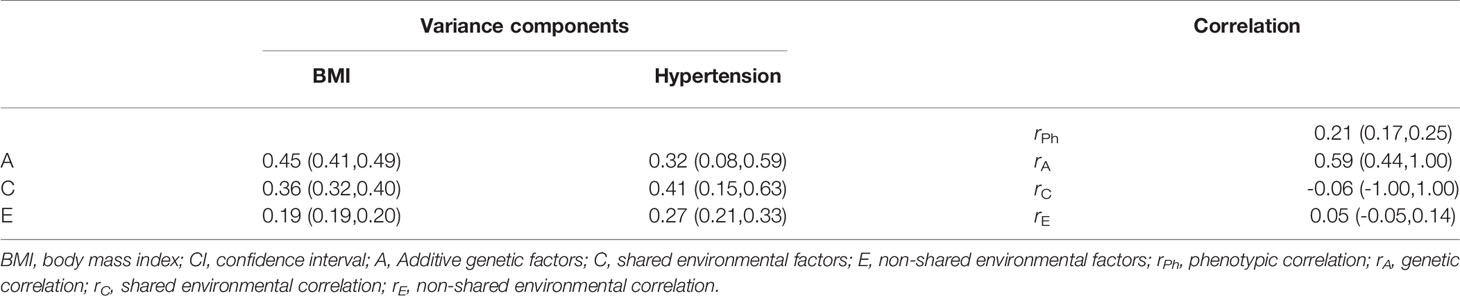
Table 6 Parameter estimates (95% CIs) from the best-fitting bivariate ACE full model of BMI and hypertension.
Considering the different effects of overweight and obesity on the risk of incident hypertension, we also separated participants who were overweight (BMI: 24- 28 kg/m2) and obesity (BMI ≥ 28 kg/m2) to explore their associations with hypertension. Under the control of potential influenced factors, both overweight and obesity increased hypertension risk, the ORs were 1.87 (95% CI: 1.57~2.24) and 2.64 (95% CI: 1.92~3.61), respectively (Supplementary Table 1). In the matched case-control study, overweight was associated with a 72% increased hypertension risk (OR=1.72, 95% CI: 1.12~2.67). However, due to the limited sample size, we found a borderline significant obesity-hypertension association in the matched analyses (OR=9.26, 95% CI: 1.00~85.50) (Supplementary Table 2). The different in ORs between unmatched and matched designs was significant for the obesity (P=0.009), but not significant for the overweight (P=0.075) (Supplementary Table 3).
In this large-scale, nationwide Chinese twin study, we found that both overweight and obesity were significantly associated with increased hypertension risk. And the associations were different between unmatched and matched analyses, and even non-significant in the co-twin analysis of MZ twins, indicating genetic or both genetic and environmental factors shared between co-twins are likely to contribute to the association. Furthermore, we found a positive correlation between BMI and hypertension, which was explained by a genetic correlation, providing evidence for the contribution of overlap genetic factors on their association.
Consistent with our findings, a growing number of studies have reported that overweight and obesity were independently associated with increased risk of hypertension. Using 5209 participants aged 30 to 62 years from the original Framingham cohort, Wilson et al. (4) found overweight and obese status were positively associated with hypertension: compared with those with normal weight, overweight increased a 48% (95% CI: 1.24~1.75) and 70% (95% CI: 1.48~1.94) risk of hypertension in the men and women, respectively; the age-adjusted RRs were 2.23 (95% CI: 1.75~2.84), and 2.63 (95% CI: 2.20~3.15) in male and female obese individuals, respectively. After 6.38-year follow-up, Qi et al. (28) reported a positive association between BMI and hypertension in the Chines: the RR was 3.13 (95% CI: 2.84~3.45) for the obesity. In the Framingham Study, Moore et al. (5) found weight loss ≥ 6.8 kg led to a 28% (RR=0.72, 95% CI: 0.49~1.05) and a 37% (RR=0.63, 95% CI: 0.42~0.95) reduction in hypertension risk for middle-aged and older adults, respectively; And sustained weight loss also reduced the hypertension risk: 22% and 26% for middle-aged and older adults, respectively. These studies provided evidence that overweight and obesity were independently associated with hypertension risk.
