
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Digit. Health , 29 March 2022
Sec. Connected Health
Volume 4 - 2022 | https://doi.org/10.3389/fdgth.2022.864003
This article is part of the Research Topic Digital Technology for Tobacco Control: Novel Data Collection, Study Designs, and Interventions View all 9 articles
 Lizbeth Benson1*
Lizbeth Benson1* Chaelin K. Ra1
Chaelin K. Ra1 Emily T. Hébert2Darla E. Kendzor1,3Jason A. Oliver1,3Summer G. Frank-Pearce1,4Jordan M. Neil1,3Michael S. Businelle1,3
Emily T. Hébert2Darla E. Kendzor1,3Jason A. Oliver1,3Summer G. Frank-Pearce1,4Jordan M. Neil1,3Michael S. Businelle1,3Background: Smoking urges and negative affect play important roles in daily cigarette smoking and smoking lapse during a cessation attempt. Traditionally, laboratory research has considered negative affect as a potential cause of smoking urges. A deeper understanding of momentary associations between negative affect and smoking urges during a smoking cessation attempt can inform treatment development efforts. This study examined whether the within-person association between negative affect and smoking urges differed before and after a quit attempt, and by intervention type.
Methods: Data are from a pilot randomized controlled trial comparing 3 smoking cessation interventions. Participants were randomly assigned to: (1) a novel, smartphone-based just-in-time adaptive intervention that tailored treatment content in real-time (Smart-T2; n = 24), (2) the National Cancer Institute QuitGuide app (n = 25), or (3) a clinic-based tobacco cessation program (TTRP; n = 23) that followed Clinical Practice Guidelines. All participants received up to 12 weeks of nicotine replacement therapy and completed up to 5 assessments per day (MPreQuit= 25.8 assessments, SD = 6.0; MPostQuit= 107.7 assessments, SD = 37.1) of their negative affect and smoking urges during the 7 days (M = 6.6 days, SD = 1.0) prior to their quit-date and the 29 days (M = 25.8 days, SD = 6.4) after their quit-date. Prior to analysis, repeated measures of smoking urges were decomposed into between-person and within-person components.
Results: After accounting for baseline nicotine dependence, Bayesian multilevel models indicated that the extent of within-person association between negative affect and smoking urges was stronger in the post-quit stage of the intervention than the pre-quit stage. Results also indicated that in the post-quit stage of the intervention, the within-person association between negative affect and smoking urges was weaker for those in the Smart-T2 and TTRP groups compared with those in the QuitGuide group. The extent of this within-person association did not differ between those in the Smart-T2 and TTRP groups.
Conclusions: These findings offer preliminary evidence that the momentary within-person association between negative affect and smoking urges increases following a quit attempt, and that the TTRP and Smart-T2 interventions may weaken this association. Research is needed to replicate and expand upon current findings in a fully powered randomized controlled trial.
Clinical Trial Registration: ClinicalTrials.gov NCT02930200; https://clinicaltrials.gov/show/NCT02930200.
Tobacco dependence is a recurring, relapsing condition (1). While most smokers want to quit, fewer than one-third of smokers use evidence-based treatments such as medication or behavioral counseling during quit attempts (2), and most smokers require several attempts before they successfully quit (3). Measurement strategies such as ecological momentary assessment (EMA), which utilize frequent self-report about behaviors and experiences in real-time (4), have allowed researchers to better understand the complicated dynamics of thoughts, feelings, and situational contexts that smokers experience during the course of a quit attempt (5). Many EMA studies have examined momentary correlates of smoking lapse during a quit attempt, including cravings (6), proximity to other smokers (7), and recent alcohol use (8).
Smoking urges and negative affect have emerged as important predictors of smoking behaviors, as well as risk factors for lapse during smoking cessation attempts (9–14). In controlled laboratory manipulations of negative affect among dependent smokers, there is strong evidence that negative affect evokes craving to smoke (15). Similarly, the findings of research examining cue-reactivity to experimentally manipulated negative affect have indicated that negative affect is associated with more ad libitum smoking (16). Further, research conducted in daily life settings has found that individuals tend to experience higher negative affect on stressor days compared to non-stressor days (17, 18). This body of work has conceptualized the extent of within-person association between stress and negative affect as reactivity. In addition to more traditionally measured stressors, such as arguments with a loved one or difficulties at work, momentary increases in smoking urges may be a particularly salient daily life stressor for individuals who are trying to quit smoking. Prior research has provided some evidence of momentary within-person associations between negative affect and smoking urges (19). However, little is known about how the momentary within-person association between negative affect and smoking urges may change following the initiation of a smoking cessation attempt. In addition, it is unclear whether the strength of this association may differ based on intervention type.
Given the dynamic nature of contextual factors contributing to increased risk of smoking lapse during a quit attempt, emerging strategies such as just-in-time adaptive interventions (JITAIs), have become increasingly relevant (20). JITAIs aim to address states of vulnerability for health behaviors (such as high-risk situations) by providing support in real-time through mobile technology (21). Decision rules are used to determine when and how to provide treatment in the relevant moment. To date, most JITAIs for substance use behaviors have used decision rules that assumed predictors of substance use were time-invariant (22). Although tailored intervention content delivered in real-time has the potential to attenuate the effect of smoking urges and negative affect on the risk of smoking lapse, a deeper understanding of the momentary, quit-stage dependent, within-person association between negative affect and smoking urges is needed to further refine these decision rules.
To advance our understanding of which psychological factors may contribute to cessation-related experiences in daily life, the present study used EMA data to assess the momentary within-person association between negative affect and smoking urges in a sample of adults receiving a smoking cessation intervention. Data were analyzed using multilevel modeling to examine (1) the extent of momentary within-person association between negative affect and smoking urges during a quit attempt, (2) whether the extent of this within-person association changed from the pre-quit to the post-quit stage of the study, and (3) whether the assigned intervention type moderated the degree of this within-person association.
A total of 81 individuals participated in the parent study. Of these participants, 9 were excluded for lack of compliance with the study protocol (see data analysis section for minimum compliance criteria). Participants in the analytic sample (nTotal = 72; nSmart−T2= 24, nQuitGuide= 25, nTTRP= 23) were, on average, 50.17 years of age (SD = 11.92, Range = 23–73 years), 49% female, 64% White (24% Black or African American, 1% Native Hawaiian or Other Pacific Islander, 6% American Indian/Alaska Native, and 5% Other), and 3% Hispanic/Latino. Participants were recruited from provider or self-referrals to the Tobacco Treatment Research Program (TTRP), located at the University of Oklahoma Health Sciences Center in Oklahoma City, Oklahoma. Individuals were eligible to participate if they (1) demonstrated an English literacy level greater than the sixth grade, (2) were willing to quit smoking 7 days from their first visit, (3) were ≥18 years of age, (4) had an expired carbon monoxide (CO) level >7 ppm suggestive of current smoking, (5) were currently smoking ≥5 cigarettes per day, (6) were willing and able to attend 4 in-person assessment sessions, and (7) had no contraindications for over-the-counter nicotine replacement therapy (NRT; i.e., uncontrolled blood pressure, myocardial infarction within the past 2 weeks, or current pregnancy or plans to become pregnant during the study period). All participants provided informed consent and received compensation for their participation.
