
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Endocrinol., 12 February 2020
Sec. Bone Research
Volume 11 - 2020 | https://doi.org/10.3389/fendo.2020.00006
This article is part of the Research TopicInnovative Therapies in Bone Biology: What can be Learned from Rare Bone Diseases?View all 14 articles
 Esmée Botman1*
Esmée Botman1* Jan Coen Netelenbos1Thomas Rustemeyer2Linda J. Schoonmade3Jakko A. Nieuwenhuijzen4Bernd P. Teunissen5Marieke Visser6Pieter Raijmakers5Adriaan A. Lammertsma5Max Dahele7Marelise Eekhoff1
Jan Coen Netelenbos1Thomas Rustemeyer2Linda J. Schoonmade3Jakko A. Nieuwenhuijzen4Bernd P. Teunissen5Marieke Visser6Pieter Raijmakers5Adriaan A. Lammertsma5Max Dahele7Marelise Eekhoff1Fibrodysplasia ossificans progressiva (FOP) is an autosomal dominant disease, characterized by the formation of heterotopic ossification (HO) in muscles, ligaments, and tendons. Flare-ups, an inflammatory process that often precedes the formation of HO, can occur spontaneously, but trauma is also a common trigger. It is not known whether radiotherapy, especially in higher doses, might cause sufficient trauma or inflammation to trigger a flare-up and subsequent HO in FOP patients. We report the case of a patient undergoing radiotherapy for the treatment of a 1-cm-wide basal cell carcinoma (BCC) of the lower lip. In addition, we present a systematic review of the available literature. Our patient received 54 Gy in 18 fractions with orthovoltage therapy, resulting in a clinical complete response of the tumor. Six months after treatment, there were no signs of HO either clinically or on [18F]NaF PET/CT. The systematic review identified 11 publications describing either radiation treatment in FOP or radiation therapy as a cause of HO in non-FOP patients. Six case reports described the use of radiation in FOP patients for various reasons, including one with a high-dose treatment of a lip BCC using superficial X-ray therapy. The remaining five studies described the use of low-dose radiotherapy to prevent or treat either an FOP flare-up or HO formation. None of these cases showed worsening of disease that could be attributed to the use of radiation therapy. Radiation induced HO in non-FOP patients was rare and occurred in five studies. The largest of these studies suggested that HO was induced after treatment with high doses, resulting in more widespread evidence of tissue damage, potentially being the end result of this damage. In conclusion, available reports suggest no contraindication to radiotherapy in FOP patients; although the number of cases was small, systematic toxicity reports often were not available, and none of the reports described high-dose, high-energy radiation treatment at locations such as muscle and joint regions.
Fibrodysplasia ossificans progressiva (FOP) is an autosomal dominant disorder, which is characterized by heterotopic ossification (HO) in muscle, ligaments, and tendons (1, 2). First ossifications usually develop at the age of 6, often affecting the upper back or neck region. With aging, the formation of HO extends to appendicular regions (3). Often, HO formation is preceded by a flare-up, an inflammatory process of uncertain origin (2, 3). Flare-ups can be provoked by (minor) trauma and infections but can also occur spontaneously (3). Whether radiotherapy can cause sufficient trauma to trigger a flare-up, leading to HO, is unclear. Previously, we have demonstrated that [18F]NaF PET can be used to detect activity of disease just prior to the formation or progression of HO (4–6). Intravenously administered labeled sodium fluoride ([18F]NaF) binds to newly formed hydroxyapatite and, therefore, can be used to detect osteoblastic activity (7). We previously reported that increased [18F]NaF uptake was observed within 1 month of surgery as the first sign of HO recurrence in an FOP patient, confirmed 6 months later with CT (6). If radiotherapy does indeed lead to HO formation, it should be detectable by either increased [18F]NaF uptake on PET or the presence of HO at the irradiated site on a follow-up CT.
In this paper, we describe a 67-year-old male patient with FOP, who underwent radiation treatment for a basal cell carcinoma (BCC) of the lower left lip. To place results into context, we then performed a systematic review of the literature to address whether radiotherapy is safe in FOP patients.
