 Sabina Kapetanovic
Sabina Kapetanovic Maiken Due Nielsen1
Maiken Due Nielsen1 Sevtap Gurdal
Sevtap Gurdal Emma Claesdotter-Knutsson
Emma Claesdotter-Knutsson- 1Department of Behavioural Studies, University West, Trollhättan, Sweden
- 2Department of Psychology, Stockholm University, Stockholm, Sweden
- 3Department of Clinical Sciences, Faculty of Medicine, Lund University, Lund, Sweden
- 4Region Skåne, Child and Adolescent Psychiatry, Regional Outpatient Care, Lund University Hospital, Lund, Sweden
Introduction: While parenting is important for the development of adolescent problem gaming, it is unknown whether treatment of such problems in adolescents has a bearing on parenting. This study aims to explore the effects of individual relapse prevention (RP) treatment for adolescent problematic gaming on parenting practices and family dynamics.
Methods: A total of 72 adolescents (74% male; Mage = 14.5 SD = 1.4), participated in the study, with n = 39 in the intervention group and n = 33 in the control group. Pre- and post-treatment data were collected on parenting practices (e.g., monitoring and communication) and family dynamics. Changes in parenting measures were analyzed using the Wilcoxon signed-rank test and Svensson's method of change analysis.
Results: Adolescents in the intervention group reported reduced family conflict and changes in specific parenting practices, including less inquiry, fewer rules and intrusion regarding gaming post-treatment. In contrast, the control group reported a decline in family cohesion at post-treatment assessment.
Discussion: The results highlight adolescents' active role in shaping family dynamics and underscore the positive spillover effects of treating adolescent problematic gaming on parenting practices and family relationships. These findings are relevant to clinical practice and deepen our understanding of the relationship between adolescent gaming, parent-child interactions, and treatment spillover effects.
Trial registration number: ClinicalTrials.gov, NCT05506384, https://clinicaltrials.gov/ct2/show/NCT05506384.
Introduction
Gaming is a common leisure activity enjoyed by individuals of all age groups, especially among children and adolescents (Boniel-Nissim et al., 2024). However, there are instances where an individual's gaming habits surpass a threshold and affect their psychosocial functioning. Minors, in particular, are known to be more vulnerable to developing problematic gaming behaviors (Kuss and Griffiths, 2012), which are often present together with changes in school-related behavior, such as skipping classes (Rehbein et al., 2015) and poor academic performance (Müller et al., 2015).
The recognition of the potential negative impact of problematic gaming has led to the provisional introduction of internet gaming disorder (IGD) in the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5; American Psychiatric Association, 2013) and the introduction of gaming disorder (GD) in the 11th revision of the International Classification of Diseases (ICD-11; World Health Organization, 2019). The DSM-5 proposes nine diagnostic criteria for IGD, including a preoccupation with gaming, withdrawal symptoms, tolerance for gaming, unsuccessful attempts to quit, loss of interest in other activities, continued gaming despite negative consequences, denial of the extent of gaming, using gaming to regulate emotions, and problems in various areas of life caused by gaming. The ICD-11 defines GD as a persistent pattern of gaming behavior characterized by impaired control, prioritizing gaming over other activities, and continuing gaming despite negative consequences (World Health Organization, 2019). Similar to the DSM-5′s classification, the problems must have persisted for at least 12 months. The prevalence of problematic gaming varies across studies as researchers use different diagnostic frameworks and instruments. A recent German study (Montag et al., 2019) suggested a prevalence rate of 5.7% for IGD when using the proposed DSM-5 criteria. In contrast, the ICD-11 framework proposed a slightly more conservative prevalence rate of 3.3% for GD. While the prevalence of problematic gaming in the general Swedish youth population is 2.3% (Gerdner and Håkansson, 2022) a significantly higher prevalence of 33% is found in clinical youth populations (André et al., 2020).
Treatment studies, primarily based on cognitive-behavioral therapy (CBT) approaches, have shown promise in reducing symptoms of IGD and related issues (King et al., 2017; Stevens et al., 2019; Kim et al., 2022). For example, a recent Swedish randomized controlled study (Kapetanovic et al., 2023) evaluated the effectiveness of an adapted form of relapse prevention (RP; Marlatt and Donovan, 2005) for treating adolescents with problem gaming. The RP for problematic gaming was developed as an individual therapeutic intervention for children between 13 and 18 years, with 5–7 sessions, aiming to identify high-risk situations that could trigger relapse and use cognitive and behavioral coping strategies to manage these situations effectively (Marlatt and Donovan, 2005). In its essence, RP operates as a form of tertiary prevention. While the potential of CBT and RP treatment programs in addressing problematic gaming has shown promising outcomes both in Sweden (André et al., 2023) and elsewhere (King et al., 2017; Stevens et al., 2019), little is known about the potential spillover effect of treatment on the larger context where children grow and develop.
Through the lens of developmental psychology, it is clear that children and adolescents are not independent entities; instead, they are intricately connected to their social environment (Sameroff, 2010). Accordingly, children and their behaviors develop in mutual and dynamic interactions with their social context. Indeed, high-quality parent-child relationships characterized by appropriate monitoring, support, and open communication are associated with reduced or low-risk gaming (Bonnaire and Phan, 2017; Choo et al., 2015; Schneider et al., 2017; Nielsen et al., 2020). On the other hand, low-quality parent-child relationships marked by conflict, poor family cohesion and coercive parenting have been linked to an increased risk of engaging in excessive and problematic gaming (Bonnaire and Phan, 2017; Choo et al., 2015; Da Charlie et al., 2011; King and Delfabbro, 2017). Additionally, research suggests that problem gamers spend less time engaged in activities with their parents (Jeong and Kim, 2011) and have generally poorer family environments than engaged gamers (i.e., those who game recreationally; Da Charlie et al., 2011). Thus, it is evident that parent-child relationships play an important role for child and adolescent gaming. However, it is also likely that children and adolescents also have impact on parents' attitudes, practices, and general parent-child relationships, given the nature of parents' and children's interactions (Sameroff, 2010). Indeed, studies suggest that adolescent IGD-symptoms predict more reactive rule setting and parental control yet poorer parent-child communication and parental care (Koning et al., 2018; Gan et al., 2021). This indicates that parent-child relationships are bidirectional: changes in parents' behaviors can predict changes in children's behaviors, and conversely, children's and adolescents' behaviors can influence parenting practices. Therefore, it is possible that children who undergo changes in their gaming behavior as a result of gaming treatment may also experience changes in the family environment and parent-child relationships.
