
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Digit. Health, 13 October 2022
Sec. Human Factors and Digital Health
Volume 4 - 2022 | https://doi.org/10.3389/fdgth.2022.954069
 Hiral Soni1*
Hiral Soni1* Julia Ivanova1
Julia Ivanova1 Hattie Wilczewski1
Hattie Wilczewski1 Alexandra Bailey1
Alexandra Bailey1 Triton Ong1
Triton Ong1 Alexa Narma1
Alexa Narma1 Brian E. Bunnell1,2
Brian E. Bunnell1,2 Brandon M. Welch1,3
Brandon M. Welch1,3
Objective: Virtual conversational agents, or chatbots, have emerged as a novel approach to health data collection. However, research on patient perceptions of chatbots in comparison to traditional online forms is sparse. This study aimed to compare and assess the experience of completing a health assessment using a chatbot vs. an online form.
Methods: A counterbalanced, within-subject experimental design was used with participants recruited via Amazon Mechanical Turk (mTurk). Participants completed a standardized health assessment using a chatbot (i.e., Dokbot) and an online form (i.e., REDCap), each followed by usability and experience questionnaires. To address poor data quality and preserve integrity of mTurk responses, we employed a thorough data cleaning process informed by previous literature. Quantitative (descriptive and inferential statistics) and qualitative (thematic analysis and complex coding query) approaches were used for analysis.
Results: A total of 391 participants were recruited, 185 of whom were excluded, resulting in a final sample size of 206 individuals. Most participants (69.9%) preferred the chatbot over the online form. Average Net Promoter Score was higher for the chatbot (NPS = 24) than the online form (NPS = 13) at a statistically significant level. System Usability Scale scores were also higher for the chatbot (i.e. 69.7 vs. 67.7), but this difference was not statistically significant. The chatbot took longer to complete but was perceived as conversational, interactive, and intuitive. The online form received favorable comments for its familiar survey-like interface.
Conclusion: Our findings demonstrate that a chatbot provided superior engagement, intuitiveness, and interactivity despite increased completion time compared to online forms. Knowledge of patient preferences and barriers will inform future design and development of recommendations and best practice for chatbots for healthcare data collection.
Patient-reported health data such as medical history and clinical questionnaires are a vital and routine component of care and research. Patient-reported data give providers a more comprehensive picture of a patient's condition so they can make informed decisions and provide high quality care. In research, patient data are vital to assess progress, make inferences, and obtain meaningful insights to improve health.
Conventional data collection methods such as paper-based or online forms can be time-consuming, unintuitive, and full of jargon (1). The language used in these forms often requires an advanced reading level to understand (1). Further, data collection via paper forms may require costly and error-prone human input (2–4). In addition, online forms must comply with privacy regulations, integrate with different tools for efficient data collection and sharing, and provide an effective user experience to ensure high-quality data–free of omissions and inaccuracies (5). Beyond paper or online forms, verbal data collection by clinicians and/or researchers is easier for patients to complete; elicit higher quality information; and generate discrete, accessible data for research (6). However, this approach requires dedicated staff, an option that is not always practical or affordable (7–9).
Virtual conversational agents (i.e., chatbots) have proven to be a promising approach to patient data collection. Chatbots simulate human conversations to provide a data collection experience that is more naturalistic and intuitive than standard forms. Patients have reported positive perceptions of chatbots including ease of use, understandability, and enjoyability (10–15). Some studies have found that chatbots improve user experience by reducing workload and enhancing ease of completing asynchronous surveys at patients’ convenience (16). Providers perceive chatbots as beneficial for administration and organizational tasks and information dissemination (17).
Research on patient experiences with data collection chatbots in comparison to conventional online or web-based forms is sparse. One study comparing family health history collection using a chatbot against an online form found that participants reported higher satisfaction, usefulness, information quality, and interface quality for the chatbot despite overall longer completion time (11). However, participants in this study were recruited from a university campus, were highly educated, and completed the study in a controlled environment with fictional scenarios and data. There is a need to investigate chatbot preferences and optimization with larger, more diverse populations.
The purpose of the present study was to compare patient data-capture experience of chatbots with online forms. The findings of this study will help understand individuals’ experiences and preferences of data collection using a chatbot and will establish recommendations for chatbot development and usability in the future.
This online study was completed via Amazon Mechanical Turk (mTurk), an online crowd-sourcing platform for remote recruitment (18). We aimed to recruit 400 mTurk workers (individuals registered as potential participants on mTurk) based in the US and ≥18 years of age by using mTurk's worker requirement filtering. After providing informed consent, participants completed the study as described in Section “Study design”. No personally identifiable information was collected. Participants were compensated $2.50 to complete this 20-minute study. This study was designated exempt by the Medical University of South Carolina Institutional Review Board (Pro00082875).
We collected information on participant characteristics (age, race, ethnicity, education, gender) and previous experience of taking surveys, including commonly used devices to complete the surveys and familiarity with survey taking.
The SUS includes 10 items that are alternatingly worded positively (e.g., I thought the system was easy to use) and negatively (e.g., I found the system unnecessarily complex)(19). Responses were anchored on a 5-point Likert Scale (i.e., 1 = Strongly Disagree to 5 = Strongly Agree).
The NPS is a one-question measure of customer loyalty and likelihood to recommend a product (How likely are you to recommend 〈tool name〉 as a survey completion tool?) and is considered a gold-standard rating (20).
We asked about participants' tool preference (chatbot vs. online form) using a structured question [i.e., Based on your experience today with the two survey tools, which of the following tools would you prefer? (Dokbot; REDCap)] and three open-ended questions regarding likes and dislikes of each tool and tool enhancement suggestions.
We measured the assessment completion time (in seconds) as the time from when the user was directed to a tool (chatbot or online form) to when the user was directed to the UXEvaluator (Section “Study design”).
This study used a counterbalanced, within-subject experimental design to conduct a large-scale, unmoderated study comparing the usability and user experience of completing a health assessment using a chatbot (i.e., Dokbot) and an online form (i.e., REDCap) (11, 21).
Dokbot is a free, secure (compliant with Health Insurance Portability and Accountability Act of 1996), simple chatbot developed to collect healthcare data in an interactive way, mimicking human-to-human interaction. Dokbot is a browser-based application that does not require downloads and is designed with a mobile-first approach, which is particularly important for patients as they are most likely to access the internet through a smartphone (22, 23). Dokbot can be customized with various names, avatars, languages, and personalities appropriate to user characteristics (e.g., age, gender, etc.) and can be integrated within different health information technology (HIT) systems (24).
REDCap is a widely used traditional web-based tool to collect health and research data in a secure way (25). REDCap can be used to conduct cross-sectional and longitudinal studies, can be integrated with various HIT systems, is customizable, and is free for REDCap consortium partners who have a valid end-user agreement with Vanderbilt University. REDCap is widely used by researchers and providers for clinical data collection (26). Hence, it was chosen as the online form comparison for this study. Figures 1, 2 show screenshots of Dokbot and REDCap, respectively.