The mechanisms underlying the overweight (obesity)-hypertension association are complex and not completely understood. Obesity can directly produce a variety of structural and functional changes of the cardiovascular system, including lower cardiac output, poorer left ventricular systolic function, higher peripheral resistance, increased left ventricular mass, left ventricular wall thickness and internal dimension (29). In addition, obesity is associated with mechanisms that could increase sympathetic nervous system (SNS) activity, which is believed to play an important role in the development of hypertension. Angiotensin II could increase SNS activity, while angiotensinogen is expressed in visceral adipocytes (30, 31). In the obesity, the inhibitory of arterial baroreflex on SNS activity is reduced, contributing to the increased SNS activity to muscle and kidney (32, 33). And the dysregulation of the hypothalamic-pituitary-adrenal axis, characterized by obesity, seems to be important to the activation of the SNS in obese humans (34).
The co-twin case-control analysis could explore associations, under the control of genetic and unmeasured early-life environmental factors. In the current study, we found the overweight-hypertension association was attenuated in the matched study, and even disappeared in the co-twin analysis of MZ twins, indicating that the observed association was fully explained by genetic and familiar factors shared within a twin pair. Our results indicate these with family history of obesity may have high hypertension risk, which showed the important to prevent hypertension in these population. However, not consistent with our findings, MR analysis has demonstrated the causal effect of obesity on hypertension. Including 119,859 participants from UK Biobank, Lee et al. (6) showed a positive association between genetically instrumented higher BMI and hypertension risk (OR= 1.64, 95% CI: 1.48~1.83). In a Korea cohort study, using genetic risk scores (GRS), created by 6 single-nucleotide polymorphisms associated with BMI, researchers found a causal effect of BMI on hypertension (OR: 1.13~1.26) (35). In addition, a large number of studies have investigated the biological mechanisms underlying obesity-hypertension association. Therefore, our findings based on statistics analysis should be interpreted with caution. More large studies from Chinese population are warranted to verify our results.
Furthermore, using bivariate twin model, we further found the positive BMI-hypertension association was explained by a genetic correlation between them, providing evidence for the contribution of overlap genes on their relationship. Including a total of 913 subjects from 179 families, Li et al. (36) found waist circumference (WC) was genetically correlated with systolic blood pressure (rA=0.27), but found no significant genetic correlations between BMI and blood pressure. Although we found no study exploring the genetic link between overweight (obesity) and hypertension, numerous studies provide evidences for the pleiotropy between obesity and hypertension. FTO (fat mass and obesity-associated) gene, the first identified gene for obesity, is the strongest BMI related genetic factors (37, 38). Meta-analysis has demonstrated the associations between FTO SNPs and obesity risk (39, 40). It is reported that FTO gene is highly expressed in the hypothalamic nuclei (41, 42), involving in the control of energy homeostasis (43) and regulation of blood pressure (44). To date, several studies have investigated the association between FTO variants and risk of hypertension. Although the results are inconsistent, many large studies showed some of FTO genotypes significantly increased risks of hypertension (45). Many other genes, such as MC4R (46–48), TNF-α (49–51), LEP (LEPR) (52–56) and β2AR (57, 58), were all associated with both obesity and hypertension. However, because of the lack of comparable co-twin studies, the roles of shared genetic factors in the relationship between overweight or obesity and hypertension are still needed to be explored.
