
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Digit. Health, 07 December 2022
Sec. Health Technology Implementation
Volume 4 - 2022 | https://doi.org/10.3389/fdgth.2022.1006447
This article is part of the Research TopicScaling-Up Health-IT - Sustainable Digital Health Implementation and DiffusionView all 9 articles
 Salomé Azevedo1,2,3,†
Salomé Azevedo1,2,3,† Federico Guede-Fernández1,4,†
Federico Guede-Fernández1,4,† Francisco von Hafe1,2
Francisco von Hafe1,2 Pedro Dias1,2
Pedro Dias1,2 Inês Lopes5Nuno Cardoso5Pedro Coelho2,6Jorge Santos6José Fragata2,6Clara Vital6
Inês Lopes5Nuno Cardoso5Pedro Coelho2,6Jorge Santos6José Fragata2,6Clara Vital6 Helena Semedo6Ana Gualdino6
Helena Semedo6Ana Gualdino6 Ana Londral1,2*
Ana Londral1,2*
Background: COVID-19 increased the demand for Remote Patient Monitoring (RPM) services as a rapid solution for safe patient follow-up in a lockdown context. Time and resource constraints resulted in unplanned scaled-up RPM pilot initiatives posing risks to the access and quality of care. Scalability and rapid implementation of RPM services require social change and active collaboration between stakeholders. Therefore, a participatory action research (PAR) approach is needed to support the collaborative development of the technological component while simultaneously implementing and evaluating the RPM service through critical action-reflection cycles.
Objective: This study aims to demonstrate how PAR can be used to guide the scalability design of RPM pilot initiatives and the implementation of RPM-based follow-up services.
Methods: Using a case study strategy, we described the PAR team’s (nurses, physicians, developers, and researchers) activities within and across the four phases of the research process (problem definition, planning, action, and reflection). Team meetings were analyzed through content analysis and descriptive statistics. The PAR team selected ex-ante pilot initiatives to reflect upon features feedback and participatory level assessment. Pilot initiatives were investigated using semi-structured interviews transcribed and coded into themes following the principles of grounded theory and pilot meetings minutes and reports through content analysis. The PAR team used the MoSCoW prioritization method to define the set of features and descriptive statistics to reflect on the performance of the PAR approach.
Results: The approach involved two action-reflection cycles. From the 15 features identified, the team classified 11 as must-haves in the scaled-up version. The participation was similar among researchers (52.9%), developers (47.5%), and physicians (46.7%), who focused on suggesting and planning actions. Nurses with the lowest participation (5.8%) focused on knowledge sharing and generation. The top three meeting outcomes were: improved research and development system (35.0%), socio-technical-economic constraints characterization (25.2%), and understanding of end-user technology utilization (22.0%).
Conclusion: The scalability and implementation of RPM services must consider contextual factors, such as individuals’ and organizations’ interests and needs. The PAR approach supports simultaneously designing, developing, testing, and evaluating the RPM technological features, in a real-world context, with the participation of healthcare professionals, developers, and researchers.
The last two decades of research and development (R&D) on remote patient monitoring (RPM) technologies mainly focused on the technicalities of providing care in unusual environments (1). Although RPM pilot design changes on a case-by-case basis, the system should comprise three components: the care team organization, the technology used, and patient engagement activities (2). Several pilot initiatives emerged from chronic diseases (3) to episodic care [e.g., surgical follow-ups (1)] to exploit the benefits of RPM, such as, continuity of outpatient care (4), improved healthcare decision-making (1), complications anticipation (4), and cost reduction (5). In surgical follow-up care, RPM can significantly reduce severe complications and increase patient safety in the most critical period after hospital discharge (6) by supporting healthcare professionals in the continuous surveillance of clinical and patient-reported outcome measures (PROMs). However, research on implementation is scarce (7). In addition, after coronavirus disease 2019 (COVID-19) pandemic outbreak, the increasing demand for RPM-based services to cope with postponing surgeries (8) and shifting in-person to remote care (9) drove ongoing pilot initiatives to scale up faster without planning (10). Constrained by time and resources, the design, development, and implementation of the scaled-up services pose risks to the access and quality of care (11).
After COVID-19, some peer-reviewed work focused on RPM implementation and two generated relevant knowledge (2,12). A French case study documents the design methodology used by a multidisciplinary team for an RPM system for cancer care (2). The authors position the RPM implementation as both a technological and organizational innovation. Therefore, an RPM service is a socio-technical system framed within a local context. The authors also reinforce the collaboration between multidisciplinary groups for proper needs identification. In a rapid implementation of a COVID-19 RPM intervention in the United States of America (USA), a team with industry, healthcare delivery, and academia members repurposed an existing application. Their study revealed an increased patient perception of safety and the emergence of an organizational method of resident and staff rotation (12). Nevertheless, both works are context-specific and different from the surgical follow-up context, which is this paper’s focus. On top of that, the first work lacks deeper knowledge of how the design, implementation, and evaluation phases are related. The second work had limitations on feature customization, reducing the opportunity to absorb feedback through iterative development cycles.
Scalability and rapid implementation of RPM services require social change and active collaboration between stakeholders. Therefore, a participatory action research (PAR) approach is needed to support the collaborative development of the technological component while simultaneously implementing and evaluating the RPM service through critical action-reflection cycles (13). Throughout a research process characterized by nonlinear, recursive cycles of action and reflection, the PAR team characterizes problems in specific contexts, understands the required changes in socio-technical systems, and consequently defines, implements, and evaluates actions to improve practice (14). There are several expected outcomes from following a PAR approach. For the scope of this paper, the farmer participatory research model (15) highlights some of the most relevant outcomes that can be adapted for the implementation of RPM services: (1) generation and adoption of new appropriate technologies by healthcare professionals and patients to increase RPM uptake in surgical follow-up; (2) better understanding, on the part of researchers, of the existing surgical follow-up service; (3) scientific characterization and understanding of the socio-technical-economics constraints to sustainable RPM care delivery; (4) development of RPM technologies that meet patients and healthcare professionals needs; (5) improved research and technological systems as a consequence of a close collaboration; (6) empowerment by improving healthcare professionals’ capacity for self-directed technology development; and finally (7) ability to adapt healthcare systems to changing conditions.
In this paper, we propose a PAR approach to guide researchers, developers, and healthcare professionals in scaling up RPM pilot initiatives and implementing RPM-based surgical follow-up services. Based on a case study in the cardiothoracic surgical department, in a Portuguese public hospital, we analysed feedback from interviews, reports, and meeting minutes from different stakeholders in the context of three previous different RPM pilot initiatives, to identify and prioritize the features required to efficiently scale up an RPM-based system.
In 2020, in the scope of the COVID-19 pandemic, the Portuguese Foundation for Science and Technology (Fundação Portuguesa para a Ciência e Tecnologia - FCT) launched a tender to support Research and Development (R&D) projects in the areas of data science and artificial intelligence (AI) in Public Administration (16). The main objective was to promote projects that could cope with pandemic-imposed challenges, improve public health services, and support citizens in better decision-making concerning health behaviors. FCT required the participation of at least one public administration entity providing health care committed to using the project results and the R&D activities. Another requirement was to provide a Data Management Plan that preserved the use of data ethical and legal aspects, such as privacy and consent issues in citizens’ data access, data sharing across different sources, and transparency of the analysis and utilization. The projects could last 24 to 36 months with a maximum funding limit per project of 240 thousand euros. This tender allocated 3 million euros from a national-based fund budget.
