 Christopher Przestrzelski1
Christopher Przestrzelski1 Felix R. Hoffmann
Felix R. Hoffmann- 1Department of Traumasurgery and Orthopedics, Klinikum Bogenhausen, Munich, Germany
- 2Surgical Management LMU Munich University Hospital, Munich, Germany
- 3Strategy & Market Research, Generali Deutschland AG, Munich, Germany
- 4Department of Health Economics, APOLLON University of Applied Sciences, Bremen, Germany
The AUD2IT-algorithm is a tool to structure the data, which is collected during an emergency treatment. The goal is on the one hand to structure the documentation of the data and on the other hand to give a standardised data structure for the report during handover of an emergency patient. AUD2IT-algorithm was developed to provide residents a documentation aid, which helps to structure the medical reports without getting lost in unimportant details or forgetting important information. The sequence of anamnesis, clinical examination, considering a differential diagnosis, technical diagnostics, interpretation and therapy is rather an academic classification than a description of the real workflow. In a real setting, most of these steps take place simultaneously. Therefore, the application of the AUD2IT-algorithm should also be carried out according to the real processes. A big advantage of the AUD2IT-algorithm is that it can be used as a structure for the entire treatment process and also is entirely usable as a handover protocol within this process to make sure, that the existing state of knowledge is ensured at each point of a team-timeout. PR-E-(AUD2IT)-algorithm makes it possible to document a treatment process that, in principle, does not have to be limited to the field of emergency medicine. Also, in the outpatient treatment the PR-E-(AUD2IT)-algorithm could be used and further developed. One example could be the preparation and allocation of needed resources at the general practitioner. The algorithm is a standardised tool that can be used by healthcare professionals of any level of training. It gives the user a sense of security in their daily work.
Introduction
In order to ensure that medical data management is of benefit to patients, it is necessary for it to be collected in a standardized manner and documented in an interoperable manner. A distinction can be made between different levels of interoperability. Structural interoperability means the ability to transfer user data from one system to another. Syntactic interoperability describes the ability to identify individual information units and data structures in the transmitted user data and to extract them for the purpose of further processing. Semantic interoperability describes the ability to interpret the extracted information units semantically correctly. Finally, the organizational interoperability describes cross-organisational coordinated workflows and processes (1).
The AUD2IT-algorithm is a tool to structure the data, which is collected during an emergency treatment. The two main goals are first to structure the documentation of the data and second to give a standardised data structure for the report during handover of an emergency patient. Accordingly, the AUD2IT-algorithm serves to ensure organizational interoperability in emergency medicine (2, 3).
The AUD2IT-algorithm was once developed to structure treatment reports in the emergency room in a uniform manner across all disciplines. In practice, it became apparent, that not only the quality of the reports was improved, but the scheme was also ideal for handing over patients. After a while, the AUD2IT-algorithm was taken up by professional societies, changed in some points, renamed to (PR_E-)AUD2IT-algorithm and as such included in the curriculum of emergency room-trainings.
Today the (PR_E-)AUD2IT-algorithm is deeply introduced in training curriculums of emergency medicine (4) and is recommended to be used in emergency departments for treatment of critical ill, non-traumatic patients (5). But in some points, there is no uniform interpretation of the application of the scheme. This discussion paper aims to reflect the existing publications and user experiences regarding the AUD2IT-algorithm, will discuss the controversial points and make recommendations for the implementation.
AUD2IT-algorithm and (Pr_E-)AUD2IT-algorithm in emergency care
The idea behind the development of the AUD2IT-algorithm was to provide residents a documentation aid, which helps to structure the medical reports without getting lost in unimportant details or losing important information. Therefore, the AUD2IT-algorithm maps the entire emergency treatment and brings together the data in clusters, which are documented chronologically. A pleasant side effect is, that the AUD2IT-algorithm can replace or include many of the numerous emergency medical action schemes such as SBAR, SAMPLER or cABCDE, thus only one single action scheme must be learned (2, 3).
The treatment process in a resuscitation room commences well before the patient even arrives. The resuscitation team is actively engaged in preparing for the patient's arrival and the entire process is carefully orchestrated to ensure the best possible outcome. So, there was a need to expand the AUD2IT-algorithm to include the phase from the alarm to the arrival of the patient in the resuscitation room. The (PR_E-)AUD2IT-algorithm was developed (6). Table 1 compares and describes the two algorithms.