Clinical studies on adolescent gaming show evidence of parent-child relationships and interactions, as well as parental involvement in child treatment being critical for beneficial treatment outcomes (Bonnaire et al., 2019; Nielsen et al., 2021). However, to what extent parenting and family dynamics change as a result of a treatment is less explored. There are, however, indications that not only can parents impact the treatment effects, but that successful treatment may also have spillover effect on parents and their relationships with their children. In fact, improvements in adolescents' depressive symptoms after treatment have been found to reduce parent-child as well as marital conflict, even when the intervention is not specifically targeting family interactions (Howard et al., 2019). In addition, reduction in adolescent substance-use after treatment seems predict reductions of mothers' psychological distress, demonstrating the positive spillover effects of treatment on the parents (Bertrand et al., 2013). If parent-child relationships are bidirectional, as suggested by scholars (Sameroff, 2010; Nielsen et al., 2020; Bonnaire et al., 2019), improvement in adolescent mental health and behaviors, including reductions in gaming problems, would inevitably have an effect on parenting and family dynamics, providing parents and their children with more high-quality interactions. As psychological interventions targeting adolescent internet related problems generally seem to have spillover effects on several aspects of adolescent psychosocial functioning (Lo et al., 2023), the spillover effect on parenting could be anticipated, even though it is not often evaluated. Therefore, exploring and understanding the potential changes in the overall parent-child relationship brought about by treatment in the context of problematic gaming is key. Following the lines of earlier research (Nielsen et al., 2020; Bonnaire et al., 2019) and theoretical perspectives (Sameroff, 2010), the aim of the present study was to examine whether, and to what extent, RP treatment for adolescent problematic gaming has impact on aspects of parent-child relationships. Specifically, we wanted to investigate whether post-treatment differences exist between adolescents in the intervention group and those in the control group regarding parent-child communication, family cohesion, and family conflict. Findings from this study could contribute to a more comprehensive understanding of the interconnected dynamics between parent-child relationships and problematic gaming and inform therapeutic approaches that consider the broader dynamics within families.
Materials and methods
The current study is part of a larger project (Kapetanovic et al., 2023) investigating the needs of both parents and children regarding problem gaming (Werner et al., 2024; Gurdal et al., 2023), as well as evaluating the effectiveness of treatments for problem gaming among children and youth (André et al., 2023).
Procedure
To identify adolescents with gaming-related problems, between September 2021 and December 2022, we conducted a screening for problematic gaming among individuals aged 13–18 who were first-time visitors to Child and Adolescent Psychiatry (CAP) clinics in Region Skåne, Sweden. The screening was conducted using Game Addiction Scale for Adolescents (GASA; Lemmens et al., 2009) as part of the standard intake procedure at CAP Region Skåne. Among 2,630 new CAP visits, 622 (≈24%) registered patients were screened with GASA. This relatively low figure was attributed to administrative issues during the screening period. Of the 622 screened patients, 123 (~20%) met the cut-off criteria for IGD and were subsequently invited to participate in a randomized control study evaluating treatment for problematic gaming in adolescents (Kapetanovic et al., 2023). The patients and their caregivers received both written and oral information regarding the study from their CAP contacts. Additionally, written information was displayed on posters in the waiting rooms of all CAP clinics in Skåne. Of the 123 invited patients, 115 patients agreed to participate in the project. However, 11 patients were excluded due to incorrect inclusion, including being underage (n = 1), not meeting the criteria (n = 2), or failing to complete post-treatment measures (n = 8). After these exclusions, 104 adolescents remained in the study.
Patients were randomly assigned to either a treatment or control group using a randomization method that involved preparing paper slips labeled as either control or treatment (Singh, 2006). Patients in the intervention group (n = 48) received RP treatment for problematic gaming, whereas those in the control group (n = 56) received treatment as usual (Kapetanovic et al., 2023). Measures of parent-child relationships were introduced as an additional component of the study 3 months after the first participants were enrolled in the larger project (thus in January 2022). The pre-treatment assessment was conducted 1 week prior to the start of the treatment, while the post-treatment assessment took place 3 months after the completion of the treatment. The adolescents and the caregivers of children below the age of 15 provided informed consent for study participation.
Participants
The total population for the current study was slightly smaller than that of the overall RCT study, with a sample size of N = 81. Of those, n = 9 participants did not provide data for the relevant measures and were therefore excluded from the analysis. Consequently, the final analytical sample consisted of N = 72 participants (74% male) aged 13–18, with a mean age of 14.5 (SD = 1.40). Of these, n = 39 participants were in the intervention group, and n = 33 were in the control group. The control group received Treatment as usual (TAU) at their home clinic and of existing practice. The TAU included counseling, medication for ADHD, antidepressants, or referral to other units. Information on the participants' gender, age, housing situation, and other diagnosis was collected (see Table 1).
