
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 14 September 2021
Sec. Thyroid Endocrinology
Volume 12 - 2021 | https://doi.org/10.3389/fendo.2021.686849
This article is part of the Research Topic Molecular Characterization of Thyroid Lesions in the Era of “Next Generation” Techniques View all 9 articles
 Jianhao Huang1,2†
Jianhao Huang1,2† Hongyan Shi1,3†
Hongyan Shi1,3† Muye Song1,4†
Muye Song1,4† Jinan Liang1,3Zhiyuan Zhang1,3Xiaohang Chen1,2
Jinan Liang1,3Zhiyuan Zhang1,3Xiaohang Chen1,2 Yongchen Liu1Sanming Wang1
Yongchen Liu1Sanming Wang1 Zeyu Wu1*
Zeyu Wu1*Background: Thyroid nodules are a very common finding in the general population. Fine-needle aspiration (FNA) has been recommended as the initial test for the evaluation of thyroid nodules. The trend on reporting as atypia of undetermined significance (AUS) has been significantly increased, but the malignant risk is still controversial among different studies. The aim of this study is to investigate the malignancy risk of thyroid nodules reported as Bethesda category III (AUS/FLUS) on initial FNA.
Method: We reviewed 272 papillary thyroid cancer (PTC) patients with suspicious thyroid nodules who underwent fine-needle aspiration and received surgical treatment during 2019 to 2020.
Results: One hundred ten (40.4%) patients were diagnosed with PTC. Multivariate analysis showed that microcalcification (p = 0.037, OR = 2.260, 95% CI: 1.051–4.860), shape (p = 0.003, OR = 4.367, 95% CI: 1.629–11.705), diameters (p = 0.002, OR = 0.278, 95% CI: 0.123–0.631), anti-thyroglobulin antibodies (TGAb) (p = 0.002, OR = 0.150, 95% CI: 0.046–0.494), anti-thyroid peroxidase antibody (A-TPO) (p = 0.009, OR = 4.784, 95% CI: 1.486–15.401), and nodule goiter (p < 0.001, OR = 0.100, 95% CI: 0.046–0.217) were independent malignant risk factors in patients with thyroid nodule classified as Bethesda category III.
Conclusion: In this study, malignant risk factors in patients with thyroid nodule classified as Bethesda category III were significantly associated with preoperative serum TGAb, A-TPO, microcalcification, irregular shape, and nodule diameters. Nodules with malignant factors should be carefully elevated; surgery may be the better option for those patients.
Fine-needle aspiration (FNA) has been widely recommended as the initial test for the evaluation of thyroid nodules. For better communication of the results of FNA among clinicians, in 2007 The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) was established (1). In 2017, the TBSRTC updated for reclassifying some neoplasms as new categories and implying cancer risk for each category, which provide management recommendation for clinicians (2).
However, Bethesda category III (atypia of undetermined significance [AUS] or follicular lesion of undetermined significance [FLUS]) carries controversy because of its heterogeneity in different populations, institutions, and pathologists. The trend on AUS has been significantly increased after the implementation of the TBSRTC (3). For an AUS/FLUS nodule, in 2017 TBSRTC, it carried 10%–30% cancer risk with cytological or architectural atypia. In recent studies, the cancer risk of the AUS nodule varied from 31.2% to 46.5% (4–7), which are obviously higher compared to those in the Bethesda System. Therefore, category III with AUS/FLUS should be reconsidered to determine the true risk of malignancy and provide proper recommendation of the clinicians.
We focused our study on investigating the malignancy risk of thyroid nodules reported as Bethesda category III (AUS/FLUS) on initial FNA, combined with the results of preoperative ultrasound examination and several common laboratory indexes, such as preoperative serum Tg (thyroglobulin) and thyroid antibodies.