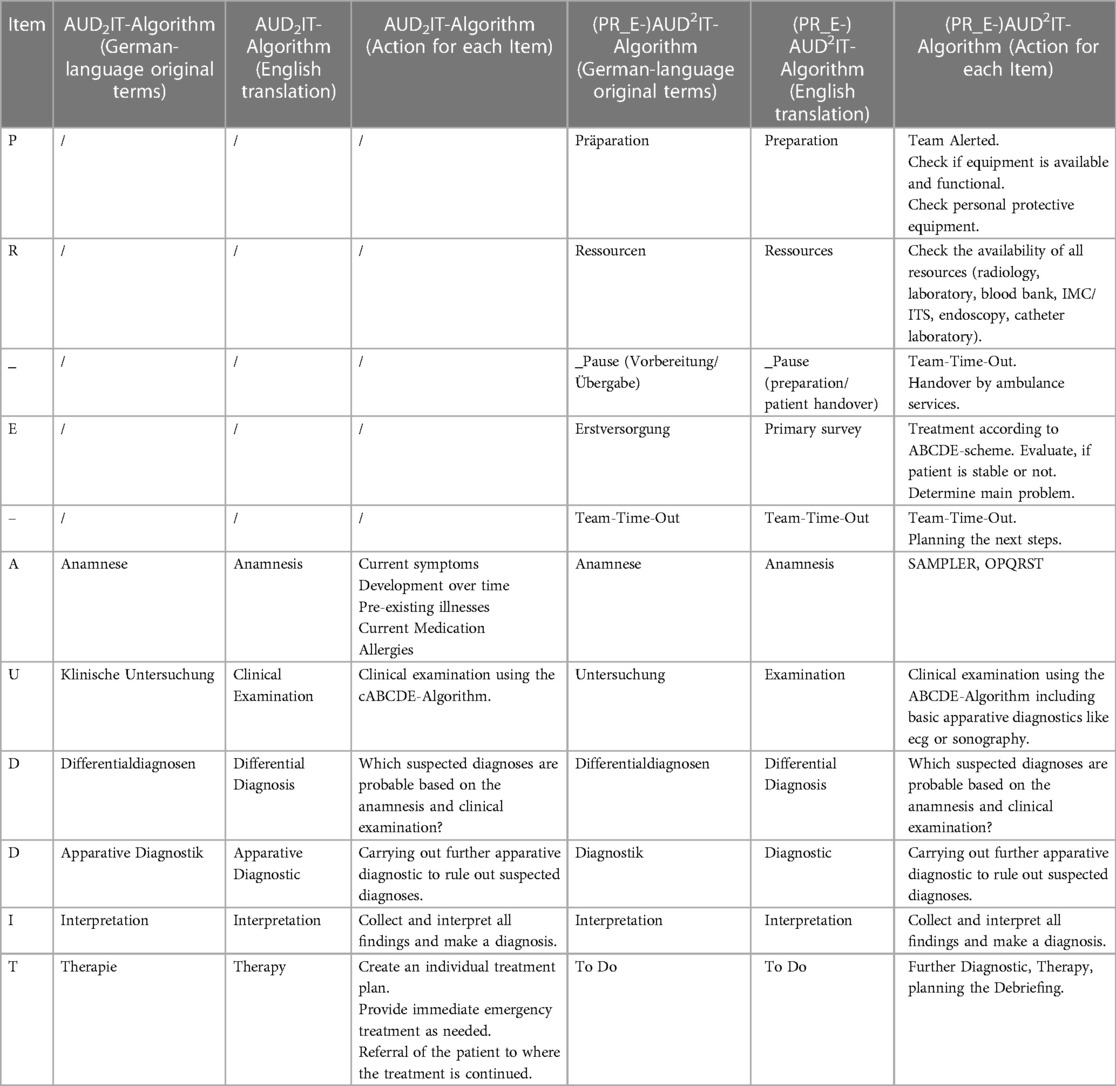
Table 1. Comparison of AUD2IT-algorithm and (PR_E-)AUD2IT-algorithm.
Considerations about how to improve the implementation of the (Pr_E-)AUD2IT-algorithm in emergency care
While the (PR_E-)-section represents a chronological period of time in preparation for care for the emergency patient, the period during the AUD2IT-section is more complicated. The sequence of anamnesis, clinical examination, considering a differential diagnosis, technical diagnostics, interpretation and therapy is rather an academic classification then a description of the real workflow. In a real setting, most of these steps take place simultaneously. Therefore, the application of the AUD2IT-algorithm should also be carried out according to the real processes.