A consortium of four partners working with RPM technologies received approval and funding for a 36-month project, evaluated with 7.3 on a 10-point scale as a “High-Impact” proposal. With a total budget of approximately 240 thousand euros, the main goal was to leverage an ongoing RPM-based follow-up pilot service at the Cardiothoracic Surgery Department of Hospital de Santa Marta, Lisbon, Portugal. The challenge involved consolidating each partner’s previous work with RPM technologies to make the system more robust and ready to integrate intelligent and adaptable digital tools that could allow the redesign and value assessment of the RPM surgical follow-up service for at least 150 patients.
The four partners, familiar with the PAR approach and respective expected outcomes, agreed to conduct this type of research to define and prioritize the development of the RPM platform features. One of the most relevant reasons is its application as a bottom-up research and development strategy for technology transfer (15,17,18) within the hospital walls. More specifically, the PAR approach is very relevant when trying to improve real-world practices because it involves a research team (PAR team) that includes researchers and practitioners who contribute actively with their scientific and practical knowledge in all research procedure phases (15).
This paper describes, using a case study strategy, how and why the PAR team identified features from previous projects and prioritized the development of an enhanced RPM-based platform in a real-world setting when there was no control over contemporary events (19). The case study has been referred to as an appropriate research strategy to enhance the phases and the transitions across the reflection and action phases (19,20). This strategy becomes particularly useful in health services research (21), particularly in this paper, to better evaluate the essential RPM-based follow-up services’ features to each relevant stakeholder and why in the context of cardiothoracic surgery (22).
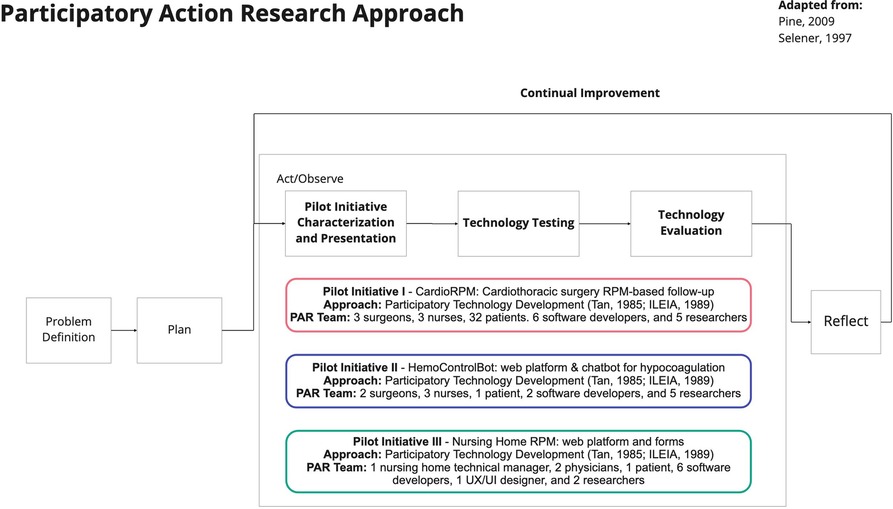
The participatory research process presented in Figure 1 involved four phases that lasted 27 months. The process is an adaption from the cycle described by Pine (18) and the models for Participatory Action Research in Organizations and the Farmer Participatory Research described by Selener (15). In the following sections, we describe the activities conducted in each phase.
The four partners were categorized into two groups according to the type of organization:
• Hospital: Hospital de Santa Marta is a state-owned public Central Hospital serving the Greater Lisbon area as part of the Central Lisbon University Hospital Centre (CHULC). It is one of the Country’s leading Internal Medicine schools and one of Portugal’s main reference centers for diagnosing and treating cardiovascular disease (23).
• Research Laboratories: One of the research laboratories focuses on applied and project-oriented research in technology development for predictive, preventive, personalized, and participatory medicine (24). The second research laboratory focuses on supporting, developing, and fostering clinical, public health, and health services research (25). The third research laboratory focuses on validating innovative methodologies to measure outcomes and costs and provide trustful scientific evidence under Value-based Healthcare principles (26).
Each partner was responsible for selecting the PAR team participants and classifying the members’ roles according to their interests in the research process without requiring a minimum number of participants. The team was composed of 12 members split according to three roles types (act as a proxy for the stakeholder groups):
• Researchers: the main interest of this group was to conduct research to generate and contribute knowledge to their scientific area. The research laboratories selected six researchers based on their expertise in digital health services design, digital health literacy, cost analysis, and previous relationship with the healthcare professionals team.
• Developers: the main interests of the developers include designing, programming, building, deploying, and maintaining features through the use of different skills and programming tools. The research laboratories selected six software developers based on their skills in AI and software development and previous relationship with the healthcare professionals team.
• Healthcare professionals (end-users): the main interest of healthcare professionals was to use technology to enhance their performance and provide high-quality patient care. In the context of the proposed technological solution, the end-users are physicians and nurses of the Cardiothoracic Surgery service selected by the service’s director. Therefore, the PAR team included three physicians and three nurses to collaborate with the developers and researchers to solve RPM-related problems. They were selected based on their previous relationship with researchers and developers and expertise in RPM-based follow-up services.
The Problem Definition Phase aimed to clarify the problem and involved three activities at two different moments: the first at the time of the grant proposal writing and the second, in a 90-min video conference group meeting, after the grant award notification. The activities for the problem formulation are the ones suggested in Design Science Research: precise problem definition, problem positioning and justification, and root causes identification (27).
The grant proposal writing included two activities. First, the PAR team conducted a literature review of academic publications (fields of cardiothoracic surgery, AI and data science, and decision support systems engineering). The team defined the problem through online collaboration using a web-based word processing application because it allows keeping track of changes and comments. To formulate the problem more precisely, the team used the web application to leave comments with feedback on others’ contributions. The final version of the problem was: in the COVID-19 pandemic context, characterized by a high demand for remote care to avoid infection, there is limited access to RPM-based surgical follow-up services.
The second activity aimed to position and justify the problem so the different PAR groups could engage in the proposal writing. Therefore, each group consolidated their perceived reasons for the problem to be relevant. The PAR team’s opinions of why the problem is significant and to whom can be split into two stakeholder groups: (i) Healthcare professionals and providers and (ii) Software developers and Researchers. On the one hand, the first group contextualized the problem as an obstacle to providing treatment to a larger sample of patients while maintaining essential high-quality healthcare using RPM and transferring the acquired knowledge and technology to other surgical follow-up services. “(Senior Surgeon) stressed that the objectives are to continue and expand the monitoring of patients undergoing cardiothoracic surgery and that this monitoring can be extrapolated to other units.”. On the other hand, the second group positioned the problem considering its scalability and the need to implement a clinical study with real-world evidence to analyze the costs and benefits of a generalized RPM service. “(Senior researcher) mentioned that it could be interesting in making the RPM platform available for other problems.”
After the grant award notification, during the project kick-off session, the PAR team focused on finding the root causes of the problem. The meeting was planned to last one hour, and all PAR team members were invited. Due to COVID-19 constraints, the meeting occurred via a video-based communication platform. To guarantee that the researchers were seen as colleagues, there was no moderator (15). There was only a note-taker, which was randomly assigned at the beginning of the meeting. The note-taker (27) wrote down all mentioned root causes, which were analyzed by the researchers using content analysis (28). Finally, the root causes were represented using an Ishikawa diagram (29). Additional details on the root causes and respective categories of the defined problem are described in the Ishikawa diagram (Supplementary Material 3).
As mentioned in the context subsection, the PAR team had to identify features from previous projects and prioritize the development of a more robust RPM-based platform capable of integrating AI-based and value assessment tools. Therefore, the planning phase aimed at promoting the discussion on the required actions to reach two objectives: (i) decide which pilot initiatives should be investigated for feature extraction; (ii) define the data collection and analysis plan for features’ characterization, evaluation, and prioritization, and reflection on the PAR approach performance.