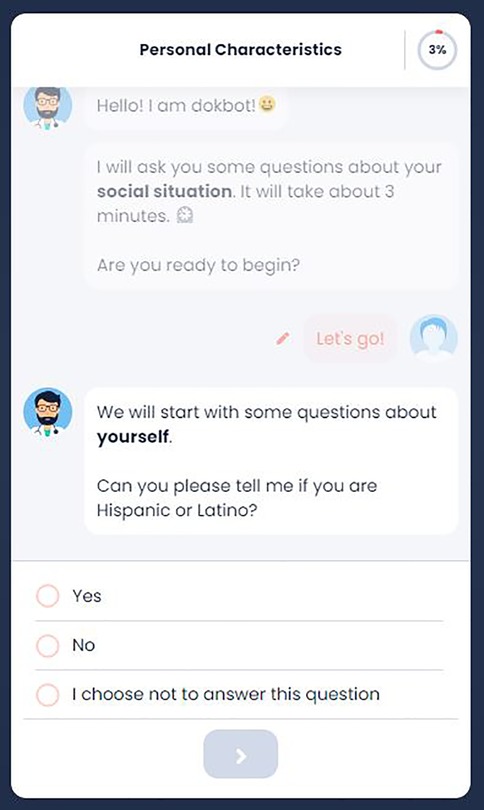
Figure 1. Dokbot interface.
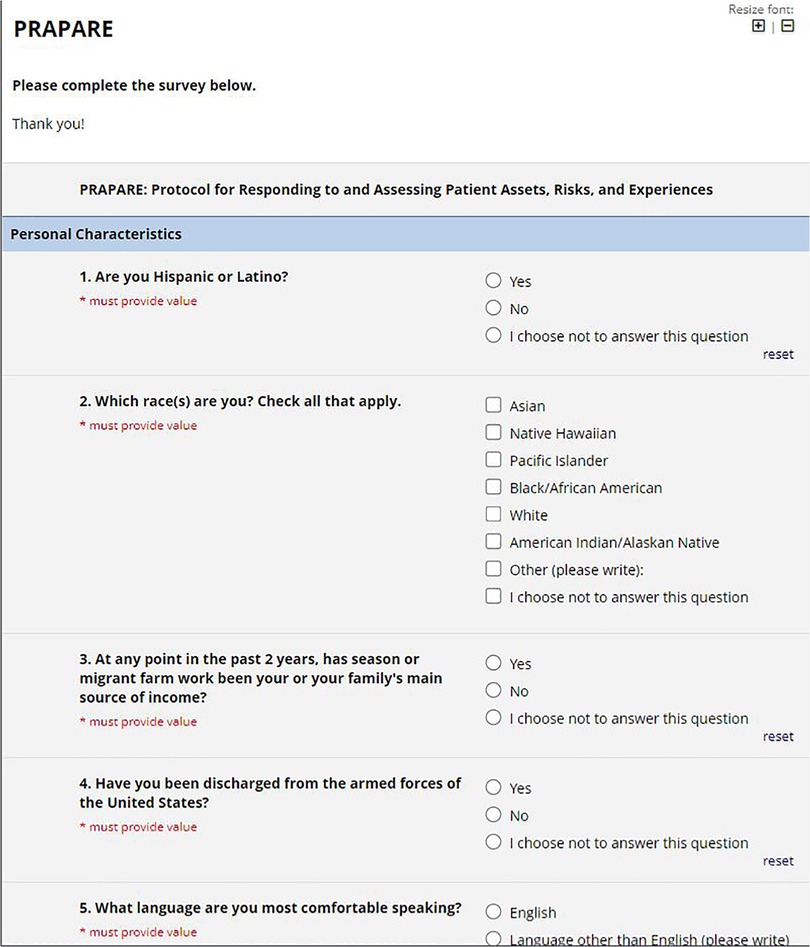
Figure 2. REDCap interface.
We developed a software tool UXEvaluator to conduct the study. UXEvaluator is a web-based tool designed to compare the usability and experience of completing web-based forms or questionnaires. The tool was developed to counterbalance condition sequence across subjects such that each condition was experienced in a random order within-subject. UXEvaluator was used to collect consent and conduct pre- and post-test surveys.
Figure 3 summarizes the overall approach of UXEvaluator and this study.
Step 1. Consent: Participants were informed about the procedures, benefits and risks, their rights, and provided informed consent prior to the study.
Step 2. Pre-test questionnaire: Participants completed a pre-test questionnaire about demographics as described in Section “Study measures”.
Step 3. Hands-on with Tool 1: At this step, participants completed the Protocol for Responding to and Assessing Patients' Assets, Risks, and Experiences (PRAPARE) health assessment. We chose this social determinant of health assessment considering its moderate length (21 questions), variety of response formats (e.g., text and numeric inputs, radio buttons, checkboxes), and broad applicability. For the standard PRAPARE question asking for a patient address, participants were instructed to input a fictional address to protect privacy. No personal identifying information was collected. All questions were required. The PRAPARE was administered using either the chatbot (i.e., Dokbot) or the online form (i.e., REDCAP), depending on random group assignment. Group A participants were assigned to complete PRAPARE with the online form first, Group B participants completed the survey using the chatbot first (Step 5).
Step 4. Tool 1 satisfaction: Once participants completed the PRAPARE questionnaire using the first randomly assigned tool, they completed SUS and NPS to assess the usability and likelihood to recommend the first tool.
Step 5. Hands-on with Tool 2: Users completed the PRAPARE assessment using the second tool. Group A participants completed the assessment using the online form and Group B participants via the chatbot.
Step 6. Tool 2 satisfaction: Participants completed SUS and NPS for the tool used in Step 5.
Step 7. Post-test questionnaire: Participants completed the tool preference measures as described in Section “Study measures”.

Figure 3. Study design.
We aimed to recruit a sample of 400 participants on mTurk. However, we observed poor data quality and careless responses with respect to SUS, qualitative responses for open-ended questions on likes and dislikes of each tool, and tool enhancement suggestions. We rejected participants with potential careless responses and recruited 127 additional participants but observed no improvements in data quality. To preserve data integrity and quality, we systematically excluded responses to eliminate acquiescence bias and careless qualitative responses based on previous evidence.
Acquiescence biases often refer to participants' tendency to agree or disagree through all questions (27). The SUS is designed with alternating positive and negative statements, such that yea- or nay-saying biases were easily detected with consecutive responses conflicting with one another. It is reported that 8 or more agreements (or disagreements) could suggest that participants could be rushing through the SUS without paying attention (28). We assessed and excluded entries where users chose positive or negative responses (e.g., strongly agree/agree or disagree/strongly disagree) for eight or more statements of SUS. Entries with 8 or more neutral responses (neither agree or disagree) were included in the analysis. We excluded responses if careless responding was observed for SUS related to one (chatbot or online form) or both tools. This resulted in the exclusion of 50 responses. Table 1 shows example responses for this step.

