 Gilly Dosovitsky
Gilly Dosovitsky Erick Kim
Erick Kim Eduardo L. Bunge
Eduardo L. Bunge- Psychology Department, Palo Alto University, Palo Alto, CA, United States
Background: The Patient Health Questionnaire-9 (PHQ-9) is a brief depression measure that has been validated. A chatbot version of the PHQ-9 would allow the assessment of depressive symptoms remotely, at a large scale and low cost.
Objective: The current study aims to: Assess the feasibility of administering the PHQ-9 in a sample of adults and older adults via chatbot, report the psychometric properties of and identify the relationship between demographic variables and PHQ-9 total scores.
Methods: A sample of 3,902 adults and older adults in the US and Canada were recruited through Facebook from August 2019 to February 2020 to complete the PHQ-9 using a chatbot.
Results: A total of 3,895 (99.82%) completed the PHQ-9 successfully. The internal consistency of the PHQ-9 was 0.896 (p < 0.05). A one factor structure was found to have good model fit [X2 (27, N = 1,948) = 365.396, p < 0.001; RMSEA = 0.080 (90% CI: 0.073, 0.088); CFI and TLI were 0.925 and 0.900, respectively, and SRMR was 0.039]. All of the demographic characteristics in this study were found to significantly predict PHQ-9 total score, however; their effect was negligible to weak.
Conclusions: There was a large sample of adults and older adults were open to completing assessments via chatbot including those over 75. The psychometric properties of the chatbot version of the PHQ-9 provide initial support to the utilization of this assessment method.
Introduction
Depressive disorders affect more than 264 million people of all ages globally according to the World Health Organization (WHO) (1). The prevalence rate of depressive disorders for adults and older adults around the world varies from 10 to 20% (2). With the high prevalence rates of depression, developing scalable and low-cost instruments to assess depression in adults and older adults is an essential public health need. Many individuals with depression do not access assessment (or treatment) due to stigma (3), economic barriers (4), or lack of engagement with specialty mental health services and high engagement with primary care where depression is not always screened (5). The Patient Health Questionnaire-9 (PHQ-9) (6) is a brief measure of depression that has been extensively validated (7–10). A chatbot version of the PHQ-9 would allow the assessment of depressive symptoms interactively, remotely, at a large scale, and low cost, however, no studies to date have assessed the validity of a chatbot version of the PHQ-9. Developing large scale and remote means of assessing depression is highly relevant since it would allow individuals to self-assess in an interactive way using just their personal devices. Having means for remote assessment is especially necessary for adults and older adults during the COVID-19 pandemic, since they are at a higher risk of getting infected during in-person visits to health care centers (11). Having the option to complete assessments on personal phones in a more interactive way can complement computer delivered assessments to reach a greater number of people.
The PHQ-9 is a reliable measure of depression with a Chronbach's alpha of 0.89 (6). Exploratory factor analyses of the PHQ-9 have shown evidence for both a one factor and two factor structure. Dum et al. (12) found that the PHQ-9 had a one-factor structure where all items had a factor loading over 0.35 and this factor accounted for 59.97% of the variance. Two other studies found that the PHQ-9 was best explained by one overarching factor; a study with racially and ethnically diverse primary care patients (8), and another study with a general population of adults in Hong Kong (9). Exploratory factor analyses of the PHQ-9 have identified a two-factor model (10). In a study on the PHQ-9 in adults and older adults in Taiwan, a two-factor structure of somatic and non-somatic symptoms was found (13), and Beard et al. (14) also found a two-factor structure, one consisting of affective and cognitive items and another consisting of somatic items.
Several studies have shown that the PHQ-9 can reliably be used in different formats such as computers (7, 15), smartphone apps (16), and tablets (17). Erbe et al. (7) found a strong correlation (0.92) between a computerized version of the PHQ-9 and the paper and pencil version at an inpatient routine mental health clinic in Germany. Fann et al. (15) assessed the feasibility and validity of administering the PHQ-9 to adult oncology and related specialty patients using a touch screen computer (15). Although, Fann et al. (15) found that the PHQ-9 administered through a touch screen computer provided valid data, the sample was relatively affluent and educated, so comfortability with technology may be lower in other samples. BinDhim et al. (16) assessed the PHQ-9 administered using a smartphone app with a sample of 8,241 adults, with a mean age of 29.4 years old, and found a completion rate of 73.9%. While this study shows that a large number of participants were willing to share their personal information through this anonymous smartphone app it is not clear if this is generalizable to older adults. Spangenberg et al. (17) assessed interformat reliability between a tablet and a paper-and-pencil version of the PHQ-9 with a sample of elderly primary care patients and concluded that the tablet version of the PHQ-9 was a valid way to electronically assess depressive symptoms in elderly patients.
