
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Digit. Health, 12 November 2024
Sec. Connected Health
Volume 6 - 2024 | https://doi.org/10.3389/fdgth.2024.1496196
 Alberto Fucarino1,†
Alberto Fucarino1,† Giovanna Zimatore1,†
Giovanna Zimatore1,† Antonio Fabbrizio1,†
Antonio Fabbrizio1,† Nuno D. Garrido2,3Victor Machado Reis2,3
Nuno D. Garrido2,3Victor Machado Reis2,3 José Vilaça-Alves2,3
José Vilaça-Alves2,3 Martina Sausa1Barbara Matteo1
Martina Sausa1Barbara Matteo1 Rafael Peixoto2Paulina Perušina4Aleksandra Aristova5
Rafael Peixoto2Paulina Perušina4Aleksandra Aristova5 Andrea De Giorgio1
Andrea De Giorgio1 Carlo Baldari1
Carlo Baldari1 Filippo Macaluso6*
Filippo Macaluso6* Enzo Iuliano1,†
Enzo Iuliano1,† Manuela Cantoia1,†
Manuela Cantoia1,†
Background: The study investigates the impact of tele-exercise on physical fitness and psychological well-being in healthy individuals. Tele-exercise, facilitated by technology, offers a flexible and accessible alternative to traditional exercise, particularly beneficial during restricted in-person interactions.
Methods: In this study, 52 participants were divided into three groups: athletes, women, and young adults. They took part in an eight-week tele-exercise program, either synchronously or asynchronously. Physical fitness was evaluated using tests such as the 2-Minute Step and Curl Up Test, while psychological well-being was assessed using the Psychological General Well-Being Index (PGWBI) and Perceived Stress Scale (PSS-10).
Results: Significant improvements in physical fitness and psychological well-being were observed in post-intervention across all groups, regardless of training mode. In the fitness tests, a significant improvement was obtained in the 2-Minute-Step (p = 0.004), in the curls up (p = 0.017), and in squats test (p = 0.004). In the forward bending test, the increment was very close to the significance (p = 0.051). In the psychological well-being tests, both PGWBI and WHO-5 scores increased after the training (p = 0.024 and p = 0.001 respectively) with no significant change in the PSS-10 score. The study found that tele-exercise can effectively introduce physical activity to previously inactive individuals and motivate them to adopt healthier lifestyle behaviors.
Conclusions: The TELEexe4ALL project demonstrates the potential of tele-exercise to improve physical fitness and psychological well-being. The study suggests that tele-exercise is a feasible and well-accepted approach for enhancing overall wellness in healthy populations.
Technological progress has brought about a significant transformation in various aspects of our lives, including the healthcare sector (1). One noteworthy advancement in this domain is the advent of tele-exercise, which involves utilizing technologies to remotely administer exercise-based interventions. Thus, tele-exercise allows for exercise programs to be delivered without the need for physical proximity, simultaneously expanding access to healthcare services (2). This approach has garnered growing interest and acknowledgement as a pioneering method to encourage physical activity and enhance health results, especially in circumstances where in-person interactions are restricted or unattainable (3–5). Hence, tele-exercise has traditionally been utilized as a means of rehabilitation, as one key benefit is its inherent flexibility and convenience since it eliminates the need for individuals to physically reach exercise facilities or clinics. As a result, it is an easily accessible option for those with mobility impairments or those living in distant locales. Remote training delivery has shown promising potential in different populations, ranging from people with chronic condition (6–8), such as Parkinson (9) or Diabetes (10), to people in rehabilitation after a stroke (11), a spinal cord injury (12) or cardiac problems (13), to healthy ones, seeking personalized exercise programs such as elders (14–17).
The literature has also shown that exercise is able to improve both the cognitive (18, 19) and emotional sphere (16, 20, 21), benefits that also seem to be maintained by tele-exercise, although the research in this regard in healthy people is still scarce (22). To all aforementioned benefits should be added the fact that tele-exercise allows both personalized prescriptions and real-time monitoring through smart devices (23), by giving the opportunity to the trainers to tailor interventions/training based on individual needs and monitor progress more effectively. However, considering tele-exercise as an exclusive mode of physical rehabilitation would be wrong and limiting. There has been a steady rise in the number of applications designed for the wellness of the general population (24–27). Additionally, the scientific community is actively researching the advantages of tele-exercise in enhancing the overall quality of life and habits of those subjects that are already in good health (16, 28, 29) and choose to stay active through remote means. Tele-exercise can benefit people of all ages and backgrounds, including athletes, seniors, and youth. Tele-exercise's positive impact on both physical wellness and mental well-being is universal, making it an effective method for enhancing overall health and well-being (14, 16, 22, 30–33).
Despite the growing evidence supporting the benefits of tele-exercise, several challenges and considerations should be addressed to ensure its successful implementation, including technological infrastructure, privacy and security concerns, and the need for appropriate training and support for both trainers and participants. Further, to our best knowledge, the effects on tele-exercise on the psychological sphere of healthy people have not been investigated. With the purpose of support and stimulate exercise, improve physical wellness and psychological wellbeing, ensuring privacy and security, it has been designed the European project called “TELEexe4ALL”, characterized—as far as we know for the first time—by designing a dedicated platform that can be accessed by people through synchronous and asynchronous mode. The open-source platform TELEexe4ALL (34) provides tele-exercise sessions based on end-user characteristics, creating homogeneous and inclusive classes. Through this platform we wanted to investigate the effects of synchronous and asynchronous tele-exercise in a heterogenous group of healthy people (from sedentary subjects to athletes) by investigating their state of well-being and physical activity. Here we present preliminary data, discussing possible future developments and scenarios.
A total of 52 participants (34 females and 18 males, aged 30.65 ± 8.86 years) were recruited for the present preliminary study and clustered in 3 intervention groups: 16 participants were athletes of both gender (ATHLETES group), 17 participants were adult women (WOMEN group), and 19 participants were young adults of both genders (YOUNG group). Each participant had the opportunity to follow a tele-exercise course either in asynchronous (N = 31; AS group) or synchronous mode (N = 21; SY group). The participants’ main characteristics and the number of participants that decided to follow the course in asynchronous or synchronous mode are shown in Table 1.

