
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Endocrinol. , 10 December 2020
Sec. Clinical Diabetes
Volume 11 - 2020 | https://doi.org/10.3389/fendo.2020.574312
 Dácil Alvarado-Martel1,2*
Dácil Alvarado-Martel1,2* Mauro Boronat1,2
Mauro Boronat1,2 María del Pino Alberiche-Ruano1,2María Andrea Algara-González2Yolanda Ramallo-Fariña3,4
María del Pino Alberiche-Ruano1,2María Andrea Algara-González2Yolanda Ramallo-Fariña3,4 Ana M. Wägner1,2*
Ana M. Wägner1,2*Background: Type 1 diabetes is a disease with complex therapeutic recommendations that require day-to-day lifestyle changes. Motivational Interviewing is a communication tool that has proved effective in changing behaviors in people with addictions, obesity and type 2 diabetes. Our objective is to evaluate the effects of a Motivational Interviewing intervention in people with type 1 diabetes.
Methods: Sixty-six patients with type 1 diabetes and hemoglobin A1c >= 8% have been included and randomly assigned (computer-generated sequence, sealed envelopes, ratio 1:1) either to the intervention or to the control group. In the intervention group, appointments every 4 months with the endocrinologist include Motivational Interviewing; in the control group, the appointments proceed as usual. Patients will be followed for 16 months. The primary outcome will be self-care behaviors, assessed by a validated questionnaire, the Diabetes Self-Care Inventory-Revised Version. Secondary outcomes include: HbA1c, motivation for self-care, self-efficacy, health-related quality of life, satisfaction with professional-patient relationship, and fulfillment of patients’ own objectives. The practitioners receive training in Motivational Interviewing in order to help them promote adherence to self-care, encourage patient motivation and improve the doctor-patient relationship. The Motivational Interviewing intervention will be evaluated by two psychologists, blinded to the assigned treatment, through video recordings of the sessions and the administration of a purpose-built questionnaire, the EVEM 2.0 scale.
Discussion: There is evidence that MI can improve self-care in type 2 diabetes. In this study, we aim to evaluate the effect of MI on self-care and HbA1c in people with type 1 diabetes.
Clinical Trial Registration: https://clinicaltrials.gov/ct2/show/NCT03906786, identifier NCT03906786.
● Research has shown that the level of motivation reported by the patient was the strongest predictor of adherence to self-care, and was also recognized as one of the greatest obstacles to adherence to treatment.
● Motivational Interviewing has shown to be effective in changing behaviors in people with addictions, obesity, and type 2 diabetes.
● The present trial will assess the effects of Motivational Interviewing on adults with type 1 diabetes.
People with type 1 diabetes (T1D) have to carry out a series of complex tasks every day in order to manage their disease and maintain good glycemic control (1). These tasks include glucose measurements, multiple insulin injections, carbohydrate counts in the diet, and management of hypoglycemia and hyperglycemia. In addition, patients must continuously make decisions regarding the adjustment of their insulin treatment and the everyday problems related to their illness (2–4). In a previous study which identified multiple factors related to self-care, the level of motivation reported by the patient was the strongest predictor of adherence to self-care, and was also recognized as one of the greatest obstacles to adherence to treatment (5). Currently, diabetes management is focused on person-centered care and empowerment, a philosophy that encourages patient involvement, awareness and participation in decisions concerning their health (6). One of the fundamental pillars for promoting empowerment of people in their self-care is therapeutic patient education (7, 8). Therapeutic patient education provides patients with the knowledge, tools and skills needed to facilitate informed decision-making and self-management of the disease (8). However, therapeutic education alone does not guarantee the involvement of patients in the care of their health (8, 9).
Since 2014, in its Standards for Diabetes Self-Management Education and Support, the American Diabetes Association recommends a set of evidence-based communication strategies which have been shown to facilitate behavioral changes and to complement therapeutic patient education. They include cognitive strategies, problem solving, enhanced self-efficacy, relapse prevention strategies and Motivational Interviewing (MI) (10, 11). To quote the creators of MI: “Motivational Interviewing is a collaborative, goal-oriented method of communication with particular attention to the language of change. It is designed to strengthen an individual’s motivation for and movement toward a specific goal by eliciting and exploring the person’s own argument for change within an atmosphere of acceptance and compassion” (12).
MI emerged for the first time in Norway in 1982, and initially focused on addictions (13). Since then, its use has spread to other areas. It has been widely applied in the management of behavior-associated diseases (14) and more than three decades of research have established it as an effective approach for improving a series of health-related behaviors (14). Currently, there is moderate, consistent and robust evidence that MI achieves behavioral changes and improves adherence to treatment in patients with alcohol abuse, unhealthy lifestyles (e.g., sedentarism, overeating) and obesity/overweight (15, 16). Brief 15-min MI interventions have also proven to be effective, though the probability of success increases with the number of encounters and with longer follow-up periods (14).
MI has been shown to be effective in improving glycemic control in people with type 2 diabetes (T2D) (16–20) and its superiority over cognitive behavioral therapy has also been demonstrated (21). MI has proved effective in reducing HbA1c in adolescents with T1D (22, 23), and in a clinical trial it also improved quality of life (24, 25). It is effective as a complement to therapeutic education (26) and to other treatments, or as an independent treatment (22). However, not all studies have reported improvement in glycemic control in T1D or T2D (27, 28). A recent systematic review, which included four randomized controlled trials, concluded that there is some evidence of benefit of MI in people with T1D, but that more research is needed to isolate the effect of MI alone on adherence to treatment and HbA1c (29).