Overall, the findings from the digital versions of the PHQ-9 (computer, tablet, and smartphone app) are congruent with the findings of Coons et al. (18) that show that electronic-based patient-reported outcomes adapted from a paper-based format produce equivalent or even more reliable data than paper versions. Additionally, a meta-analysis by Weigold et al. (19) found that participants are significantly more likely to complete and return assessments than in computerized versions. While the mentioned studies provide support for the utilization of digital versions of the PHQ-9, none of these studies focused on chatbots and older adults. Administration via chatbot has two distinct features to an online delivery. The first, is that with a chatbot, administration is interactive and can be triggered by the chatbot whereas online delivery requires the user to initiate the interaction. Second, it may be completed through text messaging, which presents each question one at a time in a more animated format rather than the typical, static questionnaire. These differences may make the chatbot version more convenient than the online version, however there are no studies that currently assess the validity of the PHQ-9 delivered by a chatbot.
In recent years, there has been an increased interest in the integration of chatbots for assessment (20) and treatment of depression (21–23). While Fitzpatrick et al. (22) and Fulmer et al. (23) reported improvements in depressive symptoms using an interactive version of the PHQ-9 through a chatbot, the psychometrics properties have not been reported. To our knowledge, only two studies reported psychometric properties of chatbot assessments. One study on the PHQ-9 delivered in Spanish by a chatbot found that the psychometric properties are comparable to the paper and pencil version (24). Another study of a loneliness scale that found quantitative equivalence between the chatbot and paper and pencil version (20). Overall, no studies to date have focused on the assessment of the PHQ-9, in English, via chatbot, for adults and older adults. Since prevalence of depression in adults and older adults is 10–20% (2), scalable methods of assessing depression for this population are needed. Thus, the current study aims to: (1) Assess the feasibility of administering the PHQ-9 in a sample of adults and older adults via chatbot. (2) Assess the psychometric properties (factor analysis and reliability) of the PHQ-9 when delivered via a chatbot to a general sample of adults and older adults. (3) Identify the relationship between demographic variables, including sex, age, ethnicity, living status, education level, and employment status, and PHQ-9 total scores.
Method
Participants
The participants of this study were 3,895 adults and older adults (over 65 years of age) in the US and Canada who were recruited through Facebook from August 2019 to February 2020, for a study on the efficacy of a chatbot for social isolation in adults and older adults reported elsewhere.
Materials
The materials for this study was the chatbot (Tess) version of the PHQ-9. Tess is a mental health chatbot that uses an AI-based computer program to engage with users to teach coping skills and provide support. Users can chat with Tess through text message conversations or Facebook Messenger. Other studies provide more information on how Tess works (21).
The PHQ-9 includes questions on the nine criteria of major depressive disorder. Scores on the PHQ-9 range from 0 to 27, each of the items scored from a 0 to 3 where 0 represents the symptom is not present at all and a 3 represents the symptom is present nearly every day. PHQ-9 scores can be categorized into the five severity levels of the PHQ-9 where a total score of <5 is “minimal,” a score of 5–9 is “mild,” a score of 10–14 is “moderate,” a score of 15–19 is “moderately severe,” and a score of 20–27 is “severe” (6). The chatbot version of the PHQ-9 would initially provide two messages to prepare participants to take the screener: “Please answer the questions as they apply to your experience over the past 2 weeks. You can respond with 0, 1, 2, or 3,” and “0 Means not at all affected, 1 means affected for several days, 2 means affected for more than half the days, and 3 means affected nearly every day. Make sense?” If users did not respond affirmatively to instructions, they were delivered in a different way until the user said they understood. Users were then asked each question on the PHQ-9 in the following format: “Over the last 2 weeks, how often have you been bothered by the problem of feeling little interest or pleasure in doing things? 0 = not at all, 1 = several days, 2 = more than half days, 3 = nearly everyday.” Users were reminded of the meaning of each number of the scale in every other question. To each question users were expected to respond with a number 0 to 3.
