 Mequannent Sharew Melaku
Mequannent Sharew Melaku Lamrot Yohannes
Lamrot Yohannes- 1Department of Health Informatics, Institute of Public Health, University of Gondar, Gondar, Ethiopia
- 2Department of Environmental and Occupational Health and Safety, Institute of Public Health, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Introduction: Generating quality data for decision-making at all levels of a health system is a global imperative. The assessment of the Ethiopian National Health Information System revealed that health information system resources, data management, dissemination, and their use were rated as “not adequate” among the six major components of the health system. Health extension workers are the frontline health workforce where baseline health data are generated in the Ethiopian health system. However, the data collected, compiled, and reported by health extension workers are unreliable and of low quality. Despite huge problems in data management practices, there is a lack of sound evidence on how to overcome these health data management challenges, particularly among health extension workers. Thus, this study aimed to assess data management practices and their associated factors among health extension workers in the Central Gondar Zone.
Method: An institution-based cross-sectional study was conducted among 383 health extension workers. A simple random sampling method was used to select districts, all health extension workers were surveyed in the selected districts, and a structured self-administered questionnaire was used for data collection. The data was entered using EpiData version 4.6 and analyzed using STATA, version 16. Bivariable and multivariable binary logistic regression analyses were executed. An odds ratio with a 95% confidence interval and a p-value of <0.05 was calculated to determine the strength of the association and to evaluate statistical significance, respectively.
Results: Of the 383 health extension workers enrolled, all responded to the questionnaire with a response rate of 100%. Furthermore, 54.7% of the respondents had good data management practices. In the multivariable logistic regression analysis, being a married woman, having good data management knowledge, having a good attitude toward data management, having 1–5 years of working experience, and having a salary ranging from 5,358 to 8,013 Ethiopian Birr were the factors significantly associated with good data management practices among health extension workers. The overall data management practice was poor with only five health extension workers out of ten having good data management practices.
1 Introduction
Healthcare information is important for effective clinical and managerial decision-making at different levels of a health system (1–3). A health information system (HIS) is one of the essential building blocks of a health system aimed at producing valid health knowledge to support clinical, public health, and management decision-making. Data management is one of the six components of HIS and it is defined as the effective coordination of people, materials, and procedures to gather, process, compile, and interpret data, and display the results using a table or graph for evidence-based decision-making. It is a system that provides the accurate, reliable, valid, and timely information necessary for the improvement of public health services, requiring effectiveness and efficiency through better management of data at all levels of implementation (2).
Health information systems in most of the world are inadequate and do not provide the needed managerial support (4–6). Globally, the majority of health facilities either do not submit any health reports or have no standardized format. This in turn creates problems in drawing inferences for managerial decision-making (7). Furthermore, data received from many health facilities are incomplete, inaccurate, and unrelated to the priority tasks and functions of local health personnel (4, 7).
Most health systems in developing countries have inadequate information systems with endless registers and sending out reports without receiving any feedback (1, 8). The HISs in most developing countries are inefficient, poor in quality, and are greatly affected by data unreliability resulting from inadequate collection and poor aggregation and analyses (9). Reports from sub-Saharan Africa indicate that vital health decisions are made based on crude estimates of disease and treatment burdens (9, 10).
The evidence consistently shows that poor data management significantly hinders health outcomes and decision-making processes at all levels, ranging from missed diagnoses at the patient level to inefficient resource allocation in hospitals and poor national-level health policies. The poor data management practices of healthcare professionals and health extension workers (HEWs) affect health outcomes and decision-making processes at all levels of the healthcare system. The impact of poor data management skills starts in individual healthcare and extends to the national level. At the individual level, it affects continuity of care, produces inaccurate and incomplete data, and leads to incorrect diagnoses and treatment, which in turn leads to death or lifelong complications for the individual (11–14). More importantly, poor data management skills significantly impact healthcare organizations by leading to the inefficient allocation of resources such as staff, medications, and equipment, hindering the effective monitoring of health facility performance and leading to a lack of accountability and underperformance in health outcomes. Without reliable data, facilities cannot measure key performance indicators (KPIs) (15–17). Finally, poor healthcare data management impacts national-level decisions. At the national level, it leads to flawed national health policies, as decision-makers lack the necessary evidence to guide policy formulation and intervention strategies. In addition, poor data management hinders effective responses to health emergencies, such as disease outbreaks (18–20).
In Ethiopia, the impact of poor data management on health outcomes and decision-making processes at all levels is described in the literature (21–25).