Patients with suspicious thyroid nodules who underwent fine-needle aspiration and received surgical treatment in the Department of General Surgery at Guangdong Provincial People’s Hospital from January 2019 to December 2020 were enrolled in this study. The study was approved by the Research Ethics Committee of Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences. All patients gave their informed consent to the collection of data according to the local ethic committee indications. The preoperative US was routinely performed to assess the thyroid nodule status in all these patients. Ultrasonographic features of malignancy included hypoechoic nodule(s), undefined margin, irregular shape (taller than wide), microcalcifications, and capsule discontinuities. In the Laboratory Department, the levels of serum Tg (normal ranges: 3.5–77 ng/ml), TGAb (anti-thyroglobulin antibodies) (normal ranges: 0–115 IU/ml), A-TPO (anti-thyroid peroxidase antibody) (normal ranges: 0–34 IU/ml), and TRAb (thyrotropin receptor antibodies) (normal ranges: 0–1.75 IU/l) were measured before surgery. Each nodule received FNA three times, performed by experienced surgeons. Patients were diagnosed with malignancy by general pathological examination in the Pathology Department; the results were confirmed by two independent experienced pathologists.
Some patients were excluded from our study basing on any one of the following criteria: 1) mixed histologic types of thyroid malignancy; 2) received prior surgery or radiotherapy of the neck; 3) patients had proper surgical indications, including hyperthyroidism, retrosternal goiter; and 4) patients received active surveillance. Finally, the total number of 272 patients met our criteria.
Statistical analysis was performed by using IBM SPSS statistics 25.0 software. Univariate analyses by the X2 test or Fisher’s exact test were performed to investigate the malignant risk factors. Multivariate analysis was performed by binary logistic regression. p values <0.05 were considered statistically significant.
