
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Digit. Health , 21 November 2022
Sec. Health Informatics
Volume 4 - 2022 | https://doi.org/10.3389/fdgth.2022.1017231
 Christie Divine Akwaowo1,2
Christie Divine Akwaowo1,2 Humphrey Muki Sabi3*
Humphrey Muki Sabi3* Nnette Ekpenyong4Chimaobi M. Isiguzo5Nene Francis Andem6Omosivie Maduka7Emem Dan2
Nnette Ekpenyong4Chimaobi M. Isiguzo5Nene Francis Andem6Omosivie Maduka7Emem Dan2 Edidiong Umoh2,8Victory Ekpin2Faith-Michael Uzoka9
Edidiong Umoh2,8Victory Ekpin2Faith-Michael Uzoka9
Electronic medical records (EMR) are extensively used in developed countries to manage patient records and facilitate consultations and follow-up of treatment. This has resulted in centralised databases where different services and clinicians can quickly access patient data to support healthcare delivery. However, adoption and usage of EMR in developing countries is not common and, in most cases, non-existent. Clinicians are dependent on patients keeping their own records manually with no centralised database to manage and control the patient medical history. The key objective of this study was to investigate the propensity of clinicians and senior management personnel in healthcare facilities to adopt EMR and evaluate the contextual factors that impact or impede adoption. Using Davis's technology adoption model extended with other factors, this study determined if contextual or situational factors are associated with barriers that impede adoption of EMRs in developing countries. Using a cross-sectional quantitative research approach, a questionnaire was designed to collect data across four states in the Niger Delta region of Nigeria. Stratified random sampling was used to select healthcare facilities that participated in the survey and selection of respondents from each healthcare facility. Data was collected by trained research assistants and a total of 1,177 valid responses were received and analysed using factor analysis and multiple regression analysis. The results from the analysis show that usefulness, critical success factors, awareness and relative advantage significantly influence clinicians' intention to adopt EMRs. Surprisingly, infrastructure availability was not statistically significant. Meanwhile, risk and data security both negatively influence adoption, indicating that user perception of risk and safety of their data decreases their propensity to adopt EMRs. The results from this study suggests that usefulness and anticipated success factors in facilitating operations within healthcare facilities have a great influence on user adoption of EMRs. Awareness, training and education of users on the effectiveness of EMRs and their usefulness will increase adoption. The results will be beneficial in helping government and healthcare leaders formulate policies that will guide and support adoption of EMR. Other policy recommendations and suggestions for future research were also proffered.
The health sector has recently seen numerous technological innovations designed to streamline the process of healthcare delivery for the health providers and consumers. Electronic medical record (EMR) is one of such innovations. This innovation has helped to reduce medication errors, adverse drug reactions, and to improve compliance to practice guidelines among health care professionals (1). For instance, by making patients’ information available electronically, health care information systems can help to prevent ordering of duplicate tests and procedures, thereby reducing expenditures on health care service (2). Hence, these innovations have been crucial to improving patient safety and quality of health in today's world.
The usual entry point for information technology (IT) in the health sector is the EMR. EMRs are increasingly being utilized worldwide, especially in developed countries. Developing countries have been found to lag behind due to organizational, financial and infrastructural factors (3). The national e-health strategy toolkit which was developed by WHO and ITU has defined EMR as a computerized medical record used to capture, store, and share information among healthcare providers in an organization, supporting the delivery of health services to patients (4). EMRs have been proven to improve quality of care and patient outcome by keeping health care providers better informed, improving the workflow process, improving communication between clinicians, improving compliance with best practices and reducing medical errors. Moreover, EMRs also allow patients to access their own medical records easily and from research stand point, it allows easy access to data (5–7).
In both public and private sectors, health care providers are being encouraged to migrate from paper-based health records to electronic storage of patient information and computer-aided decision support systems. This is partially due to a growing recognition that a better information technology infrastructure is essential to addressing certain health-related national concerns such as the need to improve the safety and quality of health care, and rising health care costs (5). However, adoption of EMR among health workers has been slow in developing countries like Nigeria. Adoption is of course more than designing or purchasing a reasonably functional technology, but also about the acceptance and use of the system by the health workers.
Recent reports show that the fit between information technology and the clinical work system will lead intended end users to accept or reject it, to use it or misuse it, to incorporate it into their routine or work around it (8). The successful implementation of innovative medical technologies, depends on acceptance by medical staff, such as doctors, nurses and other clinicians. The decision to accept or reject a new technological innovation depends on several influencing factors. For example, Ross et al. in a review of forty-four studies from North America and Europe identified barriers to implementation of EMR as adaptability, complexity, cost, external policy and incentives (9). Other contextual factors include organizational and social environments, cultures, state of the economy, medical liability and processes by which innovation is introduced (10, 11). Other barriers identified are personal attributes such as knowledge, beliefs, computer skills, experience, resistance to change and lack of health care providers' input in design and implementation of the EMR (12, 13). An effective EMR is one that serves its intended purposes after implementation, hence uptake of an EMR is just as important its performance.
Several studies have analysed the behavioural intentions of healthcare professionals to accept and use a new health information technology. In van der Meijden et al. (14), several factors which influenced the success of health information systems were reported, including: System quality attributes like ease of use, response time, useability; information quality attributes like completeness, accuracy of data, legibility; Usage attributes like number of entries, frequency of use, duration of use; User attributes like user satisfaction, attitude, user friendliness; Individual impact attributes like changes to work patterns, documentation frequency, time of day for documenting; and organizational impact attributes such as impact on patient care, communication and collaboration, reduction of staff as well as time saving (14). Chae et al. (15) reported that larger hospital size and having top management support was significantly associated with adoption and utilization of EMR by health professionals. This may be because as hospital sizes get bigger, the adoption rate of EMR increased to improve efficiency of hospital operations and patient management (15).
A mismatch between EMR functionality and the needs of health workers in practice was identified as a common deterrent to its uptake in O’Donnell et al. (13). EMRs were often viewed as lacking an easily accessible overview of key patient data such as family histories and past medical histories. Furthermore, it was reported that physicians found it difficult to record certain types of information such as emerging diagnoses and/or vague symptoms, especially for potentially sensitive or stigmatising diagnoses (13). In Nigeria, although positive attitudes and perception towards EMR was seen in the Northwest, poor knowledge was prevalent among the health workers, especially among the doctors (16). This therefore can be a major barrier to the adoption and utilization of EMR by health professionals. A review of the adoption of electronic health records (EHR) in Africa also found that it has not been widely implemented or adopted in sub-Saharan Africa (17). In another study carried out in Cameroon to develop and test an EHR system locally, it was found that there are many contextual challenges which required modelling of the system to fit the local medical practice in place and using terminology that is tailored and appropriate for their operations (18).
The main objective of this study is to investigate the factors that influence the decision of healthcare professionals to adopt and use an EMR system by answering the following research question: What are the factors that influence the decision of health workers to adopt and use EMR in developing countries?
Different models have been theorized to examine adoption of technology in an organizational setting. These have been done with the intent of understanding the attitudes, the use intentions and the behaviour towards the adoption of new technologies (11). One of the most notable is the application of the Technology Acceptance Model (TAM) to the prediction and explanation of end-user reactions to health IT. TAM is based on the theory of reasoned action (TRA) and hypothesizes that Perceived Usefulness and Perceived Ease of Use, are of primary relevance for technology acceptance. How useful technology is perceived to be is subjective and depends on how the individual thinks their jobs will be enhanced by the technology, while perceived ease of use is the subjective assessment of the effort required to learn and use the new technology. The balance between these two determines the acceptance of the technology by individuals, and their motivation to use the technology. External factors, such as support measures, have a positive effect on the perception of usefulness and on understanding a technology (11, 16). In a review of TAM usage in health care, it was able to predict 30%–70% of variance of behavioural Intention to Use (16).
Another of such theories is the Theory of Reasoned Action which was developed by Martin Fishbein and Icek Ajzen in 1975. It is a popular model from social psychology which is concerned with the determinants of consciously intended behaviours (19). TRA was proposed after the researchers had difficulty explaining the discrepancy between attitude and behaviour in previous models. The model was developed to explain whether individual behaviour such as adoption and utilization of a new technology is driven by behavioural intentions, with individual attitude, subjective norms surrounding the performance of the behaviour and ease of use of the technology affecting behaviour (19). Theory of planned behaviour has also been employed in explaining models of adoption of technology and it goes a step further than the TRA by incorporating “perceived behavioural control”, accounting for situations where the target individuals don't have total control over the behaviour (20).