Although our co-twin analysis reported that early-life environment might contribute to the overweight-hypertension association, the common environmental correlation was not significant in the twin model. Not consistent with our results, as important parts of early-life environments, a growing body of studies described that poor fetal and early postnatal growth were associated with subsequent risk of obesity and hypertension. The majority of epidemiological studies utilize birth weight and gestational age as proxy markers for suboptimal utero growth. Abundant evidences suggested that high birth weight (HBW) and large for gestational age were associated with an increased risk of obesity later in life (59–61). In a meta-analysis, including 14 cohort studies, HBW (≥4000g) was associated with higher risk of obesity (OR=1.43, 95% CI: 1.25~1.64), but not low birth weight (LBW) (<2500 g) (60). Furthermore, low birth weight (LBW) was associated with higher hypertension risk (62–65). In the Shanghai Women’s Health Study and the Shanghai Men’s Health Study, an excess risk of hypertension was observed for LBW, hazard ratio (HR) was 1.20 (95% CI: 1.11~1.30) (63). In the Swedish twin study on the fetal origins of hypertension, Bergvall et al. (65) provided evidence that LBW was associated with increased hypertension risk. Although early-life environmental factors are associated with both obesity and hypertension, whether those factors confound the overweight (obesity)-hypertension association is unknown.
Some limitations of this study need to be mentioned. First, we calculated BMI from self-reported height and weight, which could have led to an underestimation of the overweight. Besides, we collected disease information from self-reported questionnaires without measuring the blood pressure. Because of the higher proportion of patients who were not aware of their hypertension (12.3%~24.7%) in the Chinese adults (66, 67), individuals with undiagnosed hypertension might have been misclassified as hypertension-free. Both of those could have led to biased estimation for the overweight-hypertension association. Finally, despite the large sample sizes, the number of cases for stratification analyses was small, especially for the co-twin control analysis. Specifically, we obtained a borderline significant association between obesity and hypertension, due to the limited sample sizes. Thus, further investigations are needed to assess whether the genetics and early-life environmental factors account for this association.
Nonetheless, the current study has several strengths. First, the large nationwide twin cohort allowed us to explore the effects of overweight and obesity on hypertension, and simultaneously estimate the potential influence of genetic and early-life environmental factors in their relationship with sufficient power. We used GEE models, controlling for the clustering of twins within a pair, to provide evidence for the overweight-hypertension association. And further assessing the roles of genetic and familiar factors on the given association, via co-twin case-control design. Second, we only included twins who were diagnosed with hypertension during the follow-up, making the temporality clear and thus minimize the possibility of reverse causality. Third, due to DZ twins only share 50% of their genetic predisposition, co-twin matched case-control analyses including both MZ and DZ twins do not completely control for genetic factors. Therefore, we further repeated co-twin design in MZ and DZ twins separately, which verified our results.
In conclusion, with the current study, we add evidence to the positive link between overweight (obesity) and hypertension, and show the importance of genetic and family environmental factors for their association. That is, due to the common genetic predisposition, individuals with higher BMI seem to be more likely to develop into hypertension. A next step would be to verify our findings in more prospective studies, and find more genes and environments responsible for the overweight (obesity)-hypertension association.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Ethics Committee at Peking University Health Science Center (IRB00001052-11029/14021). The patients/participants provided their written informed consent to participate in this study.
WC and WG contributed to the study design and supervise the whole project. ZP, MY, HW, XPW, ZD, FW, GJ, XJW, YL, JD, and LL contributed to conduct field study and collect the data. KZ, JL, CY, SW, TH, DS, CL, and YP contributed to the results interpretation and provided critical comments. LML helped to design and supervise the whole study and obtain funding. YX analyzed data and drafted the manuscript. All authors contributed to the article and approved the submitted version.