The clinicopathological characteristics of the 272 study patients according to CLNM status are listed in Table 1. Among these, 110 (40.4%) patients were diagnosed with PTC (papillary thyroid cancer); 162 (59.6%) patients with benign nodules. The mean age was 43.8 ± 11.2. Two hundred four patients were female (75.0%), and 25.0% (68 patients) were male. One hundred seventy-seven (65.0%) patients had nodules less than 1 cm, while 95 (35.0%) patients had nodules larger than 1 cm. With the FNA pathologic result, a total of 263 (96.7%%) patients had nucleus deformity, including obvious nucleoli and large nuclei. One hundred thirty-nine (51.1%) patients had irregular cell arrangement. Nucleus grooves were found in 142 patients (52.2%), while intranuclear pseudoinclusions were observed in 39 patients (14.3%). One hundred twenty-nine (46.0%) patients had nodular goiter.
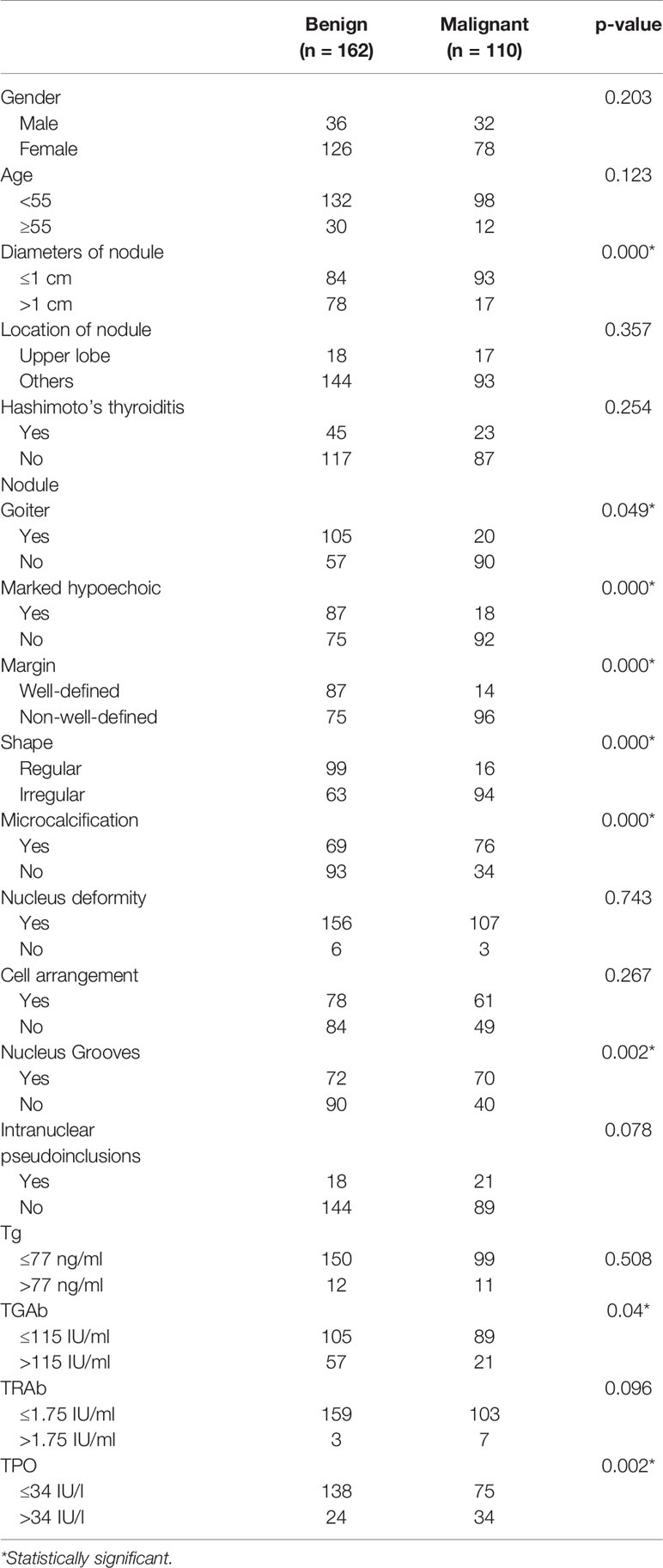
Table 1 Clinicopathological characteristics and univariate analysis of thyroid nodules (n = 272).
In the univariate analyses, as shown in Table 2, we found that malignant diagnosis in patients with thyroid nodules classified as Bethesda category III was significantly related to nodule diameter (p < 0.001), nodule goiter (p = 0.049), marked hypoechoicity (p < 0.001), margin (p < 0.001), shape (p < 0.001), microcalcification (p < 0.001), level of TGAb (p = 0.04), and A-TPO (p = 0.002), and nucleus grooves (p = 0.002). There were no significant differences in other clinicopathological factors such as age, intranuclear pseudoinclusions, Tg, or TRAb. For the multivariate analysis, a binary logistic regression was performed, and it revealed that microcalcification (p = 0.037, OR = 2.260, 95% CI: 1.051–4.860), shape (p = 0.003, OR = 4.367, 95% CI: 1.629–11.705), diameters (p = 0.002, OR = 0.278, 95% CI: 0.123–0.631), TGAb (p = 0.002, OR = 0.150, 95% CI: 0.046–0.494), A-TPO (p = 0.009, OR = 4.784, 95% CI: 1.486–15.401), and nodule goiter (p < 0.001, OR = 0.100, 95% CI: 0.046–0.217) were independent malignant risk factors in patients with thyroid nodules classified as Bethesda category III, as shown in Table 2.