The PAR team planned one 60-min video conference meeting to achieve these goals. The study selection was based on three inclusion criteria: the project followed a participatory approach, involving at least one of the four partners, who had the ownership of the intellectual property rights.
The researchers used Table 1 to guide the rest of the team in deciding on the appropriate data sources and collection and analysis methods to answer the research questions associated with each pilot initiative characterization. In this phase, 10 PAR team members met in one meeting, which lasted approximately one hour. The two main results of this phase are: the list of pilot initiative studies to extract features and the data collection and analysis plan to characterize each pilot initiative and respective features (Table 2); and the data collection and analysis plan to evaluate and prioritize each feature and reflect on the PAR approach performance.
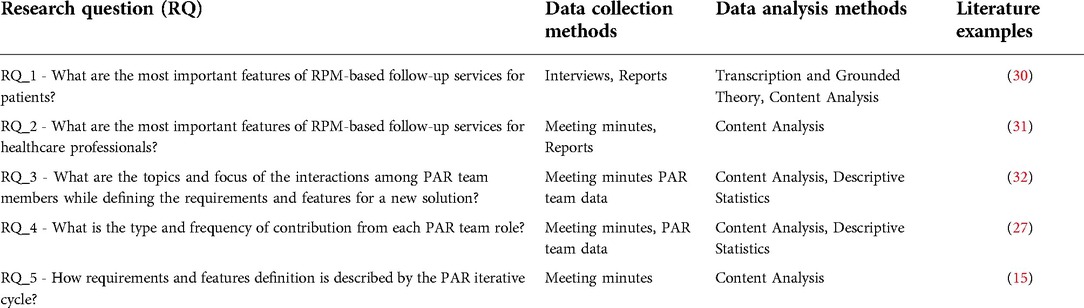
Table 1. Research questions and the respective data collection and analysis methods.
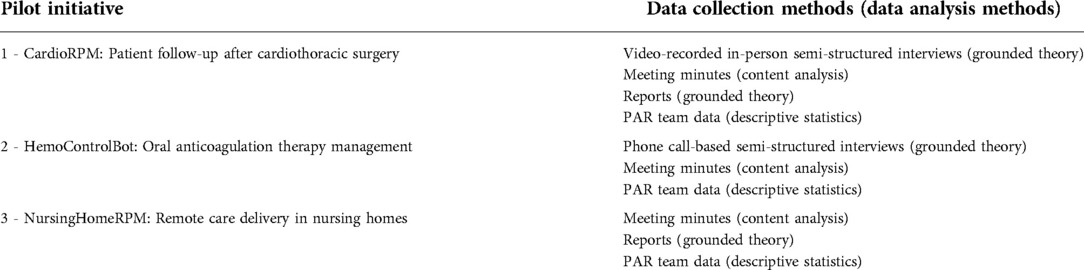
Table 2. List of pilot initiatives and respective data collection and analysis plan.
The PAR team decided that for each pilot initiative, the features should be presented, tested, and evaluated in web-based or in-person (hospital visits) group meetings. They also agreed to use meeting minutes to report participants’ observations and to use content analysis to support the decision of the final list of features and the evaluation of the PAR approach using content analysis (Supplementary Material 1). The format of the group meeting was also a result of the planning phase. At the beginning of each session, the researcher responsible for writing the minute asked for the consent of the participants to take notes on the interventions made by the participants and their respective reactions to the team. At the end of the meeting, the researcher read the out loud minute, requested approval, and proposed a date and agenda for the following meeting.
This phase involved two main activities through several not pre-planned group meetings: (i) the researchers characterized and presented the pilot initiative, its resulting features, and respective end-users feedback evaluation; and (ii) the PAR team tested and evaluated the features.
In the first activity, the researchers described the pilot initiative goal, deployment site, targeted population, previous and new intervention, RPM period, RPM collected outcomes, responsible team, the technology used, pilot activities, pilot duration, end-users involved, and end-users feedback data collection methods. For each identified feature, the researchers presented its originator, and end-users’ feedback. This information was obtained through content analysis of internal and external reports and minutes, and grounded theory analysis of interview transcripts. Internal and external reports were used to record activities execution, bugs and issues identified, and consolidate generated knowledge. Two researchers read each report, extracted all the relevant information, and combined it in a spreadsheet. For each information extracted, the researcher recorded the report date, author, and role. Similarly, all minutes’ observations were copied to spreadsheets, one spreadsheet per meeting. For each observation extracted, the researcher recorded the author. As defined in the planning phase, minutes and reports were coded according to the categories (topic, focus, interaction, reaction, outcome, and agent) described in Supplementary Material 1.
In two pilot initiatives, semi-structured interviews were used to collect patient emotions, attitudes, opinions, and experiences through two different formats: video recording and phone calls. For both, there was one researcher that transcribed each interview in Portuguese. The grounded-theory method was used and included three rounds (33). In the first round, two researchers coded the interviewer’s and interviewee’s quotes as units of text to identify the most frequently covered themes. The researchers combined the emerging themes (feedback on existing features, improvements and new ideas, generated learning, proof of acceptance, and reflections) according to their similarity and deleted the duplicates. The output of the second round allowed the researchers to define a list of possible values for each theme. The third and final round allowed the researchers to code each unit of analysis according to Supplementary Material 2. In the three rounds, when disagreements occurred, the authors reached a consensus via discussion.
The PAR team tested and evaluated the features in the second and final activity. For each feature, the team assessed the required effort, type of changes, and value for the end-user. The format and analysis of the group meetings followed the configuration and data analysis methods agreed on during the planning phase. It is crucial to notice that the presentation, testing and evaluation occurred cyclically per feature or set of features. However, we present the features’ evaluation per pilot initiative to demonstrate the results better.
The reflection phase involved several not pre-planned group meetings to define the final set of features and prioritize the development based on reflections on (i) the pilot initiative participatory level assessment; and (ii) the team’s evaluation of each feature. The participatory level assessment in each pilot initiative consisted of descriptive statistics of the type and level of participation and representation of each stakeholder group. The team used the MoSCoW (must have, should have, could have, and will not have this time) prioritization method (34) to help define agile and fast development sprints based on the previous reflections (35). When disagreements occurred, the PAR team reached an agreement via discussion, considering time and budget constraints and expected outcomes. Finally, the team reflected on the PAR approach performance through descriptive statistics of the meeting minutes content analysis concerning the number of participants and contributions made per phase, focus, topic, and research outcome more frequently referred per phase.
The next subsections describe the results obtained in the two main phases of the PAR approach in the context of this work: action and reflection.
This phase involved 11 meetings with an average participation of nine PAR team members and a duration of 44 min (8 h and 5 min in total). Each pilot initiative followed an iterative development approach illustrated in Supplementary Material 4, the corresponding study was approved by each deployment site’s ethical committee, and all participants signed informed consent.
The first pilot initiative refers to the RPM follow-up pilot service that the PAR team proposed to leverage in the scope of the funded project (Box 1). Therefore, the motivation, goal, deployment site, digitization model, and groups of end-users are the same. The main difference is the new project’s requirement of covering at least 150 patients.
Box 1. Pilot Initiative 1: CardioRPM: Patient follow-up after cardiothoracic surgery (36)
Motivation: The healthcare professionals from the cardiothoracic surgery needed to automatize health-related outcomes collection during the follow-up period after cardiothoracic surgery.
Goal: Digitize the follow-up service of patients after cardiothoracic surgery.
Deployment Site: Hospital de Santa Marta, Lisbon, Portugal.
Population: Cardiothoracic surgery patients.
