 Jenny Müller
Jenny Müller Dagmar I. Keller1,2†
Dagmar I. Keller1,2† Ksenija Slankamenac
Ksenija Slankamenac
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Disaster Emerg. Med., 05 March 2024
Sec. Emergency Health Services
Volume 2 - 2024 | https://doi.org/10.3389/femer.2024.1342904
Introduction: Older patients currently represent up to 12%−24% of all emergency department (ED) visits. While increasing in number, they are also at high risk of revisits once discharged. The rate of ED revisits within 72 h is a key indicator of the quality of care in emergency medicine and varies between 1% and 15%. The reasons for ED revisits are natural course of illness, misdiagnosis, lack of homecare, and self-discharge against medical advice. However, the risk factors for ED revisits have not been fully investigated. Therefore, this study aimed to analyze the incidence of ED revisits and identify the risk factors for ED revisits within 72 h after ED discharge.
Methods: In this retrospective study, older patients (≥70 years) were consecutively enrolled if they presented with an Emergency Severity Index of 2 or 3 in a tertiary care ED in 2019, with discharge after the ED visit. The primary endpoint was the frequency of unplanned ED revisits within 72 h after ED discharge. The secondary endpoints were the reasons and potential risk factors for ED revisits. Univariate and multivariate logistic regression models were used.
Results: A total of 592 older patients were enrolled, of whom 30 (5.1%) revisited the ED within 72 h. Gastrointestinal diagnosis [odds ratio (OR), 2.9; 95% confidence interval [CI], 1.04–8.2; p = 0.043) and nausea in particular (OR, 3.5; 95% CI, 1.3–9.4; p = 0.016) were significant risk factors for ED revisits. Furthermore, discharge against medical advice (OR, 5.6; 95% CI, 1.7–18.1; p = 0.004) and ED presentation during the night (OR, 2.7; 95% CI, 1.2–6.1; p = 0.014) were significant risk factors for ED revisits within 72 h after discharge, respectively.
Conclusion: Although the frequency of ED revisits among older patients at 72 h after discharge tends to be low and most revisits were illness-related, all older patients need to be assessed for risk factors for ED revisits. Discharge should be carefully evaluated to improve patient safety and provide the best healthcare to this frail population.
Older patients represent up to 12%−24% of all emergency department (ED) visits (1–4). The proportion of older people in society as well as in ED is constantly increasing (2, 3, 5–7). Current literature indicates that older patients are not only more likely to visit the ED but also stay longer and require more resources than younger patients (8). These patients often have multiple comorbidities that create complex health (and care) problems (1). In addition, difficult social conditions, decreased mobility, and functional capacity in older age complicate the ability to recover from illness or adapt to new circumstances after discharge (1).
Furthermore, older patients have a high risk of ED readmission (9, 10). The incidence of ED revisits after 72 h is often used as a key indicator of quality of care in emergency medicine and varies widely between 1.1% and 15.2% (11–17). The reasons for ED revisits are numerous, including natural course of an illness, misdiagnosis during ED visits, lack of care at home, or even an overly concerned reaction of a patient to discharge against medical advice (11–13, 18). Worldwide ED overcrowding is a serious issue (19). Therefore unplanned non-urgent revisits of older patients unnecessarily increases ED overcrowding (7). However, the characteristics of older and particularly vulnerable patients and causes of ED revisits have not been fully investigated. This is of considerable interest, as such information can improve patient safety and healthcare, especially for this frail population and can help prevent unnecessary ED overcrowding.
Therefore, the aim of the present study was to analyze the frequency of unplanned ED revisits and identify the reasons and risk factors for ED revisits, with focus on the older population.
In this retrospective study, patients were consecutively enrolled if they were 70 years or older, visited the tertiary care ED at the University Hospital of Zurich from January 1, 2019, to December 31, 2019, and were not hospitalized after the ED visit. Furthermore, patients were enrolled only if they were triaged as Emergency Severity Index (ESI) level 2 or 3. In Switzerland, emergency consultations in hospitals are carried out by direct referrals from e.g., general practitioners or paramedics, but also by self-referrals from patients. A large proportion of emergency patients are “walk-in” patients and come to the ED for clarification of complaints. When presenting in the ED each patient is assessed and triaged by a trained ED nurse. Patients are assigned to a medical area, and labeled according to the severity and suspected origin of their symptoms. ED patients are triaged in accordance with the ESI. ESI is a five-level triage system used to indicate the urgency of medical care and prioritize patients (20, 21). ESI level 1 demands immediate lifesaving medical attention, whereas levels 2 and 3 demand medical attention within 10–30 min and more than two resources for investigation, respectively. Medical staff response can be further delayed in levels 4 and 5, given that both do not require urgent measures and, by definition, demand either only one or no further medical resources (20, 21). Patients were excluded if they were younger than 70 years, with ESI level 1, 4, or 5, and/or were hospitalized directly in the ED. An ethic approval was given by the local ethic committee of the canton Zurich. Each patient included has given informed consent.