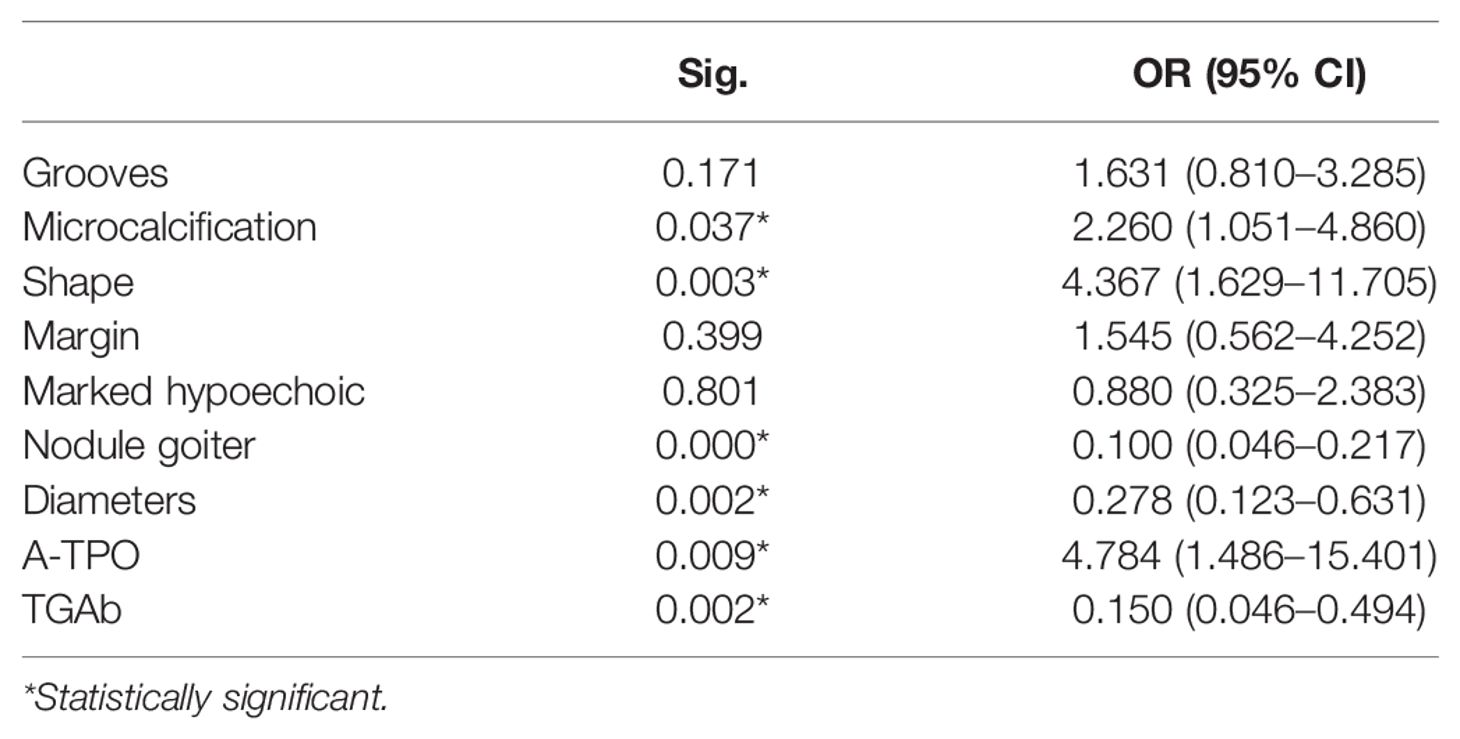
Table 2 Multivariate analysis of the malignant risk factors of thyroid nodules.
According to 2017 TBSRTC, the risk of malignancy for these Bethesda III thyroid nodules is estimated to be 10%–30%, but recent studies have reported malignancy rates significantly above the predicted ratio (2). In our retrospective study, the malignancy ratio was considerably higher, reaching 40.4% of all thyroid nodules. Ho et al. (8) presented 37.8% malignant risk which was determined based on the AUS/FLUS nodules undergoing surgery after receiving FNA, which is similar with our study. Gweon et al. (9) reported overall risk of malignancy for initial Bethesda III thyroid nodules with relatively high 55.5%. Besides, those nodules without repeat FNA show 78.3% malignant rate, significantly different from the malignant rate that received repeat FNA (37.2%). For the management of Bethesda class III nodules, repeat FNA may be recommended. However, Lee et al. (10) demonstrated that the usage of repeat FNA should be limited because of the possible unavoidable difference in the cytological interpretation. Similarly, Ogmen et al. (11) pointed out that repeat biopsy of AUS/FLUS nodules may not enhance the diagnosis of malignancy. In other studies, the risk of malignancy was found to be 31.2%–46.5%, again higher compared to the proposed one in the Bethesda System (4–7). On the contrary, Nagarkatti et al. (12) found that among 125 AUS/FLUS patients directly receiving surgery, the malignant rate was 16.0%, similar with the estimated risk rate according to 2017 TBSRTC.