This study was funded by National Natural Science Foundation of China (82073633, 81973126, 81711530051, 81573223, 81473041), and Special Fund for Health Scientific Research in the Public Welfare (201502006, 201002007). The funders had no role in study design and conduct, data collection, analysis and interpretation, preparation of the manuscript, or the decision to publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer XT declared a shared affiliation, with no collaboration, with ZP to the handling editor at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the participants and project staff who took part in the Chinese National Twin Registry for their contributions.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2021.743962/full#supplementary-material
1. GBD 2019 Risk Factors Collaborators. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet (2020) 396(10258):1223–49. doi: 10.1016/S0140-6736(20)30752-2
2. WHO. Hypertension (2019). Available at: https://www.who.int/news-room/fact-sheets/detail/hypertension.
3. WHO. Obesity and Overweight. Available at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
4. Wilson PW, D'Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and Obesity as Determinants of Cardiovascular Risk: The Framingham Experience. Arch Intern Med (2002) 162(16):1867–72. doi: 10.1001/archinte.162.16.1867
5. Moore LL, Visioni AJ, Qureshi MM, Bradlee ML, Ellison RC, D'Agostino R, et al. Weight Loss in Overweight Adults and the Long-Term Risk of Hypertension: The Framingham Study. Arch Intern Med (2005) 165(11):1298–303. doi: 10.1001/archinte.165.11.1298
6. Lyall DM, Celis-Morales C, Ward J, Iliodromiti S, Anderson JJ, Gill JMR, et al. Association of Body Mass Index With Cardiometabolic Disease in the UK Biobank: A Mendelian Randomization Study. JAMA Cardiol (2017) 2(8):882–9. doi: 10.1001/jamacardio.2016.5804
7. Goodarzi MO. Genetics of Obesity: What Genetic Association Studies Have Taught Us About the Biology of Obesity and its Complications. Lancet Diabetes Endocrinol (2018) 6(3):223–36. doi: 10.1016/S2213-8587(17)30200-0
8. Nicolaidis S. Environment and Obesity. Metabolism: Clinical and Experimental (2019) 100S:153942. doi: 10.1016/j.metabol.2019.07.006
9. Pigeyre M, Yazdi FT, Kaur Y, Meyre D. Recent Progress in Genetics, Epigenetics and Metagenomics Unveils the Pathophysiology of Human Obesity. Clin Sci (London Engl 1979) (2016) 130(12):943–86. doi: 10.1042/CS20160136
10. Poulter NR, Prabhakaran D, Caulfield M. Hypertension. Lancet (2015) 386(9995):801–12. doi: 10.1016/S0140-6736(14)61468-9
11. Carey RM, Muntner P, Bosworth HB, Whelton PK. Prevention and Control of Hypertension: JACC Health Promotion Series. J Am Coll Cardiol (2018) 72(11):1278–93. doi: 10.1016/j.jacc.2018.07.008
12. Cowley AW. The Genetic Dissection of Essential Hypertension. Nat Rev Genet (2006) 7(11):829–40. doi: 10.1038/nrg1967
13. Lundqvist E, Kaprio J, Verkasalo PK, Pukkala E, Koskenvuo M, Söderberg KC, et al. Co-Twin Control and Cohort Analyses of Body Mass Index and Height in Relation to Breast, Prostate, Ovarian, Corpus Uteri, Colon and Rectal Cancer Among Swedish and Finnish Twins. Int J Cancer (2007) 121(4):810–8. doi: 10.1002/ijc.22746