All study procedures were approved by the Institutional Review Board at the University of Oklahoma Health Sciences Center. The intervention procedure has been described in detail elsewhere (23). Relevant to the present study, all participants completed an in-person assessment at baseline, 7 days of EMAs pre-quit, an in-person assessment on their quit date, and an additional 29 days of EMA following the scheduled quit date. At the baseline in-person assessment, study personnel provided all participants with a smartphone (Samsung Galaxy On5) and trained them how to use the device to complete the EMA portion of the study. Participants also provided information on the typical time they woke up and went to sleep for each day of the week. This information was used to set the time of EMAs so that they were not scheduled when the participant was likely to be sleeping. On the first and last days of EMA, participants were prompted to respond to one daily diary. On days 2 through 35, participants were prompted 5 times per day, starting with a daily diary assessment ~30 min after waking and 4 subsequent random assessments, finishing no later than the participants' self-reported bedtime for the given day. Data collected on the smartphone app were deidentified and encrypted. In addition to the daily diary and random assessments, participants could also self-initiate EMAs at times when they felt an urge to smoke or times when they had already smoked.
At baseline, participants were randomized into either the (1) Smart-T2 smartphone-based smoking cessation app Smart-T2, (2) National Cancer Institute QuitGuide app, or (3) tobacco cessation clinic care (TTRP). Intervention types and study procedures have been described in detail previously (23, 24). Briefly, the Smart-T2 app featured just-in-time treatment messages delivered at the end of each EMA. Treatment messages were tailored to a participant's current risk of smoking lapse, determined by a weighted algorithm, as well as the highest rated of four momentary lapse triggers: urge to smoke, stress, cigarette availability, and low motivation to quit. The weighted algorithm was developed in a prior study that examined the optimal weight to assign to momentary responses for each of six lapse triggers (urge to smoke, stress, cigarette availability, interacting with someone smoking, recent alcohol use, and cessation motivation), by comparing the extent to which the estimator distinguished between moments of high vs. low risk for imminent smoking lapse in the next 4 hours (25). Results from that study showed that the final weighted lapse risk estimator successfully identified 80% of all first smoking lapses within 4 h of the smoking lapse. This lapse risk estimator was integrated into and informs the real-time tailoring of intervention messages for the Smart-T1 (24) and Smart-T2 JITAIs (23). The Smart-T app also featured on-demand quit tips. The NCI QuitGuide app (26, 27) is a free smartphone app available through Smokefree.gov and includes on-demand content such as the ability to track cravings, smoking triggers, and quit tips. Finally, the TTRP group received usual tobacco cessation treatment based on established clinical practice guidelines (28), including weekly individual counseling sessions. All three groups received a 2-week supply of over the counter nicotine replacement therapy (NRT; i.e., patches, gum, or both) and participants could request up to 8 additional weeks of NRT.
Five times per day, all participants were prompted via smartphone to report their current experiences of negative affect, smoking urges, and smoking behaviors during the week prior to their quit date and the 4 weeks subsequent to their quit date.
During each daily diary and random assessment, participants answered questions about their negative emotion experiences, chosen to span both high activation (i.e., stress, anxious, frustrated/angry, irritable, worried, and restless) and low activation (i.e., depressed, sad, and miserable) quadrants of the circumplex model (29). Response options for each of these questions ranged from Strongly Disagree (=1) to Strongly Agree (=5). The average within-person correlations among the negative emotion items were moderate to strong during both the pre-quit (Range = 0.31–0.56) and post-quit (Range = 0.31–0.52) stages of the study. Thus, a negative affect composite was computed as the average response to the nine discrete negative emotion items at each EMA. Additionally, we computed a high activation negative affect composite (irritable, frustrated/angry, worried, restless, anxious, stressed) and a low activation negative affect composite (sad, miserable, depressed) for each EMA to use in a set of secondary analyses (29).
During each daily diary and random assessment, participants reported on the extent to which they currently had an urge to smoke. Response options ranged from Strongly Disagree (=1) to Strongly Agree (=5).
To quantify quit stage in terms of pre-quit date vs. post-quit date, each of the seven days prior to each participant's scheduled quit date were recoded as 0 and each of the 29 days on or after each participant's quit date were recoded as 1.
Three dummy coded variables were created to indicate whether participants received the Smart-T2 intervention app (0 = no, 1 = yes), whether participants received the QuitGuide intervention app (0 = no, 1 = yes), and whether participants received the TTRP intervention (0 = no, 1 = yes). Given that there were three intervention treatment groups, only two dummy coded variables were used at a time. Three dummy coded variables were created so that, across two sets of analyses, treatment group differences across all three groups could be statistically evaluated.
During the baseline assessment, participants answered two items that comprise the Heaviness of Smoking Index (HSI) (30). First, participants responded to the question: At present, how long after waking do you wait before having your first cigarette (in minutes)?, using response options of 61+ min (=0), 31–60 min (=1), 6–30 min (=2), and ≤ 5 min (=3). Second, participants responded to the question: How many cigarettes do you smoke per day at present?, using response options of 1–10 cigarettes (=0), 11–20 cigarettes (=1), 21–30 cigarettes (=2), and 31+ cigarettes (=3). A smoking dependence composite was then computed as the sum of scores from the two items from each participant.
Using all available data (daily diaries, random assessments, participant-initiated urge assessments, participant-initiated smoking assessments), a momentary “smoked yet today” variable was calculated. Specifically, for a given moment within a day, participants received a score of zero if they had not reported any smoking during that assessment or in any previous assessment that day, whereas they received a score of one if they reported smoking during that assessment or in any previous assessment that day.
Several demographic variables were included as covariates in secondary models including Gender (Male = 0, Female = 1), Race (0 = Non-white, 1 = White, given that the majority of the sample reported their race as White), Age (M = 50.2 years, SD = 11.8), Education (completed ≤ high school/GED = 0, at least some college = 1), and Employment (working less than full time = 0, working full time = 1).
Momentary occasions were included in the analyses if the participant provided complete data for negative affect and smoking urge. Nine participants were excluded from the analysis sample because they did not participate in both the pre-quit and post-quit stages of the study (n = 4), or because they did not have at least 5 measurement occasions with complete data for the main analysis variables in each stage of the study (n = 5). Participants excluded from the analysis sample were relatively evenly distributed across the Smart-T2 (n = 3), QuitGuide (n = 2), and TTRP (n = 4) treatment groups. Participants included in the analyses (nTotal= 72) provided on average 25.8 pre-quit momentary assessments (SD = 6.0, Min = 5, Max = 31), and 107.7 post-quit momentary assessments (SD = 37.1, Min = 6, Max = 140). Altogether, 67% of the sample completed at least 75% of the prompted momentary assessments. Momentary assessments were uniformly completed across days such that, on average, participants responded to at least one assessment during 6.6 of the 7 pre-quit days (SD = 1.0, Min = 2, Max = 8), and 25.8 of the 29 post-quit days (SD = 6.4, Min = 2, Max = 29).
Data preparation steps included separating time-varying predictor variables into the between-person and within-person components (31). The time-invariant between-person component, SmokeUrgeBPi, was calculated as the intraindividual mean across the repeated measures of smoking urges, yielding one score per person. Similarly, the momentary within-person component, SmokeUrgeWPit was calculated for each observation for each person as the deviation from their intraindividual mean (SmokeUrgeBPi). Prior to analysis, the between-person components for smoking urges (SmokeUrgeBPi) and baseline smoking dependence (BaselineHSIi) were sample-mean centered to facilitate interpretation with respect to the prototypical person in the sample.