Previous intervention: The standard follow-up version of this service consisted of phone calls to the patient at three days, one month, three months, six months, and 12 months after the hospital discharge.
New intervention: The responsible surgical team proposed the integration of IoT devices to monitor patients remotely in the comfort of their homes during the first month after surgery to detect problems and avoid acute problems early.
RPM Period: 30 days.
RPM Outcomes Measurements: 11 in total: blood pressure and heart rate, weight, number of steps, the occurrence of blackouts, perceived alterations in surgical wound healing, picture of the surgical wound, presence of palpitations, presence of edemas, presence of dyspnea, chest pain intensity level.
Responsible Team:
Nurses: total 3 (3 female, average age of years old);Physicians: total 3 (2 male, average age of years old);Developers: total 4 (1 female and 3 male, average age of years old);Researchers: total 5 (4 female and 1 male, average age of years old) with expertise in digital health services design, digital health literacy, and cost analysis.
Pilot activities: The surgical team agreed with the existing version of the IoT kit, which includes a weight scale, blood pressure monitor, smart wristband, and an Android smartphone. A mobile application allowed patients to report outcomes through four (Yes/No) questions survey and two 4-point Likert scale questions, and a smartphone camera, and collect automatically clinical parameters from the IoT devices.
Pilot duration: The mobile application and the IoT devices’ main development was conducted in the context of heart failure and served as a basis for a customized version for this pilot. The team worked together to create an RPM platform that could ensure interoperability with the existing mobile application and IoT devices.
Pilot Duration: February 2019 to January 2021 (22 months).
End-users involved:
Patients: total 35 (18 male and 17 female, average age of years old);Nurses: total 24 (2 male and 22 female);Physicians: total 3 (3 male).
End-users feedback data collection methods: On the last day of the follow-up period, the patient replied to a service satisfaction survey and provided feedback on the overall experience through a video-recorded semi-structured interview.
The pilot initiative 1 characterization resulted in nine features (Table 3) which are: (1) outcome collection using a mobile app connected to IoT devices; (2) outcome collection using smartphone camera; (3) RPM-based therapy management; (4) web-based RPM care management platform; (5) outcome-based automated alerts; (6) RPM dynamic table; (7) RPM activities management and resource allocation monitoring; (8) an integrated ticket reporting system; and (9) periodic data fetching. The PAR team evaluated the first eight providing the most value for the end-users (patients, nurses, and physicians) since the patient, nurse, and physician feedback was very positive. Finally, the ninth feature was excluded because there was a need to have data available more frequently. The features of outcome collection using a smartphone camera, web-based RPM care management platform, and RPM activities management and resource allocation monitoring were evaluated has requiring major changes and, consequently, high effort, because of the integration of AI-based tools for optimal follow-up resources prediction based on patient risk stratification.
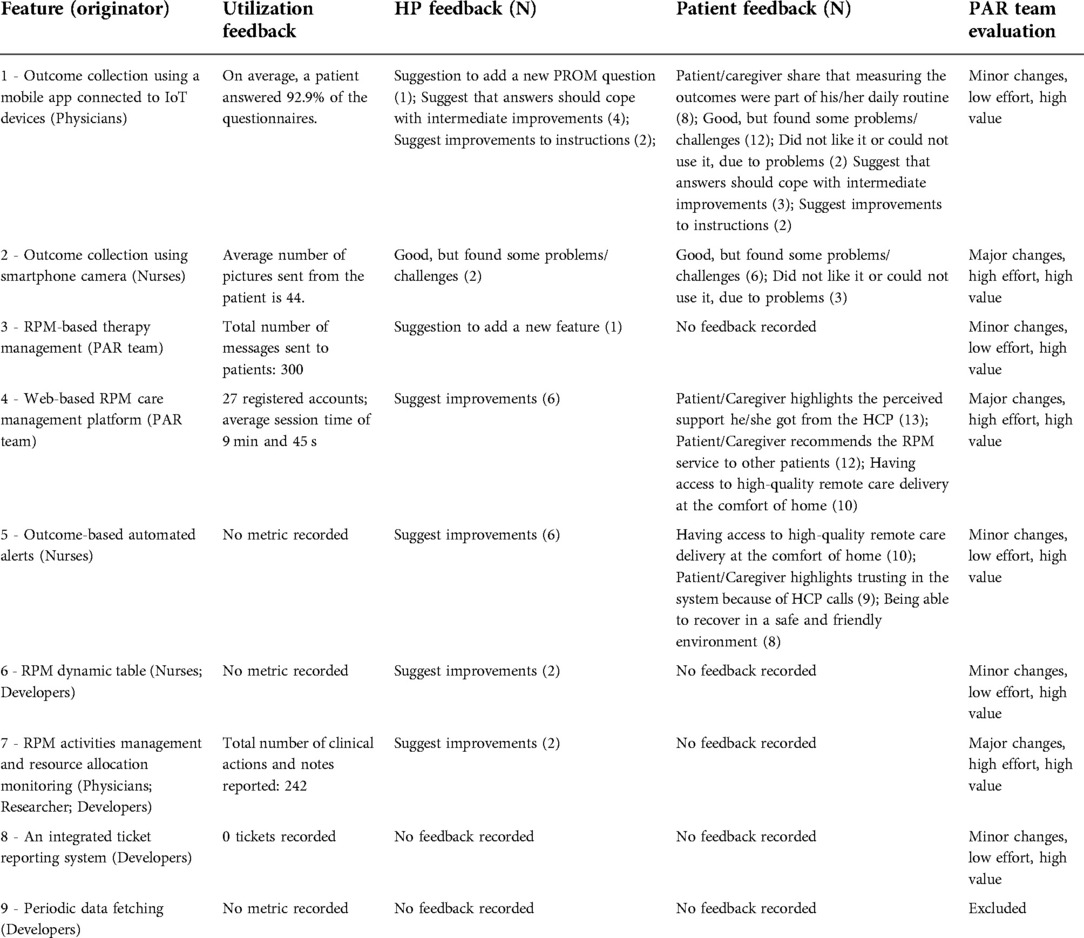
Table 3. List of features of pilot initiative 1.
The second pilot initiative refers to another RPM follow-up pilot service in the same hospital and surgical department as the funded project (Box 2). This case was selected because part of the population submitted to cardiothoracic surgery might require oral anticoagulation therapy in the long term. Therefore, understanding the technological features to provide continuous care to these patients is relevant.
Box 2. Pilot Initiative 2: HemoControlBot: Oral anticoagulation therapy management (37)
Motivation: A private medical device company needed to demonstrate the added value of the coagulometer when integrated into an RPM service.
Goal: Digitize the oral anticoagulation therapy management after cardiac surgery.
Deployment Site: Hospital de Santa Marta, Lisbon, Portugal.
Population: Patients under oral anticoagulation therapy after cardiac surgery.
Previous Intervention: The standard oral anticoagulation therapy involves frequent patient visits to the hospital to measure the International Normalized Ratio (INR) value to assess the blood’s ability to clot. Based on this and other relevant outcomes, the physician adjusts medication to avoid the risk of bleeding.
New Intervention: The responsible surgical team and a private medical device company proposed the combination of a coagulometer and a mobile text message-based RPM system to allow patients to report remotely therapy-relevant outcomes.
RPM Period: 180 days.
RPM Outcomes Measurement: 7 in total: INR, the dosage of antibiotic and anti-inflammatory drugs, the occurrence of bruises, hemorrhages, feces, nausea, and the number of trips to the hospital or health center.
Responsible Team:
Nurses: total 3 (3 female, average age of years old);Physicians: total 2 (2 male, average age of years old);Developers: total 2 (2 male, average age of years old);Researchers: total 5 (2 male, average age of years old) with expertise in digital health services design and cost analysis.
