
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol. , 03 July 2020
Sec. Translational and Clinical Endocrinology
Volume 11 - 2020 | https://doi.org/10.3389/fendo.2020.00430
This article is part of the Research Topic Advances in Endocrinology: Stem Cells and Growth Factors View all 8 articles
 Babak Arjmand1,2†
Babak Arjmand1,2† Masoumeh Sarvari2
Masoumeh Sarvari2 Sepideh Alavi-Moghadam1
Sepideh Alavi-Moghadam1 Moloud Payab3†
Moloud Payab3† Parisa Goodarzi4Kambiz Gilany5,6,7†Neda Mehrdad8
Parisa Goodarzi4Kambiz Gilany5,6,7†Neda Mehrdad8 Bagher Larijani9*†
Bagher Larijani9*†The field of cell therapy and regenerative medicine can hold the promise of restoring normal tissues structure and function. Additionally, the main targets of stem cell-based therapies are chronic diseases and lifelong disabilities without definite cures such as osteoporosis. Osteoporosis as one of the important causes of morbidity in older men and post-menopausal women is characterized by reduced bone quantity or skeletal tissue atrophy that leads to an increased risk of osteoporotic fractures. The common therapeutic methods for osteoporosis only can prevent the loss of bone mass and recover the bone partially. Nevertheless, stem cell-based therapy is considered as a new approach to regenerate the bone tissue. Herein, mesenchymal stem cells as pivotal candidates for regenerative medicine purposes especially bone regeneration are the most common type of cells with anti-inflammatory, immune-privileged potential, and less ethical concerns than other types of stem cells which are investigated in osteoporosis. Based on several findings, the mesenchymal stem cells effectiveness near to a great extent depends on their secretory function. Indeed, they can be involved in the establishment of normal bone remodeling via initiation of specific molecular signaling pathways. Accordingly, the aim herein was to review the effects of stem cell-based therapies in osteoporosis.
Osteoporosis as a chronic and long-term skeletal disorder is more common in senile people (in men after age 65 and women after age 55 years) (1–4). Accordingly, it is responsible for most of the elderly fractures through decreasing the bone mass and mineral density (BMD) (1, 5, 6). Moreover, it has been reported that osteoporosis occurs when there is an imbalance between bone cells function (7, 8). In 1993, osteoporosis is defined as “progressive systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture” by WHO (9–12). The proximal ends of the humerus and femur, the distal end of the radius, and the vertebral column are more susceptible to the osteoporotic fractures in contrast to other parts of the bone (13–15). Additionally, the hip fracture can be considered as the serious complication with high morbidity and mortality (15–17). Given the fact that the life expectancy universally is increasing and subsequently osteoporosis becomes a growing global problem with a great impact on quality of life, selecting powerful approaches for disease managing is essential. In this respect, there is no practical pharmaceutical cure (18). Recently, stem cell therapies have attained remarkable clinical consideration with a promising strategy for regenerative medicine and tissue engineering to treat various types of diseases including osteoporosis (19–26). Herein, discuss the effects of stem cell-based therapies in osteoporosis is the main objective of this review.
Bone as a highly dynamic tissue continuously undergoes modeling and remodeling via activation of bone cells (osteoblasts, osteoclast, and osteocytes) (Figure 1) (40–42). Herein, modeling is defined as separately happening of bone formation and resorption on the bone surface and remodeling is known as the coupling between bone formation and resorption for regeneration (43–46). The process of developing new bone material by osteoblasts is called bone formation (ossification or osteogenesis) which commences about 6 weeks after fertilization in embryos. There are two types of bone formation, including intramembranous and endochondral (27, 47). During intramembranous bone formation, mesenchymal stem cells (MSCs) are proliferated and differentiated into osteoblasts in areas of embryonic connective tissue which contain high vascularization. Additionally, the intramembranous bone formation that is involved in the formation of the flat bones of the clavicles, skull, and the mandible is known as a procedure of bone formation from fibrous membranes (48, 49). The endochondral bone formation is befallen at three sites including the physis, the epiphysis, and the cuboidal bones of the carpus and tarsus. It is a procedure in which the cartilage is commonly replaced by bone for the formation of the growing skeleton (50–52). In general, bone formation is controlled by various growth factors, cytokines, and hormones (40, 53, 54). Therein, osteoblasts can reply to these external signals through various signaling pathways and control the specific gene expression for cell fate determining (28, 29, 55). Accordingly, there are some signaling molecules with critical roles in osteoblast turnover including runt-related transcription factor 2 (Runx2), osterix (Osx), ß-Catenin, activating transcription factor 4 (Atf4), and activator protein 1(AP-1) family. Indeed, they have momentous roles in osteoblast differentiation and osteoblastogenesis to promote bone formation (27–33). Moreover, it has been demonstrated that fibroblast growth factors (FGFs), transforming growth factor β (TGF β), insulin-like growth factor 1 (IGF-1), bone morphogenetic proteins (BMPs), Notch, Wnt, and parathyroid hormone (PTH) have effective roles in the bone formation process (56–59). Bone formation and resorption must be balanced for bone mass maintenance (34, 38, 39). Bone resorption is the process of minerals dissolution and organic matrix degradation by osteoclasts, which depends on the osteoclasts secretions into the extracellular space (60–63). Some more important types of osteoclasts secretions are lysosomal enzymes (e.g., cathepsin K) and matrix metallopeptidase 9 (MMP-9) (41, 64, 65). Osteoclasts arise from the hematopoietic stem cells (HSC) via stimulation of receptor activation of NF-κB ligand (RANKL) and the monocyte/macrophage colony-stimulating factor (M-CSF) from osteoblasts membrane surface (60, 66, 67). RANKL and M-CSF are interacted with their receptors present on osteoclast precursors to stimulate osteoclast proliferation and differentiation (60, 68, 69). However, there is another signaling molecule called osteoprotegerin (OPG) which is also secreted by osteoblasts to interfere with the RANKL for inhibition of osteoclastogenesis (70–73). According to investigations, some inflammatory cytokines e.g., interleukin1 (IL-1), interlukin-6 (IL-6), and tumor necrosis factor-α (TNFα) can be involved in osteoclast differentiation and function (34–37). Several findings have indicated that imbalance between osteoclasts and osteoblasts functions can lead to some skeletal disorders including osteoporosis. In fact, these disorders are the consequence of decreased in osteoblast activity and/or increased in osteoclast activity (8, 41).