14. Xu W, Qiu C, Gatz M, Pedersen NL, Johansson B, Fratiglioni L. Mid- and Late-Life Diabetes in Relation to the Risk of Dementia: A Population-Based Twin Study. Diabetes (2009) 58(1):71–7. doi: 10.2337/db08-0586
15. Gao W, Cao W, Lv J, Yu C, Wu T, Wang S, et al. The Chinese National Twin Registry: A 'Gold Mine' for Scientific Research. J Intern Med (2019) 286(3):299–308. doi: 10.1111/joim.12926
16. Gao W, Li L, Cao W, Zhan S, Lv J, Qin Y, et al. Determination of Zygosity by Questionnaire and Physical Features Comparison in Chinese Adult Twins. Twin Res Hum Genet (2006) 9(2):266–71. doi: 10.1375/183242706776382446
17. Wang B, Gao W, Yu C, Cao W, Lv J, Wang S, et al. Determination of Zygosity in Adult Chinese Twins Using the 450K Methylation Array Versus Questionnaire Data. PloS One (2015) 10(4):e0123992. doi: 10.1371/journal.pone.0123992
18. Zhou B-F. Predictive Values of Body Mass Index and Waist Circumference for Risk Factors of Certain Related Diseases in Chinese Adults–Study on Optimal Cut-Off Points of Body Mass Index and Waist Circumference in Chinese Adults. BioMed Environ Sci (2002) 15(1):83–96
19. Wang S-S, Lay S, Yu H-N, Shen S-R. Dietary Guidelines for Chinese Residents (2016): Comments and Comparisons. J Zhejiang Univ Sci B (2016) 17(9):649–56. doi: 10.1631/jzus.B1600341
20. Gatz M, Svedberg P, Pedersen NL, Mortimer JA, Berg S, Johansson B. Education and the Risk of Alzheimer's Disease: Findings From the Study of Dementia in Swedish Twins. journals gerontology Ser B psychol Sci Soc Sci (2001) 56(5):P292–300. doi: 10.1093/geronb/56.5.p292
21. Xu WL, Atti AR, Gatz M, Pedersen NL, Johansson B, Fratiglioni L. Midlife Overweight and Obesity Increase Late-Life Dementia Risk: A Population-Based Twin Study. Neurology (2011) 76(18):1568–74. doi: 10.1212/WNL.0b013e3182190d09
22. Kato K, Sullivan PF, Evengård B, Pedersen NL. Premorbid Predictors of Chronic Fatigue. Arch Gen Psychiatry (2006) 63(11):1267–72. doi: 10.1002/ijc.31365
23. Bao C, Pedersen NL, Yang R, Marseglia A, Xu W, Wang Y, et al. Diabetes in Midlife and Risk of Cancer in Late Life: A Nationwide Swedish Twin Study. Int J Cancer (2018) 143(4):793–800. doi: 10.1002/ijc.31365
24. Bao C, Yang R, Pedersen NL, Xu W, Xu H, Song R, et al. Overweight in Midlife and Risk of Cancer in Late Life: A Nationwide Swedish Twin Study. Int J Cancer (2019) 144(9):2128–34. doi: 10.1002/ijc.32005
25. Rijsdijk FV, Sham PC. Analytic Approaches to Twin Data Using Structural Equation Models. Brief Bioinform (2002) 3(2):119–33. doi: 10.1093/bib/3.2.119
27. Boker S, Neale M, Maes H, Wilde M, Spiegel M, Brick T, et al. OpenMx: An Open Source Extended Structural Equation Modeling Framework. Psychometrika (2011) 76(2):306–17. doi: 10.1007/s11336-010-9200-6
28. Qi S-F, Zhang B, Wang H-J, Yan J, Du P, Zhang W, et al. Joint Effects of Age and Body Mass Index on the Incidence of Hypertension Subtypes in the China Health and Nutrition Survey: A Cohort Study Over 22years. Prev Med (2016) 89:23–30. doi: 10.1016/j.ypmed.2016.05.004
29. Bastien M, Poirier P, Lemieux I, Després J-P. Overview of Epidemiology and Contribution of Obesity to Cardiovascular Disease. Prog Cardiovasc Dis (2014) 56(4):369–81. doi: 10.1016/j.pcad.2013.10.016