The primary endpoint was the frequency of unplanned ED revisits within 72 h after discharge from the index ED. Unplanned ED revisits were defined as any revisit to the ED within 72 h without a pre-scheduled appointment in the ED. Secondary endpoints were reasons and potential risk factors for ED revisits after 72 h.
Further clinical and demographic parameters were assessed from KISIM, the hospital digital clinical information system, in order to characterize the study population: age, sex, comorbidities, Charlson comorbidity index (22, 23), prior hospital admissions or ED visits 6 months before the index ED visit, time of ED presentation (day, middle, or night shift), main symptoms, examinations (e.g., serum blood analysis, ultrasound, x-rays, computed tomography, or electrocardiography), and social variables such as need for care at home, housing conditions (e.g., living alone, living with others, living in a nursing home), and marital status.
The distribution of variables was tested for normality using the Kolmogorov-Smirnov test; normally distributed data were reported as means and standard deviations, whereas non-normally distributed data were reported as medians and interquartile ranges. Categorical data are reported as frequencies with percentages.
The regression model analyzes the association between the dependent variable (outcome) and the number of independent variables by estimating probabilities. The first endpoint (number of ED revisits) and all other secondary endpoints were compared between patients with and without ED revisits within 72 h in univariate and multivariate logistic regression models, respectively. The multivariable model was adjusted for a priori defined and known potential confounders such as age, sex, Charlson comorbidity index (< 4/≥4), and computed tomography examination during the index ED visit.
For all results, we reported the point estimates, 95% confidence intervals (CIs), and p-values (with p < 0.05 considered as statistically significant). Statistical analyses were performed using STATA SE version 16 (Stata Corp., College Station, TX, USA).
In 2019, more than 45,000 patients visited the ED of the University Hospital of Zurich. After excluding patients who did not meet the inclusion criteria, 592 patients were included in the analysis. Of these 592 patients, 30 (5.1%) revisited the ED within 72 h after discharge. The majority of patients (n = 566, 95.6%) were triaged as ESI level 3, whereas 26 patients (4.4%) were triaged as ESI level 2.
Patient characteristics and comorbidities were compared between the groups that revisited the ED within 72 h and those that did not (Table 1). The most common comorbidities were arterial hypertension, rheumatoid disease, coronary heart disease, and chronic kidney disease. Polypharmacy, defined as the intake of more than five different drugs per day (24), was present in the majority of patients (Table 1).
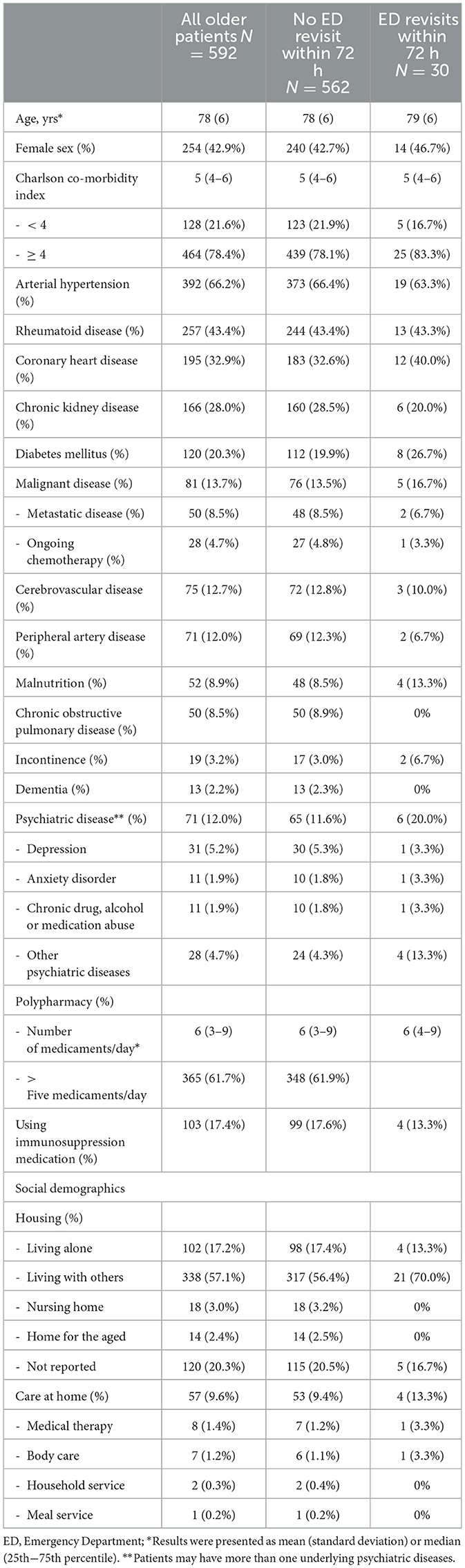
Table 1. Patients' characteristics.