Bernhard et al. say that handover is an important point within an emergency treatment and gives advice, which general conditions should be ensured during the handover-process (5). But there is lack of information about the contents and the structure of the handover. As a result, healthcare professionals may resort to employing pre-existing handover protocols; however, these protocols are frequently incomplete and may not adequately address all necessary actions. That is not necessary as the AUD2IT-algorithm can be used instead and therewith can replace most of the existing action schemes. The clue is, that on the one hand the AUD2IT-algorithm can be used as a structure for the entire treatment process and also is entirely used within this process to summarize the existing state of knowledge at each point of a team-timeout (Figure 1). It is not necessary to repeat every information at every time when the team has not changed. It is enough just to summarize changes or new findings since the last AUD2IT-check.
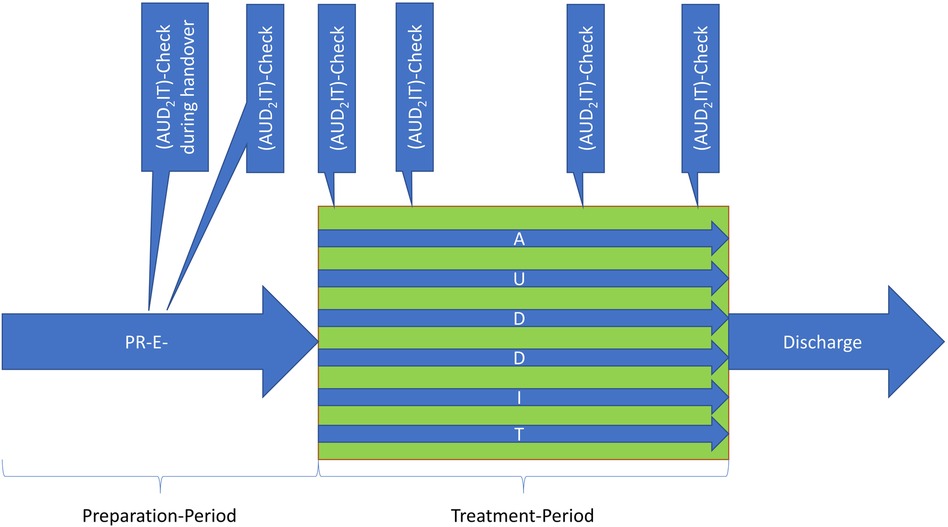
Figure 1. Using AUD2IT-algorithm as a structure for the entire treatment process and also to summarize the existing state of knowledge at each point of a team-timeout.
In this way, the AUD2IT-algorithm gets a new role and can not only be used for treatment planning and documentation, but also for all handovers.
The “U” changed during the time. While it described in the initial AUD2IT-algorithm the clinical examination, in (PR_E-)AUD2IT-algorithm it also includes an ecg or sonography (2, 3, 6). This should be critically questioned since these apparatus diagnostic are also the consequence of the anamnesis and clinical examination. In an emergency treatment, several steps take place at the same time, so it would make more sense to assign each person with a different task and thus carry out all measures according to the AUD2IT-algorithm at the same time.
The treatment documentation should be done according to the AUD2IT-algorithm by using international standards for interoperability like FHIR or HL7.
The nomenclature
Let us discuss two aspects of the nomenclature.
In the original version of the AUD2IT-algorithm, the ″2″ is subscript to make clear that it stands for two D's. The ″2″ in the initial publication of the (PR_E-)AUD2IT-algorithm is superscript, giving it meaning and suggesting, that the “D” is being squared. We recommend to go back to the original variant with a subscript ″2″, as it is also the case in other algorithms like the CHA2DS2-VASc-Score (7).
We would like to propose a recommendation on the use of brackets and hyphen. To do justice to the fact that (PR_E-) describes a chronological process while AUD2IT should be used repeatedly during an ongoing treatment process, we recommend to put the AUD2IT in brackets. The underscore and the hyphen both represent a team time out; to avoid confusion, we recommend using in both cases the same special character. Consequently, we recommend to use the notation PR-E-(AUD2IT) for the complete algorithm.
Can the Pr-E-(AUD2IT)-algorithm be used in non-emergency medical fields?
The PR-E-(AUD2IT)-algorithm makes it possible to document a treatment process that, in principle, does not have to be limited to the field of emergency medicine. After treatment in the emergency department, often follows a transition to inpatient care. The fact, that the illness occurred acutely, does not play a significant role in the handover and documentation. When the patient moves from the emergency department to another unit, data is also transferred. This often results in interface breaks, which can be countered by a uniform design of the data infrastructure. Why should it not be possible for the documentation of a treatment to be continued in the same way even after the transfer to another unit?