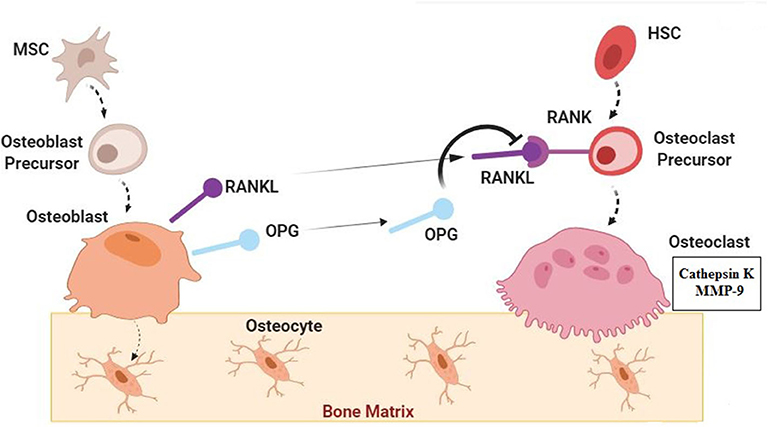
Figure 1. Normal Bone Biology; Signaling Pathways. Bone as a dynamic tissue undergoes modeling and remodeling by activation of osteoblasts, osteoclast, and osteocytes. Mesenchymal stem cells (MSCs) are proliferated and differentiated into osteoblasts. Some signaling molecules have important roles in osteoblast turnover and function including runt-related transcription factor 2 (Runx2), osterix (Osx), ß-Catenin, activating transcription factor 4(Atf4), activator protein 1(AP-1) family, fibroblast growth factors (FGFs), transforming growth factor β (TGF β), insulin-like growth factor 1 (IGF-1), bone morphogenetic proteins (BMPs), Notch, Wnt, and parathyroid hormone (PTH) (27–33). Osteoblasts which are trapped in the bone matrix are called osteocytes. Osteoclasts are derived from the hematopoietic stem cells (HSC) through the stimulation by receptor activation of NF-κB ligand (RANKL) from osteoblasts. Osteoprotegerin (OPG) which is also secreted by osteoblasts can interfere with the RANKL and inhibit osteoclastogenesis. Osteoclasts can secrete cathepsin K and matrix metallopeptidase 9 (MMP-9) in extracellular space. Some inflammatory cytokines such as. interleukin1 (IL-1), interlukin-6 (IL-6), and tumor necrosis factor-α (TNFα) can be involved in osteoclast differentiation and function (34–37). In normal condition Bone formation (by osteoblasts) and resorption (by osteoclasts) are in balanced for bone mass maintenance (34, 38, 39).
As a result of the aging process, reduction in osteoblast number, function, and longevity, lead to bone formation decreasing However, bone resorption is exceeded due to sex hormones defection. Accordingly, individuals are predisposed to osteoporosis and osteoporotic bone fractures (74–77). In fact, osteoporotic bones due to low bone mass are fragile and brittle. The compression fractures of the vertebrae and traumatic fractures of the femoral neck and the wrist are the main issues of osteoporosis. Nevertheless, the hip fractures due to their burden are more considerable and need more attention. It is estimated that by 2050 the number of hip fractures will be more than 6 million and almost the 75% of them will be occurred in the developing countries (9). Osteoporosis can be followed by various complications and disorders. Usually, low levels of estrogen in post-menopausal women is the most well-known factor (78). In clinical diagnostic techniques of osteoporosis, dual x-ray absorptiometry [DXA] is approved as a gold standard approach to diagnose and follow the osteoporosis by calculating BMD (79). The WHO defines a set of categories to diagnose osteopenia and osteoporosis. These guidelines are based on T-score and Z-score. T-score shows the number of standard deviations above or below the mean reference value for 30 year-old healthy adults. However, Z-score measures the BMD regards to the average BMD of the same age and gender (80). According to the guidelines, a score above −1 is considered normal, a score between −1 and −2.5 indicates osteopenia, and a score below −2.5 portends the osteoporosis (79). Hereupon, for individuals with osteoporosis diagnosed, various treatments are recommended to increase the quality of life and decrease the economic burden on health care system (1).
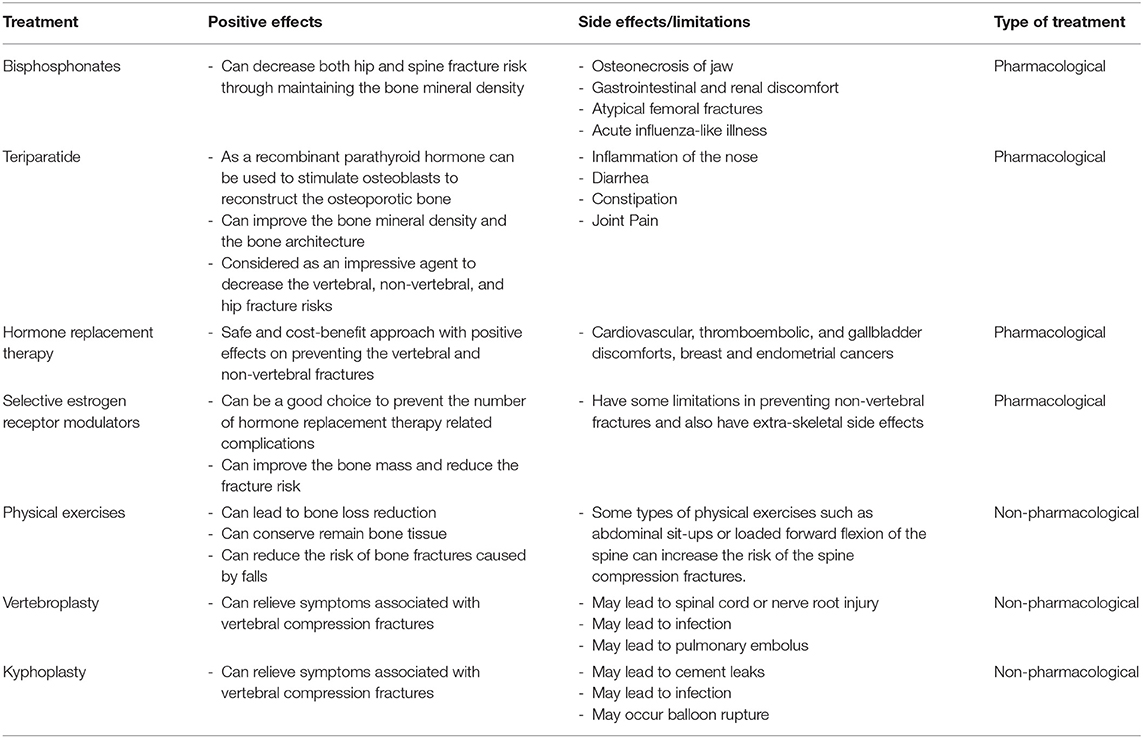
Osteoporosis cannot be cured but some of the pharmacological and non-pharmacological treatment approaches can manage it (Table 1) through the strengthening the bones and preventing the consequent fractures. In this context, using bisphosphonates, selective estrogen receptor modulators (SERMs), teriparatide, denosumab, calcitonin, and hormone replacement therapy (HRT) are the approved methods as the pharmacological treatments for osteoporosis (94). Additionally, some of the non-pharmacological treatments are including nutritional therapy, physical exercises, vertebroplasty, and kyphoplasty. Despite the preventive and therapeutical effects of these treatments, there are some limitations and side effects around using them. Hence, it is needed to apply new and more effective approaches with fewer side effects for osteoporosis management.
The clinical demand for new therapeutic methods has been led to progress in stem cell therapy and regenerative medicine (23, 95). In other words, stem cell-based therapies are becoming increasingly important in treatment of chronic and long-lasting diseases (96, 97). However, there are several parameters which need to be optimized for maximizing stem cell-based therapies potential. In this context, various basic and clinical studies related to the effects of stem cell-based therapies on diseases with no definite treatments were performed (22, 98, 99). Accordingly, some investigations were also conducted in the field of stem cell therapy for osteoporosis. Herein, the application of different types of stem cells including embryonic, induced pluripotent, and MSCs along with their secretion factors were evaluated to treat osteoporosis (100–102).