Most patients were living with other people, whereas only a few were living in a nursing home or home for older people). Almost one-fifth (17.2%) of the patients were living alone. Up to 10% were receiving some type of care at home, including medical therapy, body care, household care, or meal services (Table 1).
Regarding the medical examinations performed during the index ED visit, no significant differences were observed between patients who revisited the ED within 72 h and those who did not (Supplementary material 1).
Varying numbers of main symptoms led older patients to visit the ED. All symptoms that led to the index presentation in the ED are summarized in Supplementary material 2.
When a gastrointestinal diagnosis was made at the index emergency presentation, patients were significantly more likely to revisit the ED within 72 h [adjusted odds ratio (OR), 2.9; 95% CI, 1.04–8.2; p = 0.043] (Table 2). A more detailed sub-analysis of the symptoms causing gastrointestinal diagnosis identified that nausea at the index ED visit significantly increased the risk of ED revisits within 72 h (adjusted OR, 3.5; 95% CI, 1.3–9.4; p = 0.016). Further potential risk factors for ED revisits within 72 h were vomiting (adjusted OR, 2.8; 95% CI, 0.9–9.0; p = 0.077) and abdominal pain (adjusted OR, 2.2; 95% CI, 0.95–5.3; p = 0.065).
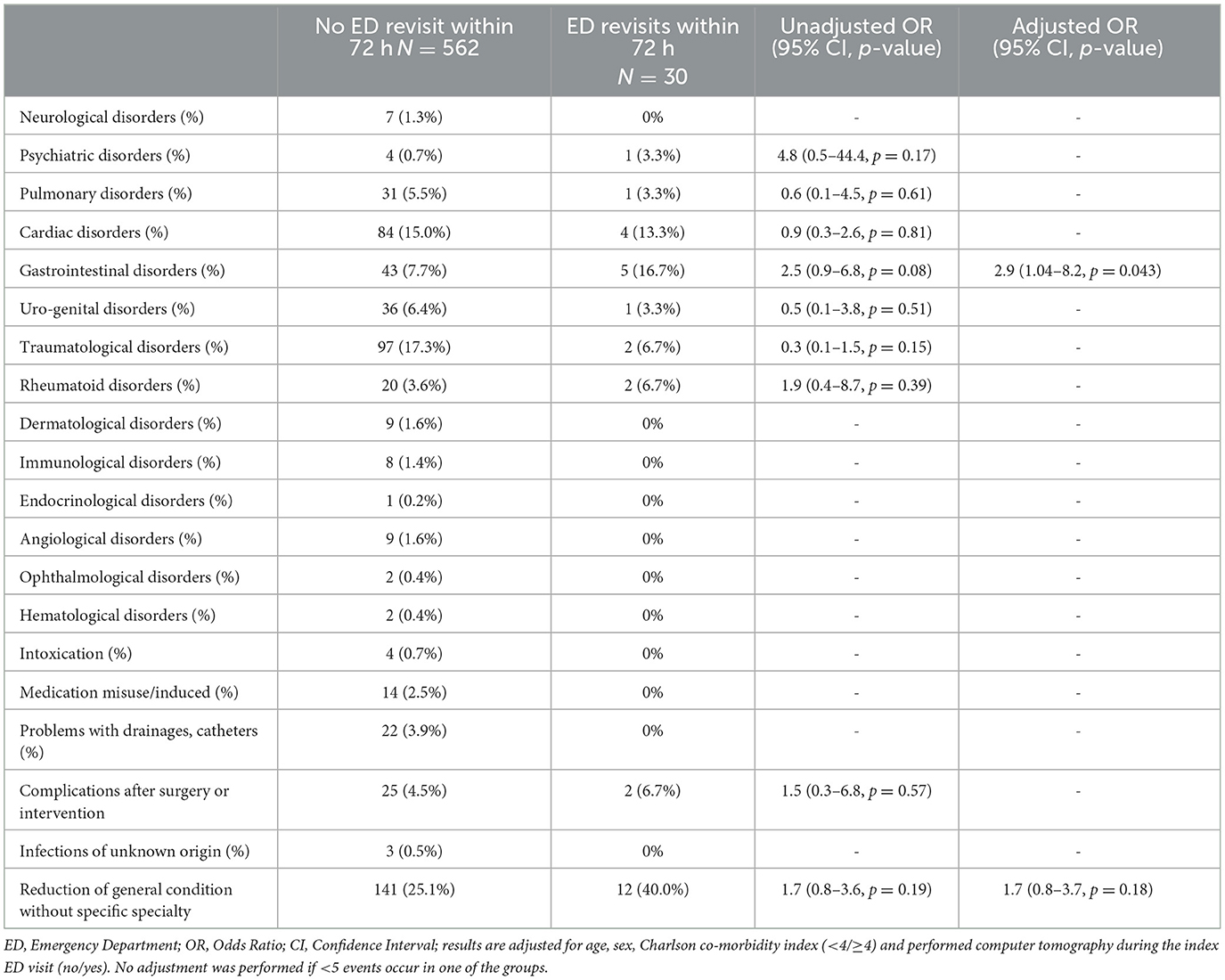
Table 2. Diagnosis at the index ED visit causing ED revisits within 72 h.
Risk factor analysis showed that age, sex, or any comorbidity was significantly associated with ED revisits (Supplementary material 3). Furthermore, none of the living conditions (with others, alone, or care at home) or hospital stay 6 months prior to the index ED visit were significant risk factors for emergency revisits within 72 h (Supplementary material 3).
Meanwhile, risk analysis showed that older patients who were discharged against ED physician's recommendation showed a significantly increased risk of visiting the ED within 72 h (unadjusted OR, 5.6; 95% CI, 1.7–18.1; p = 0.004) (Supplementary material 3). Risk analysis showed that if patients were referred to the ED by a general practitioner or an established specialist, the risks of revisiting the ED (unadjusted OR, 0.3; 95% CI, 0.1–0.98; p = 0.045) was significantly lower (Supplementary material 3).
An index ED visit during the night significantly increased the likelihood of an ED revisit within 72 h (adjusted OR, 2.7; 95% CI, 1.2–6.1; p = 0.014). In comparison, index visits during the day or middle shift showed no increased risk for ED revisits (Table 3).
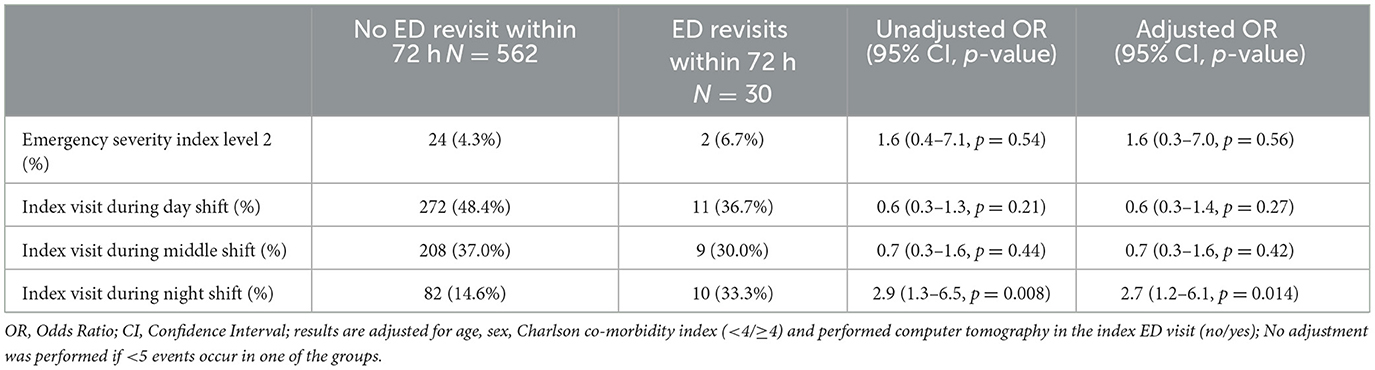
Table 3. Further risk factors for unplanned ED revisit after ED discharge.
