 Rivak Punchoo
Rivak Punchoo Sachin Bhoora
Sachin Bhoora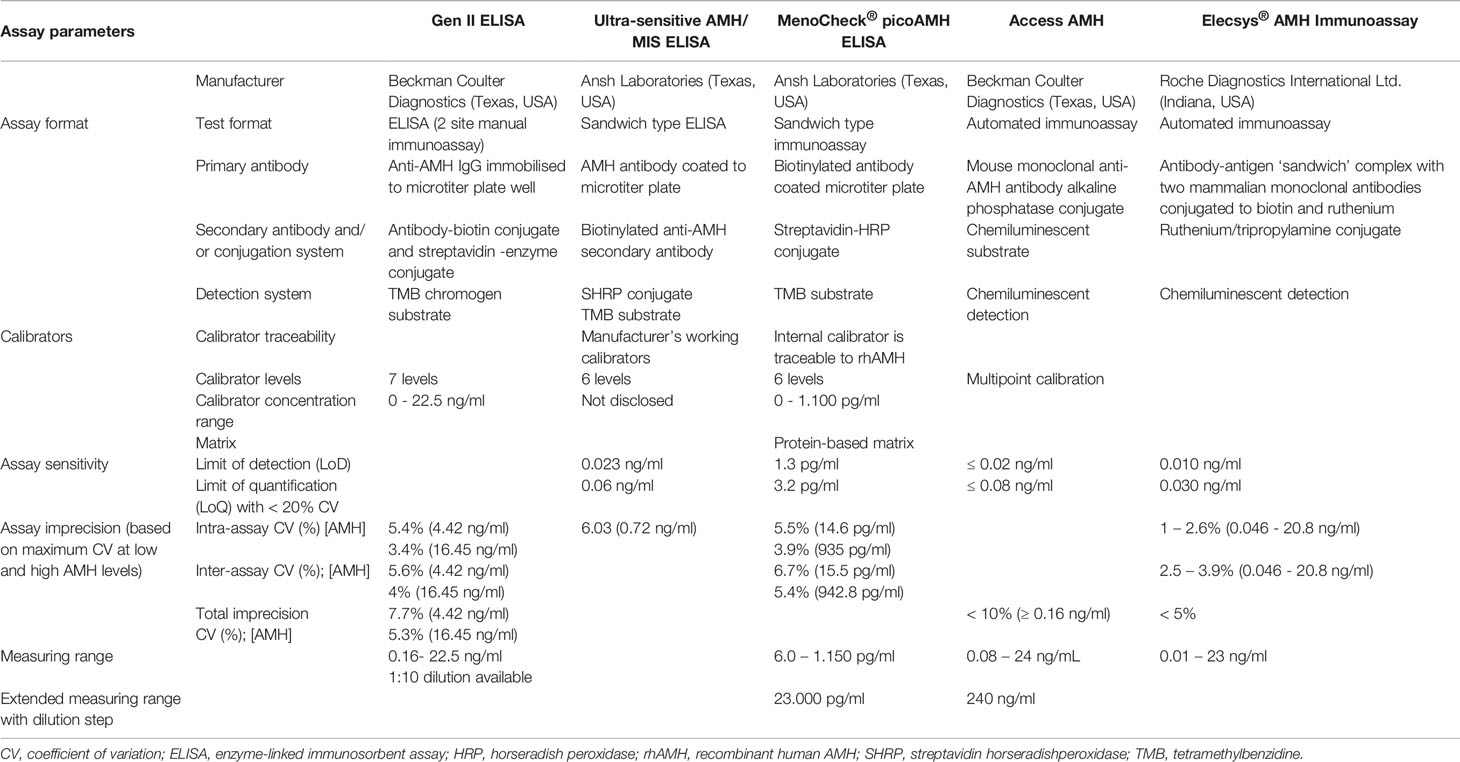

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Endocrinol. , 03 September 2021
Sec. Reproduction
Volume 12 - 2021 | https://doi.org/10.3389/fendo.2021.719029
Anti-Müllerian Hormone (AMH) is a 140 kDa homodimeric glycoprotein consisting of two identical subunits linked by disulphide bonds and is synthesised by the testes and ovaries. Its clinical applications are prediction of ovarian response and gonadotropin dose selection upon in vitro fertilization. In males, AMH is used to investigate sexual developmental disorders and gonadal function. AMH is commonly assayed by enzyme-linked immunosorbent assay or automated immunoassay formats that show variation between methods. This review applies fundamental chemical pathology concepts to explain the observed analytical variation of AMH measurement. We examine the lack of standardisation between AMH assays, the impact of antibody design on variable measurements, consider the analytical detection of AMH isoforms, review analytical interference in AMH measurement, and briefly assess systematic bias between AMH assays. The improved attempt at standardising AMH measurement by the recent approval of a WHO Reference Reagent offers promise for harmonising immunoassay results and establishing consensus medical cut-off points for AMH in disease. Standardisation, however, will need to redress the issue of poor commutability of standard reference material and further assign a standard reference procedure to quantify AMH standard reference material. The improvement of the analytical phase of AMH testing will support harmonised method development and patient care.
Müllerian Inhibiting Substance (MIS), also known as Anti-Müllerian Hormone (AMH), is a dimeric glycoprotein that is a member of the transforming growth factor-beta superfamily (1). AMH is synthesised by Sertoli and granulosa cells of the testes and ovaries, respectively (2). AMH regulates antral follicles in the human ovary before final selection and is the gatekeeper of follicular oestrogen production and selection of the dominant follicle that will undergo ovulation (3, 4). In the testes, AMH production triggers the regression of Müellerian ducts in the male foetus and is also involved in testicular development and function (5).