Table 1. Examples of participant responses for system usability scale with ≥8 same responses.
Studies have reported concerns over low data quality and careless qualitative responses from participants recruited on mTurk (29–33). Previously, researchers have noted poor qualitative responses such as short and irrelevant responses, noticeably ungrammatical or nonsense phrases, phrases copied from questions, instructions, online resources, or forms, and text strings repeated among different participants (31, 34). Research suggests removal of potentially fraudulent, careless, and duplicate responses (31).
Four researchers (HS, JI, TO, and HW) developed an exclusion coding scheme based on previous research using four criteria (Table 2). A sample of 72 responses for likes and dislikes of each tool and enhancement suggestions were coded by HS and JI to compute inter-rater agreement. There was a 93% agreement between the two coders, showing high degree of agreement. Coding disagreements resolved by discussion to reach an agreement of 100%. The remaining responses (i.e., n = 319) were coded by HS using the updated criteria agreed upon during the resolution of disagreements and reviewed by JI. One of the four exclusion criterion below was assigned to each response:
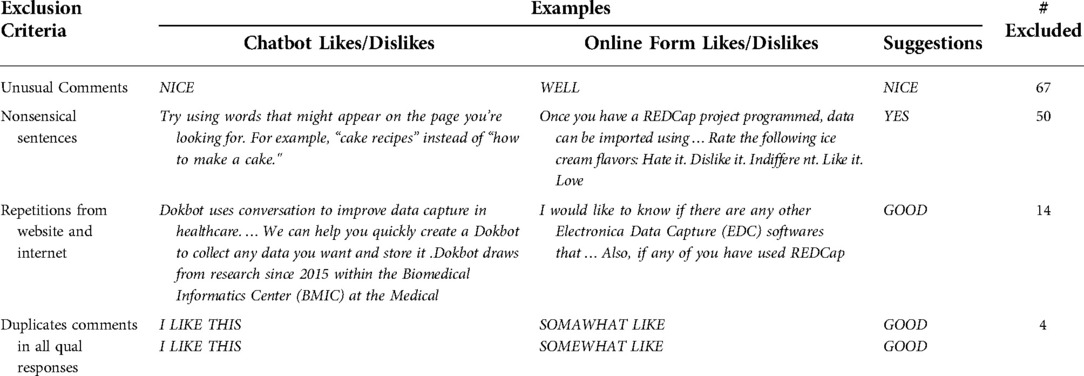
Table 2. Exclusion criteria for qualitative responses.
We excluded responses with no meaning (e.g., “users experience the interaction as the nature I like that and dislike is dislike dokbot are real things”) or did not relate to the current study (e.g.,“Try using words that might appear on the page you're looking for. For example, “cake recipes” instead of “how to make a cake”).
We also excluded responses which included direct repetitions of statements from product websites, online resources, media coverage or any other publicly available material about the chatbot (such as “Dokbot uses conversation to improve data capture in healthcare. … We can help you quickly create a Dokbot to collect any data you want and store it .Dokbot draws from research since 2015 within the Biomedical Informatics Center (BMIC) at the Medical”) or online form (“The REDCap Consortium, a vast support network of collaborators, is composed of thousands of active institutional partners in over one hundred countries who utilize and support their own individual REDCap systems”).
We excluded responses with short, unusual comments irrelevant to the question, including responses often written in all capital letters and single words irrelevant responses (e.g., for the question, “what did you like/dislike about 〈tool name〉?,” responses of “NICE”, “good”, and “WELL”). To ensure that valid responses were not eliminated, researchers cross-validated the qualitative comments with their preference of the tool (chatbot or online form). For example, in the questions asking about likes and dislikes of each tool, if a participant responded “VERY LIKE” for the chatbot and “LIKE” for the online form, we reviewed their tool preference. In this scenario, their response was included in analysis if they preferred the chatbot, but it was excluded if they preferred the online form.
We removed any duplicate qualitative responses. When we encountered potential duplicate responses, we reviewed the responses for timestamp (studies completed within a short time period), responses to demographic questions (same responses to questions asking age, gender, race, etc.). If the questions contained similar responses, we excluded all potential duplicate responses.
This step resulted in the elimination of 135 responses. Table 2 provides examples of excluded responses and related criteria.
After applying both the cleaning steps, a total of 206 responses were included in the final consideration for analysis. Quantitative data were tabulated, and descriptive statistics were used to quantify frequency, mean, median, and standard deviation for demographics and pre-test survey experience questions. SUS scores and NPS were calculated based on standardized calculations. Paired t-tests and chi-square tests were used to assess differences in SUS, NPS, time taken to complete the PRAPARE assessment, and tool preference. MS Excel and SPSS v28 were used for analyses.
Qualitative responses to open-ended post-test questions were coded to identify likes and dislikes as well as emerging themes related to the tool. Participant responses in full served as the units for coding. Content analysis was used to code participant responses into positive, negative, and neutral categories. Exploratory thematic analysis was completed using MS Excel by one team member followed by thematic analysis using MAXQDA, a qualitative coding platform (35). Over three iterations, a codebook was developed and refined by the entire research team. Another member of the team reviewed the codes, and any discrepancies were resolved through consensus. Themes were quantified and organized by frequency and topic. This process supplemented quantitative analysis. Complex coding query (intersections) was performed to identify what emergent themes were found in juxtaposition to tool opinions.
Of the 206 participants, 98 participants were in Group A and 108 were in Group B. No significant differences were found in the number of participants in the two groups (χ2(1, N = 206) = 0.4854, p = 0.4860). Table 3 describes the participant characteristics after each data exclusion (elimination of responses with acquiescence bias in SUS and careless qualitative feedback) steps. Table 4 summarizes the groups (A and B) sample size, tool preference, SUS score, NPS score, and time taken to complete the assessment after each exclusion.