The purpose of this randomized controlled clinical trial is to study the impact of the application of MI in routine follow-up visits of patients with T1D and poor metabolic control.
The hypothesis is that an intervention with MI can increase patients’ self-care behaviors, reduce HbA1c, enhance their self-efficacy and health-related quality of life, and improve the doctor-patient relationship.
This study protocol was developed in accordance with the Recommendations for Interventional Trials 2013 Statement (SPIRIT 2013) and the Consolidated Standards of Reporting Trials statement (CONSORT 2010) when applicable.
MI is defined primarily by its spirit: that is, a style that nurtures the interpersonal relationship between the therapist and the patient. It explains how the process of change is formed by different stages and how people are more likely to abandon a habit at certain stages than at others. In addition, it considers that deciding to change, to commit oneself, and to take responsibility for a therapeutic process is key to achieving behavior changes. MI uses a style of collaborative communication focused on one or several objectives and pays special attention to the language of change. It is designed to strengthen personal motivation and commitment to a specific goal, eliciting, and exploring the reasons that the person has for changing, in an atmosphere of acceptance and empathy. The approach is based on patient-centered counseling, cognitive therapy, systems theory and the social psychology of persuasion. It integrates clinical skills that promote motivation, combining managerial and non-managerial elements. In sum, it is a practical and specific contribution to daily life in which language is used to influence behavior by helping individuals express their own internal motivations, and guiding conversations in such a way that people persuade themselves to change in accordance with their own values and interests.
For maximum benefit to be derived from MI, the interviewer must have received adequate training, but must also believe in it in order to be able to influence the patient and initiate a process of change. MI involves eliciting from the patient what they already know and have, rather than giving them what they lack (for instance, knowledge, or medication) (30). This focus can improve patients’ motivation, since they choose what they want to do or change, not what others want them to do or change. By developing MI skills, practitioners can help patients identify what matters to them and then use these motivations to bring about changes in their health behavior (30).
Assessing the effectiveness of MI in the context of diabetes may appear controversial, since adherence to self-care already obliges people with diabetes to carry out multiple tasks. In fact, previous studies have focused on assessing the impact of MI on glycemic control (14, 17); to date, there are no clinical trials that study its impact on adherence to self-care behaviors in adults with T1D, or evaluate the standardized application of MI by practitioners.
This randomized, controlled, single-blind, parallel group clinical trial is carried out at the Endocrinology and Nutrition service of the Insular University Hospital, Las Palmas de Gran Canaria, a reference center in its area for the care of people with T1D.
A total of 66 people with T1D have been included in the study and will be followed over a period of 16 months. Patients who met the inclusion criteria were informed of the nature of the study and invited to participate. Subsequently, they were recruited by their endocrinologist at the outpatient clinics of the Endocrinology and Nutrition Service of the Insular University Hospital. The recruitment period lasted from March to August 2019.
Diagnosis of T1D, age over 18, at least one year of disease duration, HbA1c >= 8% and/or severe hypoglycemia in the previous 6 months.
Pregnancy either in progress or scheduled in the following 12 months; any other circumstance that, in the opinion of the investigators, might interfere with the follow-up.
Patients who meet the inclusion criteria receive written information regarding the study and are invited to participate. They are also provided with more information by phone, when they are reminded that the trial will begin at the next scheduled follow-up appointment. At this first appointment, prior to the consultation, the participants sign the informed consent document and fill in a dossier that records all the clinical, sociodemographic and psychosocial variables. These variables are listed in the Measures section below.
The participants are randomly assigned to the intervention group or control group. A computer-generated randomization list (with a 1:1 ratio) is used for each endocrinologist to prepare the labels indicating the assignment of each patient, which is kept in sealed envelopes, numbered consecutively, and stored at the unit. At the time of inclusion of a patient in the study (appointment 1), the appropriate envelope is chosen and opened to show the endocrinologist the treatment assigned. The randomization is stratified by practitioner and the treatment assigned to the first participant each day is applied to all participants scheduled on that day, in order to facilitate the application of the MI and avoid contamination between treatment groups. To limit possible bias, patients are not informed of the assigned treatment. The informed consent document explains that the study will evaluate the effects of the doctor-patient communication, though without going into detail. The researcher who generated the randomization list and prepared the envelopes for the assignment of the treatment group will not be involved in the treatment or evaluation of the participants; likewise, the researchers who will rate MI compliance and analyze the data will be blind to the treatment allocation.
The intervention will consist in the application of MI by the endocrinologist at four follow-up visits, held at 4-month intervals.
These visits proceed in the same way as standard appointments, with the addition of this new clinical approach. The visits last approximately 15–20 min, in accordance with routine hospital practices.
At each visit, the practitioner applies the four processes of MI (12):
● Engaging. This first stage serves to establish a therapeutic relationship of trust and mutual respect, if this has not already been achieved.
● Focusing. This stage is a continuous process of searching for and maintaining direction. The aim is to place the emphasis on the “focus”, i.e., the aspect that the person wants to change. It is not a static process; it may be that in other stages it is necessary to change course and renegotiate the objectives.