The clinical applications of AMH are ovarian reserve testing (6), prediction of ovarian response after controlled ovarian stimulation, prediction of the menopause onset, monitoring of ovarian effects of medication and surgical procedures, and evaluating the risk of a variety of ovarian disorders, for example, polycystic ovary disease and primary ovarian failure (7). It is also used in the investigation of male sexual developmental disorders and gonadal function.
Clinical applications require analysis along an analytical range that can accommodate accurate and reliable measurement at high and low levels of the reference interval to enable accurate diagnosis and disease monitoring. Currently, multiple immunoassays are available to quantify AMH and variability in measuring AMH is commonly reported (6, 8).
An electronic literature search was performed for the present review using PubMed and Google Scholar databases. The search terms used were: “AMH”, “MIS”, “Measurement”, “Method comparison”, “Method evaluation”, “Analytical interference”. The inclusion criteria were studies related to humans and studies which investigated AMH measurement. The exclusion criteria were articles for which full text was not available, not written in English, were grey literature, or original articles published before the last 20 years. Core textbooks in chemical pathology prescribed by the College of Medicine of South Africa were also consulted. Studies retrieved from initial searches were supplemented with additional references that were identified by manual search among the cited references.
This review will examine issues that account for variation in serum AMH measurement, emphasising the analytical phase of the total testing laboratory process. Basic concepts in chemical pathology that underly measurement variation of AMH will also be explained to provide non-laboratory trained readers with essential laboratory knowledge to rationalise the observed variations in AMH measurement. The critical issues we will explore are standardisation of AMH assays, antibody design and detection employed in AMH measurement, analytical interference, limits of detection for manual and automated AMH testing, and systematic error between AMH assays.
The measurement of AMH immunoassays has evolved over the last two decades. Assay formulations have utilized various calibrators and antibody pairs for quantification of AMH. Consequently, the bias, imprecision, and limit of detection (LoD) demonstrate variability. Newer assays utilize automated formats with improved analytical sensitivity. Table 1 summarizes key analytical characteristics of current assays commonly utilized for AMH measurement.
Immunoassays, including enzyme-linked immunosorbent assay (ELISA) format, are calibrated by defined analyte material (calibrators) to allow quantification of analyte concentration in unknown patient samples and quality control materials (14). A calibration curve can be constructed for both manual and automated immunoassays using manufacturer-assigned values to calibrators. Multiple calibrators (two or more) are used to establish a dynamic range of measurement from low to high concentration levels, which span relevant medical decision points. Therefore, the standard curve defines the assay’s measuring range and links the concentration and signal output of the calibrators to the analytical signal from unknown samples or controls. Patients’ samples and control material are quantified by extrapolating the assay signal to the concentration using a calibration curve (or its straight-line equation). A concentration value is then assigned to the unknown sample. The use of a reference procedure and reference material defines the metrological principle of standardisation. It links the patient’s test result to the pure material, ensuring a line of traceability (14–16).
AMH measurement suffers from variable assay standardisation between commercial immunoassays (8, 17). Manufacturers of AMH assays have used assay-defined proprietary calibrators derived from various sources with variably assigned values. This causes variation of standard curves between AMH assays and has contributed to the observed variation of AMH measurement by immunoassays. Reference material either from the International Standards by the WHO or Standard Reference Materials (SRM) certified by the National Institute of Standards and Technology (NIST) exist only for a limited number of measurands. This is because standardisation is expensive, demanding human resources and onerous to establish as it consists of multi-stage processes. The designation of appropriate higher-order methods to quantify pure standard material enables manufacturers to assign values to their calibrators. Thus patients results are directly traceable to the high order reference material (15).
The establishment of an international standard to calibrate AMH immunoassays will enable harmonisation of AMH testing across multiple commercial assays, standardise proficiency testing schemes, allow clinical laboratories to calibrate and control immunoassays, and support continued research and development in the measurement of AMH. The WHO Expert Committee approved the development of an international standard for AMH immunoassays in 2014. Recombinant AMH trial preparation SS-581 showed stability in lyophilised form and retained biological activity in the Müllerian duct regression assay (17).
Following on this study, a stable, lyophilised preparation of recombinant, CHO-derived AMH, encoded 16/190, was assessed by a collaborative international panel by multiple AMH immunoassays (18). Most assays detected the AMH preparation; however, unsurprisingly, considerable variation between assays was noted, ascribed to the variable method calibrators used by the individual assays. The various manufacturer calibrators are derived from native, recombinant, and non-human sources. Some assays exhibited low variability of AMH content in a comparator sample to the 16/190 preparation content estimate. The WHO assigned a mass to 16/190 based on a mean consensus amongst agreeable immunoassays.
The commutability of the AMH 16/190 material, however, was unsatisfactory. Commutability is a property of reference material that describes the equivalence of the mathematical relationships between the results of different measurement procedures for reference material and representative samples from healthy and diseased individuals (19, 20). Thus, for routine diagnostic laboratories, commutability requires validation across all assays and methods that use the reference material. This ensures that patients’ results by routine measurement procedures, for example, AMH measured by automated or manual immunoassays, have equivalent values regardless of the AMH immunoassay used for the measurement. Commutability is, therefore, an essential requirement when a reference material is to be used as a common calibrator for clinical laboratory assays or in proficiency testing schemes or by commercial manufacturers as part of their internal traceability procedures to assign value to their product calibrators. Ultimately, commutability allows evaluation of the agreement amongst various measuring procedures of patient results. As commutability was unsatisfactory for 16/190, the WHO approved 16/190 as a WHO Reference Reagent, rather than as “full” WHO International Standard (18). The reasons for poor commutability include the lack of inclusion of all AMH isoforms in the 16/190 preparation, variable epitope recognition of 16/190 by immunoassay antibodies between methods in the study, and poor alignment of the non-human protein matrix of 16/190 with serum.