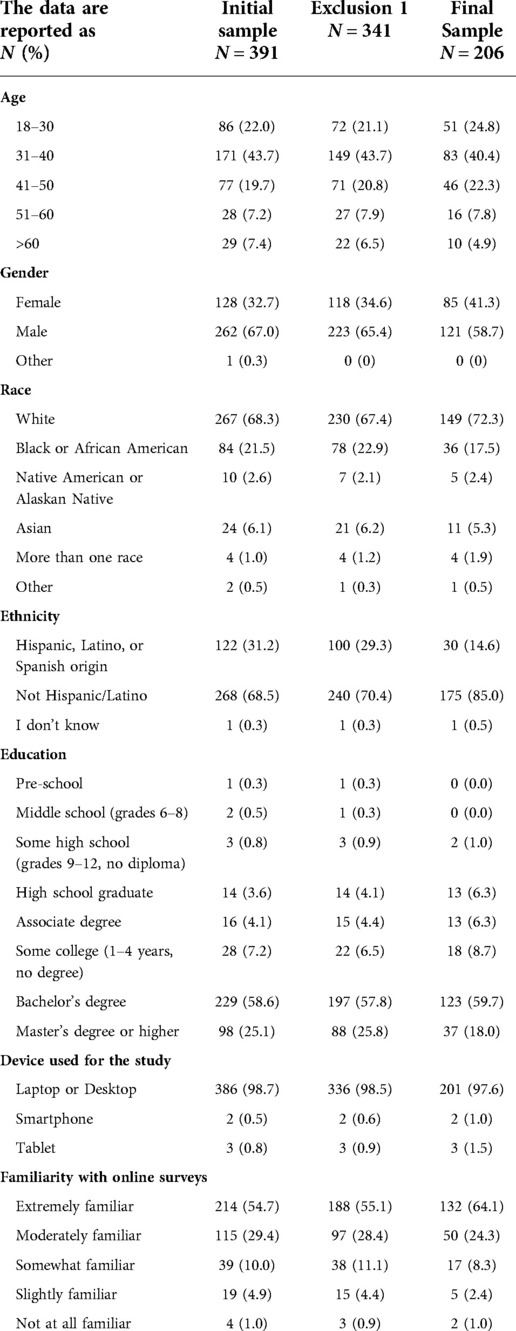
Table 3. Participant demographics.
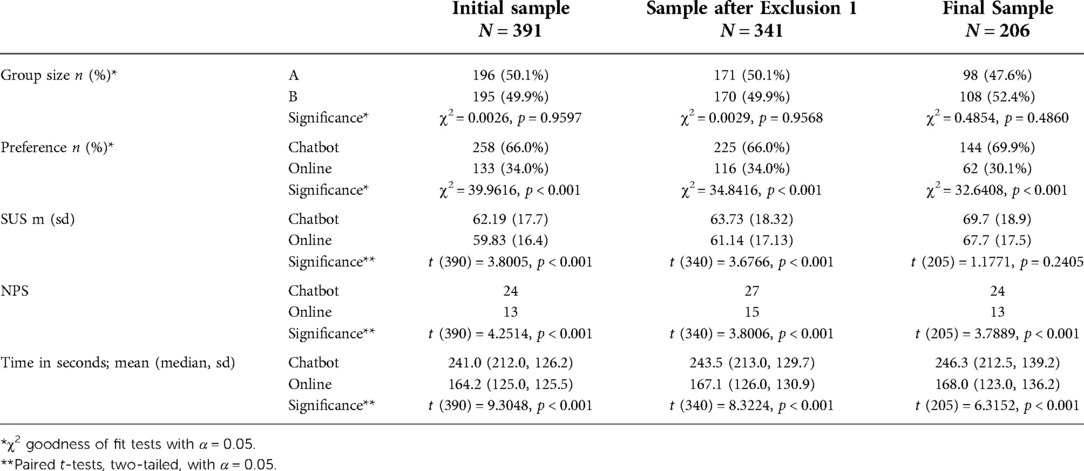
Table 4. Usability and preference characteristics at each exclusion.
The median time to complete the PRAPARE assessment was 89.5 s longer using the chatbot (median time = 212.5 s) compared to the online form (median time = 123.0 s). This difference was statistically significant (t(205) = 6.3152, p < 0.001). Overall, 148 out of 206 (71.8%) participants took longer time (118 s more) to complete the PRAPARE assessment using the chatbot. Most (99.1%; n = 107/108) of Group B participants, who completed the PRAPARE assessment using the chatbot first, took longer to complete the assessment using the chatbot. In comparison, 58.2% (n = 57/108) of participants who completed the assessment in Group A (online form and then chatbot) took longer to complete the assessment using the online form (median 60 s longer).
No significant differences were observed in SUS scores between the chatbot (M = 69.7) and online form (M = 67.7; t(205) = 1.1771, p = 0.2405). The reported NPS was significantly higher for the chatbot (NPS = 24) compared to the online form (NPS = 13; t(205) = 3.7889, p < 0.001).
Of the 206 participants included in the analyses, 144 (69.9%) preferred the chatbot and 62 (30.1%) preferred the online form. There was a statistically significant difference in the preference for the chatbot over the online form (χ2(1, N = 206) = 32.6408, p < 0.001).
The post-test questionnaire asked participants about their likes and dislikes towards the user tool and enhancement suggestions. The qualitative responses were thematically analyzed to identify common emerging themes. Table 5 presents the common emerging themes and example responses related to both the tools.
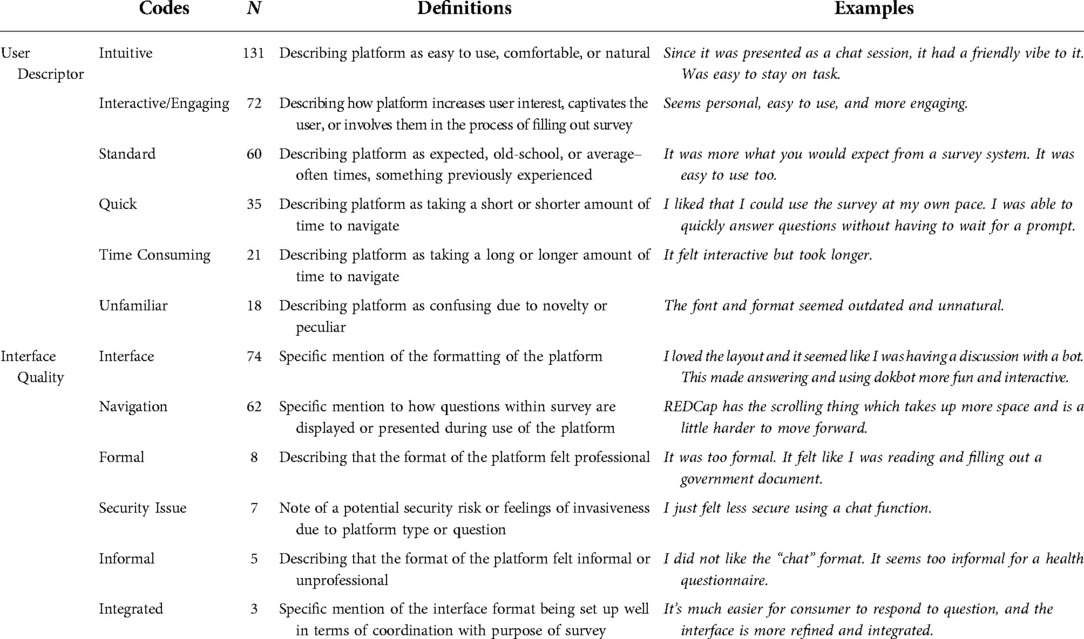
Table 5. Common emerging themes and examples.