Procedures
Recruitment efforts for this study primarily focused on Facebook advertisements. Facebook ads used text focusing on depression, loneliness, and social isolation to ensure those who clicked on the advertisement would find the content relevant to their needs. Some participants may have also been referred to the study from participants already enrolled. Users expressed their interests by initiating the conversation with the chatbot via Facebook Messenger as they were prompted to do in the advertisements.
After users expressed an interest in the chatbot, they were sent an introductory message through Facebook Messenger which explained what a chatbot is and included a link to the chatbot's privacy policy and a consent form. To access these forms, users needed to click on the links which directed users out of Facebook messenger. If participants agreed, they were directed back to the Facebook Messenger conversation to begin the assessment process. Following these messages, users received information on what they should do if they are experiencing a crisis while using the chatbot (Tess). Participants were then asked a series of demographic questions and completed the following assessments: Duke Social Support Index, Friendship Scale, Loneliness Scale, Confidence Scale, and the PHQ-9. For this study, only the participant's responses to the PHQ-9 are evaluated. Next, participants were allowed to chat with Tess for ~6 months. After completing an intervention, participants were asked about the usefulness of the chatbot Tess and were given the opportunity to complete the PHQ-9 again. This study was determined to be non-human subjects by the Institutional Review Board at Palo Alto University (Assurance Number: FWA00010885).
Analysis
Frequency distributions for demographic characteristics and completion rates for PHQ-9 scores were conducted using R (20). The internal consistency of the PHQ-9 was assessed using Cronbach's alpha and inter-item correlations using Spearman's rank correlation coefficients. Both Bartlett's test of sphericity and Kaiser-Meyer-Olkin measure of sampling adequacy were used to determine suitability of factor analysis.
The factor structure of the PHQ-9 was examined by conducting a split-half exploratory factor analysis and confirmatory factor analysis using MPlus Version 8.3 (21). An exploratory factor analysis using maximum likelihood estimation with geomin oblique rotation was conducted. Scree plots, eigenvalues (≥1), factor loadings (>0.4), and model fit of one and two factor structures were found. Then, a confirmatory factor analysis was conducted to evaluate model fit. To determine model fit, chi-squared model fit statistics (X2), comparative fit index (CFI), Tucker-Lewis index (TLI), the room mean square error of approximation (RMSEA) with 90% confidence intervals, and standardized root mean square residual (SRMR) were found. Kline (25) and Hooper et al. (26) criteria for goodness of fit were used. The following criteria were used to determine goodness of fit: (1) CFI ≥0.9; (2) TLI ≥0.95; (3) RMSEA <0.08; (4) SRMR <0.08; (5) goodness of fit p > 0.05.
Results
Demographics
There were 3,902 participants who provided consent. Seven participants' presented errors in completion of the PHQ-9 (participants submitted a response that was out of range) and their scores were excluded from the analyses. For the 3,895 participants who completed correctly, the PHQ-9 demographic characteristics are in Table 1. The majority of participants identified as female (N = 3,575, 91.79% of sample). The largest age group was participants who reported being 55–60 years old (N = 1,489, 38.22%). Most participants identified as White (N = 2,336, 59.97%), and were not living alone (N = 2,675, 68.68%). The largest number of participants reported that the highest level of education achieved was high school diploma or equivalent (N = 1,648, 42.31%). Regarding employment status, most participants reported being unable to work (N = 1,587, 40.74%). The average total PHQ-9 score was 17.60 with a standard deviation of 6.90 points.
