
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Dent. Med. , 09 March 2023
Sec. Dental Materials
Volume 4 - 2023 | https://doi.org/10.3389/fdmed.2023.1120394
This article is part of the Research Topic Applied Biophysics of the Tooth and Dental Materials View all 5 articles
 Paola Tiozzo-Lyon1,2,†
Paola Tiozzo-Lyon1,2,† Matías Andrade1,†Camila Leiva-Sabadini1,2
Matías Andrade1,†Camila Leiva-Sabadini1,2 José Morales1,2Antonia Olivares1
José Morales1,2Antonia Olivares1 Andrea Ravasio2
Andrea Ravasio2 Sebastian Aguayo1,2*
Sebastian Aguayo1,2*
Currently, a variety of laboratory tools and strategies have been developed to investigate in vivo processes using in vitro models. Amongst these, microfabrication represents a disruptive technology that is currently enabling next-generation biomedical research through the development of complex laboratory approaches (e.g., microfluidics), engineering of micrometer scale sensors and actuators (micropillars for traction force microscopy), and the creation of environments mimicking cell, tissue, and organ-specific contexts. Although microfabrication has been around for some time, its application in dental and oral research is still incipient. Nevertheless, in recent years multiple lines of research have emerged that use microfabrication-based approaches for the study of oral diseases and conditions with micro- and nano-scale sensitivities. Furthermore, many investigations are aiming to develop clinically relevant microfabrication-based applications for diagnostics, screening, and oral biomaterial manufacturing. Therefore, the objective of this review is to summarize the current application of microfabrication techniques in oral sciences, both in research and clinics, and to discuss possible future applications of these technologies for in vitro studies and practical patient care. Initially, this review provides an overview of the most employed microfabrication methods utilized in biomedicine and dentistry. Subsequently, the use of micro- and nano-fabrication approaches in relevant fields of dental research such as endodontic and periodontal regeneration, biomaterials research, dental implantology, oral pathology, and biofilms was discussed. Finally, the current and future uses of microfabrication technology for clinical dentistry and how these approaches may soon be widely available in clinics for the diagnosis, prevention, and treatment of relevant pathologies are presented.
Understanding of physiological functions in health and disease continues to be limited by the complexity of biological systems. In recent years a variety of tools and strategies have been developed to investigate in vivo processes using in vitro models (1). Within this context, microfabrication represents a disruptive technology that, after revolutionizing informatics, telecommunication, and semiconductor industries, is currently enabling next-generation biomedical investigation through the development of complex laboratory approaches (e.g., microfluidics), engineering of micrometer scale sensors and actuators (micropillars for traction force microscopy), and creation of biomimetic (in vivo-like) environments recapitulating cell-, tissue-, and organ-specific contexts (2). The term microfabrication, especially in the field of bioengineering, refers to a set of processes to control the fabrication of substrates and devices where at least one of the feature dimensions is in the micro- or nanometer scale. Generally, two strategies are used to achieve this spatial control (3). Bottom-up approaches leverage from the self-assembly properties of molecules and polymers to build up into structures of controlled geometries (e.g., atomic layer deposition, sol-gel fabrication, vapor deposition, etc.). These technologies are most suited to fabricating nanoscale structures such as surface nanotopographies. On the other hand, top-down approaches make use of various fabrication strategies whereby structures are fabricated by removing parts till the desired geometries are achieved. This typically refers to methods such as photolithography and etching, but it has been used to describe downstream processes such as soft-lithography and high-resolution 3D printing (4). In the biomedical field, microfabricated materials can be used to study e.g., the role of surface topographies on cell adhesion, differentiation, and signaling (5, 6). Furthermore, the use of micro- and nano-fabricated biomaterials is finding its way into clinical practice with great impact on tissue regeneration, nanocarrier fabrication for the delivery of therapeutic agents, extended implant lifespans, bacterial adhesion and growth prevention, and design of novel diagnostic tools for personalized medicine, amongst others (7, 8). In this review, we aimed to deliver an overview of the current understanding of microfabrication approaches in dental studies and clinical practices. In addition, we will provide a perspective guideline for currently unexplored instances where microfabrication could prove to be a game-changer in the field.
Although microfabrication has been around for a number of years, its application in dental and oral sciences is quite recent. Currently, multiple lines of research have emerged in oral sciences that use microfabrication-based approaches for the study of oral diseases and conditions, as well as for use in clinically relevant applications such as diagnostics, screening, and biomaterial manufacturing (Figure 1). Indeed, microfabrication approaches are particularly suited to recapitulate the structures and micro-architectures found in the tooth, consisting of only one non-mineralized (dental pulp) and three mineralized (enamel, dentin, and cementum) tissues (9). Furthermore, teeth are surrounded by periodontal tissues that are rich in extracellular and cellular components that have very particular microarchitectures (e.g., such as the cementum-periodontal ligament-bone interface) (10, 11). On the other hand, dental caries and periodontal disease are two of the most prevalent human pathologies worldwide, both of which result in the irreversible destruction of tissues (12, 13). Therefore, there is a continuous need to develop novel tissue-specific approaches for local regeneration as well as to create new, smart bioactive materials and drug carriers. Hence, it is no surprise that microfabrication is being explored as a potential way to fabricate novel biomaterials and scaffolds that replicate the extracellular matrix of native oral and dental tissues with micro- and nano-scale sensitivity (14).
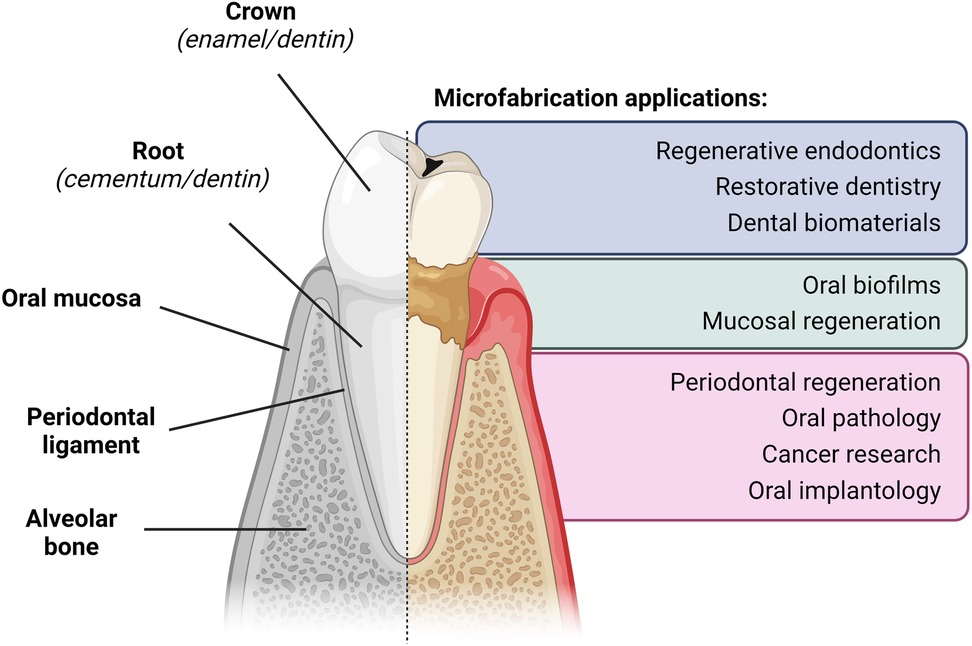
Figure 1. Summary of current research applications of microfabrication in dental research. Spatial architecture of the dental and periodontal tissues, as well as the main current applications of microfabrication-based approaches for the study of oral diseases and conditions.
Despite their increasing use in many biomedical fields, the advent of microfabricated biomaterials and devices in dental research is still quite new, and not much is known about their potential use for cutting-edge research in the oral and craniofacial fields. As a result, we have carried out a search of PubMed, Web of Science, Scopus, and Google Scholar for literature on microfabrication associated with dentistry and dental sciences. Thus, this review summarizes and discusses the most relevant applications of microfabrication in oral sciences for both research and clinics.
In recent years, a number of microfabrication methodologies have been investigated for application in biomedical research (Table 1). One of these approaches is lithography which allows for the development of structured surfaces at the micrometer and nanometer scales (15). Photolithography involves the transfer of a computer-designed pattern to a surface of interest, which is then used as a guide to modify the material by further processes such as photopolymerization or etching (16). One of its advantages is the ability to generate patterns with defined 2D micrometric geometries (17, 18). Electrospinning is another technique used in biomedical sciences where a fiber pattern is generated by ejecting a polymer solution under a high-voltage electric field into a metallic collector (28). Due to their cost-effective fabrication, high surface area, and tailored porosity, electrospun fibers have been used in oral sciences as tissue engineering scaffolds, wound dressings, and drug delivery systems (29). Furthermore, as electrospun scaffolds can be loaded with molecules, growth factors, nanoparticles, and pharmacological agents, their potential as vehicles for drug delivery can open a wide range of novel applications in dentistry in the future (29).