Table 1. Participants’ characteristics.
The enrollment into the three intervention groups was performed using a convenience sampling based on the inclusion and exclusion criteria reported in Table 2. The study was promoted using the TELEexe4ALL open-source platform, the social media channels of the project (Twitter, Facebook, Instagram), the social channels of the TELEexe4ALL partners, with the aim of recruiting potential participants. Subsequently, each potential participant filled in a questionnaire on personal data to assess the inclusion and exclusion criteria. Finally, they were assigned to the respective group (ATHLETES, YOUNG, WOMEN).
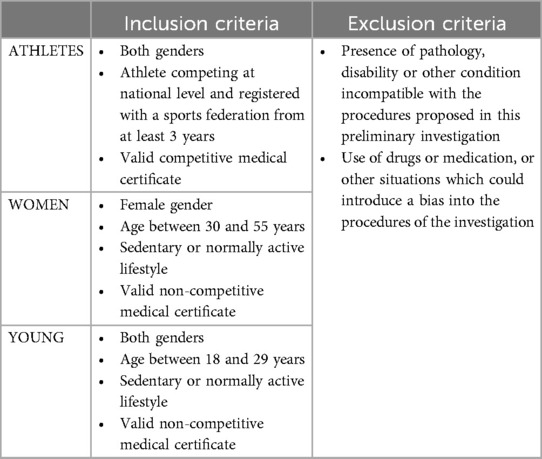
Table 2. Inclusion and exclusion criteria.
The duration of the intervention was 8 weeks. During this period the participants of WOMEN and YOUNG groups had to attend 24 exercise lessons (3 lessons/week) in telematic mode lasting 1 h per lesson. ATHLETES integrated their routine training following 16 exercise lessons (2 lessons/week). The lessons were delivered on the TELEexe4ALL open-source platform (accessible at the website www.teleexe4all.eu). Once registered, participants could choose whether to attend the lessons in synchronous or asynchronous mode and had access to all the video-lessons scheduled for their respective groups.
In this mode, all the lessons were conducted by an instructor live and in real time. Participants had to perform a series of exercises shown via video-lessons, while an experienced instructor monitored their execution and corrected them if necessary. In the synchronous mode, participants had the opportunity to interact with instructors and other participants in real-time using the meeting functionality of the TELEexe4ALL platform. The exercises shown in all the video-lessons were accurately demonstrated by an expert instructor that showed the correct execution to be performed and tried to describe the most common mistakes to be avoided. Furthermore, all the exercises proposed could be performed without the aid of any gym tool or machinery as they were designed to be feasible in a home environment.
During the lessons, the ratio between the supervising instructor and the participants ranged from 1/2 to 1/8.
In this mode, all the lessons were administered via pre-recorded video-lessons. Consequently, in the asynchronous mode, no real-time supervision by expert instructors was provided. At any time, participants had access to the same video-lessons used for the synchronous lessons, and they simply had to reproduce the exercises autonomously. Participants were asked to carry out the 24 video-lessons of training with a frequency of 3 video-lessons per week, on non-consecutive days. The platform tracked participants’ access to the video-lessons to evaluate actual compliance with scheduled days and to avoid over- or undertraining.
As in the synchronous mode, all the exercises could be performed without the aid of any gym tool or machinery.
The type of training varied based on the specific needs of the target population. The ATHLETES group performed a training protocol focusing on different strength and conditioning exercises designed for prevention of injury. The exercises aimed to produce a conditioning of the major muscles’ groups and joints. The intensity of the workouts was initially 4 RPE points (rate of perceived effort), up to a maximum of 6 RPE using Borg's CR10 scale (35). The WOMEN group performed a functional training consisting of mixed workouts to improve both cardiovascular and muscular fitness, with a particular focus on the major muscles’ groups to maximize the health benefit induced by training. The intensity of the workouts was initially 4 RPE points, up to a maximum of 8 points based on participants’ fitness level. The YOUNG group performed mixed workouts with the aim of improving cardiovascular fitness, muscular fitness, but also coordination skills. This training was designed to promote an overall improvement of all motor skills. Also in this case, the intensity of the workouts will initially be 4 RPE points, up to a maximum of 8 points depending on participants’ fitness level.
At the beginning and at the end of the 8 weeks of intervention, a series of tests were performed to evaluate the differences between pre- and post-intervention scores as explained in the following section. The tests were both physical (fitness tests) and psychological (psychological well-being, perceived stress). In the post-intervention assessment, a qualitative survey was carried out to the participants to have feedback concerning their opinions on the activity performed.
The fitness tests were selected as they do not require any equipment and specific skills, and they could be easily and safely administered in a domestic environment. The tests were performed in an autonomous manner by the participants of the WOMEN and YOUNG groups (N = 35); the participants of the ATHLETES group did not perform any fitness tests since their physical fitness level was not comparable with amateur trainees. The tests were administered at baseline and at the end of the intervention to evaluate any significant changes in these scores due to training.
The following tests were used:
2-min step test: It is a field test used to assess aerobic fitness. In this test, the participant must stand next to the wall and mark on the wall the corresponding point halfway between the kneecap and the iliac crest. Then, the participant marches in place for two minutes, raising his knees to the point that he/she marked on the wall and must count the number of steps he/she can take in two minutes. Resting is allowed during the 2 min of the test (36).
Curl up test: This test is a field test aiming to assess the strength and endurance of the abdominal muscles. The participant must lie down on a mat with their knees bent at 90°, their feet flat on the floor and their hands resting on their thighs. Then, the participants must perform a series of carl ups sliding their hands up their thighs until the fingertips touch the top of the kneecaps and then return to the starting position. The two movements (carl up and returning to the starting position) must be performed in approximately 3 s. To maintain the rhythm during the test it is advisable to use a metronome set to 20 beats per minute. The athlete must count the number of curls he/she can perform as long as he/she can maintain the rhythm of the metronome (37).
Forward bending test: This Standing test was adapted from the “Sit and reach test” (38, 39) to determine the flexibility of the spine and hips. The participant in standing position, with his/her knees extended, must bend forward trying to touch the lowest point of the lower limbs with his/her fingertips. A score is assigned based on the following criteria: 1 point is awarded if the participant reaches the thighs with his/her fingertips, 2 points if he/she reaches the knees, 3 points if he/she reaches the shins, 4 points if he/she reaches the ankles, 5 points if he/she touches the feet, and 6 points if he/she touches the floor.