HEWs are the frontline health workforce where baseline health data are generated in the Ethiopian health system (26). However, the data collected, compiled, and reported by HEWs are unreliable and of low quality (27, 28). The Community Health Information System (CHIS) is the health information system in which community health workers/HEWs practice data management (10, 29). In Ethiopia, data quality and use remain weak, particularly among health extension workers. An assessment by the Ethiopian National Health Information System indicated that health information system resources, and data management, dissemination, and use were rated as “not adequate” among the six major components of the health system. Several HIS issues arise from the poor data management practices of health extension workers.
Several studies conducted across the world identified several factors that contribute to the quality of data management practices of healthcare professionals (30–32). Evidence shows that the HIS of Ethiopia is of low quality and is affected by a lack of knowledge, practice, and insufficient analysis skills among the health workers (1, 33–37).
Despite these issues, there is a lack of sound evidence on how to overcome these health data management challenges. Therefore, assessing the data management practices of HEWs could be a valuable resource to combat these challenges. Moreover, having information about the factors affecting the data management practices of HEWs is the primary step and base for the improvement of the CHIS, the Health Management Information System (HMIS), and overall health system performance. Thus, the aim of this study was to assess data management practices and their associated factors among HEWs in the Central Gondar Zone.
2 Methods
2.1 Study area
This study was conducted in the Central Gondar Zone in the Amhara Region. Gondar is the capital city of the Central Gondar Zone and is located 173 km from Bahir Dar and 658 km from Addis Ababa. It is divided into 19 administrative districts (4 urban and 15 rural). According to a planning and program report in the Central Gondar Zone, the total projected population is 2,370,377 of which 1,180,448 are men and 1,189,929 are women. There are 9 public hospitals, 76 public health centers, and 404 health posts. There are 940 health extension workers working in these health posts.
2.2 Study design and period
A facility-based cross-sectional quantitative study was conducted from 5 to 15 September 2021 in the Central Gondar Zone.
2.3 Source and study population
The source population was all health extension workers who were working in all the districts in the Central Gondar Zone. The study population was all health extension workers currently working in the selected woredas in the Central Gondar Zone. All health extension workers who were currently working during the study period in the selected districts in the Central Gondar Zone were included and health extension workers who were seriously ill and unable to understand the purpose of the study or who were absent during the data collection period were excluded from the study.
2.4 Sample size determination and sampling procedure
The sample size was calculated using the single population proportion formula, n = Z(α/2)2 · pq/d2. We assumed: n = the required sample size; Z = the value of standard normal distribution corresponding to α/2, 1.96; p = proportion of health extension workers who have good data management practices, 53% (considering previous study conducted in East Gojjam Zone); q = proportion of health extension workers who have poor data management practices, 47%; and d = precision, 0.05. Hence, the required sample size was calculated to be 384. After adding a 10% non-response rate, a total of 423 samples was determined. However, the total number of health extension workers in the selected five districts was 383, thus we considered 383 participants for the entire analysis. The cluster sampling technique was used to select the district to be sampled. Accordingly, 5 out of 15 districts (33%) were selected using a simple random sampling technique. The selected districts were East Dembia (91), Gondar Zuria (130), West Dembia (55), Takusa (85), and the Wogera district (60). As the total number of health extension workers was less than the sample size we calculated, we included all the health extension workers in these districts.
2.5 Study variables
The outcome variable, data management practices, was assessed using 11 questions (38, 39). HEWs who scored above the median score were considered to have good data management practices. HEWs who scored below the median score were considered to have poor data management practices.
The independent variables considered for this study were categorized as follows: sociodemographic characteristics of the HEWs including age, educational status, marital status, work experience, salary, and position; behavioral factors including attitude toward data management practices and knowledge of data management practices; organizational factors including the availability of resources, governance, training, finance, transportation, reference material access, and supportive supervision; and technical factors that affect data management practices including the complexity of data collection tools, the complexity of the report format, and the presence of daily activity challenges.
2.6 Data collection tool and quality control
A self-administered, organized, and pre-tested questionnaire was created in English. The data collection process included five supervisors and 20 data collectors. A 3-day training course was provided for the data collectors and a pre-test was conducted outside the study area in West Gondar Zone (Metemma woreda) with a sample size of 10% of the sample of health extension workers in the main study (i.e., 39 health extension workers in Metemma woreda). The validity and reliability of the data collection instrument were assessed using the results of the pre-test. Based on the pre-test results and feedback from area experts, the content of the questionnaire was modified for clarity. Cronbach's alpha reliability test was conducted. A Cronbach's alpha result of 0.71 revealed that the tool was internally consistent and reliable.