Several studies have closely investigated the clinical features in the AUS/FLUS nodule to determine whether patients should receive direct surgery (6, 13). Ultrasonography was the fundamental evaluation of thyroid nodules because it can distinguish the suspicious malignant nodules that are suitable for undergoing FNA (14). In our study, we found that microcalcification and irregular shape (taller than wide) were malignant risk factors by multivariate analysis in ultrasound examination. These ultrasound features were generally considered most likely related to malignancy. In a meta-analysis including 1,851 nodules with indeterminate cytology aspirates, the presence of microcalcifications showed the best specificity (96%) (15). This finding is consistent with our results regarding microcalcifications as predictor of malignancy, with OR of 2.260 on multivariate analysis. Irregular shape (taller than wide) was also usually contributed to predict the malignancy of the intermediate thyroid nodule (14, 16, 17). Nodule size is also reported to have predictive value of malignancy in several studies (8, 18), and Jung et al. (6) suggest that size <2 cm is associated with an increased risk of well-differentiated thyroid cancer, which is also supported by Hadi et al. (19) However, Miller et al. (20) and Karman et al. (21) demonstrated that size >2 cm may be associated with thyroid malignancy. In our study, we found that nodule size in the malignant group is significantly smaller than that in the benign group, and on the multivariate analysis this factor was confirmed to be an independent predictor for malignancy and a threshold of approximately 1 cm in nodule diameter. FNA in thyroid nodules with diameter ≤1 cm is little studied, but we assumed that those with malignant ultrasound features should be carefully elevated and received FNA.
Another finding was that normal TGAb was more likely to be diagnosed as PTC than elevated TGAb (p = 0.008, OR = 3.493, with 95% CI: ranging from 1.378–8.861). TGAb, defined as thyroglobulin antibody, is a major thyroid-specific protein and mistakenly attacks healthy organs and tissues in autoimmune diseases. TGAb was widely used in the diagnosis of autoimmune thyroid diseases: Hashimoto disease, postpartum thyroiditis, neonatal hypothyroidism, and Grave’s disease. However, whether preoperative serum TGAb could predict the malignancy is still controversial (22).
Several studies discovered that autoimmune thyroiditis is associated with thyroid carcinoma, while others have proposed that the coexistence of thyroiditis in patients with thyroid nodules confers no additional risk of malignancy (23, 24). Besides, even in the absence of the histologically confirmed autoimmune thyroiditis, some studies underlined that preoperative serum TGAb was at a higher level in Differentiated Thyroid Cancer (DTC) patients than in those with benign thyroid nodules, and it was an independent predictive factor of DTC (22, 25). In our study, the incidence of malignancy in TGAb ≤115 IU/ml and TGAb >115 IU/ml was 45.9% vs. 26.9%, with a p value <0.05 in multivariate analysis, which may indicate that the presence of the autoimmune thyroiditis may interfere the malignant diagnosis of the intermediate thyroid nodules. MacDonald et al. (26) recognized that hyperplastic follicular cells on FNA samples from HT may mimic a follicular neoplasm, leading to false-positive results. Follicular cell changes in HT may be mistaken for thyroid neoplasm resulting in false-positives (27). We assume that patients had intermediate thyroid nodules and coexist with elevated TGAb which should have additional examinations to determine the malignancy, such as PET-CT and repeat FNA.