Furthermore, until a physicochemical reference method becomes available, the AMH content of 16/190 will be defined as 489 ng/ampoule, which is the mean of the estimates from a subset of valid AMH immunoassays (18). This assignment is an essential step in moving to a fully standardised reference material and reference measurement procedure for AMH measurement. In the interim, the international reagent preparation will assist commercial AMH manufacturers in re-evaluating the assignment of manufacturer calibrator values and improving harmonised comparisons between AMH immunoassays.
AMH is synthesised as a precursor hormone with a signal sequence followed by the pre-hormone segment (pro-AMH). AMH contains two cleavage sites at amino acid 229 and 451 and, when cleaved, forms a family of AMH isoforms. Proteolysis of pro-AMH results in the formation of a 58 kDa N-terminal “pro-region” domain (AMHN), and a biologically active 12.5kDa “mature” C-terminal domain (AMHC). Each 70 kDa homodimer dimerises and is linked non-covalently by disulphide bonds to form the 140 kDa AMHN,C hormone, which is glycosylated and secreted (21, 22). Commercial AMH assays target various parts of the AMH hormone. Capture and detection antibodies of ELISAs are assay-specific and, for example, target mature region and pro-region of AMH (16).
Biological activity is attributed to AMHC and AMHN,C isoforms. AMH-C-terminal homodimer is less active than the non-covalent complex. Restoration of the activity is achieved by associating the C-terminal homodimer with the N-terminal homodimer implying that the N-terminal domain functionally amplifies the C-terminal domain. This suggests that the AMH isoforms possess differential biological activity. The AMH non-covalent complex represents the most potent bioactive form of AMH, which can bind optimally to AMH receptor II (AMHRII) (23–26).
Detection of inactive, partially active, and fully active measurands by non-specific antibodies increase total measurand concentration and produces false positive results. The ratios of circulating AMH isoforms are incompletely elucidated. Biologically inactive pro-AMH and bioactive dimerised AMHN,C are both detected in blood circulation by current AMH immunoassay technology (6, 27). The quantification of total serum AMH thus represents a summation of biologically active and inactive isoforms. Therefore, the total AMH laboratory result may spuriously suggest an increased bioactive fraction of AMH that may potentially misclassify patients’ clinical states.
Antibodies are proprietary showing differential sensitivity and specificity to detect AMH isoforms in disease. The capture and detection antibodies in ELISA target unique epitopes on AMH. Therefore, the manufacturer’s specification of which isoforms are being measured will accurately estimate active AMH.
In addition, the proportion of isoforms may also vary between diseases, which will affect the quantification of total AMH. However, studies analysing the ratio of different isoforms in gonadal pathology and in healthy state are required to inform advocating selective assays to measure specific circulating isoforms (28, 29). Post-translational modification of AMH in disease needs clarification. Using the Ansh lab manual ELISA, proAMH in normo-ovulatory women was shown to constitute 3% of promature AMH (proAMH + AMHN,C) and similar studies exploring isoform detection is required (28).
Furthermore, various assay matrices, for example, with varied pH and ionic concentration, can alter the 3-dimensional structure of AMH isoforms and their detection. The assay matrix may also then influence AMH measurement. Therefore, isoforms in an assay-specific serum matrix for calibrators is crucial to reduce AMH measurement variation (6).
The evolution of antibody design for the detection of AMH from the 1990s to the present time shows changes in two areas, viz clonal selection of antibodies and variable AMH antigenic material used to raise antibodies. Furthermore, the changing demand of AMH clinical utility from a marker of testicular function to the assessment of ovarian function, ovarian reserve and disease has demanded improved limit of detection for AMH in females. This has necessitated the re-design of capture and detection antibodies for AMH immunoassays.
The various antibodies used have impacted test sensitivity. For instance, early immunoassays used polyclonal and monoclonal antibodies against the pro-AMH region of recombinant human AMH (rhAMH) and/or bovine AMH, achieving sensitivities of 0.5 ng/ml – 6.25 ng/ml (30, 31). Later ELISA tests detected total AMH by raising polyclonal and/or monoclonal antibodies to rhAMH. The capture and detection antibodies were raised against the pro-AMH and the mature regions of AMH, and therefore able to detect total AMH. The IOT assay sensitivity for the monoclonal antibody pair was 0.1 ng/ml (32) in comparison to the assay utilising a combination of monoclonal and polyclonal antibodies, and the limit of detection was 2 ng/ml (33).
In a cross-sectional study comparing AMH levels among three commercially available AMH immunoassays (AMH Gen II, Beckman Coulter; Ultrasensitive AMH, AnshLab; and picoAMH, AnshLab), significantly higher proportions of detectable AMH levels were observed with the picoAMH assay (97%) and Ultrasensitive AMH assay (92%) compared to Gen II assay (84%) (34). The AnshLab utilises similar antibody pairs for both its ELISA tests compared to Gen II assay, and antibody selection may contribute to the observed differences.
The continued development of antibody design for ELISAs for glycoprotein hormones will need to consider variation in specificity, cross-reactivities, epitope locations (35) and clinical application. Achieving agreement about relevant biological AMH isoforms will improve the specificity of AMH detection and the inter-assay agreement. Knowledge of antibody specificity will enable targeting equimolar detection of AMH isoforms; however, sharing proprietary antibody pairings is challenging but would undoubtedly standardise medical decision cut-off points.