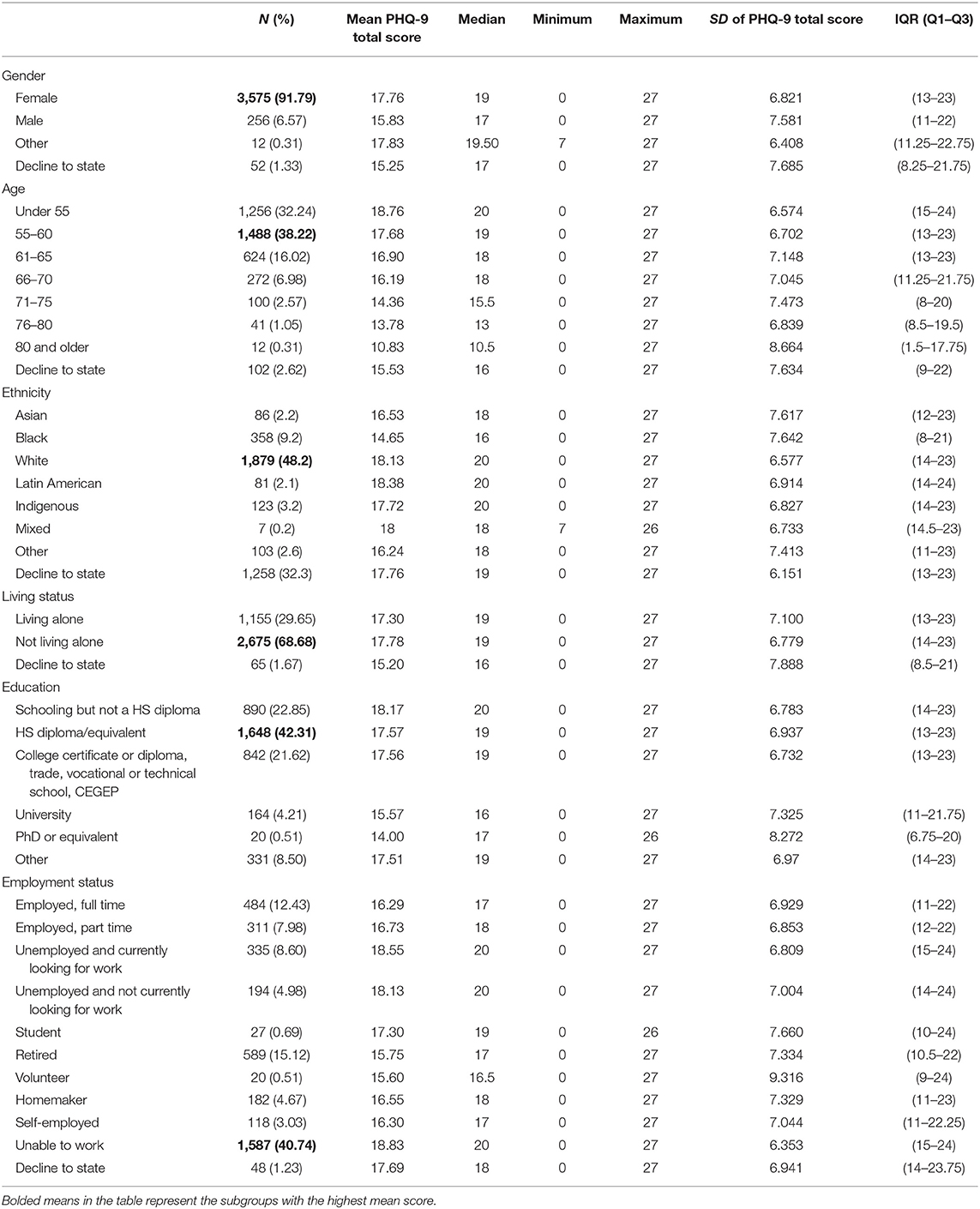
Table 1. Demographic characteristics (total N = 3,895).
Feasibility and Completion
Out of the 3,902 participants, 3,895 (99.82%) completed the PHQ-9 successfully. The seven participants that did not complete the PHQ-9 correctly identified as female. One of these participants was under 55 years old, two were between the ages of 55 and 60, two were between the ages of 66 and 70, and one was between 71 and 75. Four of the participants identified as White, one identified as Latin American, one reported they did not know, and one declined to state.
Psychometric Properties
The internal consistency of the PHQ-9 was found using Chronbach's alpha. Based on the 3,895 participants who responded to the 9 questions of the PHQ-9, Chronbach's alpha was 0.896 (p < 0.05). The inter-item correlations ranged from 0.25 to 0.59 using Spearman's rank correlation to account for non-normality of the PHQ-9. Bartlet's test of sphericity was run to determine that items are suitable for factor analysis (p < 0.05). Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.904 indicating good sampling adequacy.
Reliability
Internal reliability calculated by Chronbach's alpha. Based on the 3,895 participants who responded to the nine questions of the PHQ-9, Chronbach's alpha was 0.896 (p < 0.05).