The unified technology acceptance and use of technology (UTAUT) model was published in 2003 and is based on an analysis and comparison of up to eight technology acceptance models, including TAM, TAM2, the Theory of Reasoned Action and the Diffusion of Innovation Theory (21). This theory describes 4 major factors that underpin acceptance of health technology: performance expectancy, effort expectancy, social influence, and facilitating conditions. Performance expectancy is the expectation that the system will do the job it was set out to do, and bring about improvement. Effort expectancy is the expectation that the system is easy to use. Social influence is the perception of the extent to which others believe a new technology should be used and lastly, facilitating conditions are defined as the degree to which a user believes that an organizational and technical infrastructure can support the use of the new technology (11, 19, 20).
The technology acceptance model (TAM) (22) has been extended with additional contextual and situational constructs for this study. TAM posits that adoption of new technology is influenced by user's perception of the usefulness of the new technology and ease of use of the new technology. The ability to explain individual behavioural intentions to use new technology is based on its usefulness and ease of use, and has been widely used by many information systems (IS) researchers to explain adoption of many technologies (23–25). We have extended the TAM constructs with awareness, risks, data security, infrastructure and relative advantage to investigate the propensity of healthcare workers in medical facilities in Nigeria to adopt and use EMRs. A proposed conceptual adoption model has been developed based on the chosen theoretical model (TAM) and the additional factors used to extend the model for our research as shown in Figure 1. The model shows the relationship between the independent variables that can influence adoption of EMR and user decision to adopt and use EMR. The model proposes that relative advantage mediates usefulness of EMR and hence impacts user propensity to adopt and use EMR. The model also shows the moderating factors that can influence user decision to adopt EMR such as age, gender and years of experience in the medical field.
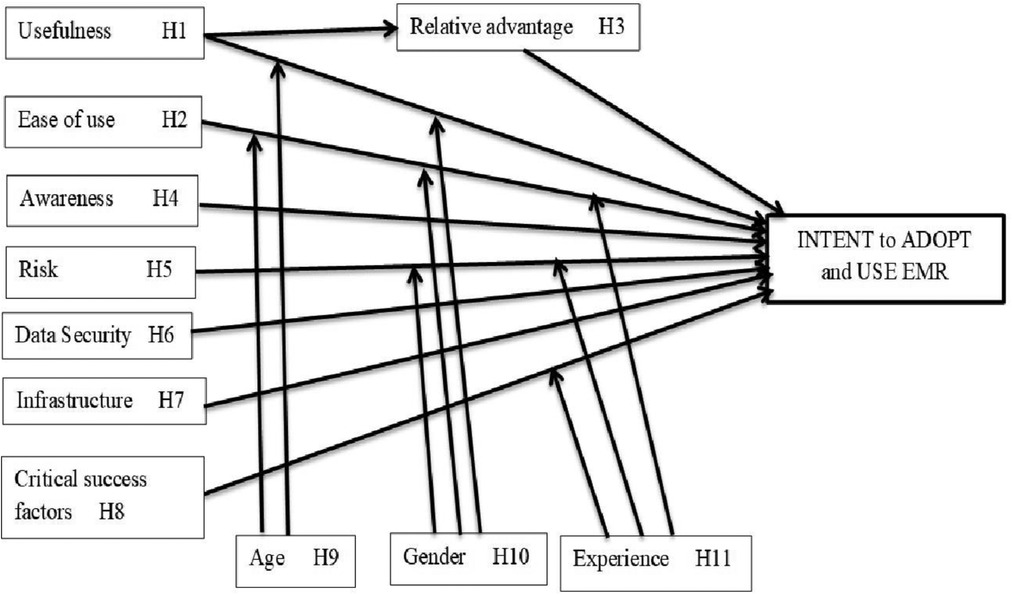
Figure 1. EMR adoption model.
We proposed the following hypotheses which will be tested in the data analysis to answer our key research question on the critical factors that influence the adoption and usage of EMR in developing countries. The hypotheses address the relationships between the independent variables that impact adoption of EMR and the dependent variables “intent to adopt EMR” and “intent to use EMR”.
The main reason individuals, organizations and governments embark on adoption of new technology is to facilitate their work and improve performance and profitability. Adoption of new technologies often requires a change in the status-quo and doing things differently. The ease of use and usefulness of new technology greatly determines user willingness to adopt and use the technology (22). The way new technology will be more efficient than previous methods and help users gain advantage over its competitors hence it will influence the decision to adopt the technology. We therefore posit that:
H1: Usefulness will positively influence user decision to adopt EMR
H2: Ease of use will positively influence user decision to adopt EMR
H3: Relative advantage will positively influence user decision to adopt EMR
Users will usually adopt and use technology that they have witnessed being used by others or have access to observe the new technology in action. Since some of these new technologies can impact user operations if not used correctly, users will usually be sceptical to adopt and use it without having prior knowledge and visibility of the benefits of using the new technology (26). Hence, we posit that:
H4: Awareness will positively influence user decision to adopt EMR
Users of new technology are usually apprehensive about the security risks and safety of their information as it is stored and transmitted through the internet or cloud (27). Despite the growing popularity of EMR due to its ability to allow quick and easy access to patient data, users are still reluctant to adopt it due to data security and privacy concerns (28). We posit that:
H5: Absence of risk will positively influence user decision to adopt EMR
H6: Data safety will positively influence user decision to adopt EMR
Infrastructural availability, which encompasses stable electricity supply, good telecommunication networks, and high-speed internet or broadband networks, play a crucial role in the smooth operation of EMR. Sub-Sahara African countries have very poor infrastructures and have been faced with problems of stable electricity over the years. Availability of appropriate infrastructure is crucial for the adoption of new technological innovations (29). We posit that:
H7: Availability of good infrastructure will positively influence user decision to adopt EMR
In order for senior management and other stakeholders to recommend or adopt new technology, there must be some critical success factors that are used to guide their decision. Technologies that align favourably with all or most of the critical success factors outlined by the organisation will most likely be adopted. Hence, we posit that:
H8: Alignment of EMR technology with business defined critical success factors will positively influence user decision to adopt EMR
Previous studies have highlighted key innovation diffusion factors which include relative advantage and emphasised the impact of relative advantage on user perception of usefulness of new technology (30). Therefore, we posit that:
H9: Relative advantage positively mediates user decision to adopt and use EMR
Research has shown that age, gender and years of experience of users can have an impact on their decision to adopt and use new technology (31). Moreover, users that are already comfortable with a particular system or way of working for years might be reluctant to change and adopt a new system (30). Meanwhile, it is very common for younger people and male users to adapt and adopt new technology. We therefore posit that:
H10a: Age will moderate impact of usefulness on user decision to adopt EMR
H10b: Age will moderate impact of ease of use on user decision to adopt EMR
H10c: Gender will moderate impact of usefulness on user decision to adopt EMR
H10d: Gender will moderate impact of ease of use on user decision to adopt EMR
H10e: Gender will moderate user perception of risk on their decision to adopt EMR
H10f: Experience will moderate impact of ease of use on user decision to adopt EMR
H10g: Experience will moderate user perception of risk on decision to adopt EMR
H10h: Experience will moderate user perception of success factors on decision to adopt EMR
We adopted a quantitative research approach for this study because it allowed us to efficiently collect responses from a large sample across four states in Nigeria in a cost-effective and timely manner (32). A survey instrument was designed and used for the data collection. Prior to using the survey tool for the data collection, it was peer reviewed by adoption experts and a pilot test carried out to ensure the reliability and validity of the tool for our data collection process. Research assistants were recruited from each state and trained on the data collection tool. The questionnaire was transformed and then loaded unto the ODK (Open data kit) which was used by the research assistants for data collection. The ODK is an easy-to-use data collection app that runs on the android operating system. The advantage of using the ODK is that data can be collected and stored when the tablet is offline and when connected to the internet, the data is automatically saved on a central database (33). Each research assistant was given an android tablet with the ODK running on it for the data collection.
This study was conducted in four states in the Niger Delta region viz: Akwa-Ibom, Cross Rivers, Rivers and Imo states. A Stratified random sampling method was used to select respondents for this study. The target population was all medical facilities in the four states purposefully selected for the study based on accessibility and budget availability. Using a two-step stratification process, the researchers came up with a stakeholder grouping to ensure all stakeholders were represented in the data collection. End users of EMR being Clinicians (doctors, nurses, laboratory scientists/technologists and Pharmacists) and administrators at managerial level were selected from the secondary and tertiary medical facilities. At the primary health facilities, the officers in charge and the community health extension workers (CHEWs) were the respondents.
Respondents were randomly selected from the various stakeholder groups in each medical facility. The survey was administered by the research assistants and responses entered into the ODK. Self-administration was not used because respondents were not trained on how to use the ODK. The data collection was carried out over a period of 6 weeks and all data was then collated in the ODK database and transferred into an excel spreadsheet for processing and analysis. In total, 1,177 valid responses were received for analysis.