Squat test: This field test aims to assess the strength and endurance of the lower limb muscles. The participants must stand approximately 40–50 cm in front of a chair, with the back facing the chair and with the feet shoulder-width apart. Then, the participant must squat down until he/she lightly touches the chair with his/her buttocks (but without sitting down), and then stand back up and repeat this sequence of movements until they are unable to continue. The participant must count the total number of squats performed. Resting is not allowed and the two movements (squat down and return to the starting position) must be performed in approximately 3 s (40).
As for Fitness tests, the tests psychological tests were administered at baseline and at the end of the intervention to evaluate any significant changes in these scores due to training. All the tests were administered via TELEexe4ALL platform. The following psychological tests were administered to all participants to assess the influence of tele-exercise on psychological well-being:
• Perceived stress scale (PSS-10): We used the Italian version of the Perceived Stress Scale (41, 42), which is a10-item self-report measure of perceived stress to evaluate the degree to which respondents appraise events as stressful during the past month. Items are rated on a 5-point Likert scale (from 0 = never, to 4 = very often), and higher total scores indicate greater perceived stress.
• World health organization—five well-being index (WHO-5): It is a questionnaire that is commonly used to assess subjective well-being and mental health (43). It is a self-reported measure that consists of five items, each focusing on different aspects of well-being. Participants are asked to rate each item on a 6-point Likert scale ranging from 0 to 5, with higher scores indicating greater well-being. The items assess feelings of happiness, interest in daily activities, energy levels, and overall satisfaction with life.
• Short form of the psychological general well-being index (PGWBI a/b): The questionnaire assesses both individual's subjective well-being and psychological health. The Italian version (44) is a short self-report measure that consists of 6 items, each one covering one dimension of well-being: anxiety, depressed mood, positive well-being, self-control, general health, and vitality. It is designed to capture both positive and negative aspects of well-being in the past month, providing a comprehensive assessment of an individual's psychological state. Each item is rated on a 6-point Likert scale, ranging from 0 (none of the time) to 5 (all of the time).
Three months into the conclusion of the training period, participants were contacted for a follow-up survey. Thirty-five participants (26 females; 9 males) filled in the questionnaires. The participants represented the three groups whose characteristics are described in Table 3. As for the psychological well-being tests, this survey was administered via TELEexe4ALL platform.

Table 3. Characteristics of the sample who completed the qualitative post survey.
The qualitative post survey consisted of 19 items assessing: (1) the participants’ degree of satisfaction, (2) their possible increased involvement in weekly exercise after participation in the project, and (3) any suggestions or criticisms. Two items were categorical ordered items, respectively investigating the engagement in physical exercise programs before and after the participation in the present project, 14 items were 5-point Likert scale (Strongly disagree, Disagree, Neither agree nor disagree, Agree, Strongly agree), investigating the opinion of the participants on different aspects of the project (45), while the last 3 items were open-ended items, asking for eventual suggestion or criticism.
A priori power analysis indicated that a total sample size of 30 subjects was required to detect a medium effect size (f = 0.25) given a coefficient of correlation p = 0.60 with 80% power and alfa = 0.05, using ANOVA repeated measure, within factors.
A Kolmogorov–Smirnov Test of Normality was performed to confirm if variables were normally distributed.
Repeated measures analysis of variance (RM-ANOVA) was used to assess main time effects of methods (pre vs. post), the interaction time*groups (ATHLETES, WOMEN, YOUNG) and interaction effects, time*mode (AS, SY). All the scores obtained by the fitness and psychological tests were considered as dependent variables for the analyses. Partial Eta square (η2p) was also computed as an indicator of the effect size of the analysis.
Statistical analysis of qualitative post survey: Firstly, a descriptive frequency analysis performed on the two categorical items respectively investigating the engagement in physical exercises programs before and after the participation were performed. Then, another descriptive analysis (mean score ± SD) of the 14 Likert scaled items was calculated. This descriptive analysis was performed for all participants as a single group, and separately for each one of the three groups ATHLETES, WOMEN, and YOUNG. The non-parametric Kruskal-Wallis's test was successively used to compare the results of the three groups to evaluate whether significant differences existed among them. Finally, the last 3 items, that were open-ended items, were analyzed in qualitative way by grouping the suggestions and indications based on their similarity.
For all the analyses, statistical significance was defined as p ≤ 0.05 and all results were expressed as mean ± SD for continuous variables, or percentage and numerosity for categorical variables.
All statistical analysis was performed by SPSS version 27.0 software (SPSS Inc., Chicago, IL, USA).
All the participants considered in this preliminary study results completed 100% of the proposed lessons.
RM-ANOVA results show statistically significant differences in the pre-post administrations of the tests. At the end of the training period, participants performed a mean of 166.11 ± 42.45 steps in 2-Minute-Step test, instead of the 140.28 ± 42.65 steps they reached before starting the training. These results are significantly different (F = 9.497, η2p = 0.213, p = 0.004).
At the end of the study, participants were also able to perform a mean of 40.17 ± 19.73 curls up, instead of the previous 35.69 ± 19.56 in the pre-test (F = 6.274, η2p = 0.152, p = 0.017), and a mean of 51.28 ± 38.03 squats instead of 42.86 ± 32.27 (F = 9.640, η2p = 0.216, p = 0.004). They also registered an increase in the mean number of forward bending (F = 4.093, η2p = 0.105, p = 0.051) that is very close to significance.
Furthermore, RM-ANOVA reported a significant difference when considering the interaction with groups only in the 2-Minute Step Test with a better trend for the YOUNG trainees. No significant differences were found in the interaction time*mode (synchronous vs. asynchronous mode). The complete results are reported in Table 4.