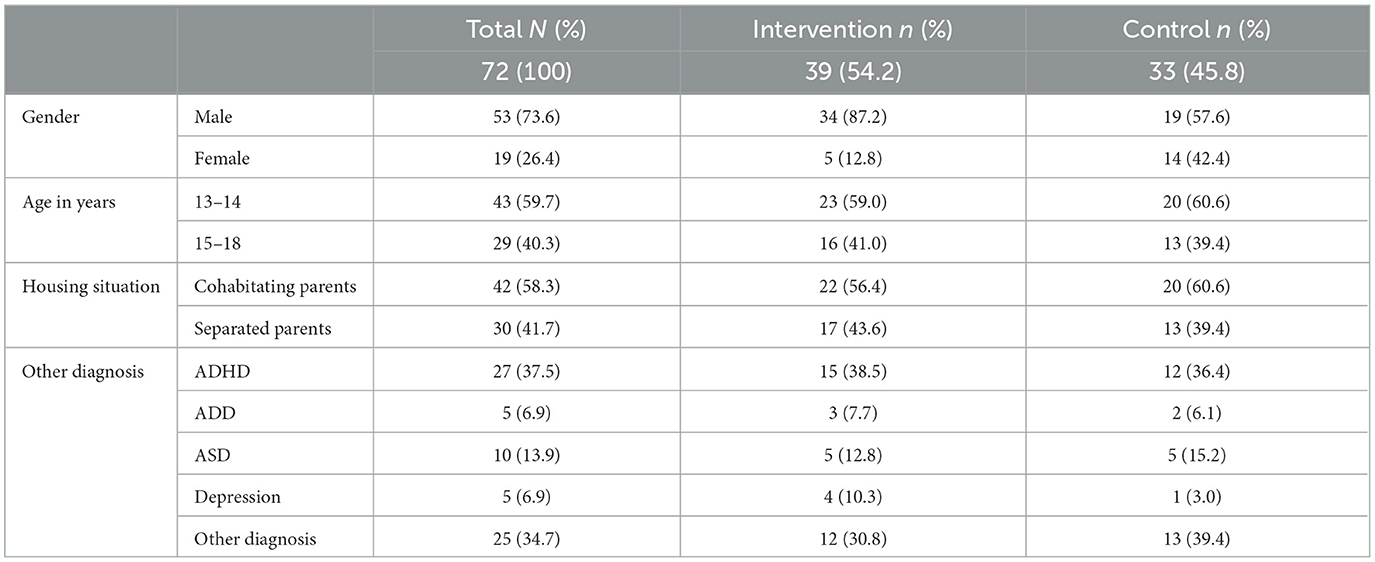
Table 1. Sample characteristics.
Intervention
The study is based on a randomized controlled study evaluating an RP treatment for problematic gaming (Kapetanovic et al., 2023). The treatment manual was based on the theoretical grounds of RP for alcohol and substance abuse (Marlatt and Donovan, 2005) however adapted to be suitable for children with problematic gaming. The participants in the intervention group received RP treatment at their respective CAP clinics or via a video link. The treatment was performed by a licensed psychologist, a social worker, or a psychiatrist, all competent in CBT. Notably, the parents did not participate nor were they present during the treatment sessions. The treatment consisted of three main components: (1) setting goals, (2) understanding and identifying high-risk situations and problem behaviors, and (3) consolidating the new activity schedule and identifying future high-risk behaviors. The participants received theme-specific homework between sessions to be evaluated and discussed at the next meeting. The RP treatment consisted of seven sessions of 45 min each over a period of seven to 9 weeks. The treatment was considered completed if the participants completed a minimum of five sessions.
Measures
Parent-child communication
To evaluate aspects of parent-child communication, a modified version of the parental monitoring scale (Stattin and Kerr, 2000) was employed, including items that specifically assess parent-child communication on gaming. The instrument consisted of 26 items organized into six subscales (see Supplementary Table 1). The first subscale, child disclosure (T1: α = 0.55; T2: α = 0.54), comprises seven items, assessing the extent to which children openly share information about their experiences. An example of an original item is, “Do you like to tell your parents where you went and what you did during the evening?” and an example of an added item is “Do you talk to your parents about your gaming activities?” Parental knowledge (T1: α = 0.71; T2: α = 0.63) assesses the extent to which parents are aware of their children's whereabouts and activities using five items, such as “Do your parents know what you spend your money on?” and “Do your parents know how much of your time is spent on gaming?” Parental solicitation (T1: α = 0.70; T2: α = 0.69) examines parents' efforts to gather information about their children's whereabouts and activities, using six items, such as “During the past month, how often have your parents started a conversation with you about your free time?” and “How often do your parents inquire about your gaming activities?” Parental control (T1: α = 0.72; T2: α = 0.83) consists of five items to evaluate the frequency with which parents establish rules or limitations, such as “How often do your parents set rules or limits on where you go right after school?” and “How often do your parents set rules or limits on your gaming activities?” Lastly, child feeling overly controlled by parents (α = 0.79; T2: α = 0.71) comprised three items to assess the extent to which children feel controlled by their parents, such as “Do you feel as though your parents control everything in your life?” and “Do you feel that your parents are overly intrusive in your gaming activities?” Participants respond to the items using a 5-point scale, with the answer options tailored to match the specific content of each item.
Family dynamics
To evaluate family dynamics, the general family functioning scale (Bloom, 1985) was employed (see Supplementary Table 2). This scale evaluates family cohesion and conflict as indicators of overall family dynamics. Participants were asked to rate how much each statement applied to their family. Family cohesion (T1: α = 0.79; T2: α = 0.71) was assessed using six items that capture aspects of the emotional bonding and support within the family. An example of an item is “There is a feeling of togetherness in our family.” Family conflict (T1: α = 0.62; T2: α = 0.67 was evaluated using five items that capture instances of discord and physical aggression among family members. An example of an item is, “We fight a lot in my family.” Participants respond to the items using a 4-point Likert scale, ranging from 1 = not true at all to 4 = very true.
Data analysis
Non-parametric tests were utilized for data analysis to account for the lack of assumptions regarding normality and to enhance robustness against outliers. This approach allows for a more reliable examination of the data, particularly when working with ordinal or non-normally distributed variables (McKillup, 2011). Consequently, the Wilcoxon signed-rank test was used to compare pre- and post-treatment results. Generally, a p-value of ≤ 0.05 denotes statistical significance; however, it is also crucial to evaluate its clinical significance. There are instances where statistical significance is not achieved due to a small sample size, yet the findings remain clinically relevant (Bland, 2015). Clinical relevance emphasizes the practical impact of a finding, focusing on whether the observed difference is meaningful and applicable in real-world clinical settings, regardless of statistical significance (Abdul Raheem, 2024). Thus, this study considers statistical and clinical significance when interpreting the results.
To evaluate changes in individuals' responses to the gaming-related items from pre- to post-treatment, Svensson's method (Svensson, 1993, 2001) for analyzing ordinal data was employed. This method calculates three main measures. The proportion of agreement between two measures among individuals is shown as percent agreement (PA, 0–100%). The degree of systematic change in responses on an item at two timepoints is measured by relative position (RP). Relative position (RP) varies between −1 and +1, indicating either improvement or deterioration from pre-treatment assessment. Relative concentration (RC, −1 to +1) is another measure used to analyze the shift in ratings. RC is calculated as the difference between two probabilities, where a positive value indicates that the responses are more concentrated toward post-test, and a negative value indicates that the responses are more concentrated at pre-test. The difference is statistically significant if the 95% confidence interval does not cover zero.