A-TPO, in our study, was significantly correlated with the malignancy of the nodule classified as Bethesda category III (p = 0.009, OR = 4.784, 95% CI: 1.486–15.401). A-TPO, defined as thyroid peroxidase antibody, is the antibody against TPO which plays an important role in the production of thyroid hormones. The presence of A-TPO may indicate thyroid damage by the autoimmune system, which may induce the malignant change of the thyroid nodule. The existence of A-TPO confers the risk of PTC with thyroid nodules, demonstrated by Wu et al. (28). However, other few studies may not identify the relationship between the level of A-TPO and the malignancy risk of the thyroid nodules (29, 30).
In addition, our study had a relatively small sample size, which may limit the statistical power of subgroup analysis. Moreover, our study was only a single-center retrospective analysis. It needs to be further verified by multicenter prospective studies.
In this study, malignant risk factors in patients with thyroid nodule classified as Bethesda category III was significantly associated with preoperative serum TGAb and A-TPO, which were little studied and still controversial in previous studies. The other independent predictors were microcalcification, irregular shape, and nodule diameters. Nodules with diameter ≤1 cm with malignant ultrasound features should be carefully elevated and receive FNA.
Thus, these factors are worth being considered by the surgeons when evaluating the thyroid nodule classified as Bethesda category III. Larger multicenter studies are necessary to be carried out to help clinicians build a strategy toward thyroid nodule classified as Bethesda category III.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The study was approved by the Research Ethics Committee of Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences. All patients gave their written informed consent to the collection of data according to the Research Ethics Committee of Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences.
Conception and design: JH, MS, and HS. Provision of study materials or patients: YL, SW, and ZW. Collection and assembly of database: JH, MS, HS, JL, ZZ, and XC. Data analysis: JH, MS, and HS. All authors contributed to the article and approved the submitted version.
This work was supported by Guangdong Basic and Applied Basic Research Foundation (No. 2020A1515010126), Scientific Research Staring Foundation for the Returned Overseas from Guangdong Provincial People’s Hospital (No. 2017x02) and Guangdong Provincial People’s Hospital Scientific Foundation for Distinguished Young Scholars of Guangdong Province (No. KJ012019441).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cibas ES, Ali SZ. The Bethesda System For Reporting Thyroid Cytopathology. Am J Clin Pathol (2009) 132(5):658–65. doi: 10.1309/ajcpphlwmi3jv4la
2. Cibas ES, Ali SZ. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid (2017) 27(11):1341–6. doi: 10.1089/thy.2017.0500
3. Bongiovanni M, Krane JF, Cibas ES, Faquin WC. The Atypical Thyroid Fine-Needle Aspiration: Past, Present, and Future. Cancer Cytopathol (2012) 120(2):73–86. doi: 10.1002/cncy.20178
4. Mileva M, Stoilovska B, Jovanovska A, Ugrinska A, Petrushevska G, Kostadinova-Kunovska S, et al. Thyroid Cancer Detection Rate and Associated Risk Factors in Patients With Thyroid Nodules Classified as Bethesda Category III. Radiol Oncol (2018) 52(4):370–6. doi: 10.2478/raon-2018-0039