To examine (1) the extent of within-person association between negative affect and smoking urges and (2) whether quit stage moderates the extent of within-person association between negative affect and smoking urges, we fit a multilevel linear regression model,
where repeated measures of negative affect for participant i during moment t are modeled as a function of a person-specific intercept, β0i, changes driven by concurrent smoking urges, β1i, changes driven by pre- vs. post-quit stage, β2i, the interplay between smoking urges and quit stage, β3i, and residual differences, eit. Person-specific coefficients were simultaneously modeled as a function of person-level predictors,
where γ00, γ10, γ20, and γ30, and are sample-level parameters describing the prototypical person, and γ01, γ02, γ03, and γ04, describe how individual differences in smoking urges, baseline smoking dependence, and intervention treatment group are associated with participants' negative affect. Random effects (u0i, u1i, u2i, u3i) were allowed to co-vary with one another, but not with eit. Additionally, we examined whether the results held after accounting for demographic variables.
To examine whether intervention type moderates the within-person association between negative affect and smoking urges, we fit a multilevel linear regression model,
where repeated measures of negative affect for participant i during moment t are modeled as a function of a person-specific intercept, β0i, changes driven by concurrent smoking urges, β1i, and residual differences, eit. Person-specific coefficients were simultaneously modeled as a function of person-level predictors,
where γ00 and γ10 and are sample-level parameters describing the prototypical person, and γ01, γ02, γ03, γ04, γ11, γ12, describe how individual differences in smoking urges, baseline smoking dependence, and intervention treatment group are associated with participants' negative affect and/or moderate the within-person association between smoking urges and negative affect. Random effects (u0i, u1i) were allowed to covary with one another, but not with eit. Additionally, we examined whether the results held after accounting for demographic variables.
For those individuals included in the analytic sample (i.e., those who had at least 5 days of complete data for each quit stage), missing data were relatively low for the pre-quit (17% across all people and all possible assessments) and post-quit (24% across all people and all possible assessments) stages. Thus, we treated missing data as missing at random. All analyses were performed in R version 4.1.1. and R Studio version 2021.09.0 (32, 33). All figures were created in R using the ggplot2 package (34). The brms package was used to fit the multilevel models specified above in the Bayesian statistical framework to facilitate model convergence with a full random effects structure. For each model, estimation included two chains and we specified default weakly informative prior probability distributions (35, 36). The first 1,000 samples from each chain were used for the “warm-up” phase of the sampling algorithm, and discarded. Another 8,000 samples were run in each chain after warm-up, and these 16,000 samples were used to estimate the mean for a point estimate (labeled as Estimate in the model result tables), and the 95% credible interval (labeled as 95% CI in the model result tables). The 95% CI can be interpreted as a 95% probability that the true parameter is contained in the interval.
Descriptives for and correlations among main study variables are presented in Table 1. The average intensity of momentary negative affect was similar across the pre-quit stage (M = 2.1 SD = 0.7) and the post-quit stage (M = 2.1 SD = 0.8) of the study. The average intensity of smoking urges was descriptively slightly higher during the pre-quit stage (M = 3.1, SD = 0.7) compared with the post-quit stage (M = 2.8, SD = 0.9) of the study. Given that participants were instructed to smoke as usual during the pre-quit stage, smoking rates were relatively high such that for 86% of the pre-quit moments, participants had already smoked at some point in the day. For the post-quit stage, smoking rates were much lower such that participants had already smoked at some point in the day for only 26% of the post-quit moments. Similarly, on average, participants smoked at least once per day for 80% (SD = 22.5, Min = 0%, Max = 100%) of their pre-quit days and smoked at least once per day for 36% (SD = 37.3, Min = 0%, Max = 100%) of their post-quit days. Prior to the main analyses, we calculated intraclass correlation coefficients to examine how much variance in the variables pertinent to the present study could be attributed to the momentary and person levels of analysis. For negative affect, 33% of the variation could be considered within-person variation, with the remaining 67% considered between-person variation. For smoking urges, 56% of the variation could be considered within-person variation and 44% could be considered between-person variation. Given considerable variation at both levels of analysis for negative affect (the outcome variable), we proceeded to fit the multilevel models. Results are described in the following sections and reported in Table 2.
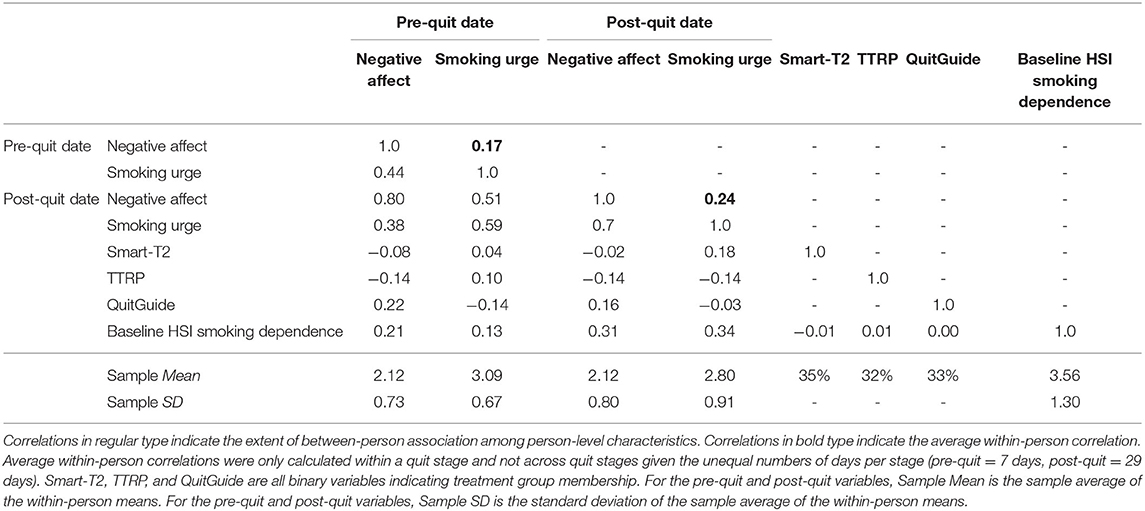
Table 1. Descriptives and correlations (between- and within-person) among study variables.
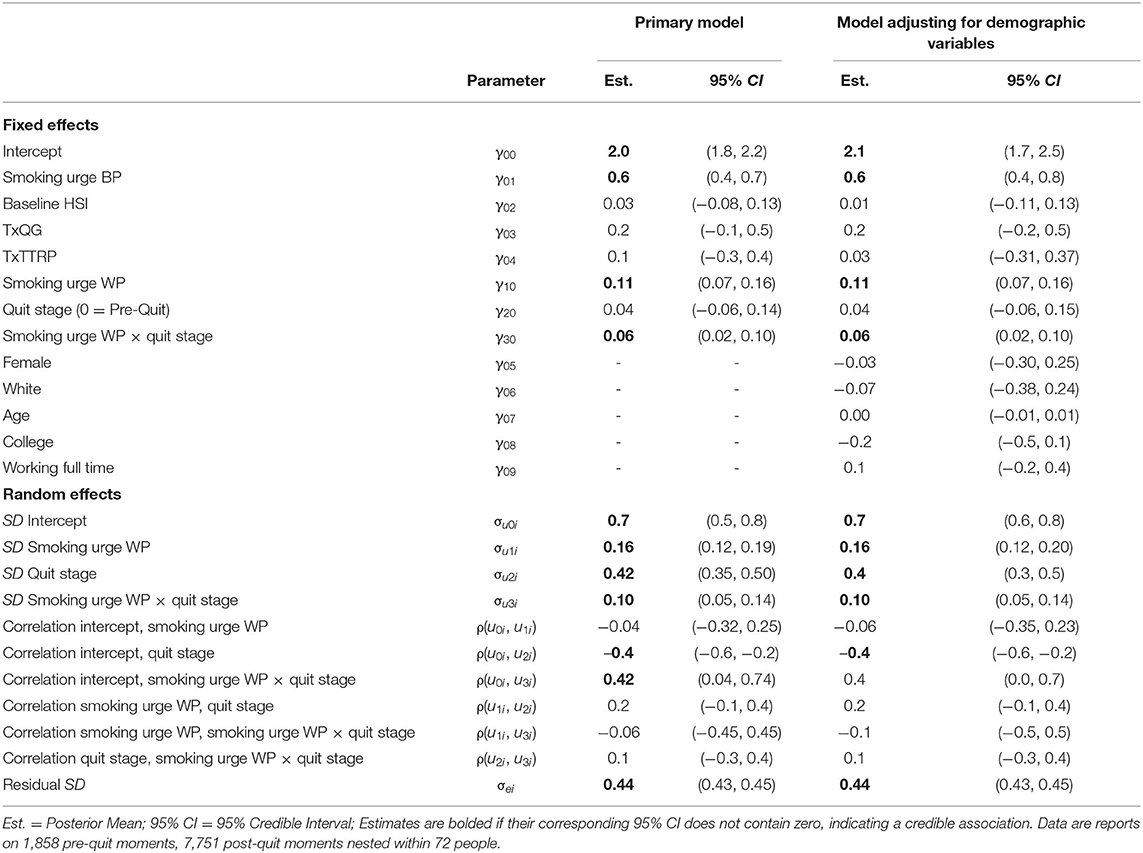
Table 2. Results from multilevel models examining differences in within-person negative affect association with smoking urges based on quit stage.