2.7 Data processing and analysis
Data entry was performed using the EpiData version 4.6 software package and was analyzed using STATA version 16 software. Descriptive statistics were computed to describe the sociodemographic variables. Bivariable and multivariable binary logistic regression analyses were conducted to measure the association between the dependent and independent variables. Variables with a p-value less than 0.2 in the bivariable regression analysis were included in the multivariable regression analysis. Multivariable binary logistic regression analysis was conducted to determine the variables significantly associated with the data management practices of health extension workers. The enter method for multivariable binary logistic regression analysis was used to control for the confounding effects of the independent variables. Odds ratios with a 95% confidence level and p-value at <0.05 were calculated to ascertain the strength of the association and to indicate statistical significance, respectively. Prior to conducting the logistic regression model, assumptions of multi-collinearity were checked. Furthermore, the multivariable binary logistic regression was fitted using the Hosmer–Lemeshow goodness of fit test.
2.8 Ethical consideration
Ethical clearance for this research was obtained from the Institute of Public Health Research Review Ethics Committee at the University of Gondar. A supporting letter was also obtained from the Central Gondar Zonal Health Department. Official letters of cooperation were received from the respective woredas and local health posts. During the data collection, confidentiality and privacy were assured by maintaining the anonymity of participants. Written consent was given by each health professional. The health professionals participated voluntarily and could withdraw from the study at any time if they were not happy with the survey.
3 Results
3.1 Sociodemographic characteristics of the respondents
Of the 383 participants, all responded to the questionnaire with a response rate of 100%. The mean age of the study participants was 29 years and 84.6% of the respondents were level IV HEWs (Table 1).
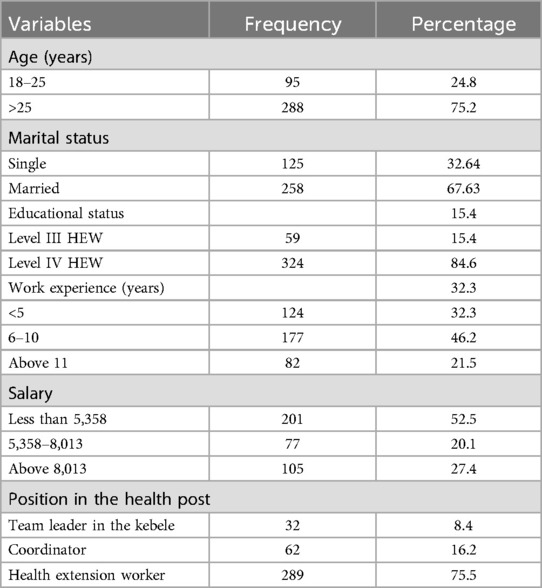
Table 1. Sociodemographic characteristics of the health extension workers in the Central Gondar Zone, north Ethiopia, in 2021.
3.2 Knowledge of data management practices
In total, 320 (83.6%) of the HEWs knew that data management is a procedure that includes data collection and registration. Furthermore, 329 (85.9%) HEWs used data for planning, decision-making, and prevention of disease. The majority of the HEWs, 256 (66.8%), knew to register and tally routine activities reports as a source of data, and 191 (49.9%) and 249 (65%) HEWs knew to ensure accuracy and completeness in data/reports, respectively. Finally, 57% and 49.9% percent of health extension workers had good knowledge of and a good attitude toward data management practices, respectively (Figure 1).
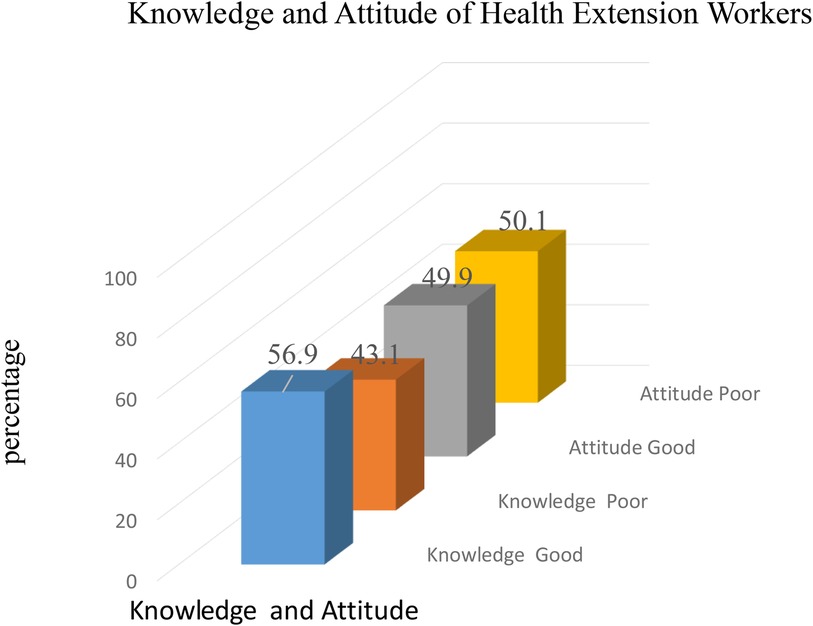
Figure 1. Level of data management knowledge and attitudes among HEWs in the Central Gondar Zone, north Ethiopia.