Osteoporosis is a multifactorial disorder with endogenous and exogenous components (103, 104). Cell-based regenerative medicine can be invaluable in osteoporosis treatment through bone resorption modulation, fractures susceptibility reduction, and lost mineral density enhancement. These are possible by increasing the number of progenitor stem cells and improve the function of stem cells (proliferation and differentiation into bone-forming cells) (20, 102, 105, 106). Since the bone tissue repair cascade can be controlled by local signals from various cytokines and growth factors through the inducing osteoprogenitor cells migration, differentiation, proliferation, revascularization, and extracellular matrix production (56, 107, 108), stem cells (especially MSCs) can support bone regeneration by secreting bioactive molecules such as IGF-1, TGF-β, vascular endothelial growth factor (VEGF), angiogenin, hepatocyte growth factor (HGF), IL-6, and etc. (56, 109–113). On the other hand, MSCs derived exosomes are other factors which their effects on preventing the bone loss and promoting bone remodeling processes (during osteogenesis, osteoclastogenesis, and angiogenesis) have been demonstrated in vitro and in vivo (114–116).
Although particular protocols are demanded to direct differentiation of embryonic stem cells (ESCs) (from the inner cell mass of a blastocyst) and induced pluripotent stem cells (iPSCs) (embryonic–like stem cells reprogrammed from adult cells) toward the osteoblasts and osteocyte-like cells (bone-forming cells), some of investigations were shown that application of these most known pluripotent stem cells in osteoporosis treatment is limited due to ethical concerns (20, 117, 118). Recently, implementation of very small embryonic-like stem cells (VSELs) (non-hematopoietic pluripotent cells that express embryonic characteristics markers and stored during the organogenesis in organs and tissues) as the autologous treatment for decreasing the aging processes which lead to osteoporosis and other skeletal disorders is taken into consideration. However, according to some studies, VSELs population will decrease with aging (20, 119, 120).
In osteoporosis, there is a reduction in endogenous MSCs function (proliferation, differentiation, and consequently bones formation). Accordingly, they are the most common types of stem cells investigated in osteoporosis treatment. In this respect, examples of MSCs transplantation in osteoporotic animal models and humans were shown in Table 2. MSCs are an important example of non-hematopoietic stem cells with less ethical concerns and numerous advantages for clinical usage, containing accessibility and ease of harvesting, immunosuppressive outcomes, multi-lineal differentiation ability (especially ability to differentiate into osteoblasts), and any possibility of malignant transformation (21, 131–133). Additionally, as a subset of stromal stem cells, they can be obtained from various tissue sources. Bone marrow derive MSCs (BM-MSCs) with high osteogenic differentiation capability are the most common types of MSCs which have been used for osteoporosis (20, 24, 134–136). Herein, accumulating evidence indicates that alternation in the molecular mechanisms which modulate osteoblast differentiation in MSCs will make the MSC therapies reliable and more effective for osteoporosis (105, 137–139). While in accordance with other studies the most therapeutic impressions of MSCs are due to their supporting regenerative microenvironment ability and paracrine effects rather than their differentiation ability. In other words, MSC transplantation might open a new chapter in osteoporosis treatment specifically through paracrine effects (Figure 2) (140–143).

Table 2. Examples of MSCs transplantation in osteoporotic animal models and humans.
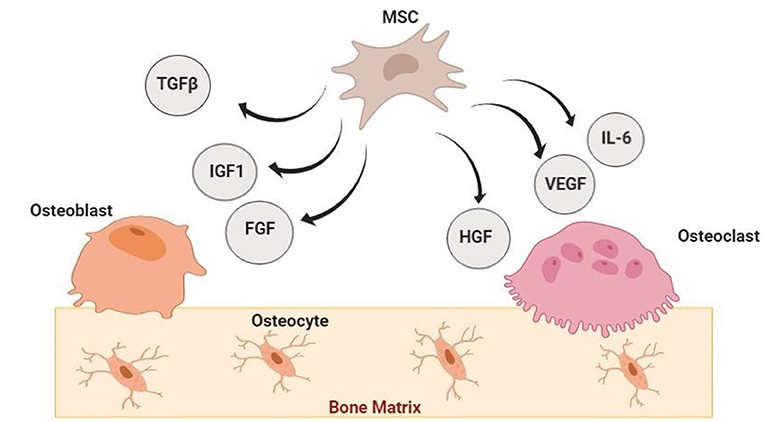
Figure 2. Paracrine Effects of Mesenchymal Stem Cells in Bone Regeneration. Mesenchymal stem cells (MSCs) can participate in bone regeneration by secreting bioactive molecules such as Insulin-like growth factor 1 (IGF-1), Transforming growth factor β (TGF-β), vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF), interleukin−6 (IL-6), and fibroblast growth factor (FGF) (140–143).
The burden of osteoporosis is raised by an increase in the proportion of older persons in societies. Routine treatments only alleviate the symptoms partially. Hence, they are not sufficient enough. Therein, regenerative medicine sheds light on the treatment of osteoporosis. Specifically, MSCs therapy is the most common technique of regenerative medicine in osteoporosis treatment. Moreover, using small molecules (e.g., PTH and oxytocin) which employ endogenous stem cells for osteoporosis treatment will be intertwined in future management (20, 144). Despite the many investigations in cell therapy for osteoporosis, further studies are still demanded to fulfill the gaps including the definite differentiation fate and biodistribution of transplanted stem cells. On the other hand, in accordance with growing advances in osteoporosis personalized medicine (the applying of specific medical treatment based on the individual characteristics of each patient), it is required to identify the important bone loss signaling pathways and genes involved in each individual (145–148). In this context, metabolomics evaluation (the principled investigation of small molecules profile in a biological system) (149, 150) also can be helpful to the osteoporosis diagnosis of individuals with a genetic capacity (151, 152). Additionally, the biomedical using of exosomal based treatments will present novel approaches in clinical practice for osteoporosis (116).
BA contributed substantially to the conception and design of the study. MP conducted search strategy and data collection. MS and SA-M drafted critical revision of the article. PG and KG revised the article critically for important intellectual content. NM gave final approval of the version to be submitted and any revised version. BL agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank Dr. Mohsen Khorshidi and Shokouh Salimi for their considerable assistance.
BMD, Bone Mineral Density; WHO, World Health Organization; MSCs, Mesenchymal Stem Cells; Runx2, Runt-related transcription factor 2; OSX, Osterix; Atf4, Activating transcription factor 4; AP-1, Activator Protein 1; FGFs, Fibroblast Growth Factors; TGF-β, Transforming Growth Factor β; IGF-1, Insulin-like Growth Factor 1; BMP, Bone Morphogenetic Protein; PTH, Parathyroid hormone; MMP-9, Matrix Metallopeptidase 9; M-CSF, Monocyte/Macrophage Colony-Stimulating Factor; OPG, Osteoprotegerin; HSC, Hematopoietic Stem Cells; IL-1, Interleukin1; Il-6, Interleukin 6; TNFα, Tumor Necrosis Factor α; DXA, Dual X-ray Absorptiometry; SERMs, Selective Estrogen Receptor Modulators; IV, Intravenous; HRT, Hormone Replacement Therapy; VEGF, Vascular Endothelial Growth Factor; HGF, Hepatocyte Growth Factor; ESCs, Embryonic Stem Cells; iPSCs, induced Pluripotent Stem Cells; VELs, Very small Embryonic-Like stem cells; BM- MSCs, Bone Marrow Mesenchymal Stem Cells.