Participants often perceived the chatbot's interface as conversational, interactive, intuitive–comparable to having a natural conversation. One participant said, “I did like the way it was designed and had the feeling that I was talking to a human.”
Participants also felt the chatbot was easy (intuitive) to use. One participant mentioned, “[chatbot] was very easy to use and it was amazing to handle,” and another participant commented, “I liked how easy it was to use [chatbot]. I liked how it seemed as if it were progressing through questions without me having to click things. I didn't dislike anything about [chatbot]”.
Participants also commented on the design and layout of the chatbot's interface. Participants perceived that the interface was modern and easy to navigate. Considering the mobile-first approach, participants appreciated that they did not need to scroll through the screen. Participants also liked the presentation of the information and the systematic flow. As the chatbot presents questions one-by-one, there are fewer chances of skipping a response and focusing on the presented question or task. A participant commented, “it was easier to fill out without worrying if you accidentally skipped a question.” However, some participants perceived that the display was small, presented a large amount of information, and felt informal for healthcare assessments.
Some participants also reported the chatbot felt time-consuming, which aligned with the longer average completion time for the chatbot. They mentioned that “it's a bit slower compared to seeing all questions at once on the [online] survey.” Whereas most participants perceived the chatbot as natural and engaging as talking to a human, a few participants were concerned about the privacy of the information due to the chat-based nature. One participant noted, “I just felt less secure using a chat function.”
When discussing interface quality, six participants mentioned security issues with one participant mentioning security twice in their responses. One participant commented that the online form was a “simple and honest way to gather information. No manipulation or misleading.” While three participants specifically noted some type of discomfort as associated with the chat function (Table 5), the other three participants felt the chatbot was asking sensitive questions: “Seemed a bit invasive. Not sure what the actual purpose was. Why would it need my address?” and “It seemed to ask really personal questions and it made me suspicious…”
Participants often perceived the online form's interface to be less favorable. Although some participants commented that the interface was simple, straightforward, formal, and presented all information at once, participants commonly perceived the interface as old school or traditional. Participants disliked the design and layout of the assessment including, design and size of the response areas, alignment of questions, color scheme, and readability. One participant commented, “it's kinda stressful with the way the items are aligned.”
Participants did acknowledge that the online form's interface was quick and less time-consuming compared to the chatbot, but it was also less engaging and efficient: “I felt [the online form] was a bit faster. However, I felt it was less personable than the other [chatbot] tool”.
Additionally, complex coding queries were done with the most populated codes to determine whether there was discussion of multiple topics by participants in a meaningful way (Table 6). Navigation was often discussed in tandem with whether the product was intuitive (25 codes), quick (13 codes), and interactive/engaging (10 codes): “I thought it was exceedingly intuitive, snappy, and it felt more personable and engaging than REDCap. I liked the chatbot nature of dokbot. It allowed for much more efficient progression through the questions. There wasn’t anything I disliked.”
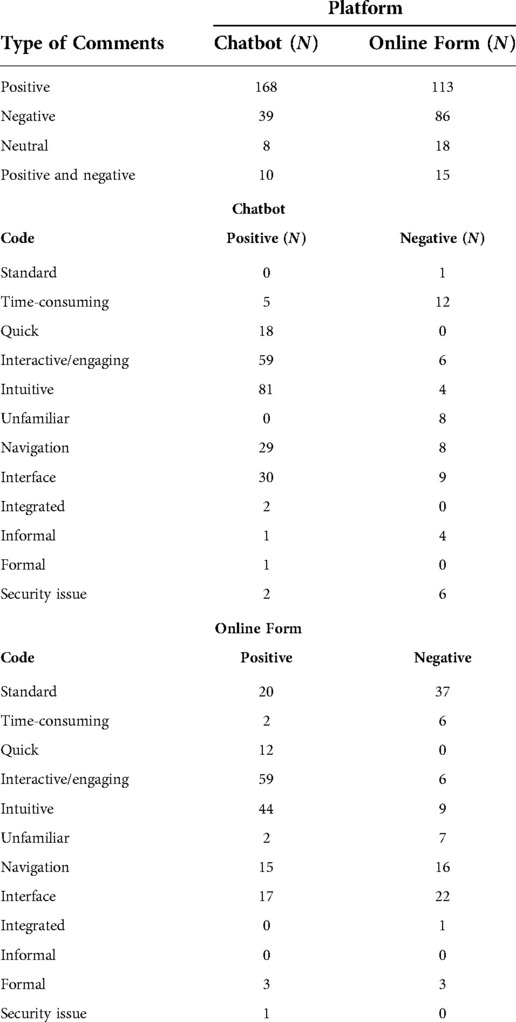
Table 6. Positive and negative perception resulting from complex coding query.
Meanwhile, interface was most often discussed in tandem with interactive/engaging (10 codes), intuitive (15 codes), and unfamiliar (4 codes): “I just didn’t feel I was able to read and interact with it in a comfortable manner…and it felt a bit more rushed as if someone was waiting on me to answer the question…”
When looking at whether participants provided positive, negative, or neutral commentary, the chatbot received majority positive responses (59.8%), while the online form received majority negative responses (68.8%). When further analyzed, the chatbot received most of its positive comments regarding its interactive/engaging and intuitive interface: “It seems like chatting with a real human, it is so engaging.” The online form, on the other hand, received most of its positive commentary regarding its standard and intuitive interface: “It was more what you would expect from a survey system. It was easy to use too.” Further, the online form's negative comments focused on that same standard trait: “Bland. straightforward.”
Our goal was to explore virtual conversational agents or chatbots as an effective means to facilitate healthcare data collection. We present one of the earliest studies assessing user preferences of chatbots for data collection in comparison with traditional online forms. Participants preferred the chatbot's interface, reporting higher usability and significantly higher likelihood to recommend it as a data collection tool. The reported SUS scores for the chatbot (69.7) was higher than the average industry benchmark score of 68 (19, 36). The NPS score of the chatbot (NPS = 24) was higher than the online form (NPS = 13). The chatbot received the majority (59.8%) of positive responses with comments remarking on its conversational, intuitive nature, “…it seemed like I was having a discussion with a bot. This made answering and using dokbot more fun and interactive.” While the standard online form's interface received the majority (68.8%) of negative responses, some of its most positive participant comments praised its familiarity: “Very standard, easy to use and worked well, I could get a larger overview of the entire survey.” One participant encapsulated the feeling of the form being standard simply, “Bland. straightforward.” The modern layout and the mobile, human-like interface and design of the chatbot was the source of the most positive comments. Indeed, though the standard interface survey was considered intuitive (most likely due to prior exposure), the chatbot was intuitive due to its engaging nature: “Since it was presented as a chat session, it had a friendly vibe to it. Was easy to stay on task.” Even with negative comments, the chatbot appeared to make data collection easier and more enjoyable to navigate for participants, suggesting chatbot could be a better way to collect data.