Immunoassays suffer analytical interference from a broad range of sources, including heterophile antibodies, human anti-animal antibodies, serum proteins (e.g. rheumatoid factor, binding proteins), drugs and drug metabolites, and abnormal serum indices (e.g. haemolysis, lipaemia and hyperproteinaemia). The laboratory usually flags significant interference; however, low-level interference may be undetected and adversely affect test interpretation (36–38). As AMH is run only on immunoassay format, it is susceptible to varied analytical interference.
The use of biotin-streptavidin-based immunoassays has demonstrated positive and negative analytical interference in competitive and non-competitive sandwich immunoassays, respectively (39, 40). Many AMH assays use biotin-streptavidin based measurement and are at risk for this type of interference. Platforms that use alternative methods of antigen capture do not show this analytical interference (40, 41). Manufacturers’ instructions on maximum tolerable concentrations of in vivo biotin levels, guidelines on biotin supplementation and time-to-sample interval, re-formulation of biochemical assays, and studies investigating biotin interference have collectively improved biotin immunoassay interference.
Complement levels can interfere with AMH measurement. The unmodified AMH Gen II produced erroneously low AMH concentrations, especially in fresh patient samples. The interference resulted from the binding of C1q to the capture antibody IgG2a and subsequently activating the complement cascade and c3b deposition, causing steric hindrance preventing AMH-binding to the capture antibody (42). This interaction was favoured by the assay matrix, which allowed complement activation and by the use of a capture antibody that strongly activated complement. Introducing a pre-dilution step to the revised version of AMH Gen II improved complement interference, although it may cause positive bias (43). Interestingly, the automated Beckman Access and Roche Elecsys AMH assays are not affected by complement interference despite using the same antibody pairs as the Beckman AMH Gen II assay (40–42).
The improvement in assay imprecision and LoD has evolved with newer automated AMH assays. These automated immunoassays also utilise chemiluminescent detection, which increases the assay sensitivity and permits low-level AMH detection. For example, Elecys® AMH Immunoassay (Roche Diagnostics International Ltd, Indiana, USA) and the Access AMH assay (Beckman-Coulter Diagnostics (USA) demonstrate respective LoD of 0.01 ng/ml and 0.02 ng/ml (11, 13).
Using proficiency testing material quantified by ten laboratories by the AMH GenII ELISA over a 15-month scheme, the within-laboratory reproducibility was good; however, the between laboratory variability showed a wide range of average values compared to the consensus mean (-24.0% to +22.7%) (44) emphasising inter-laboratory imprecision of manual ELISA testing. Manufacturer data also identifies a broader imprecision of intra-assay and inter-assay CVs for the AMH GenII ELISA (≤5.4% and ≤5.6%) compared to automated assays: Access AMH (≤1.7% and ≤2.8%) and Elecsys AMH Immunoassay (≤2.6% and ≤3.9%) (11, 13). The Ansh Lab’s picoAMH ELISA has CVs above >5%; however, their Ultra-Sensitive ELISA has CVs <5% (10, 12). It is not surprising that manual ELISA assays are generally less precise as the multi-step human handling requires pipetting small volumes, performing multiple wash steps and carefully timing incubations.
The superior analytical performance of automated assays is especially valuable at fixed cut-off medical decision points to avoid misclassification. For example, patients who receive ovarian stimulation have binary clinical response cut-off points of ≤0.75ng/ml and ≥3.50 ng/ml that identify low and high responses to stimulation (45). The increased detection limits and sensitivity of automated assays allow the determination of AMH at low concentrations. This is illustrated by comparison laboratory evaluation data between the AMH Gen II ELISA assay and the Elecys® AMH assay in orthotopic transplantation of ovarian tissue after gonadotoxic treatment (46). The enhanced analytical performance of automated assays can also benefit tumour marker applications, such as detecting recurrence of granulosa cell ovarian tumours (47–49).
The total analytical error, which accounts for variability between AMH assays, is derived from a summation of random error and systematic error. Random error is unpredictable and can be derived from various sources during the performance of the test in a laboratory, for example, incorrect aspiration of sample volume by automated or manual AMH assays. Random error contributes to the imprecision of an assay expressed mathematically by the coefficient of variation (CV). High CV values indicate wider imprecision and are less desired for an assay. In contrast, systematic error provides a measure of accuracy (bias) and is further subdivided into contributions from a constant error component and a proportional error component. Constant error is independent of the measurand concentration, and proportional error varies with the concentration of the analyte being measured. Statistical regression methods between two assays quantify slope (proportional error) and y-intercept (constant error). The correlation coefficient (R2) indicates the closeness of the sample data points to the regression line and provides a measure of random error. A perfect comparison between two assays is a slope = 1, y-intercept = 0 and a R2 = 1 (15, 50).
Assay-specific calibrators can reveal systematic error between methods in a method comparison study. The bias of an assay expresses the sample’s value relative to a true value and provides a measure of accuracy between the comparator and reference method. A bias of 0%, for example, indicates that there is a complete agreement of sample measurement between two different assays. Table 2 summarizes method comparison studies for AMH measurement. In general, these studies demonstrate variability in measurement between AMH assays. Furthermore, the importance of developing high order reference procedures and an international reference material is foregrounded to enable medical laboratories to establish a chain of analytical traceability from the patient’s result back to the primary reference material.