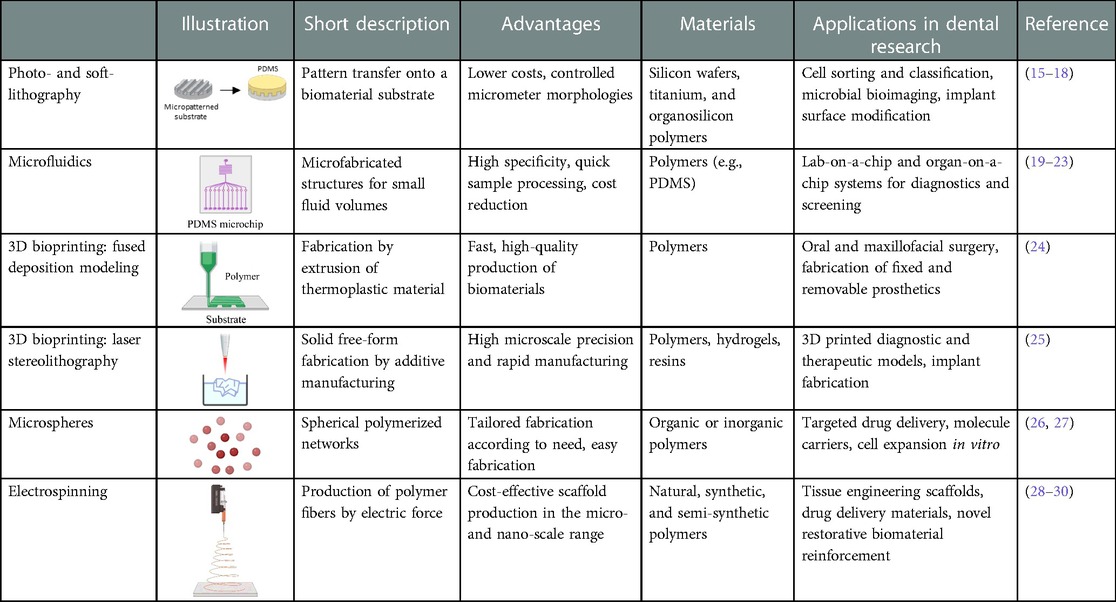
Table 1. Commonly used microfabrication approaches in oral and dental research.
Other microfabrication techniques of interest include three-dimensional (3D) printing via fused deposition modeling or laser stereolithography, methods that allow the creation of biomaterials via additive manufacturing (24, 25). In these approaches, 3D materials are designed in specialized software and divided into a series of 2D layers with an equal thickness (31), which are then printed layer-by-layer until the full material is completed (32). Furthermore, the fabrication of microspheres for the bespoke delivery of drugs and molecules has also been explored with potential uses in bone and tissue regeneration (26, 27).
Microfluidic chip-based models, fabricated via soft lithography and molding, typically consist of polydimethylsiloxane (PDMS) platforms presenting channels and reservoirs that allow fluids to be controlled and manipulated at the microscale (19–21). These chips provide several advantages including precise control of experimental conditions (e.g., flow, the concentration of chemical species, rate of chemical reactions) while allowing inspection of biological samples via microscopy and reducing laboratory costs by decreasing the number of reagents needed for each experiment (17). Perhaps the most promising avenue in microchip-based models is the development of lab-on-a-chip and organ-on-a-chip systems in biomedicine and dentistry. On the one hand, lab-on-a-chip approaches can be used as diagnostic tools for small samples of a bodily fluid such as blood, saliva, or urine, in order to identify proteins, hormones, or pathogens, among others (22). On the other hand, organs-on-a-chip are intended to replicate the environment and physiology of a particular tissue or organ in a complex three-dimensional in vitro model (23). Therefore, these systems are being used to study the physiology of tissues and organs of interest, as well as specific pathologies and potential pharmacological treatment of these conditions. To date, microfabricated chips have been manufactured to replicate the function of organs such as the pulmonary system, cardiovascular system, brain, liver, and kidneys, among others (22).
In addition to the above, there remains an interest in integrating different organs on a chip into one overall system to evaluate the interaction between different organs in the laboratory. This approach, also known as human-on-a-chip or multiorgan-on-a-chip, would have the potential to study not only the therapeutic effect of a drug in a certain target organ but also evaluate its potential toxicity to other relevant organs (33). However, the fabrication of these models is a great challenge due to the difficulty of integrating different systems on a microfabricated chip in an effective and cost-efficient way (34).
When a tooth is subjected to acute damage such as a carious lesion, trauma, or dental fracture, it can cause irreversible inflammation or necrosis of the dental pulp. Given this scenario, one of the most utilized therapeutic options is endodontic treatment; however, several complications may arise including disruption of the mechanical properties of the tooth that significantly increases fracture risk (35). On the other hand, a tooth loses its sensory capacity after endodontic treatment; therefore, any secondary caries lesions on the tooth may not generate symptoms and complicate the detection of these pathologies in a timely manner. Faced with these limitations, pulp regeneration strategies were proposed many years ago as a therapeutic alternative in cases of irreversible pulpitis or pulp necrosis. Nevertheless, there are multiple limitations that hinder its widespread implementation in clinics, such as the limited vascularization of the tooth that hinders pulpal regeneration cell viability post-intervention (36). To overcome these difficulties, a range of microfabrication techniques are being explored as possible alternatives for the study of pulpal regeneration as well as for the development of new clinical approaches (Table 2).
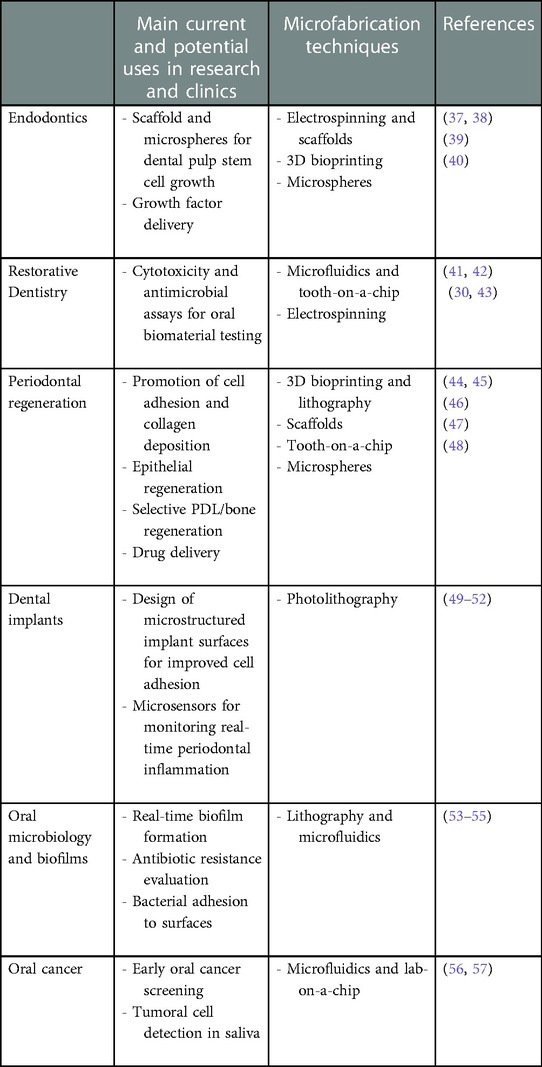
Table 2. Main microfabrication approaches in oral and dental research.
Within the literature, the manufacture of scaffolds made of both natural and synthetic polymers in which dental pulp stem cells can be cultured has been reported (37). The microfabrication techniques used to manufacture these scaffolds include electrospinning, 3D printing, self-assembly, and micro/nanosphere systems (39). Amongst these, Li et al. designed a microsphere-based injectable system that acts as a scaffold for dental stem cell proliferation (40). Here, researchers manufactured a scaffold system made of biodegradable polylactic acid (PLA) microspheres which contained heparin-conjugated gelatin nanospheres containing vascular endothelial growth factor (VEGF). This system acted as both a transport and scaffolding medium for dental pulp stem cells, while at the same time acting as a sustained release system for VEGF over time (40). Furthermore, the fibrillar structure and high porosity of these materials were comparable to the extracellular matrix of collagen. Finally, the authors noted that in this system, the degradation and absorption of microspheres produced a sustained and controlled release of VEGF when injected into the root canal of extracted human teeth and subsequently implanted into an animal model. After 9 weeks, the proliferation and differentiation of dental pulp stem cells toward odontoblasts were observed, accompanied by a large number of blood vessels throughout the pulp (40). Furthermore, Albuquerque et al. have developed an antibiotic-containing PDS fiber scaffold using electrospinning. Metronidazole, minocycline, and ciprofloxacin were incorporated into the scaffold and tested against endodontic pathogens such as Enterococcus faecalis and Actinomyces naeslundii. The scaffold had the ability to sustainably release the antibiotic mixture causing bacterial death without affecting dental pulp stem cell proliferation and migration (38). However, studies regarding the use of microfabrication in dental pulp regeneration are mostly restricted to in vivo or in vitro experiments, so the extrapolation of these results into the clinical setting remains quite limited. In the future, researchers hope to use these and other microfabrication approaches—such as vasculature engineering—to generate scaffolds that promote dental pulp revascularization and regeneration after injury or restorative treatment with predictable outcomes (58).