Many patients experienced a reduced general condition as the main symptom during emergency presentation. However, reduction in general condition as the main symptom did not show a significant association (adjusted OR, 1.7; 95% CI, 0.8–3.7; p = 0.18) with increased ED revisits within 72 h after the index visit (Table 2).
Table 4 presents the reasons for unplanned ED revisits within 72 h. The main symptoms were mostly (66.7%) identical to those at the index ED visit. Only a few patients revisited the ED for care (3.3%) or social problems (6.7%) (Table 4). Most unplanned ED revisits were for medical reasons (60%). Of the 30 patients who revisited the ED within 72 h after the index ED visit, 22 (73.3%) were admitted (Table 4).
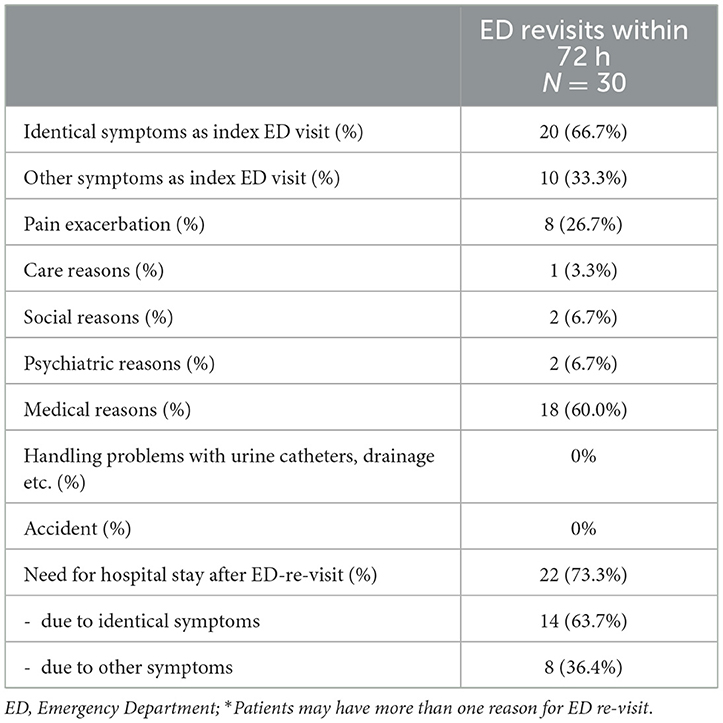
Table 4. Reasons for unplanned ED revisits.
Older patients represent a large proportion of all patients who present to the ED (1–4). Considering their increasing numbers (2, 3, 5, 6) these specific older populations were analyzed, focusing on ED revisits after the index ED discharge. One in 20 older patients presented again within 72 h of discharge from the ED. Three major risk factors for ED revisits within 72 h were identified: gastrointestinal diagnosis, especially those who experienced nausea during the index visit; an index ED visit during the night; self-discharge from the ED against physicians' recommendations.
The rate of ED revisits is often used as a key indicator of the quality of care in the ED (15, 25). In the present study, the ED readmission rate within 72 h was 5.1%. This value is lower than that of other studies, which have readmission rates ranging from 1.1% to 15.2% (11–17), indicating a very good quality of care. We assume that these results were achieved through good and evidence-based emergency medicine and care, focusing on rapid medical clarification, correct diagnosis, and timely provision of medication, information, and instructions as well as a close linkage between patients and primary care physicians. In the future, discharge should be carefully considered in older emergency patients with nausea and/or gastrointestinal disorders, and the possible advantages and disadvantages should be well discussed. Particularly in this frail population, emergency revisits within a few h or days are costly and worsen overall outcomes.
One of the three main reasons for ED revisits within 72 h was gastrointestinal diagnosis made during the index ED visit. This result is supported by existing literature (1, 11, 14, 26–28). In the present sub-analysis, nausea was found to be a significant risk factor for ED revisits. In the literature, abdominal symptoms are mostly grouped and analyzed together (10, 24–26). To the best of our knowledge, abdominal pain is the only gastrointestinal symptom that has been regularly analyzed as a separate risk factor. Abdominal pain was also analyzed as a risk factor in the current study and showed a clear trend with an increased OR; however, it was not a significant risk factor owing to a low event rate in the patient population. Similar results were obtained for vomiting. Nonetheless, Wu et al. stated that symptom-based diagnosis, including nausea, is a significant risk factor for ED revisits (11). We interpret this increased number of revisits as gastrointestinal symptoms, including nausea, which are often non-specific and have multiple differential diagnoses.