1. Sözen T, Özişik L, Başaran NÇ. An overview and management of osteoporosis. Eur J Rheumatol. (2017) 4:46. doi: 10.5152/eurjrheum.2016.048
2. Curtis JR, Safford MM. Management of osteoporosis among the elderly with other chronic medical conditions. Drugs Aging. (2012) 29:549–64. doi: 10.2165/11599620-000000000-00000
3. Alswat KA. Gender disparities in osteoporosis. J Clin Med Res. (2017) 9:382. doi: 10.14740/jocmr2970w
4. Compston JE, McClung MR, Leslie WD. Osteoporosis. Lancet. (2019) 393:364–76. doi: 10.1016/S0140-6736(18)32112-3
5. Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. (2002) 359:1761–7. doi: 10.1016/S0140-6736(02)08657-9
6. Dobbs MB, Buckwalter J, Saltzman C. Osteoporosis: the increasing role of the orthopaedist. Iowa Orthopaed J. (1999) 19:43.
7. Letarouilly J-G, Broux O, Clabaut A. New insights into the epigenetics of osteoporosis. Genomics. (2019) 111:793–8. doi: 10.1016/j.ygeno.2018.05.001
8. Feng X, McDonald JM. Disorders of bone remodeling. Ann Rev Pathol Mech Dis. (2011) 6:121–45. doi: 10.1146/annurev-pathol-011110-130203
9. Genant HK, Cooper C, Poor G, Reid I, Ehrlich G, Kanis J, et al. Interim report and recommendations of the World Health Organization task-force for osteoporosis. Osteopor Int. (1999) 10:259. doi: 10.1007/s001980050224
10. Todd J, Robinson R. Osteoporosis and exercise. Postgrad Med J. (2003) 79:320–3. doi: 10.1136/pmj.79.932.320
11. Binkley N. Osteoporosis in men. Arquivos Brasil Endocrinol Metabol. (2006) 50:764–74. doi: 10.1590/S0004-27302006000400021
12. Bawa Se. The significance of soy protein and soy bioactive compounds in the prophylaxis and treatment of osteoporosis. J Osteopor. (2010). 2010:891058. doi: 10.4061/2010/891058
13. Nuti R, Brandi ML, Checchia G, Di Munno O, Dominguez L, Falaschi P, et al. Guidelines for the management of osteoporosis and fragility fractures. Intern Emerg Med. (2019) 14:85–102. doi: 10.1007/s11739-018-1874-2
14. Bono CM, Einhorn TA. Overview of osteoporosis: pathophysiology and determinants of bone strength. Eur Spine J. (2003) 12(Suppl. 2):S90–6. doi: 10.1007/s00586-003-0603-2
15. Osterhoff G, Morgan EF, Shefelbine SJ, Karim L, McNamara LM, Augat P. Bone mechanical properties and changes with osteoporosis. Injury. (2016) 47:S11–20. doi: 10.1016/S0020-1383(16)47003-8
16. Carpintero P, Caeiro JR, Carpintero R, Morales A, Silva S, Mesa M. Complications of hip fractures: a review. World J Orthoped. (2014) 5:402. doi: 10.5312/wjo.v5.i4.402
17. Lee Y-K, Koo K-H. Osteoporotic hip fracture in the elderly patients: physicians' views. J Korean Med Sci. (2013) 28:976–7. doi: 10.3346/jkms.2013.28.7.976
18. Skjodt MK, Frost M, Abrahamsen B. Side effects of drugs for osteoporosis and metastatic bone disease. Br J Clin Pharmacol. (2019) 85:1063–71. doi: 10.1111/bcp.13759
19. Dzobo K, Thomford NE, Senthebane DA, Shipanga H, Rowe A, Dandara C, et al. Advances in regenerative medicine and tissue engineering: innovation and transformation of medicine. Stem Cells Int. (2018) 2018:2495848. doi: 10.1155/2018/2495848
20. Paspaliaris V, Kolios G. Stem cells in osteoporosis: from biology to new therapeutic approaches. Stem Cells Int. (2019) 2019:1730978. doi: 10.1155/2019/1730978
21. Aghebati-Maleki L, Dolati S, Zandi R, Fotouhi A, Ahmadi M, Aghebati A, et al. Prospect of mesenchymal stem cells in therapy of osteoporosis: a review. J Cell Physiol. (2019) 234:8570–8. doi: 10.1002/jcp.27833
22. Goodarzi P, Payab M, Alavi-Moghadam S, Larijani B, Rahim F, Bana N, et al. Development and validation of Alzheimer's Disease animal model for the purpose of regenerative medicine. Cell Tissue Bank. (2019) 20:141–51. doi: 10.1007/s10561-019-09773-8
23. Goodarzi P, Aghayan HR, Payab M, Larijani B, Alavi-Moghadam S, Sarvari M, et al. Human fetal skin fibroblast isolation and expansion for clinical application. Methods Mol Biol. (2019) 2109:261–73. doi: 10.1007/7651_2019_233
24. Goodarzi P, Falahzadeh K, Aghayan H, Payab M, Larijani B, Alavi-Moghadam S, et al. Therapeutic abortion and ectopic pregnancy: alternative sources for fetal stem cell research and therapy in Iran as an Islamic country. Cell Tissue Bank. (2019) 20:11–24. doi: 10.1007/s10561-018-9741-y
25. Payab M, Goodarzi P, Heravani NF, Hadavandkhani M, Zarei Z, Falahzadeh K, et al. Stem cell and obesity: current state and future perspective. Cell Biol Transl Med. (2018) 2:1–22. doi: 10.1007/5584_2018_227
26. Goodarzi P, Aghayan HR, Larijani B, Soleimani M, Dehpour A-R, Sahebjam M, et al. Stem cell-based approach for the treatment of Parkinson's disease. Med J Islamic Repub Iran. (2015) 29:168.
27. Nakashima K, de Crombrugghe B. Transcriptional mechanisms in osteoblast differentiation and bone formation. Trends Genet. (2003) 19:458–66. doi: 10.1016/S0168-9525(03)00176-8
28. Fung Ling Chau J, Fook Leong W, Li B. Signaling pathways governing osteoblast proliferation, differentiation and function. Histol Histopathol. (2009) 24:1593–606. doi: 10.14670/HH-24.1593
29. Huang W, Yang S, Shao J, Li YP. Signaling and transcriptional regulation in osteoblast commitment and differentiation. Front Biosci. (2007) 12:3068. doi: 10.2741/2296
30. Yu S, Franceschi RT, Luo M, Fan J, Jiang D, Cao H, et al. Critical role of activating transcription factor 4 in the anabolic actions of parathyroid hormone in bone. PloS ONE. (2009) 4:e7583. doi: 10.1371/journal.pone.0007583
31. Meyer MB, Benkusky NA, Pike JW. The RUNX2 cistrome in osteoblasts characterization, down-regulation following differentiation, and relationship to gene expression. J Biol Chem. (2014) 289:16016–31. doi: 10.1074/jbc.M114.552216
32. Long F. Building strong bones: molecular regulation of the osteoblast lineage. Nat Rev Mol Cell Biol. (2012) 13:27–38. doi: 10.1038/nrm3254
33. Soltanoff CS, Chen W, Yang S, Li YP. Signaling networks that control the lineage commitment and differentiation of bone cells. Crit Rev Eukaryot Gene Exp. (2009) 19:1–46. doi: 10.1615/CritRevEukarGeneExpr.v19.i1.10
34. Parra-Torres AY, Valdés-Flores M, Orozco L, Velázquez-Cruz R. Molecular aspects of bone remodeling. Topics in Osteoporosis. Rijeka: INTECH. (2013). p. 1–27.