5. Lee KH, Shin JH, Oh YL, Hahn SY. Atypia of Undetermined Significance in Thyroid Fine-Needle Aspiration Cytology: Prediction of Malignancy by US and Comparison of Methods for Further Management. Ann Surg Oncol (2014) 21(7):2326–31. doi: 10.1245/s10434-014-3568-y
6. Jung Y, Yoon H, Hwang M, Shin S, Cho J-S, Lee J, et al. Atypia of Undetermined Significance on Thyroid Fine Needle Aspiration: Surgical Outcome and Risk Factors for Malignancy. Ann Surg Treat Res (2014) 86:109–14. doi: 10.4174/astr.2014.86.3.109
7. Ozluk Y, Pehlivan E, Gulluoglu MG, Poyanli A, Salmaslioglu A, Colak N, et al. The Use of the Bethesda Terminology in Thyroid Fine-Needle Aspiration Results in a Lower Rate of Surgery for Nonmalignant Nodules: A Report From a Reference Center in Turkey. Int J Surg Pathol (2011) 19(6):761–71. doi: 10.1177/1066896911415667
8. Ho AS, Sarti EE, Jain KS, Wang H, Nixon IJ, Shaha AR, et al. Malignancy Rate in Thyroid Nodules Classified as Bethesda Category III (AUS/FLUS). Thyroid (2014) 24(5):832–9. doi: 10.1089/thy.2013.0317
9. Gweon HM, Son EJ, Youk JH, Kim JA. Thyroid Nodules With Bethesda System III Cytology: Can Ultrasonography Guide the Next Step? Ann Surg Oncol (2013) 20(9):3083–8. doi: 10.1245/s10434-013-2990-x
10. Lee Y, Kim BH, Suh S, Seo H, Seo BK, Cho K, et al. Comparison of Cytological Results Obtained by Repeated US-Guided Fine-Needle Aspiration Biopsies of Thyroid Nodules: Focus on the Rate of Malignancy and Diagnostic Concordance. Diagn Cytopathol (2009) 37:492–7. doi: 10.1002/dc.21043
11. Evranos Ogmen B, Aydin C, Kilinc I, Aksoy Altinboga A, Ersoy R, Cakir B. Can Repeat Biopsies Change the Prognoses of AUS/FLUS Nodule? Eur Thyroid J (2020) 9(2):92–8. doi: 10.1159/000504705
12. Nagarkatti SS, Faquin WC, Lubitz CC, Garcia DM, Barbesino G, Ross DS, et al. Management of Thyroid Nodules With Atypical Cytology on Fine-Needle Aspiration Biopsy. Ann Surg Oncol (2013) 20(1):60–5. doi: 10.1245/s10434-012-2601-2
13. Hegedüs L. Clinical Practice. The Thyroid Nodule. N Engl J Med (2004) 351(17):1764–71. doi: 10.1056/NEJMcp031436
14. Yoon JH, Kwak JY, Kim EK, Moon HJ, Kim MJ, Kim JY, et al. How to Approach Thyroid Nodules With Indeterminate Cytology. Ann Surg Oncol (2010) 17(8):2147–55. doi: 10.1245/s10434-010-0992-5
15. Remonti LR, Kramer CK, Leitão CB, Pinto LC, Gross JL. Thyroid Ultrasound Features and Risk of Carcinoma: A Systematic Review and Meta-Analysis of Observational Studies. Thyroid (2015) 25(5):538–50. doi: 10.1089/thy.2014.0353
16. Méndez W, Rodgers SE, Lew JI, Montano R, Solórzano CC. Role of Surgeon-Performed Ultrasound in Predicting Malignancy in Patients With Indeterminate Thyroid Nodules. Ann Surg Oncol (2008) 15(9):2487–92. doi: 10.1245/s10434-008-0052-6
17. Topaloglu O, Baser H, Cuhaci FN, Sungu N, Yalcin A, Ersoy R, et al. Malignancy is Associated With Microcalcification and Higher AP/T Ratio in Ultrasonography, But Not With Hashimoto’s Thyroiditis in Histopathology in Patients With Thyroid Nodules Evaluated as Bethesda Category III (AUS/FLUS) in Cytology. Endocrine (2016) 54(1):156–68. doi: 10.1007/s12020-016-0982-x