In the current investigation, index ED presentation during the night was also a significant risk factor for revisiting the ED within 72 h. Soh et al. (27) reported that 23.7% of all ED patients visited during the night, and among those who visited the ED again, patients with an index ED visit during the night comprise an increased percentage of 30.1%. Shy et al. (13) reported that 43.8% of the patients present during the night at the index ED visit, and the rate increased to 54.8% in the analysis of revisits. Other studies showed no association between the timing of the index presentation and the rate of revisits (16). ED presentation at night as a risk factor is likely dependent on the particular hospital and its resources and responsibilities (13). We are a tertiary care hospital, and most critically ill patients in the region are transferred to our ED. In addition, as it is located in the city center, our hospital has a high number of walk-in patients. Owing to the retrospective nature of this study, it was not possible to evaluate why nighttime emergency presentation is a risk factor for older patients. One possible explanation could be that the overnight assessment and therapy in the ED stabilized older patients to such an extent that they were confident to go home in the morning. Older patients are often hesitant about admission because they are reluctant to leave their functional environments. Further studies are needed to determine the reason for such a finding.
Furthermore, early discharge against doctors' recommendations also contributed significantly to unplanned revisits within 72 h. Other studies have confirmed that discharge against medical advice is a risk factor for ED readmission in general, within 72 h, within 14 days, and within 30 days (12, 13, 27, 29–32). The main reasons for discharge against medical advice are financial burden, homelessness, and multiple comorbidities (29, 30, 33). Furthermore, dissatisfaction about a delay in treatment may be another reason for early discharge against medical advice (33), while trust in the physician does not seen to be disturbed (34). In the current study, the reason for discharge against medical advice could not be determined from the medical records. In a few cases, older patients did not want to remain hospitalized despite detailed information and increased risk because they had pets and had no one to look after them or they simply did not want any further therapy at that time.
A referral to the ED from a general practitioner or an established specialist was a protective factor. This could be explained by better follow-up care. Other studies have shown that well-organized follow-up can reduce the number of ED revisits (35).
Our data showed that a reduction in one's general condition was not a significant risk factor for ED revisits in older patients. This is in line with other studies that suggest no increased risk for unscheduled ED return in patients with a worsening general state (18, 36).
This single-center study was conducted in a city with a high density of hospitals offering emergency care. It is possible that ED revisits were missed owing to presentation to other EDs in the area. The relatively small sample size resulting from the strict in- and exclusion criteria can be seen as a further limitation. This enabled a specific analysis but nonetheless the small sample size must still be taken into account and further studies in this vulnerable patient population are needed in the future. Given the hospital information system and the extensive set of data used for this study, we do not consider our retrospective design as a limitation, especially since we had no missing data in the endpoints. Additionally, we minimized confounding bias by performing a regression analysis.
The frequency of ED revisits at 72 h after ED discharge was low and was mostly illness-related. ED revisits are associated with gastrointestinal diagnoses and symptoms, index presentation during the night, and self-discharge against medical advice. All older patients should be assessed for risk factors for ED revisits. With decreased ED revisits, we can redirect resources toward improving patient safety, providing the best healthcare to this frail patient population, and reducing ED staff workload and overcrowding.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the Ethic Committee of Canton Zürich, Switzerland. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JM: Data curation, Visualization, Writing—original draft, Writing—review & editing. DK: Investigation, Supervision, Visualization, Writing—original draft, Writing—review & editing. KS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Visualization, Writing—original draft, Writing—review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to thank Editage (www.editage.com) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/femer.2024.1342904/full#supplementary-material
1. Bentley J, Meyer J. Repeat attendance by older people at accident and emergency departments. J Adv Nurs. (2004) 48:149–56. doi: 10.1111/j.1365-2648.2004.03182.x
2. Aminzadeh F, Dalziel WB. Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med. (2002) 39:238–47. doi: 10.1067/mem.2002.121523
3. Samaras N, Chevalley T, Samaras D, Gold G. Older patients in the emergency department: a review. Ann Emerg Med. (2010) 56:261–9. doi: 10.1016/j.annemergmed.2010.04.015
4. Sough B, Gauthier T, Clair D, Le Gall A, Menecier P, Mangola B. Elders of 75 and over at an emergency service. Geriatr Psychol Neuropsychiatr Vieil. (2012) 10:151–8. doi: 10.1684/pnv.2012.0351
5. Moons P, Arnauts H, Delooz HH. Nursing issues in care for the elderly in the emergency department: an overview of the literature. Accid Emerg Nurs. (2003) 11:112–20. doi: 10.1016/S0965-2302(02)00163-7