Statistical Package for Social Sciences (SPSS) was used to perform the data analysis. A reliability test on the full dataset resulted in a Cronbach Alpha value of 0.94, hence confirming the reliability of the data for further analysis. The data analysis and results were divided into three sections to cover descriptive analysis, factor analysis and multiple regression analysis.
Respondent profiles and the various characteristics of their medical facilities are shown in Table 1. Most of the respondents were female (60.7%) with the majority falling in the 31–50 years old age group (69%) which is consistent with the optimal working age group in the country. Most of the medical facilities had public ownership (58.4%). It was interesting to see that most of the medical facilities (46.6%) depend on the administration to make decisions on new technology adoption while very few (6.7%) relied on their IT department for such decisions. The analysis also shows that more nurses (37%) responded to the survey followed by doctors (28%) and 72% did not provide any rank. Only medical doctors are given Ranks, hence only the 329 medical doctors provided responses for rank while others left it blank.
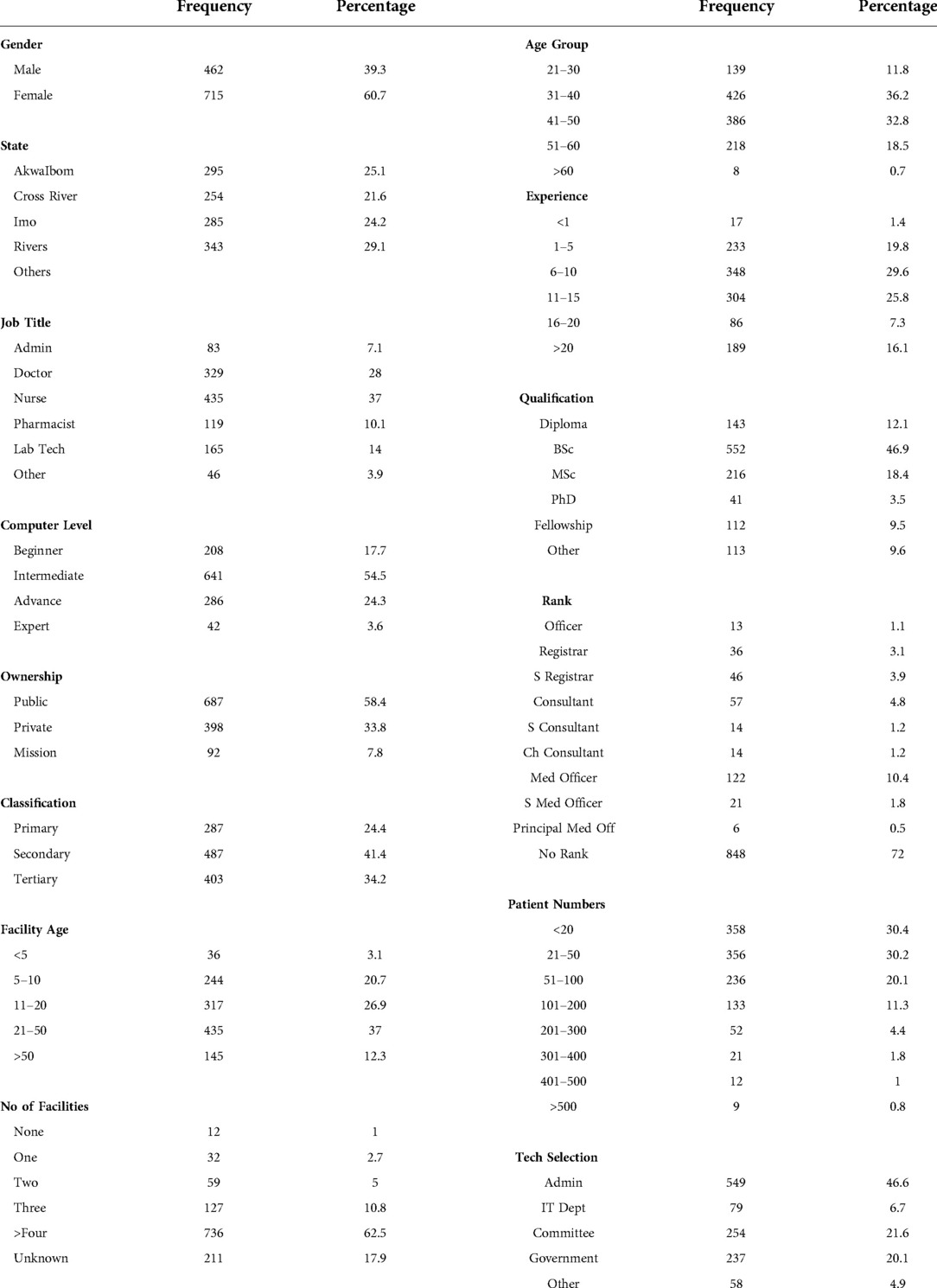
Table 1. Descriptive statistics (N = 1,177).
In order to perform factor analysis on our data, we executed the Kaiser-Meyer-Olkin (KMO) test of sampling adequacy and Bartlett's test of sphericity. This resulted in a KMO value of 0.940 and a Bartlett's test of sphericity (approx. Chi-square) value of 24,369.354 (Appendix B). The KMO value is above the 0.6 threshold required for good factor analysis and lies in the “marvellous” range (>0.9) as defined by Kaiser and Rice (34). Moreover, the result was significant (p < .001) indicating that our variables are significantly correlated and the sampling was adequate to perform factor analysis.
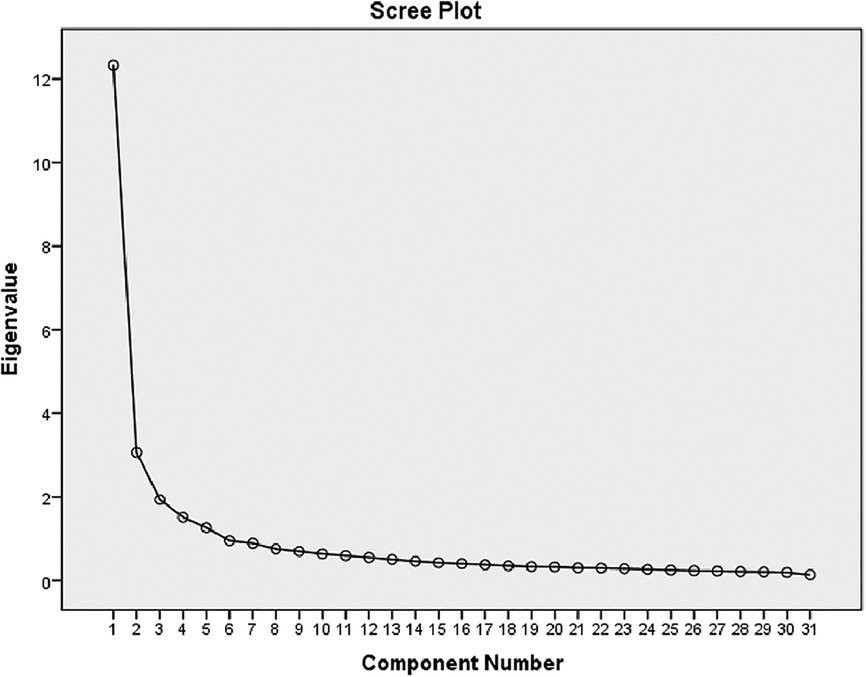
Exploratory factor analysis was performed on the dataset using principal component analysis (PCA) in order to extract the significant variables that impact user propensity to adopt EMR. The analysis was performed on 31 measured variables from our survey tool resulting in five factors being extracted (see Appendix C), which had eigenvalues greater than 1 (35). This is further supported by the scree plot (Appendix D) which shows the five factors retained with eigenvalues ≥1 based on the eigenvalue cut-off rule. However, it is worth noting that all the proposed components for this study loaded under the 5 factors retained after the factor analysis. Hence, regression analysis was carried out on the full dataset since no components were eliminated by the factor analysis.
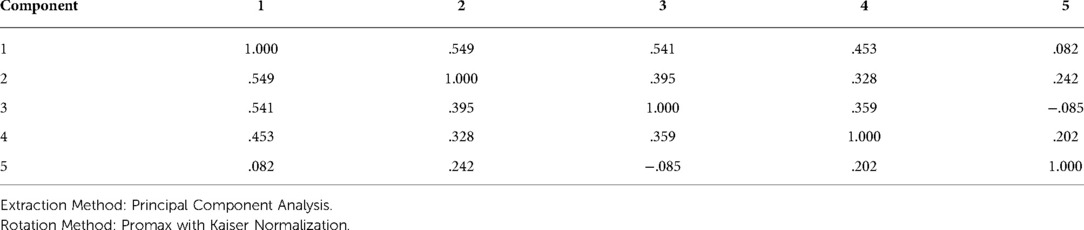
The correlation matrix shown in Appendix E was used to determine if there was correlation between the component's variables or not. According to Tabachnick and Fidell (36), if the absolute value of correlations exceeds.32, then there is a 10% (or more) overlap in variance among factors, hence, the need to do oblique rotation. Since our matrix shows values greater than this threshold, we further executed a promax rotation on the data to identify and name the measured variables that loaded on the retained components.