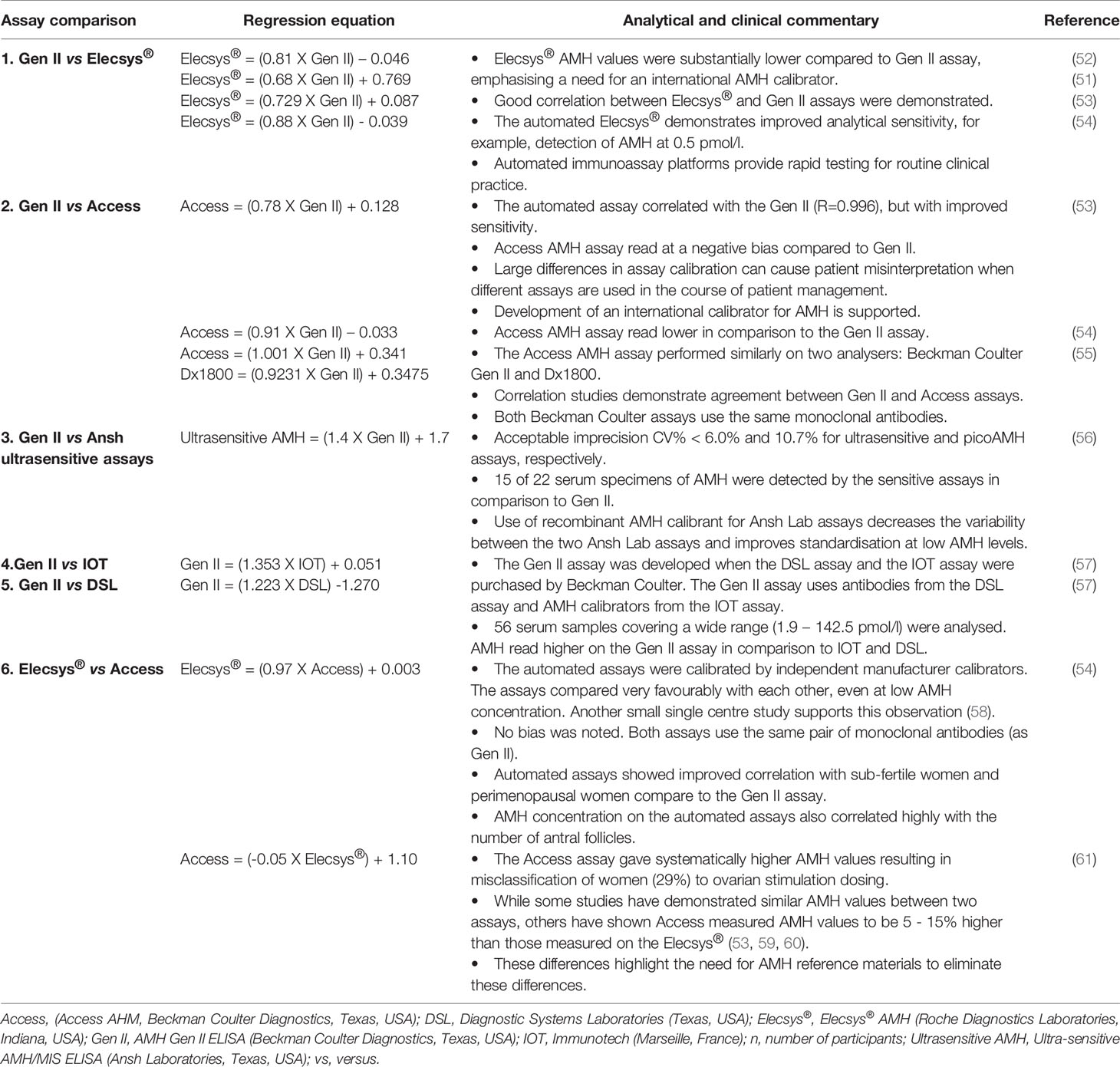
Table 2 Method comparison evaluations between commercial AMH assays.
Comparative assay studies on the workhorse AMH GenII ELISA (reference assay) and comparator assays (Access and Elecys®) demonstrate variation. Regression analysis showed slopes between 0.68 and 1, and y-intercepts between -0.039 and +0.769, respectively, in the method comparison studies implicating significant systematic error variation between the assays (51, 53–55, 62). Furthermore, based on cut-off medical decision points at concentrations of 1 ng/ml and 5 ng/ml, biases were calculated using regression equations derived from seven assay comparison studies that assessed performance between manual and automated assays. Biases between -25.2% and + 45% were noted between Gen II and the Elecsys® assay, and biases of between -9% to +34% were identified between Gen II and the Access assay (6). Systematic error in AMH assays contributes to assay variability and can be detected by method comparison studies of AMH assays.
AMH between-method variability can be ascribed to various processes in the analytical phase of testing. The most significant contributor is the lack of international standardised material to ensure uniform calibration. To this end, the assignment of a WHO Reference Reagent is promising in improving comparability between assays. Other factors that influence inter-assay variation include antibody design with variable specificity, incomplete knowledge about which isoform to measure, and method vulnerability to analytical interferences. Future improvement at the analytical phase of testing for AMH will support the safe establishment of comparable medical decision cut-off points between AMH immunoassays.