● Evoking. This stage is aimed at eliciting “change talk” from the patient, so that he or she persuades him or herself to change. It begins with the expression of a desire, reason, or need. This stage promotes self-efficacy, one of the most powerful predictors of successful behavior. MI promotes change because it impacts on people’s self-efficacy.
● Planning. This stage is characterized by the presence of specific actions. There is less maintenance talk (regarding the behavior to be changed) and more change talk. The person begins to visualize the change and imagines the possible positive results. MI ends when the person commits to the plan.
Before the first appointment and 4 months after the fourth appointment, the participants complete the questionnaires. In each of the five visits the HbA1c value will be recorded.
A sample of 25 baseline appointments 1 was videotaped in order to assess the application of MI, and serve as ongoing training for the practitioners. A similar procedure will be followed for appointment 4. The practitioners who apply MI have previously received training.
MI is a set of skills designed to help patients overcome their ambivalence to change by evoking motivation and commitment. Professionals can gain expert experience in this method, for example, through an eight-step program (Motivational Interviewing Network of Trainers- MINT), which can be completed in 16 h.
The three endocrinologists have received structured MI training through theoretical-practical workshops taught by a psychologist with previous training and experience in MI. The workshops, which included didactic instruction and interactive exercises, were divided into two 3- to 4-h sessions and two to four additional 60- to 90-min encounters. The training started 3 months before recruitment, continued until the intervention began and addressed the contents established by MINT (Table 1). Interactive exercises included interviews conducted with real playing (i.e., colleagues who proposed something they would like to change, in order to make the practice more realistic), as well as role playing (i.e., using cases that are built on the context of T1D). Furthermore, real-patient interviews were overseen by the psychologist, both directly and through visualization of video recordings, and feedback was provided. Finally, all researchers read the MI book “Motivational interviewing: helping people change” (15). In addition, as a reminder, they were given a magnet on which the main tasks associated with MI are printed, to be put up in a visible place in their unit.
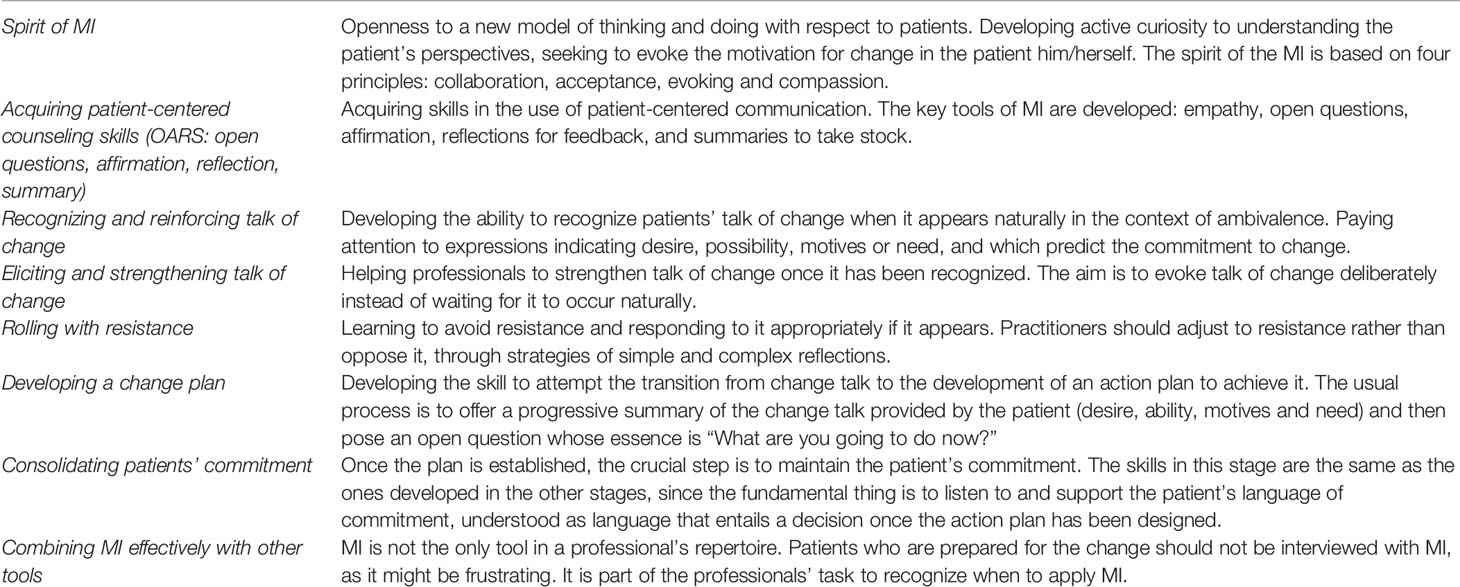
Table 1 Contents of the theoretical-practical MI workshop.
To avoid skill erosion and further improve MI performance, regular coaching and feedback-based, post-training sessions were held at baseline and are repeated at 2- to 3-month intervals during the intervention trial, to adhere to evidence-based practices (31). Individual reading of the book “Motivational Interviewing in Diabetes: facilitating self-care” (32) will complement the post-training sessions.