First, we examined whether the extent of within-person association between negative affect and smoking urges differed by quit stage (pre- vs. post-quit). The results indicated that for the prototypical participant assigned to the Smart-T2 intervention (the reference group), with average baseline smoking dependence and average momentary smoking urges, their average level negative affect was expected to be 2.0 (γ00) on pre-quit occasions. Further, the results showed that individuals' average level of negative affect did not credibly differ from pre-quit date to post-quit date (γ20 = 0.04). However, the results indicated that individuals in the sample credibly differed from one another in their average levels of negative affect during the pre-quit (σu0 = 0.7) and post-quit (σu2 = 0.4) stages of the study. Additionally, between-person differences in smoking urges were credibly associated with between-person differences in negative affect such that those who tended to have more intense smoking urges, on average, over the course of the study period also tended to have higher negative affect (γ01 = 0.6).
Within-person variation in smoking urges were also credibly associated with negative affect (γ10 = 0.1). Further, the extent of within-person association between negative affect and smoking urges was moderated by quit stage (γ30 = 0.1). As shown in Figure 1, there was a stronger association between smoking urges and negative affect during the post-quit stage of the intervention (green solid line) compared with the pre-quit stage of the intervention (coral dashed line). The results also showed that there was considerable heterogeneity across participants in the strength of the within-person association between negative affect and smoking urges during the pre-quit (σu1 = 0.2) and post-quit (σu2 = 0.1) stages (shown by the faint coral and green lines in Figure 1), and that those who tended to have higher average negative affect during the pre-quit stage also tended to have stronger links between their negative affect and their smoking urges during the post-quit stage [ρ(u0i, u3i)], but not the pre-quit stage [ρ(u0i, u1i)]. All results held after accounting for demographic covariates (see right two columns of Table 2).
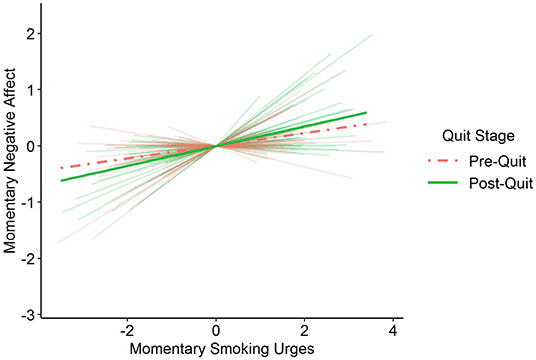
Figure 1. Prototypical within-person association between momentary smoking urges and momentary negative affect moderated by quit stage [pre-quit date (0 = study days 0 through 6), post-quit date (1 = study days 7 through 35)]. Individuals' negative affect and smoking urges were coupled to a greater extent during the post-quit stage (green solid line) compared with the pre-quit stage (coral dashed line). Faint background lines show the range of between-person differences in the within-person association between smoking urges and negative affect during both the pre-quit (coral) and post-quit (green) stages.
Second, we examined whether the extent of within-person association between negative affect and smoking urges differed by intervention type during the post-quit stage of the study. As shown in Figure 2, the results indicated that those who received the Smart-T2 intervention (the reference group; γ10 = 0.16) showed a weaker association between their momentary experiences of negative affect and smoking urges compared with those who received the QuitGuide intervention (γ11 = 0.1) during the post-quit stage of the study. In contrast, the extent of the within-person association between negative affect and smoking urges did not differ between those who received the Smart-T2 intervention and those who received the TTRP intervention (γ12 = −0.1). We also re-ran the analysis, re-specifying the TTRP group as the reference to examine whether the extent of association differed between those assigned to TTRP and those assigned to QuitGuide. The results showed that those who received the TTRP intervention showed a weaker association between their momentary experiences of negative affect and smoking urges (the reference group; γ10 = 0.10) compared with those who received the QuitGuide intervention (γ11 = 0.2). Similar to the prior section, all results held after accounting for demographic covariates (see third model in Table 3).
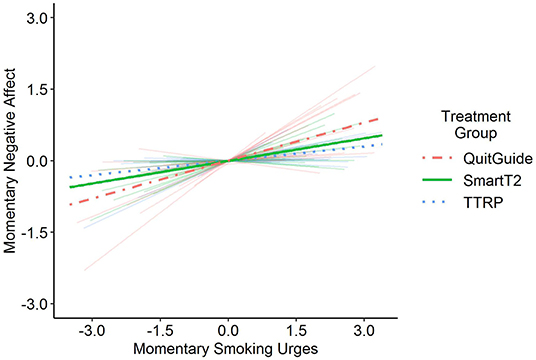
Figure 2. The within-person association between momentary negative affect and smoking urges was moderated by intervention type during the post-quit stage of the study. Specifically, those who received SmartT2 (green solid line) and TTRP (blue dotted line) did not differ from one another in the extent to which their momentary negative affect experiences were associated with their momentary smoking urges. Additionally, those who received QuitGuide (coral dashed line) showed a stronger within-person association between their experiences of negative affect and smoking urges compared with those who received SmartT2 and those who received TTRP. The faint background lines depict person-specific associations.