3.3 Data management practices of health extension workers
Only 203 (53%) of the HEWs practiced CHIS in their health post according to the required standard. A majority, 291 (76%), correctly registered their daily activities and 246 (64.2%) HEWs used the collected data after converting it into usable information or a report. Finally, 54.3% of the health extension workers had good data management practices (Figure 2).

Figure 2. Level of data management practices among health extension workers in the Central Gondar Zone, northwest Ethiopia.
3.4 Technical characteristics of health extension workers
In total, 311 (81.2%) HEWs reported that the registration books, reporting formats, and CHIS materials were easy and simple for them to understand. A majority, 90.9%, responded that they were being challenged by their daily activities (Table 2).
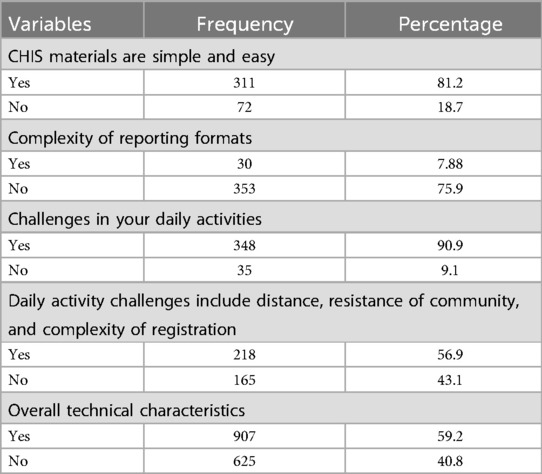
Table 2. Technical characteristics related to data management practices in the Central Gondar Zone, northwest Ethiopia, in 2021.
3.5 Organizational characteristics of the health extension workers
In total, 310 (80.9%) HEWs had training on data collection, processing, and handling practices, 66 (17.2%) respondents did not have reference material for data management practices in their office, 325 (84.9%) had been supplied with field books, and 315 (82.2%) HEWs had obtained stationery from their respective health office/health center (Table 3).
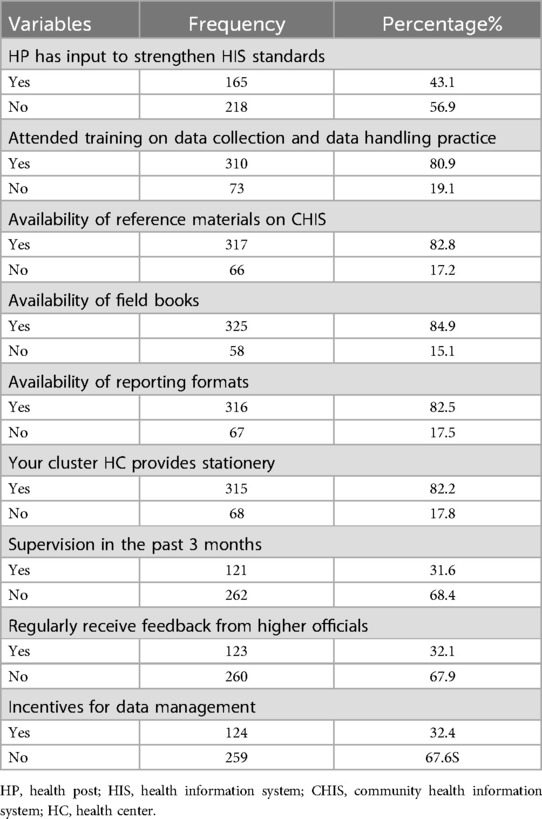
Table 3. Organizational characteristics related to data management practices in the Central Gondar Zone, Northwest Ethiopia, in 2021.
3.6 Factors associated with data management practice
The multivariable logistic regression analysis identified the significant factors associated with data management practice. Accordingly, the respondent's attitude, knowledge, work experience, salary, and marital status were significantly associated with their data management practices. Married women were nearly six times (adjusted odd ratio (AOR) = 6, 95% CI = 2.82–12.14) more likely to have good data management practices compared to unmarried women. Health extension workers who had good knowledge of data management practices were 4.7 times more likely to practice good data management (AOR = 4.7, 95% CI = 2.49–8.70). Health extension workers who had a good attitude toward data management practices were six times more likely to have good data management practices (AOR = 6.2, 95% CI = 3.34–11.32). Health extension workers who had 1–5 years of working experience were more likely to have good data management practices (AOR = 4, 95% CI = 1.25–10.5) compared to HEWs who had more than 10 years of working experience. Health extension workers whose monthly income was 5,358–8,013 Ethiopian Birr were 2.7 times more likely to have good data management practices than those who had a monthly salary of less than 5,358 Ethiopian Birr (AOR = 2.7, 95% CI = 1.23–5.95) (Table 4).