Factor Analysis
To identify and validate the factor structure of the PHQ-9, a split-half exploratory factor analysis (EFA)/confirmatory factor analysis (CFA) was conducted using maximum likelihood estimation with geomin oblique rotation. Each participant was randomly assigned to either the EFA (N = 1,948) or CFA (N = 1,947) group. For the EFA, eigenvalues, factor loadings, and fit indices were evaluated. Only one factor structure yielded an eigenvalue ≥1. All factor loadings for the one factor model had loadings of 0.467 or higher. Factor loadings for the one and two-factor models are presented in Table 2. The one factor structure indicated poor model fit as evidenced by X2 (27, N = 1,948) = 365.396, p < 0.001; CFI and TLI were 0.925 and 0.900, respectively, and SRMR was 0.039. RMSEA = 0.080 (90% CI: 0.073, 0.088) indicated good model fit. EFA indicated some support for a two and three factor structure. However, given the low loadings and cross loadings in the two and three factor structure as well as parsimony, a one-factor structure was determined for this sample. Communalities for each item is presented in Table 2. A CFA was conducted for the other half of the sample, demonstrating poor model fit [X2 (27, N = 1,947) = 417.652, p < 0.001]; the CFI and TLI were 0.932 and 0.910, respectively, and SRMR was 0.039. RMSEA was 0.086 (90% CI: 0.079, 0.094) and indicated mediocre fit. It should be noted that Bentler and Bonnet (27) found that large sample size can influence goodness of fit in chi-square models.
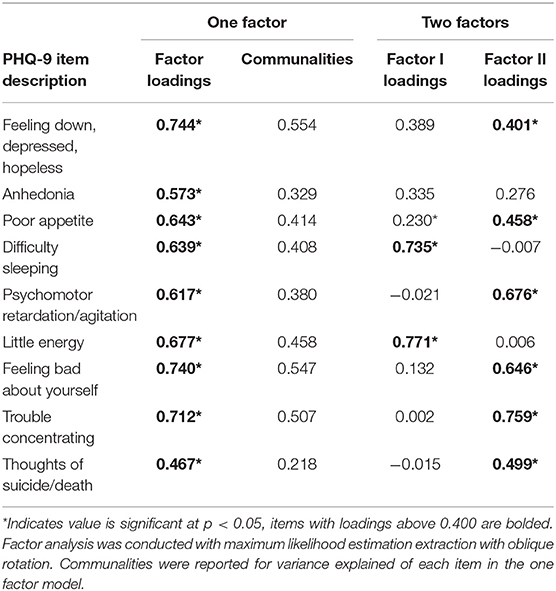
Table 2. Results of exploratory factor analysis.
Differences in Scores Based on Demographic Variables
To analyze differences caused by demographic characteristics, we examined the distribution of scores. Skew (−0.74) and kurtosis (−0.28) indicated a normal distribution of scores, however; Shapiro-Wilk (W = 0.934, p < 0.01) and the Kolmogorov-Smirnov test (D = 0.12, p < 0.01) indicated non-normally distributed data. Levene's, Fligner-Killeen, and Brown-Forsythe homogeneity tests indicated non-homogeneity of variance for gender and age. To account for the non-normality and heteroscedasticity of variance, non-parametric testing was conducted for further analyses. PHQ-9 total score was evaluated based on the user's demographic characteristics. Given the non-normal distribution of PHQ-9 scores, Kruskal-Wallis ANOVAs were conducted. ANOVAs for all demographic variables were significant at p < 0.05. Results of ANOVA for all demographic characteristics are presented in Table 3 below. For all variables E2 indicate negligible to weak effect size and that demographic variables were predictive of PHQ-9 total score.
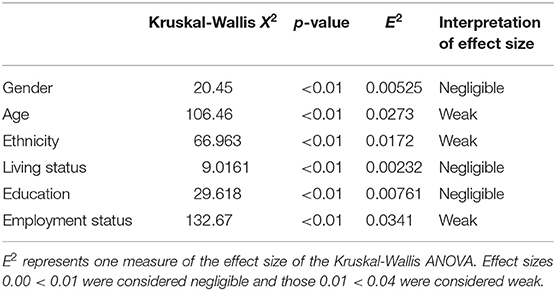
Table 3. Results of Kruskal-Wallis ANOVA examining PHQ-9 total score across demographic variables.
Severity
Since PHQ-9 scores were not normally distributed, breakdown by severity was assessed. The breakdown of participants by severity levels is presented in Table 4. The Severe category had the largest number of participants compared to any other category (N = 1,872, 48.06%) with an average score of 23.78, and was the largest category for most age groups.