35. Azuma Y, Kaji K, Katogi R, Takeshita S, Kudo A. Tumor necrosis factor-α induces differentiation of and bone resorption by osteoclasts. J Biol Chem. (2000) 275:4858–64. doi: 10.1074/jbc.275.7.4858
36. Yokota K, Sato K, Miyazaki T, Kitaura H, Kayama H, Miyoshi F, et al. Combination of tumor necrosis factor α and interleukin-6 induces mouse osteoclast-like cells with bone resorption activity both in vitro and in vivo. Arthr Rheumatol. (2014) 66:121–9. doi: 10.1002/art.38218
37. Zhao R. Immune regulation of osteoclast function in postmenopausal osteoporosis: a critical interdisciplinary perspective. Int J Med Sci. (2012) 9:825. doi: 10.7150/ijms.5180
38. Lorincz C, Manske SL, Zernicke R. Bone health: part 1, nutrition. Sports Health. (2009) 1:253–60. doi: 10.1177/1941738109334213
39. Dunstan CR, Blair JM, Zhou H, Seibel MJ. Bone, mineral, connective tissue metabolism. Oxford: Elsevier (2007). p. 495–520.
40. Florencio-Silva R, Sasso GRS, Sasso-Cerri E, Simões MJ, Cerri PS. Biology of bone tissue: structure, function, and factors that influence bone cells. Biomed Res Int. (2015) 2015:421746. doi: 10.1155/2015/421746
41. Bilezikian JP, Raisz LG, Martin TJ. Principles of Bone Biology. New York, NY: Academic press (2008).
43. Sims NA, Gooi JH (editors). Bone remodeling: multiple cellular interactions required for coupling of bone formation and resorption. Semin Cell Dev Biol. (2008) 19:444–51. doi: 10.1016/j.semcdb.2008.07.016
44. Allen MR, Burr DB. Bone modeling and remodeling. Basic Appl Bone Biol. (2014) 2014:75–90. doi: 10.1016/B978-0-12-416015-6.00004-6
45. Langdahl B, Ferrari S, Dempster DW. Bone modeling and remodeling: potential as therapeutic targets for the treatment of osteoporosis. Ther Adv Musculoskel Dis. (2016) 8:225–35. doi: 10.1177/1759720X16670154
46. Sims NA, Martin TJ. Coupling the activities of bone formation and resorption: a multitude of signals within the basic multicellular unit. BoneKEy Rep. (2014) 3:481. doi: 10.1038/bonekey.2013.215
47. Caetano-Lopes J, Canhao H, Eurico Fonseca J. Osteoblasts and bone formation. Acta Reumatol Portuguesa. (2007) 32:103–10.
48. Lonergan SM, Topel DG, Marple DN. The Science of Animal Growth and Meat Technology. Ames, IA: Academic Press (2018).
49. Netter FH. Musculoskeletal System: Anatomy, Physiology, and Metabolic Disorders. Summit, NJ: Ciba-Geigy Corp. (1987). p. 169.
50. Brighton CT, Sugioka Y, Hunt RM. Cytoplasmic structures of epiphyseal plate chondrocytes. Quantitative evaluation using electron micrographs of rat costochondral junctions with special reference to the fate of hypertrophic cells. J Bone Joint Surg Am. (1973) 55:771–84. doi: 10.2106/00004623-197355040-00012
51. Labens R, Schramme MC, Barr AR. Orthopaedics 1: diagnosis of lameness/diseases of joints and bones. In: Mair T, Love S, Schumacher J, Smith R, Frazer G, editors. Equine Medicine, Surgery and Reproduction. Oxford: W.B. Saunders (2013). p. 309–28.
52. de Crombrugghe B, Lefebvre V, Nakashima K. Regulatory mechanisms in the pathways of cartilage and bone formation. Curr Opin Cell Biol. (2001) 13:721–8. doi: 10.1016/S0955-0674(00)00276-3
53. Javed A, Chen H, Ghori FY. Genetic and transcriptional control of bone formation. Oral Maxillofacial Surg Clin. (2010) 22:283–93. doi: 10.1016/j.coms.2010.05.001
54. Lee SH, Kim TS, Choi Y, Lorenzo J. Osteoimmunology: cytokines and the skeletal system. BMB Rep. (2008) 41:495. doi: 10.5483/BMBRep.2008.41.7.495
55. Hayrapetyan A, Jansen JA, van den Beucken JJ. Signaling pathways involved in osteogenesis and their application for bone regenerative medicine. Tissue Eng Part B Rev. (2015) 21:75–87. doi: 10.1089/ten.teb.2014.0119
56. Linkhart TA, Mohan S, Baylink DJ. Growth factors for bone growth and repair: IGF, TGFβ and BMP. Bone. (1996) 19:S1–2. doi: 10.1016/S8756-3282(96)00138-X
57. Tan S, Zhang B, Zhu X, Ao P, Guo H, Yi W, et al. Deregulation of bone forming cells in bone diseases and anabolic effects of strontium-containing agents and biomaterials. Biomed Res Int. (2014) 2014:814057. doi: 10.1155/2014/814057
58. Marie PJ, Kassem M. Osteoblasts in osteoporosis: past, emerging, and future anabolic targets. Eur J Endocrinol. (2011) 165:1. doi: 10.1530/EJE-11-0132
59. Yuan J, Xin F, Jiang W. Underlying signaling pathways and therapeutic applications of pulsed electromagnetic fields in bone repair. Cell Physiol Biochem. (2018) 46:1581–94. doi: 10.1159/000489206
61. Hienz SA, Paliwal S, Ivanovski S. Mechanisms of bone resorption in periodontitis. J Immunol Res. (2015) 2015:615486. doi: 10.1155/2015/615486
63. Teitelbaum SL. Bone resorption by osteoclasts. Science. (2000) 289:1504–8. doi: 10.1126/science.289.5484.1504
64. Dong Z, Bonfil RD, Chinni S, Deng X, Trindade Filho JC, Bernardo M, et al. Matrix metalloproteinase activity and osteoclasts in experimental prostate cancer bone metastasis tissue. Am J Pathol. (2005) 166:1173–86. doi: 10.1016/S0002-9440(10)62337-1
65. Henriksen K, Bollerslev J, Everts V, Karsdal MA. Osteoclast activity and subtypes as a function of physiology and pathology—implications for future treatments of osteoporosis. Endocr Rev. (2011) 32:31–63. doi: 10.1210/er.2010-0006
66. Udagawa N, Takahashi N, Jimi E, Matsuzaki K, Tsurukai T, Itoh K, et al. Osteoblasts/stromal cells stimulate osteoclast activation through expression of osteoclast differentiation factor/RANKL but not macrophage colony-stimulating factor. Bone. (1999) 25:517–23. doi: 10.1016/S8756-3282(99)00210-0