In dentistry, the interaction between biomaterials and oral tissues is a crucial component for biocompatibility and the long-term success of dental restorations. However, many difficulties remain in order to correctly replicate the in vivo tissue-biomaterial interface in the in vitro setting. To solve this problem, França et al. have been pioneering the implementation of microfluidic-based systems to replicate the physiology of dental pulp and its interaction with different biomaterials (41). For this, they designed a device called “tooth-on-a-chip” by using a combination of PDMS and polymethylmethacrylate (PMMA) by employing 3D printing and microfabrication. By designing two parallel channels separated by a block of human dentin, stem cells from the apical papilla were co-cultured with different dental biomaterials to replicate the pulp-dentin-biomaterial interface and evaluate the pulp response in real time. In an initial publication, they evaluated the cytotoxicity of materials used in restorative dentistry such as hydroxyethyl methacrylate, resin-based adhesive systems, and phosphoric acid by employing their tooth-on-a-chip system (41). Subsequently, in a second study, the authors used the same device to evaluate the effect of different calcium silicate-based cements and their ability to induce cell proliferation in pulp cells (42). Authors observed differences in cell proliferation, viability, morphology, transforming growth factor-β expression, and antimicrobial activity according to the employed biomaterials (42). Overall, these microfluidic systems are highly reproducible in vitro platforms for the high-throughput evaluation of biomaterials for restorative dentistry; however, clinical studies are still needed to validate the in vivo effectiveness of these approaches. Nevertheless, the further development of tooth-on-a-chip devices shows great promise for the real-time evaluation of biomaterials, molecules, and drug therapies against cells and biofilms of clinical interest (Table 2).
Furthermore, microfabrication techniques are gaining traction as a tool for the development of dental materials such as fiber-reinforced composites, which have shown improved mechanical properties compared to regular-filled composites (43). In Tian et al., the incorporation of nylon 6 fibers into a resin matrix was achieved with electrospinning, resulting in spun nylon 6 nanofibers with an average of 250 nm diameter. The fiber was then milled and incorporated into a resin matrix in various mass fractions (1%, 2%, 4%, and 8%) to observe their effect on the mechanical properties of the resulting biomaterial. Results demonstrated an increase in flexural strength, elastic modulus, and work of fracture for the small mass fraction groups (1% and 2%) (30). Similar to the previously discussed literature, this work is also mostly focused on in vitro formulations and testing, and further efforts must be made to validate the use of these microfabricated biomaterials in the clinical setting.
The use of microfabrication has also potentiated cutting-edge research on periodontal regeneration (Table 2). Periodontal tissues such as the alveolar bone, periodontal ligament (PDL), and oral mucosa are highly complex, and as such, there is a need to develop small-scale biomimetic biomaterials to effectively regenerate areas with extended tissue destruction following periodontal disease (59). To do so, some groups have utilized 3D-printed microfabrication to generate surfaces with micropillar cues to promote the deposition of aligned collagen fibers for PDL regeneration (44). After seeding with PDL cells, authors observed cellular alignment and the deposition of orientated collagen amongst the micropillars in an animal model, showing promise as an approach for the guided reconstruction of soft tissues (44). Furthermore, Suzuki et al. fabricated a collagen membrane to be used as scaffolding for both extraoral and intraoral epithelial regeneration by mimicking the shape and distribution of dermal papillae (46). Firstly, the authors employed lithography to generate microfabricated surface topographies in order to mimic the tissue pattern of the epidermis and dermis. Subsequently, a tilapia collagen mixture was poured into the molds and further crosslinked in order to improve the mechanical properties of the membrane (46). Overall, the authors observed epithelial regeneration directly associated with the membrane structure and suggest that this technique may have the potential to function as a membrane that allows cell regeneration in a biomimetic way.
In other work, Lee et al. have focused on creating microstructured materials with region-specific properties to simulate the cementum-PDL-alveolar bone complex for optimized periodontal regeneration (45). For this, authors engineered specific microarchitectures for each region and selectively loaded the scaffold with either amelogenin, connective tissue growth factor, or bone morphogenic protein to promote cementum, PDL, and alveolar bone regeneration, respectively. These micro-channeled substrates were generated via 3D bioprinting and were found to promote distinct cell differentiation, collagen deposition, and mineralization within the construct in both in vitro and in vivo experiments (45). On the other hand, Vurat et al. designed a microfabricated model to replicate the interface between the PDL and alveolar bone, similar to a tooth-on-a-chip system. The authors used 3D bioprinting to fabricate hydrogel blocks containing human periodontal ligament fibroblasts and osteoblasts. Subsequently, both hydrogels were united and the resulting microtissue was included in a PDMS chip containing a circuit that allowed the diffusion of culture media to monitor cell viability and migration over time (47). The authors used tetracycline as a model drug for the antibiotic treatment of periodontal disease and were able to measure its uptake by the scaffold-encapsulated cells. Overall, the use of these models to study the response of periodontal and alveolar bone cells to drug loading or bioactive molecules is of great interest for future studies on the treatment of periodontal diseases. However, more clinical research is still needed in order to translate these systems into clinics and patient care.
Furthermore, oral bone regeneration is also an area that has gained much interest due to the increased use of dental implants for tooth replacement. Currently, the treatment for bone defects is mainly based on the use of bone grafts that provide an osteoconductive media for regeneration. Therefore, the complementation of bone regeneration with microfabricated osteoinductors such as growth factors is currently being explored. In this context, Ma et al. developed an injectable system of poly (lactic acid) (PLA) microspheres carrying gelatin nanospheres bound to bone morphogenetic protein (BMP-2). This system allowed both improved cell adhesion and a sustained release of BMP-2 from the microspheres over time (48). There is also a growing interest in the use of scaffold-free approaches for regenerative periodontics and endodontics, including the use of extracellular vesicles, spheroids, and tissue strands that aim to promote the development of a biomimetic extracellular matrix for regeneration (60). The microfabrication of tissue-specific stem cell niches that promote local tissue regeneration is also of great interest (8). Nevertheless, most of these investigations remain strictly in vitro and challenges remain in order to translate these microfabricated technologies and biomaterials into standardized and reproducible clinical approaches, particularly as the microarchitecture of the periodontal region is highly complex compared to other tissues.
A crucial element for the success of titanium dental implant treatments in dentistry is the correct integration of the implant into the periodontium (including the alveolar bone) and the surrounding soft tissues. To achieve this, it is known that the surface topography and roughness of the implant are important factors to achieve intimate contact between the alveolar bone and the titanium surface (61). Therefore, it is no surprise that the use of microfabrication techniques has been implemented to attain biologically active titanium surfaces (Table 2) (62).
For example, Doll et al. have published different strategies to design and fabricate surface patterns on titanium frameworks (49). They initially proposed a subtractive method by acid etching using photolithography. However, as the substrates in which lithography techniques are used are usually flat, a flexible photomask was manufactured to apply this technique onto a dental implant surface by using a mechanism allowing rotation of the implants while they are exposed to ultraviolet light (49). By employing this method, they obtained microscale features up to 1.5 µm sizes with the hope of improving fibroblast and epithelial cell adhesion to dental implants, in order to increase soft tissue interactions with dental implant biomaterials in the future.
On the other hand, the same group of researchers published a proposal for an additive method using a photolithography method. However, instead of using chemical etching, they proposed the use of anodic oxidation in which an oxide layer is formed on the titanium surface (50). Furthermore, in a recent investigation, Moreira et al. developed micropatterned silica coatings consisting of either lines or micropillars to increase osteointegration in zirconia dental implants (51). The resulting surfaces displayed increased hydrophilicity compared to controls and therefore showed great promise to promote cellular attachment and long-term osseointegration.