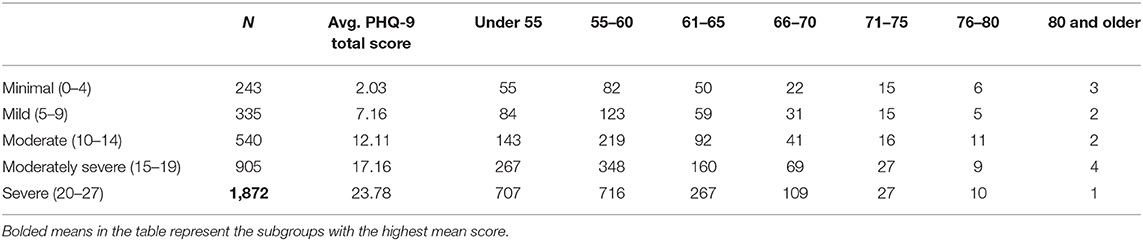
Table 4. Prevalence of severity rates (total N = 3,895).
Discussion
The current study analyzed data from 3,895 adults and older adults who completed the PHQ-9. The majority of which were female, over 55, and around 40% of the sample identified as an ethnicity other than White. Analysis of the psychometric properties of the chatbot version of the PHQ-9 are consistent with psychometrics of the paper and pencil version. A one structure model was found to have good model fit with strong internal consistency. All demographic characteristics analyzed in this study had a significant, but weak effect on the PHQ-9 total score.
Regarding the feasibility of using a chatbot to assess depressive symptoms, two points should be noted. First, the large sample recruited in this study may indicate that individuals were open to completing assessments via chatbot. Additionally, the high completion rate (99.8%) shows that the assessment was relatively easy for participants to complete, including those over 75, indeed, all of the participants over 75 (N = 53) completed the chatbot version of the PHQ-9 correctly. To note, a previous study of a smartphone app version of the PHQ-9 showed a lower completion rate of 73.9% (16). These results show that the chatbot attracted a large sample of adults and older adults, with low education, with a large portion of individuals that were unable to work; and nonetheless yielded high completion rates the PHQ-9. Thus, assessments via chatbots could be considered as a viable modality for assessment delivery for older adults.
The psychometric properties found provide evidence of the validity of the chatbot version of the PHQ-9. The internal reliability was 0.896 which indicated good reliability between items. The EFA and CFA showed that a one factor structure was most appropriate even though there was some support for two and three factor structures. However, given the support for a one factor structure for ethnically diverse samples in a paper version of the PHQ-9 (8, 9, 12), low loadings or cross loadings in the two and three factor structure, and parsimony, a one-factor structure was determined for this sample. All factor loadings for the one factor model had loadings of 0.467 or higher. The item with the highest factor loading was feeling depressed (0.744) and the lowest was thoughts of death (0.467). Since dysphoria is one of the main symptoms of depression, it was expected that this item would have one of the highest loadings in a single factor structure. Interestingly, Fiske et al. (28) found that older adults (over 65 years of age) are less likely to present symptoms of dysphoria and much more likely to report loss of interest in life and somatic symptoms. It is possible that this difference is explained by the inclusion of adults (under 55) and older adults in this study and that the recruitment ads focused on sadness and loneliness.
There were no to weak differences in scores when analyzed by demographic characteristics. Gender, age, ethnicity, living status, education, and employment status were not strong predictors of PHQ-9 total scores. Though the sample was diverse, the differences in group sizes may be what led to this finding. Future studies should prioritize including a representative sample to understand more about the relationship between demographic characteristics and PHQ-9 total score.
Due to COVID-19, there is a need for digital assessments to address the immediate mental and physical health needs of patients of all ages, especially the older ones that are at a higher risk. Completing a paper and pencil assessment and even exchanging a tablet with a preloaded assessment in the waiting room may increase disease transmission. This study shows that adults and older adults were able to complete the PHQ-9 on their personal device which represents a safer alternative. Additionally, the psychometric properties of the chatbot version of the PHQ-9 support the integration of this assessment in the studies utilizing chatbots to treat depression.