30. Reid IA. Interactions Between ANG II, Sympathetic Nervous System, and Baroreceptor Reflexes in Regulation of Blood Pressure. Am J Physiol (1992) 262(6 Pt 1):E763–78. doi: 10.1152/ajpendo.1992.262.6.E763
31. Engeli S, Negrel R, Sharma AM. Physiology and Pathophysiology of the Adipose Tissue Renin-Angiotensin System. Hypertension (2000) 35(6):1270–7. doi: 10.1161/01.hyp.35.6.1270
32. Alvarez GE, Beske SD, Ballard TP, Davy KP. Sympathetic Neural Activation in Visceral Obesity. Circulation (2002) 106(20):2533–6. doi: 10.1161/01.cir.0000041244.79165.25
33. Grassi G, Seravalle G, Dell'Oro R, Turri C, Bolla GB, Mancia G. Adrenergic and Reflex Abnormalities in Obesity-Related Hypertension. Hypertension (2000) 36(4):538–42. doi: 10.1161/01.hyp.36.4.538
34. Dodt C, Wallin G, Fehm HL, Elam M. The Stress Hormone Adrenocorticotropin Enhances Sympathetic Outflow to the Muscle Vascular Bed in Humans. J Hypertens (1998) 16(2):195–201. doi: 10.1097/00004872-199816020-00010
35. Lee M-R, Lim Y-H, Hong Y-C. Causal Association of Body Mass Index With Hypertension Using a Mendelian Randomization Design. Med (Baltimore) (2018) 97(30):e11252. doi: 10.1097/MD.0000000000011252
36. Li JKY, Ng MCY, So WY, Chiu CKP, Ozaki R, Tong PCY, et al. Phenotypic and Genetic Clustering of Diabetes and Metabolic Syndrome in Chinese Families With Type 2 Diabetes Mellitus. Diabetes Metab Res Rev (2006) 22(1):46–52. doi: 10.1002/dmrr.577
37. Frayling TM, Timpson NJ, Weedon MN, Zeggini E, Freathy RM, Lindgren CM, et al. A Common Variant in the FTO Gene Is Associated With Body Mass Index and Predisposes to Childhood and Adult Obesity. Sci (New York NY) (2007) 316(5826):889–94. doi: 10.1126/science.1141634
38. Xi B, Mi J. Genome-Wide Association Studies of Common Obesity: Now and Future. BioMed Environ Sci (2013) 26(10):787–91. doi: 10.3967/bes2013.001
39. Peng S, Zhu Y, Xu F, Ren X, Li X, Lai M. FTO Gene Polymorphisms and Obesity Risk: A Meta-Analysis. BMC Med (2011) 9:71. doi: 10.1186/1741-7015-9-71
40. Zhao N-N, Dong G-P, Wu W, Wang J-L, Ullah R, Fu J-F. FTO Gene Polymorphisms and Obesity Risk in Chinese Population: A Meta-Analysis. World J Pediatr WJP (2019) 15(4):382–9. doi: 10.1007/s12519-019-00254-2
41. Gerken T, Girard CA, Tung Y-CL, Webby CJ, Saudek V, Hewitson KS, et al. The Obesity-Associated FTO Gene Encodes a 2-Oxoglutarate-Dependent Nucleic Acid Demethylase. Sci (New York NY) (2007) 318(5855):1469–72. doi: 10.1126/science.1151710
42. Schmid PM, Heid I, Buechler C, Steege A, Resch M, Birner C, et al. Expression of Fourteen Novel Obesity-Related Genes in Zucker Diabetic Fatty Rats. Cardiovasc Diabetol (2012) 11:48. doi: 10.1186/1475-2840-11-48
43. Wardle J, Carnell S, Haworth CMA, Farooqi IS, O'Rahilly S, Plomin R. Obesity Associated Genetic Variation in FTO Is Associated With Diminished Satiety. J Clin Endocrinol Metab (2008) 93(9):3640–3. doi: 10.1210/jc.2008-0472
44. Guyenet PG. The Sympathetic Control of Blood Pressure. Nat Rev Neurosci (2006) 7(5):335–46. doi: 10.1038/nrn1902
