
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Dent. Med. , 22 January 2021
Sec. Pediatric Dentistry
Volume 1 - 2020 | https://doi.org/10.3389/fdmed.2020.623768
 Nomin Badrakhkhuu1
Nomin Badrakhkhuu1 Yusuke Matsuyama2Miyu Yoshizawa Araki1Yuko Unnai Yasuda1
Yusuke Matsuyama2Miyu Yoshizawa Araki1Yuko Unnai Yasuda1 Takuya Ogawa1Tsasan Tumurkhuu3
Takuya Ogawa1Tsasan Tumurkhuu3 Ganjargal Ganburged3Amarsaikhan Bazar4
Ganjargal Ganburged3Amarsaikhan Bazar4 Takeo Fujiwara2*
Takeo Fujiwara2* Keiji Moriyama1*
Keiji Moriyama1*Objective: Malocclusion has been reported to affect the daily lives of schoolchildren adversely, but little is known regarding the association between malocclusion and academic performance. We aimed to investigate the association between malocclusion and academic performance among adolescents in Mongolia.
Methods: We conducted a cross-sectional study of 767 students aged 7–16 years from two public schools in Ulaanbaatar, Mongolia. Three orthodontists evaluated the need for malocclusion treatment in the participants and determined the type of malocclusion using the Index of Orthodontic Treatment Need and dental casts. The academic scores of study participants in 20 subjects were provided by their schools. Z-scores within subjects were calculated and aggregated into both overall and in six groups of subject categories comprised of mathematics, science, social science, language, arts, and physical education. A multiple linear regression analysis was performed to determine the association between malocclusion, malocclusion type, and academic score adjusted for gender, age, school, and family income.
Results: Of the 767 students, 32.6% had malocclusion, and dental crowding was the most prevalent type (162 cases, 21.1%). Malocclusion was not significantly associated with the z-score of overall academic score [coefficient: 0.04, 95% confidence interval (CI): −0.11 to 0.19]; however, dental crowding was significantly associated with the overall academic score (coefficient: −0.19, 95% CI: −0.35 to −0.03), after adjusting for covariates. Other types of malocclusion were not associated with academic scores. Among the six subject categories, arts (coefficient: −0.20, 95% CI: −0.36 to −0.04) and physical education (coefficient: −0.24, 95% CI: −0.42 to −0.07) were significantly associated with dental crowding.
Conclusions: Schoolchildren in Mongolia with dental crowding may be prone to poor academic performance, particularly in arts and physical education classes. Further randomized controlled trials are needed to determine whether the treatment of crowding boosts academic performance.
Higher academic performance predicts socioeconomic status in adulthood (1). Various factors determine the academic performance of students; these factors can be divided into three categories: socioeconomic, environmental, and the student's individual factors (2). Health status is included in the student's individual factors (2), and a significant body of research has demonstrated that student health determines academic achievement in school (3, 4). Student health factors, such as body mass index (BMI) (5), quality and duration of sleep (6), diabetes (7), consumption of sweets (8), and depression (9), have been found to be associated with academic performance.
Oral health is also associated with academic performance. Dental caries, being the most prevalent dental disease (10), impair the daily lives of schoolchildren by causing problems with eating, smiling, and sleeping (11). As such, dental caries may be an oral health problem affecting the academic performance of students (12). A previously published literature review of 17 studies showed an inverse association between the number of days absent from school due to dental problems and academic performance (13). Another study found associations between dental problems and psychosocial outcomes, such as shyness, unfriendliness, feeling worthless, and unhappiness, in adolescents (14). A cross-sectional study of 2,871 schoolchildren in North Carolina suggested that the improvement of children's oral health may be a way to improve their educational experience (15).
Despite many studies focusing on dental caries as a determinant of academic performance (14, 16), to our knowledge, only one study has focused on the association of malocclusion with academic performance (17). It is well-known that some types of malocclusion lead to functional and, most importantly, esthetic limitations (18). Esthetic problems can lead to psychological discomfort of the patient, including tenseness, and self-consciousness (18); thereby, it may influence academic performance of children. A study conducted in India reported that severe malocclusion, as evaluated by the dental aesthetic index (DAI), influenced the psychosocial well-being of adolescents, who may avoid participating in social activities and tend to underperform academically (17). However, the DAI is unable to individually assess some occlusal traits, such as a deep overbite (19). Specific types of malocclusion were proven to affect different aspects of adolescents' life, including oral symptoms, functional limitations, and social well-being (20). Therefore, additional studies using other valid orthodontic indices to explore further the pathway of association between malocclusion types and academic performance are required. Also, the above study suggested that students with malocclusion academically underperformed, but the study failed to assess academic performance thoroughly by each subject category (17). As not all classes require students' interactions, more investigation with the academic subject category is needed.