RP conceived the idea for this article. RP and SB conducted the literature search and drafted the manuscript. Both authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cate RL, Mattaliano RJ, Hession C, Tizard R, Farber NM, Cheung A, et al. Isolation of the Bovine and Human Genes for Müllerian Inhibiting Substance and Expression of the Human Gene in Animal Cells. Cell (1986) 45(5):685–98. doi: 10.1016/0092-8674(86)90783-X
2. Jeppesen JV, Anderson RA, Kelsey TW, Christiansen SL, Kristensen SG, Jayaprakasan K, et al. Which Follicles Make the Most Anti-Mullerian Hormone in Humans? Evidence for an Abrupt Decline in AMH Production at the Time of Follicle Selection. Mol Hum Reprod (2013) 19(8):519–27. doi: 10.1093/molehr/gat024
3. van Houten EL, Themmen AP, Visser JA. Anti-Müllerian Hormone (AMH): Regulator and Marker of Ovarian Function. Ann Endocrinol (Paris) (2010) 71(3):191–7. doi: 10.1016/j.ando.2010.02.016
4. Tal R, Seifer DB. Ovarian Reserve Testing: A User's Guide. Am J Obstet Gynecol (2017) 217(2):129–40. doi: 10.1016/j.ajog.2017.02.027
5. Matuszczak E, Hermanowicz A, Komarowska M, Debek W. Serum AMH in Physiology and Pathology of Male Gonads. Int J Endocrinol (2013) 2013:128907. doi: 10.1155/2013/128907
6. Moolhuijsen LME, Visser JA. Anti-Müllerian Hormone and Ovarian Reserve: Update on Assessing Ovarian Function. J Clin Endocrinol Metab (2020) 105(11):3361–73. doi: 10.1210/clinem/dgaa513
7. Leader B, Baker VL. Maximizing the Clinical Utility of Antimüllerian Hormone Testing in Women's Health. Curr Opin Obstet Gynecol (2014) 26(4):226–36. doi: 10.1097/GCO.0000000000000087
8. Dewailly D, Andersen CY, Balen A, Broekmans F, Dilaver N, Fanchin R, et al. The Physiology and Clinical Utility of Anti-Mullerian Hormone in Women. Hum Reprod Update (2014) 20(3):370–85. doi: 10.1093/humupd/dmt062
9. AMH Gen II ELISA. Beckman Coulter (2009). Available at: http://biowel.com/pdf/Kit%20Insert%20A79758C-03.pdf.
10. Ultra-Sensitive AMH/MIS Webster. TX: Ansh Labs (2014). Available at: https://www.anshlabs.com/wp-content/uploads/inserts/AL105.pdf.
11. Access Anti-Müllerian Hormone (AMH). Beckman Coulter (2017). Available at: https://www.beckmancoulter.com/wsrportal/techdocs?docname=/cis/b15676/a/Access%20AMH_B15676-A_English.pdf.
12. Meno-Check® picoAMH ELISA Webster. TX: Ansh Labs (2018). Available at: https://www.anshlabs.com/wp-content/uploads/inserts/AL124.pdf.
13. Elecsys® AMH (Anti-Mullerian Hormone). Roche Diagnostics (2021). Available at: https://diagnostics.roche.com/global/en/products/params/elecsys-amh-anti-mullerian-hormone.html.
14. Porstmann T, Kiessig ST. Enzyme Immunoassay Techniques. An Overview. J Immunol Methods (1992) 150(1-2):5–21. doi: 10.1016/0022-1759(92)90061-W
15. Miller GW, Sandberg S. Quality Control of the Analytical Examination Process. In: Rifai N, editor. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 6 ed. St. Louis, Mo: Elsevier (2018).
16. The Complete ELISA Guide. Abcam (2021). Available at: https://www.abcam.com/protocols/the-complete-elisa-guide.
17. Ferguson JM, Pépin D, Duru C, Matejtschuk P, Donahoe PK, Burns CJ. Towards International Standardization of Immunoassays for Müllerian Inhibiting Substance/Anti-Müllerian Hormone. Reprod BioMed Online (2018) 37(5):631–40. doi: 10.1016/j.rbmo.2018.08.012
18. Ferguson J, Hockley J, Rigsby P, Burns C. Establishment of a WHO Reference Reagent for Anti-Mullerian Hormone. Reprod Biol Endocrinol (2020) 18(1):86. doi: 10.1186/s12958-020-00641-9
19. International Organisation for Standardization (ISO). In Vitro Diagnostic Medical Devices — Measurement of Quantities in Samples of Biological Origin — Description of Reference Materials. Geneva, Switzerland: ISO (2002). p. 15194.
20. International Organisation for Standardization (ISO). In Vitro Diagnostic Medical Devices — Measurement of Quantities in Biological Samples — Metrological Traceability of Values Assigned to Calibrators and Control Materials. ISO 17511. Geneva, Switzerland: ISO (2003).