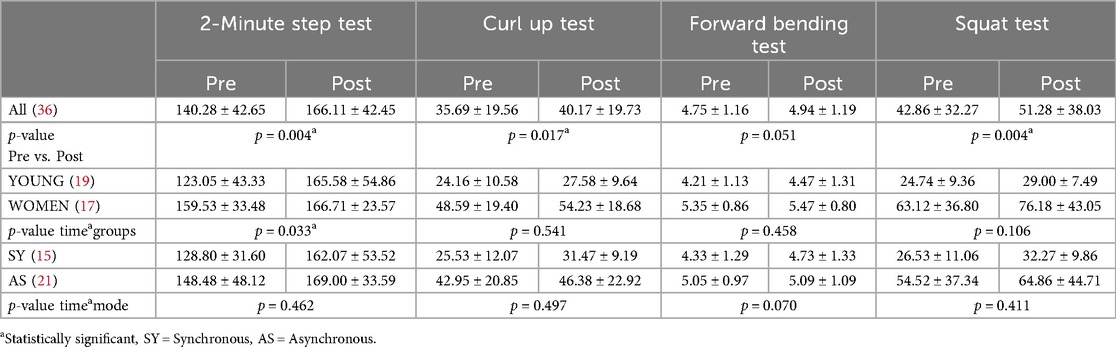
Table 4. Results of the fitness tests.
Perceived stress (PSS-10) registered low levels with no significant change after the training period as shown in Table 5 (F = 3.743, η2p = 0.068, p = 0.059). The levels of stress were aligned with data from the Italian validation (42).
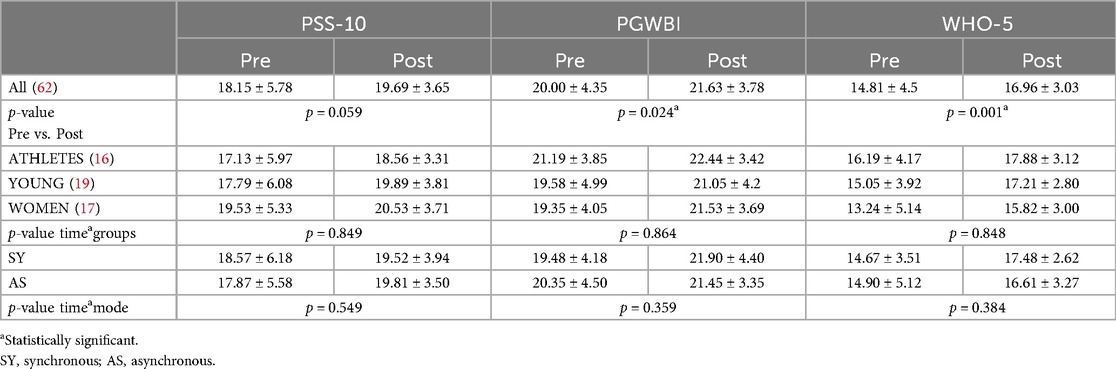
Table 5. Results of the psychological tests.
The levels of wellbeing, as detected through the short form of PGWBI, were at the ≈66% at baseline. The score significantly increased after the training showing +1.63 points on average (F = 5.376, η2p = 0.095, p = 0.024).
RM-ANOVA also showed a significant amelioration in pre-post comparison for WHO-5 test on wellbeing (F = 12.343, η2p = 0.195, p = 0.001), whose mean total score increases from 14.81 ± 4.53 to 16.96 ± 3.03, remaining largely over the cut off for depression (43). The RM-ANOVA reported no differences when considering the interaction with group and mode.
Results of the descriptive frequency analysis performed on the two categorical items respectively investigating the engagement in physical exercises programs before and after participation in the project are reported in Table 6. As predictable, Athletes declared to train all day or all week both before and after the project. The frequency for the YOUNG and WOMEN groups allows for a better interpretation of the effects of the program: sedentary participants decreased from 32% to 12% and physical activity during the week increased both as once a week (from 20% to 25.71%) and more days a week (from 28.57% to 40%) habit.

Table 6. The engagement in physical exercises programs before and after participation in the project.
The mean score ± SD of the 14 Likert scaled items calculated for all the participants considered as one group, and for each one of the three groups, as well as the results of the non-parametric Kruskal-Wallis's test comparing the results of the three groups are instead reported in Table 7 score ranged from 1 (Worst) to 5 (Best).
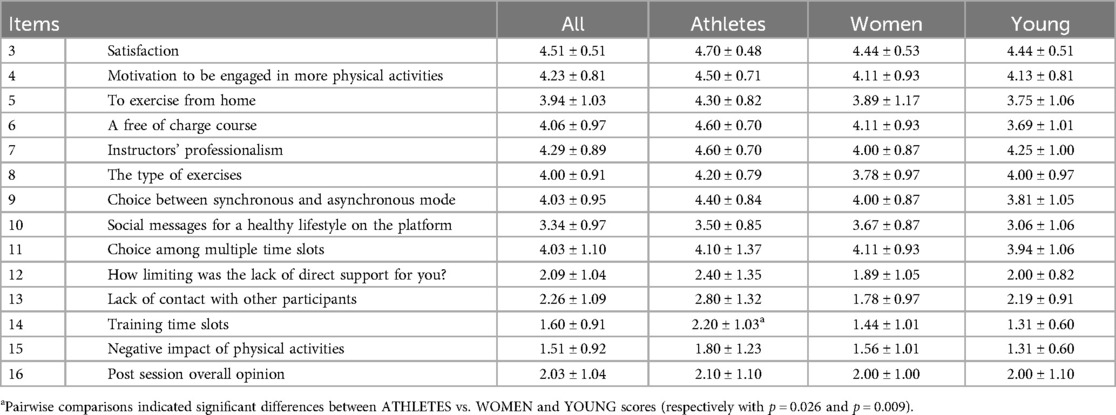
Table 7. Positive and negative assessment of the program.
Participants were all very satisfied with the program (score: 4.5 ± 0.51) and felt motivated to engage in more physical activities (score: 4.23 ± 0.81) with no differences among the groups (except for Training Time Slots p < 0.006). The most important features of the project were all scored above 3.30 on a Likert scale of 5 points. The most appreciated item was the instructors’ professionalism (4.29 ± 0.89), while the least appreciated was receiving social messages for a healthy lifestyle on the platform (3.34 ± 0.97).