6. Statistik Bf. Bevölkerungsdaten im Zeitvergleich, 1950-2020. Wiesbaden: Bundesamt für Statistik (2021).
7. Gulacti U, Lok U, Celik M, Aktas N, Polat H. The ED use and non-urgent visits of elderly patients. Turk J Emerg Med. (2016) 16:141–5. doi: 10.1016/j.tjem.2016.08.004
8. Moons P, De Ridder K, Geyskens K, Sabbe M, Braes T, Flamaing J, et al. Screening for risk of readmission of patients aged 65 years and above after discharge from the emergency department: predictive value of four instruments. Eur J Emerg Med. (2007) 14:315–23. doi: 10.1097/MEJ.0b013e3282aa3e45
9. Deschodt M, Devriendt E, Sabbe M, Knockaert D, Deboutte P, Boonen S, et al. Characteristics of older adults admitted to the emergency department (ED) and their risk factors for ED readmission based on comprehensive geriatric assessment: a prospective cohort study. BMC Geriatr. (2015) 15:54. doi: 10.1186/s12877-015-0055-7
10. Friedmann PD, Jin L, Karrison TG, Hayley DC, Mulliken R, Walter J, et al. Early revisit, hospitalization, or death among older persons discharged from the ED. Am J Emerg Med. (2001) 19:125–9. doi: 10.1053/ajem.2001.21321
11. Wu CL, Wang FT, Chiang YC, Chiu YF, Lin TG, Fu LF, et al. Unplanned emergency department revisits within 72 hours to a secondary teaching referral hospital in Taiwan. J Emerg Med. (2010) 38:512–7. doi: 10.1016/j.jemermed.2008.03.039
12. Huggins C, Robinson RD, Knowles H, Cizenski J, Mbugua R, Laureano-Phillips J, et al. Large observational study on risks predicting emergency department return visits and associated disposition deviations. Clin Exp Emerg Med. (2019) 6:144–51. doi: 10.15441/ceem.18.024
13. Shy BD, Loo GT, Lowry T, Kim EY, Hwang U, Richardson LD, et al. Bouncing back elsewhere: multilevel analysis of return visits to the same or a different hospital after initial emergency department presentation. Ann Emerg Med. (2018) 71:555–63. doi: 10.1016/j.annemergmed.2017.08.023
14. Hayward J, Hagtvedt R, Ma W, Gauri A, Vester M, Holroyd BR. Predictors of admission in adult unscheduled return visits to the emergency department. West J Emerg Med. (2018) 19:912–8. doi: 10.5811/westjem.2018.8.38225
15. Verelst S, Pierloot S, Desruelles D, Gillet JB, Bergs J. Short-term unscheduled return visits of adult patients to the emergency department. J Emerg Med. (2014) 47:131–9. doi: 10.1016/j.jemermed.2014.01.016
16. Sung CW, Lu TC, Fang CC, Lin JY, Yeh HF, Huang CH, et al. Factors associated with a high-risk return visit to the emergency department: a case-crossover study. Eur J Emerg Med. (2021) 28:394–401. doi: 10.1097/MEJ.0000000000000851
17. Liu SW. Risk factors of admission in 72-h return visits to emergency department. Tzu Chi Med J. (2021) 33:169–74. doi: 10.4103/tcmj.tcmj_155_20
18. Nuñez S, Hexdall A, Aguirre-Jaime A. Unscheduled returns to the emergency department: an outcome of medical errors? Qual Saf Health Care. (2006) 15:102–8. doi: 10.1136/qshc.2005.016618
19. Gulacti U, Lok U. Non-urgent adult patients in the emergency department. Turk J Emerg Med. (2018) 18:123. doi: 10.1016/j.tjem.2018.06.002
20. Wuerz RC, Milne LW, Eitel DR, Travers D, Gilboy N. Reliability and validity of a new five-level triage instrument. Acad Emerg Med. (2000) 7:236–42. doi: 10.1111/j.1553-2712.2000.tb01066.x
21. Grossmann FF, Delport K, Keller DI. Emergency severity index - deutsche übersetzung eines validen triageinstruments. Notfall Rettungsmed. (2009) 12:290–2. doi: 10.1007/s10049-009-1156-7
22. Charlson Comorbidity Index (CCI). Available online at: https://www.mdcalc.com/charlson-comorbidity-index-cci (accessed February 19, 2021).