In principle, all inpatient and outpatient treatments at case level could be documented with the AUD2IT-algorithm. The result would be a clear standardization of data infrastructures, which is for example reflected in uniform treatment reports and user interfaces of IT applications. Further studies should evaluate whether these considerations can also be proven in practice.
Also, in the outpatient treatment the PR-E-(AUD2IT)-algorithm could be used and further developed. One example could be the preparation and allocation of needed resources at the general practitioner. The algorithm is a standard tool that can be used by medical personnel of any level of training. It gives the user a sense of security in their daily work.
Conclusions
1. We recommend to use the notation PR-E-(AUD2IT) for the complete algorithm.
2. Disregard the employment of action schemes such as SBAR or Sampler and instead adopt the PR-E-(AUD2IT)-algorithm instead as a comprehensive alternative algorithm.
3. Use the “PR-E-” as a chronologic guide to prepare for the treatment, but use (AUD2IT) as a chronological action scheme as well as a single-point handover-scheme.
4. There is no reason not to use the PR-E-(AUD2IT)-algorithm for other medical issues like in non-emergency outpatient departments or post-emergency-units. The process is the same, data are the same so the structure should be the same as well.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
FH gave the idea for this study. All authors discussed how to improve AUD2IT-Scheme, CP and CJ from an emergency doctors perspective and AJ from a nursing perspective. CP and FH gave the main input in writing the article. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lehne M, Sass J, Essenwanger A, Schepers J, Thun S. Why digital medicine depends on interoperability. NPJ Digit Med. (2019) 2:79. doi: 10.1038/s41746-019-0158-1
2. Hoffmann F, Gröning I. Das AUDIT-schema als instrument für eine strukturierte notfallversorgung. Notfall Rettungsmedizin. (2019) 22 (Suppl 1):S9–10. doi: 10.1007/s10049-019-00645
3. Hoffmann F, Gröning I. Das AUD2IT-Schema als Instrument für Eine Strukturierte Notfallversorgung. Bremen: Deutsche Gesellschaft für Interdisziplinäre Notfall- und Akutmedizin e.V. (DGINA) (2019).
4. Michael M, Biermann H, Gröning I, Pin M, Kümpers P, Kumle B, et al. Development of the interdisciplinary and interprofessional course concept “advanced critical illness life support”. Front Med (Lausanne). (2022) 9:939187. doi: 10.3389/fmed.2022.939187
5. Bernhard M, Kumle B, Dodt C, Gräff I, Michael M, Michels G, et al. Versorgung kritisch kranker, nicht-traumatologischer Patienten im Schockraum: Empfehlungen der Deutschen Gesellschaft für Interdisziplinäre Notfall- und Akutmedizin zur Strukturierung, Organisation und Ausstattung sowie Förderung von Qualität, Dokumentation und Sicherheit in der Versorgung kritisch kranker, nicht-traumatologischer Patienten im Schockraum in der Bundesrepublik Deutschland. Notfall Rettungsmedizin. (2022) 25(Suppl 1):1–14. doi: 10.1007/s10049-022-00997-y
6. Gröning I, Hoffmann F, Biermann H, Pin M, Michael M, Wasser C, et al. Das (PR_E-)AUD2IT-Schema als Rückgrat für eine strukturierte Notfallversorgung und Dokumentation nichttraumatologischer kritisch kranker Schockraumpatienten. Notfall Rettungsmed. (2021) 73(4):504. doi: 10.1007/s10049-021-00878-w
Keywords: handover, emergency medicine, process management, interoperability (IoP), data
Citation: Przestrzelski C, Jakob A, Jakob C and Hoffmann FR (2024) Discussion paper: implications for the further development of the successfully in emergency medicine implemented AUD2IT-algorithm. Front. Digit. Health 6:1249454. doi: 10.3389/fdgth.2024.1249454
Received: 30 June 2023; Accepted: 19 March 2024;
Published: 4 April 2024.
Edited by:
Uwe Aickelin, The University of Melbourne, AustraliaReviewed by:
Yi Zhang, Harvard Medical School, United States© 2024 Przestrzelski, Jakob, Jakob and Hoffmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Felix R. Hoffmann RmVsaXguSG9mZm1hbm5AdW5pLWR1ZXNzZWxkb3JmLmRl