Microfabrication has also been used to generate real-time sensors for monitoring inflammation surrounding dental implants. In this context, Kim et al. developed a temperature-based polymer microsensor to monitor implant survival and predict potential failures (52). By using photolithography, authors fabricated polymer microfilms that were wrapped around dental implant abutments and were able to sense temperature changes in the surrounding environment. The microsensor sensitivity paired with its adequate mechanical and chemical resistance suggests its potential use in clinics to develop personalized diagnoses and long-term follow-up for dental implant treatments.
The formation of multispecies biofilms in the oral cavity is an important problem in dentistry as they play a key role in the development of diseases such as dental caries, periodontitis, and peri-implantitis (63–65). More specifically, the dysregulation of the oral microbiota (dysbiosis) due to the over-proliferation of certain pathological strains is associated with site-specific ecological changes (66). Until now, the incubation of microorganisms in closed systems under static conditions where nutrients are depleted, and waste products accumulate has been the most utilized approach. Nowadays, however, thanks to microfabrication it is possible to assess biofilm formation on surfaces using microfluidic devices that simulate different hydrodynamic flow conditions (67). Furthermore, microfabricated systems can be used to study the effect of antibiotics and antimicrobial molecules on bacteria, as well as the resulting changes that occur at the bacterial and biofilm levels (Table 2) (68).
Within this context, there are several approaches to characterize bacterial adhesion and biofilm formation using microfabrication-derived approaches. For example, Straub et al. monitored bacterial adhesion in real-time using a microfluidic system coupled with optical microscopy, observing how medium composition can impact biofilm formation (53), and Tang et al. utilized a microfluidic chip to explore the biofilm dynamics of antibiotic-resistant Escherichia coli (54). More specifically in dentistry, Alvarez-Escobar et al. have recently employed lithography techniques to study intraoral bacterial adhesion to substrates (55). Authors designed PDMS plates with different surface patterns that were subsequently incorporated into intraoral retainers for 24-hour in vivo bacterial adhesion and biofilm formation. Although no significant differences in biofilm formation were observed among substrates, this pilot study proposes a method to study bacterial adhesion directly onto different dental biomaterials or dental tissue specimens (55).
Finally, microfabrication and microfluidic techniques are also being developed as novel low-cost screening strategies for oral cancers, particularly with the objective of early detection and treatment (Table 2). Proof of concept and early designs for lab-on-a-chip-based microfluidic systems looked to automatize the detection of certain saliva-based markers for oral squamous cell carcinoma (56). However, more recently, Zoupanou et al. designed a microfabricated chip with the ability to immobilize circulating tumor cells (57). To do this, a PMMA microfabricated chip containing a microfluidics circuit was constructed using laser ablation techniques and further treated to bind epithelial cellular adhesion molecule (EpCAM), an important membrane biomarker expressed by tumor cells of epithelial origin. By using this system, researchers were able to effectively immobilize circulating tumor cells with the aid of anti-EpCAM antibodies and demonstrated the potential of this system as a plug-and-play device for rapid and easy oral cancer screening (57).
Until recently, microfabrication approaches in dentistry have been mostly utilized in the in vitro setting for the study of relevant oral diseases and conditions. However, there is a growing interest in the use of microfabrication-based techniques and methods for clinical applications in a variety of dental disciplines (Figure 2). Among these techniques, 3D bioprinting has gained a lot of traction within clinical dentistry (69, 70) and is currently being explored in the fields of prosthodontics, maxillofacial surgery, orthodontics, endodontics, and periodontics (71, 72). Furthermore, the fabrication of 3D printed materials with microscale topographies seeks to promote the biological interaction of biomaterials with human tissues to improve the long-term prognosis of dental treatments in clinics (73).
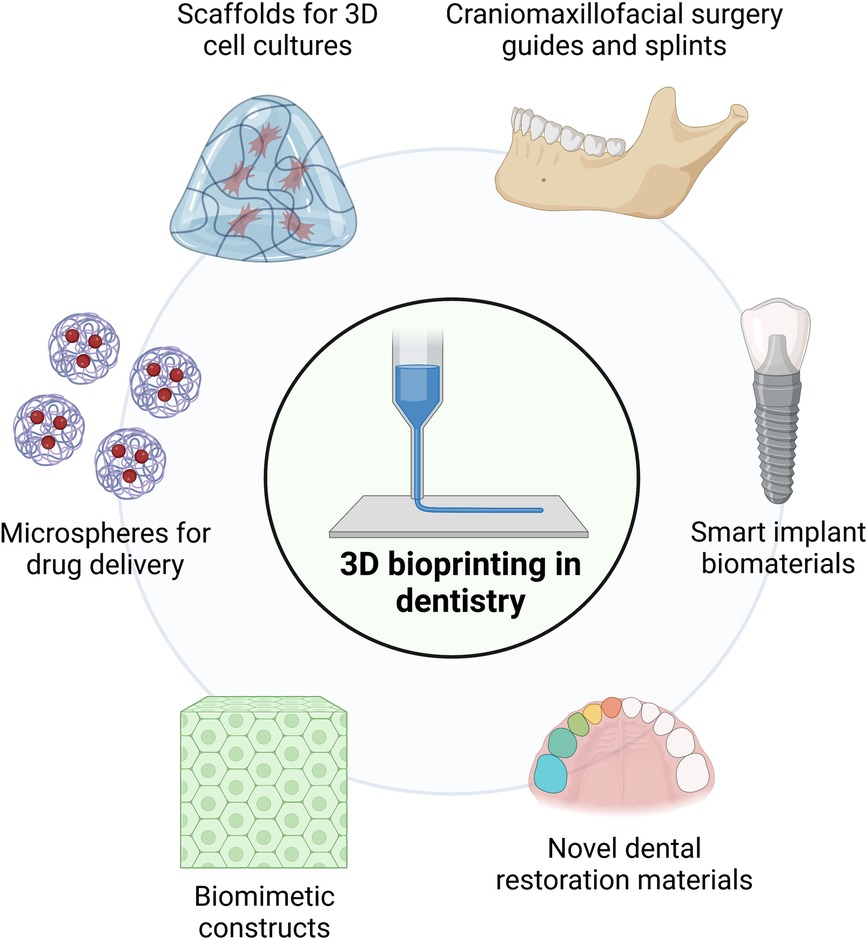
Figure 2. Current and potential clinical uses of microfabrication and 3D bioprinting in dentistry.
Currently, the process of combining cells with 3D-printed polymers to create 3D cell cultures for tissue engineering, drug screening, or in vitro disease models is increasing its popularity (74). Microfabrication approaches based on spheroid/microtissue systems have given rise to potential applications for the clinical regeneration of damaged tissues as well as the construction of in-vitro tissue models to understand cell behavior (75). Many methodologies utilize scaffolds manufactured from natural or synthetic polymers such as collagen (76), or PLA and poly (glycolic acid) (PGA), respectively (77). The scaffolds then act as templates that allow cells to adhere, proliferate, and expand throughout the 3D matrix and eventually generate mature cell-laden grafts with features comparable to native tissue. Studies have shown that the phenotype of scaffold-seeded cells can be regulated by a combination of different biological and physical stimuli (74, 78, 79). Additionally, 3D bioprinting technology offers the unprecedented ability of engineering biomaterials that mimic the shape, structure, and function of native tissues and organs (80). The resulting 3D-printed biomaterials are expected to serve as biomimetic constructs that ensure increased cell viability and support of tissue and organ functionality (81, 82). Recently, a couple of case reports have pioneered the use of 3D bioprinting for the treatment of periodontal defects (83) and alveolar cleft reconstruction (84); nevertheless, larger clinical trials are necessary in order to determine the long-term success of these approaches for reliable tissue regeneration.
3D printing has several advantages compared to traditional approaches, mainly due to the rapid and high-precision production and customization of biomaterials with microscale sensitivity (85). In addition, 3D printing provides personalized service at a lower cost for patients and thus simplifies the complex workflow related to the production of some dental appliances (69). From a clinical perspective, the use of 3D-printed restorations has shown notable advantages, such as reduced internal and marginal gaps compared to milled restorations (70) and rapid manufacturing of complex geometries (86). From the biomaterial perspective, a variety of materials can be used to create complex geometric shapes and precisely meet dental needs, especially when combined with 3D scanning of the patient's tissues. For example, advances in intraoral and extraoral 3D scanning technologies, cone beam computed tomography (CBCT), and other CAD/CAM technologies have fueled the use of 3D printing in the field of oral and maxillofacial surgery (87–89). On the other hand, temporary crowns obtained by 3D printing have shown greater mechanical resistance since their construction eliminates operator-induced errors (90). Furthermore, dental crowns and bridges can be manufactured using 3D printing technology (91), and in some cases, a variety of materials can be printed simultaneously with favorable detail reproducibility (92). In the case of removable prostheses, resin bases can be generated without the need for impressions or cast models (86). However, these technologies are not yet widely available in clinics and there remains a lack of long-term clinical studies assessing the durability and biological effect of 3D-printed dental biomaterials.