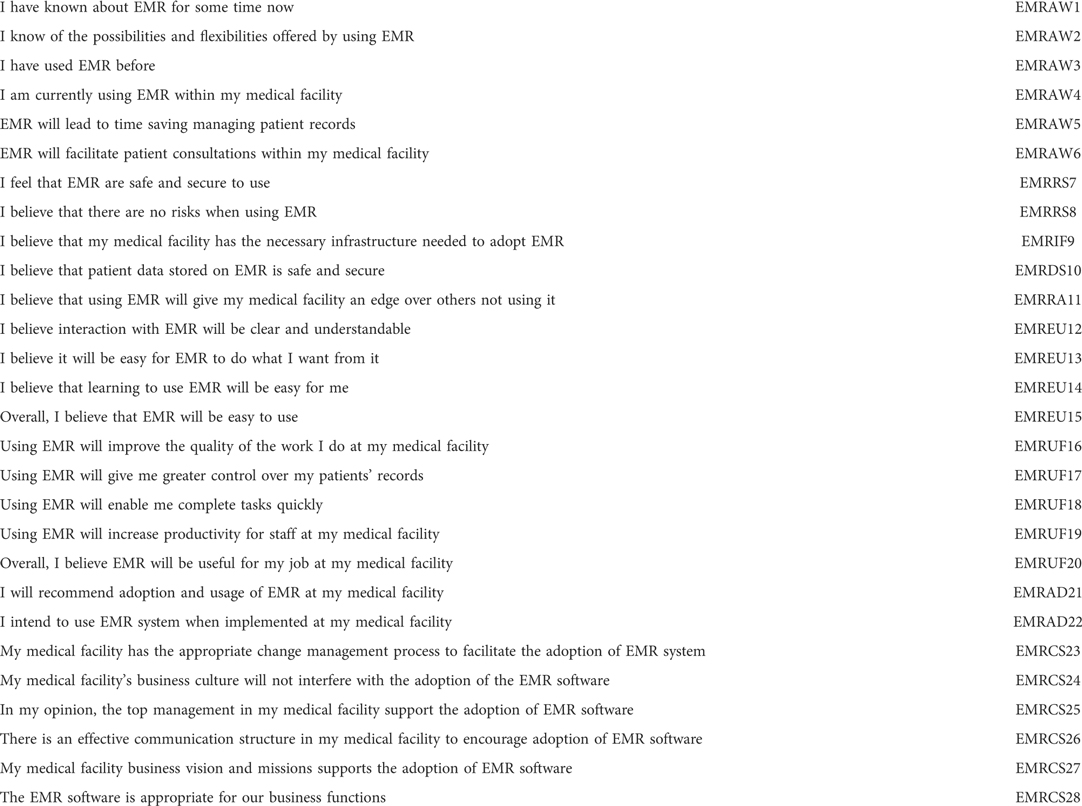
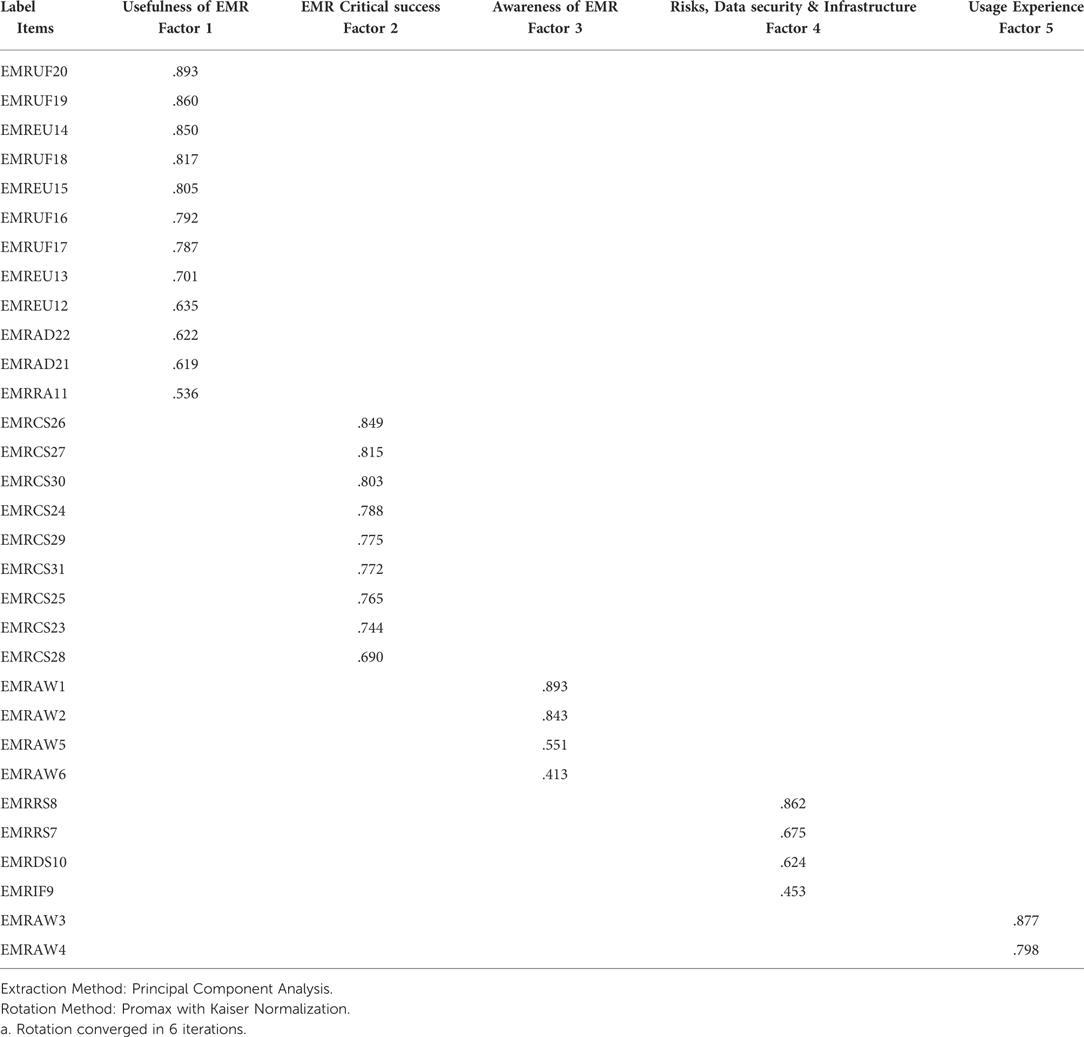
Appendix F shows the factor loading communalities for the 5 factors that were retained from the factor analysis and rotated using promax method to allow for ease of analysis and naming. The factors were named based on the majority of items that loaded for those factors. The full details of the measured variables based on the survey tool can be found in Appendix A. Measured variables that had loading coefficients less than 0.4 were suppressed during the factor analysis hence only variables with loading above 0.4 were returned. The results show that usefulness of EMR based on the survey item “Overall, I believe EMR will be useful for my job at my medical facility” had the highest factor loading. Meanwhile the lowest loading was for the item “EMR will facilitate patient consultations within my medical facility”.
In order to choose the type of regression analysis we could perform on the dataset; we needed to determine if the data was normally distributed or not. Since we had over 100 respondents (1,177 respondents), test of normality was performed on the data using the Kolmogorov-Smirnov test which is used for datasets greater than 100. The variables were transformed by calculating the means and the test for normality performed on the transformed data. The results showed that all variables were significant (p < 0.05) hence indicating that the data was not normally distributed. Since the data is not normally distributed, we carried out ordinal regression analysis instead of linear regression analysis.
The ordinal regression analysis model fitting information (Table 2) shows a significant improvement in fit of the final model over the null model [χ2(107) = 1,169.904, p < .001]. Meanwhile the goodness-of-fit test results show a Pearson chi-square test [χ2 (7,981) = 12,284.829, p < .001] and Deviance chi-square test [χ2 (7,981) = 1,957.612, p > .05]. The non-significant test result indicate that the model fits the data well (37). The Pseudo R-square value (Nagelkerke value) for this test (R2 = .674) indicates that 67.4% of the variance in user intention to adopt and use EMR can be explained by the independent variables considered in this study. The test of parallel lines was not significant (p > .05) hence indicating that we have not violated the test of proportional odds, hence the results obtained from the ordinal regression can be used to expound the impact of the independent variables on user intention to adopt and use EMR.