The Kruskal-Wallis's test showed significant differences only in the item n. 14 “Training time slots” with a significant overall difference among the three groups (H = 10.351, η2 = 0.261, p = 0.006). Pairwise comparisons showed significant differences between ATHLETES vs. WOMEN and YOUNG scores (respectively with p = 0.026 and p = 0.009).
The main objective of this study was to evaluate whether the implementation of a tele-exercise platform could benefit on a physical and psychological level different categories of users in good health, in “the post-covid era”. The technological advancements and availability of digital interconnection technologies have made exercise activities through telematics more enjoyable. Although the concept of tele-exercise dates back to the early 2000s (14), it only gained popularity a decade later (46, 47). The unfortunate period of the COVID-19 pandemic has renewed interest in physical activity carried out in a telematics mode (4, 48, 49). Tele-exercise is now a beneficial tool for everyone, not just critically ill patients or those undergoing rehabilitation, as research has shown. Some recent studies addressed online applications for exercise promotion in a telematics mode (50–52). We hope that the international scientific community will continue to explore the benefits of tele-exercise, as an effective way to improve the poor physical activity habits of a consistent number of European and Western citizens.
Indeed, we know from literature that even the programs that focus on healthy individuals could have some critical shortcomings. To ensure maximum participation rates, a tele-exercise program should not just provide a downloadable application but also a platform that can be accessed from any device. Furthermore, to cater to diverse individuals with different needs, synchronous and asynchronous training modes should be provided simultaneously.
Finally, to optimize the results, exercise programs must be as personalized as possible. These are the exact features that the TELEexe4ALL project is aimed to improve.
Furthermore, authors have recently proposed a new method for detecting the aerobic metabolic threshold (53, 54). This method relies solely on heart-rate time series, which eliminates the need for visual inspection; in future, it can be easily implemented in applications that gather data from portable heart rate monitors and during specific tele-exercise sessions. It is implied that one can automatically determine one's level of fitness and access it personally.
In this work the participants were divided into three groups and underwent a tele-exercise program for eight weeks, with different training frequencies and modes, as explained in the previous sections.
The results of the physical and psychological tests in the post-intervention showed significant improvements compared to the pre-intervention scores, regardless of the mode of training (synchronous vs. asynchronous).
In the fitness tests (that were underwent only by YOUNG and WOMEN groups), the RM-ANOVA results indicated statistically significant differences in the participants’ pre-post performances of 2-Minute Step Test, curls up, squat, and forward bending. Participation in the training program by untrained and slightly trained (young and women) allowed an increase in their fitness level after a relatively short period, regardless of age, gender, and physical test considered. In particular, analyses indicated a significant interaction time*group in the performance of the 2-Minute Step Test: YOUNG participants improved more than WOMEN, probably due to their lower level in the baseline. We know from literature that less trained individuals increase their performance higher than normally trained (see Table 4) (55). The improvement in the physical fitness outcomes obtained in the present study is in accordance with previous study and review in literature (14, 56). However, it should be noted that a comparison of the present results with the literature is complicated given that the studies present in the literature are very heterogeneous in terms of participants (often with pathologies), proposed training protocols (which are often related to rehabilitation training) and duration of the intervention.
Regular exercise not only improved physical fitness but also had a positive impact on overall psychological well-being, as measured by the WHO-5 and PGWBI questionnaires, with no difference related either to the participants’ characteristics, nor to the modality of the tele-exercise (synchronous vs. asynchronous).
Furthermore, the qualitative survey showed a good level of satisfaction of the participants concerning the program and a high level of motivation to engage in more physical activities. In detail, the possibility of planning the session slots resulted more important for athletes who already have a strict training schedule, the other groups preferred asynchronous mode and were enough motivated to complete their training program.
This data allows us to confirm that the first course of TELEExe4all project has in fact achieved its objective of promoting more active lifestyles. The project therefore not only proved useful from the point of view of improving physical fitness and from a psychological point of view, but also proved to be well accepted by the participants and feasible in its current version.
In conclusion, the study confirms the importance of physical activity in overall wellness and well-being; the results also suggest that tele-exercise can be an effective and well-received method for enhancing physical fitness and psychological well-being in healthy individuals, regardless of the participant group, exercise mode nor level of activity.
The primary goal of our work is to promote healthier lifestyle habits amongst participants, with a focus on sustaining these habits over time. Encouragingly, we have observed a rise in the number of individuals who have engaged in at least some physical activity throughout the week, as opposed to their previously sedentary state. We have found that tele-exercise is an effective means of introducing physical activity to those who were previously inactive and can serve as a catalyst for the adoption of healthier lifestyle behaviors.
In this paper, the results provide valuable insights into the potential and various benefits, both physically and psychologically, of tele-exercise and lay the groundwork for future research in this area. One more asset of this work is represented by multidisciplinary study design and the aim to offer a free platform for healthy people to exercise with fitness purpose in an environment scientifically controlled and with activities that do not need any particular device to be performed.
This current preliminary analysis has some limitations, particularly on the number of participants. As the study is ongoing, tele-exercise sessions were still going on the platform to expand the sample of subjects who participate in the TELEexe4ALL project and to include other categories, such as elderly people (57, 58) and people with disabilities. Although these categories often face difficulties in interfacing with the latest technologies, in authors’ opinion they may be among those who benefit most from the practice of tele-exercise, as demonstrated by other studies (59–61). In general, it should be underlined that accessibility to this type of platform is in any case subordinate to a certain level of IT knowledge and this may be a limitation of the study as people with low IT knowledge may not be attracted by this type of proposal.
The self-reporting data may also result in a limitation due to the risk of reliability of the measures, nonetheless participants’ performance during the tele-exercise sessions resulted generally aligned with the pre-session evaluation and were checked and monitored by the instructors in both modes of training.