A 67-year-old male patient with FOP presented with a 1-cm-wide, progressive lesion of the lower left lip. The patient has the classic variant (R206H) of FOP. The cumulative analog joint involvement scale (CAJIS) score was 25 (8). The patient had not had a flare-up for at least 5 years. However, disease activity was observed at multiple sites on [18F]NaF PET/CT performed during annual follow-ups.
A skin biopsy, performed with caution to minimize damage to surrounding tissues, diagnosed an infiltrative BCC. It extended up to the deep biopsy margin (2 mm). Since surgery is known as a trigger for a flare-up, radiation treatment was preferred over surgical excision. Because the patient is wheelchair bound due to FOP, orthovoltage therapy was considered as the most practical method, as he could remain in his wheelchair during treatment. The patient underwent 18 sessions (fractions) of radiotherapy over a period of ~4 weeks, with each fraction delivering a dose of 3 Gy for a total dose of 54 Gy. The BCC showed complete clinical remission after treatment. However, soon after treatment, the patient reported increased difficulty in eating because of decreased mobility of the lower lip. In combination with pre-existing jaw ankyloses, the loss of lip mobility increased the difficulty of eating and drinking. To assess whether these problems were caused by formation of HO in the irradiated area, [18F]NaF PET/CT (Gemini TF-64; Philips Medical Systems, Best, Netherlands) was performed. This scan, performed 6 months after completion of radiation therapy, did not show any evidence of HO formation, i.e., no increased tracer uptake in the irradiated area, nor any CT evidence of HO in the treated region. In addition, the radiation therapy did not lead to a significant increase in overall activity of disease throughout the body. Almost 2 years after the irradiation, there was still no sign of HO formation at the irradiated site, confirmed by physical examination.
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (www.prisma-statement.org). A comprehensive search was performed in the bibliographic databases PubMed and Embase.com from inception to December 6th, 2018, in collaboration with a medical librarian (LS). Search terms included controlled terms (MesH in PubMed and Emtree in Embase) as well as free text terms. The following terms were used (including synonyms and closely related words) as index terms or free text words: “fibrodysplasia ossificans,” “radiotherapy,” “heterotopic ossification,” and “myositis ossificans.” The search was performed without date or language restrictions. Duplicate articles were excluded. The full search strategies for all databases can be found in the Supplementary Material.
Using this search strategy, 731 articles were identified. Articles describing radiotherapy in FOP patients or radiation therapy as a (probable) cause of HO were eligible for inclusion (Figure 1). The articles were systematically assessed by two independent reviewers (EB and JCN). Discrepancies were resolved by consensus. After screening titles, abstract, and articles, 11 publications were selected for this systematic review. Of these 11 articles, 6 articles addressed radiotherapy in FOP, and 5 the relationship between irradiation and the formation of HO.
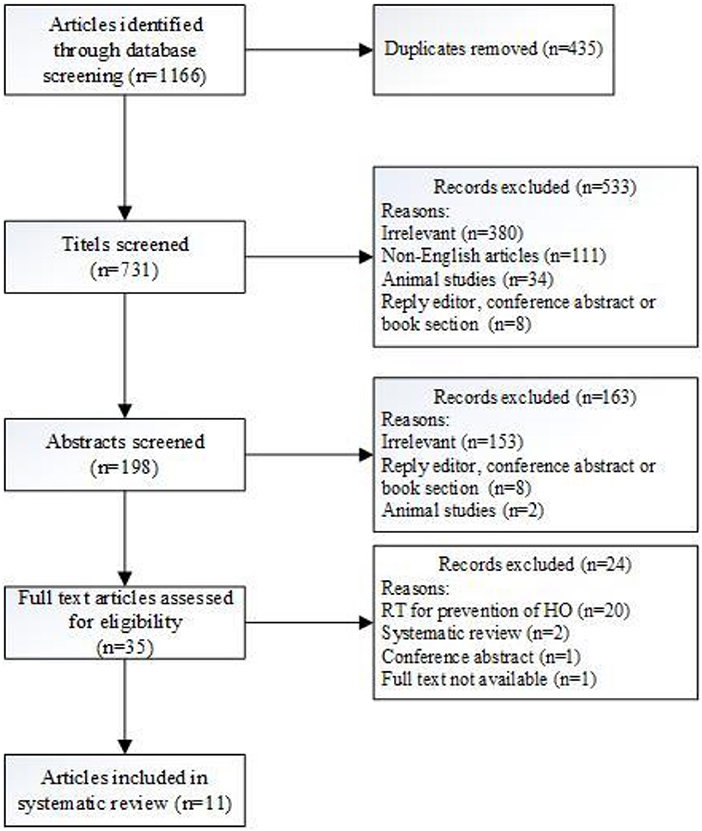
Figure 1. Flowchart of the study selection process.