23. Charlson ME, Pompei P, Ales KL, MacKenzie CR, A. new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
24. Dovjak P. Polypharmacy in elderly people. Wien Med Wochenschr. (2022) 172:109–13. doi: 10.1007/s10354-021-00903-0
25. Kuan WS, Mahadevan M. Emergency unscheduled returns: can we do better? Singapore Med J. (2009) 50:1068–71.
26. Sheikh S. Risk factors associated with emergency department recidivism in the older adult. West J Emerg Med. (2019) 20:931–8. doi: 10.5811/westjem.2019.7.43073
27. Soh CHW, Lin Z, Pan DST, Ho WH, Mahadevan M, Chua MT, et al. Risk factors for emergency department unscheduled return visits. Medicina. (2019) 55:457. doi: 10.3390/medicina55080457
28. Hutchinson CL, Curtis K, McCloughen A, Qian S, Yu P, Fethney J. Identifying return visits to the emergency department: a multi-centre study. Australas Emerg Care. (2021) 24:34–42. doi: 10.1016/j.auec.2020.05.007
29. Hasan O, Samad MA, Khan H, Sarfraz M, Noordin S, Ahmad T, et al. Leaving against medical advice from in-patients departments rate, reasons and predicting risk factors for re-visiting hospital retrospective cohort from a tertiary care hospital. Int J Health Policy Manag. (2019) 8:474–9. doi: 10.15171/ijhpm.2019.26
30. Choi M, Kim H, Qian H, Palepu A. Readmission rates of patients discharged against medical advice: a matched cohort study. PLoS ONE. (2011) 6:e24459. doi: 10.1371/journal.pone.0024459
31. Tan SY, Feng JY, Joyce C, Fisher J, Mostaghimi A. Association of hospital discharge against medical advice with readmission and in-hospital mortality. JAMA Netw Open. (2020) 3:e206009. doi: 10.1001/jamanetworkopen.2020.6009
32. Spooner KK, Saunders JJ, Chima CC, Zoorob RJ, Salemi JL. Increased risk of 30-day hospital readmission among patients discharged against medical advice: a nationwide analysis. Ann Epidemiol. (2020) 52:77–85. doi: 10.1016/j.annepidem.2020.07.021
33. Hassankhani H, Soheili A, Vahdati SS, Amin Mozaffari F, Wolf LA, Wiseman T. “Me first, others later” a focused ethnography of ongoing cultural features of waiting in an iranian emergency department. Int Emerg Nurs. (2019) 47:100804. doi: 10.1016/j.ienj.2019.100804
34. Bagi HRM, Khamnian Z, Hatami F, Vahdati SS, Yazdani R, Rahnemayan S. Assessment of social trust in relatives of discharged patients with personal consent and other relatives of patients. J Patient Exp. (2022) 9:23743735221113053. doi: 10.1177/23743735221113053
35. Tessitore A, Brennan-Cook J. Improving outpatient follow-up through innovative appointment scheduling at emergency department discharge. Adv Emerg Nurs J. (2021) 43:71–8. doi: 10.1097/TME.0000000000000340
36. Pereira L, Choquet C, Perozziello A, Wargon M, Juillien G, Colosi L, et al. Unscheduled-return-visits after an emergency department (ED) attendance and clinical link between both visits in patients aged 75 years and over: a prospective observational study. PLoS ONE. (2015) 10:e0123803. doi: 10.1371/journal.pone.0123803
Keywords: revisit, emergency medicine, emergency department, seniors, older person/people
Citation: Müller J, Keller DI and Slankamenac K (2024) Unplanned revisits of older patients to the emergency department. Front. Disaster Emerg. Med. 2:1342904. doi: 10.3389/femer.2024.1342904
Received: 04 January 2024; Accepted: 19 February 2024;
Published: 05 March 2024.
Edited by:
Muhammad Waseem, Lincoln Medical Center, United StatesReviewed by:
Umut Gulacti, Adiyaman University, TürkiyeCopyright © 2024 Müller, Keller and Slankamenac. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ksenija Slankamenac, a3NlbmlqYS5zbGFua2FtZW5hY0B1c3ouY2g=
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.