Finally, although economical for users and participants, the development of this type of platform could be expensive for the platform administrators in terms of development and management due to the need to ensure functionality and data security for participants. Therefore, the costs and benefits of using this type of platform should be evaluated in the long term (38).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics Committee of the University of Trás-os-Montes & Alto Douro protocol Doc73-CE-UTAD-2019 (13/01/2020). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
AlF: Conceptualization, Project administration, Writing – original draft, Writing – review & editing. GZ: Formal Analysis, Writing – original draft. AnF: Data curation, Supervision, Writing – review & editing. NG: Resources, Validation, Writing – review & editing. VR: Funding acquisition, Validation, Writing – review & editing. JV-A: Resources, Validation, Writing – review & editing. MS: Visualization, Writing – review & editing. BM: Formal Analysis, Visualization, Writing – original draft. RP: Investigation, Validation, Writing – review & editing. PP: Resources, Validation, Writing – review & editing. AA: Writing – review & editing. AD: Supervision, Validation, Writing – review & editing. CB: Supervision, Validation, Writing – review & editing. FM: Conceptualization, Funding acquisition, Writing – original draft. EI: Conceptualization, Investigation, Project administration, Validation, Writing – review & editing. MC: Conceptualization, Formal Analysis, Project administration, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the European Union, grant number: 101089869—TELEexe4ALL— ERASMUS-SPORT-2022-SCP. The views and opinions expressed are, however, those of the author(s) only and do not necessarily reflect those of the European Union or the European Education and Culture Executive Agency (EACEA). Neither the European Union nor EACEA can be held responsible for them. Nuno Garrido, Victor Machado Reis, Rafael Peixoto and José Vilaça-Alves were also funded by the Portuguese Foundation for Science and Technology (FCT), IP., project number UIDB/04045/2020. This study has been designed and conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ethics Committee of the University of Trás-os-Montes & Alto Douro protocol Doc73-CE-UTAD-2019 (13/01/2020). An online informed consent was obtained from all participants. Personal data of the participants was collected and treated in accordance with the current European Union regulation on the protection of personal data.
We wish to thank APG Progetto Giovani for devising the platform. We also wish to acknowledge the effort of Alessandra Varone in the data entry.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Stoumpos AI, Kitsios F, Talias MA. Digital transformation in healthcare: technology acceptance and its applications. Int J Environ Res Public Health. (2023) 20(4):3407. doi: 10.3390/ijerph20043407
2. Li S, Li Y, Liang Q, Yang WJ, Zi R, Wu X, et al. Effects of tele-exercise rehabilitation intervention on women at high risk of osteoporotic fractures: study protocol for a randomised controlled trial. BMJ open. (2022) 12(11):e064328. doi: 10.1136/bmjopen-2022-064328
3. Smith AC, Thomas E, Snoswell CL, Haydon H, Mehrotra A, Clemensen J, et al. Telehealth for global emergencies: implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. (2020) 26(5):309–13. doi: 10.1177/1357633X20916567
4. Stavrou VT, Astara K, Ioannidis P, Vavougios GD, Daniil Z, Gourgoulianis KI. Tele-exercise in non-hospitalized versus hospitalized post-COVID-19 patients. Sports (Basel). (2022) 10(11):179. doi: 10.3390/sports10110179
5. Fabbrizio A, Macaluso F. Internet of medical things (IOMT) and integrated home assistance. Euromediterranean Biomed J. (2021) 16:78–9. doi: 10.3269/1970-5492.2021.16.18
6. Rodríguez MÁ, Crespo I, Del Valle M, Olmedillas H. Home-based vigorous tele-exercise in people with Parkinson’s disease: feasibility beyond complexity. J Parkinsons Dis. (2021) 11(2):843–5. doi: 10.3233/JPD-212541
7. Baehr LA, Kaimal G, Bruneau M Jr, Finley M. Development and feasibility of a group tele-exercise program for individuals with spinal cord injury. J Neurol Phys Ther. (2023) 47(4):200–7. doi: 10.1097/NPT.0000000000000449
8. Kim Y, Mehta T, Tracy T, Young HJ, Pekmezi DW, Rimmer JH, et al. A qualitative evaluation of a clinic versus home exercise rehabilitation program for adults with multiple sclerosis: the tele-exercise and multiple sclerosis (TEAMS) study. Disabil Health J. (2023) 16(3):101437. doi: 10.1016/j.dhjo.2022.101437
9. Lai B, Bond K, Kim Y, Barstow B, Jovanov E, Bickel CS. Exploring the uptake and implementation of tele-monitored home-exercise programs in adults with Parkinson’s disease: a mixed-methods pilot study. J Telemed Telecare. (2020) 26(1-2):53–63. doi: 10.1177/1357633X18794315
10. Marios TA, Smart N, Dalton S. The effect of tele-monitoring on exercise training adherence, functional capacity, quality of life and glycemic control in patients with type II diabetes. J Sports Sci Med. (2012) 11(1):51–6.24137063
11. Stephenson A, Howes S, Murphy PJ, Deutsch JE, Stokes M, Pedlow K, et al. Factors influencing the delivery of telerehabilitation for stroke: a systematic review. PLoS One. (2022) 17(5):e0265828. doi: 10.1371/journal.pone.0265828
12. Gomes Costa RR, Dorneles JR, Veloso JHCL, Gonçalves CWP, Ribeiro Neto F. Does tele-exercise training for tetraplegia meet the spinal cord injury-specific physical activity guidelines? A 7-month longitudinal study. J Telemed Telecare. (2023) 15:1357633X231188989. doi: 10.1177/1357633X231188989