Patients randomly assigned to the control group will receive their four follow-up visits with standard medical care. The visits will be held with the same health practitioners, at the same intervals as in the intervention group, and will last a similar length of time. At each of the visits the HbA1c will be recorded, and before the first visit and 4 months after the fourth visit controls will complete the questionnaires in the same way as the intervention group.
Participants will continue with their usual follow-up routine for diabetes care. They are not asked for anything additional.
The results of the study will be presented to the scientific community at scientific meetings and in a research article. The results will also be disseminated in the local press and on the web page of the research group. Patients will also be informed of the results at the diabetes unit, once the trial has finished.
The main variable of the study is adherence to self-care, measured through a validated questionnaire, the Diabetes Self-Care Inventory-Revised version (SCI-R). The secondary variables are: HbA1c, self-efficacy (EAG), health-related Quality of Life (ViDa1), satisfaction with the doctor-patient relationship, motivation for self-care, satisfaction with self-care, degree of fulfilment of a personal goal initially proposed by the participant, and a series of sociodemographic and clinical variables listed below. The time intervals for the measurements are shown in Table 2.
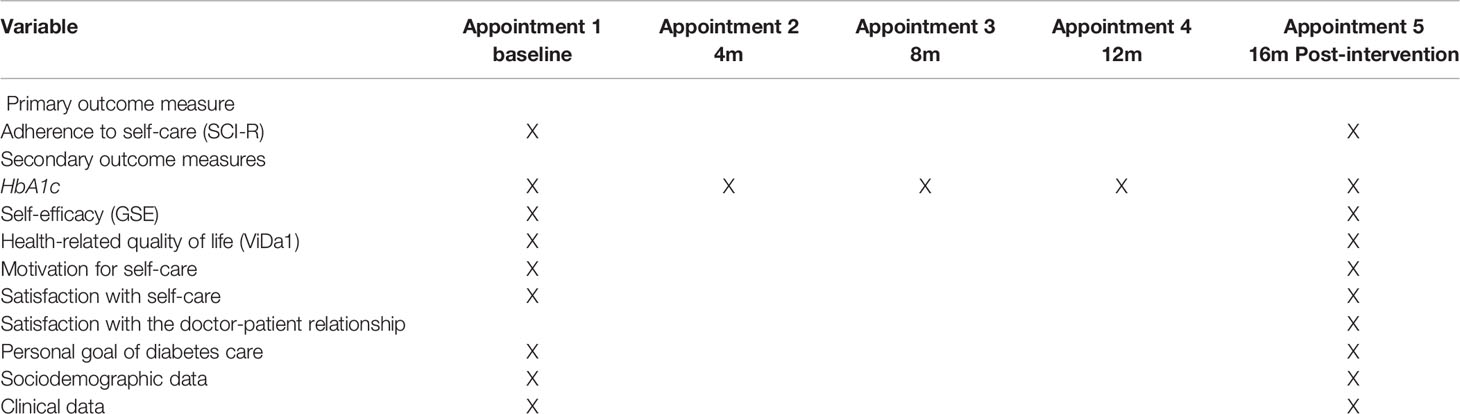
Table 2 Time points of measurements.
The validated Spanish version of the SCI-R (33) will be used. This inventory consists of 15 items referring to self-care behaviors in the treatment of diabetes, which are scored on a Likert scale ranging from (1 = “never” to 5 = “always”). The scores are converted with a formula, and the responses range from 0 to 100; higher scores indicate higher levels of self-care.
This data sheet is designed specifically for the study and it covers the following sociodemographic and clinical variables: sex, age, level of education (unschooled, primary, secondary, and university studies), employment status, living arrangements, duration of disease, type of drug treatment, treatment with psychoactive drugs, carbohydrate count, level of training in diabetes, diabetes chronic complications, and the limitation they represented for participants’ daily lives, number of hypoglycemia episodes per week, number of daily capillary glucose readings, and previous history of acute complications (admissions for severe hyperglycemia or hypoglycemia). Medical variables are confirmed via the patients’ medical history.
Glycated hemoglobin (HbA1c) (measured by HPLC or by point-of-care Alere Afinion AS100, standardized against DCCT/NGSP) is the standard measure for evaluating glycemic control over the last 2–3 months. The ADA recommendations suggest a general target level for HbA1c of less than 7% to reduce risk of diabetic complications (11).
The General Self-Efficacy Scale (34) is administered in its validated Spanish version (35). This scale measures respondents’ expectations regarding their ability to cope adequately with a problematic situation. Responses are recorded on a Likert scale (1 = “not at all” to 5 = “totally”) and the score range is 1–50. Higher scores indicate a higher perception of self-efficacy.
Health-related quality of life is measured with the ViDa1 (36), which contains 34 items grouped in four dimensions: interference of diabetes in daily life, self-care, well-being, and worry about the disease. The response format is a Likert scale ranging from (1 = “strongly disagree” to 5 = “strongly agree”). A total score is obtained for each subscale, with a higher value indicating a higher level of the respective aspect.
Motivation for self-care is measured on a Likert scale of 1–10, where 10 is the maximum score. This item is formulated specifically for this study.
Satisfaction with self-care is measured with a Likert scale of 1–10, where 10 is the maximum score. This item is formulated specifically for this study.
Satisfaction with the doctor-patient relationship is measured with a Likert scale of 1–10, where 10 is the maximum score. This item is formulated specifically for this study.