The technology used: The surgical team demanded that the RPM system should not be dependent on the type of mobile phone to increase accessibility. Therefore, patients reported the outcomes by answering seven 4-point Likert scale questions via the lowest cost communication channel, i.e., short message service (SMS).
Pilot Activities: The team worked together to create an SMS-based RPM platform that automatically generates SMSs asking the patient to report the required outcomes.
Pilot Duration: December 2019 to June 2022 (7 months).
End-users involved:
Patients: total 19 (9 male and 10 female, average age of years old);Physicians: total 2 (2 male).
End-users feedback data collection methods: On the last day of the follow-up period, the researcher conducted a phone call-based semi-structured interview to collect the patient’s feedback, considering the interaction with technology and the overall experience.
The pilot initiative 2 characterization resulted in four features (Table 4), which are: (1) outcome collection using a mobile-based chatbot; (2) RPM-based therapy management using chatbot; (3) surgical team alert email notification; and (4) instant data availability. The PAR team evaluated the second and fourth features providing the most value for the end-users (physicians) since the physician feedback was very positive. The first feature was assessed as low value as the IoT devices were already selected as the channel to collect the outcomes. In addition, the third feature was also evaluated as low value since physicians and nurses had to assess the patient’s RPM data daily.

Table 4. List of features of pilot initiative 2.
The third pilot initiative refers to an RPM follow-up pilot service conducted by one of the partners of the PAR team in the scope of the COVID-19 pandemic (Box 3). The main similarity between the pilot initiative and the funded project was the isolation context of the target population during follow-up. The second similarity consists of adapting existing technology to the needs of an elderly population, maximizing user interaction and experience.
Box 3. Pilot Initiative 3: NursingHomeRPM: Remote care delivery in nursing homes (38)
Motivation: Portugal 2020 funded research and development projects for testing and optimization of technological infrastructures in the context of COVID-19.
Goal: Digitize the care provided in a nursing home during the COVID-19 pandemic with each partner’s existing technology.
Deployment Site: Private nursing home, Cascais, Portugal.
Population: Nursing home residents.
Previous Intervention: The standard care provided in the nursing home required formal caregivers to register physical needs, including personal hygiene or grooming, dressing, toileting, transferring or ambulating, and eating in a notebook.
New Intervention: The digital transformation consisted of developing and implementing a mobile application that could connect with IoT devices to monitor its residents.
RPM Period: 30 days.
RPM Outcomes Measurements: seven in total - blood pressure, temperature, blood oxygen levels, blood glucose levels, daily mood tracker, ability to conduct activities of daily living, and quality of life.
Responsible Team:
Nursing Home Professionals: total 1 (1 male, age of 45 years old);Physicians: total 1 (1 female, age of 45 years old);Developers: total 8 (3 female and 5 male, average age of years old);Researchers: total 3 (2 female and 1 male, average age of years old) with expertise in digital health services design, digital and cost analysis;User Interaction/User Experience (UX/UI) designer: total 1 (1 female, age of 30 years old).
The technology used: The developers proposed an existing IoT kit to be used in the nursing home to collect outcomes, which includes an oximeter, blood pressure monitor, thermometer, glucometer, and an Android tablet. A mobile application allowed nursing home staff to report outcomes through several (Yes/No) questions survey and 4-point Likert scale questions, automatically collecting clinical parameters from the IoT devices.
Pilot Activities: The team worked together to create an RPM platform with multiple user roles (manager, physician, nurse, informal caregiver, and patient) to collect patient outcomes.
Pilot Duration: June to November 2020 (5 months).
End-users involved:
Patients: total 10 (5 male and 5 female with an average age of years old);Physician: total 1 (1 female);Nurses: total 1 (1 male);Nursing Home: 1 director (male), 6 staff (6 female).
End-users feedback data collection methods: User experience and interaction testing sessions were conducted with the nursing home director, one staff member, and one nursing home resident.
The pilot initiative 3 characterization resulted in four features (Table 5), which are: (1) outcome collection using a mobile app connected to IoT devices; (2) RPM-based therapy management; (3) interoperability using FHIR; and (4) role definition. The PAR team evaluated the first three providing the most value for end-users (Nursing Home director and physicians) since the director and physician considered as a must-have requirement. Although the fourth feature was considered to provide moderate value, the PAR team considered that it required significant changes and high effort to develop.

Table 5. List of features of pilot initiative 3.
This phase involved five meetings with an average participation of eight PAR team members and an average of 42 min (3 h and 30 min in total).
An overview of Figure 2 reveals that the participation level according to each group was Developers (33.1%), Researchers (31.5%), Physicians (17.1%), Nurses (15.0%), and Patients (3.2%). The Researchers played the leading role in the Problem Definition and Planning phases (73.9% and 58.3%, respectively). In the Action and Observation phases, the Researchers group was the most participating group (34.3% and 53.9%, respectively). Finally, in the Reflection phase, the most participating role was the Nurses (34.2%). A more detailed analysis of each pilot initiative informs that the Researchers participated more in the first pilot initiative (39.7%), Developers and Physicians share the first position in the second pilot initiative (29.4%), and the Developers in the third pilot initiative (45.8%). In contrast, the patients were only present, with minor participation, in the first and third pilot initiatives (5.5% and 4.5%, respectively). In the first pilot initiative, the Reflection phase was the phase with the highest participation roles diversity, and the Planning phase was the lowest. In the second pilot initiative, the Problem Definition, Action, and Observation were the phases with the highest participation roles diversity. Finally, the third pilot initiative had no participation in Planning and Observation phases and the highest participation role diversity in the Action phase.
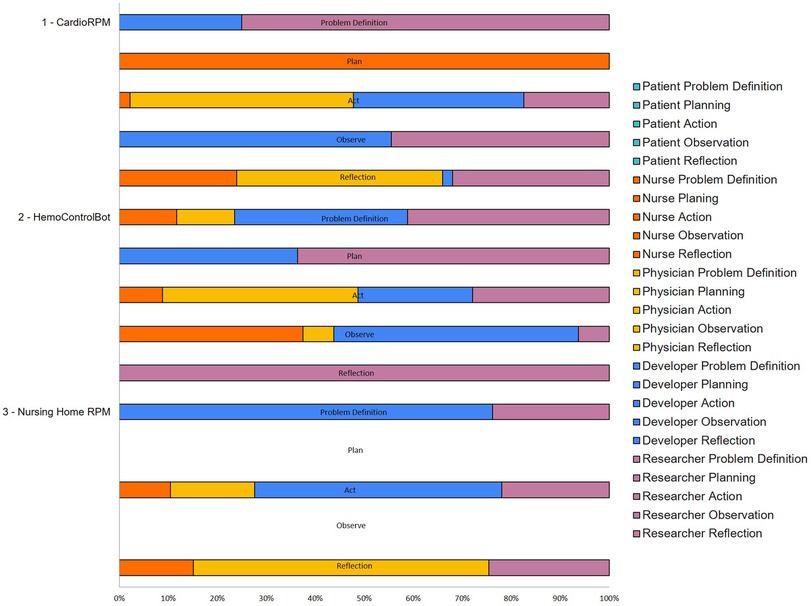
Figure 2. Level of participation of each team role per PAR phase per pilot initiative.
From the three pilot initiatives the PAR team extracted 15 features and classified 11 as must-haves. Figure 3 illustrates the feature prioritization for development. All the features classified with high value for the end-users were prioritized as Must-Have on the enhanced version of the RPM-platform. The feature of Role definition was prioritized as Should-Have because although it was evaluated as a moderate-value feature, it implied significant changes and, consequently, high effort to implement. In contrast, the email notification feature was prioritized as Could-Have because although it imposes lower changes and minor effort, it was evaluated to bring low value to the end users.