Not including our own case, radiotherapy in FOP has been described in six other case reports (Table 1). One case reported the radical (high-dose) treatment of a lip BCC using superficial (90 Kv) X-ray therapy (12). The remaining five cases described the use of low-dose radiotherapy to prevent or treat FOP flare-ups or HO formation (9–11, 13, 14). In 4/5 of these cases, a beneficial effect on flare-up symptoms or HO formation was reported (9–11, 14). In 2/5 cases, one or two additional treatment modalities were also reported: a non-steroidal anti-inflammatory drug (NSAID) in both cases and a bisphosphonate in one of them (9, 11). None of the cases reported clinical deterioration or excessive toxicity as a result of radiotherapy (containing) treatment. All but one reported a relatively low dose of radiation (9, 11, 13, 14), consistent with the literature on HO prevention in non-FOP patients (15). Interestingly, Soldic et al. described clinical and radiological benefits after very low doses of fractionated radiotherapy (as low as 2 Gy in two fractions) (14). In the remaining case, which was very similar to ours, a patient received 35 Gy in five fractions on consecutive days for the treatment of a right upper lip BCC. There was a complete response with no evidence of HO at the irradiated site (12). Whether this was confirmed radiographically is not known. In addition, the time interval between radiation therapy and follow-up was not reported. In summary, based on a limited sample of seven patients with FOP (including ours), a range of radiotherapy doses appear to have been well-tolerated, with no reports of excessive or unexpected HO formation and no reports to suggest that the intended outcomes (primarily prevention, treatment of HO, and treatment of BCC) were any worse than expected. However, there was no systematic toxicity reporting, and none of the reports described high-dose, high-energy treatment at specific sites, including muscle and joint regions.
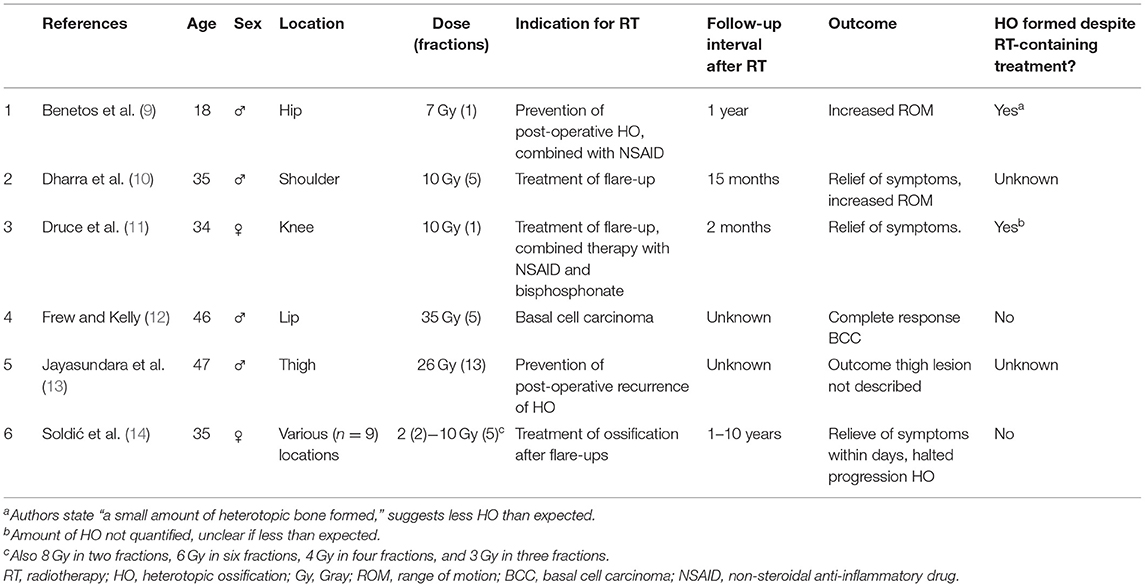
Table 1. Articles describing radiotherapy in patients with fibrodysplasia ossificans progressiva.