Patients set themselves a health-related goal which they aim to achieve through their participation in the trial. The degree of achievement is measured with a Likert scale (1–10).
To evaluate the application of MI by the practitioners, video recordings of 25 patients were carried out at the first visit. At the fourth visit, all patient interviews will be recorded, and a random sample of 25 will be evaluated. A mobile phone with a tripod and an external memory card are used to make the video recordings. The recordings will be evaluated by two external observers using the Motivational Interviewing Rating Scale (MIAS/EVEM 2.0) (37). This scale has been previously validated for the application of MI in primary care; applied to several clinical sessions, it discriminates between the sessions in which the method has been used (and establishes to what degree) and the ones in which it has not been used. The raters will not know a priori to which group the patients in the recordings have been assigned.
Based on the number of patients followed in the clinic and the percentage with an HbA1c above 8%, we estimated that each of the three clinical researchers involved in the trial would be able to recruit around 20 patients in 4 months. With an expected sample size of 60 participants, we would be able to detect inter-group differences of 12.8 points on the SCI-R questionnaire and of 0.85% in HbA1c, with a power of 90% and a two-sided alpha of.05 [assuming an SD of 15 points in the SCI -R and 1% in HbA1c in line with previous studies (5)]. The equivalent detectable differences with a power of 0.8 would be 11 points and 0.74% respectively (calculated with http://hedwig.mgh.harvard.edu/sample_size/js/js_parallel_quant.html). This was an approximate estimation assuming the normality of the variable.
In order to retain most of the patients during follow-up, if someone misses an appointment, the patient is contacted and the visit is re-scheduled. Specific efforts will be made for the final evaluation visit. If a physical appointment cannot be achieved, the questionnaires will be sent and completed by e-mail or, if this is not feasible, the patient with be interviewed by phone. We expect the loss to follow-up to be below 10%.
Intention to treat analysis will be performed: i.e., all randomized participants who have attended at least one intervention (or control) session will be included in the analyses. The main analysis for primary and secondary outcomes, except HbA1c, will be a generalized linear model (GLM) including the intervention arm, the baseline score of the dependent variable and other variables imbalanced at baseline as covariates. The dependent variable will be the post-intervention score. The GLM does not need a normal distribution in the dependent variable (38), although the distribution of the variables will be analyzed using de Shapiro- Wilk test to perform an adequate descriptive analysis. The choice of the link function will depend on the distribution of the variable.
For the HbA1c, a GLM for multilevel analysis will be used including the intervention arm, baseline HbA1c and other imbalanced variables in the baseline as covariates. First-level are those corresponding to each measurement along follow-up (repeated time measurements); the second level includes patients’ variables. The model will also include an interaction term between the intervention-arm and time (follow-up), allowing for differences in the intervention effect between follow-up assessments (39). The effect that identifies the intervention arm is considered fixed, whereas the intercept is considered random. An autoregressive [AR (1)] covariance structure will be used in the model.
Other variables will be added as confounders in the model, as secondary sensitivity analyses. We will first fit separate models including each confounder, one at a time. Those variables whose inclusion in the model changes the estimates’ treatment effect by at least 10% will be considered as confounders. As suggested in the CONSORT statement, decisions about confounders will not be based on P value (40).
In the case of missing values, these will be accommodated with multiple imputation procedure in Stata 15.0 software (Stata Corporation) (41). This procedure saves cases for the analysis and can be considered an intention-to-treat analysis. Analysis under multiple imputations is valid for randomly missed data (42). A threshold of.05 will be used to define the statistical significance of those tests.
For the MIAS/EVEM 2.0 scale, the Intraclass Correlation Coefficient (ICC) will be used.
This study protocol presents the design of a randomized controlled clinical trial aimed to evaluate the impact of an MI intervention on the self-care behaviors of people with T1D. We expect the MI-based intervention to improve the doctor-patient relationship and to increase the motivation for self-care, and with it, self-care behaviors. We also expect improvements in glycemic control and increases in self-efficacy and health-related quality of life.
There is evidence that MI can improve self-care in T2D (20, 21). In T1D, to date, however, its application has focused on adolescents, in whom some studies have shown a statistically significant improvement in glycemic control (21–24, 29, 43) but others have not (27). At present, there are no published data on the effect of MI in adults with T1D.
Increasing adherence to self-care is a challenge in a chronic disease such as T1D. An MI-based intervention to replace the traditional interview may improve glycemic control and thus prevent chronic complications in the future. In this study, we aim to evaluate the effect of MI on self-care and HbA1c.
We acknowledge that this study has some limitations. MI is a complex tool to learn; it takes time to manage it correctly, practitioners may not be experts in its use and learned skills tend to wear off. In order to reduce training erosion, regular coaching and feedback will be provided throughout the trial. On the other hand, the same practitioner will apply MI to some patients and the traditional interview to the others (control group), which carries a certain risk of contamination between the study groups. To minimize contamination, participants seen by the same practitioner on the same day were assigned to the same treatment group, which could, of course, lead to some imbalance between the sizes of the groups. To monitor if MI is indeed applied in the intervention group and not in the control group, the sessions will be blindly evaluated at the first and last visits of the study. Finally, not all patients are comfortable with this method of interviewing, a situation that may hinder its application. Regarding outcomes, self-care, the primary outcome, comprises an array of behaviors, which might not accurately reflect the success of MI if change is focused on a single behavior, selected by the patient. The assessment of the achievement of self-defined goals should, at least partially, account for this drawback. Furthermore, some concepts will be examined on an exploratory basis using only a single-item and not a psychometrically tested measure, so these findings should be interpreted as descriptive and with caution. Finally, the sample size of this trial will be able to detect relatively large, clinically relevant changes in the primary and some of the secondary endpoints. However, it might be underpowered to detect smaller, albeit still relevant effect sizes. The low number of healthcare professionals included in the trial, which act as randomization clusters, does not allow the effect associated with the health professionals to be included in the analysis. This could potentially lead to bias, since the variance associated with the healthcare professionals cannot be estimated.