Results
Tables 2A, B present the descriptive statistics of the outcome variables in the intervention and control groups at pre- and post-treatment assessment.
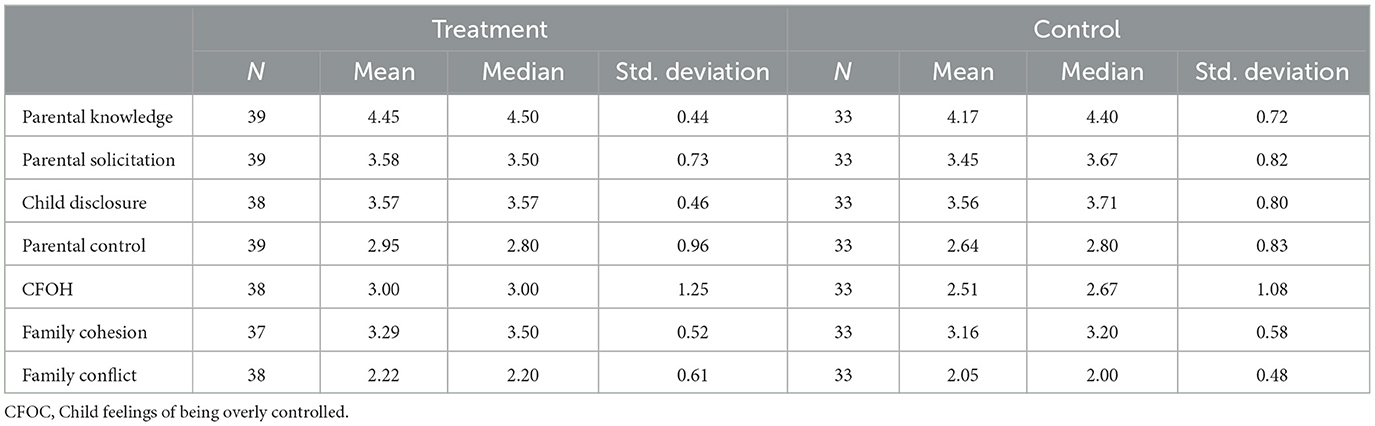
Table 2A. Descriptive statistics of the pre-treatment measures in the control and intervention groups.
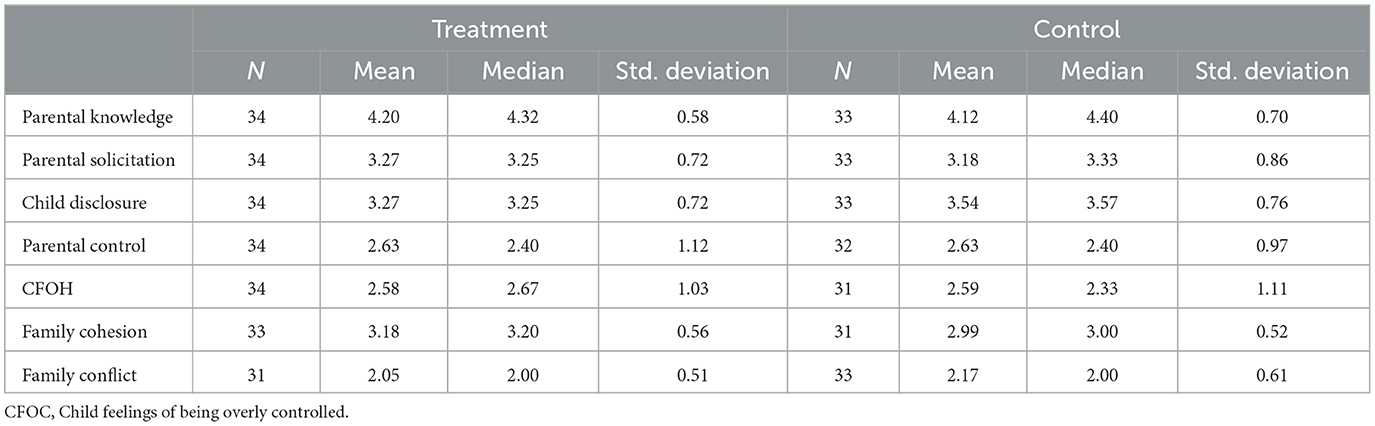
Table 2B. Descriptive statistics of the post-treatment measures in the control and intervention groups.
Table 3 displays the results of the Wilcoxon signed-rank test on the differences between intervention and control groups at pre- and post-treatment assessments. The p-values reaching statistical significance are highlighted in bold. The analysis indicates that the intervention group showed significantly less family conflict post-treatment, while the control group exhibited significantly less family cohesion post-treatment. Notably, none of the measures of parent-child communication reached statistical significance.
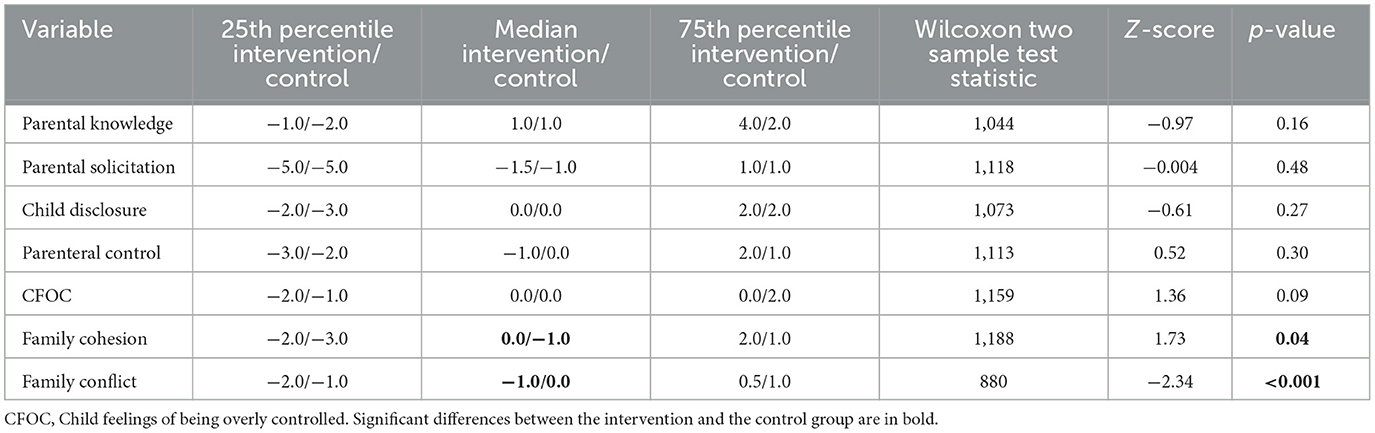
Table 3. Results of the Wilcoxon two-sample test on group level differences in scores at pre- and post-treatment.