Mongolia obtained democracy in 1990 and gradually transitioned into the market economy. At the same time, drastic changes also occurred in the education system as it changed from the 10-years school system to a 12-years school system (21). According to the Education Law, a citizen of Mongolia must obtain basic compulsory education and has a right to access general secondary education free of charge. Governmental funding for education increased by a factor of 1.54 from 1992 to 2002, and by a factor of 1.76 from 2003 to 2013 (22). The market economy also led to lifestyle and dietary changes. Brushing habits, the intake of sweets, and prolonged breastfeeding resulted in significant odds ratios for the development of caries (23), with an average of more than one-third of primary teeth decayed or filled in 5-year-old children (10). Consequently, preliminary primary teeth loss due to severe caries can cause malocclusion to develop in Mongolians (24). It was previously reported that the prevalence of malocclusion among Mongolian adolescents was 35.2% (25). Because the prevalence is low compared to that of other countries (26), the number of adolescents receiving orthodontic treatment is much smaller (1.2%) (25). Thus, the investigation is needed to understand better the association between malocclusion and academic performance among adolescents in East Asian populations, including developing countries like Mongolia, where the malocclusion is emerging, and few children are being treated.
This cross-sectional study used data from a longitudinal population-based epidemiological investigation. The study field was Ulaanbaatar, the capital city of Mongolia. The population of Ulaanbaatar was ~1,372,000 at the time of data collection, representing almost half of the country's population (46.8%) (27). Participants were recruited from two public schools that agreed to participate in the survey, with one located more centrally in the Bayanzurh district and the other in the suburban Songino Khairhan district. Two classes were randomly selected from grades 4 to 10 (i.e., aged 7–16 years old) in each school. Exclusion criteria were the presence of orthodontic treatment history. The detailed methods of the survey have been published elsewhere (25).
This article is structured according to STROBE guidelines for cross-sectional studies. Written informed consent was obtained from the caregivers through the classroom teachers. The study was approved by the Ethical Review Board of the Mongolian National University of Medical Science (No. 13-12/1A) and Tokyo Medical and Dental University (No. D2013-071).
Academic performance was evaluated by the final grades of the students at the end of the school year, provided by the schools. Public schools have the same criteria for the academic assessment of their students, which are established by the municipal secretary of education. Academic performance in Mongolia is graded by percentage (ranges from 0% to 100%; 60% is the passing grade). A total of 20 school subjects were classified into six groups following the ministerial decree and regarding the type of science (28) as follows: math group (mathematics subject only), natural science group (chemistry, biology, science, and physics subjects), social sciences group (health, geography, history, civil education, and social science subjects), language group (English language, Mongolian language, literature, Mongolian script, and Russian language subjects), arts group (craft, arts, music, and drafting subjects), and physical education group (physical education subject only). All academic performance scores were standardized (i.e., converted to z-score) within the grade. The mean score for each group of subjects and overall subjects was calculated and used as the dependent variable in subsequent analysis.
Three orthodontists (TT, GG, TO) evaluated the need for malocclusion treatment and type of malocclusion using the Dental Health Component of the Index of Orthodontic Treatment Need (IOTN) (29) and dental casts of the participants. Calibration of the investigators showed high inter-rater reliability (κ = 0.68, 96.7% agreement) (25). IOTN grades range from 1 to 5, and grades 1–3 are considered as “no treatment needed,” while grades 4 and 5 are considered as “needs treatment.” Malocclusion type was diagnosed by the following criteria: increased overjet (>6 mm overjet) and reverse overjet (< -1 mm overjet), deep bite (>3.5 mm overbite), and crowding (≥5 mm crowding), which were recorded as “need for treatment.” Anterior and posterior cross bite, scissor bite, and hypodontia were also recorded if present.