All study-related information will be stored securely at the study site. All participant information will be stored in locked file cabinets in areas with limited access. All reports, data collection, process, and administrative forms will be identified by a coded ID [identification] number only to maintain participant confidentiality. All records that contain names or other personal identifiers, such as locator forms and informed consent forms, will be stored separately from study records identified by code number. All local databases will be secured with password-protected access systems. Forms, lists, logbooks, appointment books, and any other listings that link participant ID numbers to other identifying information will be stored in a separate, locked file in an area with limited access or in secure, password-protected electronic files.
The informed consent model used in this study is the one established by the local Ethics Committee.
AW. Address: Endocrinology and Nutrition Dept. Complejo Hospitalario Universitario Insular Materno-Infantil Gran Canaria, Av. Marítima s/n. 35016, Las Palmas de Gran Canaria, Spain. Tel: +34 928453431. FAX: +34 928442586.
Any modifications to the protocol which may impact on the conduct of the study, potential benefit of the patient or may affect patient safety, including changes of study objectives, study design, patient population, sample sizes, study procedures, or significant administrative aspects will require a formal amendment to the protocol. Such amendment will be agreed upon approved by the Ethics Committee of Las Palmas prior to implementation.
All investigators will have access to the trial data sets. Project data sets will be housed locally and will be password protected. Access to cleaned, anonimized data sets will be available to external investigators upon request. The present manuscript does not include data.
Participants may withdraw from the study for any reason at any time. In the informed consent model, a section is included for the participant to withdraw their participation if they deem it appropriate. Efforts will be made to minimize drop-outs, as described above.
The study was reviewed and approved by CEIm Provincial Hospital Universitario de Gran Canaria Dr. Negrin (HUGCDN). Barranco de la Ballena s/n. Hospital Universitario de Gran Canaria Dr. Negrı́n, Edificio de Investigación, Planta principal. 35019 Las Palmas de Gran Canaria (Las Palmas) Phone: (+34)928 450971 – 928 449071– 928 449286 Y2VpbXByb3ZscGEuc2NzQGdvYmllcm5vZGVjYW5hcmlhcy5vcmc=. The patients/participants provided their written informed consent to participate in this study.
DA-M participated in the design of the study, provided MI training for practitioners, contacted the participants by phone, performed the interviews to complete the questionnaires, and wrote the first draft of this article. MB participated in the study design, received MI training, recruited patients, applied MI to the participants, and contributed to the writing of this article. MP received MI training, recruited patients, and applied MI to the participants. MA-G received MI training and conducted interviews to complete the questionnaires. AW participated in the design of the study, received MI training, recruited patients, applied the MI to the participants, and contributed to the writing of this article. YR-F designed the statistical plan. All authors contributed to the article and approved the submitted version.
This work is supported by and unrestricted grant from the Menarini Group, Spain, as well as by a competitive, peer-reviewed grant from Fundación Mapfre Guanarteme [PI 2019], Las Palmas de Gran Canaria, Spain. The funders have had no role in the design of the trial and will have no role in the collection, analysis or interpretation of the data, nor in the preparation or publication of the manuscripts related to this trial.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This article was submitted as a preprint to Research Square as Alvarado-Martel et al. 2020 (44).
MI, motivational interviewing; MINT, Motivational Interviewing Network of Trainers; T1D, type 1 diabetes; T2D, type 2 diabetes.