Five studies were found suggesting that radiation received by non-FOP patients eventually led to HO at the irradiated site (Table 2) (16–20). The interval between actual treatment and formation of HO varied between 1 and 33 years. The largest patient series was from Carl et al. who reported on 15 cases with a range of primary tumors (breast, anal, endometrial, sarcoma, seminoma, bladder, and cervical) (16). Radiation types varied and include cobalt, neutrons, and brachytherapy. Biologically effective doses (for late normal tissue damage, with α/β = 3) ranged from 67 to 214 Gy. However, potential overlap between fields means that local doses may have been higher. HO developed 2–31 years after radiotherapy. Importantly, all patients first developed other signs of tissue damage ranging from plexopathy to ulceration and necrosis as a result of radiation therapy, leading the authors to propose that HO in these patients was an end stage response to the tissue damage caused by radiotherapy. In the other four case reports, neither dose nor tissue damage as a result of treatment was specified (17–20). In three of these cases, no trigger other than radiotherapy for HO was present (18–20). In the remaining case, the authors stated that HO in the ankylosed mandible might have been caused by a combination of factors, including chemotherapy, radiation, prolonged intubation, immobilization, and critical illness neuromyopathy (17).
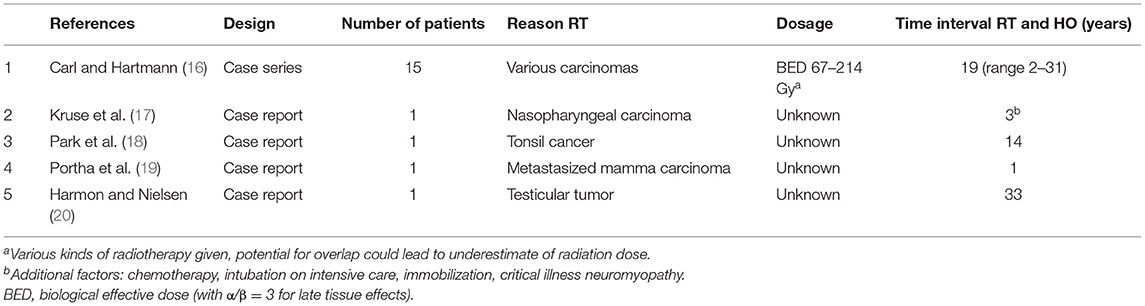
Table 2. Articles describing the formation of heterotopic ossification in non-FOP patients as a late effect of radiotherapy.
To the best of our knowledge, this is the first systematic review of literature relating to the use of radiotherapy in patients with FOP. Including our own case, we found only seven cases in the literature. The available reports suggest that radiotherapy in FOP patients does not lead to the formation of HO at the irradiated site. In addition, there were no reports of excessive or unexpected toxicity and no indication that the intended treatment outcome was poorer than expected. Some caution is required, however, as the number of cases is very small, there was no uniform systematic toxicity reporting or post-radiotherapy assessment, there are limited long-term data, and the effect of high-dose, high-energy radiation to, for example, muscle and joint regions was not described.