Multiple linear regression analysis was applied to investigate the association between malocclusion, malocclusion type, and academic performance. Sex, age, school, and family income were adjusted because a previous study among adolescents with malocclusion reported gender differences in academic performance (17), and another study reported the association of family income with the academic performance of adolescents (30) and malocclusion severity (31). The school variable was controlled as two public schools in our study are from centrally and suburban areas of Ulaanbaatar, which could have differences in average academic performance and malocclusion treatment needs. Family income level was assessed by the questionnaire and categorized into low (<500 thousand tugriks), average (510 thousand −1,000 thousand tugriks) and high (>1,001 thousand tugriks; 1 USD ~1,437 tugriks). P < 0.05 was considered statistically significant. All analyses were performed using the Stata 15 SE software program (StataCorp LP, college Station, TX, USA).
Table 1 describes the demographic characteristics of the participants. Of the 767 participants [mean age: 11.3; standard deviation (SD): 1.9; 43.8% male], 250 adolescents (32.6%) had a need for orthodontic treatment. Overall, the families of 131 (17.1%) adolescents had a high family income, 395 (51.5%) had average income levels, and 213 (27.8%) had low income levels. A chi-squared test revealed no significant association between the above demographic characteristics and the presence of malocclusion with the need for orthodontic treatment.
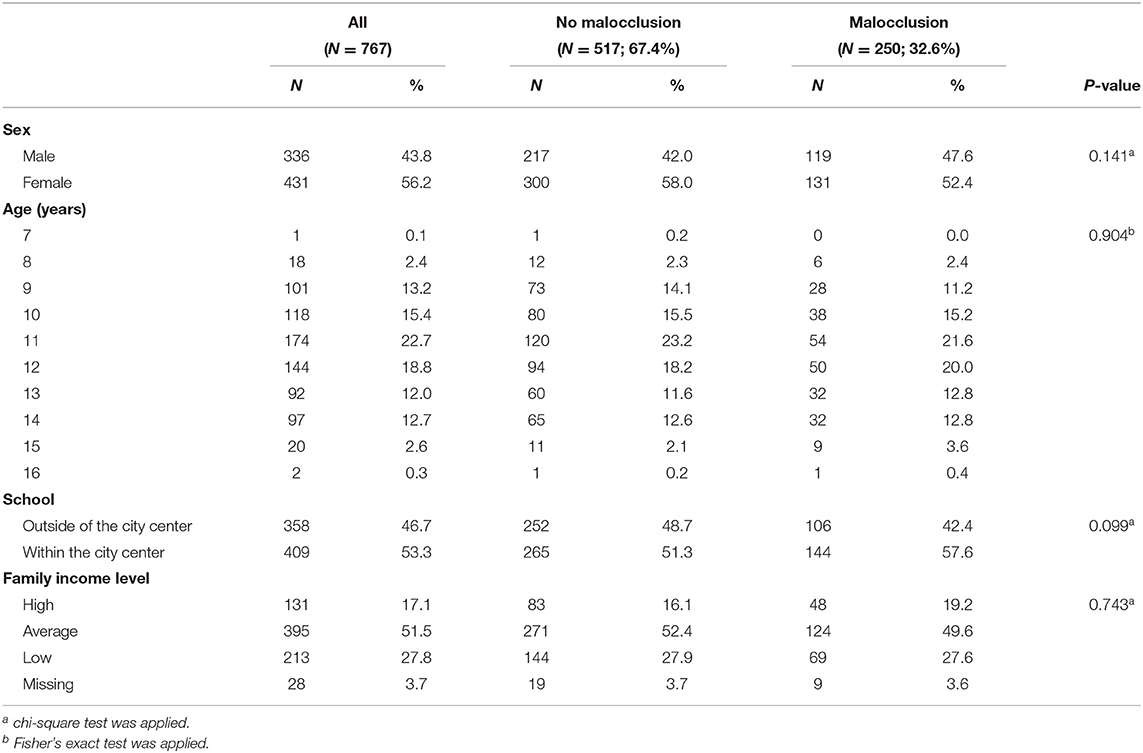
Table 1. Demographic characteristics of the participants, by presence of malocclusion.
As Table 2 shows, the most common malocclusion type was dental crowding (21.1%) and the least common was reverse overjet (1.6%). Meanwhile, anterior (9.4%) and posterior (6.8%) crossbites were the second and third most abundant types of malocclusion, respectively. Hypodontia (4.6%), scissor bite (4.2%), and increased overjet (3.8%) had approximately equal rates of occurrence.
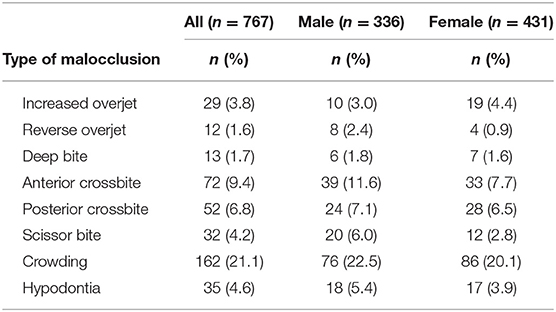
Table 2. Malocclusion type distribution.