Limitations
One limitation in this study was that only the chatbot version of the PHQ-9 was administered. Future studies on chatbot administrations of the PHQ-9 should compare reliability between a paper version and chatbot version as was done previously with the computer format of the PHQ-9 (7) and touch screen computer version (15). Additionally, construct validity and criterion validity have not been assessed, thus these findings should be interpreted as preliminary.
Regarding the sample of participants, since the majority were female the results may not generalize to adults of other genders. While over 40% of the sample reported an ethnicity other than White, studies with more diverse samples are needed. Additionally, age was assessed categorically rather than continuously with the youngest age option being “<55.” For the 32.34% of the final sample who indicated they were younger than 55, the variance and lowest age is not known. Thus, future studies should assess age continuously.
Lastly, participants in this study were recruited through Facebook and engaged with the chatbot only through Facebook Messenger. Thus, the results of this study should be interpreted with caution as it may not generalize to older adults who are less technologically savvy. To gain a better understanding of older adults' openness to interacting with the chatbot version of the PHQ-9, recruitment efforts may need to be diversified beyond Facebook.
Conclusions
Finding a low cost and scalable format to deliver depression screeners would allow large numbers of people to be assessed. The current study showed that the PHQ-9 delivered through a chatbot was reliable and presented a one factor structure with depressed mood as the item with the highest loading. These findings provide preliminary support to the utilization of a chatbot version of the PHQ-9 for the assessment of depression for adults and older adults which represents a safe assessment method during the current pandemic.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Palo Alto University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. Depression. (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/depression (accessed December 12, 2020).
2. Barua A, Ghosh MK, Kar N, Basilio MA. Prevalence of depressive disorders in the elderly. Ann Saudi Med. (2011) 31:620–4. doi: 10.4103/0256-4947.87100
3. Conner KO, Copeland VC, Grote NK, Koeske G, Rosen D, Reynolds CF, et al. Mental health treatment seeking among older adults with depression: the impact of stigma and race. Am J Geriatr Psychiatry. (2010) 18:531–43. doi: 10.1097/JGP.0b013e3181cc0366
4. Crystal S, Sambamoorthi U, Walkup JT, Akincigil A. Diagnosis and treatment of depression in the elderly medicare population: predictors, disparities, and trends: diagnosis and treatment of depression. J Am Geriatr Soc. (2003) 51:1718–28. doi: 10.1046/j.1532-5415.2003.51555.x
5. Smith R, Meeks S. Screening older adults for depression: barriers across clinical discipline training. Innov Aging. (2019) 3:igz011. doi: 10.1093/geroni/igz011
6. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
7. Erbe D, Eichert H-C, Rietz C, Ebert D. Interformat reliability of the patient health questionnaire: validation of the computerized version of the PHQ-9. Internet Interv. (2016) 5:1–4. doi: 10.1016/j.invent.2016.06.006
8. Huang FY, Chung H, Kroenke K, Delucchi KL, Spitzer RL. Using the patient health questionnaire-9 to measure depression among racially and ethnically diverse primary care patients. J Gen Intern Med. (2006) 21:547–52. doi: 10.1111/j.1525-1497.2006.00409.x
9. Yu X, Tam WWS, Wong PTK, Lam TH, Stewart SM. The Patient Health Questionnaire-9 for measuring depressive symptoms among the general population in Hong Kong. Compr Psychiatry. (2012) 53:95–102. doi: 10.1016/j.comppsych.2010.11.002
10. Zhong Q, Gelaye B, Rondon M, Sánchez SE, García PJ, Sánchez E, et al. Comparative performance of Patient Health Questionnaire-9 and Edinburgh Postnatal Depression Scale for screening antepartum depression. J Affect Disord. (2014) 162:1–7. doi: 10.1016/j.jad.2014.03.028