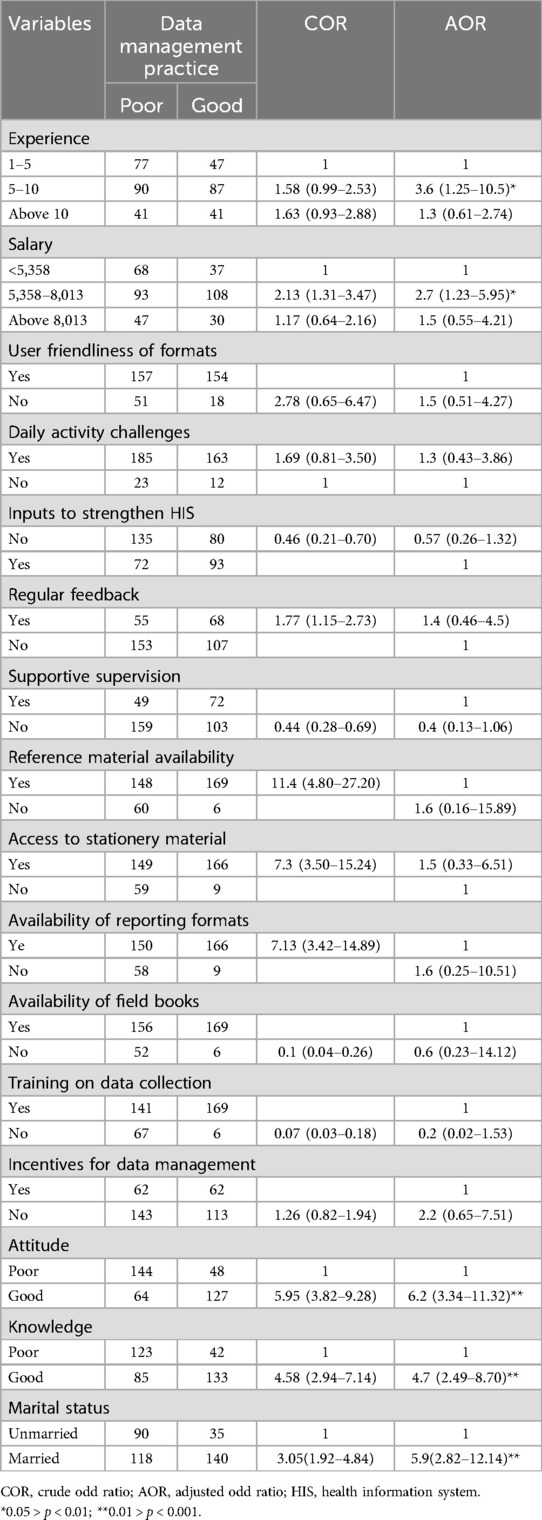
Table 4. Factors associated with data management practices among health extension workers in the Central Gondar Zone, North Ethiopia, in 2021.
4 Discussion
Primary healthcare units are major sources of routine healthcare data for the Ethiopian health system since they are in rural settings where approximately 85% of the country's population lives. Healthcare information is important for effective clinical and managerial decision-making at different levels of the healthcare system. Hence, the primary focus of this study was to determine the data management practices of HEWs and their determinant factors.
In this study, only 54.3% of the HEWs had good data management practices. Thus, this could severely affect the decision-making practices of the Ethiopian health system in terms of resource allocation, planning, service quality, and equity. This finding is in line with a study conducted in the East Gojam Zone (38, 39) while it was lower than a study’s finding from Southern Ethiopia (34), in which three-quarters of HEWs had good data management practices. However, the finding of this study is higher compared to another study’s findings in Ethiopia and Palestine (40). This inconsistency is due to differences in data management knowledge such as supervision, study time, community type, and regular feedback. Furthermore, the finding of this study is contrary to a task analysis study conducted in Ethiopia (41), where 97% of the health extension workers perceived themselves to be competent and proficient in performing tasks in all program areas. The wide discrepancy between their data management performance and perception might be due to health extension workers reporting that they do not receive consistent feedback. If there were appropriate and timely feedback, they might understand their performance level better.
The respondent's attitude, knowledge, work experience, salary, and marital status were significantly associated with their data management practices in the Central Gondar Zone.
HEWs who had good data management knowledge were more likely to have good data management practices compared to HEWs who had poor data management knowledge (AOR = 4.7, 95% CI = 2.49–8.70). This finding is supported by different studies conducted in Ethiopia (30, 34, 42, 43) and abroad (44). It is indisputable that good data management knowledge is a prerequisite for good data management practice.