Table 3 shows both the overall academic score and the score within each group of subjects after standardizing by malocclusion treatment needs and dental crowding treatment needs. Students with malocclusion had higher scores overall (z = 0.06; z = 0.03), and in science (z = 0.10; z = 0.00), language (z = 0.05; z = 0.03), arts (z = 0.12; z = 0.02), and physical education (z = 0.07; z = 0.02) than students without malocclusion. In contrast, students with dental crowding had lower academic scores than students without crowding in all subject categories.
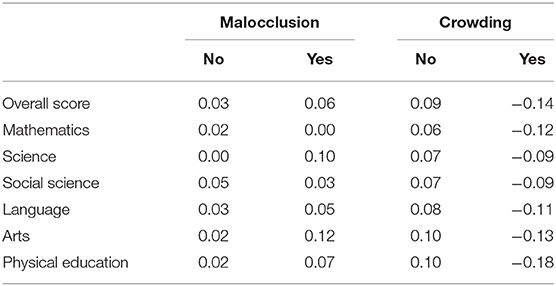
Table 3. Mean of academic score (Z-score) by malocclusion status and crowding.
Table 4 shows the association between malocclusion treatment need, malocclusion type, and overall academic score. Malocclusion treatment need was not associated with the overall academic score in the crude model [coefficient: 0.04; 95% confidence interval (CI): −0.11–0.19] or the adjusted model (coefficient: 0.08; 95% CI: −0.06–0.22). Among malocclusion types, only dental crowding exhibited a significant association with academic performance [coefficient: −0.23; 95% CI: (−0.40)–(−0.06)], and it remained significant in the adjusted model [coefficient: −0.19; 95% CI: (−0.35)–(−0.03)].
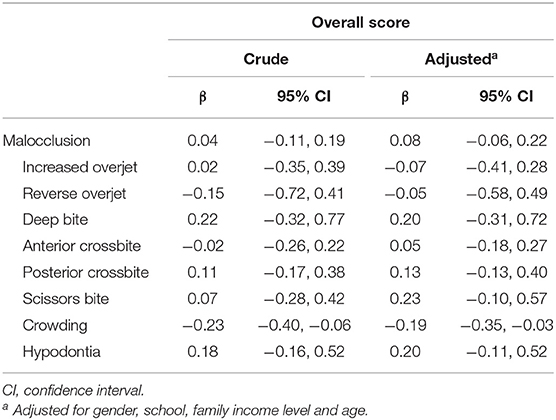
Table 4. Association between malocclusion type and overall Z score.
The association between crowding and each subject group was further evaluated to determine which groups of subjects were associated with crowding (Table 5). The arts subjects group [coefficient: −0.20; 95% CI: (−0.36)–(−0.04)] and physical education subject group [coefficient: −0.24; 95% CI: (−0.42)–(−0.07)] had significant associations with dental crowding after adjusting for covariates. Mathematics, science, social science, and language subject groups were not significantly associated with dental crowding.
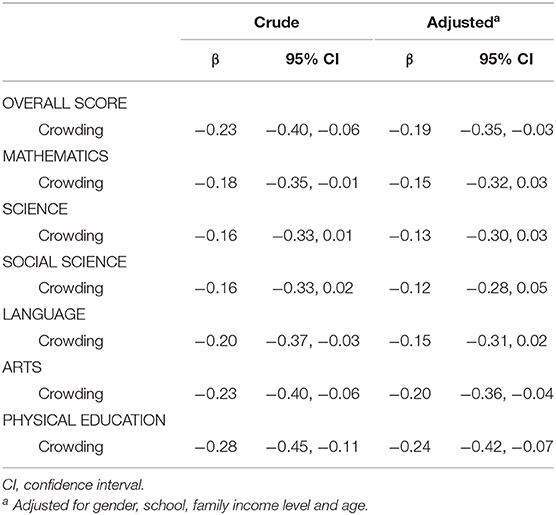
Table 5. Association between crowding and Z–score on each subject group.
We employed objective measurements of malocclusion and academic performance to reveal that malocclusion was not significantly associated with academic performance in schoolchildren in Mongolia. However, dental crowding was significantly associated with lower overall academic performance, particularly in arts and physical education subjects.