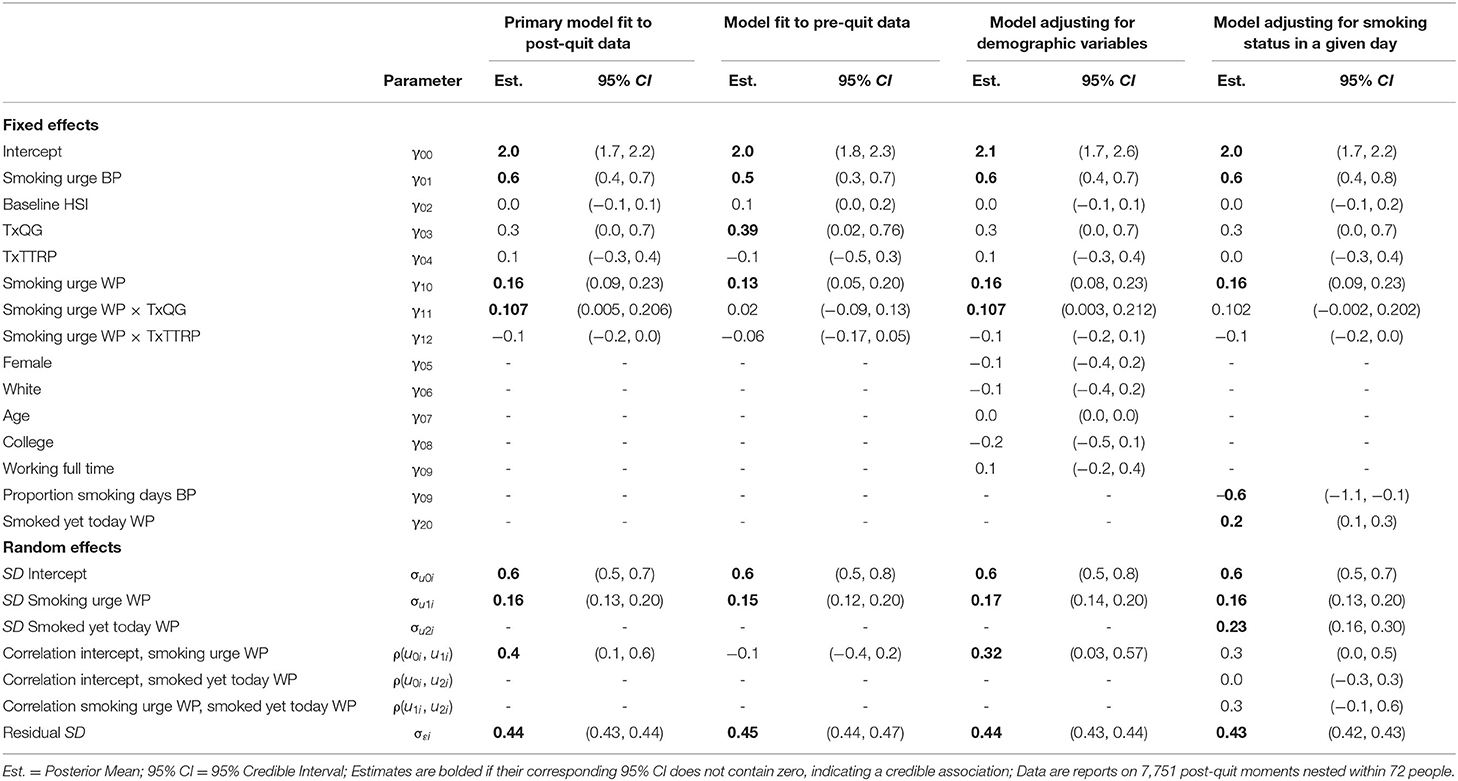
Table 3. Results from multilevel models examining differences in within-person negative affect association with smoking urges based on mHealth intervention type.
As an additional check, we re-ran the analysis, applied to just the pre-quit data when exposure to the interventions was still relatively low and when individuals were not actively trying to quit smoking. As expected, the results showed that during the pre-quit stage of the study, there were no credible differences in the extent of within-person association between negative affect and smoking urges attributed to intervention type (γ10 = 0.13, γ11 = 0.02, γ12 = −0.06; second model in Table 3). For ease of presentation and interpretation, we fit the model separately to the pre-quit data and post-quit data. The results were similar though when the model was simultaneously fit to the pre- and post-quit data such that there was a credible 3-way interaction involving momentary smoking urges, intervention stage, and treatment group.
As a sensitivity check, we fit an additional model examining whether intervention type differences in association still held after accounting for whether in a given moment the participant had smoked yet that day. Although the posterior mean estimate was similar to the primary model (γ11_PrimaryModel = 0.11, γ11_SensitivityModel = 0.10), the credible interval included zero for the sensitivity model. In other words, after accounting for whether a participant smoked yet in a given day, there were no longer credible differences in the extent of within-person association between negative affect and smoking urges based on whether the participant received Smart-T2 or QuitGuide. Similar to the primary model, the results showed that the within-person association between negative affect and smoking urges did not differ for those in the Smart-T2 and TTRP groups (γ11_SensitivityModel = −0.07). Also similar to the primary model, when we re-fit the sensitivity analysis model with TTRP specified as the reference group, those in the QuitGuide group showed a stronger within-person association between their negative affect and smoking urges compared with those in the TTRP group during the post-quit stage (γ11_SensitivityModel = 0.2).
In a set of secondary analyses, we examined whether the results differed based on the activation of the negative affect composites. Results are presented in Table 4.
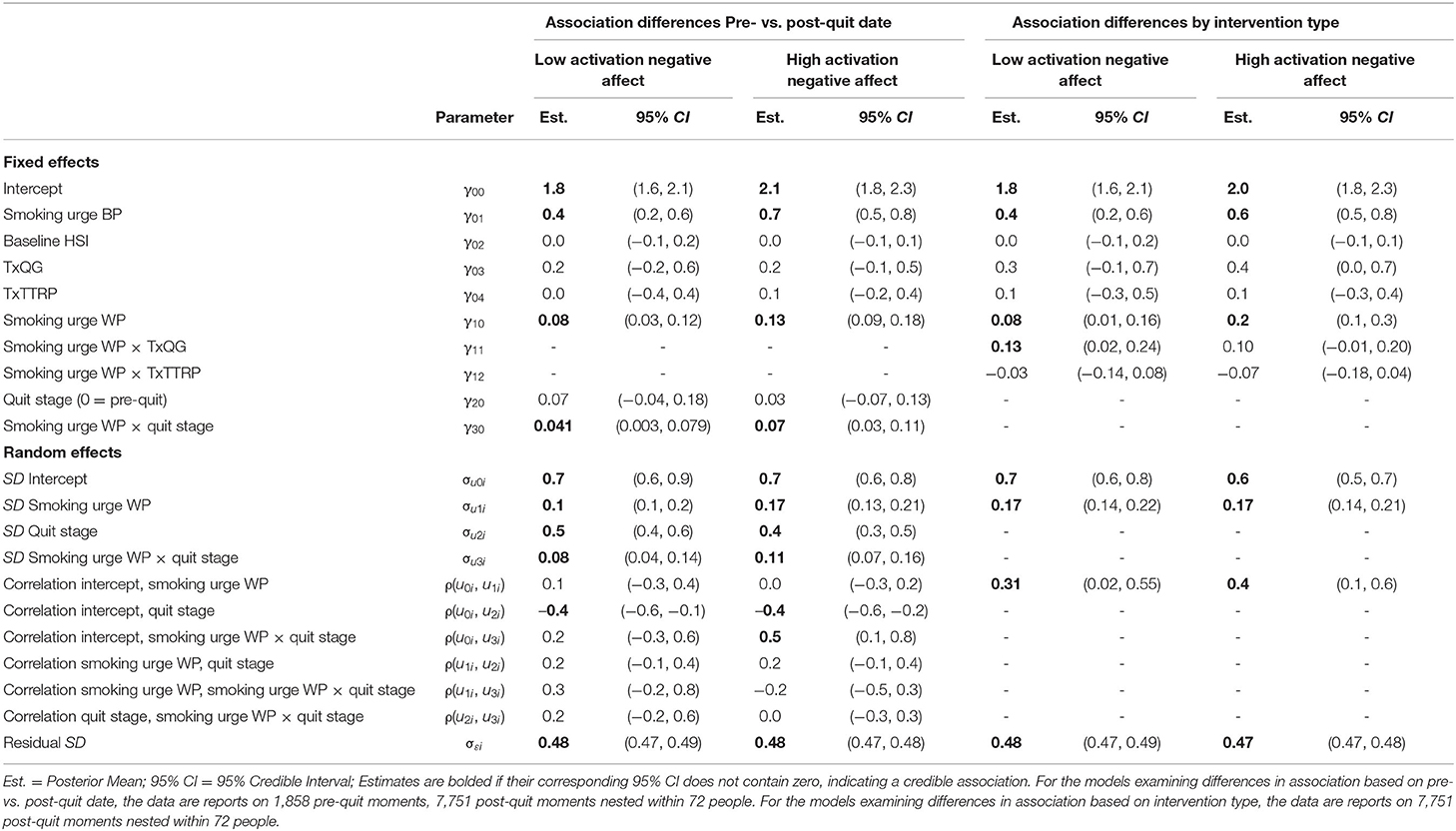
Table 4. Results from secondary analyses examining negative affect association with smoking urges based on low activation and high activation negative affect.