Similarly, HEWs who had a good attitude toward data management practices were six times (AOR = 6, 95% CI = 3.34–11.32) more likely to handle data effectively compared to HEWs who had a poor attitude. Various studies support this finding (8, 21, 26). Thus, attitude is a key factor in the data management practices of HEWs as those who have a good attitude toward data management practices work harder to improve the quality of data and data management practices in their organization.
Married HEWs were nearly six times (AOR = 6, 95% CI = 2.82–12.14) more likely to have good data management practices compared to unmarried HEWs. This could be due to marriage being a key determinant factor for commitment since it is the first step to taking responsibility. Thus, women who are engaged or married have data management practices.
Health extension workers who had 1–5 years of working experience were more likely to have good data management practices (AOR = 4, 95% CI = 1.25–10.5) compared to HEWs who had more than 10 years of working experience. This might be because health extension workers who are more experienced may overwhelmed by the activities they have handled for a long period of time and they may be unmotivated by their lifestyle and working environment.
Finally, health extension workers who had a monthly income of 5,358–8,013 Ethiopian Birr had better data management practices than those who had a monthly salary of less than 5,358 Ethiopian Birr (AOR = 2.7, 95% CI = 1.23–5.95). This could be because a better salary raises a HEW’s motivation to adhere to good data management practices.
5 Conclusion
Overall, data management practices were poor with only 54.3% of respondents having good data management practices. Having a good knowledge of data management, availability of field books and registration books, and the understandability of the existing CHIS forms and materials were predictors of good data management practices. The Amhara Regional Health Bureau, in collaboration with Federal Ministry of Health (FMoH), needs to make HMIS/CHIS formats and field notebooks available to health posts. Access to regular data management training and data management information resources for HEWs is also required.
5.1 Limitations of the study
The study was not adequately supported by qualitative data. Determining data management knowledge and practice using the median score of knowledge and practice questions may also be a limitation of this study. Furthermore, limited geographic scope, self-reporting bias, a short study period, and the exclusion of health extension workers who are unable to read were limitations of this study.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical clearance of this research was obtained from the department of health informatics at University of Gondar. During the data collection, the issue of confidentiality and privacy was assured by maintaining the anonymity of participants. Written consent was taken from each health extension workers. Health extension workers who were not voluntary and participants can withdraw from the study at any time if they were unable to complete the survey.
Author contributions
MM: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. LY: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to acknowledge the University of Gondar for providing us with this opportunity to conduct this study. We would like to extend our heartfelt appreciation to our families for their unreserved support, advice, and encouragement throughout our life and work period. We would like to forward our thanks and appreciation to the Central Gondar Zonal Health Department for their unreserved support in giving information about the Zone and its population profile. Acknowledgment also goes to ChatGPT-4.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
HIMS, health information management system; HP, health post; HIS, health information system; KPI, key performance indicators; HEW, health extension worker; CHIS, community health information system; HC, health center; COR, crude odd ratio; AOR, adjusted odd ratio; FMoH, Federal Ministry of Health.
References
1. Mengiste SA. Analysing the challenges of IS implementation in public health institutions of a developing country: the need for flexible strategies. J Health Inform Dev Ctries. (2010) 4(1):1–17.
2. World Health Organization. Health Information Systems: Toolkit on Monitoring Health Systems Strengthening. Geneva: WHO (2008).
3. AbouZahr C, Boerma T. Health information systems: the foundations of public health. Bull W H O. (2005) 83:578–83.16184276
4. Allotey PA, Reidpath D. Information quality in a remote rural maternity unit in Ghana. Health Policy Plan. (2000) 15(2):170–6. doi: 10.1093/heapol/15.2.170
5. Mahmood S, Ayub M. Accuracy of primary health care statistics reported by community based lady health workers in district Lahore. JPMA J Pakistan Med Assoc. (2010) 60(8):649.20726196
6. De La Torre C, Unfried K. Monitoring and Evaluation at the Community Level: A Strategic Review of MEASURE Evaluation Phase III Accomplishments and Contributions. Chapel Hill, NC: MEASURE Evaluation (2014).