Table 4 displays the changes observed in single-item gaming responses between pre- and post-treatment assessments. High RP and/or RC values and low RV values indicate a more consistent and uniform change pattern within the group. Conversely, high RV values suggest deviations from the common change pattern, indicating a more diverse pattern of change. The results show a trend where adolescents in the treatment group reported a decrease in parental inquiries about their gaming habits (item V1p), fewer rules about gaming (item V2e), and less parenting intrusion into gaming activities (V2h) at the post-test, as compared to pre-test.
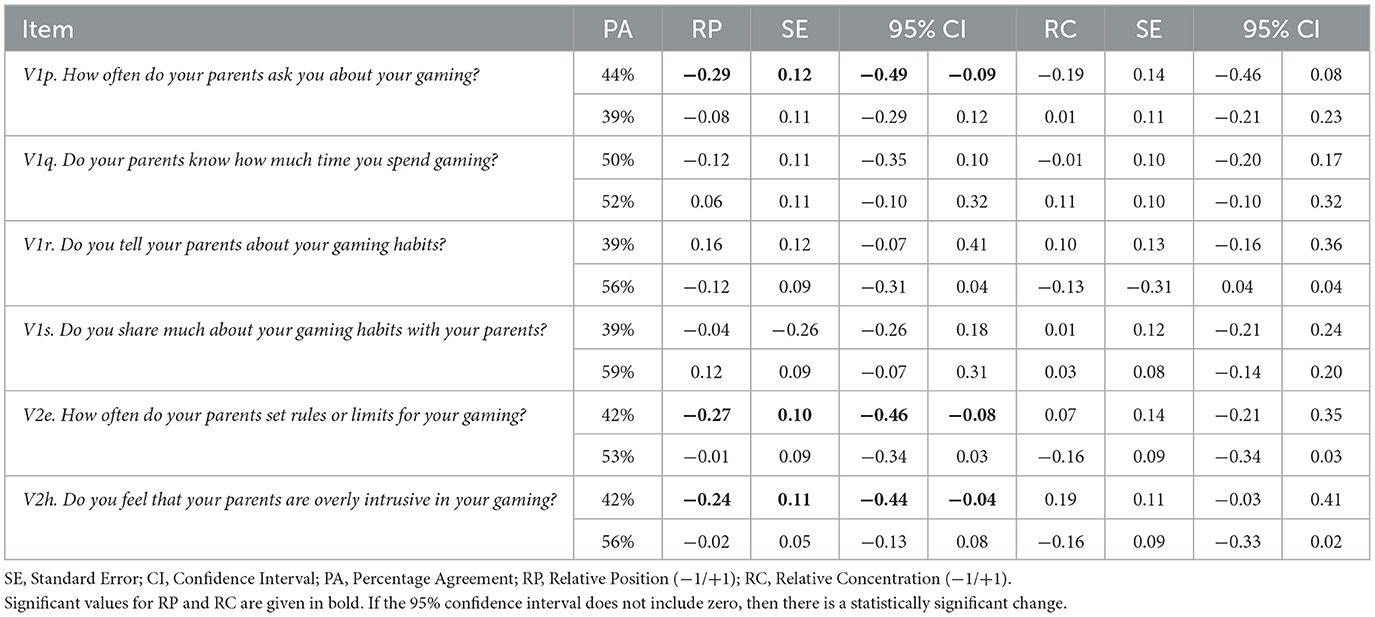
Table 4. Test-retest analysis using Svensson's method for paired ordinal data for the adolescents in the treatment (1st row) and control (2nd row) group.
Discussion
The present study aimed to investigate changes in parent-child relationships following adolescents undergoing individual RP treatment for problematic gaming. The findings of the present study revealed several insights. First, adolescents in the intervention group reported less family conflict at the post-treatment assessment compared to the control group. In addition, adolescents in the control group indicated lower levels of family cohesion than the intervention group, which suggests that RP had a positive spillover effect on the quality of family dynamics, including interactions between parents and their children. These findings are congruent with prior research showing spillover effects from treatment to parent-child relationships (Howard et al., 2019; Bertrand et al., 2013). One possible explanation for this finding is that successful treatment of problematic gaming (André et al., 2023) may decrease parental distress, as has been observed in treatment studies related to adolescent substance abuse (Bertrand et al., 2013). Previous research has found that a reduction in parental distress is associated with reduced family conflicts and increased parental nurturing behavior, possibly through greater parental cognitive and emotional investment in the parent-child relationship (Kahng et al., 2008). As such, although parents play a critical role in adolescent gaming and in the efficacy of treating gaming problems (Nielsen et al., 2020; Bonnaire et al., 2019), the successful treatment of problematic gaming (André et al., 2023) is likely to influence the general family dynamics. These findings are consistent with the developmental psychopathology perspective, where children are not merely participants but active agents directly influencing the function and wellbeing of the family (Sameroff, 2010). In this perspective, interactions between parents and children are reciprocal; that is, the behaviors and attitudes of parents have an impact on their children, while the behaviors and attitudes of children also influence their parents.
Given the positive changes observed in family interactions, it might have been expected that overall parent-child communication, including general child disclosure, would also improve. However, our findings did not support this expectation. One possible explanation is that improvements in family dynamics and relationships, which form the broader family climate (Darling and Steinberg, 1993; Kapetanovic et al., 2019) may be necessary precursors for changes in more specific aspects of parental practices. As family interactions strengthen, they may provide the foundation for more meaningful and open communication between parents and children. As our study design did not allow for testing this hypothesis, it warrants further investigation in future research.