1. American Association of Diabetes Educators. AADE7 Self-Care Behaviors. Diabetes Educ (2008) 34:445–9. doi: 10.1177/0145721708316625
2. Anderson RM, Funnell MM. Patient empowerment: reflections on the challenge of fostering the adoption of a new paradigm. Patient Educ Couns (2005) 57:153–7. doi: 10.1016/j.pec.2004.05.008
3. Borus JS, Laffel L. Adherence challenges in the management of type 1 diabetes in adolescents: prevention and intervention. Curr Opin Pediatr (2010) 22:405–11. doi: 10.1097/MOP.0b013e32833a46a7
4. Alvarado-Martel D, Velasco R, Sánchez-Hernández RM, Carrillo A, Nóvoa FJ, Wägner AM. Quality of life and type 1 diabetes: A study assessing patients’ perceptions and self-management needs. Patient Prefer Adherence (2015) 9:1315–23. doi: 10.2147/PPA.S87310
5. Alvarado-Martel D, Ruiz Fernández MA, Vigaray MC, Carrillo A, Boronat M, Montesdeoca AE, et al. Identification of psychological factors associated with adherence to self-care behaviors amongst patients with type 1 diabetes. J Diabetes Res (2019) 627:6271591. doi: 10.1155/2019/6271591
6. Funnell MM, Anderson RM. Patient Empowerment: A Look Back, A Look Ahead. Diabetes Educ (2003) 29:454–64. doi: 10.1177/014572170302900310
7. Mulcahy K, Maryniuk M, Peeples M, Peyrot M, Tomky D, Weaver T, et al. Diabetes Self-Management Education Core Outcomes Measures. Diabetes Educ (2003) 29:768–83. doi: 10.1177/014572170302900509
8. Golay A, Lagger G, Chambouleyron M, Carrard I, Lasserre-Moutet A. Therapeutic education of diabetic patients. Diabetes Metab Res Rev (2008) 24(3):192–6. doi: 10.1002/dmrr.798
9. DiMatteo MR. Variations in patients’ adherence to medical recommendations: A quantitative review of 50 years of research. Med Care (2004) 42:200–9. doi: 10.1097/01.mlr.0000114908.90348.f9
10. Haas L, Maryniuk M, Beck J, Cox CE, Duker P, Edwards L, et al. National standards for diabetes self-management education and support. Diabetes Care (2014) 37(Suppl 1):1630–7. doi: 10.2337/dc14-S144
11. Beck J, Greenwood DA, Blanton L, Bollinger ST, Butcher MK, Condon JE, et al. National Standards for diabetes self-management education and support. Diabetes Educ (2018) 44:35–50. doi: 10.1177/0145721718754797
12. Miller WR, Rollnick S. La entrevista motivacional. Ediciones Paidós (3rd edition). Barcelona, Spain (2015).
13. Miller WR. Motivational Interviewing with Problem Drinkers. Behav Cogn Psychother (1983) 11:147–72. doi: 10.1017/S0141347300006583
14. Rubak S, Sandbæk A, Lauritzen T, Christensen B. Motivational interviewing: A systematic review and meta-analysis. Br J Gen Pract (2005) 55:305–12.
15. Miller WR. Applications of motivational interviewing. Motivational interviewing. In: Helping people change, 3rd ed. New York: Guilford Press (2013). doi: 10.5195/MITRIP.2013.32
16. Bóveda Fontán J, Pérula de Torres LÁ, Campiñez Navarro M, Bosch Fontcuberta JM, Barragán Brun N, Prados Castillejo JA. Current evidence on the motivational interview in the approach to health care problems in primary care. Aten Primaria (2013) 45:486–95. doi: 10.1016/j.aprim.2013.01.014
17. Lundahl B, Moleni T, Burke BL, Butters R, Tollefson D, Butler C, et al. Motivational interviewing in medical care settings: A systematic review and meta-analysis of randomized controlled trials. Patient Educ Couns (2013) 93:157–68. doi: 10.1016/j.pec.2013.07.012
18. Martins RK, McNeil DW. Review of Motivational Interviewing in promoting health behaviors. Clin Psychol Rev (2009) 29:283–93. doi: 10.1016/j.cpr.2009.02.001
19. Hettema J, Steele J, Miller WR. Motivational Interviewing. Annu Rev Clin Psychol (2005) 1:91–111. doi: 10.1146/annurev.clinpsy.1.102803.143833
20. Chen SM, Creedy D, Lin H-S, Wollin J. Effects of motivational interviewing intervention on self-management, psychological and glycemic outcomes in type 2 diabetes: A randomized controlled trial. Int J Nurs Stud (2012) 49:637–44. doi: 10.1016/j.ijnurstu.2011.11.011
21. Hawkins SY. Improving glycemic control in older adults using a videophone motivational diabetes self-management intervention. Res Theory Nurs Pract (2010) 24:217–32. doi: 10.1891/1541-6577.24.4.217
22. Christie D, Channon S. The potential for motivational interviewing to improve outcomes in the management of diabetes and obesity in paediatric and adult populations: A clinical review. Diabetes Obes Metab (2014) 16:381–7. doi: 10.1111/dom.12195
23. Viner RM, Christie D, Taylor V, Hey S. Motivational/solution-focused intervention improves HbA1c in adolescents with Type 1 diabetes: A pilot study. Diabet Med (2003) 20:739–42. doi: 10.1046/j.1464-5491.2003.00995.x
24. Channon SJ, Channon SJ, Huws-Thomas M, Huws-Thomas M, Rollnick S, Rollnick S, et al. A Multicenter Randomized Controlled Trial of Motivational Interviewing in Teenagers With Diabetes. Diabetes Care (2007) 30:1390–5. doi: 10.2337/dc06-2260
25. Gregory JW, Channon S. Motivational interviewing to improve blood-glucose control in childhood diabetes. Paediatr Child Health (2009) 19:331–4. doi: 10.1016/j.paed.2009.03.013
26. Wang YCA, Stewart SM, Mackenzie M, Nakonezny PA, Edwards D, White PC. A randomized controlled trial comparing motivational interviewing in education to structured diabetes education in teens with type 1 diabetes. Diabetes Care (2010) 33:1741–3. doi: 10.2337/dc10-0019
27. Rosenbek Minet LK, Wagner L, Lønvig EM, Hjelmborg J, Henriksen JE. The effect of motivational interviewing on glycaemic control and perceived competence of diabetes self-management in patients with type 1 and type 2 diabetes mellitus after attending a group education programme: A randomised controlled trial. Diabetologia (2011) 54:1620–9. doi: 10.1007/s00125-011-2120-x
28. Jones A, Gladstone BP, Lübeck M, Lindekilde N, Upton D, Vach W. Motivational interventions in the management of HbA1c levels: A systematic review and meta-analysis. Prim Care Diabetes (2014) 8:91–100. doi: 10.1016/j.pcd.2014.01.009
29. Dehghan-Nayeri N, Ghaffari F, Sadeghi T, Mozaffari N. Effects of Motivational Interviewing and Adherence to Treatment Regimens Among Patients with Type 1 Diabetes a Systematic Review. Diabetes Spectr (2019) 32:112–7. doi: 10.2337/ds18-0038
30. Rollnick S, Miller WR, Butler CC, Mark SA. Motivational Interviewing in Health Care: Helping Patients Change Behavior. COPD (2008) 5:203. doi: 10.1080/15412550802093108
31. Schwalbe CS, Oh HY, Zweben A. Sustaining motivational interviewing: a meta-analysis of training studies. Addiction (2014) 109:1287–94. doi: 10.1111/add.12558
32. Steinberg MP, Miller WR. Motivational Interviewing in Diabetes Care. In: Facilitating Self-Care. New York: Guidlford Press (2015).