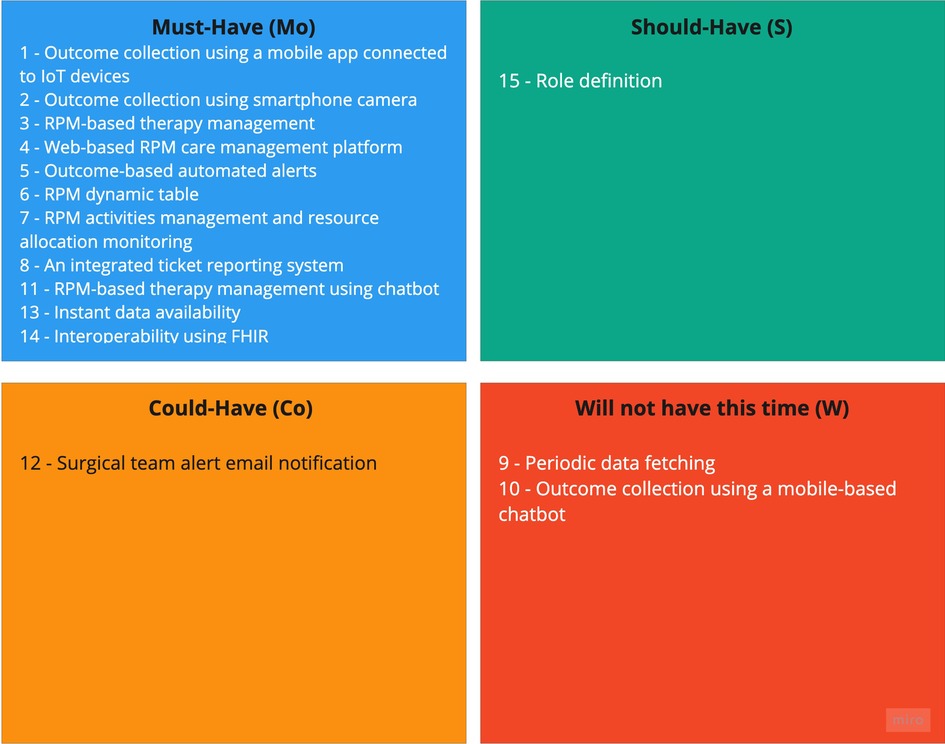
Figure 3. Diagram of the features of the three previously developed pilot initiatives. Each category is represented with a letter and a color: must-have - Mo (blue), should-have - S (green), could-have Co (yellow), and will not have this time - W (red).
The top three topics most covered across the phases were Design (39.7%), Development (22.2%), and Execution and Implementation (18.5%). The top three meeting focus were Data Analysis Framework Requirements (23.4%), Study Protocol Writing (16.6%), Modelling and Simulation (15.6%). The top three meeting outcomes contributions were: Improved research and development system (35.0%), Better characterization and understanding of the complex socio-technical-economic constraints to sustainable software development production and care service provision (25.2%), and Better understanding, on the part of researchers, of systems used by healthcare professionals and patients (22.0%). The participation level according to each role in the meetings was: Researchers (52.9%), Developers (47.5%), Physicians (46.7%), and Nurses (5.8%). The top three contributions of the participants involve suggesting or planning actions (42.2%), sharing or generating knowledge (22.4%), and discussing the solution (13.5%). Figure 4 exposes the most frequent type of contribution by each PAR team role. Physicians, Researchers, and Developers suggest and plan more actions (44.2%, 39.1%, and 47.8%, respectively), while Nurses are more dedicated to share and generate knowledge (71.4%). The participation level according to of each role in the meetings was: Researchers (52.9%), Developers (47.5%), Physicians (46.7%), and Nurses (5.8%). The approach involved two action-reflection cycles illustrated in Figure 5. In this figure, it is also illustrated the distribution of the meetings per phase to define the final list of features and prioritize the development. Most of the meetings were dedicated to the Action phase (9 meetings), followed by the Reflection Phase (5 meetings), Observation (2 meetings), and Problem Definition (1 meeting) and Planning (1 meeting).
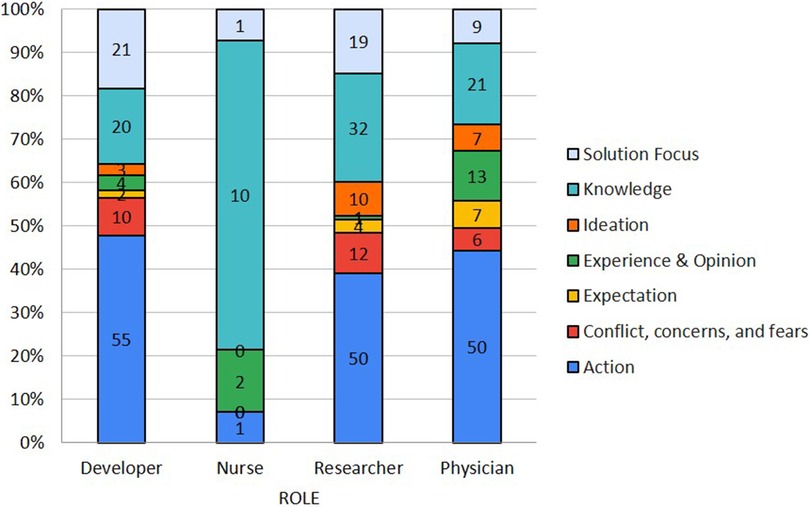
Figure 4. Different contributions according to PAR team role.
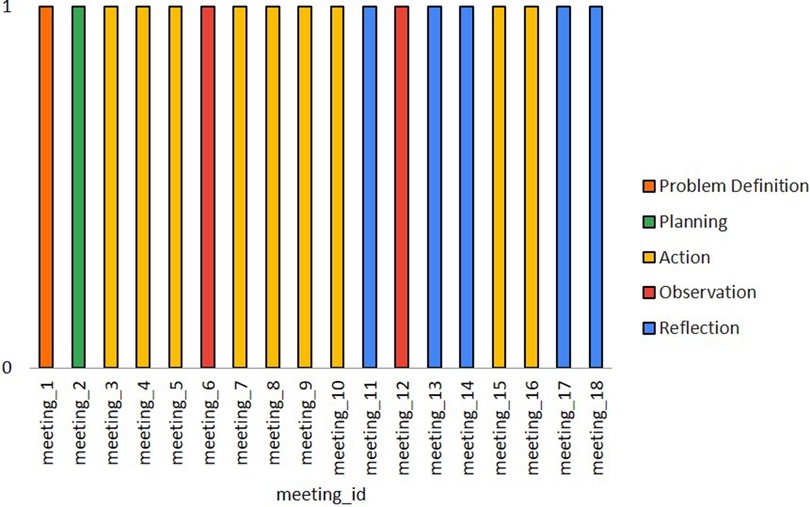
Figure 5. Distribution of meetings per phase.
The proposed RPM-based platform (Supplementary Material 5) is the result of a PAR approach and comprises features suggested, tested, and evaluated by different relevant stakeholders, from end-users, such as patients and healthcare professionals, to software developers and researchers. These features make the platform more robust and ready to integrate value assessment and AI-based decision support tools to increase access to RPM surgical follow-up care in pandemic contexts.