11. Shahid Z, Kalayanamitra R, McClafferty B, Kepko D, Ramgobin D, Patel R, et al. COVID-19 and older adults: what we know. J Am Geriatr Soc. (2020) 68:926–9. doi: 10.1111/jgs.16472
12. Dum M, Pickren J, Sobell LC, Sobell MB. Comparing the BDI-II and the PHQ-9 with outpatient substance abusers. Addict Behav. (2008) 33:381–7. doi: 10.1016/j.addbeh.2007.09.017
13. Chen I-P, Liu S-I, Huang H-C, Sun F-J, Huang C-R, Sung M-R, et al. Validation of the patient health questionnaire for depression screening among the elderly patients in Taiwan. Int J Gerontol. (2016) 10:193–7. doi: 10.1016/j.ijge.2016.05.002
14. Beard C, Hsu KJ, Rifkin LS, Busch AB, Björgvinsson T. Validation of the PHQ-9 in a psychiatric sample. J Affect Disord. (2016) 193:267–73. doi: 10.1016/j.jad.2015.12.075
15. Fann JR, Berry DL, Wolpin S, Austin-Seymour M, Bush N, Halpenny B, et al. Depression screening using the Patient Health Questionnaire-9 administered on a touch screen computer. Psychooncology. (2009) 18:14–22. doi: 10.1002/pon.1368
16. BinDhim NF, Hawkey A, Trevena L. A systematic review of quality assessment methods for smartphone health apps. Telemed E-Health. (2015) 21:97–104. doi: 10.1089/tmj.2014.0088
17. Spangenberg L, Glaesmer H, Boecker M, Forkmann T. Differences in Patient Health Questionnaire and Aachen Depression Item Bank scores between tablet versus paper-and-pencil administration. Qual Life Res. (2015) 24:3023–32. doi: 10.1007/s11136-015-1040-5
18. Coons SJ, Gwaltney CJ, Hays RD, Lundy JJ, Sloan JA, Revicki DA, et al. Recommendations on evidence needed to support measurement equivalence between Electronic and Paper-Based Patient-Reported Outcome (PRO) measures: ISPOR ePRO Good Research Practices Task Force Report. Value Health. (2009) 12:419–29. doi: 10.1111/j.1524-4733.2008.00470.x
19. Weigold A, Weigold IK, Natera SN. Response rates for surveys completed with paper-and-pencil and computers: using meta-analysis to assess equivalence. Soc Sci Comput Rev. (2019) 37:649–68. doi: 10.1177/0894439318783435
20. Caballer A, Belmonte O, Castillo A, Gasco A, Sansano E, Montoliu R. Equivalence of chatbot and paper-and-pencil versions of the De Jong Gierveld loneliness scale. Curr Psychol. (2020) 1–8. doi: 10.1007/s12144-020-01117-0
21. Dosovitsky G, Pineda BS, Jacobson NC, Chang C, Escoredo M, Bunge EL. Artificial intelligence chatbot for depression: descriptive study of usage. JMIR Form Res. (2020) 4:e17065. doi: 10.2196/17065
22. Fitzpatrick KK, Darcy A, Vierhile M. Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (Woebot): a randomized controlled trial. JMIR Ment Health. (2017) 4:e7785. doi: 10.2196/mental.7785
23. Fulmer R, Joerin A, Gentile B, Lakerink L, Rauws M. Using psychological artificial intelligence (Tess) to relieve symptoms of depression and anxiety: randomized controlled trial. JMIR Ment Health. (2018) 5:e64. doi: 10.2196/mental.9782
24. Arrabales R. Perla: a conversational agent for depression screening in digital ecosystems. design, implementation and validation. ArXiv 200812875 Cs (2020). doi: 10.31234/osf.io/nfas4
25. Kline RB. Principles and Practice of Structural Equation Modeling. 4th ed. New York, NY: The Guilford Press (2016).
26. Hooper D, Coughlan J, Mullen M. Structural equation modeling: guidelines for determining model fit. Electron J Bus Res Methods. (2007) 6:53–60. doi: 10.21427/D7CF7R
27. Bentler P, Bonett D. Significance tests and goodness-of-fit in analysis of covariance structures. Psychol Bull. (1980) 88:588–606. doi: 10.1037/0033-2909.88.3.588
Keywords: chatbot, assessment, PHQ-9, mobile health, depression
Citation: Dosovitsky G, Kim E and Bunge EL (2021) Psychometric Properties of a Chatbot Version of the PHQ-9 With Adults and Older Adults. Front. Digit. Health 3:645805. doi: 10.3389/fdgth.2021.645805
Received: 24 December 2020; Accepted: 06 April 2021;
Published: 30 April 2021.
Edited by:
David Daniel Ebert, University of Erlangen Nuremberg, GermanyReviewed by:
Ram Bajpai, Keele University, United KingdomMarvin Franke, Friedrich-Alexander Universität Erlangen-Nürnberg, Germany
Copyright © 2021 Dosovitsky, Kim and Bunge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo L. Bunge, ZWJ1bmdlQHBhbG9hbHRvdS5lZHU=