First, we examined whether the extent of within-person association between negative affect and smoking urges differed by quit stage using the low activation negative affect composite and the high activation negative affect composite. The results showed that for both low activation negative affect and high activation negative affect, the extent of within-person association between negative affect and smoking urges was stronger during the post-quit stage of the study compared with the pre-quit stage of the study (γ30 = 0.04, γ30 = 0.07, respectively).
Second, we examined whether the extent of within-person association between negative affect and smoking urges differed by intervention type during the post-quit stage using the low activation negative affect composite and the high activation negative affect composite. The results indicated that those who received the Smart-T2 intervention (the reference group; γ10 = 0.08) showed a weaker within-person association between their momentary experiences of low activation negative affect and smoking urges compared with those who received the QuitGuide intervention (γ11 = 0.13). Although the posterior mean estimate was similar to the prior model and the original model (γ11 = 0.13), there was not a credible difference between the Smart-T2 and QuitGuide groups in the extent of within-person association between high activation negative affect and smoking urges. Similar to the primary model, for both low activation negative affect and high activation negative affect, the extent of within-person association between negative affect and smoking urges did not differ between those who received the Smart-T2 intervention and those who received the TTRP intervention (γ12 = −0.03, γ12 = −0.07, respectively). Also similar to the primary model, when we re-fit the sensitivity analysis model with TTRP specified as the reference group, those who received QuitGuide group showed a stronger within-person association between their momentary experiences of negative affect and smoking urges, for both low activation negative affect and high activation negative affect during the post-quit stage (γ11 = 0.2, γ11 = 0.2, respectively).
The present study is the first to use EMA data to examine how within-person associations between negative affect and smoking urges change across pre-quit and post-quit stages of a smoking cessation attempt, and differ based on intervention type. Results indicated that in moments when individuals' smoking urges were higher than usual, their negative affect also tended to be higher than usual. Second, we found that the extent of within-person association between negative affect and smoking urges was stronger during the post-quit stage compared with the pre-quit stage of the study. Third, we found that the within-person association between post-quit negative affect and smoking urges did not differ for those assigned to the Smart-T2 and TTRP groups. In contrast, those who received the QuitGuide intervention showed a stronger within-person association between their momentary experiences of negative affect and smoking urges during the post-quit stage compared with the other two groups. For each of the main findings, we also observed substantial differences across participants (regardless of intervention type) in the strength of the within-person association between their momentary experiences of negative affect and smoking urges. Further, results from sensitivity and secondary analyses indicated that the moderation by intervention type may not be credible after accounting for whether a person had already smoked that day, and may be driven primarily by low activation negative emotions (i.e., sad, miserable, and depressed). Altogether, results from the present study, discussed in the following sections, contribute to a growing literature on how the relation between momentary experiences of negative affect and smoking urges in daily life may change from pre- to post-quit, and shed light on the features of interventions that may help mitigate these changes in service of smoking cessation.
Although individuals' negative affect tended to be relatively stable, on average, during the pre-quit and post-quit stages, we found evidence of substantial within-person variability in momentary negative affect during both stages. Further, we found evidence of a within-person association between momentary experiences of negative affect and smoking urges. Specifically, on occasions when individuals' negative affect was higher than usual, their smoking urges also tended to be higher than usual. This finding aligns with prior studies conducted in both laboratory and in vivo settings (11, 15, 16).
Extending prior work, we observed that the extent of within-person association between negative affect and smoking urges was stronger during the post-quit stage of the intervention compared with the pre-quit stage. In other words, the coupling between individuals' momentary experiences of negative affect and smoking urges tended to be stronger during times when they were actively trying to avoid smoking compared with times when they were not actively trying to avoid smoking. Prior research has shown that nicotine withdrawal can cause both urges and negative affect and that these symptoms can also increase the likelihood of smoking lapse (11, 37). Thus, it is not surprising that our findings showed that the within-person association between negative affect and smoking urges became stronger when nicotine withdrawal increased post-quit. Smoking cessation interventions that aim to de-couple the within-person covariation between negative affect and smoking urges, may reduce the salience of smoking urges, and thus help to reduce the likelihood of smoking lapse.
Study findings related to the pre-/post-quit change in the extent of within-person association between negative affect and smoking urges may have implications for future intervention development. For example, we observed that individuals who tended to have higher average negative affect during the pre-quit stage also tended to have stronger coupling between their momentary experiences of negative affect and smoking urges during the post-quit stage of the study. This finding could be applied in future interventions by using dynamic characteristics (e.g., intraindividual mean of momentary negative affect scores) calculated from pre-quit data as a screening or tailoring tool for post-quit intervention delivery. As an example, smokers who display high characteristic negative affect during the pre-quit stage (within-person mean of momentary negative affect) could receive more intervention content focused on de-coupling the association between negative affect and smoking urges than those who have lower characteristic negative affect during the pre-quit stage. Overall, these findings align with the goals of personalized medicine by highlighting potential ways to temporally and contextually tailor interventions to boost overall effectiveness (21).
Several interesting preliminary findings emerged pertaining to differences in the extent of within-person association between negative affect and smoking urges based on intervention type during the post-quit stage. First, the average within-person association between negative affect and smoking urges was stronger for those assigned to QuitGuide compared with those assigned to Smart-T2 or TTRP. One plausible explanation of this finding is that there were important differences in the extent of personalization across the interventions. For example, those assigned to TTRP received personalized feedback from a counselor on how to cope with negative affect, smoking urges, and other smoking lapse risk factors. In contrast, those assigned to Smart-T2 and QuitGuide received all intervention content via smartphone. It is possible that the Smart-T2 intervention partially de-coupled the momentary relationship between negative affect and smoking urges by providing tailored real-time messages focused on addressing and/or coping with these relapse risk symptoms up to 5 times per day. Relatedly, individuals in the Smart-T2 and TTRP groups both reported higher levels of treatment satisfaction compared with the QuitGuide group, and felt that their treatment “knew how to help [them] quit smoking” (23). We also checked whether this finding might be attributable to differences in intervention efficacy, but found that the 4-week follow-up abstinence rates were relatively similar across the 3 interventions (nSmartT2= 6 people, nQuitGuide= 7 people, nTTRP= 8 people). Together, these findings provide promising preliminary evidence that the Smart-T2 intervention may, like traditional smoking cessation counseling, reduce the extent of within-person association between momentary experiences of negative affect and smoking urges.