45. He D, Fu M, Miao S, Hotta K, Chandak GR, Xi B. FTO Gene Variant and Risk of Hypertension: A Meta-Analysis of 57,464 Hypertensive Cases and 41,256 Controls. Metabolism: Clin Exp (2014) 63(5):633–9. doi: 10.1016/j.metabol.2014.02.008
46. Marcadenti A, Fuchs FD, Matte U, Sperb F, Moreira LB, Fuchs SC. Effects of FTO RS9939906 and MC4R RS17782313 on Obesity, Type 2 Diabetes Mellitus and Blood Pressure in Patients With Hypertension. Cardiovasc Diabetol (2013) 12:103. doi: 10.1186/1475-2840-12-103
47. da Silva AA, do Carmo JM, Wang Z, Hall JE. Melanocortin-4 Receptors and Sympathetic Nervous System Activation in Hypertension. Curr Hypertens Rep (2019) 21(6):46. doi: 10.1007/s11906-019-0951-x
48. Lotta LA, Mokrosiński J, Mendes de Oliveira E, Li C, Sharp SJ, Ja L, et al. Human Gain-of-Function MC4R Variants Show Signaling Bias and Protect Against Obesity. Cell (2019) 177(3). doi: 10.1016/j.cell.2019.03.044
49. Pausova Z, Deslauriers B, Gaudet D, Tremblay J, Kotchen TA, Larochelle P, et al. Role of Tumor Necrosis Factor-Alpha Gene Locus in Obesity and Obesity-Associated Hypertension in French Canadians. Hypertension (2000) 36(1):14–9. doi: 10.1161/01.hyp.36.1.14
50. Li Y-y. Tumor Necrosis Factor-Alpha G308α Gene Polymorphism and Essential Hypertension: A Meta-Analysis Involving 2244 Participants. PloS One (2012) 7(4):e35408. doi: 10.1371/journal.pone.0035408
51. Yao Y-S, Chang W-W, Jin Y-L. Association Between TNF-A Promoter -308G/A Polymorphism and Essential Hypertension in the Asian Population: A Meta-Analysis. J Renin-Angiotensin-Aldosterone System JRAAS (2017) 18(4):1470320317741066. doi: 10.1177/1470320317741066
52. Li Y-X, Zhang Q, Shang X-M, Li Y-Q, Liu X-K, Liu C-Q, et al. Association of Two Well-Defined Polymorphisms in Leptin and Leptin Receptor Genes With Hypertension and Circulating Leptin: A Meta-Analysis. Arch Med Res (2015) 46(1):38–46. doi: 10.1016/j.arcmed.2014.11.012
53. Kilpeläinen TO, Carli JFM, Skowronski AA, Sun Q, Kriebel J, Feitosa MF, et al. Genome-Wide Meta-Analysis Uncovers Novel Loci Influencing Circulating Leptin Levels. Nat Commun (2016) 7:10494. doi: 10.1038/ncomms10494
54. de Luis DA, Perez Castrillón JL, Dueñas A. Leptin and Obesity. Minerva Med (2009) 100(3):229–36.
55. Pan WW, Myers MG. Leptin and the Maintenance of Elevated Body Weight. Nat Rev Neurosci (2018) 19(2):95–105. doi: 10.1038/nrn.2017.168
56. Gu P, Jiang W, Chen M, Lu B, Shao J, Du H, et al. Association of Leptin Receptor Gene Polymorphisms and Essential Hypertension in a Chinese Population. J Endocrinological Invest (2012) 35(9):859–65. doi: 10.3275/8238
57. Daghestani MH, Warsy A, Daghestani MH, Al-Odaib AN, Eldali A, Al-Eisa NA, et al. Arginine 16 Glycine Polymorphism in β2-Adrenergic Receptor Gene is Associated With Obesity, Hyperlipidemia, Hyperleptinemia, and Insulin Resistance in Saudis. Int J Endocrinol (2012) 2012:945608. doi: 10.1155/2012/945608
58. Gjesing AP, Andersen G, Burgdorf KS, Borch-Johnsen K, Jørgensen T, Hansen T, et al. Studies of the Associations Between Functional Beta2-Adrenergic Receptor Variants and Obesity, Hypertension and Type 2 Diabetes in 7,808 White Subjects. Diabetologia (2007) 50(3):563–8. doi: 10.1007/s00125-006-0578-8