67. Yamashita T, Takahashi N, Udagawa N. New roles of osteoblasts involved in osteoclast differentiation. World J Orthoped. (2012) 3:175. doi: 10.5312/wjo.v3.i11.175
68. Ross FP. M-CSF, c-Fms, and signaling in osteoclasts and their precursors. Ann N Y Acad Sci. (2006) 1068:110–6. doi: 10.1196/annals.1346.014
69. Park JH, Lee NK, Lee SY. Current understanding of RANK signaling in osteoclast differentiation and maturation. Mol Cells. (2017) 40:706–13. doi: 10.14348/molcells.2017.0225
70. Chen X, Wang Z, Duan N, Zhu G, Schwarz EM, Xie C. Osteoblast–osteoclast interactions. Connect Tissue Res. (2018) 59:99–107. doi: 10.1080/03008207.2017.1290085
71. Wright HL, McCarthy HS, Middleton J, Marshall MJ. RANK, RANKL and osteoprotegerin in bone biology and disease. Curr Rev Musculoskelet Med. (2009) 2:56–64. doi: 10.1007/s12178-009-9046-7
72. Faccio R, Choi Y, Teitelbaum SL, Takayanagi H. The osteoclast: the pioneer of osteoimmunology. Osteoimmunology. (2011) 2011:141–85. doi: 10.1016/B978-0-12-375670-1.10006-8
73. Boyce BF, Xing L. Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res Ther. (2007) 9:S1. doi: 10.1186/ar2165
74. Rachner TD, Khosla S, Hofbauer LC. Osteoporosis: now and the future. Lancet. (2011) 377:1276–87. doi: 10.1016/S0140-6736(10)62349-5
76. Demontiero O, Vidal C, Duque G. Aging and bone loss: new insights for the clinician. Ther Adv Musculoskelet Dis. (2012) 4:61–76. doi: 10.1177/1759720X11430858
77. Lai P, Song Q, Yang C, Li Z, Liu S, Liu B, et al. Loss of Rictor with aging in osteoblasts promotes age-related bone loss. Cell Death Dis. (2016) 7:e2408. doi: 10.1038/cddis.2016.249
78. Peris P, Guanabens N, Monegal A, Suris X, Alvarez L, De Osaba MM, et al. Aetiology and presenting symptoms in male osteoporosis. Rheumatology. (1995) 34:936–41. doi: 10.1093/rheumatology/34.10.936
79. El-Desouki MI. Osteoporosis in postmenopausal Saudi women using dual x-ray bone densitometry. Saudi Med J. (2003) 24:953–6.
80. Dimai HP. Use of dual-energy X-ray absorptiometry (DXA) for diagnosis and fracture risk assessment; WHO-criteria, T-and Z-score, and reference databases. Bone. (2017) 104:39–43. doi: 10.1016/j.bone.2016.12.016
81. Abrahamsen B. Adverse effects of bisphosphonates. Calcified Tissue Int. (2010) 86:421–35. doi: 10.1007/s00223-010-9364-1
82. McClung MR. Bisphosphonates. Endocrinol Metab Clin North Am. (2003) 32:253–71. doi: 10.1016/S0889-8529(02)00079-8
83. Han SL, Wan SL. Effect of teriparatide on bone mineral density and fracture in postmenopausal osteoporosis: meta-analysis of randomised controlled trials. Int J Clin Pract. (2012) 66:199–209. doi: 10.1111/j.1742-1241.2011.02837.x
84. Finkelstein JS, Wyland JJ, Lee H, Neer RM. Effects of teriparatide, alendronate, or both in women with postmenopausal osteoporosis. J Clin Endocrinol Metab. (2010) 95:1838–45. doi: 10.1210/jc.2009-1703
85. An KC. Selective estrogen receptor modulators. Asian Spine J. (2016) 10:787. doi: 10.4184/asj.2016.10.4.787
86. Kulak Júnior J, Kulak CA, Taylor HS. SERMs in the prevention and treatment of postmenopausal osteoporosis: an update. Arq Brasil Endocrinol Metab. (2010) 54:200–5. doi: 10.1590/S0004-27302010000200016
87. Eriksen EF, Keaveny TM, Gallagher ER, Krege JH. Literature review: the effects of teriparatide therapy at the hip in patients with osteoporosis. Bone. (2014) 67:246–56. doi: 10.1016/j.bone.2014.07.014
88. Gambacciani M, Levancini M. Hormone replacement therapy and the prevention of postmenopausal osteoporosis. Przeglad menopauzalny Menopause Rev. (2014) 13:213. doi: 10.5114/pm.2014.44996
89. Hickey M, Elliott J, Davison SL. Hormone replacement therapy. BMJ. (2012) 344:e763. doi: 10.1136/bmj.e763
90. Marcucci G, Brandi ML. Vertebroplasty and balloon kyphoplasty in osteoporosis: friends or foes? Clin Cases Min Bone Metab. (2009) 6:203.
91. Moreira LD, Oliveira ML, Lirani-Galvão AP, Marin-Mio RV, Santos RN, Lazaretti-Castro M. Physical exercise and osteoporosis: effects of different types of exercises on bone and physical function of postmenopausal women. Arq Brasil Endocrinol Metab. (2014) 58:514–22. doi: 10.1590/0004-2730000003374
92. Kerr C, Bottomley C, Shingler S, Giangregorio L, de Freitas HM, Patel C, et al. The importance of physical function to people with osteoporosis. Osteoporosis Int. (2017) 28:1597–607. doi: 10.1007/s00198-017-3911-9
93. Levine JP. Pharmacologic and nonpharmacologic management of osteoporosis. Clin Cornerstone. (2006) 8:40–53. doi: 10.1016/S1098-3597(06)80064-5
94. Cramer JA, Gold DT, Silverman SL, Lewiecki EM. A systematic review of persistence and compliance with bisphosphonates for osteoporosis. Osteoporosis Int. (2007) 18:1023–31. doi: 10.1007/s00198-006-0322-8
95. Goodarzi P, Aghayan HR, Soleimani M, Norouzi-Javidan A, Mohamadi-Jahani F, Jahangiri S, et al. Stem cell therapy for treatment of epilepsy. Acta Med Iran. (2014) 52:651–5.
96. Aghayan HR, Goodarzi P, Arjmand B. GMP-compliant human adipose tissue-derived mesenchymal stem cells for cellular therapy. In: Walker J, editor. Stem Cells and Good Manufacturing Practices. New York, NY: Humana Press (2014). pp. 93–107.
97. Ghodsi M, Heshmat R, Amoli M, Keshtkar AA, Arjmand B, Aghayan H, et al. The effect of fetal liver-derived cell suspension allotransplantation on patients with diabetes: first year of follow-up. Acta Med Iran. (2012) 50:541–6.