In secondary analyses, we examined whether results differed after negative affect was parsed into high activation (e.g., frustrated/angry) and low activation (e.g., sad) components. For both high and low activation, the extent of within-person association between negative affect and smoking urges was stronger during the post-quit stage. Additionally, compared to individuals in the QuitGuide group, those in the Smart-T2 group tended to have weaker within-person association between their low-activation negative affect and their smoking urges. However, the same difference was not credibly observed for high activation negative affect. One potential explanation for this finding pertains to differences in effort required to access intervention content, and how such effort may be more or less likely invested when negative affect and/or urges are high. Participants randomized to the Smart-T2 group immediately received intervention content after completing each brief assessment and could also access intervention content on demand via the app. In contrast, those randomized to QuitGuide only received on-demand intervention content when they specifically sought it out by opening the QuitGuide app. The automated, prompted, and consistent delivery of the Smart-T2 intervention content may have been particularly useful in moments when individuals were experiencing higher smoking urges than usual and low activation negative affect. Prior research has shown that low activation negative affect is associated with lower approach motivation (38). In contrast, for high activation moments, it may be that the intervention differences were “washed out” because participants were in an affective state that has been shown to be associated with higher approach motivation, and thus more likely to exert effort to access (approach) intervention content from their assigned intervention (39). Future research would benefit from further study of differences in negative affect activation and effort-based differences in exposure to intervention content.
This study has several strengths and limitations. The dense sampling methodology that was used (i.e., up to five EMAs per day) during the 7 pre-quit days and 29 post-quit days afforded opportunities to study within-person associations between momentary smoking urges and negative affect as well as changes in the extent of within-person association by quit stage. In contrast, the present study was designed to collect pilot data on the efficacy of the Smart-T2 intervention, and thus was not specifically powered to detect between-group (e.g., intervention type) differences in the extent of within-person associations between negative affect and smoking urges. A follow-up study is currently in the data collection phase, with more individuals per intervention type, that will be better powered to detect these cross-level interactions (40).
A second limitation is that a substantial portion of the sample reported smoking on all 29 post-quit days of the study. This high rate of post-quit smoking may have implications for whether the intervention type differences in the extent within-person association between negative affect and smoking urges could be detected. Results from the sensitivity analyses suggested that on occasions when individuals had smoked at some point already that day, their negative affect tended to be higher than usual. Thus, once an individual smokes in a given day, it may be that they are less susceptible to intervention content or that intervention content may be interpreted as less relevant for the remainder of the day. Future work should focus on further disentangling the complex associations between negative affect, smoking urges, and smoking behaviors in larger, adequately powered samples.
Another limitation is that the modeling strategy used in the present study assumed consistent within-person associations during the post-quit stage; however, this may not be the case (41). As individuals progressed further into the intervention and went longer without smoking, the extent to which momentary changes in their negative affect were coupled with momentary changes in smoking urges may have diminished. Future work could benefit from implementing other modeling techniques to test whether the post-quit association parameter should be time-varying. Similarly, the present study focused on understanding concurrent within-person associations between smoking urges and negative affect, but it may also be that these associations are bidirectional. Thus, future work should examine the temporal ordering of these associations and whether the extent of within-person association in one direction is stronger than the other direction using methods such as multilevel vector autoregressive modeling (42–44). Altogether, work in this area will afford better understanding of how these within-person dynamic characteristics change over the course of smoking cessation attempt(s) and inform theory on how the smoking behavior change process operates.
Findings from the present study offer preliminary evidence that the within-person association between negative affect and smoking urges increases following a quit attempt, and that the TTRP and Smart-T2 interventions may attenuate this within-person association during the post-quit stage, compared with the QuitGuide intervention. Future work should determine if these findings are replicated in a fully powered randomized controlled trial and whether interventions designed to reduce negative affect in the context of smoking urges reduce the intensity of subsequent urges as well as the likelihood of smoking lapses. Altogether, the present study adds to a growing literature that focuses on how psychological variables (e.g., urge and negative affect) covary during a quit attempt. Study findings may inform future smoking cessation JITAI development.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by University of Oklahoma Health Sciences Center. The patients/participants provided their written informed consent to participate in this study.
MB and DK conceptualized the parent study and collected study data. LB conceived of the presented study idea, analyzed the data, and drafted the methods, results, tables, and figures. MB, CR, and EH provided initial feedback on the present study idea. LB, CR, and EH drafted the introduction and discussion. CR, EH, DK, JO, SF-P, JN, and MB provided conceptual feedback and edited the manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the Oklahoma Tobacco Settlement Endowment Trust (Grant Number 092-016-0002) and used the mobile health shared resource of the Stephenson Cancer Center via an NCI Cancer Center Support Grant (Grant Number P30CA225520). Manuscript preparation was additionally supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number R00DA046564. This study was funded by MB's start-up package.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
MB and DK are inventors of the Insight mHealth Platform, which was used to develop the Smart-T2 app. They receive royalties related to its use.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. U.S. Department of Health and Human Services. Smoking Cessation: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health (2020).
2. Babb S. Quitting smoking among adults—United States, 2000–2015. MMWR Morb Mortal Weekly Rep. (2017) 65:1457–64. doi: 10.15585/mmwr.mm6552a1
3. Chaiton M, Diemert L, Cohen JE, Bondy SJ, Selby P, Philipneri A, et al. Estimating the number of quit attempts it takes to quit smoking successfully in a longitudinal cohort of smokers. BMJ Open. (2016) 6:e011045. doi: 10.1136/bmjopen-2016-011045
4. Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annu Rev Clin Psychol. (2008) 4:1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415
5. Shiffman S. Ecological momentary assessment (EMA) in studies of substance use. Psychol Assess. (2009) 21:486. doi: 10.1037/a0017074
6. Shiffman S, Gwaltney CJ, Balabanis MH, Liu KS, Paty JA, Kassel JD, et al. Immediate antecedents of cigarette smoking: an analysis from ecological momentary assessment. J Abnorm Psychol. (2002) 111:531–45. doi: 10.1037/0021-843X.111.4.531
7. Shapiro D, Jamner LD, Davydov DM, James P. Situations and moods associated with smoking in everyday life. Psychol Addict Behav. (2002) 16:342–5. doi: 10.1037/0893-164X.16.4.342
8. Businelle MS, Lam CY, Kendzor DE, Cofta-Woerpel L, McClure JB, Cinciripini PM, et al. Alcohol consumption and urges to smoke among women during a smoking cessation attempt. Exp Clin Psychopharmacol. (2013) 21:29–37. doi: 10.1037/a0031009
9. Minami H, McCarthy DE, Jorenby DE, Baker TB. An ecological momentary assessment analysis of relations among coping, affect and smoking during a quit attempt. Addiction. (2011) 106:641–50. doi: 10.1111/j.1360-0443.2010.03243.x
10. Piasecki TM. Relapse to smoking. Clin Psychol Rev. (2006) 26:196–215. doi: 10.1016/j.cpr.2005.11.007
11. Shiffman S, Waters AJ. Negative affect and smoking lapses: a prospective analysis. J Consult Clin Psychol. (2004) 72:192–201. doi: 10.1037/0022-006X.72.2.192
12. Shiffman S, Balabanis MH, Gwaltney CJ, Paty JA, Gnys M, Kassel JD, et al. Prediction of lapse from associations between smoking and situational antecedents assessed by ecological momentary assessment. Drug Alcohol Depend. (2007) 91:159–68. doi: 10.1016/j.drugalcdep.2007.05.017
13. McCarthy DE, Piasecki TM, Fiore MC, Baker TB. Life before and after quitting smoking: an electronic diary study. J Abnorm Psychol. (2006) 115:454. doi: 10.1037/0021-843X.115.3.454
14. Brandon TH. Negative affect as motivation to smoke. Curr Dir Psychol Sci. (1994) 3:33–7. doi: 10.1111/1467-8721.ep10769919
15. Heckman BW, Kovacs MA, Marquinez NS, Meltzer LR, Tsambarlis ME, Drobes DJ, et al. Influence of affective manipulations on cigarette craving: a meta-analysis. Addiction. (2013) 108:2068–78. doi: 10.1111/add.12284
16. Heckman BW, Carpenter MJ, Correa JB, Wray JM, Saladin ME, Froeliger B, et al. Effects of experimental negative affect manipulations on ad libitum smoking: a meta-analysis. Addiction. (2015) 110:751–60. doi: 10.1111/add.12866
17. Almeida DM. Resilience and vulnerability to daily stressors assessed via diary methods. Curr Dir Psychol Sci. (2005) 14:64–8. doi: 10.1111/j.0963-7214.2005.00336.x
18. Smyth JM, Sliwinski MJ, Zawadzki MJ, Scott SB, Conroy DE, Lanza ST, et al. Everyday stress response targets in the science of behavior change. Behav Res Ther. (2018) 101:20–9. doi: 10.1016/j.brat.2017.09.009
19. Shiyko M, Naab P, Shiffman S, Li R. Modeling complexity of EMA data: time-varying lagged effects of negative affect on smoking urges for subgroups of nicotine addiction. Nicotine Tob Res. (2014) 16(Suppl. 2):S144–150. doi: 10.1093/ntr/ntt109
20. Spruijt-Metz D, Nilsen W. Dynamic models of behavior for just-in-time adaptive interventions. IEEE Pervasive Comput. (2014) 13:13–7. doi: 10.1109/MPRV.2014.46
21. Nahum-Shani I, Smith SN, Spring BJ, Collins LM, Witkiewitz K, Tewari A, et al. Just-in-time adaptive interventions (JITAIs) in mobile health: key components and design principles for ongoing health behavior support. Ann Behav Med. (2018) 52:446–62. doi: 10.1007/s12160-016-9830-8
22. Perski O, Hebert ET, Naughton F, Hekler EB, Brown J, Businelle MS. Technology-mediated just-in-time adaptive interventions (JITAIs) to reduce harmful substance use: a systematic review. Addiction. (2021). doi: 10.1111/add.15687. [Epub ahead of print].