It is known that proper tissue adaptation is critical for removable denture stability and retention (93) and in this context, Tasaka et al. found that 3D printed dentures had a higher precision than those produced by conventional thermal polymerization (94). Overall, resin-based 3D printing involves the use of photosensitive materials that are cured and molded under light irradiation (95). More specifically, these resins are deposited on a model-building platform and cured with an ultraviolet (UV) laser to generate a morphology of interest according to a computer-generated design (96). Therefore, these approaches can generate a wide variety of material densities, hardness, flexibilities, and porosities. Furthermore, surface printing resolutions in the tens-of-microns range together with the fabrication of complex geometries are important advantages of these approaches compared to conventional prosthesis manufacturing (97, 98).
Additionally, there is much research centered on using 3D bioprinting to fabricate dental implant biomaterials with micrometer features to promote tissue integration. Recent work by Yin et al. employed 3D-printed implants with micropore channel architecture to improve alveolar bone height preservation and promote cell differentiation and actin remodeling (99). Further investigations have functionalized polymer biomaterials with chlorhexidine-containing silica nanoparticles embedded in PDMS to confer antibacterial properties (100). Also, 3D bioprinting is currently being explored to generate microporous carbon fiber and hydroxyapatite constructs to enhance the toughness and strength of scaffolds for bone regeneration (101). However, most of these materials remain still in the developmental phase, with investigations limited to in vitro mechanical characterization and pre-clinical testing. However, it is expected that soon there will be a strong increase in available biomaterials and equipment to use 3D bioprinting in the clinics, particularly associated with microscale and nanoscale topographies and geometries to promote biological activity and long-term integration to the host tissues.
As discussed throughout this review, the use of microfabrication approaches is slowly gaining traction within dental research and clinics. Although these approaches continue to be mostly experimental at the moment, their use in clinical diagnostics and treatment is expected to increase in the future with waning costs and increasing ease of use of microfabrication methods. For example, the microfabrication of functionalized biomaterials for dental applications is an interesting avenue for the development of new, smart biomaterials with high clinical predictability. Particularly for the oral cavity, it is of interest to explore microstructures that could promote host cell adhesion and differentiation while simultaneously deterring bacterial adhesion and biofilm formation (102, 103). This would be highly relevant for the regeneration of periodontal defects in anatomical regions where biofilms play a crucial role in health and disease. The use of electrospinning for the construction of bioactive microfabricated scaffolds for restorative dentistry is also being investigated, particularly to develop antibacterial and functional biomaterial for restorative dentistry (104–106). Additionally, the use of microfluidics and organ-on-a-chip systems could serve as a cost-effective and direct point-of-care testing option for the diagnosis of a range of oral diseases, particularly for use in remote communities and areas with limited availability of high-cost diagnostic facilities (Figure 3).
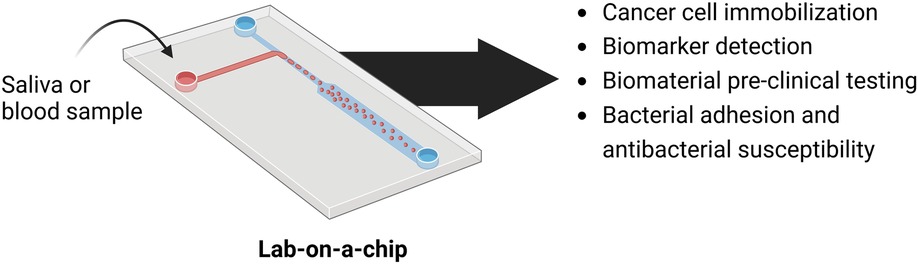
Figure 3. Summary of lab-on-a-chip approaches currently being explored for pre-clinical and clinical applications in dentistry. Microfluidics-based lab-on-a-chip systems are expected to serve as low-cost diagnostic platforms for saliva and blood screening against cells and biomarkers of interest. Furthermore, these microchips have shown great potential for the easy and cost-effective pre-clinical evaluation of the cytotoxic and antibacterial properties of novel dental biomaterials.
Furthermore, recent progress in the development of smart materials has potentiated the development of highly innovative approaches such as 4D bioprinting (Figure 4) (107). Unlike 3D printing, 4D printing fabricates pre-programmable biological constructs capable of actively altering their shape in response to surrounding environmental changes (108). The potential use of these smart materials for the restoration of periodontal osseous defects and caries-affected teeth could aid the rehabilitation of oral diseases in a personalized medicine approach. Moreover, the combination of advanced imaging techniques with 3D and 4D printed biomaterials could provide fast and customized surgical reconstruction for patients with craniofacial trauma, improving emergency care and long-term repair and regeneration in these individuals.

Figure 4. 4D bioprinting as a tool for the development of cutting-edge smart dental biomaterials.
In summary, microfabrication is currently being used to explore many crucial physiological and pathological processes across an important number of dental disciplines, and utilized in a wide range of in vitro setups to study the interaction of biomaterials with host cells and microbiome components. To date, most of these approaches are not yet available in clinics but are expected to quickly gain traction due to their rapid development and promising in vitro and pre-clinical results. Currently, some clinical uses of 3D bioprinting are available, although the range of applications is expected to increase rapidly in the coming years to include smart-biomaterial printing, point-of-care diagnostics, and novel restorative materials for soft and hard tissue regeneration.
Literature search and summary were carried out by PTL, MA, CLS, JM, AO, and SA. Table illustrations were created by CLS and SA. The initial drafting of the manuscript was done by PTL, MA, CLS, AR, and SA. Finally, PTL, MA, CLS, JM, AO, AR, and SA critically reviewed the manuscript. All authors contributed to the article and approved the submitted version.
This work has been supported by ANID FONDECYT #1220804 and #1210872, ANID/SCIA/ACT192015, and ANID FONDEQUIP EMQ210101.
Illustrations for the table and figures were created with Biorender.com.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hughes JH, Kumar S. Synthetic mechanobiology: engineering cellular force generation and signaling. Curr Opin Biotechnol. (2016) 40:82–9. doi: 10.1016/j.copbio.2016.03.004
2. Grenci G, Bertocchi C, Ravasio A. Integrating microfabrication into biological investigations: the benefits of interdisciplinarity. Micromachines (Basel). (2019) 10:252. doi: 10.3390/mi10040252
3. Biswas A, Bayer IS, Biris AS, Wang T, Dervishi E, Faupel F. Advances in top–down and bottom–up surface nanofabrication: techniques, applications & future prospects. Adv Colloid Interface Sci. (2012) 170:2–27. doi: 10.1016/j.cis.2011.11.001
4. Verhulsel M, Vignes M, Descroix S, Malaquin L, Vignjevic DM, Viovy J-L. A review of microfabrication and hydrogel engineering for micro-organs on chips. Biomaterials. (2014) 35:1816–32. doi: 10.1016/j.biomaterials.2013.11.021
5. Lim JY, Donahue HJ. Cell sensing and response to micro- and nanostructured surfaces produced by chemical and topographic patterning. Tissue Eng. (2007) 13:1879–91. doi: 10.1089/ten.2006.0154