To our knowledge, only one study in India (17) has evaluated the association between malocclusion and academic performance in children; this study reported that students with severe malocclusion are more likely to exhibit poor academic performance (17). In contrast, we did not find a significant difference in academic performance depending on the need for malocclusion treatment. The inconsistency of these findings might be explained by the severity of the condition, given that the previous study focused on the academic performance of adolescents with severe malocclusion. They evaluated malocclusion with the DAI, which scores malocclusion on a continuous scale and differentiates cases within severity levels. Our measurement, the IOTN, evaluates orthodontic treatment needs but does not rank cases with greater or lesser need for treatment within grades (32). Instead, we evaluated the type of malocclusion, which was not evaluated in the previous study, and found that dental crowding was significantly associated with academic performance.
Social and biological pathways might explain the link between malocclusion and low academic performance of children. Malocclusion is associated with the emotional well-being and self-esteem of school children (33, 34). Poor oral condition results in an impaired smile and these children are likely to be socially excluded and perform poorly at school (12). Dental crowding, which showed association with overall, arts, and physical education performance, often presents in the anterior portion and can induce gingivitis (35). Symptoms such as gum bleeding and bad breath were associated with lower self-esteem and academic performance in children (12).
As for biological pathways, dental crowding is associated with headache (36), resulting in poor academic performance (37). Occlusal contact decreased by dental crowding (38) might reduce trigeminal nerve stimulation (39). Sensorimotor signals from the trigeminal nerve activate specific brain areas and, as a consequence, improve cognitive performance (40); a lack of signals from the trigeminal nerve causes cognitive impairment (41). Dental crowding as a chronic stressor might enhance the secretion of stress-activated neuronal responses in the hippocampus area. Thereby, it may suppress learning and memory ability (42, 43). Another study has proven that occlusal condition can influence the increase in cerebral blood flow generated by a motor task involving the fingers (44). This result is consistent with that of previous studies that have found occlusion to be important for maintaining and/or enhancing motor function (45). Further, a recent functional magnetic resonance imaging (fMRI) study revealed that molar biting was positively associated with the blood oxygenation level-dependent (BOLD) signal and electromyogram (EMG) activity of the masseter and temporal muscles, while incisal biting was negatively correlated with them (39). Their finding suggests molars engage in powerful chewing given that the brain areas related to powerful motor control are activated, whereas brain areas related to fine motor control are activated by incisor biting (39). According to the evaluation criteria of school subjects in Mongolia, the art subject category requires drawing skills, playing musical instruments, learning precision in drafting class, and handcrafting in crafts class (46). Such tasks might require fine motor skills, potentially explaining why dental crowding was associated with reduced scores in arts and physical education subjects in the present study.
Our study has several limitations. First, when evaluating the association of malocclusion treatment need and academic performance, only the worst occlusal trait was used to diagnose the malocclusion. However, we additionally evaluated all malocclusion types that meet the criteria. Second, only two public schools were recruited into the study, which can be a potential source of sampling bias. The findings might not be directly applicable to children living in rural areas in Mongolia. Third, our post-hoc power calculation showed that the statistical power to detect the overall academic score difference by malocclusion treatment need was 6.8%. Thus, we might have failed to detect the difference in population means. Fourth, due to the cross-sectional design of our study, no cause-and-effect relationship can be inferred from our data. The biological mechanism requires investigation through future studies, and a randomized controlled trial is also necessary to determine if the treatment of crowding increases academic performance.
In conclusion, we found that dental crowding is significantly associated with the academic performance of Mongolian adolescents. Our findings suggest that schoolchildren with dental crowding tend to show poor academic performance. Due to the rapid economic and social changes in Mongolia, our findings are important for comparison with future studies. Promoting oral health in school settings might improve children's academic performance. For example, regular dental health checkups in schools, which has not been previously implemented in Mongolia, might contribute to the early detection of malocclusion.
The datasets presented in this article are not readily available because of privacy or ethical restrictions. Requests to access the datasets should be directed to Keiji Moriyama, ay1tb3JpeWFtYS5tb3J0QHRtZC5hYy5qcA==.