33. Jansà M, Vidal M, Giménez M, Conget I, Galindo M, Roca D, et al. Psychometric analysis of the Spanish and Catalan versions of the Diabetes Self-Care Inventory-Revised version questionnaire. Patient Prefer Adherence (2013) 7:997–1005. doi: 10.2147/PPA.S50271
34. Jerusalem M, Schwarzer R. Self-efficacy as a resource factor in stress appraisal processes. IRS, editor. Washington: DC: Hemisphere (1992). p. 195–213.
35. Baessler R, Schwarcer J. Evaluación de la autoeficacia: Adaptación española de la escala de Autoeficacia General Vol. 2. Ansiedad y Estrés (1996) p. 1–8.
36. Alvarado-Martel D, Ruiz Fernández MA, Vigaray MC, Carrillo A, Boronat M, Montesdeoca AE, et al. ViDa1: The development and validation of a new questionnaire for measuring health-related quality of life in patients with type 1 diabetes. Front Psychol (2017) 8:904. doi: 10.3389/fpsyg.2017.00904
37. Campiñez Navarro M, Pérula de Torres LÁ, Bosch Fontcuberta JM, Barragán Brun N, Arbonies Ortiz JC, Novo Rodríguez JM, et al. Measuring the quality of motivational interviewing in primary health care encounters: The development and validation of the motivational interviewing assessment scale (MIAS). Eur J Gen Pract (2016) 22:182–8. doi: 10.1080/13814788.2016.1177508
38. McCullagh P, Nelder JA. Generalized Linear Models. London, UK: Chapman & Hall (1983, 1989). doi: 10.1007/978-1-4899-3244-0
39. Finucane MM, Samet JH, Horton NJ. Translational methods in biostatistics: linear mixed effect regression models of alcohol consumption and HIV disease progression over time. Epidemiol Perspect Innov (2007) 4:8. doi: 10.1186/1742-5573-4-8
40. Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. Ann Intern Med (2001) 134:657–62. doi: 10.7326/0003-4819-134-8-200104170-00011
41. White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med (2011) 30(4):377–99. doi: 10.1002/sim.4067
43. Ismail K, Maissi E, Thomas S, Chalder T, Schmidt U, Bartlett J, et al. A randomised controlled trial of cognitive behaviour therapy and motivational interviewing for people with type 1 diabetes mellitus with persistent sub-optimal glycaemic control: A diabetes and psychological therapies (ADaPT) study. Health Technol Assess (2010) 14(22):1–101. doi: 10.3310/hta14220
44. Alvarado-Martel D, Boronat M, Alberiche MP, Algara MA, Wägner AM. Motivational Interviewing and Self-care in Type 1 Diabetes:a randomized controlled clinical trial study protocol. Research Square [Preprint] (2020). Available at: https://www.researchsquare.com/article/rs-12241/v1 (Accessed 24th June 2020).
Keywords: type diabetes 1, adherence, self-care, motivational interviewing, self-efficacy, health related quality of life, randomised controlled trial
Citation: Alvarado-Martel D, Boronat M, Alberiche-Ruano MdP, Algara-González MA, Ramallo-Fariña Y and Wägner AM (2020) Motivational Interviewing and Self-Care in Type 1 Diabetes: A Randomized Controlled Clinical Trial Study Protocol. Front. Endocrinol. 11:574312. doi: 10.3389/fendo.2020.574312
Received: 19 June 2020; Accepted: 06 November 2020;
Published: 10 December 2020.
Edited by:
Andrea Icks, Heinrich Heine University of Düsseldorf, GermanyReviewed by:
Burkhard Haastert, mediStatistica, Neuenrade, GermanyCopyright © 2020 Alvarado-Martel, Boronat, Alberiche-Ruano, Algara-González, Ramallo-Fariña and Wägner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana M. Wägner, YW5hLndhZ25lckB1bHBnYy5lcw==; Dácil Alvarado-Martel, ZGFjaWwuYWx2YXJhZG9AdWxwZ2MuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.