21. Nelson SM, La Marca A. The Journey From the Old to the New AMH Assay: How to Avoid Getting Lost in the Values. Reprod BioMed Online (2011) 23(4):411–20. doi: 10.1016/j.rbmo.2011.06.011
22. Lee MM, Donahoe PK. Mullerian Inhibiting Substance: A Gonadal Hormone With Multiple Functions. Endocr Rev (1993) 14(2):152–64. doi: 10.1210/edrv-14-2-152
23. Donahoe PK. Müllerian Inhibiting Substance in Reproduction and Cancer. Mol Reprod Dev (1992) 32(2):168–72. doi: 10.1002/mrd.1080320213
24. Nachtigal MW, Ingraham HA. Bioactivation of Müllerian Inhibiting Substance During Gonadal Development by a Kex2/Subtilisin-Like Endoprotease. Proc Natl Acad Sci USA (1996) 93(15):7711–6. doi: 10.1073/pnas.93.15.7711
25. Pepinsky RB, Sinclair LK, Chow EP, Mattaliano RJ, Manganaro TF, Donahoe PK, et al. Proteolytic Processing of Mullerian Inhibiting Substance Produces a Transforming Growth Factor-Beta-Like Fragment. J Biol Chem (1988) 263(35):18961–4. doi: 10.1016/S0021-9258(18)37375-7
26. di Clemente N, Jamin SP, Lugovskoy A, Carmillo P, Ehrenfels C, Picard JY, et al. Processing of Anti-Mullerian Hormone Regulates Receptor Activation by a Mechanism Distinct From TGF-Beta. Mol Endocrinol (Baltimore Md) (2010) 24(11):2193–206. doi: 10.1210/me.2010-0273
27. Pankhurst MW, McLennan IS. Human Blood Contains Both the Uncleaved Precursor of Anti-Mullerian Hormone and a Complex of the NH2- and COOH-Terminal Peptides. Am J Physiol Endocrinol Metab (2013) 305(10):E1241–7. doi: 10.1152/ajpendo.00395.2013
28. Wissing ML, Mikkelsen AL, Kumar A, Kalra B, Pors SE, Flachs EM, et al. Associations of Different Molecular Forms of Antimüllerian Hormone and Biomarkers of Polycystic Ovary Syndrome and Normal Women. Fertil Steril (2019) 112(1):149–55.e1. doi: 10.1016/j.fertnstert.2019.03.002
29. La Marca A. Ovarian AntimüLlerian Hormone System: More Complex Than was Thought. Fertil Steril (2019) 112(1):42–3. doi: 10.1016/j.fertnstert.2019.04.042
30. Baker ML, Metcalfe SA, Hutson JM. Serum Levels of Müllerian Inhibiting Substance in Boys From Birth to 18 Years, as Determined by Enzyme Immunoassay. J Clin Endocrinol Metab (1990) 70(1):11–5. doi: 10.1210/jcem-70-1-11
31. Hudson PL, Dougas I, Donahoe PK, Cate RL, Epstein J, Pepinsky RB, et al. An Immunoassay to Detect Human Müllerian Inhibiting Substance in Males and Females During Normal Development. J Clin Endocrinol Metab (1990) 70(1):16–22. doi: 10.1210/jcem-70-1-16
32. Long WQ, Ranchin V, Pautier P, Belville C, Denizot P, Cailla H, et al. Detection of Minimal Levels of Serum Anti-Müllerian Hormone During Follow-Up of Patients With Ovarian Granulosa Cell Tumor by Means of a Highly Sensitive Enzyme-Linked Immunosorbent Assay. J Clin Endocrinol Metab (2000) 85(2):540–4. doi: 10.1210/jcem.85.2.6378
33. Carré-Eusèbe D, Imbeaud S, Harbison M, New MI, Josso N, Picard JY. Variants of the Anti-Müllerian Hormone Gene in a Compound Heterozygote With the Persistent Müllerian Duct Syndrome and His Family. Hum Genet (1992) 90(4):389–94. doi: 10.1007/BF00220465
34. Su HI, Sammel D, Homer MV, Bui K, Haunschild C, Stanczyk FZ, et al. Comparability of Antimüllerian Hormone Levels Among Commercially Available Immunoassays. Fertil Steril (2014) 101(6):1766–72.e1. doi: 10.1016/j.fertnstert.2014.02.046
35. Madersbacher S, Wolf H, Gerth R, Berger P, Haunschild C, Stanczyk FZ. Increased ELISA Sensitivity Using a Modified Method for Conjugating Horseradish Peroxidase to Monoclonal Antibodies. J Immunol Methods (1992) 152(1):9–13. doi: 10.1016/0022-1759(92)90083-6
36. Kricka LJ. Human Anti-Animal Antibody Interferences in Immunological Assays. Clin Chem (1999) 45(7):942–56. doi: 10.1093/clinchem/45.7.942
37. Kricka LJ. Interferences in Immunoassay–Still a Threat. Clin Chem (2000) 46(8 Pt 1):1037–8. doi: 10.1093/clinchem/46.8.1037
38. Selby C. Interference in Immunoassay. Ann Clin Biochem (1999) 36( Pt 6):704–21. doi: 10.1177/000456329903600603
39. Why Should Patients be Worried About Biotin. Abbott Core Laboratory (2021). Available at: https://www.corelaboratory.abbott/int/en/biotin-consumers.html.
40. Colon PJ, Greene DN. Biotin Interference in Clinical Immunoassays. J Appl Lab Med (2018) 2(6):941–51. doi: 10.1373/jalm.2017.024257
41. Waghray A, Milas M, Nyalakonda K, Siperstein AE. Falsely Low Parathyroid Hormone Secondary to Biotin Interference: A Case Series. Endocr Pract (2013) 19(3):451–5. doi: 10.4158/EP12158.OR
42. Turner KA, Larson BJ, Kreofsky NC, Willrich MAV, Bornhorst JA, Algeciras-Schimnich A. Assessment of Complement Interference in Anti-Müllerian Hormone Immunoassays. Clin Chem Lab Med (2019) 58(1):e8–e10. doi: 10.1515/cclm-2019-0496
43. Han X, McShane M, Sahertian R, White C, Ledger W. Pre-Mixing Serum Samples With Assay Buffer Is a Prerequisite for Reproducible Anti-Mullerian Hormone Measurement Using the Beckman Coulter Gen II Assay. Hum Reprod (2014) 29(5):1042–8. doi: 10.1093/humrep/deu050
44. Zuvela E, Walls M, Matson P. Within-Laboratory and Between-Laboratory Variability in the Measurement of Anti-Müllerian Hormone Determined Within an External Quality Assurance Scheme. Reprod Biol (2013) 13(3):255–7. doi: 10.1016/j.repbio.2013.04.005
45. Fertility Problems: Assessment and Treatment: National Institute for Health and Care Excellence (NICE) (2013). Available at: https://www.nice.org.uk/guidance/cg156/resources/fertility-problems-assessment-and-treatment-pdf-35109634660549.