The assessment took significantly longer (i.e., 89.5 s more) to complete using the chatbot compared to the traditional online form. This could be due to the conversational format of the chatbot, which presents questions and information in a controlled sequence rather than presenting questions all at once. This could lead to increased scrolling to previously answered questions and more clicks while responding to questions and other presented information, ultimately leading to a longer time to complete the assessment. Qualitative analyses supported these results, showing that while some (n = 12/206) participants perceived the chatbot as time consuming, an equal number of participants (n = 12/206) noted the online form's interface felt faster: “The layout appeared simple and old-school. But I found it to be easier and faster to work on than the dokbot.” However, only 5.8% (n = 12/206) of participants reported chatbots felt time-consuming in their qualitative responses, so it is possible that the chatbot was more engaging and not perceived as taking longer to complete; one participant noted, “It seemed to move a lot quicker and less tedious” and another that “it felt interactive but took longer.” Similar findings have been attributed to engagement in previous research (11). More research focusing on the user behaviors while interacting with the chatbot and the quality of data collected could help better understand the equilibrium between experience with the chatbot and impact of completion time.
While the chatbot may have taken longer to complete than the online form, time to complete was not necessarily a negative consideration. The chatbot was reported to be faster to complete by 18 (8.7%) participants, while the online form was reported as faster by 12 (5.8%). Results show that the chatbot was still preferred, even with greater time consumption, suggesting substantial engagement and an intuitive interface have a greater weight on preferences. One participant noted this interplay, stating, “I think time seems to go faster with dokbot. It has the feel of a more personal conversation, instead of the basic form survey…” While prior research has shown that chatbots increase feelings of engagement, this study also shows engagement may supersede the ideal of quick healthcare forms (37). Consequently, patients may spend more time providing quality information to their healthcare provider. Further research with a clinical sample size is needed to determine quality and patient preference on this topic.
In addition, a few participants showed concerns for sharing personal health information via chatbot. It is possible that the lack of familiarity with the chatbot as a tool for health data collection or a third-party solution could have raised these concerns. While three participants mentioned their security concern using a chatbot, the other three instances of security concerns may be a result of participants completing a health survey in a study environment. Indeed, one of these participants felt uncomfortable, asking “…why would it need my address?”, though such information is typical in healthcare assessment forms. Additionally, mTurk educates participants and researchers not to provide specific location information, so it is possible that some participants did not notice the instructions to input a fictional address provided by the researchers (38). Ultimately, reassuring participants and communicating compliance with privacy regulations such as HIPAA and data safety could potentially alleviate these concerns. Though this study had few cases of security concerns emerge (2.9%, n = 6/206), future research should explore patients' feelings of security and appropriateness of chatbots in collecting their health data for their health care provider.
A major cause for concern in this study was the quality of the data collected via mTurk. Research has shown that careless, nonsystematic, and potential bot responses have resulted in removal of a significant amount of data in some studies (30, 31). Although our larger sample size without excluding any participants echoed current findings (chatbot preferred over online form), we observed careless and missing quantitative and qualitative responses resulting in poor data quality. To improve data quality and preserve integrity, we performed a data cleaning process informed by literature and research. These exclusions resulted in an 47.3% reduction in our sample size (i.e., 206/391). In future, researchers should consider these factors and establish more robust screening approaches and strategies to identify and avoid careless and bot responses.
Overall, our study findings establish chatbots as a modern, friendly, and intuitive approach to health data collection compared to traditional online forms or the conventional use of chatbots as therapy or education delivery mechanisms in healthcare. With the growing use of mobile devices to obtain health information, this approach can help collect high-quality, complete, more accurate data from patients, thereby enhancing the processes and workflows of health data collection (39, 40).
We recruited participants via mTurk, which may not be representative of the general population. We aimed to recruit participants who were 18 years or older but made no further specifications for age, gender, race, or education. However, our findings were consistent with previous studies with well-educated and underserved populations (11–14).
Considering the remote and unmoderated nature of this recruitment, individuals may have completed the assessments and questionnaires inaccurately or disingenuously. It is possible that individuals may have completed the assessment in a hurry or taken additional time to complete the assessment at their own convenience. In the future, researchers should ensure more objective checks and criteria for approval of mTurk responses and refer to previous research on the challenges of recruitment via public platforms such as mTurk.
Further, biases can occur from paid survey pools, specifically at low levels of compensation (41). It is possible that this study may see framing effect bias due to this recruitment approach; however, such a framing effect is more likely seen regarding questions of money and risk–topics not considered in this study.
We targeted a large-scale recruitment of 400 individuals, but this approach resulted in inclusion of only 206 individuals. The loss of statistical power could impact the generalizability of these results.
Lastly, it is possible that the preference of chatbot could be related to its conversational nature, but also could be due to other factors such as its visual and structural information representation. In this study, the chatbot and online form differed in their visual appearance and information representation. The chatbot presented a modern interface with systematic one-by-one questions compared to the online form, which presented all questions at once. The chatbot also included features such as progress tracking which were not present in the online form. Hence, the findings may not be generalizable in comparison to other modern online forms presenting one-by-one flow of questions. Future studies should compare Dokbot with other HIPAA-compliant healthcare tools designed for online clinical and research data collection.
This is one of the first studies assessing individual preferences towards two different tools for health data collection. Our findings have identified the areas of improvement for Dokbot, including completion time, information, and conversation presentation, as well as privacy and security concerns. We aim to conduct future studies to better understand these concerns and identify ways to improve Dokbot. Also, this study focused on the usability and experience of collecting data using two different interfaces: a chatbot and an online form. We did not look into the quality of data collected using these forms. Future studies should focus on assessing the data quality, including the accuracy, reliability, and completeness of health data.
Though we aimed to conduct the study with 400 participants, we have reported partial results including 206 participants. In the future, we aim to identify a better recruitment platform and conduct large scale validation of our findings. In addition, we are conducting a detailed, moderated study comparing preferences of the chatbot with online form as well as paper form. This study aims to better understand preferences with the inclusion of validated measures of perceived usefulness and ease-of-use based on the Technology Acceptance Model, cognitive and task load based on the NASA Task Load Index (NASA-TLX), and system satisfaction using the IBM Computer System Usability Questionnaire (CSUQ) (42–44).