98. Yu D, Silva GA. Stem cell sources and therapeutic approaches for central nervous system and neural retinal disorders. Neurosurg Focus. (2008) 24:E11. doi: 10.3171/FOC/2008/24/3-4/E10
99. Kuraitis D, Giordano C, Suuronen EJ, Ruel M. Cell therapy to regenerate the ischemic heart. Cardiac Regen Repair. (2014) 1:118–137. doi: 10.1533/9780857096708.2.118
100. Li F, Zhou C, Xu L, Tao S, Zhao J, Gu Q. Effect of stem cell therapy on bone mineral density: a meta-analysis of preclinical studies in animal models of osteoporosis. PloS ONE. (2016) 11:e0149400. doi: 10.1371/journal.pone.0149400
101. Ilic D, Miere C, Lazic E. Umbilical cord blood stem cells: clinical trials in non-hematological disorders. Br Med Bull. (2012) 102:43–57. doi: 10.1093/bmb/lds008
102. Chaparro O, Linero I. Regenerative medicine: a new paradigm in bone regeneration. Adv Techn Bone Regen. (2016) 1:253–74. doi: 10.5772/62523
103. Marini F, Cianferotti L, Brandi ML. Epigenetic mechanisms in bone biology and osteoporosis: can they drive therapeutic choices? Int J Mol Sci. (2016) 17:1329. doi: 10.3390/ijms17081329
104. Alagiakrishnan K, Juby A, Hanley D, Tymchak W, Sclater A. Role of vascular factors in osteoporosis. J Gerontol Ser A Biol Sci Med Sci. (2003) 58:M362–6. doi: 10.1093/gerona/58.4.M362
105. Phetfong J, Sanvoranart T, Nartprayut K, Nimsanor N, Seenprachawong K, Prachayasittikul V, et al. Osteoporosis: the current status of mesenchymal stem cell-based therapy. Cell Mol Biol Lett. (2016) 21:12. doi: 10.1186/s11658-016-0013-1
106. Antebi B, Pelled G, Gazit D. Stem cell therapy for osteoporosis. Curr Osteoporos Rep. (2014) 12:41–7. doi: 10.1007/s11914-013-0184-x
107. Martín-del-Campo M, Sampedro JG, Flores-Cedillo ML, Rosales-Ibañez R, Rojo L. Bone regeneration induced by strontium folate loaded biohybrid scaffolds. Molecules. (2019) 24:1660. doi: 10.3390/molecules24091660
108. Beamer B, Hettrich C, Lane J. Vascular endothelial growth factor: an essential component of angiogenesis and fracture healing. HSS J. (2010) 6:85–94. doi: 10.1007/s11420-009-9129-4
109. Xiao L, Sobue T, Esliger A, Kronenberg MS, Coffin JD, Doetschman T, et al. Disruption of the Fgf2 gene activates the adipogenic and suppresses the osteogenic program in mesenchymal marrow stromal stem cells. Bone. (2010) 47:360–70. doi: 10.1016/j.bone.2010.05.021
110. Choy L, Skillington J, Derynck R. Roles of autocrine TGF-β receptor and Smad signaling in adipocyte differentiation. J Cell Biol. (2000) 149:667–82. doi: 10.1083/jcb.149.3.667
111. Ugarte F, Ryser M, Thieme S, Fierro FA, Navratiel K, Bornhäuser M, et al. Notch signaling enhances osteogenic differentiation while inhibiting adipogenesis in primary human bone marrow stromal cells. Exp Hematol. (2009) 37:867–75. doi: 10.1016/j.exphem.2009.03.007
112. Byun MR, Jeong H, Bae SJ, Kim AR, Hwang ES, Hong JH. TAZ is required for the osteogenic and anti-adipogenic activities of kaempferol. Bone. (2012) 50:364–72. doi: 10.1016/j.bone.2011.10.035
113. James AW. Review of signaling pathways governing MSC osteogenic and adipogenic differentiation. Scientifica. (2013) 2013:684736. doi: 10.1155/2013/684736
114. Gao M, Gao W, Papadimitriou JM, Zhang C, Gao J, Zheng M. Exosomes—the enigmatic regulators of bone homeostasis. Bone Res. (2018) 6:1–3. doi: 10.1038/s41413-018-0039-2
115. Chu C, Wei S, Wang Y, Wang Y, Man Y, Qu Y. Extracellular vesicle and mesenchymal stem cells in bone regeneration: recent progress and perspectives. J Biomed Mater Res Part A. (2019) 107:243–50. doi: 10.1002/jbm.a.36518
116. Behera J, Tyagi N. Exosomes: mediators of bone diseases, protection, and therapeutics potential. Oncoscience. (2018) 5:181. doi: 10.18632/oncoscience.421
117. Csobonyeiova M, Polak S, Zamborsky R, Danisovic L. iPS cell technologies and their prospect for bone regeneration and disease modeling: a mini review. J Adv Res. (2017) 8:321–7. doi: 10.1016/j.jare.2017.02.004
118. Song L, Xie XB, Peng LK, Yu SJ, Peng YT. Mechanism and treatment strategy of osteoporosis after transplantation. Int J Endocrinol. (2015) 2015:280164. doi: 10.1155/2015/280164
119. Kassmer SH, Krause DS. Very small embryonic-like cells: biology and function of these potential endogenous pluripotent stem cells in adult tissues. Mol Reprod Dev. (2013) 80:677–90. doi: 10.1002/mrd.22168
120. Ratajczak MZ, Zuba-Surma EK, Shin DM, Ratajczak J, Kucia M. Very small embryonic-like (VSEL) stem cells in adult organs and their potential role in rejuvenation of tissues and longevity. Exp Gerontol. (2008) 43:1009–17. doi: 10.1016/j.exger.2008.06.002
121. Hong B, Lee S, Shin N, Ko Y, Kim D, Lee J, et al. Bone regeneration with umbilical cord blood mesenchymal stem cells in femoral defects of ovariectomized rats. Osteopor Sarcop. (2018) 4:95–101. doi: 10.1016/j.afos.2018.08.003
122. Hendrijantini N, Kusumaningsih T, Rostiny R, Mulawardhana P, Danudiningrat CP, Rantam FA. A potential therapy of human umbilical cord mesenchymal stem cells for bone regeneration on osteoporotic mandibular bone. Eur J Dentist. (2018) 12:358–62. doi: 10.4103/ejd.ejd_342_17
123. Diao Y, Ma Q, Cui F, Zhong Y. Human umbilical cord mesenchymal stem cells: osteogenesis in vivo as seed cells for bone tissue engineering. J Biomed Mater Res Part A. (2009) 91:123–31. doi: 10.1002/jbm.a.32186
124. Uri O, Behrbalk E, Folman Y. Local implantation of autologous adipose-derived stem cells increases femoral strength and bone density in osteoporotic rats: a randomized controlled animal study. J Orthopaed Surg. (2018) 26:2309499018799534. doi: 10.1177/2309499018799534
125. Mirsaidi A, Genelin K, Vetsch JR, Stanger S, Theiss F, Lindtner RA, et al. Therapeutic potential of adipose-derived stromal cells in age-related osteoporosis. Biomaterials. (2014) 35:7326–35. doi: 10.1016/j.biomaterials.2014.05.016
126. Cho SW, Sun HJ, Yang JY, Jung JY, Choi HJ, An JH, et al. Human adipose tissue-derived stromal cell therapy prevents bone loss in ovariectomized nude mouse. Tissue Engineering Part A. (2012) 18:1067–78. doi: 10.1089/ten.tea.2011.0355
127. Qi M, Zhang L, Ma Y, Shuai Y, Li L, Luo K, et al. Autophagy maintains the function of bone marrow mesenchymal stem cells to prevent estrogen deficiency-induced osteoporosis. Theranostics. (2017) 7:4498. doi: 10.7150/thno.17949