46. Janse F, Donnez J, Anckaert E, de Jong FH, Fauser BCJM, Dolmans M-M. Limited Value of Ovarian Function Markers Following Orthotopic Transplantation of Ovarian Tissue After Gonadotoxic Treatment. J Clin Endocrinol Metab (2011) 96(4):1136–44. doi: 10.1210/jc.2010-2188
47. Chen S, Yang B, Fan J. Diagnostic Value of Anti-Mullerian Hormone in Ovarian Granulosa Cell Tumor: A Meta-Analysis. Eur J Obstet Gynecol Reprod Biol (2020) 253:266–72. doi: 10.1016/j.ejogrb.2020.08.011
48. Chong YH, Campbell AJ, Farrand S, McLennan IS. Anti-Müllerian Hormone Level in Older Women: Detection of Granulosa Cell Tumor Recurrence. Int J Gynecol Cancer (2012) 22(9):1497–9. doi: 10.1097/IGC.0b013e318270ac69
49. Rey RA, Lhommé C, Marcillac I, Lahlou N, Duvillard P, Josso N, et al. Antimüllerian Hormone as a Serum Marker of Granulosa Cell Tumorsof the Ovary: Comparative Study With Serum Alpha-Inhibin and Estradiol. Am J Obstet Gynecol (1996) 174(3):958–65. doi: 10.1016/S0002-9378(96)70333-2
50. Kaplan L, Pesce A, Kazmierczak S. Clinical Chemistry: Theory, Analysis, Correlation. St Louis, Mo: Mosby (2003).
51. Hyldgaard J, Bor P, Ingerslev HJ, Tørring N. Comparison of Two Different Methods for Measuring Anti-Mullerian Hormone in a Clinical Series. Reprod Biol Endocrinol (2015) 13(1):107. doi: 10.1186/s12958-015-0101-5
52. Klemt V, Hofmann V, Gassner D. First Fully Automated Immunoassay for Anti-Müllerian Hormone (AMH) on the Cobas E Analyzers. Switzerland: Roche Diagnostics International (2014). Available from: http://www.cobas.roche.it/content/dam/cobas_com/pdf/product/Elecsys%20AMH/Poster_ESHRE_First%20fully%20automated%20immunoassay%20for%20Anti-Mullerian.pdf.
53. Nelson SM, Pastuszek E, Kloss G, Malinowska I, Liss J, Lukaszuk A, et al. Two New Automated, Compared With Two Enzyme-Linked Immunosorbent, Antimüllerian Hormone Assays. Fertil Steril (2015) 104(4):1016–21.e6. doi: 10.1016/j.fertnstert.2015.06.024
54. van Helden J, Weiskirchen R. Performance of the Two New Fully Automated Anti-Müllerian Hormone Immunoassays Compared With the Clinical Standard Assay. Hum Reprod (2015) 30(8):1918–26. doi: 10.1093/humrep/dev127
55. Pearson K, Long M, Prasad J, Wu YY, Bonifacio M. Assessment of the Access AMH Assay as an Automated, High-Performance Replacement for the AMH Generation II Manual ELISA. Reprod Biol Endocrinol (2016) 14(1):8. doi: 10.1186/s12958-016-0143-3
56. Welsh P, Smith K, Nelson SM. A Single-Centre Evaluation of Two New Anti-Mullerian Hormone Assays and Comparison With the Current Clinical Standard Assay. Hum Reprod (2014) 29(5):1035–41. doi: 10.1093/humrep/deu036
57. Li HWR, Ng EHY, Wong BPC, Anderson RA, Ho PC, Yeung WSB. Correlation Between Three Assay Systems for Anti-Müllerian Hormone (AMH) Determination. J Assist Reprod Genet (2012) 29(12):1443–6. doi: 10.1007/s10815-012-9880-1
58. Tadros T, Tarasconi B, Nassar J, Benhaim J-L, Taieb J, Fanchin R. New Automated AntimüLlerian Hormone Assays Are More Reliable Than the Manual Assay in Patients With Reduced Antral Follicle Count. Fertil Steril (2016) 106(7):1800–6. doi: 10.1016/j.fertnstert.2016.08.045
59. Pigny P, Gorisse E, Ghulam A, Robin G, Catteau-Jonard S, Duhamel A, et al. Comparative Assessment of Five Serum Antimüllerian Hormone Assays for the Diagnosis of Polycystic Ovary Syndrome. Fertil Steril (2016) 105(4):1063–9.e3. doi: 10.1016/j.fertnstert.2015.12.023
60. Li HW, Wong BP, Ip WK, Yeung WS, Ho PC, Ng EH. Comparative Evaluation of Three New Commercial Immunoassays for Anti-Müllerian Hormone Measurement. Hum Reprod (2016) 31(12):2796–802. doi: 10.1093/humrep/dew248
61. Iliodromiti S, Salje B, Dewailly D, Fairburn C, Fanchin R, Fleming R, et al. Non-Equivalence of Anti-Müllerian Hormone Automated Assays-Clinical Implications for Use as a Companion Diagnostic for Individualised Gonadotrophin Dosing. Hum Reprod (2017) 32(8):1710–5. doi: 10.1093/humrep/dex219
Keywords: Anti-Müllerian Hormone, AMH, Müellerian inhibiting substance, MIS, standardisation, analytical interference
Citation: Punchoo R and Bhoora S (2021) Variation in the Measurement of Anti-Müllerian Hormone – What Are the Laboratory Issues? Front. Endocrinol. 12:719029. doi: 10.3389/fendo.2021.719029
Received: 01 June 2021; Accepted: 09 August 2021;
Published: 03 September 2021.
Edited by:
Jung Ryeol Lee, Seoul National University, South KoreaReviewed by:
Seido Takae, St. Marianna University School of Medicine, JapanCopyright © 2021 Punchoo and Bhoora. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rivak Punchoo, cml2YWsucHVuY2hvb0B1cC5hYy56YQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.