Our study did not include many older adults (age >60 years; n = 10, 4.9%). Older adults tend to experience greater difficulty navigating online interfaces, and little research has explored their unique experiences and challenges with online health data collection (12). We are in the process of systematically reviewing the literature about chatbots for health data collection among older adults and evaluating the cognitive load, usability, and ease-of-use of chatbot-delivered health forms among 300 older adults using the platform Prolific.co (45). We chose this online platform as researchers have reported on the high quality of data collected using Prolific.co (29).
Collectively, the outcomes of these studies will help develop strategies and recommendations for improving Dokbot as a more intuitive and interactive healthcare data collection tool.
This manuscript presents an early study assessing the experience and preference of chatbots as health-data capture mechanisms. The findings demonstrate chatbots can be an intuitive and useful approach to modern healthcare data collection, increasing engagement and interaction among patients. Factors negatively influencing application of chatbots in data collection may include increased completion time and privacy concerns. However, our findings demonstrated that high engagement, intuitiveness, and interactive experience supersede the negative influences. The findings of this research will inform design and development of recommendations and best practices for chatbots for healthcare data collection.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Medical University of South Carolina. The patients/participants provided their written informed consent to participate in this study.
All authors contributed equally to conceptualization, research, and manuscript preparation. All authors contributed to the article and approved the submitted version.
This work was supported by the National Library of Medicine through Improving data capture in clinical research using a chatbot (1R41LM013419-01) grant. The content is solely a responsibility of the authors and does not necessarily represent the official views of the NLM. Dr. Bunnell was funded by the National Institute of Mental Health (Grant Numbers K23MH118482 and R41MH126734) and Dr. Welch was funded by the National Cancer Institute (Grant Number K07CA211786 and 1R41CA239867).
We thank Kurt Hills (senior technical writer, Doxy.me Inc.) for providing his time and expertise in reviewing this manuscript. We thank Dr. Kapil Madathil at Clemson University for his expertise and guidance.
Welch is a shareholder of Doxy.me Inc, Dokbot LLC, ItRunsInMyFamily.com, and Adhere.ly LLC, all of which integrate Dokbot into their software solutions. Bunnell holds a leadership position in Doxy.me Inc and is a shareholder of Adhere.ly LLC. These solutions integrate Dokbot into their software solutions. Authors Hiral Soni, Julia Ivanova, Triton Ong, Hattie Wilczewski, Alexa Narma, and Alexandra Bailey are employees of Doxy.me Inc., a commercial telemedicine company. Other authors declare no other conflicts of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Soni H, Grando A, Murcko A, Bayuk M, Chandrashekar P, Mukundan M, et al. Current state of electronic consent processes in behavioral health: outcomes from an observational study. AMIA Annu Symp Proc. (2017) 2017:1607–16. Available at: https://www.ncbi.nlm.nih.gov/pubmed/29854231
2. Commito K. How to go Paperless. HomeCare Magazine (2017). Available at: https://www.homecaremag.com/operations/june-2017/how-go-paperless (cited 2022 Apr 18).
3. Gulledge M. Go Paperless: Increase Efficiency, Lower Costs. Review of Optometric Business (2014). Available at: https://www.reviewob.com/go-paperless-increase-efficiency-lower-costs/ (cited 2022 Apr 18).
4. Breaking Down the Cost-Saving Benefits of AP Automation. AvidXchange (2021). Available at: https://www.avidxchange.com/blog/cost-saving-benefits-ap-automation-solutions-breakdown/ (cited 2022 Apr 18).
5. U.S. Department of Health and Human Services, Office for Civil Rights. Summary of the HIPAA Privacy Rule. Available at: https://www.hhs.gov/hipaa/for-professionals/privacy/laws-regulations/index.html (cited 2021 Dec 10).
6. Bowling A. Mode of questionnaire administration can have serious effects on data quality. J Public Health. (2005) 27(3):281–91. doi: 10.1093/pubmed/fdi031
7. Endacott R. Clinical research 4: qualitative data collection and analysis. Intensive Crit Care Nurs. (2005) 21:123–7. doi: 10.1016/j.iccn.2004.10.001
8. Pathak V, Jena B, Kalra S. Qualitative research. Perspect Clin Res. (2013) 4(3):192. doi: 10.4103/2229-3485.115389
9. Hennessy M, Hunter A, Healy P, Galvin S, Houghton C. Improving trial recruitment processes: how qualitative methodologies can be used to address the top 10 research priorities identified within the PRioRiTy study. Trials. (2018) 19(1):584. doi: 10.1186/s13063-018-2964-1
10. Tudor Car L, Dhinagaran DA, Kyaw BM, Kowatsch T, Joty S, Theng Y-L, et al. Conversational agents in health care: scoping review and conceptual analysis. J Med Internet Res. (2020) 22(8):e17158. doi: 10.2196/17158
11. Ponathil A, Ozkan F, Welch B, Bertrand J, Chalil Madathil K. Family health history collected by virtual conversational agents: an empirical study to investigate the efficacy of this approach. J Genet Couns. (2020) 29(6):1081–92. doi: 10.1002/jgc4.1239
12. Ponathil A, Ozkan F, Bertrand J, Agnisarman S, Narasimha S, Welch B, et al. An empirical study investigating the user acceptance of a virtual conversational agent interface for family health history collection among the geriatric population. Health Inform J. (2020) 26(4):2946–66. doi: 10.1177/1460458220955104
13. Wang C, Bickmore T, Bowen DJ, Norkunas T, Campion M, Cabral H, et al. Acceptability and feasibility of a virtual counselor (VICKY) to collect family health histories. Genet Med. (2015) 17(10):822–30. doi: 10.1038/gim.2014.198
14. Cerda Diez ME, Cortés D, Trevino-Talbot M, Bangham C, Winter MR, Cabral H, et al. Designing and evaluating a digital family health history tool for spanish speakers. Int J Environ Res Public Health. (2019) 16(24):4979. doi: 10.3390/ijerph16244979
15. Abd-Alrazaq AA, Alajlani M, Ali N, Denecke K, Bewick BM, Househ M. Perceptions and opinions of patients about mental health chatbots: scoping review. J Med Internet Res. (2021) 23(1):e17828. doi: 10.2196/17828
16. Welch BM, Allen CG, Ritchie JB, Morrison H, Hughes-Halbert C, Schiffman JD. Using a chatbot to assess hereditary cancer risk. JCO Clin Cancer Inform. (2020) 4:787–93. doi: 10.1200/CCI.20.00014
17. Palanica A, Flaschner P, Thommandram A, Li M, Fossat Y. Physicians’ perceptions of chatbots in health care: cross-sectional web-based survey. J Med Internet Res. (2019) 21(4):e12887. doi: 10.2196/12887
18. Amazon Mechanical Turk. Available from: https://www.mturk.com/ (cited 2022 May 11).
19. Brooke J. SUS: a quick and dirty usability scale. In: Jordan PW, Thomas B, McClelland IL, Weerdmeester B, editors. Usability evaluation in industry. CRC Press (1996). p. 189–94.