One discussion point that can be extracted from these reports is the timing of radiotherapy. Pignolo et al. described that most flare-ups resolved spontaneously within 8 weeks, except those of the hip and back, and of the latter, 75% resolved within 12 weeks (3). One patient was irradiated for a flare-up at the iliopsoas muscle. Radiotherapy was combined with physiotherapy, indomethacin, and disodium etidronate (11). Disodium etidronate, a bisphosphonate, has been used in the past to prevent formation of HO in FOP (21–23), but because of its varying success and side effects, nowadays its use is limited (24). The flare-up was present for 5 weeks prior to treatment. Two months after treatment, it was reported that edema was significantly diminished and pain was relieved (11). Whether this was due to the multi-modality treatment or whether the lesion would have spontaneously resolved is not known with certainty. However, in this case, the patient already had evidence of femoral neurapraxia and neurological deficits at presentation due to the mass. In such a situation, urgent initiation of treatment to avoid permanent nerve damage is important. For milder, non-threatening, flare-ups, a period of observation, to see whether spontaneous regression occurs, would be appropriate. Although apparently effective in the short term, combination treatment did not prevent HO formation, as follow-up CT revealed the presence of calcification at the affected site (11). Unfortunately, the longer-term outcome is not known. Soldic et al. also reported the benefit of radiotherapy in their patient who underwent multiple irradiations at different locations over a prolonged period (14). They used calcification detected on radiographs or CT as a marker of disease. Interestingly, despite low doses of radiation, they reported non-progression of calcification for periods of up to 10 years, and they did not report having to treat previously treated areas again. In the future, it would be interesting to assess disease activity before and after treatment with [18F]NaF PET/CT, as this could objectively assess effects of radiotherapy on disease activity (4–6).
The choice between radiotherapy and other treatments need consideration. Treatment of a tumor or prevention/treatment of HO formation both seem reasonable indications based on the literature. The choice between radiotherapy and other modalities will depend on various factors:
1. The risk of secondary tumor induction by radiation, and the effect of radiation on bone.
A single radiation fraction of, e.g., 7 Gy, as used in myositis ossificans traumatica (MOT) to prevent HO, has only rarely led to a malignancy at the irradiated site (25). Pellegrini et al. hypothesized that this low incidence is due to the already advanced age of most patients developing MOT and the latency period for the malignancy to develop (26). Younger patients have a higher risk of developing a secondary malignancy as a consequence of radiation treatment (27). Even though life expectancy of FOP patients is limited (28), and therefore, the lifetime chance to develop a secondary malignancy due to radiotherapy is also limited, the treatment of a secondary malignancy (e.g., by surgery) is catastrophic for FOP patients.
Radiation can also have negative effects on bone metabolism, both locally and systemically (29). In addition, FOP patients often underwent multiple glucocorticoid treatments (3), which can also lead to bone toxicity, e.g., reduction in bone mineral density of skeletal bone. Strategies to maximize bone health and mitigate bone toxicity from FOP treatments are required.
2. The potential of either a flare-up or HO formation by alternative therapy (e.g., surgery).
Although Benetos et al. reported good outcome after surgery followed by indomethacin and radiotherapy (9), traumatic injury is a major trigger for FOP flare-ups and subsequent HO (3, 28). Radiotherapy to prevent HO reoccurrence after surgery is a known and effective strategy in MOT (15, 30, 31), Indomethacin, an NSAID, is known for its post-operative preventative role in MOT (32). Usually, surgery is avoided in FOP because of the effects it can have on disease progression, although resection of HO has been performed to try and improve function, and surgery may also be necessary in certain urgent conditions. If surgery is required, post-operative radiotherapy and/or NSAID treatment to prevent HO formation should be considered.
3. Patient tolerance or risk of non-radiotherapy side effects.
Glucocorticoids are commonly used for the treatment of flare-ups because of their anti-inflammatory effect. Although their effect on prevention of flare-ups and HO formation has never been rigorously tested, about half of the patients report an improvement in flare-up symptoms when treated with glucocorticoids (3). However, known side effects are, among others, weight gain, proximal myopathy, glucose intolerance, suppression of endogenous hormones, and gastrointestinal toxicity (33). There is extensive experience with NSAIDs in FOP patients (24). About one-third of patients use NSAIDs for flare-ups, although they can lead to gastrointestinal issues and renal toxicity (3). Radiotherapy should not be seen as a replacement for anti-inflammatory drugs but, rather, as a complementary treatment strategy to be considered in certain clinical situations and for selected patients.