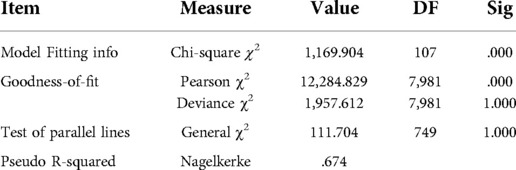
Table 2. Ordinal regression results.
In order to confirm the results from the ordinal regression analysis before proceeding to interpret the results, we further carried out the ordinal regression using generalised linear model and ordinal logistic response. The results were consistent with the initial ordinal regression analysis but additionally provided a test for the proposed model constructs to indicate which variables were statistically significant in influencing user decision to adopt and use EMR. The model test results show that awareness, risk, relative advantage, usefulness and critical success factors were statistically significant as factors that impact adoption of EMR. Meanwhile, infrastructure, data security and ease of use were not statistically significant in influencing user adoption of EMR, see Table 3. We further performed a test for collinearity to ensure that the variables are not highly correlated. The tolerance values for all the independent variables were above the 0.10 threshold and the variance inflation factor (VIF) was less than the maximum permitted value of 10.0 (38). This therefore indicates that our data was not correlated and can be used to analyse the impact of the independent variables on our dependent variable (intent to adopt EMR).
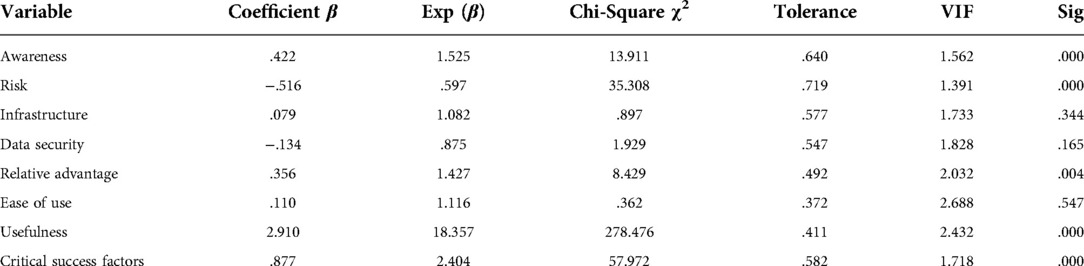
Table 3. Model test.
The Exp(β) values represent the odds ratios that reflect the multiplicative changes in the odds of being in a higher category on the dependent variable for every one unit increase in the dependent variable, holding all other independent variables constant. So, odds ratios greater than 1 will represent increasing probability of impacting the dependent variable while odds ratios of less than 1 will represent decreasing probability of impacting the dependent variable. The results therefore show that usefulness has the highest impact to increase adoption of EMR with an odds ratio of 18.357. This indicates that user propensity to adopt EMR increases by a factor of 18.357 for every one unit increase in user perception of its usefulness. This is followed by critical success factors with odds ratio of 2.404, awareness with odds ratio of 1.525 and relative advantage with odds ratio of 1.427. Even though infrastructure availability and ease of use have odds ratios above 1, they are not statistically significant. Meanwhile, risk and data security both have odds ratios below 1 with negative coefficients. This indicates that user perception of risk and safety of their data when using EMR decreases their propensity to adopt EMR.
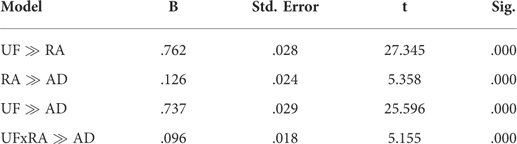
In our proposed model, we posited that relative advantage will mediate user perception of usefulness of EMR. We also posited that age, gender and experience have moderating effects on user intention to adopt and use EMR. The results of the mediation and moderation analysis are shown in Appendix G and Appendix H respectively. The results show that the direct impact of both usefulness and relative advantage on adoption and usage of EMR are significant (p < .001). To calculate the mediation effect of relative advantage on usefulness of EMR, a Sobel test (39) was conducted to determine if this mediation was significant and the mediation coefficient was also computed (see row in Appendix F) resulting a positive coefficient of 0.096. Hence, we can conclude that relative advantage has a positive significant mediating impact on usefulness of EMR.
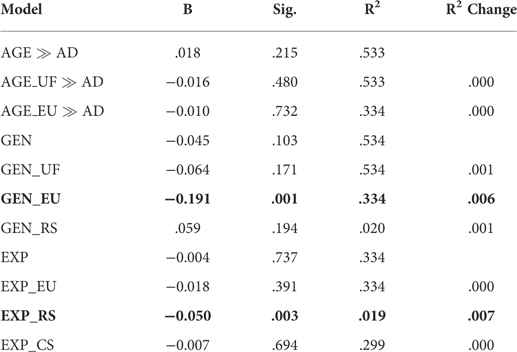
The moderation test was done by calculating the interaction term between the moderating variable and the moderated variable and then using SPSS to run a simple linear regression on the variables (Appendix H). The moderation test revealed that age, gender and experience do not have direct significant impact on user decision to adopt and use EMR. However, gender has a significant impact (p < .05) on user perception on ease of use of EMR and hence influence it adoption. Also, experience has significant impact (p < .05) on user perception of risk when it comes to the adoption of EMR. Meanwhile, the moderation effects of age on usefulness, age on ease of use, gender on usefulness, gender on risk, experience on ease of use and experience on critical success factors were statistically not significant thereby rejecting the hypotheses that posited that these factors will have a moderating impact on user decision to adopt and use EMR.
The results from the model test using ordinal regression analysis, mediation test and moderation tests were used to test the hypotheses that were propounded in the conceptual design. Table 4 provides the results of the hypotheses tests and shows that eight of the proposed hypotheses were supported (p < 0.05). Usefulness of EMR (H1) had the highest coefficient thereby indicating that users are more inclined to adopt and use EMR due to its usefulness. This was followed by critical success factors (H8) which indicates that users will only adopt EMR if it can fulfil certain conditions that will ensure success of their operations. Surprisingly, ease of use (H2) was not deemed to be very crucial for the adoption and usage of EMR hence the hypothesis was not supported despite many prior studies showing that ease of use is relevant to user adoption and use of new technology. The mediation test shows that relative advantage does have a significant positive impact on the usefulness of EMR (β = 0.096, p = 0.000). The results also show that age did not have any moderating impact on usefulness or ease of use of EMR meanwhile gender significantly mediates the impact of ease of use of EMR and experience was also found to significantly mediate perception of risk in the adoption and use of EMR. It is also worth noting that risk (H5) has a significant negative impact on user decision to adopt and use EMR. This is consistent with prior adoption studies which have highlighted user reluctance to adopt new technology if there is a perception of risks to their operations or data.
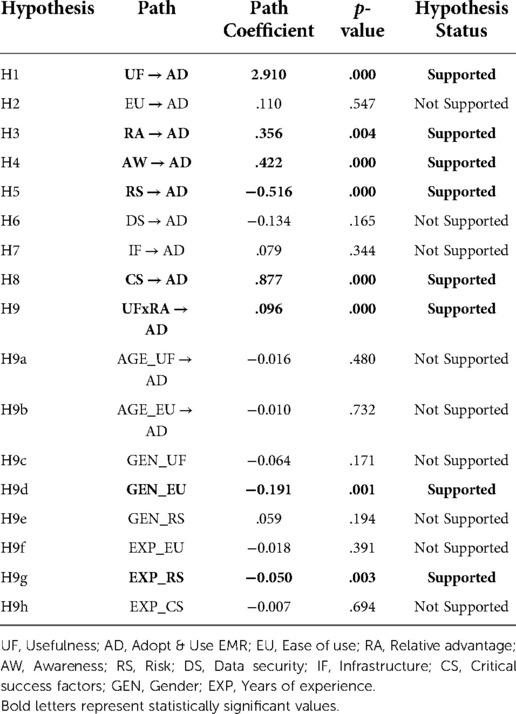
Table 4. Hypotheses test results.
Poor health information system has been identified as a major challenge in the health-care system in many sub-Saharan African countries including Nigeria. Although, EMR is an important tool to improve access to patient information with attendant improved quality of care, EMR has not been widely implemented/adopted in sub-Saharan Africa especially Nigeria. Thus, this study sought to identify factors that affect the adoption of EMR in Nigeria.