The PAR project was initiated by a consortium of partners, funded by a Portuguese national research agency, that aimed to ensure that the following cycle of technological development would allow the provision of care to a larger and diversified sample of patients in a public hospital. Therefore, patients and healthcare professionals had to be part of the research process so that their needs were not compromised at the expense of scalability (39). Problem definition and context characterization are two important domains usually neglected by researchers in scalability assessment (40). The most important features for the patients were the outcomes collection using a mobile application, smartphone camera, and IoT devices, outcome-based automated alerts, and the web-based RPM care management platform. Patients refer to these features by highlighting how they changed their daily routines to provide information to physicians and nurses and how the latter called them every time the outcome values were not the ones expected. In addition to the patient-preferred features, physicians also showed a preference for the feature of RPM dynamic table and RPM-based therapy management using a chatbot. This is explained by the healthcare professionals’ need to act quickly on generated alerts, automatize some of their actions, and provide personalized care accordingly. In contrast, developers and researchers showed a preference for backend features. On the one hand, developers suggested features related to interoperability using standard data formats and instant data availability. On the other hand, researchers suggested features that would support their research, such as concerning the feature of RPM activities management and resource allocation monitoring (41).
The PAR approach allowed the aggregation of different stakeholders’ opinions of the problem, guaranteeing their engagement throughout the project and the general interest of the research. As discussed by experts in digital health the interdisciplinary co-creation is an enabler for scaling up digital solutions (41). The flexibility inherent to this approach enabled collaboration among partners to select the final set of features by sharing previously conducted work, experience, and acquired knowledge. Therefore, the proposed RPM solution may have a high agreement with the users’ needs avoiding wasting time and resources, which is particularly relevant in healthcare providing services (42). This RPM platform helps to give more personalized care: the platform provides useful patient information to be used by the clinical team to make patient-centered medical decisions from the collected data. In addition, the high reported levels of adherence concerning some features may indicate that the patients are prone to use these RPM systems to interact and to be followed up by clinical teams. Some patient testimonials revealed they felt they were being followed up closely, conveying a greater sense of (2).
The proposed platform data infrastructure allows data collection considering the patient pathway. Contrary to most hospitals’ information systems (43), this platform collects data associated with the different activities of the patient journey during the intervention. For each activity in the patient pathway, the allocated resources type, quantity, and time are recorded. This information is integrated with the outcomes’ stability analysis allowing the intervention’s value assessment.
The dynamic and iterative nature of the research process allowed the different stakeholders to cover distinct topics from design to execution and implementation and focus, such as data analysis framework requirements and modeling and simulation simultaneously, rather than sequentially, as in other research approaches. This work also emphasized how the information flows and is exchanged among physicians, nurses, researchers, and developers, revealing that all should be in the different phases of software development cycles.
This work has some limitations considering the implementation of the PAR approach since the patients were only part of the research process indirectly through feedback evaluation in two of the three case studies. This limitation was caused by the COVID-19 context that excluded the option of group meetings with the patients. Another limitation was the lack of observations considering the topics that generated more or less agreement during meetings. This would allow a better analysis of leadership dominant and oppressive roles in the PAR team (41). The PAR approach encourages the researchers to focus on the practitioners’ problems and work collaboratively on solutions to those problems (15); therefore, another limitation might be related to the generalizability of the RPM platform to other contexts. Two significant limitations of the proposed RPM-based platform are, first, the lack of integration with the hospital’s information system. Second, the limited sample of patients that tested each feature. However, the PAR team is already running a clinical study with 150 patients.
Future work should focus on the evaluation of the implemented value assessment and AI-based decision-support tools’ impact on the clinical practice to increase access to high-quality RPM-based surgical follow-up services. outcomes’ stability analysis allowing the intervention’s value assessment.
RPM-based follow-up services were highly adopted during the pandemic, driving healthcare organizations to scale-up ongoing pilot initiatives. The scalability of RPM services must consider contextual factors, such as individuals’ and organizations’ interests and needs, that influence its uptake into routine use. The PAR approach allowed to simultaneously design, develop, test, and evaluate the RPM platform features with the contribution of patients, healthcare professionals, developers, and researchers. Participatory research is needed to scale up RPM technologies into widespread clinical routine usage.
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request. Requests to access the datasets should be directed to ana.londral@vohcolab.org.
The studies involving human participants were reviewed and approved by Ethical Committee of Centro Hospitalar Lisboa Central and given the study registration number: CA2651 and 1057-2021. Ethics Research Committee of Nova Medical School—FCM-UNL (CEFCM) and given the study registration number: 77/2021/CEFCM. The patients/participants provided their written informed consent to participate in this study.
SA, FG, PD, AL, IL, JS, PC, and JF contributed to the conception and design of the study. PD and NC organized the database and designed the data collection tools. JS, PC, CV, HS, and AG collected the data. SA and FG wrote the first draft of the manuscript. PD, FV, and IL wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
This research has been supported by Fundação para a Ciência e Tecnologia (FCT) under CardioFollow.AI project (DSAIPA/AI/0094/2020) and Lisboa-05-3559-FSE-000003.
We want to acknowledge Roche Diagnostics, Vodafone Portugal, Future Healthcare, Plux Wireless Biosignals, and HealthySystems for providing technological support for conducting this research work. The authors want to thank the staff members of Residência Geriátrica Alapraia for their part in enrolment and data collection. We also extend our gratitude to all our participants who took part in these studies.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdgth.2022.1006447/full#supplementary-material.
1. Vegesna A, Tran M, Angelaccio M, Arcona S. Remote patient monitoring via non-invasive digital technologies: a systematic review. Telemed E Health. (2017) 23:3–17. doi: 10.1089/tmj.2016.0051
2. Ferrua M, Minvielle E, Fourcade A, Lalloué B, Sicotte C, Di Palma M, et al. How to design a remote patient monitoring system? A French case study. BMC Health Serv Res. (2020) 20:434. doi: 10.1186/s12913-020-05293-4
3. Pare G, Jaana M, Sicotte C. Systematic review of home telemonitoring for chronic diseases: the evidence base. J Am Med Inform Assoc. (2007) 14:269–77. doi: 10.1197/jamia.M2270
4. Baginski BN, Byrne KA, Vaz DG, Barber R, Blackhurst D, Tibbett TP, et al. Development, implementation of a remote patient monitoring program for heart failure: a single-centre experience. ESC Heart Failure. (2021) 8:1349–58. doi: 10.1002/ehf2.13214
5. Pekmezaris R, Mitzner I, Pecinka KR, Nouryan CN, Lesser ML, Siegel M, et al. The impact of remote patient monitoring (telehealth) upon medicare beneficiaries with heart failure. Telemed E Health. (2012) 18:101–8. doi: 10.1089/tmj.2011.0095
6. Park DK, Jung EY, Park RW, Lee YH, Hwang HJ, Son IA, et al. Telecare system for cardiac surgery patients: implementation, effectiveness. Healthc Inform Res. (2011) 17:93. doi: 10.4258/hir.2011.17.2.93
7. Farias FACd, Dagostini CM, Bicca YdA, Falavigna VF, Falavigna A. Remote patient monitoring: a systematic review. Telemed E Health. (2020) 26:576–83. doi: 10.1089/tmj.2019.0066
8. Werger AC, Breel J, van Kuijk S, Bulte CSE, Koopman S, Scheffer GJ, et al. Outcome in patients undergoing postponed elective surgery during the COVID-19 pandemic (TRACE II): study protocol for a multicentre prospective observational study. BMJ Open. (2022) 12:e060354. doi: 10.1136/bmjopen-2021-060354
9. Mehrotra A, Ray K, Brockmeyer DM, Barnett ML, Bender JA. Rapidly converting to “virtual practices”: outpatient care in the era of Covid-19. NEJM Catalyst Innov Care Deliv. (2020) 1. doi: 10.1056/CAT.20.0091
10. Doraiswamy S, Abraham A, Mamtani R, Cheema S. Use of telehealth during the COVID-19 pandemic: scoping review. J Med Internet Res. (2020) 22:e24087. doi: 10.2196/24087
11. Gordon WJ, Henderson D, DeSharone A, Fisher HN, Judge J, Levine DM, et al. Remote patient monitoring program for hospital discharged COVID-19 patients. Appl Clin Inform. (2020) 11:792–801. doi: 10.1055/s-0040-1721039
12. Annis T, Pleasants S, Hultman G, Lindemann E, Thompson JA, Billecke S, et al. Rapid implementation of a COVID-19 remote patient monitoring program. J Am Med Inform Assoc. (2020) 27:1326–30. doi: 10.1093/jamia/ocaa097
13. Keahey J. Sustainable development, participatory action research: a systematic review. Syst Pract Action Res. (2021) 34:291–306. doi: 10.1007/s11213-020-09535-8
16. Fundação para a Ciência e Tecnologia. FCT projects. Website (2022). Available from: https://www.fct.pt/apoios/projectos/concursos/datascience/index.phtml.en (Accessed October 18, 2022).