Even though radiotherapy seems safe in FOP patients, one should keep in mind that post-irradiation tissue damage (e.g., fibrosis) leading to (even minimal) mobility/function loss can have a significant impact on the quality of life of patients. Patients are highly dependent on their remaining function, and any disturbance can significantly affect daily life. Any intervention, including radiotherapy, should take this into account, and where possible, risks should be kept as low as possible.
In conclusion, the risk of HO induction by radiation in non-FOP patients is, as demonstrated by the few cases in our systematic review, very small and usually part of more widespread tissue damage. Based on available literature, radiotherapy-induced HO formation does not seem to be a problem in non-FOP or FOP patients. As follow-up data are limited, radiotherapy for FOP patients should only be considered in specific situations, e.g., post-operatively after surgery or to reduce flare-up edema when causing neurological deficits. As [18F]NaF is the only in vivo disease activity marker currently available, pre-treatment and follow-up imaging using [18F]NaF PET/CT should be considered to evaluate the effects of interventions, including radiation, on local, and systemic FOP activity.
All datasets generated for this study are included in the article/Supplementary Material.
The studies involving human participants were reviewed and approved by Medical Ethical Review Board, Amsterdam UMC, Vrije Universiteit Amsterdam, Netherlands. The patient/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
EB, ME, JAN, MD, and TR: study design, data analysis, data interpretation, and drafting manuscript. EB, ME, JCN, MD, and TR: study conduct. EB, ME, JCN, and LS: data collection. PR, BT, AL, MV, and JAN: revising manuscript content. EB, ME, JAN, MD, TR, AL, BT, PR, MV, LS, and JAN: approving final version of manuscript. EB, ME, and MD: taking responsibility for the integrity of the data analysis.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank the patient for sharing the data with us.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2020.00006/full#supplementary-material
1. Cohen RB, Hahn GV, Tabas JA, Peeper J, Levitz CL, Sando A, et al. The natural history of heterotopic ossification in patients who have fibrodysplasia ossificans progressiva. A study of forty-four patients. J Bone Joint Surg Am. (1993) 75:215–9. doi: 10.2106/00004623-199302000-00008
2. Kaplan FS, Le Merrer M, Glaser DL, Pignolo RJ, Goldsby RE, Kitterman JA, et al. Fibrodysplasia ossificans progressiva. Best Pract Res Clin Rheumatol. (2008) 22:191–205. doi: 10.1016/j.berh.2007.11.007
3. Pignolo RJ, Bedford-Gay C, Liljesthröm M, Durbin-Johnson BP, Shore EM, Rocke DM, et al. The natural history of flare-Ups in fibrodysplasia ossificans progressiva (FOP): a comprehensive global assessment. J Bone Miner Res. (2016) 31:650–6. doi: 10.1002/jbmr.2728
4. Eekhoff EMW, Botman E, Coen Netelenbos J, de Graaf P, Bravenboer N, Micha D, et al. [18F]NaF PET/CT scan as an early marker of heterotopic ossification in fibrodysplasia ossificans progressiva. Bone. (2017) 109:143–46. doi: 10.1016/j.bone.2017.08.012
5. Botman E, Raijmakers PGHM, Yaqub M, Teunissen B, Netelenbos C, Lubbers W, et al. Evolution of heterotopic bone in fibrodysplasia ossificans progressiva: an [18F]NaF PET/CT study. Bone. (2019). 124:1–6. doi: 10.1016/j.bone.2019.03.009
6. Eekhoff EMW, Netelenbos JC, de Graaf P, Hoebink M, Bravenboer N, Micha D, et al. Flare-up after maxillofacial surgery in a patient with fibrodysplasia ossificans progressiva: an [18F]-NaF PET/CT study and a systematic review. JBMR Plus. (2018) 2:55–8. doi: 10.1002/jbm4.10008
7. Segall G, Delbeke D, Stabin MG, Even-Sapir E, Fair J, Sajdak R, et al. SNM practice guideline for sodium 18F-fluoride PET/CT bone scans 1.0. J Nucl Med. (2010) 51:1813–20. doi: 10.2967/jnumed.110.082263
8. Kaplan FS, Al Mukaddam M, Pignolo RJ. A cumulative analogue joint involvement scale (CAJIS) for fibrodysplasia ossificans progressiva (FOP). Bone. (2017) 101:123–8. doi: 10.1016/j.bone.2017.04.015
9. Benetos IS, Mavrogenis AF, Themistocleous GS, Kanellopoulos AD, Papagelopoulos PJ, Soucacos PN. Optimal treatment of fibrodysplasia ossificans progressiva with surgical excision of heterotopic bone, indomethacin, and irradiation. J Surg Orthop Adv. (2006) 15:99–104.