The studies involving human participants were reviewed and approved by Ethical Review Board of the Mongolian National University of Medical Science (No. 13-12/1A) and Tokyo Medical and Dental University (No. D2013-071). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
NB contributed to conception, design, data acquisition, analysis, and interpretation and drafted and critically revised the manuscript. YM contributed to design, analysis, and interpretation and critically revised the manuscript. MA, YY, and TO contributed to conception, design, data acquisition, and interpretation and critically revised the manuscript. TT, GG, and AB contributed to data acquisition and critically revised the manuscript. TF contributed to design, data acquisition, analysis, and interpretation and critically revised the manuscript. KM contributed to conception and design and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank all participants of the longitudinal population-based Craniofacial Collaborative Research survey for their cooperation and the administration and teachers of both schools for providing research material. This work was supported by the grants-in-aid for scientific research from the Japan Society for the Promotion of Science, grant number 25305037.
1. Spengler M, Damian RI, Roberts BW. How you behave in school predicts life success above and beyond family background, broad traits, and cognitive ability. J Pers Soc Psychol. (2018) 114:620–36. doi: 10.1037/pspp0000185
2. Ivanovic DM, Almagià AF, Arancibia VC, Ibaceta C V., Arias VF, Rojas TR, et al. A multifactorial approach of nutritional, intellectual, brain development, cardiovascular risk, socio-economic, demographic and educational variables affecting the scholastic achievement in Chilean students: an eight- year follow-up study. PLoS ONE. (2019) 14:e0212279 doi: 10.1371/journal.pone.0212279
3. McIsaac J-LD, Kirk SFL, Kuhle S. The association between health behaviours and academic performance in canadian elementary school students: a cross-sectional study. Int J Environ Res Public Health. (2015) 12:14857–71. doi: 10.3390/ijerph121114857
4. Minkkinen J, Lindfors P, Kinnunen J, Finell E, Vainikainen MP, Karvonen S, et al. Health as a predictor of students' academic achievement: a 3-level longitudinal study of finnish adolescents. J Sch Health. (2017) 87:902–10. doi: 10.1111/josh.12572
5. Correa-Burrows P, Rodriguez Y, Blanco E, Gahagan S, Burrows R. Increased adiposity as a potential risk factor for lower academic performance: a cross-sectional study in chilean adolescents from low-to-middle socioeconomic background. Nutrients. (2018) 10:1133. doi: 10.3390/nu10091133
6. Susan Shur-Fen G. Prevalence of sleep problems and their association with inattention/hyperactivity among children aged 6-15 in Taiwan. J Sleep Res. (2006) 15:403–14. doi: 10.1111/j.1365-2869.2006.00552.x
7. Potts TM. Perception of difficulty and glucose control: effects on academic performance in youth with type I diabetes. World J Diabetes. (2015) 6:527. doi: 10.4239/wjd.v6.i3.527
8. Nakahara N, Matsuyama Y, Kino S, Badrakhkhuu N, Ogawa T, Moriyama K, et al. The consumption of sweets and academic performance among mongolian children. Int J Environ Res Public Health. (2020) 17:8912. doi: 10.3390/ijerph17238912
9. Riglin L, Petrides KV, Frederickson N, Rice F. The relationship between emotional problems and subsequent school attainment: a meta-analysis. J Adolesc. (2014) 37:335–46. doi: 10.1016/j.adolescence.2014.02.010
10. Yun S-W, Shin S-C, Chang Y-S, Kim H-K, Sohn S-J, Kim J-K, et al. A survey of dental caries in mongolia in 2014. Int J Clin Prev Dent. (2014) 10:165–78. doi: 10.15236/ijcpd.2014.10.3.165
11. Jürgensen N, Petersen PE. Oral health and the impact of socio-behavioural factors in a cross sectional survey of 12-year old school children in Laos. BMC Oral Health. (2009) 9:29. doi: 10.1186/1472-6831-9-29
12. Maharani DA, Adiatman M, Rahardjo A, Burnside G, Pine C. An assessment of the impacts of child oral health in Indonesia and associations with self-esteem, school performance and perceived employability. BMC Oral Health. (2017) 17:65. doi: 10.1186/s12903-017-0358-5
13. Paula de JS, Mialhe FL. Impact of oral health conditions on school performance and lost school days by children and adolescents: what are the actual pieces of evidence? Brazilian J Oral Sci. (2013) 12:189–98. doi: 10.1590/S1677-32252013000300008
14. Guarnizo-Herreño CC, Wehby GL. Children's dental health, school performance, and psychosocial well-being. J Pediatr. (2012) 161:1153–9.e2. doi: 10.1016/j.jpeds.2012.05.025
15. Blumenshine SL, Vann WF, Gizlice Z, Lee JY. Children's school performance: impact of general and oral health. J Public Health Dent. (2008) 68:82–7. doi: 10.1111/j.1752-7325.2007.00062.x
16. Jackson SL, Vann WF, Kotch JB, Pahel BT, Lee JY. Impact of poor oral health on children's school attendance and performance. Am J Public Health. (2011) 101:1900–6. doi: 10.2105/AJPH.2010.200915
17. Basha S, Parameshwarappa P, Mohamed RN, Swamy HS. Untreated gross dental malocclusion in adolescents: psychological impact and effect on academic performance in school. Oral Heal Prev Dent. (2016) 14:63–9. doi: 10.3290/j.ohpd.a35003
18. Chen M, Feng ZC, Liu X, Li ZM, Cai B, Wang DW. Impact of malocclusion on oral health-related quality of life in young adults. Angle Orthod. (2015) 85:986–91. doi: 10.2319/101714-743.1
19. Borzabadi-Farahani A, Eslamipour F, Asgari I. A comparison of two orthodontic aesthetic indices. Aust Orthod J. (2012) 28:30–6.