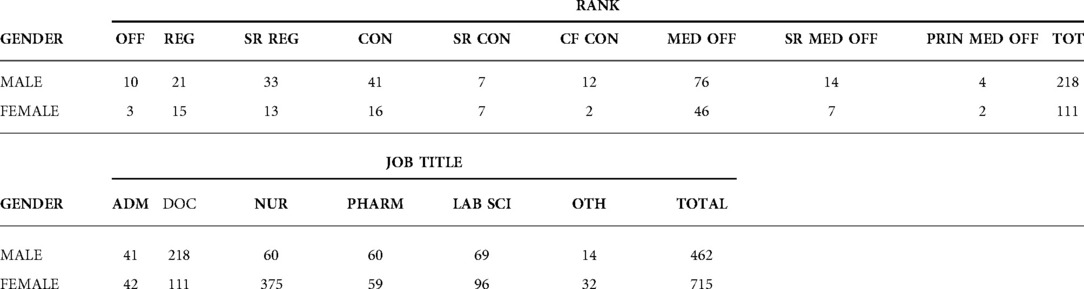
The demographics of this study reveals some interesting findings about the Nigerian health sector. In this study, we deliberately set out to study a good mix of decision makers and system users. Majority of the respondents were female, between the 31–50 age group. Most of the medical facilities were in the public sector. While this is consistent with the age of the working class in Nigeria, the female preponderance presupposes that there are more females in the facilities. However, further analysis suggests they are not equitably distributed in the different cadres, being skewed towards the lower cadres as compared to administrative/managerial positions (see Appendix I). This is in keeping with studies that show that although women make up a large proportion of the health workforce, very few are in senior managerial/leadership positions (40). It was interesting to see that while most of the medical facilities depended on the administration to make decisions on new technology adoption, very few (6.7%) relied on their IT department for such decisions. The reasons may be due to the weak ICT systems currently in place as most of the facilities had ICT units manned by only one or two staff as opposed to having IT departments.
Although the study targeted administrators and those who were able to make decisions in the system, the researchers were surprised to see that only 28% of the respondents were medical doctors. This confirms the global shortage of physicians and the capital flight of physicians in Nigeria.
Our study results also show that the majority of respondents had intermediate level of computer literacy which can directly impact their willingness to adopt and use EMR systems. This is consistent with studies conducted on computer and internet use by doctors in a Nigerian teaching hospital which revealed that the overall proficiency of the respondents in computer-based competencies was below average with only 26.7% sufficiently familiar with computer tools to perform advanced tasks (18, 41). A study of three hospitals in Ethiopia also revealed that health professionals who were computer literate are more likely to adopt EMR than their counterparts who are not computer literate.
In our study, usefulness of new technology was an important facilitator to user willingness to adopt and use the technology. It had the highest impact to increase adoption of EMR with an odds ratio of 18.357, which indicates that user propensity to adopt EMR increases by a factor of 18.357 for every one unit increase in user perception of its usefulness. This is comparable with a study done in Taiwan among Nurses (42) and in another study done in Sri Lanka, where human factors such as lack of awareness on the benefits of EMR, lack of knowledge and experience on how to use EMR, negative perceptions and attitudes on EMR were vital barriers to successful implementation and adoption of EMR (43). Also, a study among Physicians in Iran showed that perceived usefulness has a direct and significant effect on physicians' attitudes toward EMRs' adoption (44). A systematic review by Ross et al. (9) showed that usefulness was an important factor in adoption of EMR. These however contrast with a study in Skopje, Macedonia among health professionals which showed that usefulness of a new technology was not an important factor in its adoption (45).
Perceived ease of use and awareness which are important factors for adoption in this study have been linked with training, knowing the benefits of EMR, access to information, improved knowledge and experience of EMR. Surprisingly, ease of use (H2) was not deemed to be very crucial for the adoption and usage of EMR hence the hypothesis was not supported despite many prior studies showing that ease of use is relevant to user adoption and use of new technology (43). A study on acceptance of health information technology among health professionals revealed that ease of use was an important factor on the adoption of EMR (45). In other studies, ease of use was a significant contributor to adoption of EMR (42, 46).
Critical success factors that guide management and stakeholders' decisions to adopt new technology was significant in this study and had an odds ratio of 2.404 which indicates that user propensity to adopt EMR increases by a factor of 2.404 for every one unit increase in user perception of its critical success factor. Management and stakeholder engagement and support increases adoption and implementation of EMR through fostering a sense of ownership, building confidence, acceptance, enjoyment and self-pride (9). Organizational leadership had been shown to play a great role in providing resources to adopt and use EMRs. Results from a study on Jordan hospitals revealed a positive relationship between management support and adoption of new technology (47). Pantuvo et al. (48) revealed that the critical success factors for adoption and implementation of EMR in Nigeria were enforceable legislation.
Awareness with odds ratio of 1.525 was significant and indicates that user propensity to adopt EMR increases by a factor of 1.525 for every one unit increase in user awareness. Previous study had linked awareness to having good attitude towards EMR. A study of three hospitals in Ethiopia showed that health professionals who had good attitude towards EMR were 1.56 times more likely to readily adopt EMR compared to those health professionals who had poor attitude (3). Access to information and knowledge increases the adoption of EMR (41). This may be due to the fact that health professionals who have information on EMR or witnessed EMR being used before with the visibility of its benefit may have the tendency to accept the advantage of technology and likely to be ready for EMR adoption. Relative advantage, which is the way new technology will perform better than the one being replaced, will also influence decisions to adopt the technology. In this study, relative advantage had an odds ratio of 1.427 which indicates that user propensity to adopt EMR increases by a factor of 1.427 for every one unit increase in user perception of its relative advantage. This is similar to the study by Scott et al. (49) on uptake of the Canadian Heart Health Kit which found that relative advantage significantly influences physicians' intention to use the new innovation. The mediation test shows that relative advantage also has a significant positive impact on the usefulness of EMR.
Previous authors had described available resources to include the availability of suitable infrastructure important for implementation of EMR successfully. Infrastructure features included electricity supply, available bandwidth, access to reliable internet connectivity, access to computers, electrical power and access to phone lines and mobile phones (9). In Nigeria, lack of constant supply of electricity (48) as well as poor internet services are barriers to successful adoption and implementation of a nationwide EMR (41). Infrastructural availability is a major inhibitory factor to the adoption of EMR in Nigeria as documented by other studies but was found not to be statistically significant in our study. Many hospitals in Nigeria depend mainly on alternative power supply commonly called “generator” for their operations, EMR may not be used consistently because of the constant power outage. Also, internet connectivity is very low in Nigeria. A study conducted on the use of health information and communication technologies by health workers in seven state hospitals and a private hospital in the South Western Zone, Ogun State, Nigeria, reported that only one of the hospitals examined was connected to the internet, and none of them had a website (50). Previous study showed that health professionals who believed that there was good technical Infrastructure for EMR system were 1.78 times more likely to adopt EMR system (3).
In this study risk and safety of data were negatively correlated with adoption of EMR as they both had negative coefficients. This indicates that user perception of risk and safety of their data when using EMR decreases their propensity to adopt EMR. This is comparable with a systematic review on factors that influence the implementation of e-health, where concerns over patients’ privacy, security threats and perceived threats over patients and health professionals' relationship were seen as barriers to adoption of EMR (9). A study on factors affecting the adoption of EMR by nurses in Tamil Nadu, India, showed that risk was a barrier to adoption of EMR (46). In this study, the moderation test revealed that age, gender and experience do not have direct significant impact on user decision to adopt and use EMR. This is in contrast to a study done in Ethiopia that revealed that health professionals aged 30–34 years were 52% less likely to be ready for EMR system than younger health professionals (3) and another systematic review that showed that younger primary care physicians were more inclined to use EMR than older physician (13). This maybe so because younger respondent had multiple access to internet than older respondent (51). More so, younger people naturally tend to have more motive, interest, and readiness to accept new technology developments than older people (3).
The results of our study also showed that age did not have any moderating impact on usefulness or ease of use of EMR. Biruk et al. (3) found out that male health professionals were 1.87 times more likely to be ready to adopt EMR system than female health professionals. However, in our study, gender had a significant impact (p < .05) on user perception on ease of use of EMR and hence influence it adoption. This may be so because several studies have shown that males are more proficient in computer use than females (41, 51). Also, experience has significant impact (p < .05) on user perception of risk when it comes to the adoption of EMR.
This study set out to explore the factors that influence the decision of healthcare professionals to adopt and use an EMR system in developing countries. A conceptual adoption model was developed based on an extended TAM model which included constructs of awareness, risks, data security, infrastructure and relative advantage to investigate the propensity of stakeholders in Nigeria to adopt and use electronic medical records. The results of our model testing shows that usefulness has the highest impact on adoption of EMR. This is followed by critical success factor, awareness and relative advantage. However, though infrastructure availability and ease of use were also important in the model, they were not statistically significant. Meanwhile, user perception of risk and safety of their data when using EMR decreases user propensity to adopt EMR.