6. Ruprecht V, Monzo P, Ravasio A, Yue Z, Makhija E, Strale PO, et al. How cells respond to environmental cues—insights from bio-functionalized substrates. J Cell Sci. (2017) 130:51–61. doi: 10.1242/jcs.196162
7. Nadine S, Chung A, Diltemiz SE, Yasuda B, Lee C, Hosseini V, et al. Advances in microfabrication technologies in tissue engineering and regenerative medicine. Artif Organs. (2022) 46:E211–43. doi: 10.1111/aor.14232
8. Ramos-Rodriguez DH, MacNeil S, Claeyssens F, Asencio IO. The use of microfabrication techniques for the design and manufacture of artificial stem cell microenvironments for tissue regeneration. Bioengineering. (2021) 8:50. doi: 10.3390/bioengineering8050050
9. Pitts NB, Zero DT, Marsh PD, Ekstrand K, Weintraub JA, Ramos-Gomez F, et al. Dental caries. Nat Rev Dis Primers. (2017) 3:17030. doi: 10.1038/nrdp.2017.30
10. Park CH. Biomaterial-based approaches for regeneration of periodontal ligament and cementum using 3D platforms. Int J Mol Sci. (2019) 20:4364. doi: 10.3390/ijms20184364
11. Yu M, Luo D, Qiao J, Guo J, He D, Jin S, et al. A hierarchical bilayer architecture for complex tissue regeneration. Bioact Mater. (2022) 10:93–106. doi: 10.1016/j.bioactmat.2021.08.024
12. James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
13. Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and tooth loss in adults in the United States, 2011–2012. NCHS Data Brief. (2015)(197):197. doi: 10.1080/713604647
14. Ahadian S, Ostrovidov S, Fujie T, Parthiban SP, Kaji H, Sampathkumar K, et al. In: Vishwakarma A, Sharpe P, Shi S, Ramalingam, editors. Microfabrication and nanofabrication techniques. Stem Cell Biology and Tissue Engineering in Dental Sciences. Academic Press (2015). pp. 207–219. doi: 10.1016/B978-0-12-397157-9.00017-5
15. Duffy DC, McDonald JC, Schueller OJA, Whitesides GM. Rapid prototyping of microfluidic systems in poly(dimethylsiloxane). Anal Chem. (1998) 70:4974–84. doi: 10.1021/ac980656z
16. Vora KD, Peele AG, Shew B-Y, Harvey EC, Hayes JP. Fabrication of support structures to prevent SU-8 stiction in high aspect ratio structures. Microsyst Technol. (2007) 13:487–93. doi: 10.1007/s00542-006-0201-4
17. Yager P, Edwards T, Fu E, Helton K, Nelson K, Tam MR, et al. Microfluidic diagnostic technologies for global public health. Nature. (2006) 442:412–8. doi: 10.1038/nature05064
18. Fan R, Vermesh O, Srivastava A, Yen BKH, Qin L, Ahmad H, et al. Integrated barcode chips for rapid, multiplexed analysis of proteins in microliter quantities of blood. Nat Biotechnol. (2008) 26:1373–8. doi: 10.1038/nbt.1507
19. Sosa-Hernández JE, Villalba-Rodríguez AM, Romero-Castillo KD, Aguilar-Aguila-Isaías MA, García-Reyes IE, Hernández-Antonio A, et al. Organs-on-a-chip module: a review from the development and applications perspective. Micromachines (Basel). (2018) 9:536. doi: 10.3390/mi9100536
20. Wang X, Sun Q, Pei J. Microfluidic-based 3D engineered microvascular networks and their applications in vascularized microtumor models. Micromachines (Basel). (2018) 9:1–26. doi: 10.3390/mi9100493
21. Jeon JS, Bersini S, Whisler JA, Chen MB, Dubini G, Charest JL, et al. Generation of 3D functional microvascular networks with human mesenchymal stem cells in microfluidic systems. Integr Biol (United Kingdom). (2014) 6:555–63. doi: 10.1039/c3ib40267c
22. Azizipour N, Avazpour R, Rosenzweig DH, Sawan M, Ajji A. Evolution of biochip technology: a review from lab-on-a-chip to organ-on-a-chip. Micromachines (Basel). (2020) 11:599. doi: 10.3390/mi11060599
23. Leung CM, de Haan P, Ronaldson-Bouchard K, Kim G-A, Ko J, Rho HS, et al. A guide to the organ-on-a-chip. Nat Rev Methods Primers. (2022) 2:33. doi: 10.1038/s43586-022-00118-6
24. Wasti S, Adhikari S. Use of biomaterials for 3D printing by fused deposition modeling technique: a review. Front Chem. (2020) 8:315. doi: 10.3389/fchem.2020.00315
25. Hagiwara T. Recent progress of photo-resin for rapid prototyping, “resin for stereolithography.” Macromol Symp. (2001) 175:397–402. doi: 10.1002/1521-3900(200110)175:1397::AID-MASY397%3E3.0.CO;2-Y
26. Wright B, Parmar N, Bozec L, Aguayo SD, Day RM. A simple and robust method for pre-wetting poly (lactic-co-glycolic) acid microspheres. J Biomater Appl. (2015) 30(2):147–59. doi: 10.1177/0885328215577297
27. Katsarov P, Shindova M, Lukova P, Belcheva A, Delattre C, Pilicheva B. Polysaccharide-based micro- and nanosized drug delivery systems for potential application in the pediatric dentistry. Polymers (Basel). (2021) 13:3342. doi: 10.3390/polym13193342
28. Jin S, Yeung AWK, Zhang C, Tsoi JK-H. A bibliometric analysis of electrospun nanofibers for dentistry. J Funct Biomater. (2022) 13(3):90. doi: 10.3390/jfb13030090
29. Zafar M, Najeeb S, Khurshid Z, Vazirzadeh M, Zohaib S, Najeeb B, et al. Potential of electrospun nanofibers for biomedical and dental applications. Materials (Basel). (2016) 9(2):73. doi: 10.3390/ma9020073
30. Tian M, Gao Y, Liu Y, Liao Y, Xu R, Hedin NE, et al. Bis-GMA/TEGDMA dental composites reinforced with electrospun nylon 6 nanocomposite nanofibers containing highly aligned fibrillar silicate single crystals. Polymer. (2007) 48(9):2720–8. doi: 10.1016/j.polymer.2007.03.032
31. Lu Y, Chen SC. Micro and nano-fabrication of biodegradable polymers for drug delivery. Adv Drug Deliv Rev. (2004) 56:1621–33. doi: 10.1016/j.addr.2004.05.002
32. Matsuda T, Mizutani M, Arnold SC. Molecular design of photocurable liquid biodegradable copolymers. 1. Synthesis and photocuring characteristics. Macromolecules. (2000) 33:795–800. doi: 10.1021/ma991404i
33. Picollet-D’hahan N, Zuchowska A, Lemeunier I, le Gac S. Multiorgan-on-a-chip: a systemic approach to model and decipher inter-organ communication. Trends Biotechnol. (2021) 39:788–810. doi: 10.1016/j.tibtech.2020.11.014
34. Zheng F, Fu F, Cheng Y, Wang C, Zhao Y, Gu Z. Organ-on-a-chip systems: microengineering to biomimic living systems. Small. (2016) 12:2253–82. doi: 10.1002/smll.201503208
35. Moosavi H, Afshari S, Manari F. Fracture resistance of endodontically treated teeth with different direct corono-radicular restoration methods. J Clin Exp Dent. (2017) 9:454–9. doi: 10.4317/jced.53160
36. Jung C, Kim S, Sun T, Cho Y-B, Song M. Pulp-dentin regeneration: current approaches and challenges. J Tissue Eng. (2019) 10:2041731418819263. doi: 10.1177/2041731418819263
37. Kaushik SN, Kim B, Walma AMC, Choi SC, Wu H, Mao JJ, et al. Biomimetic microenvironments for regenerative endodontics. Biomater Res. (2016) 20:14. doi: 10.1186/s40824-016-0061-7
38. Albuquerque MTP, Valera MC, Nakashima M, Nör JE, Bottino MC. Tissue-engineering-based strategies for regenerative endodontics. J Dent Res. (2014) 93(12):1222–31. doi: 10.1177/0022034514549809
39. Jazayeri HE, Lee S, Kuhn L, Fahimipour F, Tahriri M, Tayebi L. Polymeric scaffolds for dental pulp tissue engineering: a review. Dent Mater. (2019) 36:e47–58. doi: 10.1016/j.dental.2019.11.005
40. Li X, Ma C, Xie X, Sun H, Liu X. Pulp regeneration in a full-length human tooth root using a hierarchical nanofibrous microsphere system. Acta Biomater. (2016) 35:57–67. doi: 10.1016/j.actbio.2016.02.040
41. França CM, Tahayeri A, Rodrigues NS, Ferdosian S, Puppin Rontani RM, Sereda G, et al. The tooth on-a-chip: a microphysiologic model system mimicking the biologic interface of the tooth with biomaterials. Lab Chip. (2020) 20:405–13. doi: 10.1039/C9LC00915A