10. Dharra N, Srivastava R, Halder S, Hukku S. Role of radiotherapy in management of Fibrodysplasia ossificans progressiva. Int J Orthopaedics Sci. (2017) 3:813–6. doi: 10.22271/ortho.2017.v3.i2i.88
11. Druce M, Morris VH, Stamp TC. A case report of myositis ossificans progressiva complicated by femoral nerve compression treated with radiotherapy. Rheumatology. (2002) 41:947–8. doi: 10.1093/rheumatology/41.8.947
12. Frew JA, Kelly CG. Radiotherapy for management of skin cancers in fibrodysplasia ossificans progressiva: a case report and review of the literature. J Cancer Res Ther. (2008) 4:37–8. doi: 10.4103/0973-1482.39603
13. Jayasundara JA, Punchihewa GL, de Alwis DS. An unusual case of adult onset progressive heterotopic ossification suggesting a variant form of fibrodysplasia ossificans progressiva. Singapore Med J. (2012) 53:e83–6.
14. Soldić Z, Murgić J, Radić J, Dabelić N, Jazvić M, Brozić JM, et al. Radiation therapy in treatment of fibrodysplasia ossificans progressiva: a case report and review of the literature. Coll Antropol. (2011) 35:611–4.
15. Milakovic M, Popovic M, Raman S, Tsao M, Lam H, Chow E. Radiotherapy for the prophylaxis of heterotopic ossification: a systematic review and meta-analysis of randomized controlled trials. Radiother Oncol. (2015) 116:4–9. doi: 10.1016/j.radonc.2015.05.022
16. Carl UM, Hartmann KA. Heterotopic calcification as a late radiation effect: report of 15 cases. Br J Radiol. (2002) 75:460–3. doi: 10.1259/bjr.75.893.750460
17. Kruse AL, Dannemann C, Grätz KW. Bilateral myositis ossificans of the masseter muscle after chemoradiotherapy and critical illness neuropathy–report of a rare entity and review of literature. Head Neck Oncol. (2009) 1:30. doi: 10.1186/1758-3284-1-30
18. Park J, Lee S, Joo KB. Growing heterotopic calcification in the prevertebral space of a cervical spine as a late complication of irradiation: case report. Korean J Radiol. (2014) 15:140–4. doi: 10.3348/kjr.2014.15.1.140
19. Portha C, Coche G, Moussa K, Guyon JC, Monnier A, Schraub S, et al. Ossification of the posterior longitudinal ligament after cervical irradiation. Neuroradiology. (1982) 24:111–3. doi: 10.1007/BF00339201
20. Harmon DC, Nielsen GP. Case 38-1994 - a 55-year-old man with a paraspinal mass and a history of radiation treatment of a testicular tumor. N Engl J Med. (1994) 331:1079–84. doi: 10.1056/NEJM199410203311609
21. Hall JG, Schaller JG, Worsham NG, Horning MR, Staheli LT. Fibrodysplasia ossificans progressiva (myositis ossificans progressiva) treatment with disodium etidronate. J Pediatr. (1979) 94:679–80. doi: 10.1016/S0022-3476(79)80056-6
22. Rogers JG, Geho WB. Fibrodysplasia ossificans progressiva. a survey of forty-two cases. J Bone Joint Surg Am. (1979) 61:909–14. doi: 10.2106/00004623-197961060-00019
23. Brantus JF, Meunier PJ. Effects of intravenous etidronate and oral corticosteroids in fibrodysplasia ossificans progressiva. Clin Orthop Relat Res. (1998) 346:117–20. doi: 10.1097/00003086-199801000-00017