7. Makombe SD, Hochgesang M, Jahn A, Tweya H, Hedt B, Chuka S, et al. Assessing the quality of data aggregated by antiretroviral treatment clinics in Malawi. Bull W H O. (2008) 86:310–4. doi: 10.2471/BLT.07.044685
8. Chaulagai CN, Moyo CM, Koot J, Moyo HB, Sambakunsi TC, Khunga FM, et al. Design and implementation of a health management information system in Malawi: issues, innovations and results. Health Policy Plan. (2005) 20(6):375–84. doi: 10.1093/heapol/czi044
9. Nyamtema AS. Bridging the gaps in the health management information system in the context of a changing health sector. BMC Med Inform Decis Mak. (2010) 10(1):1–6. doi: 10.1186/1472-6947-10-36
10. Jeremie N, Kaseje D, Olayo R, Akinyi C. Utilization of community-based health information systems in decision making and health action in Nyalenda, Kisumu County, Kenya. Univ J Med Sci. (2014) 2(4):37–42. doi: 10.13189/ujmsj.2014.020401
11. Schneider EC, Ridgely MS, Meeker D, Hunter LE, Khodyakov D, Rudin RS. Promoting patient safety through effective health information technology risk management. Rand Health Quarterly. (2014) 4(3):1–61.28083315
12. Rudin RS, Motala A, Goldzweig CL, Shekelle PG. Usage and effect of health information exchange: a systematic review. Ann Intern Med. (2014) 161(11):803–11. doi: 10.7326/M14-0877
13. Menachemi N, Rahurkar S, Harle CA, Vest JR. The benefits of health information exchange: an updated systematic review. J Am Med Inform Assoc. (2018) 25(9):1259–65. doi: 10.1093/jamia/ocy035
14. Sadoughi F, Nasiri S, Ahmadi H. The impact of health information exchange on healthcare quality and cost-effectiveness: a systematic literature review. Comput Methods Programs Biomed. (2018) 161:209–32. doi: 10.1016/j.cmpb.2018.04.023
15. Sittig DF, Singh H. A new socio-technical model for studying health information technology in complex adaptive healthcare systems. In: Patel VL, Kannampallil TG, Kaufman DR, editors. Cognitive Informatics for Biomedicine Human Computer Interaction in Healthcare. Cham: Springer (2015). p. 59–80.
16. Beck LB. The role of outcomes data in health-care resource allocation. Ear Hear. (2000) 21(4):89S–96. doi: 10.1097/00003446-200008001-00011
17. Griffin S, Claxton K, Sculpher M. Decision analysis for resource allocation in health care. J Health Serv Res Policy. (2008) 13(3_suppl):23–30. doi: 10.1258/jhsrp.2008.008017
18. World Health Organization. Regional Strategy for Fostering Digital Health in the Eastern Mediterranean Region (2023–2027). World Health Organization, Regional Office for the Eastern Mediterranean (2022).
19. World Health Organization. Future of Digital Health Systems: Report on the WHO Symposium on the Future of Digital Health Systems in the European Region: Copenhagen, Denmark, 6–8 February 2019. Geneva: World Health Organization (2019).
20. Leerapan B, Teekasap P, Urwannachotima N, Jaichuen W, Chiangchaisakulthai K, Udomaksorn K, et al. System dynamics modelling of health workforce planning to address future challenges of Thailand’s universal health coverage. Hum Resour Health. (2021) 19:1–16. doi: 10.1186/s12960-020-00545-0
21. Tilahun B, Fritz F. Modeling antecedents of electronic medical record system implementation success in low-resource setting hospitals. BMC Med Inform Decis Mak. (2015) 15:1–9. doi: 10.1186/s12911-015-0192-0
22. Bauni E, Ndila C, Mochamah G, Nyutu G, Matata L, Ondieki C, et al. Validating physician-certified verbal autopsy and probabilistic modeling (InterVA) approaches to verbal autopsy interpretation using hospital causes of adult deaths. Popul Health Metr. (2011) 9:1–12. doi: 10.1186/1478-7954-9-49
23. Zenbaba D, Sahiledengle B, Debela MB, Tufa T, Teferu Z, Lette A, et al. Determinants of incomplete vaccination among children aged 12 to 23 months in Gindhir District, Southeastern Ethiopia: unmatched case–control study. Risk Manag Healthc Policy. (2022) 15:1669–79. doi: 10.2147/RMHP.S295806
24. Misganaw A, Naghavi M, Walker A, Mirkuzie AH, Giref AZ, Berheto TM, et al. Progress in health among regions of Ethiopia, 1990–2019: a subnational country analysis for the global burden of disease study 2019. Lancet. (2022) 399(10332):1322–35. doi: 10.1016/S0140-6736(21)02868-3
25. Wordofa MA, Garedew FT, Debelew GT, Ereso BM, Daka DW, Abraham G, et al. Quality of health data in public health facilities of Oromia and Gambela regions, Ethiopia. Ethiop J Health Dev. (2022) 36(2):1–11.
26. Girma S, Kitaw Y, Ye-Ebiy Y, Seyoum A, Desta H, Teklehaimanot A. Human resource development for health in Ethiopia: challenges of achieving the millennium development goals. Ethiop J Health Dev. (2007) 21(3):1–16. doi: 10.4314/ejhd.v21i3.10052
27. Abajebel S, Jira C, Beyene W. Utilization of health information system at district level in Jimma zone Oromia regional state, South West Ethiopia. Ethiop J Health Sci. (2011) 21:1–12.