17. Sumberg J, Okali C. Farmers, on-farm research and the development of new technology. Exp Agric. (1988) 24:333–42. doi: 10.1017/s0014479700016185
19. Aberdeen T, Yin RK. (2009). Case study research: design and methods (4th ed.). Thousand Oaks, CA: Sage. Can J Action Res. (2013) 14:69–71. doi: 10.33524/cjar.v14i1.73
20. Hancock D, Algozzine B, Lim JH. Doing case study research: a practical guide for beginning researchers. 4th ed. New York, USA: Teachers College Press (2021).
21. Bentley M, Minstrell M, Bucher H, Morrissey M, Robinson A, Stirling C. A case study evaluation protocol to assess processes, effectiveness, impact of a nurse practitioner-led memory clinic. Health. (2014) 6:748–56. doi: 10.4236/health.2014.68096
22. Wong G, Greenhalgh T, Westhorp G, Pawson R. Realist methods in medical education research: what are they, what can they contribute? Med Educ. (2011) 46:89–96. doi: 10.1111/j.1365-2923.2011.04045.x
23. Centro Hospitalar Lisboa Central. Hospital de Santa Marta. Website (2022). Available from: https://www.chlc.min-saude.pt/hospital-santa-marta/ (Accessed October 18, 2022).
24. Fraunhofer. Fraunhofer Portugal. Website (2022). Available from: https://www.fraunhofer.pt/en/about.html (Accessed October 18, 2022).
25. NOVA Medical School. NOVA Medical School. Website (2022). Available from: https://www.nms.unl.pt/pt-pt/nms (Accessed October 18, 2022).
26. Value for Health CoLAB. Value for Health CoLAB. Website (2022). Available from: https://vohcolab.org/about-us/ (Accessed October 18, 2022).
27. Johannesson P, Perjons E. A method framework for design science research. An Introduction to Design Science. New York, USA: Springer International Publishing (2021). p. 77–93. Available from: http://doi.org/10.1007/978-3-030-78132-3˙4.
28. Krippendorff K. Content analysis: an introduction to its methodology. 3rd ed. Los Angeles, London: SAGE (2013).
29. Mind Tools. Cause and effect analysis: Identifying the likely causes of problems. Website (2022). Available from: http://www.mindtools.com/pages/article/newTMC˙03.htm (Accessed October 18, 2022).
30. Douglas FC, Gray DA, van Teijlingen ER. Using a realist approach to evaluate smoking cessation interventions targeting pregnant women and young people. BMC Health Serv Res. (2010) 10:49–55. doi: 10.1186/1472-6963-10-49
31. Granström E, Wannheden C, Brommels M, Hvitfeldt H, Nyström ME. Digital tools as promoters for person-centered care practices in chronic care? Healthcare professionals’ experiences from rheumatology care. BMC Health Serv Res. (2020) 20:1108–22. doi: 10.1186/s12913-020-05945-5
32. van Tol LS, Smaling HJA, Groothuijse JM, Doornebosch AJ, Janus SIM, Zuidema SU, et al. COVID-19 management in nursing homes by outbreak teams (MINUTES)—study description and data characteristics: a qualitative study. BMJ Open. (2021) 11:e053235. doi: 10.1136/bmjopen-2021-053235
33. Glaser BG, Strauss AL. The discovery of grounded theory: strategies for qualitative research. 5. paperback print ed. New Brunswick: Aldine Transaction (2010).
34. Clegg D, Barker R. CASE method fast-track: a RAD approach. Wokingham, England; Reading, Mass.: Berkshire, UK; Redwood Shores, CA, USA: Addison-Wesley Pub. Co.; Oracle (1994).
35. Miranda E. Moscow rules: A quantitative exposé. Lecture Notes in Business Information Processing. Springer International Publishing (2022). p. 19–34. Available from: http://doi.org/10.1007/978-3-031-08169-9˙2.
36. Londral A, Azevedo S, Dias P, Ramos C, Santos J, Martins F, et al. Developing and validating high-value patient digital follow-up services: a pilot study in cardiac surgery. BMC Health Serv Res. (2022) 22:680. doi: 10.1186/s12913-022-08073-4
37. Dias P, Cardoso M, Guede-Fernandez F, Martins A, Londral A. Remote patient monitoring systems based on conversational agents for health data collection. Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies. Vienna, Austria: SCITEPRESS - Science and Technology Publications (2022). p. 812–820. Available from: http://doi.org/10.5220/0011011000003123.
38. EasyHealth 4 Covid. EasyHealth 4 Covid. Website (2021). Available from: https://easyhealth4covid.vohcolab.org/ (Accessed October 18, 2022).
39. Kvedar JC, Fogel AL. Why real-world results are so challenging for digital health. NEJM Catalyst. (2017) 3(4). doi: 10.1056/CAT.17.0453
40. Azevedo S, Rodrigues TC, Londral AR. Domains and methods used to assess home telemonitoring scalability: systematic review. JMIR Mhealth Uhealth. (2021) 9:e29381. doi: 10.2196/29381
41. Schlieter H, Marsch LA, Whitehouse D, Otto L, Londral AR, Teepe GW, et al. Scale-up of digital innovations in health care: expert commentary on enablers and barriers. J Med Internet Res. (2022) 24:e24582. doi: 10.2196/24582
42. Ch A, Barros P, Barry M, et al. Defining value in value-based healthcare: report of the expert panel on effective ways of investing in health (EXPH). Luxembourg: Publications Office of the European Union (2019).
Keywords: collaboration, follow-up care, implementation, participatory action research, remote patient monitoring
Citation: Azevedo S, Guede-Fernández F, von Hafe F, Dias P, Lopes I, Cardoso N, Coelho P, Santos J, Fragata J, Vital C, Semedo H, Gualdino A and Londral A (2022) Scaling-up digital follow-up care services: collaborative development and implementation of Remote Patient Monitoring pilot initiatives to increase access to follow-up care. Front. Digit. Health 4:1006447. doi: 10.3389/fdgth.2022.1006447
Received: 29 July 2022; Accepted: 16 November 2022;
Published: 7 December 2022.
Edited by:
Lisa Marsch, Dartmouth College, United StatesReviewed by:
Emily Hickmann, Technical University Dresden, Germany,© 2022 Azevedo, Guede-Fernández, von Hafe, Dias, Lopes, Cardoso, Coelho, Santos, Fragata, Vital, Semedo, Gualdino and Londral. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Londral YW5hLmxvbmRyYWxAdm9oY29sYWIub3Jn
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Health Technology Implementation, a section of the journal Frontiers in Digital Health
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.