We found several noteworthy differences in gaming-specific parenting practices. Adolescents who received treatment for problematic gaming reported that parents asked fewer questions about gaming, set fewer rules for gaming, and interfered less with gaming activities post-treatment compared to the control group. Several potential explanations can be considered for these changes in parenting practices. Given that treatment programs for problematic gaming often result in reduced gaming time and problem symptoms (Stevens et al., 2019; André et al., 2023), the perceived necessity for rule-setting and monitoring adolescent gaming behaviors might have diminished. Furthermore, a qualitative study conducted by our research team showed that adolescents who underwent treatment engaged more in alternative leisure activities and spent more time with parents due to reduced gaming (Gurdal et al., 2023). These changes may have affected the quality of the parent-child relationship, including different and more positive patterns of interactions between parents and their adolescent children, which ultimately could reduce the need for monitoring and rule-setting. As aforementioned, successful treatment of the problem could have alleviated parental stress and conflict within the family, contributing to an overall more harmonious environment where parents felt less inclined to intrude on adolescents' activities.
Conversely, adolescents in the control group reported a general decline in family cohesion at the post-treatment assessment compared to the pre-test. This suggests that perceived family connectedness waned over time without intervention. These findings are consistent with prior research that identified links between IGD and decreased participation in social activities involving parents (Jeong and Kim, 2011). Furthermore, the literature also indicates a link between problematic gaming and lower levels of parental warmth and emotional availability (Da Charlie et al., 2011; King and Delfabbro, 2017). These trends emphasize the necessity of providing adolescents with timely treatment, not only to safeguard the wellbeing of the adolescents but also to prevent further rifts in the parent-child relationship and overall family dynamics.
In sum, the findings from our study suggest that the treatment of adolescent problematic gaming has some spillover effects on overall parent-child relationships, including reduced family conflict, as well as some specific parenting practices relating to gaming, including parental interference in gaming activities. Our findings are congruent with the notion that adolescents are active participants in the family dynamic and that changes brought about by successful treatment have the potential to affect parental practices and family interactions (Sameroff, 2010). By exploring these interconnected relationships, the study underscores the importance of considering the family context in both the development and implementation of treatment programs for problematic gaming. This holistic approach can enhance the effectiveness of interventions and support healthier family environments, ultimately promoting better outcomes for both adolescents and their families.
Limitations
This study has several limitations that should be considered when interpreting the results. Firstly, the participants presented various mental health issues alongside problematic gaming. Consequently, it is essential to interpret the findings within the clinical framework of Swedish adolescents in CAP settings. Given the comorbidity of problematic gaming with other psychiatric disorders (Gerdner and Håkansson, 2022; André et al., 2020), this study still offers valuable insights, particularly relevant within clinical contexts. Another important limitation is that participants were recruited from a sample of adolescents seeking treatment at CAP clinics. As participants visited CAP clinics with various non-gaming-related health complaints, they were subject to other forms of treatment, including medical and therapeutic intervention. Consequently, these other treatments might have inadvertently influenced the outcomes in both the intervention and control groups. Moreover, alpha for some of the measures was low (e.g., child disclosure). It is possible that the clinical group of adolescents included in the CAP clinics may have different interactions and communication with parents in comparison with children in the general population who these measures were developed for and are tested with. The use of a single-item analysis design may have alleviated this limitation. Additionally, our relatively small sample size may have limited the statistical power of the analysis (Button et al., 2013). As a result, no further analyses based on adolescent gender or age—both of which an important factors in parent-child relationships as well as gaming (André et al., 2020; Koning et al., 2018) could be conducted. It is essential to acknowledge that there might be additional differences between the groups, which a larger and more diverse participant pool could uncover. An additional limitation of the study lies in the absence of follow-up assessments regarding the impact of therapy on participants' problem gaming and their parent-child relationships over longer time. Consequently, the durability of treatment effects remains uncertain. Furthermore, the exclusion of parents from the intervention represents a limitation, as involving parents is crucial when addressing life transitions in children and adolescents (Bonnaire et al., 2019). Indeed, considering that the child development happens in the dynamic interaction with the family (Sameroff, 2010), it is plausible that a reduction in problematic gaming could be achieved by not only focusing on the child's treatment but also by enhancing family dynamics. Lastly, the study lacks parents' thoughts about parental communication and parent child relation, potentially yielding divergent responses compared to those provided by the youth (Kapetanovic and Boson, 2022). Despite these limitations, the results provide valuable knowledge that may be used to develop and improve treatment of adolescent problematic gaming.
Future research
Future research should aim to build on the findings of the present study by incorporating a larger sample size and longer follow-up periods to better understand the lasting effects of treatment on both adolescents and their parent-child relationships. Additionally, developing more specific measures related to gaming and parenting practices would enhance the accuracy of assessing the nuances in these dynamics. Including parental reports in future studies could also provide a more comprehensive perspective on the changes in family interactions and parenting strategies. By addressing these aspects, researchers can further clarify the complex interplay between problematic gaming and family functioning, ultimately contributing to more effective treatment interventions that support not only the adolescents but also their families in navigating these challenges.
Conclusion
The present study contributes valuable insights into the complex interplay between adolescents' problematic gaming and parent-child relationships. Our research highlights the significance of addressing adolescent problematic gaming to improve family wellbeing and parent-child relationships. The findings reveal that adolescents who had undergone RP for problematic gaming experience reduced family conflict, while adolescents in the control group reported significantly less family cohesion, suggesting that addressing problematic gaming can have spillover effects on general family interactions. Moreover, this study uncovered changes in specific parenting practices related to gaming. Adolescents who received treatment reported fewer questions, rules, and interference in gaming activities. Such a finding indicates that treatment of adolescent gaming problems could lead to less need for parental monitoring, which inevitably could provide more opportunities for other high-quality interactions between parents and their children. The implication of our study holds significant relevance for both clinical practice and our understanding of the intricate interplay between problematic gaming in youth, parent-child relationships, and treatment spillover effects. In particular, our findings underscore the urgency of timely interventions which, in a holistic manner, could have a bearing on both adolescent behavior and mental health, and improved family dynamics.
Data availability statement
The de-identified data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study involving humans was approved by Swedish Ethical Review Authority (Ref 2019-04797, December 13, 2019; Ref 2021-05592-01, January 3 202; Ref 2022-01289-02, March 15, 2022). The study was conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin as well as the participants themselves.
Author contributions
SK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. MD: Writing – original draft, Writing – review & editing. SG: Funding acquisition, Project administration, Writing – original draft, Writing – review & editing. EC-K: Funding acquisition, Project administration, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Swedish Research Council for Health, Working Life and Welfare (FORTE) under Grant [No. 2021-01696].