13. Sankaran S, Dendale P, Coninx K. Evaluating the impact of the HeartHab app on motivation, physical activity, quality of life, and risk factors of coronary artery disease patients: multidisciplinary crossover study. JMIR Mhealth Uhealth. (2019) 7(4):e10874. doi: 10.2196/10874
14. Wu GE, Keyes LM. Group tele-exercise for improving balance in elders. Telemedicine and e-Health. (2006) 12(5):561–70. doi: 10.1089/tmj.2006.12.561
15. Mosca IE, Salvadori E, Gerli F, Fabbri L, Pancani S, Lucidi G, et al. Analysis of feasibility, adherence, and appreciation of a newly developed tele-rehabilitation program for people with MCI and VCI. Front Neurol. (2020) 27(11):583368. doi: 10.3389/fneur.2020.583368
16. Zengin Alpozgen A, Kardes K, Acikbas E, Demirhan F, Sagir K, Avcil E. The effectiveness of synchronous tele-exercise to maintain the physical fitness, quality of life, and mood of older people—a randomized and controlled study. Eur Geriatr Med. (2022) 13(5):1177–85. doi: 10.1007/s41999-022-00672-y
17. De Giorgio A, Kuvačić G, Milić M, Padulo J. The brain and movement: how physical activity affects the brain. MJSSM. (2018) 7(2):63–8. doi: 10.26773/mjssm.180910
18. Hraste M, De Giorgio A, Jelaska PM, Padulo J, Granić I. When mathematics meets physical activity in the school-aged child: the effect of an integrated motor and cognitive approach to learning geometry. PLoS One. (2018) 13(8):e0196024. doi: 10.1371/journal.pone.0196024
19. Kahraman T, Savci S, Ozdogar AT, Gedik Z, Idiman E. Physical, cognitive and psychosocial effects of telerehabilitation-based motor imagery training in people with multiple sclerosis: a randomized controlled pilot trial. J Telemed Telecare. (2020) 26(5):251–60. doi: 10.1177/1357633X18822355
20. Kuvačić G, Fratini P, Padulo J, Antonio DI, De Giorgio A. Effectiveness of yoga and educational intervention on disability, anxiety, depression, and pain in people with CLBP: a randomized controlled trial. Complement Ther Clin Pract. (2018) 31:262–7. doi: 10.1016/j.ctcp.2018.03.008
21. De Giorgio A, Padulo J, Kuvačić G. Effectiveness of yoga combined with back school program on anxiety, kinesiophobia and pain in people with non-specific chronic low back pain: a prospective randomized trial. MLTJ. (2019) 08(01):104. doi: 10.32098/mltj.01.2018.13
22. Wilke J, Mohr L, Yuki G, Bhundoo AK, Jiménez-Pavón D, Laiño F, et al. Train at home, but not alone: a randomised controlled multicentre trial assessing the effects of live-streamed tele-exercise during COVID-19-related lockdowns. Br J Sports Med. (2022) 56(12):667–75. doi: 10.1136/bjsports-2021-104994
23. Fabbrizio A, Fucarino A, Cantoia M, De Giorgio A, Garrido ND, Iuliano E, et al. Smart devices for health and wellness applied to tele-exercise: an overview of new trends and technologies such as IoT and AI. Healthcare (Basel, Switzerland). (2023) 11(12):1805. doi: 10.3390/healthcare11121805
24. Available online at: https://github.com/topics/telehealth (accessed September 05, 2024).
25. https://www.nike.com/it/ntc-app (accessed September 05, 2024).
26. https://ecqi.healthit.gov/fhir (accessed September 05, 2024).
27. https://www.jefit.com (accessed September 05, 2024).
28. Saran T, Pedrycz A, Mucha D, Mucha D. Follow-up monitoring of physical activity after rehabilitation by means of a mobile application: effectiveness of measurements in different age groups. Adv Clin Exp Med. (2018) 27(8):1037–44. doi: 10.17219/acem/69131
29. Fucarino A, Fabbrizio A, Garrido ND, Iuliano E, Reis VM, Sausa M, et al. Emerging technologies and open-source platforms for remote physical exercise: innovations and opportunities for healthy population-A narrative review. Healthcare (Basel). (2024) 12(15):1466. doi: 10.3390/healthcare12151466
30. Domínguez-Muñoz A, Carlos-Vivas J, Barrios-Fernandez S, Adsuar JC, Morenas-Martín J, Garcia-Gordillo MA, et al. Pedagogical proposal of tele-exercise based on “square stepping exercise” in preschoolers: study protocol. Int J Environ Res Public Health. (2021) 18:16. doi: 10.3390/ijerph18168649
31. Dagenais M, Parker O, Galway S, Gammage K. Online exercise programming among older adults: a scoping review. J Aging Phys Act. (2022) 31(2):289–302. doi: 10.1123/japa.2021-0417
32. Lagera PGD, Chan SR, Yellowlees PM. Asynchronous technologies in mental health care and education. Curr Treat Options Psychiatry. (2023) 10:59–71. doi: 10.1007/s40501-023-00286-6
33. Ruchi D, Saloni M, Ramesh K, Indrajeet S, Sunil K, Anissa MA, et al. Effect of teleyoga before COVID-19 and during pandemic: a narrative review. Recent Adv Anti-Infect Drug Discov. (2023) 18(3):178–87. doi: 10.2174/2772434418666230223104608
34. Available online at: https://www.teleexe4all.eu/ (accessed September 05, 2024).
35. Borg G. Borg’s Pperceived Eexertion and Ppain Sscales. Champaign, IL, USA: Human kinetics (1998).
37. McArdle WD, Katch FI, Katch VL, et al. Training muscles to become stronger. In: McArdle WD, editor. Essentials of Exercise Physiology 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins (2010). 22. p. 490–528.
38. Lemmink KAPM, Kemper HC, de Greef MH, Rispens P, Stevens M. The validity of the sit-and-reach test and the modified sit-and-reach test in middle-aged to older men and women. Res Q Exerc Sport. (2003) 74(3):331–6. doi: 10.1080/02701367.2003.10609099
39. Mayorga-Vega D, Merino-Marban R, Viciana J. Criterion-related validity of sit-and-reach tests for estimating hamstring and lumbar extensibility: a meta-analysis. J Sports Sci Med. (2014) 13:1–14.24570599
40. Mackenzie B. (2005). Squats Test. Available online at: https://www.brianmac.co.uk/squatest.htm (accessed September 05, 2024).
41. Cohen S, Williamson G. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, editors. The Social Psychology of Health: Claremont Symposium on Applied Social Psychology. Newbury Park, CA: SAGE Publications, Inc. (1988). p. 31–67.