20. Araki M, Yasuda Y, Ogawa T, Tumurkhuu T, Ganburged G, Bazar A, et al. Associations between malocclusion and oral health-related quality of life among Mongolian adolescents. Int J Environ Res Public Health. (2017) 14:902. doi: 10.3390/ijerph14080902
21. UNESCO Bangkok. Secondary Education Regional Information Base: Country Profile – Mongolia. (2009). Available online at: http://uis.unesco.org/sites/default/files/documents/secondary-education-regional-information-base-country-profile-for-mongolia-en.pdf (accessed November 8, 2019).
22. Mongolian education alliance. Review Survey of Education Sector. (2013) Available online at: https://www.eri.mn/download/dfijcw68 (accessed January 16, 2020).
23. Jigjid B, Ueno M, Shinada K, Kawaguchi Y. Early childhood caries and related risk factors in Mongolian children. Commun Dent Health. (2009) 26:121–8. doi: 10.1922/CDH_2298Jigjid08
24. Fields HW, Proffit WR. Moderate nonskeletal problems in preadolescent children: preventive and interceptive treatment in family practice. In: Proffit WR, Fields HW, Sarver DM, editor. Contemporary orthodontics. 5th ed. St. Louis, MO: Mosby Inc.; Elsevier (2013). p. 395–445.
25. Tumurkhuu T, Fujiwara T, Komazaki Y, Kawaguchi Y, Tanaka T, Inazawa J, et al. Association between maternal education and malocclusion in Mongolian adolescents: a cross-sectional study. BMJ Open. (2016) 6:e012283. doi: 10.1136/bmjopen-2016-012283
26. Komazaki Y, Fujiwara T, Ogawa T, Sato M, Suzuki K, Yamagata Z, et al. Prevalence and gender comparison of malocclusion among Japanese adolescents: a population-based study. J World Fed Orthod. (2012) 1:e67–72. doi: 10.1016/j.ejwf.2012.07.001
27. National Statistics Office of Mongolia. Ulaanbaatar Population Statistics. (2013) Available online at: http://ubstat.mn/Report (accessed December 4, 2019).
28. Government of Mongolia Ministry of Education Culture Science and Sports. Ministerial Decree NºA61. Ulaanbaatar: Government of Mongolia, Ministry of Education, Culture, Science and Sports (2017).
29. Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. (1989) 11:309–20. doi: 10.1093/oxfordjournals.ejo.a035999
30. Echeverría SE, Vélez-Valle E, Janevic T, Prystowsky A. The role of poverty status and obesity on school attendance in the United States. J Adolesc Heal. (2014) 55:402–7. doi: 10.1016/j.jadohealth.2014.03.012
31. Healey DL, Gauld RD, Thomson WM. The socio-demographic and malocclusion characteristics of adolescents presenting for specialist orthodontic treatment in New Zealand practices. Aust Orthod J. (2015) 31:20–5.