Acknowledgments
We acknowledge the time and efforts from children, adolescents, and clinicians participating in the study. We also acknowledge Frida André and Mats Nilsson for their support with data structuring and analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. Specifically, ChatGPT was used to address language issues, such as awkward phrasing and grammatical errors, throughout the manuscript as part of the language proofreading process. ChatGPT has not been used for any other purposes.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdpys.2024.1492685/full#supplementary-material
References
Abdul Raheem, Y. (2024). Statistical significance versus clinical relevance: key considerations in interpretation medical research data. Ind. J. Commun. Med. 49, 791–795. doi: 10.4103/ijcm.ijcm_601_23
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5™, 5th Edn. Washington, DC: American Psychiatric Association.
André, F., Broman, N., Håkansson, A., and Claesdotter-Knutsson, E. (2020). Gaming addiction, problematic gaming and engaged gaming-prevalence and associated characteristics. Addict. Behav. Rep. 12:100324. doi: 10.1016/j.abrep.2020.100324
André, F., Kapetanovic, S., Einarsson, I., Trebbin Harvard, S., Franzén, L., Möttus, A., et al. (2023). Relapse prevention therapy for internet gaming disorder in Swedish child and adolescent psychiatric clinics: a randomized controlled trial. Front. Psychiat. 14:1256413. doi: 10.3389/fpsyt.2023.1256413
Bertrand, K., Richer, I., Brunelle, N., Beaudoin, I., Lemieux, A., and Menard, J.-M. (2013). Substance abuse treatment for adolescents: how are family factors related to substance use change? J. Psychoact. Drugs 45, 28–38. doi: 10.1080/02791072.2013.763560
Bloom, B. L. A. (1985). factor analysis of self-report measures of family functioning. Fam. Process 24, 225–239. doi: 10.1111/j.1545-5300.1985.00225.x
Boniel-Nissim, M., Marino, C., Galeotti, T., Blinka, L., Ozolina, K., Craig, W., et al. (2024). A Focus on Adolescent Social Media Use and Gaming in Europe, Central Asia and Canada. Health Behaviour in School-aged Children International Report From the 2021/2022 Survey. Volume 6. Copenhagen: WHO Regional Office for Europe.
Bonnaire, C., Liddle, H. A., Har, A., Nielsen, P., and Phan, O. (2019). Why and how to include parents in the treatment of adolescents presenting Internet gaming disorder? J. Behav. Addict. 8, 201–212. doi: 10.1556/2006.8.2019.27
Bonnaire, C., and Phan, O. (2017). Relationships between parental attitudes, family functioning and Internet gaming disorder in adolescents attending school. Psychiat. Res. 255, 104–110. doi: 10.1016/j.psychres.2017.05.030
Button, K. S., Ioannidis, J. P., Mokrysz, C., Nosek, B. A., Flint, J., Robinson, E. S., et al. (2013). Power failure: why small sample size undermines the reliability of neuroscience. Nat. Rev. Neurosci. 14, 365–376. doi: 10.1038/nrn3475
Choo, H., Sim, T., Liau, A. K., Gentile, D. A., and Khoo, A. (2015). Parental influences on pathological symptoms of video-gaming among children and adolescents: a prospective study. J. Child Fam. Stud. 24, 1429–1441. doi: 10.1007/s10826-014-9949-9
Da Charlie, C. W., HyeKyung, C., and Khoo, A. (2011). Role of parental relationships in pathological gaming. Proc. Soc. Behav. Sci. 30, 1230–1236. doi: 10.1016/j.sbspro.2011.10.238
Darling, N., and Steinberg, L. (1993). Parenting style as context: an integrative model. Psychol. Bull. 113:487. doi: 10.1037/0033-2909.113.3.487
Gan, X., Li, H., Li, M., Yu, C., Jin, X., Zhu, C., et al. (2021). Parenting styles, depressive symptoms, and problematic online game use in adolescents: a developmental cascades model. Front. Publ. Health 9:710667. doi: 10.3389/fpubh.2021.710667
Gerdner, A., and Håkansson, A. (2022). Prevalence and comorbidity in a Swedish adolescent community sample-gambling, gaming, substance use, and other psychiatric disorders. BMC Psychiat. 22:594. doi: 10.1186/s12888-022-04218-1
Gurdal, S., Kapetanovic, S., Einarsson, I., Boson, K., and Claesdotter-Knutsson, E. (2023). Adolescents' perceptions of a relapse prevention treatment for problematic gaming-a qualitative study. Healthcare 2023:366. doi: 10.3390/healthcare11172366
Howard, K. R., Reinecke, M. A., Lavigne, J. V., Gouze, K. R., and Jordan, N. (2019). Marital and parent-child relationships during treatment for adolescent depression: child-driven and bidirectional effects. J. Abnorm. Child Psychol. 47, 1841–1850. doi: 10.1007/s10802-019-00566-x
Jeong, E. J., and Kim, D. H. (2011). Social activities, self-efficacy, game attitudes, and game addiction. Cyberpsychol. Behav. Soc. Network. 14, 213–221. doi: 10.1089/cyber.2009.0289
Kahng, S. K., Oyserman, D., Bybee, D., and Mowbray, C. (2008). Mothers with serious mental illness: when symptoms decline does parenting improve? J. Fam. Psychol. 22:162. doi: 10.1037/0893-3200.22.1.162
Kapetanovic, S., and Boson, K. (2022). Discrepancies in parents' and adolescents' reports on parent-adolescent communication and associations to adolescents' psychological health. Curr. Psychol. 41, 4259–4270. doi: 10.1007/s12144-020-00911-0
Kapetanovic, S., Gurdal, S., Einarsson, I., Werner, M., André, F., Håkansson, A., et al. (2023). Relapse prevention therapy for problem gaming or internet gaming disorder in Swedish child and youth psychiatric clinics: protocol for a randomized controlled trial. JMIR Res. Protocol. 12:e44318. doi: 10.2196/44318
Kapetanovic, S., Skoog, T., Bohlin, M., and Gerdner, A. (2019). Aspects of the parent-adolescent relationship and associations with adolescent risk behaviors over time. J. Fam. Psychol. 33:1. doi: 10.1037/fam0000436
Kim, J., Lee, S., Lee, D., Shim, S., Balva, D., Choi, K.-H., et al. (2022). Psychological treatments for excessive gaming: a systematic review and meta-analysis. Sci. Rep. 12:20485. doi: 10.1038/s41598-022-24523-9
King, D. L., and Delfabbro, P. H. (2017). Features of parent-child relationships in adolescents with Internet gaming disorder. Int. J. Ment. Health Addict. 15, 1270–1283. doi: 10.1007/s11469-016-9699-6
King, D. L., Delfabbro, P. H., Wu, A. M., Doh, Y. Y., Kuss, D. J., Pallesen, S., et al. (2017). Treatment of Internet gaming disorder: an international systematic review and CONSORT evaluation. Clin. Psychol. Rev. 54, 123–133. doi: 10.1016/j.cpr.2017.04.002
Koning, I. M., Peeters, M., Finkenauer, C., and Van Den Eijnden, R. J. J. M. (2018). Bidirectional effects of Internet-specific parenting practices and compulsive social media and Internet game use. J. Behav. Addict. 7, 624–632. doi: 10.1556/2006.7.2018.68
Kuss, D. J., and Griffiths, M. D. (2012). Online gaming addiction in children and adolescents: a review of empirical research. J. Behav. Addict. 1, 3–22. doi: 10.1556/JBA.1.2012.1.1
Lemmens, J. S., Valkenburg, P. M., and Peter, J. (2009). Development and validation of a game addiction scale for adolescents. Media Psychol. 12, 77–95. doi: 10.1080/15213260802669458
Lo, C. K. M., Chan, K. L., Yu, L., Chui, W. W. H., and Ip, P. (2023). Long-term effects of psychosocial interventions on internet-related disorders: a meta-analysis. Comput. Hum. Behav. 138:107465. doi: 10.1016/j.chb.2022.107465
Marlatt, G. A., and Donovan, D. M. (2005). Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors. New York, NY: Guilford Press.