42. Rodrigues NS, França CM, Tahayeri A, Ren Z, Saboia VPA, Smith AJ, et al. Biomaterial and biofilm interactions with the pulp-dentin complex-on-a-chip. J Dent Res. (2021) 100:1136–43. doi: 10.1177/00220345211016429
43. Garoushi S, Gargoum A, Vallittu PK, Lassila L. Short fiber-reinforced composite restorations: a review of the current literature. J Investig Clin Dent. (2018) 9(3):e12330. doi: 10.1111/jicd.12330
44. Pilipchuk SP, Monje A, Jiao Y, Hao J, Kruger L, Flanagan CL, et al. Integration of 3D printed and micropatterned polycaprolactone scaffolds for guidance of oriented collagenous tissue formation in vivo. Adv Healthc Mater. (2016) 5:676–87. doi: 10.1002/adhm.201500758
45. Lee CH, Hajibandeh J, Suzuki T, Fan A, Shang P, Mao JJ. Three-Dimensional printed multiphase scaffolds for regeneration of periodontium Complex. Tissue Eng Part A. (2013) 20:1342–51. doi: 10.1089/ten.tea.2013.0386
46. Suzuki A, Kodama Y, Miwa K, Kishimoto K, Hoshikawa E. Manufacturing micropatterned collagen scaffolds with chemical—crosslinking for development of biomimetic tissue—engineered oral mucosa. Sci Rep. (2020) 10(1):22192. doi: 10.1038/s41598-020-79114-3
47. Vurat MT, Şeker Ş, Lalegül-Ülker Ö, Parmaksiz M, Elçin AE, Elçin YM. Development of a multicellular 3D-bioprinted microtissue model of human periodontal ligament-alveolar bone biointerface: towards a pre-clinical model of periodontal diseases and personalized periodontal tissue engineering. Genes Dis. (2022) 9:1008–23. doi: 10.1016/j.gendis.2020.11.011
48. Ma C, Jing Y, Sun H, Liu X. Hierarchical nanofibrous microspheres with controlled growth factor delivery for bone regeneration. Adv Healthc Mater. (2015) 4:2699–708. doi: 10.1002/adhm.201500531
49. Doll PW, Doll C, Käßer L, Häfner M, Spindler B, Ahrens R, et al. Rotational UV-lithography using flexible chromium-coated polymer masks for the fabrication of microstructured dental implant surfaces: a proof of concept. J Micromech Microeng. (2020) 30:045008. doi: 10.1088/1361-6439/ab70c0
50. Doll PW, Ahrens R, Guber AE. Etch-less microfabrication of structured TiO2 implant coatings on bulk titanium grade 23 by direct lithographic anodic oxidation. J Micromech Microeng. (2021) 31:035007. doi: 10.1088/1361-6439/abdae6
51. Moreira A, Madeira S, Buciumeanu M, Fialho J, Carvalho A, Silva F, et al. Design and surface characterization of micropatterned silica coatings for zirconia dental implants. J Mech Behav Biomed Mater. (2022) 126:105060. doi: 10.1016/j.jmbbm.2021.105060
52. Kim JJ, Stafford GR, Beauchamp C, Kim SA. Development of a dental implantable temperature sensor for real-time diagnosis of infectious disease. Sensors. (2020) 20:3953. doi: 10.3390/s20143953
53. Straub H, Eberl L, Zinn M, Rossi RM, Maniura-Weber K, Ren Q. A microfluidic platform for in situ investigation of biofilm formation and its treatment under controlled conditions. J Nanobiotechnol. (2020) 18:166. doi: 10.1186/s12951-020-00724-0
54. Tang P-C, Eriksson O, Sjögren J, Fatsis-Kavalopoulos N, Kreuger J, Andersson DI. A microfluidic chip for studies of the dynamics of antibiotic resistance selection in bacterial biofilms. Front Cell Infect Microbiol. (2022) 12:896149. doi: 10.3389/fcimb.2022.896149
55. Alvarez-Escobar M, Freitas SC, Hansford D, Monteiro FJ, Pelaez-Vargas A. Soft lithography and minimally human invasive technique for rapid screening of oral biofilm formation on new microfabricated dental material surfaces. Int J Dent. (2018) 2018:4219625. doi: 10.1155/2018/4219625
56. Ziober BL, Mauk MG, Falls EM, Chen Z, Ziober AF, Bau HH. Lab-on-a-chip for oral cancer screening and diagnosis. Head Neck. (2008) 30:111–21. doi: 10.1002/hed.20680
57. Zoupanou S, Volpe A, Primiceri E, Gaudiuso C, Ancona A, Ferrara F, et al. SMILE platform: an innovative microfluidic approach for on-chip sample manipulation and analysis in oral cancer diagnosis. Micromachines (Basel). (2021) 12:885. doi: 10.3390/mi12080885
58. Dissanayaka WL, Zhang C. The role of vasculature engineering in dental pulp regeneration. J Endod. (2017) 43:S102–6. doi: 10.1016/j.joen.2017.09.003
59. Green DW, Lee J-S, Jung H-S. Small-scale fabrication of biomimetic structures for periodontal regeneration. Front Physiol. (2016) 7:6. doi: 10.3389/fphys.2016.00006
60. Banerjee K, Radhakrishnan J, Ayyadurai N, Ganesan P, Kamini NR. Advances in neoteric modular tissue engineering strategies for regenerative dentistry. J Sci: Adv Mater Devices. (2022) 7:100491. doi: 10.1016/j.jsamd.2022.100491
61. Walter N, Stich T, Docheva D, Alt V, Rupp M. Evolution of implants and advancements for osseointegration: a narrative review. Injury. (2022) 53(Suppl 3):S69–S73. doi: 10.1016/j.injury.2022.05.057
62. Ainslie KM, Desai TA. Microfabricated implants for applications in therapeutic delivery, tissue engineering, and biosensing. Lab Chip. (2008) 8:1864–78. doi: 10.1039/B806446F
63. Álvarez S, Leiva-Sabadini C, Schuh CMAP, Aguayo S. Bacterial adhesion to collagens: implications for biofilm formation and disease progression in the oral cavity. Crit Rev Microbiol. (2021) 48(1):83–95. doi: 10.1080/1040841X.2021.1944054
64. Schuh CMAP, Benso B, Naulin PA, Barrera NP, Bozec L, Aguayo S. Modulatory effect of glycated collagen on oral streptococcal nanoadhesion. J Dent Res. (2020) 100:82–9. doi: 10.1177/0022034520946320
65. Xiao J, Hara AT, Kim D, Zero DT, Koo H, Hwang G. Biofilm three-dimensional architecture influences in situ pH distribution pattern on the human enamel surface. Int J Oral Sci. (2017) 9:74–9. doi: 10.1038/ijos.2017.8
66. Hajishengallis G, Darveau RP, Curtis MA. The keystone-pathogen hypothesis. Nat Rev Microbiol. (2012) 10:717–25. doi: 10.1038/nrmicro2873
67. Kim J, Park H-D, Chung S. Microfluidic approaches to bacterial biofilm formation. Molecules. (2012) 17:9818–34. doi: 10.3390/molecules17089818
68. Guliy OI, Evstigneeva SS, Bunin VD. Microfluidic bioanalytical system for biofilm formation indication. Talanta. (2022) 247:123541. doi: 10.1016/j.talanta.2022.123541
69. Lin L, Fang Y, Liao Y, Chen G, Gao C, Zhu P. 3D printing and digital processing techniques in dentistry: a review of literature. Adv Eng Mater. (2019) 21:1801013. doi: 10.1002/adem.201801013
70. Alharbi N, Alharbi S, Cuijpers VMJI, Osman RB, Wismeijer D. Three-dimensional evaluation of marginal and internal fit of 3D-printed interim restorations fabricated on different finish line designs. J Prosthodont Res. (2018) 62:218–26. doi: 10.1016/j.jpor.2017.09.002
71. Prechtel A, Reymus M, Edelhoff D, Hickel R, Stawarczyk B. Comparison of various 3D printed and milled PAEK materials: effect of printing direction and artificial aging on martens parameters. Dent Mater. (2019) 36:197–209. doi: 10.1016/j.dental.2019.11.017
72. Oberoi G, Nitsch S, Edelmayer M, Janjić K, Müller AS, Agis H. 3D Printing—encompassing the facets of dentistry. Front Bioeng Biotechnol. (2018) 6:172. doi: 10.3389/fbioe.2018.00172
73. Tao O, Kort-Mascort J, Lin Y, Pham HM, Charbonneau AM, ElKashty OA, et al. The applications of 3D printing for craniofacial tissue engineering. Micromachines (Basel). (2019) 10:480. doi: 10.3390/mi10070480
74. Zhang YS, Xia Y. Multiple facets for extracellular matrix mimicking in regenerative medicine. Nanomedicine. (2015) 10:689–92. doi: 10.2217/nnm.15.10
75. Ji S, Guvendiren M. Recent advances in bioink design for 3D bioprinting of tissues and organs. Front Bioeng Biotechnol. (2017) 5:23. doi: 10.3389/fbioe.2017.00023
76. Glowacki J, Mizuno S. Collagen scaffolds for tissue engineering. Biopolymers. (2008) 89:338–44. doi: 10.1002/bip.20871