20. Your Guide to Net Promoter Score (NPS) in 2022. Qualtrics (2020). Available at: https://www.qualtrics.com/experience-management/customer/net-promoter-score/ (cited 2022 May 11).
21. Allen M. Counterbalancing. Available at: https://methods.sagepub.com/reference/the-sage-encyclopedia-of-communication-research-methods/i3526.xml (cited 2022 Apr 27).
22. Marler W. Mobile phones and inequality: findings, trends, and future directions. New Media / Society. (2018) 20(9):3498–520. doi: 10.1177/1461444818765154
23. Topic: Mobile internet usage worldwide. Statista. Available at: https://www.statista.com/topics/779/mobile-internet/ (cited 2022 May 13).
24. Dokbot: A better way to collect data from patients. Available at: https://dokbot.io/ (cited 2021 Oct 1).
25. Software – REDCap. Available at: https://www.project-redcap.org/software/ (cited 2022 Feb 19).
26. REDCap. Available at: https://www.project-redcap.org/ (cited 2022 May 11).
27. Acquiescence Bias: What it is / How to Stop it . Qualtrics (2020). Available at: https://www.qualtrics.com/blog/avoiding-the-yes-bias/ (cited 2022 Apr 19).
28. Sauro J. A practical guide to the system usability scale- background, benchmarks / best practices. Denver, Colorado: Measuring Usability LLC (2011).
29. Eyal P, David R, Andrew G, Zak E, Ekaterina D. Data quality of platforms and panels for online behavioral research. Behav Res Methods. (2021) 54:1643–62. doi: 10.3758/s13428-021-01694-3
30. Kennedy R, Clifford S, Burleigh T, Waggoner PD, Jewell R, Winter NJG. The shape of and solutions to the MTurk quality crisis. Political Sci Res Methods. (2020) 8(4):614–29. doi: 10.1017/psrm.2020.6. Available from: https://www.cambridge.org/core/services/aop-cambridge-core/content/view/521AEEB9A9753D5C6038440BD123826C/S2049847020000060a.pdf/div-class-title-the-shape-of-and-solutions-to-the-mturk-quality-crisis-div.pdf (cited 2022 Apr 25).
31. Chmielewski M, Kucker SC. An MTurk crisis? Shifts in data quality and the impact on study results. Soc Psychol Personal Sci. (2020) 11:464–73. doi: 10.1177/1948550619875149
32. Barends AJ, de Vries RE. Noncompliant responding: comparing exclusion criteria in MTurk personality research to improve data quality. Pers Individ Dif. (2019) 143:84–9. doi: 10.1016/j.paid.2019.02.015. Available at: https://www.sciencedirect.com/science/article/pii/S0191886919300972
33. MacInnis CC, Boss HCD, Bourdage JS. More evidence of participant misrepresentation on mturk and investigating who misrepresents. Pers Individ Dif. (2020) 152:109603. doi: 10.1016/j.paid.2019.109603. Available at: https://www.sciencedirect.com/science/article/pii/S0191886919305355
34. Dennis SA, Goodson BM, Pearson C. (2019). Online Worker Fraud and Evolving Threats to the Integrity of MTurk Data: A Discussion of Virtual Private Servers and the Limitations of IP-Based Screening Procedures. Available at: https://papers.ssrn.com/abstract=3233954 (cited 2022 Apr 25).
35. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3(2):77–101. doi: 10.1191/1478088706qp063oa. Available at: https://www.tandfonline.com/doi/abs/10.1191/1478088706qp063oa
36. Hyzy M, Bond R, Mulvenna M, Bai L, Dix A, Leigh S, et al. System usability scale benchmarking for digital health apps: meta-analysis. JMIR Mhealth Uhealth. (2022) 10(8):e37290. doi: 10.2196/37290
37. Schuetzler RM, Grimes GM, Giboney J. An Investigation of Conversational Agent Relevance, Presence, and Engagement. AMCIS (2018). Available at: https://www.semanticscholar.org/paper/c1e3b89480ddf56c4015c524933eb00da3379ff0 (cited 2022 Apr 25).
38. Mechanical Turk (MTurk). (2020). Available at: https://www.compliance.iastate.edu/sites/default/files/imported/irb/guide/docs/MTurk-guidance.pdf
39. Heimlich R. More Use Cell Phones to Get Health Information. Pew Research Center (2012). Available at: https://www.pewresearch.org/fact-tank/2012/11/14/more-use-cell-phones-to-get-health-information/ (cited 2022 Apr 18).
40. Hamou A, Guy S, Lewden B, Bilyea A, Gwadry-Sridhar F, Bauer M. Data collection with iPhone web apps efficiently collecting patient data using mobile devices. The 12th IEEE international conference on e-health networking, applications and Services (2010). p. 235–9. doi: 10.1109/HEALTH.2010.5556565
41. Goodman JK, Cryder CE, Cheema A. Data collection in a flat world: the strengths and weaknesses of mechanical Turk samples. J Behav Decis Mak. (2013) 26(3):213–24. doi: 10.1002/bdm.1753. Available at: https://onlinelibrary.wiley.com/doi/10.1002/bdm.1753
42. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. Miss Q. (1989) 13(3):319–40. doi: 10.2307/249008. Available at: http://www.jstor.org/stable/249008
43. Lewis JR. IBM Computer usability satisfaction questionnaires: psychometric evaluation and instructions for use. Int J Hum-Comput Interact. (1995) 7(1):57–78. doi: 10.1080/10447319509526110
44. Hart SG, Staveland LE. Development of NASA-TLX (task load Index): results of empirical and theoretical research. In: Hancock PA, Meshkati N, editors. Advances in psychology, North-Holland (1988). p. 139–83. Available at: https://www.sciencedirect.com/science/article/pii/S0166411508623869
45. Quickly find research participants you can trust. Available from: https://www.prolific.co/ (cited 2022 Apr 18).
Keywords: health data collection, patient experience, virtual conversational agents, chatbots, usability
Citation: Soni H, Ivanova J, Wilczewski H, Bailey A, Ong T, Narma A, Bunnell BE and Welch BM (2022) Virtual conversational agents versus online forms: Patient experience and preferences for health data collection. Front. Digit. Health 4:954069. doi: 10.3389/fdgth.2022.954069
Received: 26 May 2022; Accepted: 16 September 2022;
Published: 13 October 2022.
Edited by:
Niranjan Bidargaddi, Flinders University, AustraliaReviewed by:
Richard Leibbrandt, Flinders University, Australia© 2022 Soni, Ivanova, Wilczewski, Bailey, Ong, Narma, Bunnell and Welch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hiral Soni aGlyYWwuc29uaUBkb3h5Lm1l
Specialty Section: This article was submitted to Human Factors and Digital Health, a section of the journal Frontiers in Digital Health
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.