42. Mondo M, Sechi C, Cabras C. Psychometric evaluation of three versions of the Italian perceived stress scale. Curr Psychol. (2021) 40:1884–92. doi: 10.1007/s12144-019-0132-8
43. Sischka P, Costa A, Steffgen G, Schmidt AF. The WHO-5 well-being index—validation based on item response theory and the analysis of measurement invariance across 35 countries. J Affect Disord. (2020) 1:100020. doi: 10.1016/j.jadr.2020.100020
44. Grossi E, Groth N, Mosconi P, Cerutti R, Pace F, Compare A, et al. Development and validation of the short version of the psychological general well-being Index (PGWB-S). HRQOL. (2006) 4:88. doi: 10.1186/1477-7525-488
45. Likert R. A technique for the measurement of attitudes. Archives of Psychology. (1932) 140:1–55.
46. Hong J, Kim J, Kim SW, Kong HJ. Effects of home-based tele-exercise on sarcopenia among community-dwelling elderly adults: body composition and functional fitness. Exp Gerontol. (2017) 87:33–9. doi: 10.1016/j.exger.2016.11.002
47. Giordano A, Bonometti GP, Vanoglio F, Paneroni M, Bernocchi P, Comini L, et al. Feasibility and cost-effectiveness of a multidisciplinary home-telehealth intervention programme to reduce falls among elderly discharged from hospital: study protocol for a randomized controlled trial. BMC Geriatr. (2016) 16(1):209. doi: 10.1186/s12877-016-0378-z
48. Stavrou VT, Astara K, Ioannidis P, Vavougios GD, Daniil Z, Gourgoulianis KI. Tele-exercise in non-hospitalized versus hospitalized post-COVID-19 Patients. Sports (Basel). (2022) 10(11):179. doi: 10.3390/sports10110179
49. Schneider V, Kale D, Herbec A, Beard E, Fisher A, Shahab L. UK Adults’ exercise locations, use of digital programs, and associations with physical activity during the COVID-19 pandemic: longitudinal analysis of data from the health behaviours during the COVID-19 pandemic study. JMIR Form Res. (2022) 6(6):e35021. doi: 10.2196/35021
50. Lin II, Chen YL, Chuang LL. Test-Retest reliability of home-based fitness assessments using a Mobile app (R plus health) in healthy adults: prospective quantitative study. JMIR Form Res. (2021) 5(12):e28040. doi: 10.2196/28040
51. Lavín-Pérez AM, León-Llamas JL, Salas Costilla FJ, Collado-Mateo D, López de Las Heras R, Gasque Celma P, et al. Validity of on-line supervised fitness tests in people with low back pain. Healthcare (Basel). (2023) 11(7):1019. doi: 10.3390/healthcare11071019
52. Gu J, Tong X, Meng S, Xu S, Huang J. Remote cardiac rehabilitation program during the COVID-19 pandemic for patients with stable coronary artery disease after percutaneous coronary intervention: a prospective cohort study. BMC Sports Sci Med Rehabil. (2023) 15(1):79. doi: 10.1186/s13102-023-00688-2
53. Zimatore G, Falcioni L, Gallotta MC, Bonavolontà V, Campanella M, De Spirito M, et al. Recurrence quantification analysis of heart rate variability to detect both ventilatory thresholds. PLoS One. (2021) 16(10):e0249504. doi: 10.1371/journal.pone.0249504
54. Zimatore G, Gallotta MC, Campanella M, Skarzynski PH, Maulucci G, Serantoni C, et al. Etecting metabolic thresholds from nonlinear analysis of heart rate time series. A review. Int J Environ Res Public Health. (2022) 19(19):12719. doi: 10.3390/ijerph191912719
55. Bayles MP. CSM’s Exercise Testing and Prescription. Philadelphia (USA): Lippincott Williams & Wilkins (2023).
56. Amorese AJ, Ryan AS. Home-based tele-exercise in musculoskeletal conditions and chronic disease: a literature review. Front Rehabil Sci. (2022) 24(3):811465. doi: 10.3389/fresc.2022.811465
57. Cuccia F, Mortellaro G, Trapani G, Valenti V, Ognibene L, De Gregorio G, et al. Acute and late toxicity and preliminary outcomes report of moderately hypofractionated helical tomotherapy for localized prostate cancer: a mono-institutional analysis. Radiol Med. (2020) 125(2):220–7. doi: 10.1007/s11547-019-01095-9
58. Cuccia F, Fiorentino A, Corrao S, Mortellaro G, Valenti V, Tripoli A, et al. Moderate hypofractionated helical tomotherapy for prostate cancer in a cohort of older patients: a mono-institutional report of toxicity and clinical outcomes. Aging Clin Exp Res. (2020) 32(4):747–53. doi: 10.1007/s40520-019-01243-1
59. Chan KOW, Yuen PP, Fong BYF, Law VTS, Ng FSF, Fung WCP, et al. Effectiveness of telehealth in preventive care: a study protocol for a randomised controlled trial of tele-exercise programme involving older people with possible sarcopenia or at risk of fall. BMC Geriatr. (2023) 23(1):845. doi: 10.1186/s12877-023-04535-4
60. Yoo I, Kong HJ, Joo H, Choi Y, Kim SW, Lee KE, et al. User experience of augmented reality glasses-based tele-exercise in elderly women. Healthc Inform Res. (2023) 29(2):161–7. doi: 10.4258/hir.2023.29.2.161
61. Stonsaovapak C, Sangveraphunsiri V, Jitpugdee W, Piravej K. Telerehabilitation in older Thai community-dwelling adults. Life (Basel). (2022) 12(12):2029. doi: 10.3390/life12122029
Keywords: tele-exercise, physical fitness, psychological well-being, healthy populations, lifestyle behaviors
Citation: Fucarino A, Zimatore G, Fabbrizio A, Garrido ND, Reis VM, Vilaça-Alves J, Sausa M, Matteo B, Peixoto R, Perušina P, Aristova A, De Giorgio A, Baldari C, Macaluso F, Iuliano E and Cantoia M (2024) Fitness and psychological effects of tele-exercise in healthy populations. Preliminary study. Front. Digit. Health 6:1496196. doi: 10.3389/fdgth.2024.1496196
Received: 13 September 2024; Accepted: 11 October 2024;
Published: 12 November 2024.
Edited by:
Pradeep Nair, Central University of Himachal Pradesh, IndiaReviewed by:
Jennifer A. Bunn, Sam Houston State University, United StatesCopyright: © 2024 Fucarino, Zimatore, Fabbrizio, Garrido, Reis, Vilaça-Alves, Sausa, Matteo, Peixoto, Perušina, Aristova, De Giorgio, Baldari, Macaluso, Iuliano and Cantoia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Filippo Macaluso, ZmlsaXBwby5tYWNhbHVzb0B1bmlwYS5pdA==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.