32. Jenny J, Cons NC. Comparing and contrasting two orthodontic indices, the index of orthodontic treatment need and the dental aesthetic index. Am J Orthod Dentofacial Orthop. (1996) 110:410–6. doi: 10.1016/S0889-5406(96)70044-6
33. Bittencourt JM, Martins LP, Bendo CB, Vale MP, Paiva SM. Negative effect of malocclusion on the emotional and social well-being of Brazilian adolescents: a population-based study. Eur J Orthod. (2017) 39:628–33. doi: 10.1093/ejo/cjx020
34. Badran SA. The effect of malocclusion and self-perceived aesthetics on the self-esteem of a sample of Jordanian adolescents. Eur J Orthod. (2010) 32:638–44. doi: 10.1093/ejo/cjq014
35. Ashley FP, Usiskin LA, Wilson RF, Wagaiyu E. The relationship between irregularity of the incisor teeth, plaque, and gingivitis: a study in a group of schoolchildren aged 11-14 years. Eur J Orthod. (1998) 20:65–72. doi: 10.1093/ejo/20.1.65
36. Komazaki Y, Fujiwara T, Ogawa T, Sato M, Suzuki K, Yamagata Z, et al. Association between malocclusion and headache among 12- to 15-year-old adolescents: a population-based study. Community Dent Oral Epidemiol. (2014) 42:572–80. doi: 10.1111/cdoe.12111
37. Rocha-Filho PAS, Santos P V. Headaches, quality of life, and academic performance in schoolchildren and adolescents. Headache J Head Face Pain. (2014) 54:1194–202. doi: 10.1111/head.12394
38. English JD, Buschang PH, Throckmorton GS. Does malocclusion affect masticatory performance? Angle Orthod. (2002) 72:21–7. doi: 10.1043/0003-3219(2002)072<0021:DMAMP>2.0.CO;2
39. Yoshizawa H, Miyamoto JJ, Hanakawa T, Shitara H, Honda M, Moriyama K. Reciprocal cortical activation patterns during incisal and molar biting correlated with bite force levels: an fMRI study. Sci Rep. (2019) 9:8419. doi: 10.1038/s41598-019-44846-4
40. Hirano Y, Obata T, Takahashi H, Tachibana A, Kuroiwa D, Takahashi T, et al. Effects of chewing on cognitive processing speed. Brain Cogn. (2013) 81:376–381. doi: 10.1016/j.bandc.2012.12.002
41. Iinuma M. Relationship between the early toothless condition and hippocampal functional morphology. Anat Physiol. (2013) 4:3. doi: 10.4172/2161-0940.1000149
42. Arakawa Y, Ichihashi Y, Iinuma M, Tamura Y, Iwaku F, Kubo KY. Duration-dependent effects of the bite-raised condition on hippocampal function in SAMP8 mice. Okajimas Folia Anat Jpn. (2007) 84:115–9. doi: 10.2535/ofaj.84.115
43. Otsuka T, Watanabe K, Hirano Y, Kubo K, Miyake S, Sato S, et al. Effects of mandibular deviation on brain activation during clenching: An fMRI preliminary study. Cranio J Craniomandib Pract. (2009) 27:88–93. doi: 10.1179/crn.2009.014
44. Tramonti Fantozzi MP, Diciotti S, Tessa C, Castagna B, Chiesa D, Barresi M, et al. Unbalanced occlusion modifies the pattern of brain activity during execution of a finger to thumb motor task. Front Neurosci. (2019) 13:499. doi: 10.3389/fnins.2019.00499
45. Ishijima T, Hirai T, Koshino H, Konishi Y, Yokoyama Y. The relationship between occlusal support and physical exercise ability. J Oral Rehabil. (1998) 25:468–71. doi: 10.1046/j.1365-2842.1998.00254.x
Keywords: malocclusion, academic performance, epidemiology, orthodontics, quality of life, Mongolia
Citation: Badrakhkhuu N, Matsuyama Y, Araki MY, Yasuda YU, Ogawa T, Tumurkhuu T, Ganburged G, Bazar A, Fujiwara T and Moriyama K (2021) Association Between Malocclusion and Academic Performance Among Mongolian Adolescents. Front. Dent. Med. 1:623768. doi: 10.3389/fdmed.2020.623768
Received: 30 October 2020; Accepted: 29 December 2020;
Published: 22 January 2021.
Edited by:
Mohammad Khursheed Alam, Al Jouf University, Saudi ArabiaReviewed by:
Flavio Demarco, Federal University of Pelotas, BrazilCopyright © 2021 Badrakhkhuu, Matsuyama, Araki, Yasuda, Ogawa, Tumurkhuu, Ganburged, Bazar, Fujiwara and Moriyama. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Takeo Fujiwara, ZnVqaXdhcmEuaGx0aEB0bWQuYWMuanA=; Keiji Moriyama, ay1tb3JpeWFtYS5tb3J0QHRtZC5hYy5qcA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.