24. Kaplan FS, Al Mukaddam M, Baujat G, Brown M, Cali A, Cho T-J, et al. The medical management of fibrodysplasia ossificans progressiva: current treatment considerations. Proc Intl Clin Council FOP. (2019) 1:1–111
25. Sheybani A, TenNapel MJ, Lack WD, Clerkin P, Hyer DE, Sun W, et al. Risk of radiation-induced malignancy with heterotopic ossification prophylaxis: a case-control analysis. Int J Radiat Oncol Biol Phys. (2014) 89:584–9. doi: 10.1016/j.ijrobp.2014.03.008
26. Pellegrini VD Jr, Gregoritch SJ. Preoperative irradiation for prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am. (1996) 78:870–81. doi: 10.2106/00004623-199606000-00010
27. Kamran SC, Berrington de Gonzalez A, Ng A, Haas-Kogan D, Viswanathan AN. Therapeutic radiation and the potential risk of second malignancies. Cancer. (2016) 122:1809–21. doi: 10.1002/cncr.29841
28. Kitterman JA, Kantanie S, Rocke DM, Kaplan FS. Iatrogenic harm caused by diagnostic errors in fibrodysplasia ossificans progressiva. Pediatrics. (2005) 116:e654–61. doi: 10.1542/peds.2005-0469
29. Zhang J, Qiu X, Xi K, Hu W, Pei H, Nie J, et al. Therapeutic ionizing radiation induced bone loss: a review of in vivo and in vitro findings. Connect Tissue Res. (2018) 59:509–22. doi: 10.1080/03008207.2018.1439482
30. van Leeuwen WM, Deckers P, de Lange WJ. Preoperative irradiation for prophylaxis of ectopic ossification after hip arthroplasty. A randomized study in 62 hips. Acta Orthop Scand. (1998) 69:116–8. doi: 10.3109/17453679809117609
31. Seegenschmiedt MH, Keilholz L, Martus P, Goldmann A, Wölfel R, Henning F, et al. Prevention of heterotopic ossification about the hip: final results of two randomized trials in 410 patients using either preoperative or postoperative radiation therapy. Int J Radiat Oncol Biol Phys. (1997) 39:161–71. doi: 10.1016/S0360-3016(97)00285-X
32. Burd TA, Lowry KJ, Anglen JO. Indomethacin compared with localized irradiation for the prevention of heterotopic ossification following surgical treatment of acetabular fractures. J Bone Joint Surg Am. (2001) 83:1783–8. doi: 10.2106/00004623-200112000-00003
Keywords: fibrodysplasia ossificans progressiva (FOP), radiotherapy, heterotopic ossification (HO), [18F]NaF PET/CT, ACVR1 gene mutation
Citation: Botman E, Netelenbos JC, Rustemeyer T, Schoonmade LJ, Nieuwenhuijzen JA, Teunissen BP, Visser M, Raijmakers P, Lammertsma AA, Dahele M and Eekhoff M (2020) Radiotherapy in Fibrodysplasia Ossificans Progressiva: A Case Report and Systematic Review of the Literature. Front. Endocrinol. 11:6. doi: 10.3389/fendo.2020.00006
Received: 11 November 2019; Accepted: 07 January 2020;
Published: 12 February 2020.
Edited by:
Gudrun Stenbeck, Brunel University London, United KingdomReviewed by:
Michaël R. Laurent, University Hospitals Leuven, BelgiumCopyright © 2020 Botman, Netelenbos, Rustemeyer, Schoonmade, Nieuwenhuijzen, Teunissen, Visser, Raijmakers, Lammertsma, Dahele and Eekhoff. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Esmée Botman, ZS5ib3RtYW5AYW1zdGVyZGFtdW1jLm5s
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.