McKillup, S. (2011). Statistics Explained: an Introductory Guide for Life Scientists. Cambridge: Cambridge University Press.
Montag, C., Schivinski, B., Sariyska, R., Kannen, C., Demetrovics, Z., Pontes, H. M., et al. (2019). Psychopathological symptoms and gaming motives in disordered gaming-A psychometric comparison between the WHO and APA diagnostic frameworks. J. Clin. Med. 8:1691. doi: 10.3390/jcm8101691
Müller, K. W., Janikian, M., Dreier, M., Wölfling, K., Beutel, M. E., Tzavara, C., et al. (2015). Regular gaming behavior and internet gaming disorder in European adolescents: results from a cross-national representative survey of prevalence, predictors, and psychopathological correlates. Eur. Child Adolesc. Psychiat. 24, 565–574. doi: 10.1007/s00787-014-0611-2
Nielsen, P., Christensen, M., Henderson, C., Liddle, H. A., Croquette-Krokar, M., Favez, N., et al. (2021). Multidimensional family therapy reduces problematic gaming in adolescents: a randomised controlled trial. J. Behav. Addict. 10, 234–243. doi: 10.1556/2006.2021.00022
Nielsen, P., Favez, N., and Rigter, H. (2020). Parental and family factors associated with problematic gaming and problematic internet use in adolescents: a systematic literature review. Curr. Addict. Rep. 7, 365–386. doi: 10.1007/s40429-020-00320-0
Rehbein, F., Kliem, S., Baier, D., Mößle, T., and Petry, N. M. (2015). Prevalence of internet gaming disorder in German adolescents: diagnostic contribution of the nine DSM-5 criteria in a state-wide representative sample. Addiction 110, 842–851. doi: 10.1111/add.12849
Sameroff, A. A. (2010). unified theory of development: a dialectic integration of nature and nurture. Child Dev. 81, 6–22. doi: 10.1111/j.1467-8624.2009.01378.x
Schneider, L. A., King, D. L., and Delfabbro, P. H. (2017). Family factors in adolescent problematic Internet gaming: a systematic review. J. Behav. Addict. 6, 321–333. doi: 10.1556/2006.6.2017.035
Singh, G. (2006). Randomization made easy for small size controlled clinical trials. JIAMSE 16, 75–78.
Stattin, H., and Kerr, M. (2000). Parental monitoring: a reinterpretation. Child Dev. 71, 1072–1085. doi: 10.1111/1467-8624.00210
Stevens, M. W., King, D. L., Dorstyn, D., and Delfabbro, P. H. (2019). Cognitive-behavioral therapy for Internet gaming disorder: a systematic review and meta-analysis. Clin. Psychol. Psychother. 26, 191–203. doi: 10.1002/cpp.2341
Svensson, E. (1993). Analysis of Systematic and Random Differences Between Paired Ordinal Categorical Data (Thesis), Göteborg University, Göteborg, Sweden.
Svensson, E. (2001). Construction of a single global scale for multi-item assessments of the same variable. Statist. Med. 20, 3831–3846. doi: 10.1002/sim.1148
Werner, M., Kapetanovic, S., Nielsen, M., Gurdal, S., Andersson, M. J., Panican, A., et al. (2024). When the relationship is at stake: parents' perception of the relationship with a child with problematic gaming and their perceived need for support. Healthcare 12:851. doi: 10.3390/healthcare12080851
Keywords: parent-child bonds, internet gaming disorder, problematic gaming, Child and Adolescent Psychiatry, treatment
Citation: Kapetanovic S, Due Nielsen M, Gurdal S and Claesdotter-Knutsson E (2024) Transforming family dynamics: unexpected positive effects of treatment for adolescent gaming problems on family relationships. Front. Dev. Psychol. 2:1492685. doi: 10.3389/fdpys.2024.1492685
Received: 07 September 2024; Accepted: 25 November 2024;
Published: 18 December 2024.
Edited by:
Jordan Ashton Booker, University of Missouri, United StatesReviewed by:
Shelia Kennison, Oklahoma State University, United StatesJuliet M. Nyanamba, University of Minnesota Twin Cities, United States
Copyright © 2024 Kapetanovic, Due Nielsen, Gurdal and Claesdotter-Knutsson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabina Kapetanovic, c2FiaW5hLmthcGV0YW5vdmljQGh2LnNl
†ORCID: Sabina Kapetanovic orcid.org/0000-0002-2998-7289
Sevtap Gurdal orcid.org/0000-0001-7881-5670
Emma Claesdotter-Knutsson orcid.org/0000-0002-6832-2482