77. Shin H, Jo S, Mikos AG. Biomimetic materials for tissue engineering. Biomaterials. (2003) 24:4353–64. doi: 10.1016/S0142-9612(03)00339-9
78. Place ES, Evans ND, Stevens MM. Complexity in biomaterials for tissue engineering. Nat Mater. (2009) 8:457–70. doi: 10.1038/nmat2441
79. Tayalia P, Mooney DJ. Controlled growth factor delivery for tissue engineering. Adv Mater. (2009) 21:3269–85. doi: 10.1002/adma.200900241
80. Malda J, Visser J, Melchels FP, Jüngst T, Hennink WE, Dhert WJA, et al. 25th Anniversary article: engineering hydrogels for biofabrication. Adv Mater. (2013) 25:5011–28. doi: 10.1002/adma.201302042
81. Skardal A, Mack D, Kapetanovic E, Atala A, Jackson JD, Yoo J, et al. Bioprinted amniotic fluid-derived stem cells accelerate healing of large skin wounds. Stem Cells Transl Med. (2012) 1:792–802. doi: 10.5966/sctm.2012-0088
82. Lee V, Singh G, Trasatti JP, Bjornsson C, Xu X, Tran TN, et al. Design and fabrication of human skin by three-dimensional bioprinting. Tissue Eng Part C Methods. (2013) 20:473–84. doi: 10.1089/ten.tec.2013.0335
83. Rasperini G, Pilipchuk SP, Flanagan CL, Park CH, Pagni G, Hollister SJ, et al. 3D-printed bioresorbable scaffold for periodontal repair. J Dent Res. (2015) 94:153S–7S. doi: 10.1177/0022034515588303
84. Ahn G, Lee J-S, Yun W-S, Shim J-H, Lee U-L. Cleft alveolus reconstruction using a three-dimensional printed bioresorbable scaffold with human bone marrow cells. J Craniofac Surg. (2018) 29:1880–3. doi: 10.1097/SCS.0000000000004747
85. Zanetti EM, Aldieri A, Terzini M, Calì M, Franceschini G, Bignardi C. Additively manufactured custom load-bearing implantable devices. Australas Med J. (2017) 10:689–700. doi: 10.21767/AMJ.2017.3093
86. Bassoli E, Gatto A, Iuliano L, Grazia Violante M. 3D Printing technique applied to rapid casting. Rapid Prototyp J. (2007) 13:148–55. doi: 10.1108/13552540710750898
87. Oh J. Recent advances in the reconstruction of cranio-maxillofacial defects using computer-aided design/computer-aided manufacturing. Maxillofac Plast Reconstr Surg. (2018) 40:2. doi: 10.1186/s40902-018-0141-9
88. Huang MF, Alfi D, Alfi J, Huang AT. The use of patient-specific implants in oral and maxillofacial surgery. OralMaxillofac Surg Clin. (2019) 31:593–600. doi: 10.1016/j.coms.2019.07.010
89. Louvrier A, Marty P, Barrabé A, Euvrard E, Chatelain B, Weber E, et al. How useful is 3D printing in maxillofacial surgery? J Stomatol Oral Maxillofac Surg. (2017) 118:206–12. doi: 10.1016/j.jormas.2017.07.002
90. Karaokutan I, Sayin G, Kara O. In vitro study of fracture strength of provisional crown materials. J Adv Prosthodont. (2015) 7:27–31. doi: 10.4047/jap.2015.7.1.27
91. Park J, Lee J, Bae S. In vitro assessment of the marginal and internal fi ts of interim implant restorations fabricated with different methods. J Prosthet Dent. (2016) 116(4):536–42. doi: 10.1016/j.prosdent.2016.03.012
92. Abduo J, Lyons K, Bennamoun M. Trends in computer-aided manufacturing in prosthodontics: a review of the available streams. Int J Dent. (2014) 2014:783948. doi: 10.1155/2014/783948
93. Yoon S, Oh C, Lee SJ, Han J. Tissue surface adaptation of CAD-CAM maxillary and mandibular complete denture bases manufactured by digital light processing: a clinical study. J Prosthet Dent. (2019) 124(6) 682-9. doi: 10.1016/j.prosdent.2019.11.007
94. Tasaka A, Matsunaga S, Odaka K, Ishizaki K, Ueda T, Abe S, et al. Accuracy and retention of denture base fabricated by heat curing and additive manufacturing. J Prosthodont Res. (2019) 63:85–9. doi: 10.1016/j.jpor.2018.08.007
95. Layani M, Wang X, Magdassi S. Novel materials for 3D printing by photopolymerization. Adv Mater. (2018) 30:1706344. doi: 10.1002/adma.201706344
96. Methani MM, Revilla-León M, Zandinejad A. The potential of additive manufacturing technologies and their processing parameters for the fabrication of all-ceramic crowns: a review. J Esthet Restor Dent. (2020) 32:182–92. doi: 10.1111/jerd.12535
97. Ionita CN, Mokin M, Varble N, Bednarek DR, Xiang J, Snyder KV, et al. Challenges and limitations of patient-specific vascular phantom fabrication using 3D polyjet printing. Proc SPIE Int Soc Opt Eng. (2014) 9038:90380M. doi: 10.1117/12.2042266
98. Gross BC, Erkal JL, Lockwood SY, Chen C, Spence DM. Evaluation of 3D printing and its potential impact on biotechnology and the chemical sciences. Anal Chem. (2014) 86:3240–53. doi: 10.1021/ac403397r
99. Yin S, Zhang W, Tang Y, Yang G, Wu X, Lin S, et al. Preservation of alveolar ridge height through mechanical memory: a novel dental implant design. Bioact Mater. (2021) 6:75–83. doi: 10.1016/j.bioactmat.2020.07.015
100. Mai H-N, Hyun DC, Park JH, Kim D-Y, Lee SM, Lee D-H. Antibacterial drug-release polydimethylsiloxane coating for 3D-printing dental polymer: surface alterations and antimicrobial effects. Pharmaceuticals. (2020) 13:304. doi: 10.3390/ph13100304
101. Zhao X, Liu A, Zhou L, Yang Z, Wei S, Zhao Z, et al. 3D Printing of bioactive macro/microporous continuous carbon fibre reinforced hydroxyapatite composite scaffolds with synchronously enhanced strength and toughness. J Eur Ceram Soc. (2022) 42:4396–409. doi: 10.1016/j.jeurceramsoc.2022.04.012
102. McCabe JF, Yan Z, al Naimi OT, Mahmoud G, Rolland SL. Smart materials in dentistry. Aust Dent J. (2011) 56:3–10. doi: 10.1111/j.1834-7819.2010.01291.x
103. Wang Z, Li B, Cai Q, Li X, Yin Z, Li B, et al. Advances and prospects in antibacterial-osteogenic multifunctional dental implant surface. Front Bioeng Biotechnol. (2022) 10:921338. doi: 10.3389/fbioe.2022.921338
104. Münchow EA, da Silva AF, Piva E, Cuevas-Suárez CE, de Albuquerque MTP, Pinal R, et al. Development of an antibacterial and anti-metalloproteinase dental adhesive for long-lasting resin composite restorations. J Mater Chem B. (2020) 8:10797–811. doi: 10.1039/D0TB02058C
105. Seo S-J, Kim H-W, Lee J-H. Electrospun nanofibers applications in dentistry. J Nanomater. (2016) 2016:5931946. doi: 10.1155/2016/5931946
106. Porter MLA, Münchow EA, Albuquerque MTP, Spolnik KJ, Hara AT, Bottino MC. Effects of novel 3-dimensional antibiotic-containing electrospun scaffolds on dentin discoloration. J Endod. (2016) 42:106–12. doi: 10.1016/j.joen.2015.09.013
107. Zhou W, Qiao Z, Nazarzadeh Zare E, Huang J, Zheng X, Sun X, et al. 4D-printed dynamic materials in biomedical applications: chemistry, challenges, and their future perspectives in the clinical sector. J Med Chem. (2020) 63:8003–24. doi: 10.1021/acs.jmedchem.9b02115
Keywords: microfabrication, organ-on-a-chip, dental research, microarchitecture, 3D printing, photolithography, oral biomaterials
Citation: Tiozzo-Lyon P, Andrade M, Leiva-Sabadini C, Morales J, Olivares A, Ravasio A and Aguayo S (2023) Microfabrication approaches for oral research and clinical dentistry. Front. Dent. Med 4:1120394. doi: 10.3389/fdmed.2023.1120394
Received: 9 December 2022; Accepted: 13 February 2023;
Published: 9 March 2023.
Edited by:
James K. H. Tsoi, The University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Abdul Samad Khan, Imam Abdulrahman Bin Faisal University, Saudi Arabia© 2023 Tiozzo-Lyon, Andrade, Leiva-Sabadini, Morales, Olivares, Ravasio and Aguayo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sebastian Aguayo, c2ViYXN0aWFuLmFndWF5b0B1Yy5jbA==
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Dental Materials, a section of the journal Frontiers in Dental Medicine
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.