28. Belay H, Azim T, Kassahun H. Assessment of health management information system (HMIS) performance in SNNPR, Ethiopia. Meas Eval. (2013) 3:1–25.
29. Yitayew S. Data Management Practice and Associated Factors of Health Extension Workers in East Gojjam Zone, Northwest Ethiopia, 2014. Sharjah, U.A.E.: University of Gondar (2014).
30. Umar U, Olumide E, Bawa S. Village health workers’ and traditional birth attendants’ record keeping practices in two rural LGAs in Oyo State, Nigeria. Afr J Med Med Sci. (2003) 32(2):183–92. http://adhlui.com.ui.edu.ng/jspui/handle/123456789/2603
31. Raeisi AR, Saghaeiannejad S, Karimi S, Ehteshami A, Kasaei M. District health information system assessment: a case study in Iran. Acta Inform Med. (2013) 21(1):30. doi: 10.5455/aim.2012.21.30-35
32. Mwangu M. Quality of a routine data collection system for health: case of Kinondoni district in the Dar es Salaam region, Tanzania. S Afr J Inf Manag. (2005) 7(2):1–7. https://hdl.handle.net/10520/AJA1560683X_213
33. Andargie G, Addisse M. Assessment of utilization of HMIS at distrinformationcommuincation technology level with particular emphasis on the HIV/AIDS program in North Gondar Amhara Region Ethiopian Public Health Association (EPHA). Extract MPH Theses. (2007) 3:50–62.
34. Shagake S, Mengistu M, Zeleke A. Data management knowledge, practice and associated factors of Ethiopian health extension workers in Gamo Gofa Zone, Southern Ethiopia: a cross-sectional study. J Health Med Informat. (2014) 5(150):2. doi: 10.4172/2157-7420.1000150
35. Asemahagn MA. Determinants of routine health information utilization at primary healthcare facilities in Western Amhara, Ethiopia. Cogent Med. (2017) 4(1):1387971. doi: 10.1080/2331205X.2017.1387971
36. Yarinbab TE, Assefa MK. Utilization of HMIS data and its determinants at health facilities in east Wollega zone, Oromia regional state, Ethiopia: a health facility based cross-sectional study. Med Health Sci. (2018) 7(1):1–9.
37. Moh E. Federal Democratic Republic of Ethiopia Ministry of Health Health Sector Development Program IV October 2010 Contents. October 2010. (2014):1–137.
38. Yitayew S, Asemahagn MA, Zeleke AA. Primary healthcare data management practice and associated factors: the case of health extension workers in northwest Ethiopia. Open Med Inform J. (2019) 13(1):2–7. doi: 10.2174/1874431101913010002
39. Ngusie HS, Shiferaw AM, Bogale AD, Ahmed MH. Health data management practice and associated factors among health professionals working at public health facilities in resource limited settings. Adv Med Educ Pract. (2021) 12:855. doi: 10.2147/AMEP.S320769
40. Mimi Y. The Routine Health Information System in Palestine: Determinants and Performance. London, UK: City University London (2015).
41. Desta FA, Shifa GT, Dagoye DW, Carr C, Van Roosmalen J, Stekelenburg J, et al. Identifying gaps in the practices of rural health extension workers in Ethiopia: a task analysis study. BMC Health Serv Res. (2017) 17(1):1–9. doi: 10.1186/s12913-017-2804-0
42. Teklegiorgis K, Tadesse K, Terefe W, Mirutse G. Level of data quality from health management information systems in a resources limited setting and its associated factors, eastern Ethiopia. S Afr J Inf Manag. (2016) 18(1):1–8. doi: 10.4102/sajim.v18i1.612
43. Tadesse K, Gebeyoh E, Tadesse G. Assessment of health management information system implementation in Ayder referral hospital, Mekelle, Ethiopia. Int J Intell Inf Syst. (2014) 3(4):34. doi: 10.11648/j.ijiis.20140304.11
Keywords: data, data management practice, health extension workers, associated factors, Central Gondar Zone
Citation: Melaku MS and Yohannes L (2024) Data management practice of health extension workers and associated factors in Central Gondar Zone, northwest Ethiopia. Front. Digit. Health 6:1479184. doi: 10.3389/fdgth.2024.1479184
Received: 11 August 2024; Accepted: 14 October 2024;
Published: 6 November 2024.
Edited by:
Anwar Musah, University College London, United KingdomReviewed by:
Ramachandran Venkataramanan, Karkinos Healthcare, IndiaTathagata Bhattacharjee, University of London, United Kingdom
Copyright: © 2024 Melaku and Yohannes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mequannent Sharew Melaku, bWVxdXNoYXJldzhAZ21haWwuY29t