128. Cao L, Liu G, Gan Y, Fan Q, Yang F, Zhang X, et al. The use of autologous enriched bone marrow MSCs to enhance osteoporotic bone defect repair in long-term estrogen deficient goats. Biomaterials. (2012) 33:5076–84. doi: 10.1016/j.biomaterials.2012.03.069
129. Ocarino ND, Boeloni JN, Jorgetti V, Gomes DA, Goes AM, Serakides R. Intra-bone marrow injection of mesenchymal stem cells improves the femur bone mass of osteoporotic female rats. Connect Tissue Res. (2010) 51:426–33. doi: 10.3109/03008201003597049
130. Wang Z, Goh J, De SD, Ge Z, Ouyang H, Chong JS, et al. Efficacy of bone marrow–derived stem cells in strengthening osteoporotic bone in a rabbit model. Tissue Eng. (2006) 12:1753–61. doi: 10.1089/ten.2006.12.1753
131. Hamza AA, Fikry EM, Abdallah W, Amin A. Mechanistic insights into the augmented effect of bone marrow mesenchymal stem cells and thiazolidinediones in streptozotocin-nicotinamide induced diabetic rats. Sci Rep. (2018) 8:1–8. doi: 10.1038/s41598-018-28029-1
132. Bianco P, Cao X, Frenette PS, Mao JJ, Robey PG, Simmons PJ, et al. The meaning, the sense and the significance: translating the science of mesenchymal stem cells into medicine. Nat Med. (2013) 19:35–42. doi: 10.1038/nm.3028
133. Su P, Tian Y, Yang C, Ma X, Wang X, Pei J, et al. Mesenchymal stem cell migration during bone formation and bone diseases therapy. Int J Mol Sci. (2018) 19:2343. doi: 10.3390/ijms19082343
134. Chen HT, Lee MJ, Chen CH, Chuang SC, Chang LF, Ho ML, et al. Proliferation and differentiation potential of human adipose-derived mesenchymal stem cells isolated from elderly patients with osteoporotic fractures. J Cell Mol Med. (2012) 16:582–92. doi: 10.1111/j.1582-4934.2011.01335.x
135. Liu HY, Chiou JF, Wu AT, Tsai CY, Leu JD, Ting LL, et al. The effect of diminished osteogenic signals on reduced osteoporosis recovery in aged mice and the potential therapeutic use of adipose-derived stem cells. Biomaterials. (2012) 33:6105–12. doi: 10.1016/j.biomaterials.2012.05.024
136. Steinert AF, Rackwitz L, Gilbert F, Nöth U, Tuan RS. Concise review: the clinical application of mesenchymal stem cells for musculoskeletal regeneration: current status and perspectives. Stem Cells Transl Med. (2012) 1:237–47. doi: 10.5966/sctm.2011-0036
137. Pino AM, Rosen CJ, Rodríguez JP. In osteoporosis, differentiation of mesenchymal stem cells (MSCs) improves bone marrow adipogenesis. Biol Res. (2012) 45:279–87. doi: 10.4067/S0716-97602012000300009
138. Infante A, Rodríguez CI. Osteogenesis and aging: lessons from mesenchymal stem cells. Stem Cell Res Ther. (2018) 9:1–7. doi: 10.1186/s13287-018-0995-x
139. Oryan A, Kamali A, Moshiri A, Eslaminejad MB. Role of mesenchymal stem cells in bone regenerative medicine: what is the evidence? Cells Tissues Organs. (2017) 204:59–83. doi: 10.1159/000469704
140. Nimiritsky PP, Eremichev RY, Alexandrushkina NA, Efimenko AY, Tkachuk VA, Makarevich PI. Unveiling mesenchymal stromal cells' organizing function in regeneration. Int J Mol Sci. (2019) 20:823. doi: 10.3390/ijms20040823
141. Linero I, Chaparro O. Paracrine effect of mesenchymal stem cells derived from human adipose tissue in bone regeneration. PloS ONE. (2014) 9:e107001. doi: 10.1371/journal.pone.0107001
142. Sanchooli T. Prospect of mesenchymal stem cells conditioned medium in tissue regeneration. Gene Cell Tissue. (2017) 4:965849. doi: 10.5812/gct.64645
143. Ratajczak MZ, Kucia M, Jadczyk T, Greco NJ, Wojakowski W, Tendera M, et al. Pivotal role of paracrine effects in stem cell therapies in regenerative medicine: can we translate stem cell-secreted paracrine factors and microvesicles into better therapeutic strategies? Leukemia. (2012) 26:1166–73. doi: 10.1038/leu.2011.389
144. Huber BC, Grabmaier U, Brunner S. Impact of parathyroid hormone on bone marrow-derived stem cell mobilization and migration. World J Stem Cells. (2014) 6:637. doi: 10.4252/wjsc.v6.i5.637
145. Goldshtein I, Rouach V, Shamir-Stein N, Yu J, Chodick G. Role of side effects, physician involvement, and patient perception in non-adherence with oral bisphosphonates. Adv Ther. (2016) 33:1374–84. doi: 10.1007/s12325-016-0360-3
146. Arjmand B, Abdollahi M, Larijani B. Precision medicine: a new revolution in healthcare system. Iran Biomed J. (2017) 21:282–3.
147. Arjmand B, Goodarzi P, Mohamadi-Jahani F, Falahzadeh K, Larijani B. Personalized regenerative medicine. Acta Med Iran. (2017) 55:144–9.
148. Arjmand B, Larijani B. Personalized medicine: a new era in endocrinology. Acta Med Iran. (2017) 55:142–3.
149. Goodarzi P, Alavi-Moghadam S, Payab M, Larijani B, Rahim F, Gilany K, et al. Metabolomics analysis of mesenchymal stem cells. Int J Mol Cell Med. (2019) 8:30–40. doi: 10.22088/IJMCM.BUMS.8.2.30
150. Larijani B, Goodarzi P, Payab M, Alavi-Moghadam S, Rahim F, Bana N, et al. Metabolomics and cell therapy in Diabetes Mellitus. Int J Mol Cell Med. (2019) 8:41–48. doi: 10.22088/IJMCM.BUMS.8.2.41
151. Zhao Q, Shen H, Su KJ, Zhang JG, Tian Q, Zhao LJ, et al. Metabolomic profiles associated with bone mineral density in US Caucasian women. Nutr Metab. (2018) 15:1–9. doi: 10.1186/s12986-018-0296-5
Keywords: cell therapy, chronic diseases, mesenchymal stem cells, osteoporosis, regenerative medicine
Citation: Arjmand B, Sarvari M, Alavi-Moghadam S, Payab M, Goodarzi P, Gilany K, Mehrdad N and Larijani B (2020) Prospect of Stem Cell Therapy and Regenerative Medicine in Osteoporosis. Front. Endocrinol. 11:430. doi: 10.3389/fendo.2020.00430
Received: 27 August 2019; Accepted: 01 June 2020;
Published: 03 July 2020.
Edited by:
Andrea Ballini, University of Bari Aldo Moro, ItalyReviewed by:
Stefania Cantore, City Unity College Athens, GreeceCopyright © 2020 Arjmand, Sarvari, Alavi-Moghadam, Payab, Goodarzi, Gilany, Mehrdad and Larijani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bagher Larijani, bGFyaWphbmliQHR1bXMuYWMuaXI=
†ORCID: Babak Arjmand orcid.org/0000-0001-5001-5006
Moloud Payab orcid.org/0000-0002-9311-8395
Kambiz Gilany orcid.org/0000-0003-2916-7245
Bagher Larijani orcid.org/0000-0001-5386-7597
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.