Our results suggest that the Nigerian health care delivery system is ready to adopt EMR. However, several challenges remain for the successful adoption and implementation of EMR in the Niger Delta region and by implication similar contexts in developing countries. In this study, infrastructural availability being lack of or poor internet connectivity and lack of constant supply of electricity were not seen as barriers to successful adoption and implementation of an EMR system. While this may be due to dependence by many hospitals in Nigeria on alternative power supply for their operations, however, this remains a huge challenge, especially in peripheral facilities as EMR may not be used consistently because of the constant power outage. Lack of functional websites is also a challenge for majority of the hospitals.
We therefore make the following policy recommendations:
The key role of the government in health would be improved formulation of policies on EMR adoption with regulatory bodies to oversee its implementation. In Nigeria, EMR is a new technology in the nascent stages of adoption in several states. Regulation is also rudimentary. The government thus should be actively involved, designating appropriate agencies to partner with the federal ministry of health to develop regulatory policies and guidelines. More so, there should be increased funding to health and functional health records department in all health facilities. The government, management and stakeholders should ensure improvement of infrastructures for the adoption, implementation and sustainability of EMR. Stable electricity to health facilities should be prioritized. Government should fast-track the development of an e-health infrastructure, such as internet backbone and satellite technology, as well as the spread of high-speed broadband data services. Develop legislative and implementation frameworks for public-private partnerships in the health sector in order to attract private sector investment and ensure the sustainability of EMR projects. Regulation of data safety, protection and Risk management should be addressed to encourage stakeholder buy-in for adoption of EMR.
The management should also prioritize and invest in EMR implementation and maintenance of innovative EMR systems that will lead to more efficient service delivery at their facilities. The investment will cover training, infrastructure installation and maintenance. Management should set up an effective system that will deal with feedbacks promptly.
In preparation for the adoption of digital interventions especially EMRs in LMICs, hospital management need to be ready to commit the resources and investments to make them successful. Topmost on the priority list would be electrical power supply and deploying adequately trained staff to run functional ICT departments. This would be key to the smooth functioning of any EMR system.
Critical success factor such as early involvement of stakeholders to build up the requirements of end users and reduce resistance to change is highly recommended. The perceived benefits of EMR should be identified and communicated to stakeholders as much as possible. The hospital management should be involved in enforcing policies on EMR, training and motivating the workforce and have sustainable funding for EMR. Training and retraining of medical personnel should also be encouraged through in-school training on medical informatics, in-service training on ICT and continuing medical education.
To ensure effective implementation, Training of all personnel on management of the system should also be encouraged, besides in-service training on ICT medical informatics. There is also need to integrate in-school training on medical informatics in medical and allied medical courses as all members of the health team would be end users of any EMR system.
EMR system vendors should demonstrate its usefulness and ease of use to the healthcare workers beyond reasonable doubt. Safety of data should be sacrosanct. This should guide their decision on which type to EMR program to buy into. This process should be rigorously and painstakingly done because one breach is enough to lead to system collapse, loss of confidence and numerous litigations. The administrator should have a mechanism at inception of EMR that will work at identifying, categorizing and assessing cyber risks. Mitigation of risks should be prompt and demonstrable so as to engender confidence in the system.
At individual level, our results showed that critical success factor showed a positive impact on ease of adoption. This suggests that both the end users and administrators should understand and promote EMR systems, with adequate reference to successful systems to motivate their staff to adopt and use it. Improving awareness will encourage staff to invest their time and finances to educate and upgrade themselves in preparation for adoption of IT innovations which is critical to improved patient care and service delivery.
We recommend further research on readiness to adopt other digital innovations for the health system including medical decision-making systems and telemedicine.
This study was cross-sectional quantitative research focused only on the Niger Delta region of Nigeria. Due to budgetary and time constraints, it could not be extended to the western and northern states. However, we are of the opinion that the adoption challenges faced in the states selected for this study will be very similar to those faced across the whole country. We will therefore recommend further research with a national coverage. Our study also focused just on the adoption of EMR but there are many other medical decision support systems in use today. Hence, we also encourage future research to focus on adoption of medical decision support systems and telemedicine in similar contexts.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by University of Uyo Teaching Hospital, Uyo Institutional Health Research Ethical Committee (IHREC). Ref: UUTH/AD/S/96/VOL.XXI/564. The patients/participants provided their written informed consent to participate in this study.
CDA: Study conception and objectives, questionnaire design, coordination of pilot and full data collection, writing of parts of discussion and conclusion. HMS: Questionnaire design, Conceptual design and hypotheses formulation, pilot data analysis, writing of methodology, data analysis and writing of results section, abstract and manuscript formatting. NE: Study objectives, Questionnaire design, Data collection, Writing part of the discussion writing of results section, abstract and manuscript formatting policy recommendations. CMI: Study objectives, Questionnaire design, Data collection, Writing part of the discussion writing of results section, abstract and manuscript formatting policy recommendations. NFA: Questionnaire design, Writing part of the discussion, abstract and manuscript formatting, policy recommendations. OM: Questionnaire design, manuscript formatting. ED: Writing of introduction and literature review, data collection. EU: Loading of questionnaire into ODK, managing data collected, exporting of data collected into Excel format ready for analysis, Coordination of field project, ensuring integrity of data. VE: Writing of introduction and literature review. FMO: Study conception and design, overall manuscript proofreading and correction. All authors contributed to the article and approved the submitted version.
This is the first of a series of papers on adoption of technological innovations in LMICs. This study is a subset of preliminary papers on a grant from the New Frontiers in Research Fund of Canada. New Frontiers in Research Fund Exploration (Toronto, Ontario, CAt GRANT_NUMBER: #102079).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Alotaibi YK, Federico F. The impact of health information technology on patient safety. Saudi Med J. (2017) 38(12):1173. doi: 10.15537/smj.2017.12.20631
2. Odekunle FF. Current roles and applications of electronic health record in the healthcare system. Int J Med Res Health Sci. (2016) 5(12):48–51.
3. Biruk S, Yilma T, Andualem M, Tilahun B. Health Professionals’ readiness to implement electronic medical record system at three hospitals in Ethiopia: a cross sectional study. BMC Med Inform Decis Mak. (2014) 14(1):115. doi: 10.1186/s12911-014-0115-5
4. Hamilton C. The WHO-ITU national eHealth strategy toolkit as an effective approach to national strategy development and implementation. Stud Health Technol Inform. (2013) 192:913–6.23920691
5. Manca DP. Do electronic medical records improve quality of care? Can Fam Physician. (2015) 61(10):846–7.26472786
6. Alpert J. The electronic medical record in 2016: advantages and disadvantages. Digit Med. (2016) 2:48. doi: 10.4103/2226-8561.189504
7. Institute of Medicine (US) Committee on Data Standards for Patient Safety. Key Capabilities of An Electronic Health Record System Letter Report [Internet]. Key Capabilities of an Electronic Health Record System: Letter Report. US: National Academies Press (2003) [cited 2022 Mar 25]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK221800/
8. Holden RJ, Karsh BT. The technology acceptance model: its past and its future in health care. J Biomed Inform. (2010) 43(1):159–72. doi: 10.1016/j.jbi.2009.07.002
9. Ross J, Stevenson F, Lau R, Murray E. Factors that influence the implementation of e-health: a systematic review of systematic reviews (an update). Implement Sci. (2016) 11(1):146. doi: 10.1186/s13012-016-0510-7
10. Safi S, Thiessen T, Schmailzl KJ. Acceptance and resistance of new digital technologies in medicine: qualitative study. JMIR Res Protoc. (2018) [cited 2021 Apr 6] 7(12):e11072. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6299231/ doi: 10.2196/11072
11. de Almeida JPL, Farias JS, Carvalho HS, de Almeida JPL, Farias JS, Carvalho HS. Drivers of the technology adoption in healthcare. BBR Brazilian Bus Rev. (2017) 14(3):336–51. doi: 10.15728/bbr.2017.14.3.5
12. Gesulga JM, Berjame A, Moquiala KS, Galido A. Barriers to electronic health record system implementation and information systems resources: a structured review. Procedia Comput Sci. (2017) 124:544–51. doi: 10.1016/j.procs.2017.12.188
13. O’Donnell A, Kaner E, Shaw C, Haighton C. Primary care physicians’ attitudes to the adoption of electronic medical records: a systematic review and evidence synthesis using the clinical adoption framework. BMC Med Inform Decis Mak. (2018) 18(1):101. doi: 10.1186/s12911-018-0703-x
14. van der Meijden MJ. Determinants of success of inpatient clinical information systems: a literature review. J Am Med Inform Assoc. (2003) 10(3):235–43. doi: 10.1197/jamia.M1094
15. Chae YM, Yoo KB, Kim ES, Chae H. The adoption of electronic medical records and decision support systems in Korea. Healthc Inform Res. (2011) 17(3):172. doi: 10.4258/hir.2011.17.3.172
16. Mu’awiyyah BS, Hussien AT, Abdulazeez AO, Istifanus AJ. Knowledge, attitude and perception of healthcare workers on use of electronic medical records in ahmadu bello university teaching hospital, Zaria, Kaduna State Northwest Nigeria. J Med Bas Sci Res. (2021) 2(1):1–12.