23. Hébert ET, Ra CK, Alexander AC, Helt A, Moisiuc R, Kendzor DE, et al. A mobile just-in-time adaptive intervention for smoking cessation: pilot randomized controlled trial. J Med Internet Res. (2020) 22:e16907. doi: 10.2196/16907
24. Businelle MS, Ma P, Kendzor DE, Frank SG, Vidrine DJ, Wetter DW. An ecological momentary intervention for smoking cessation: evaluation of feasibility and effectiveness. J Med Internet Res. (2016) 18:e321. doi: 10.2196/jmir.6058
25. Businelle MS, Ma P, Kendzor DE, Frank S, Wetter DW, Vidrine DJ. Using intensive longitudinal data collected via mobile phone to detect imminent lapse in smokers undergoing a scheduled quit attempt. J Med Internet Res. (2016) 18:e275. doi: 10.2196/jmir.6307
26. NCI. QuitGuide. Available online at: https://smokefree.gov/apps-quitguide (accessed January 3, 2017).
27. Buller DB, Borland R, Bettinghaus EP, Shane JH, Zimmerman DE. Randomized trial of a smartphone mobile application compared to text messaging to support smoking cessation. Telemedicine e-Health. (2014) 20:206–14. doi: 10.1089/tmj.2013.0169
28. Fiore MC, Jaén CR, Baker TB, Bailey WC, Benowitz NL, Curry SJ. Treating Tobacco Use and Dependence: 2008 Update. Rockville, MD: US Department of Health and Human Services (2008).
29. Russell JA. A circumplex model of affect. J Pers Soc Psychol. (1980) 39:1161. doi: 10.1037/h0077714
30. Heatherton TF, Kozlowski LT, Frecker RC, Rickert W, Robinson J. Measuring the heaviness of smoking: using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br J Addict. (1989) 84:791–800. doi: 10.1111/j.1360-0443.1989.tb03059.x
31. Bolger N, Laurenceau JP. Intensive Longitudinal Methods: An Introduction to Diary and Experience Sampling Research. New York, NY: Guilford Publications (2013).
32. RStudio Team,. RStudio: Integrated Development for RStudio R, PBC. Boston, MA: RStudio (2020). Available online at: http://www.rstudio.com/
33. R Core Team,. R: A language environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria (2020). Available online at: https://www.R-project.org/
34. Wickham H,. ggplot2: Elegant Graphics for Data Analysis. New York, NY: Springer-Verlag (2016). Available online at: https://ggplot2.tidyverse.org
35. Bürkner P-C,. brms: An R package for Bayesian multilevel models using Stan. J Statist Softw. (2017) 80:1–28. Available online at: https://cran.r-project.org/web/packages/brms/vignettes/brms_overview.pdf
36. Bürkner P-C. Advanced bayesian multilevel modeling with the r package brms. R J. (2018) 10:395–411. doi: 10.32614/RJ-2018-017
37. Piasecki TM, Jorenby DE, Smith SS, Fiore MC, Baker TB. Smoking withdrawal dynamics: I. Abstinence distress in lapsers and abstainers. J Abnorm Psychol. (2003) 112:3. doi: 10.1037/0021-843X.112.1.3
38. Gable P, Harmon-Jones E. The blues broaden, but the nasty narrows: attentional consequences of negative affects low and high in motivational intensity. Psychol Sci. (2010) 21:211–5. doi: 10.1177/0956797609359622
39. Harmon-Jones E, Harmon-Jones C, Price TF. What is approach motivation? Emot Rev. (2013) 5:291–5. doi: 10.1177/1754073913477509
40. Businelle MS. Smartphone Based Smoking Cessation Intervention for Socioeconomically Disadvantaged Adults. Oklahoma City, OK: National Cancer Institute, 1R01CA221819-01A1 (2019).
41. Shiyko MP, Lanza ST, Tan X, Li R, Shiffman S. Using the time-varying effect model (TVEM) to examine dynamic associations between negative affect and self confidence on smoking urges: differences between successful quitters and relapsers. Prev Sci. (2012) 13:288–99. doi: 10.1007/s11121-011-0264-z
42. Bringmann LF, Ferrer E, Hamaker EL, Borsboom D, Tuerlinckx F. Modeling nonstationary emotion dynamics in dyads using a time-varying vector-autoregressive model. Multivariate Behav Res. (2018) 53:293–314. doi: 10.1080/00273171.2018.1439722
43. Li Y, Wood J, Ji L, Chow S-M, Oravecz Z. Fitting multilevel vector autoregressive models in Stan, JAGS, and Mplus. Struct Eq Model Multidiscip J. 2021:1–24. doi: 10.1080/10705511.2021.1911657
Keywords: digital health, mHealth, smoking cessation, just-in-time adaptive intervention (JITAI), negative affect (NA)
Citation: Benson L, Ra CK, Hébert ET, Kendzor DE, Oliver JA, Frank-Pearce SG, Neil JM and Businelle MS (2022) Quit Stage and Intervention Type Differences in the Momentary Within-Person Association Between Negative Affect and Smoking Urges. Front. Digit. Health 4:864003. doi: 10.3389/fdgth.2022.864003
Received: 27 January 2022; Accepted: 28 February 2022;
Published: 29 March 2022.
Edited by:
Inbal Billie Nahum-Shani, University of Michigan, United StatesReviewed by:
John Dziak, The Pennsylvania State University (PSU), United StatesCopyright © 2022 Benson, Ra, Hébert, Kendzor, Oliver, Frank-Pearce, Neil and Businelle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lizbeth Benson, bGl6YmV0aC1iZW5zb25Ab3Voc2MuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.