18. Sippel RS, Elaraj DM, Khanafshar E, Kebebew E, Duh QY, Clark OH. Does the Presence of Additional Thyroid Nodules on Ultrasound Alter the Risk of Malignancy in Patients With a Follicular Neoplasm of the Thyroid? Surgery (2007) 142(6):851–7; discussion 7.e1-2. doi: 10.1016/j.surg.2007.08.011
19. Al-Hakami HA, Alqahtani R, Alahmadi A, Almutairi D, Algarni M, Alandejani T. Thyroid Nodule Size and Prediction of Cancer: A Study at Tertiary Care Hospital in Saudi Arabia. Cureus (2020) 12(3):e7478. doi: 10.7759/cureus.7478
20. Miller B, Burkey S, Lindberg G, Snyder W, Nwariaku F. Prevalence of Malignancy Within Cytologically Indeterminate Thyroid Nodules. Am J Surg (2004) 188:459–62. doi: 10.1016/j.amjsurg.2004.07.006
21. Kamran SC, Marqusee E, Kim MI, Frates MC, Ritner J, Peters H, et al. Thyroid Nodule Size and Prediction of Cancer. J Clin Endocrinol Metab (2013) 98(2):564–70. doi: 10.1210/jc.2012-2968
22. Xiao Y, Zhou Q, Xu Y, Yuan SL, Liu QA. Positive Thyroid Antibodies and Risk of Thyroid Cancer: A Systematic Review and Meta-Analysis. Mol Clin Oncol (2019) 11(3):234–42. doi: 10.3892/mco.2019.1886
23. Fiore E, Rago T, Latrofa F, Provenzale MA, Piaggi P, Delitala A, et al. Hashimoto's Thyroiditis is Associated With Papillary Thyroid Carcinoma: Role of TSH and of Treatment With L-Thyroxine. Endocr Relat Cancer (2011) 18(4):429–37. doi: 10.1530/erc-11-0028
24. Grani G, Calvanese A, Carbotta G, D'Alessandri M, Nesca A, Bianchini M, et al. Thyroid Autoimmunity and Risk of Malignancy in Thyroid Nodules Submitted to Fine-Needle Aspiration Cytology. Head Neck (2015) 37(2):260–4. doi: 10.1002/hed.23587
25. Kim ES, Lim DJ, Baek KH, Lee JM, Kim MK, Kwon HS, et al. Thyroglobulin Antibody is Associated With Increased Cancer Risk in Thyroid Nodules. Thyroid (2010) 20(8):885–91. doi: 10.1089/thy.2009.0384
26. MacDonald L, Yazdi HM. Fine Needle Aspiration Biopsy of Hashimoto's Thyroiditis. Sources of Diagnostic Error. Acta Cytol (1999) 43(3):400–6. doi: 10.1159/000331088
27. Kumarasinghe MP, De Silva S. Pitfalls in Cytological Diagnosis of Autoimmune Thyroiditis. Pathology (1999) 31(1):1–7. doi: 10.1080/003130299105430
28. Wu X, Lun Y, Jiang H, Gang Q, Xin S, Duan Z, et al. Coexistence of Thyroglobulin Antibodies and Thyroid Peroxidase Antibodies Correlates With Elevated Thyroid-Stimulating Hormone Level and Advanced Tumor Stage of Papillary Thyroid Cancer. Endocrine (2014) 46(3):554–60. doi: 10.1007/s12020-013-0121-x
29. Wong SL, Grodski S, Yeung MJ, Serpell JW. Anti-Thyroid Antibodies as a Predictor of Thyroid Cancer. ANZ J Surg (2015) 85(11):849–53. doi: 10.1111/ans.12453
Keywords: thyroid cancer, autoimmune thyroid antibodies, tumor size, fine needle aspirate (FNA), microcalcification
Citation: Huang J, Shi H, Song M, Liang J, Zhang Z, Chen X, Liu Y, Wang S and Wu Z (2021) Surgical Outcome and Malignant Risk Factors in Patients With Thyroid Nodule Classified as Bethesda Category III. Front. Endocrinol. 12:686849. doi: 10.3389/fendo.2021.686849
Received: 06 May 2021; Accepted: 18 August 2021;
Published: 14 September 2021.
Edited by:
Dario de Biase, University of Bologna, ItalyReviewed by:
Gianluca Donatini, Centre Hospitalier Universitaire (CHU) de Poitiers, FranceCopyright © 2021 Huang, Shi, Song, Liang, Zhang, Chen, Liu, Wang and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zeyu Wu, d3UuemV5dUBob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.