17. Odekunle FF, Odekunle RO, Shankar S. Why sub-Saharan Africa lags in electronic health record adoption and possible strategies to increase its adoption in this region. Int J Health Sci. (2017) 11(4):59.
18. Kamadjeu RM, Tapang EM, Moluh RN. Designing and implementing an electronic health record system in primary care practice in sub-Saharan Africa: a case study from Cameroon. Inform Prim Care. (2005) 13(3):179–186. doi: 10.14236/jhi.v13i3.595
19. Odoyo C, Liyala S, Odongo B, Abeka S. Theory of reasoned action as an underpinning to technological innovation adoption studies. World J Comput Appl Technol. (2016) 4:1–7. doi: 10.13189/wjcat.2016.040101
20. Alwahaishi S, Snášel V. Modeling the determinants influencing the diffusion of mobile internet. J Phys: Conf Ser. (2013) 423:012037. doi: 10.1088/1742-6596/423/1/012037
21. Ammenwerth E. Technology acceptance models in health informatics: TAM and UTAUT. Stud Health Technol Inform. (2019) 263:64–71.31411153
22. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. (1989) 13(3):319–40. doi: 10.2307/249008
23. Gefen D, Karahanna E, Straub DW. Trust and TAM in online shopping: an integrated model. MIS Q. (2003) 27(1):51–90. doi: 10.2307/30036519
24. Awamleh R, Fernandes C. Internet Banking: An empirical investigation into the extent of adoption by banks and the determinants of customer satisfaction in the United Arab Emirates.
25. Moon JW, Kim YG. Extending the TAM for a world-wide-web context. Inform Manage. (2001) 38(4):217–30. doi: 10.1016/S0378-7206(00)00061-6
26. Lundvall BA. Innovation as an interactive process: user-producer interaction to the national system of innovation. Afr J Sci Technol Innov Dev. (2009) 1(2_3):10–34.
27. Sumter LQ. Cloud computing: security risk. Inproceedings of the 48th annual southeast regional conference (2010). p. 1–4
28. Qian Y, Fang Y, Gonzalez JJ. Managing information security risks during new technology adoption. Comput Secur. (2012) 31(8):859–69. doi: 10.1016/j.cose.2012.09.001
29. Porter WW, Graham CR. Institutional drivers and barriers to faculty adoption of blended learning in higher education. Br J Educ Technol. (2016) 47(4):748–62. doi: 10.1111/bjet.12269
30. Sabi HM, Uzoka FM, Langmia K, Njeh FN, Tsuma CK. A cross-country model of contextual factors impacting cloud computing adoption at universities in sub-saharan Africa. Inform Syst Front. (2018) 20(6):1381–404. doi: 10.1007/s10796-017-9739-1
31. Akinnuwesi BA, Uzoka FM, Fashoto SG, Mbunge E, Odumabo A, Amusa OO, et al. A modified UTAUT model for the acceptance and use of digital technology for tackling COVID-19. Sustainable Oper Comput. (2022) 3:118–35. doi: 10.1016/j.susoc.2021.12.001
32. Creswell JW. Mapping the field of mixed methods research. J Mix Methods Res. (2009) 3(2):95–108. doi: 10.1177/1558689808330883
33. Collect data anywhere. Available from: https://getodk.org/ (Accessed July 8, 2022).
34. Kaiser HF, Rice J. Little jiffy, mark IV. Educ Psychol Meas. (1974) 34(1):111–7. doi: 10.1177/001316447403400115
35. Kaiser HF. The application of electronic computers to factor analysis. Educ Psychol Meas. (1960) 20(1):141–51. doi: 10.1177/001316446002000116
36. Tabachnick BG, Fidell LS. Experimental designs using ANOVA. Belmont, CA: Thomson/Brooks/Cole (2007).
37. Field T. Prenatal depression effects on early development: a review. Infant Behav Dev. (2011) 34(1):1–4. doi: 10.1016/j.infbeh.2010.09.008
38. Pallant J. SPSS Survival manual: A step by step guide to data analysis using IBM SPSS. 7th ed. Maidenhead: Routledge Open University Press (2020).
39. Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol Methodol. (1982) 13:290–312. doi: 10.2307/270723
40. World Economic Forum. 7 out of 10 global health leaders are men: 7 out of 10 global health leaders are men according to a new report | World Economic Forum (weforum.org). Accessed.
41. Awokola BI, Abioye-Kuteyi EA, Ogundele OA. Computer and internet use by doctors in a Nigerian Teaching Hospital: A survey of the wesley guild unit of Obafemi Awolowo University Teaching Hospitals complex. World Fam Med J. (2011) 99(305):1–5. 11th July 2022. doi: 10.5742/mejfm.2011.99086
42. Kuo KM, Liu CF, Ma CC. An investigation of the effect of nurses’ technology readiness on the acceptance of mobile electronic medical record systems. BMC Med Inform Decis Mak. (2013) 13(1):1–4. doi: 10.1186/1472-6947-13-1
43. Dayananda M. Factors influencing adoption of electronic medical records in government hospitals of Sri Lanka. Int J Sci Res Comput Sci Eng Inform Technol. (2020) 6(6):190–9. doi: 10.32628/CSEIT206624
44. Abdekhoda M, Ahmadi M, Gohari M, Noruzi A. The effects of organizational contextual factors on physicians’ attitude toward adoption of Electronic Medical Records. J Biomed Inform. (2015) 53:174–9. doi: 10.1016/j.jbi.2014.10.008
45. Ketikidis P, Dimitrovski T, Lazuras L, Bath PA. Acceptance of health information technology in health professionals: an application of the revised technology acceptance model. Health Informatics J. (2012) 18(2):124–34. doi: 10.1177/1460458211435425
46. Singh B, Muthuswamy P. Factors affecting the adoption of electronic health records by nurses. World Appl Sci J. (2013) 28(11):1531–5.
47. AL-nassar BA, Abdullah MS, Sheik Osman WR. Overcoming challenges to use electronic medical records system (EMRs) in Jordan hospitals. Int J Comput Sci Netw Secur. (2011) 11(8):51–8.
48. Pantuvo JS, Naguib R, Wickramasinghe N. Towards implementing a nationwide electronic health record system in Nigeria. Int J Healthc Deliv Reform Initiat. (2011) 3(1):39–55. doi: 10.4018/jhdri.2011010104
49. Scott SD, Plotnikoff RC, Karunamuni N, Bize R, Rodgers W. Factors influencing the adoption of an innovation: an examination of the uptake of the Canadian Heart Health Kit (HHK). Implement Sci. (2008) 3(1):1–8. doi: 10.1186/1748-5908-3-41
50. Ajiboye BA, Adekoya AJ, Alawiye MK, Oyedipe WJ. Knowledge and utilization of health information and communication technologies (HICTs) by health workers of the North-Eastern health zone of Ogun State, Nigeria. Informatics Health Soc Care. (2014) 39(2):104–23. doi: 10.3109/17538157.2013.858044
51. Asangansi IE, Adejoro OO, Farri O, Makinde O. Computer use among doctors in Africa: survey of trainees in a Nigerian teaching hospital. J Health Inform Dev Ctries. (2008) 2(1).
.

.

.
.
.
.
.
.
.
Keywords: electronic medical records, digital health, medical informatics, adoption of eHealth, Nigeria, developing countries
Citation: Akwaowo CD, Sabi HM, Ekpenyong N, Isiguzo CM, Andem NF, Maduka O, Dan E, Umoh E, Ekpin V and Uzoka F (2022) Adoption of electronic medical records in developing countries—A multi-state study of the Nigerian healthcare system. Front. Digit. Health 4:1017231. doi: 10.3389/fdgth.2022.1017231
Received: 11 August 2022; Accepted: 28 October 2022;
Published: 21 November 2022.
Edited by:
Sonika Tyagi, Monash University, AustraliaReviewed by:
Vinaytosh Mishra, Fore School of Management, India© 2022 Akwaowo, Sabi, Ekpenyong, Isiguzo, Andem, Maduka, Dan, Umoh, Ekpin and Uzoka. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Humphrey Muki Sabi aHVtcGhyZXlzYWJpQGdtYWlsLmNvbQ==
Specialty Section: This article was submitted to Health Informatics, a section of the journal Frontiers in Digital Health
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.