59. Johnsson IW, Haglund B, Ahlsson F, Gustafsson J. A High Birth Weight is Associated With Increased Risk of Type 2 Diabetes and Obesity. Pediatr Obes (2015) 10(2):77–83. doi: 10.1111/ijpo.230
60. Zhao Y, Wang S-F, Mu M, Sheng J. Birth Weight and Overweight/Obesity in Adults: A Meta-Analysis. Eur J Pediatr (2012) 171(12):1737–46. doi: 10.1007/s00431-012-1701-0
61. Derraik JGB, Maessen SE, Gibbins JD, Cutfield WS, Lundgren M, Ahlsson F. Large-for-Gestational-Age Phenotypes and Obesity Risk in Adulthood: A Study of 195,936 Women. Sci Rep (2020) 10(1):2157. doi: 10.1038/s41598-020-58827-5
62. Knop MR, Geng T-T, Gorny AW, Ding R, Li C, Ley SH, et al. Birth Weight and Risk of Type 2 Diabetes Mellitus, Cardiovascular Disease, and Hypertension in Adults: A Meta-Analysis of 7 646 267 Participants From 135 Studies. J Am Heart Assoc (2018) 7(23):e008870. doi: 10.1161/JAHA.118.008870
63. Xia Q, Cai H, Xiang Y-B, Zhou P, Li H, Yang G, et al. Prospective Cohort Studies of Birth Weight and Risk of Obesity, Diabetes, and Hypertension in Adulthood Among the Chinese Population. J Diabetes (2019) 11(1):55–64. doi: 10.1111/1753-0407.12800
64. Tian J-Y, Cheng Q, Song X-M, Li G, Jiang G-X, Gu Y-Y, et al. Birth Weight and Risk of Type 2 Diabetes, Abdominal Obesity and Hypertension Among Chinese Adults. Eur J Endocrinol (2006) 155(4):601–7. doi: 10.1530/eje.1.02265
65. Bergvall N, Iliadou A, Johansson S, de Faire U, Kramer MS, Pawitan Y, et al. Genetic and Shared Environmental Factors do Not Confound the Association Between Birth Weight and Hypertension: A Study Among Swedish Twins. Circulation (2007) 115(23):2931–8. doi: 10.1161/CIRCULATIONAHA.106.674812
66. Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, et al. Status of Hypertension in China: Results From the China Hypertension Survey, 2012-2015. Circulation (2018) 137(22):2344–56. doi: 10.1161/CIRCULATIONAHA.117.032380
67. Lu J, Lu Y, Wang X, Li X, Linderman GC, Wu C, et al. Prevalence, Awareness, Treatment, and Control of Hypertension in China: Data From 1·7 Million Adults in a Population-Based Screening Study (China PEACE Million Persons Project). Lancet (2017) 390(10112):2549–58. doi: 10.1016/S0140-6736(17)32478-9
Keywords: BMI, hypertension, genetics, early-life environments, twin study
Citation: Xi Y, Gao W, Zheng K, Lv J, Yu C, Wang S, Huang T, Sun D, Liao C, Pang Y, Pang Z, Yu M, Wang H, Wu X, Dong Z, Wu F, Jiang G, Wang X, Liu Y, Deng J, Lu L, Cao W and Li L (2021) The Roles of Genetic and Early-Life Environmental Factors in the Association Between Overweight or Obesity and Hypertension: A Population-Based Twin Study. Front. Endocrinol. 12:743962. doi: 10.3389/fendo.2021.743962
Received: 19 July 2021; Accepted: 15 September 2021;
Published: 05 October 2021.
Edited by:
Patricia Khashayar, Ghent University, BelgiumReviewed by:
Xiaocao Tian, Qingdao Municipal Center for Disease Control and Prevention, ChinaCopyright © 2021 Xi, Gao, Zheng, Lv, Yu, Wang, Huang, Sun, Liao, Pang, Pang, Yu, Wang, Wu, Dong, Wu, Jiang, Wang, Liu, Deng, Lu, Cao and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenjing Gao, cGt1ZXBpZ3dqQDEyNi5jb20=; Weihua Cao, Y2Fvd2VpaHVhNjBAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.